S-4/A: Registration of securities issued in business combination transactions
Published on October 30, 2017
As filed with the Securities and Exchange Commission on October 30, 2017
Registration No. 333-219898
SECURITIES AND EXCHANGE COMMISSION
WASHINGTON, D.C. 20549
AMENDMENT NO. 1
TO
FORM S-4
REGISTRATION STATEMENT
UNDER
THE SECURITIES ACT OF 1933
APOLLO MEDICAL HOLDINGS, INC.
(Exact name of registrant as specified in its charter)
|
Delaware (State or Other Jurisdiction of Incorporation or Organization) |
8742 (Primary Standard Industrial Classification Code Number) |
20-8046599 (I.R.S. Employer Identification Number) |
700 N. Brand Blvd., Suite 1400
Glendale, CA 91203
(818) 396-8050
(Address, Including Zip Code, and Telephone Number,
Including Area Code, of Registrant’s Principal Executive Offices)
Warren Hosseinion, M.D.
Chief Executive Officer
Apollo Medical Holdings, Inc.
700 N. Brand Blvd., Suite 1400
Glendale, CA 91203
(818) 396-8050
(Name, address, including zip code, and telephone
number, including area code, of agent for service)
Copies to:
|
Mark Mihanovic, Esq. Paul Carr-Rollitt, Esq. Gary Emmanuel, Esq. McDermott Will & Emery LLP 2049 Century Park East, 38th Floor Los Angeles, CA 90067 (310) 277-4110 |
Thomas Lam, M.D. Chief Executive Officer Network Medical Management, Inc. 1668 S. Garfield Avenue Alhambra, CA 91801 (626) 282-0288 |
Tin Kin Lee, Esq. Tin Kin Lee Law Offices 1811 Fair Oaks Avenue South Pasadena, CA 91030 (626) 229-9828 |
Approximate date of commencement of proposed sale to the public: As soon as practicable after this Registration Statement is declared effective and all other conditions to the transaction contemplated by the Agreement and Plan of Merger, dated as of December 21, 2016, as amended on March 30, 2017 and October 17, 2017, described in the enclosed joint proxy statement/prospectus have been satisfied or waived.
If the securities being registered on this Form are being offered in connection with the formation of a holding company and there is compliance with General Instruction G, check the following box. ¨
If this Form is filed to register additional securities for an offering pursuant to Rule 462(b) under the Securities Act, check the following box and list the Securities Act registration statement number of the earlier effective registration statement for the same offering. ¨
If this Form is a post-effective amendment filed pursuant to Rule 462(d) under the Securities Act, check the following box and list the Securities Act registration statement number of the earlier effective registration statement for the same offering. ¨
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company or an emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company” and “emerging growth company” in Rule 12b-2 of the Exchange Act.
| Large accelerated filer ¨ | Accelerated filer ¨ |
| Non-accelerated filer ¨ (Do not check if a smaller reporting company) | Smaller reporting company x |
| Emerging Growth company ¨ |
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 7(a)(2)(B) of the Securities Act ☐
If applicable, place an X in the box to designate the appropriate rule provision relied upon in conducting this transaction:
| Exchange Act Rule 13e-4(i) (Cross-Border Issuer Tender Offer) | ¨ |
| Exchange Act Rule 14d-1(d) (Cross-Border Third-Party Tender Offer) | ¨ |
CALCULATION OF REGISTRATION FEE
|
Title of each class of securities to be registered |
Amount to be registered |
Proposed maximum offering price per share |
Proposed maximum aggregate offering price |
Amount
of registration fee (1) |
||||||||||||
| Shares of common stock, $0.001 par value | 38,640,879 | (2)(3) | N/A | $ | 5,184,447 | (4) | $ | 645.46 | ||||||||
| Warrants to purchase shares of common stock | 1,750,000 | (5) | N/A | N/A | (6 | ) | ||||||||||
| Shares of common stock, $0.001 par value, issuable upon exercise of the warrants | 1,750,000 | (3)(7) | N/A | $ | 18,350,000 | (8) | $ | 2,284.58 | (9) | |||||||
| (1) | This fee has been calculated pursuant to Section 6(b) of the Securities Act of 1933, as amended, at a rate equal to $124.50 per $1,000,000 of the proposed maximum aggregate offering price. |
| (2) | Relates to common stock of Apollo Medical Holdings, Inc. (“ApolloMed”), issuable to holders of common stock of Network Medical Management, Inc. (“NMM”), in the proposed merger (the “Merger”) of Apollo Acquisition Corp., a wholly owned subsidiary of the registrant, with and into NMM, with NMM continuing as the surviving corporation. The amount of ApolloMed common stock to be registered includes (i) the estimated maximum number of 32,081,931 shares of ApolloMed common stock that are expected to be issued at the closing of the Merger, (ii) an estimated maximum number of 3,279,474 shares of ApolloMed common stock expected to be issuable to NMM shareholders at closing of the Merger but held back to secure certain indemnification rights of ApolloMed, (iii) an estimated maximum number of 3,279,474 shares of ApolloMed common stock representing the number of shares that may be issued in the future to NMM shareholders (as of closing of the Merger in respect of certain indemnification obligations |
| (3) | Pursuant to Rule 416, this registration statement also covers additional securities that may be issued as a result of stock splits or stock dividends of ApolloMed or similar transactions. |
| (4) | Estimated solely for purposes of calculating the registration fee in accordance with Rule 457(f)(2) of the Securities Act of 1933, as amended, based upon the estimated book value of the NMM shares to be exchanged in the Merger. NMM is a private company, and no market exists for its securities. |
| (5) | Represents warrants to purchase common stock of ApolloMed issuable to holders of common stock of NMM as of the time of the Merger. |
| (6) | In accordance with existing SEC interpretations, the entire registration fee for the warrants is allocated to the ApolloMed common stock registered underlying the warrants, and no separate fee is recorded for the warrants to purchase shares of ApolloMed common stock. |
| (7) | Represents the number of shares of common stock issuable upon exercise of the warrants. |
| (8) | The proposed maximum aggregate offering price of the shares of common stock of ApolloMed issuable upon exercise of the (i) warrants to purchase 850,000 shares of ApolloMed common stock based on the $11.00 per share exercise price of the warrants and the (ii) warrants to purchase 900,000 shares of ApolloMed common stock based on the $10.00 per share exercise price of the warrants. |
| (9) | $1,571.71 previously paid. |
The registrant hereby amends this registration statement on such date or dates as may be necessary to delay its effective date until the registrant shall file a further amendment which specifically states that this registration statement shall thereafter become effective in accordance with Section 8(a) of the Securities Act of 1933 or until the registration statement shall become effective on such date as the Securities and Exchange Commission, acting pursuant to said Section 8(a), may determine.
The information in this joint proxy statement/prospectus is not complete and may be changed. We may not sell these securities until the registration statement filed with the Securities and Exchange Commission is declared effective. This joint proxy statement/prospectus is not an offer to sell these securities and it is not soliciting an offer to buy these securities in any state where the offer or the sale is not permitted.
SUBJECT TO COMPLETION, DATED OCTOBER 30, 2017
PRELIMINARY JOINT PROXY STATEMENT/PROSPECTUS
 |

|
To the stockholders of Apollo Medical Holdings, Inc. and the shareholders of Network Medical Management, Inc.:
On December 21, 2016, Apollo Medical Holdings, Inc., a Delaware corporation (“ApolloMed”), Network Medical Management, Inc., a California corporation (“NMM”), Apollo Acquisition Corp., a California corporation and a wholly owned subsidiary of ApolloMed (“Merger Sub”), and Kenneth Sim (the “Shareholders’ Representative”) entered into an agreement and plan of merger (as amended on March 30, 2017 and October 17, 2017, the “Merger Agreement”) that provides for, among other things, the merger of Merger Sub with and into NMM, with NMM continuing as the surviving entity and a wholly owned subsidiary of ApolloMed, on the terms and conditions set forth in the Merger Agreement (the “Merger”). The boards of directors of each of ApolloMed and NMM have approved the Merger Agreement and the transactions contemplated by the Merger Agreement, including the Merger. If consummated, the Merger will be made effective at the time of filing a certificate of merger (the “Certificate of Merger”) with the Secretary of State of the State of California or at such later time as agreed to by the parties in writing and specified in the Certificate of Merger (the “Effective Time”).
Pursuant to the Merger Agreement, at the Effective Time, each issued and outstanding share of NMM common stock will be converted into the right to receive such number of fully paid and nonassessable ApolloMed shares of common stock that results in the NMM shareholders having a right to receive (A) an aggregate number of shares of ApolloMed common stock that represents 82% of the total issued and outstanding shares of ApolloMed common stock immediately following the Effective Time, assuming there are no NMM dissenting shareholder interests as of the Effective Time, calculated in accordance with the Merger Agreement (see “THE MERGER AGREEMENT – Effects of Merger; Merger Consideration” beginning on page 159), plus (B) an aggregate of 2,566,666 shares of ApolloMed common stock, assuming there are no NMM dissenting shareholder interests as of the Effective Time. In addition, each NMM shareholder shall be entitled to receive such shareholder’s pro rata portion of (i) warrants to purchase an aggregate of 850,000 shares of ApolloMed common stock, exercisable at $11.00 per share and (ii) warrants to purchase an aggregate of 900,000 shares of ApolloMed common stock, exercisable at $10.00 per share. At the Effective Time, pre-Merger ApolloMed stockholders will continue to own and hold their existing shares of ApolloMed common stock. At the Effective Time, ApolloMed will hold back 10% of the total number of shares of ApolloMed common stock issuable to pre-Merger NMM shareholders in the Merger to secure indemnification rights of ApolloMed and its affiliates under the Merger Agreement. Separately, any indemnification of pre-Merger NMM shareholders under the Merger Agreement will be made by the issuance by ApolloMed to pre-Merger NMM shareholders of new additional shares of common stock (capped at the same number of shares of ApolloMed common stock as are subject to the holdback for the indemnification of ApolloMed).
ApolloMed’s common stock is currently quoted on OTC Pink and traded under the symbol “AMEH.” ApolloMed has applied for listing of its common stock on the NASDAQ Global Market effective as of the closing of the Merger. No assurance can be given that ApolloMed’s application will be approved. On December 21, 2016, the last full trading day before the announcement of the Merger, the last reported sale price of ApolloMed common stock was $3.99 per share, and, on [·], 2017, the latest practicable date prior to the date of this joint proxy statement/prospectus, the last reported sale price of ApolloMed common stock was $[·] per share. ApolloMed and NMM urge you to obtain current market quotations for the price of ApolloMed common stock.
The Merger has been structured to qualify as a “reorganization” within the meaning of Section 368(a) of the Internal Revenue Code of 1986, as amended.
| 2 |
ApolloMed and NMM each will hold a special meeting of its shareholders. ApolloMed stockholders will be asked to consider and vote on the following proposals: (i) to approve the Merger between Merger Sub and NMM pursuant to the terms and conditions of the Merger Agreement and the Merger Agreement and the transactions contemplated thereunder, including the issuance of shares of common stock and warrants of ApolloMed to NMM shareholders as merger consideration in the Merger (the “ApolloMed Merger Proposal”); (ii) to approve amendments to the ApolloMed Restated Certificate of Incorporation (the “ApolloMed Charter”) and Restated Bylaws (“ApolloMed Bylaws”) to divide the board of directors of ApolloMed into three classes (the “Board Classification Proposal”); (iii) to elect nine directors to serve as members of ApolloMed’s board for one-year, two-year or three-year terms (the “Election of Directors Proposal”); (iv) to consider and vote on a proposal to approve, in a non-binding advisory vote, certain compensation arrangements for ApolloMed’s named executive officers (the “ApolloMed Compensation Proposal”); and (v) to consider and vote upon a proposal to adjourn the special meeting to a later date or dates, if necessary, to permit the solicitation of additional proxies if, based upon the tabulated vote at the time of the special meeting, there are not sufficient votes to approve one or more proposals presented to ApolloMed stockholders for vote (the “ApolloMed Adjournment Proposal”).
The ApolloMed special meeting will be held on [●], 2017 at [●][a.m.][p.m.], Pacific Standard Time, at 700 N. Brand Blvd., Suite 1400, Glendale, California.
NMM shareholders will be asked to consider and vote on the following proposals: (i) to approve the Merger between NMM and Merger Sub pursuant to the terms and conditions of the Merger Agreement and the transactions contemplated thereunder (the “NMM Merger Proposal”); and (ii) to consider and vote upon a proposal to adjourn the special meeting to a later date or dates, if necessary, to permit the solicitation of additional proxies if, based upon the tabulated vote at the time of the special meeting, there are not sufficient votes to approve one or more proposals presented to ApolloMed shareholders for vote (the “NMM Adjournment Proposal”).
The NMM special meeting will be held on [●], 2017 at [●][a.m.][p.m.], Pacific Standard Time, at 1668 S. Garfield Avenue, Alhambra, California.
Completion of the Merger is conditioned upon the satisfaction or waiver of all closing conditions under the Merger Agreement, including, (i) the adoption and approval of the ApolloMed Merger Proposal, the Board Classification Proposal, and each of the directors in the Election of Directors Proposal by the affirmative vote of holders of (a) a majority of the shares of ApolloMed common stock Series A preferred stock and Series B preferred stock, voting together as one class on an as-converted basis, and (b) a majority of the shares of ApolloMed common stock, Series A preferred stock and Series B preferred stock, voting together as one class on an as-converted basis, not owned by NMM (excluding shares of preferred stock owned by NMM) and (ii) approval of the NMM Merger Proposal by the affirmative vote of NMM shareholders holding at least 95% of the outstanding shares of NMM common stock and representing at least 95% in number of the NMM shareholders.
ApolloMed’s board of directors determined that it is advisable and in the best interest of ApolloMed and its stockholders for ApolloMed to enter into the Merger Agreement and the board authorized and approved the terms of the Merger Agreement and the transactions contemplated thereby, approved the Merger Agreement and recommends that ApolloMed stockholders vote “FOR” the ApolloMed Merger Proposal, “FOR” the Board Classification Proposal, “FOR” each of the directors in the Election of Directors Proposal, “FOR” the ApolloMed Compensation Proposal and “FOR” the ApolloMed Adjournment Proposal.
NMM’s board of directors has determined that it is advisable and in the best interest of NMM and its shareholders to enter into the Merger Agreement, the board has authorized and approved the terms of the Merger Agreement and the transactions contemplated thereby, has approved the Merger Agreement and recommends that NMM shareholders vote “FOR” the NMM Merger Proposal and “FOR” the NMM Adjournment Proposal.
This joint proxy statement/prospectus provides you with important information about the special meetings and about ApolloMed and NMM and the proposed Merger and other transactions and documents related to the Merger.
Please carefully read this entire joint proxy statement/prospectus, including “RISK FACTORS” beginning on page 44.
Your vote is very important. Whether or not you plan to attend the special meeting of ApolloMed or the special meeting of NMM, please take the time to vote by completing and returning the enclosed proxy card to ApolloMed or NMM, as applicable, or by granting your proxy electronically over the Internet or by telephone. If your shares are held in “street name,” you must instruct your broker in order to vote on all proposals.
| 3 |
Sincerely,
| Warren Hosseinion, M.D. | Thomas Lam, M.D. |
| Chief Executive Officer | Chief Executive Officer |
| Apollo Medical Holdings, Inc. | Network Medical Management, Inc. |
Neither the Securities and Exchange Commission nor any state securities commission has approved or disapproved of the ApolloMed common stock to be issued in the Merger or determined if this joint proxy statement/prospectus is accurate or complete. Any representation to the contrary is a criminal offense.
This joint proxy statement/prospectus is dated [●], 2017 and is first being mailed to ApolloMed stockholders and NMM shareholders on or about [●], 2017.
| 4 |
APOLLO MEDICAL HOLDINGS, INC.
700 N. Brand Blvd., Suite 1400
Glendale, CA 91203
NOTICE OF SPECIAL MEETING OF STOCKHOLDERS
TO BE HELD ON [●], 2017
To the Stockholders of Apollo Medical Holdings, Inc.:
NOTICE IS HEREBY GIVEN that a special meeting of the stockholders (the “ApolloMed special meeting”) of Apollo Medical Holdings, Inc., a Delaware corporation (“ApolloMed”), will be held on [●], 2017, at [●][a.m.][p.m.], Pacific Standard Time, at 700 N. Brand Blvd., Suite 1400, Glendale, California 91203, to consider and vote upon the following matters:
(1) The ApolloMed Merger Proposal — to approve the merger between Apollo Acquisition Corp., a California corporation and a wholly owned subsidiary of ApolloMed (“Merger Sub”), and Network Medical Management, Inc., a California corporation (“NMM”), pursuant to the terms and conditions of the Agreement and Plan of Merger (the “Merger Agreement”), dated as of December 21, 2016, as amended on March 30, 2017 and October 17, 2017, among ApolloMed, Merger Sub, NMM and Kenneth Sim, M.D., the Merger Agreement and the transactions contemplated thereunder, including the issuance of shares of common stock and warrants of ApolloMed to NMM shareholders as merger consideration in the Merger (the “ApolloMed Merger Proposal”);
(2) The Board Classification Proposal – to approve amendments to the ApolloMed Restated Certificate of Incorporation (the “ApolloMed Charter”) and Restated Bylaws (“ApolloMed Bylaws”) to divide the board of directors of ApolloMed into three classes (the “Board Classification Proposal”);
(3) The Election of Directors Proposal – to elect nine directors to serve as members of ApolloMed’s board for one-year, two-year or three-year terms (the “Election of Directors Proposal”);
(4) The ApolloMed Compensation Proposal – to consider and vote on a proposal to approve, in a non-binding advisory vote, certain compensation arrangements for ApolloMed’s named executive officers (the “ApolloMed Compensation Proposal”); and
(5) The ApolloMed Adjournment Proposal – to consider and vote upon a proposal to adjourn the special meeting to a later date or dates, if necessary, to permit the solicitation of additional proxies if, based upon the tabulated vote at the time of the special meeting, there are not sufficient votes to approve one or more proposals presented to stockholders for vote (the “ApolloMed Adjournment Proposal”).
ApolloMed’s board has fixed the close of business on [●], 2017, as the record date for the special meeting. Only holders of record of shares of ApolloMed common stock and Series A preferred stock and Series B preferred stock at the close of business on such date are entitled to receive notice of, and vote at, the special meeting or at any postponement(s) or adjournment(s) of the special meeting. A complete list of ApolloMed’s stockholders of record entitled to vote at the special meeting will be available for 10 days before the special meeting at our principal executive office for inspection by stockholders during ordinary business hours for any purpose germane to the special meeting.
Approval of each of the ApolloMed Merger Proposal, the Board Classification Proposal and each of the directors in the Election of Directors Proposal requires the affirmative vote of holders of (i) a majority of the shares of ApolloMed common stock and Series A preferred stock and Series B preferred stock, voting together as one class on an as-converted basis, and (ii) a majority of the shares of ApolloMed common stock, Series A preferred stock and Series B preferred stock, voting together as one class on an as-converted basis, not owned by NMM. The ApolloMed Compensation Proposal and the ApolloMed Adjournment Proposal requires the affirmative vote of a majority of the shares of ApolloMed stock entitled to vote present in person or represented by proxy at the ApolloMed special meeting.
| 5 |
APOLLOMED’S BOARD DETERMINED THAT IT IS ADVISABLE AND IN THE BEST INTEREST OF APOLLOMED AND ITS STOCKHOLDERS TO ENTER INTO THE MERGER AGREEMENT AND THE BOARD HAS AUTHORIZED AND APPROVED THE TERMS OF THE MERGER AGREEMENT AND THE TRANSACTIONS CONTEMPLATED THEREBY. APOLLOMED’S BOARD APPROVED THE MERGER AGREEMENT AND RECOMMENDS THAT APOLLOMED STOCKHOLDERS VOTE “FOR” THE APOLLOMED MERGER PROPOSAL, “FOR” THE BOARD CLASSIFICATION PROPOSAL, “FOR” EACH OF THE DIRECTORS IN THE ELECTION OF DIRECTORS PROPOSAL, “FOR” THE APOLLOMED COMPENSATION PROPOSAL AND “FOR” THE APOLLOMED ADJOURNMENT PROPOSAL
Your vote is very important. If your shares are registered in your name as a stockholder of record of ApolloMed, whether or not you expect to attend the special meeting, please sign and return the enclosed proxy card promptly in the envelope provided or promptly submit your proxy by telephone or over the Internet following the instructions on the proxy card, to ensure that your shares will be represented at the special meeting.
If your shares are held in “street name” through a broker, trust, bank or other nominee, and you received the notice of the special meeting through your broker or through another intermediary, please complete and return the materials in accordance with the instructions provided to you by such broker or other intermediary to instruct such broker or other intermediary how to vote your shares or contact your broker or other intermediary directly in order to obtain a proxy issued to you by your nominee holder to attend the special meeting and vote in person. Failure to do so may result in your shares not being eligible to be voted by proxy at the special meeting.
You may revoke a proxy at any time prior to its exercise at the meeting by following the instructions in the enclosed joint proxy statement/prospectus.
IMPORTANT NOTICE REGARDING THE AVAILABILITY OF PROXY MATERIALS FOR THE SPECIAL MEETING OF STOCKHOLDERS TO BE HELD ON [●], 2017: This notice is not a form for voting and presents only an overview of the more complete joint proxy statement/prospectus. We urge you to read the accompanying joint proxy statement/prospectus, including its annexes and the section entitled “RISK FACTORS” beginning on page 44, carefully and in their entirety. Copies of the joint proxy statement/prospectus and the accompanying proxy card are available, without charge on the internet at http://irdirect.net/AMEH/sec_filings and www.proxyvote.com, respectively, and can be obtained by calling (818) 396-8050 or sending an e-mail to Investors@apollomed.net. To obtain timely delivery, ApolloMed stockholders must request the materials no later than five business days prior to the ApolloMed special meeting. If you have any questions concerning the proposals, the ApolloMed special meeting of stockholders or the accompanying joint proxy statement/prospectus or need help voting your shares of ApolloMed capital stock, please contact Mihir Shah at (818) 396-8050.
| By Order of the Board of Directors, | |
| /s/ Gary Augusta | |
| Gary Augusta | |
| Chairman of the Board of Directors |
[●], 2017
| 6 |
NETWORK MEDICAL MANAGEMENT, INC.
1668 S. Garfield Avenue, 3rd Floor
Alhambra, CA, 91801
NOTICE OF SPECIAL MEETING OF SHAREHOLDERS
TO BE HELD ON [●], 2017
To the Shareholders of Network Medical Management, Inc.:
NOTICE IS HEREBY GIVEN that a special meeting of the shareholders (the “NMM special meeting”) of Network Medical Management, Inc., a California corporation (“NMM”) will be held on [●], 2017, at [●][a.m.][p.m.], Pacific Standard Time, at 1668 S. Garfield Avenue, 3rd Floor, Alhambra, California 91801, to consider and vote upon the following matters:
(1) The NMM Merger Proposal – to approve the merger between NMM and Apollo Acquisition Corp., a California corporation (“Merger Sub”), pursuant to the terms and conditions of the Agreement and Plan of Merger (the “Merger Agreement”), dated as of December 21, 2016, as amended on March 30, 2017 and October 17, 2017, among Apollo Medical Holdings, Inc., a Delaware corporation (“ApolloMed”), the Merger Sub, NMM and Kenneth Sim, M.D., as the shareholders’ representative, the Merger Agreement and the transactions contemplated thereunder (the “NMM Merger Proposal”); and
(2) The NMM Adjournment Proposal – to consider and vote upon a proposal to adjourn the special meeting to a later date or dates, if necessary, to permit the solicitation of additional proxies if, based upon the tabulated vote at the time of the special meeting, there are not sufficient votes to approve one or more proposals presented to shareholders for vote (the “NMM Adjournment Proposal”).
NMM’s board of directors has fixed the close of business on [●], 2017 as the record date for the special meeting. Only holders of record of shares of NMM common stock at the close of business on such date are entitled to receive notice of, and vote at, the special meeting or at any postponement(s) or adjournment(s) of the special meeting. A complete list of our shareholders of record entitled to vote at the special meeting will be available for 10 days before the special meeting at NMM’s principal executive office for inspection by shareholders during ordinary business hours for any purpose germane to the special meeting.
Eddie Lam, M.D., Thomas Lam, M.D., Su Kin Lee, M.D., Kenneth Sim, M.D., Theresa Tseng, M.D., Yang Chern Tseng, M.D., and Albert Young, M.D. have each entered into an agreement with ApolloMed pursuant to which each has agreed to vote all of the shares of NMM common stock owned or controlled by them in favor of the NMM Merger Proposal and the Merger Agreement. As of the close of business on [●], 2017, the record date for the special meeting, Eddie Lam, M.D., Thomas Lam, M.D., Su Kin Lee, M.D., Kenneth Sim, M.D., Theresa Tseng, M.D., Yang Chern Tseng, M.D., and Albert Young, M.D. collectively owned, directly or indirectly, [●] shares of NMM common stock, which represented approximately [●]% of the outstanding shares of NMM common stock.
Approval of the NMM Merger Proposal requires the affirmative vote of NMM shareholders holding at least 95% of the outstanding shares of NMM common stock and representing at least 95% in number of the NMM shareholders. The NMM Adjournment Proposal requires the affirmative vote of a majority of the outstanding shares of NMM stock entitled to vote present in person or represented by proxy at the NMM special meeting.
You are entitled to the right to seek appraisal of the fair value of your shares of NMM common stock under Chapter 13 of the California Corporations Code. A summary of the dissenters’ rights that may be available to you are described in “THE MERGER – Dissenters’ Rights” on page 154.
NMM’S BOARD DETERMINED THAT IT IS ADVISABLE AND IN THE BEST INTEREST OF NMM AND ITS SHAREHOLDERS TO ENTER INTO THE MERGER AGREEMENT AND THE BOARD HAS AUTHORIZED AND APPROVED THE TERMS OF THE MERGER AGREEMENT AND THE TRANSACTIONS CONTEMPLATED THEREBY. NMM’S BOARD APPROVED THE MERGER AGREEMENT AND RECOMMENDS THAT NMM SHAREHOLDERS VOTE “FOR” THE NMM MERGER PROPOSAL AND “FOR” THE NMM ADJOURNMENT PROPOSAL.
| 7 |
Your vote is very important. Whether or not you expect to attend the special meeting, please sign and return the enclosed proxy card promptly in the envelope provided to ensure that your shares will be represented at the special meeting.
You may revoke a proxy at any time prior to its exercise at the meeting by following the instructions in the enclosed joint proxy statement/prospectus.
IMPORTANT NOTICE REGARDING THE AVAILABILITY OF PROXY MATERIALS FOR THE SPECIAL MEETING OF SHAREHOLDERS TO BE HELD ON [●], 2017: This notice is not a form for voting and presents only an overview of the more complete joint proxy statement/prospectus. We urge you to read the accompanying joint proxy statement/prospectus, including its annexes and the section entitled “RISK FACTORS” beginning on page 44, carefully and in their entirety. Copies of the joint proxy statement/prospectus and the accompanying proxy card can be obtained, without charge, by calling (626) 229-9828 or sending an e-mail to tlee@tinkinlee.com. To obtain timely delivery, NMM shareholders must request the materials no later than 5 business days prior to the NMM special meeting. If you have any questions concerning the proposals, the NMM special meeting or the accompanying joint proxy statement/prospectus or need help voting your shares of NMM common stock, please contact Tin Kin Lee at (626) 229-9828.
| By Order of the Board of Directors, | |
| /s/ Kenneth Sim | |
| Kenneth Sim | |
| Chairman of the Board of Directors |
| 8 |
REFERENCE TO ADDITIONAL INFORMATION
This joint proxy statement/prospectus incorporates important business and financial information about ApolloMed that is not included in or delivered with this document. Additional information about ApolloMed is available to you without charge upon your request. You can obtain any of the documents filed with or furnished to the Securities and Exchange Commission, or the “SEC,” by ApolloMed at no cost from the SEC’s website at http://www.sec.gov. You may also request copies of these documents at no cost by requesting them in writing or by telephone at the following address and telephone number:
Apollo Medical Holdings, Inc.:
700 N. Brand Blvd., Suite 1400
Glendale, CA 91203
Attention: Corporate Secretary
Telephone: (818) 396-8050
E-mail: tthai@apollomed.net
To obtain timely delivery of these documents, you must request them no later than five business days before the date of the special meeting. This means that Apollo stockholders should request documents by [●], 2017 and NMM shareholders requesting documents must do so by [●], 2017.
You should rely only on the information contained in this document. No one has been authorized to provide you with information that is different from that contained in this document. This document is dated [●], 2017, and you should assume that the information in this document is accurate only as of such date. Neither the mailing nor delivery of this document to ApolloMed stockholders or NMM shareholders nor the issuance by ApolloMed of shares of ApolloMed common stock in connection with the Merger will create any implication to the contrary.
ABOUT THIS JOINT PROXY STATEMENT/PROSPECTUS
This joint proxy statement/prospectus, which forms a part of a registration statement on Form S-4 filed with the SEC by ApolloMed (File No. 333-219898), constitutes a prospectus of ApolloMed under Section 5 of the Securities Act of 1933, as amended, with respect to the shares of ApolloMed common stock to be issued to the NMM shareholders in connection with the Merger. This joint proxy statement/prospectus does not contain all of the information included in the registration statement, certain items of which are contained in schedules and exhibits to the registration statement as permitted by the rules and regulations of the SEC. You should refer to the registration statement and its exhibits to read that information. Statements made in this joint proxy statement/prospectus as to certain of ApolloMed’s contracts, agreements or other documents referred to are not necessarily complete and you should refer to the exhibits attached to the registration statement for copies of the actual contract, agreement or other document. This information is available by mail from the Public Reference Room of the SEC and at the Internet website that the SEC maintains, as well as from other sources, including from ApolloMed at the address provided above.
This joint proxy statement/prospectus also constitutes a notice of meeting and a proxy statement with respect to an ApolloMed special meeting of stockholders, at which time ApolloMed stockholders will be asked to consider and vote upon certain proposals as further described herein. This joint proxy statement/prospectus also constitutes a notice of meeting and a proxy statement with respect to a NMM special meeting of shareholders, at which time NMM shareholders will be asked to consider and vote upon certain proposals as further described herein.
You should rely only on the information contained in this joint proxy statement/prospectus to vote your shares. Neither ApolloMed nor NMM has authorized anyone to give any information or make any representation about the Merger, ApolloMed or NMM that is different from, or in addition to, the information or representations contained in this joint proxy statement/prospectus. Therefore, if anyone does give you information or representations of this sort, you should not rely on it or them. The information contained in this joint proxy statement/prospectus speaks only as of the date of this document unless the information specifically indicates that another date applies.
| 9 |
This joint proxy statement/prospectus does not constitute an offer to sell, or a solicitation of an offer to buy, any securities, or the solicitation of a proxy, in any jurisdiction to any person or entity to whom it is unlawful to make any such offer or solicitation. Information contained in this joint proxy statement/prospectus regarding ApolloMed or its affiliates has been provided by ApolloMed and information contained in this joint proxy statement/prospectus regarding NMM or its affiliates has been provided by NMM.
| 10 |
TABLE OF CONTENTS
| 11 |
| 12 |
| 13 |
| 14 |
| 15 |
QUESTIONS AND ANSWERS
The following are answers to some questions that you, as an ApolloMed stockholder or NMM shareholder, may have regarding the proposed merger and the other proposals being considered. We urge you to carefully read this entire joint proxy statement/prospectus, including the annexes, because the information in this section does not provide all the information that might be important to you.
Unless the context otherwise requires, references in this joint proxy statement/prospectus to “ApolloMed” refers to Apollo Medical Holdings, Inc., a Delaware corporation, “Merger Sub” refers to Apollo Acquisition Corp., a California corporation and a wholly owned subsidiary of ApolloMed, and “NMM” refers to Network Medical Management, Inc., a California corporation.
QUESTIONS AND ANSWERS ABOUT THE MERGER
Q: Why am I receiving this joint proxy statement/prospectus?
A: You are receiving this joint proxy statement/prospectus because ApolloMed, Apollo Acquisition Corp., NMM and Kenneth Sim, M.D. (the “Shareholders’ Representative”) have signed an Agreement and Plan of Merger, dated as of December 21, 2016, as amended on March 30, 2017 and on October 17, 2017 (the “Merger Agreement”), which is described in more detail in this joint proxy statement/prospectus. In connection with the merger and as contemplated by the Merger Agreement, the stockholders of ApolloMed and the shareholders of NMM are being asked to vote upon certain proposals as further described herein.
This joint proxy statement/prospectus contains important information about the merger and the proposals being voted on by ApolloMed stockholders and NMM shareholders, and you should read it carefully. This document collectively serves as a joint proxy statement of ApolloMed and NMM and a prospectus of ApolloMed. It is a joint proxy statement because both the ApolloMed board of directors (the “ApolloMed board” or the “ApolloMed board of directors”) and NMM board of directors (the “NMM board” or the “NMM board of directors”) are soliciting proxies from their respective shareholders. It is a prospectus because ApolloMed will issue shares of ApolloMed common stock to NMM shareholders in connection with the merger. Your vote is important. You are encouraged to submit your proxy as soon as possible after carefully reviewing this joint proxy/prospectus and its annexes.
A complete copy of the Merger Agreement is attached to this joint proxy statement/prospectus as Annex A or a more complete discussion of the proposed merger, its effects and the other transactions contemplated by the Merger Agreement, see “The Merger.”
Q: What will happen in the merger?
A: At the closing of the merger, Merger Sub will merge with and into NMM, with NMM continuing as the surviving entity and a wholly owned subsidiary of ApolloMed (the “Merger”). The surviving entity and ApolloMed are collectively referred to in this joint proxy statement/prospectus as the “combined company.” If consummated, the Merger will be made effective by filing a certificate of merger (the “Certificate of Merger”) with the Secretary of State of the State of California or at such later time as agreed to by the parties in writing and specified in the Certificate of Merger (the “Effective Time”).
Pursuant to the Merger Agreement, at the Effective Time, each issued and outstanding share of NMM common stock will be converted into the right to receive such number of fully paid and nonassessable ApolloMed shares of common stock that results in the NMM shareholders having a right to receive (A) an aggregate number of shares of ApolloMed common stock that represents 82% of the total issued and outstanding shares of ApolloMed common stock immediately following the Effective Time, assuming there are no NMM dissenting shareholder interests as of the Effective Time, calculated in accordance with the Merger Agreement (see “THE MERGER AGREEMENT – Effects of Merger; Merger Consideration” beginning on page 159), plus (B) an aggregate of 2,566,666 shares of ApolloMed common stock, assuming there are no NMM dissenting shareholder interests as of the Effective Time (the “Additional Shares”). In addition, each NMM shareholder shall be entitled to receive such shareholder’s pro rata portion of (i) warrants to purchase an aggregate of 850,000 shares of ApolloMed common stock, exercisable at $11.00 per share and (ii) warrants to purchase an aggregate of 900,000 shares of ApolloMed common stock, exercisable at $10.00 per share (collectively, the “Warrant Consideration”). At the Effective Time, pre-Merger ApolloMed stockholders will continue to own and hold their existing shares of ApolloMed common stock. At the Effective Time, ApolloMed will hold back 10% of the total number of shares of ApolloMed common stock issuable to pre-Merger NMM shareholders in the Merger to secure indemnification of ApolloMed and its affiliates under the Merger Agreement (the “Holdback Shares”). Separately, indemnification of pre-Merger NMM shareholders under the Merger Agreement will be made by the issuance by ApolloMed to pre-Merger NMM shareholders of new additional shares of common stock (capped at the same number of shares of ApolloMed common stock as the Holdback Shares). For a more complete description of what NMM shareholders will receive in the Merger, please see the section “THE MERGER AGREEMENT — Effects of Merger; Merger Consideration” in this joint proxy statement/prospectus.
| 16 |
Q: When do ApolloMed and NMM expect to complete the Merger?
A: ApolloMed and NMM anticipate that the Merger will be consummated promptly following the ApolloMed and NMM special meetings, provided that all other conditions to the consummation of the Merger in the Merger Agreement have been satisfied or waived. However, it is possible that the failure to timely meet the closing conditions specified in the Merger Agreement or other factors outside of the control of ApolloMed or NMM control could require ApolloMed and NMM to complete the Merger at a later time or not at all. See “THE MERGER AGREEMENT — Conditions to Completion of the Merger” on page 166 of this joint proxy statement/prospectus for a more complete summary of the conditions that must be satisfied prior to closing.
Q: Why are the two companies proposing to merge?
ApolloMed and NMM believe that the combined company following the Merger will have the potential to establish a leading position in the population health management market. ApolloMed and NMM believe that the combined company will have the following potential advantages: (i) increased and synergistic operational expertise and capabilities, increased scale, including financial, clinical, network size as well as the aforementioned operational attributes, which would potentially create near and long-term value for both ApolloMed stockholders and NMM shareholders; (ii) an experienced management team; and (iii) the potential to access additional sources of capital. For a discussion of ApolloMed and NMM reasons for the Merger, please see the section entitled “The Merger — ApolloMed’s Reasons for the Merger” and “The Merger —NMM’s Reasons for the Merger” in this joint proxy statement/prospectus.
Q: What do I need to do now?
A: After you have carefully read this joint proxy statement/prospectus and have decided how you wish to vote your shares, please authorize a proxy to vote your shares promptly so that your shares are represented and voted at the ApolloMed and NMM special meeting.
QUESTIONS AND ANSWERS FOR APOLLOMED STOCKHOLDERS
Q: What will I receive in the Merger?
A: If the Merger is completed, ApolloMed stockholders will not receive any consideration in the Merger and will continue to hold the shares of ApolloMed common stock that they hold immediately prior to the Merger.
ApolloMed’s common stock is currently quoted on OTC Pink and traded under the symbol “AMEH.” ApolloMed has applied for listing of its common stock on the NASDAQ Global Market effective as of the closing of the Merger. No assurance can be given that ApolloMed’s application will be approved. On December 21, 2016, the last full trading day before the announcement of the Merger, the last reported sale price of ApolloMed common stock was $3.99 per share, and, on [●], 2017, the latest practicable date prior to the date of this joint proxy statement/prospectus, the last reported sale price of ApolloMed common stock was $[●] per share.
ApolloMed stockholders will experience significant dilution as a result of the issuance of ApolloMed common stock and warrants to the NMM shareholders as merger consideration in connection with the Merger.
Immediately following completion of the Merger, the current ApolloMed stockholders will continue to hold 6,033,495 shares, or 16.7% of the outstanding common stock of ApolloMed, and former NMM shareholders will own 30,052,587 shares, or 83.3% of the outstanding common stock of ApolloMed (both percentages assuming (A) the issuance of 30,052,587 shares of ApolloMed common stock to former merger NMM shareholders, (B) excluding (i) 499,000 shares of common stock issuable upon the exercise of a Convertible Promissory Note to Alliance Apex, LLC (“Alliance”) for $4.99 million (as amended on October 16, 2017, the “Alliance Note”), (ii) shares of common stock issuable upon the exercise of the Warrant Consideration, and (C) without giving effect to any shares of common stock issuable upon payment of any indemnification obligations under the Merger Agreement (“Indemnification Shares”)).
In the event all of the Warrant Consideration were to be exercised or converted in full and without giving effect to the issuance of any Indemnification Shares or shares issuable upon exercise of the Alliance Note, then immediately following completion of the Merger, current ApolloMed stockholders, would own 6,033,495 shares of common stock, and their combined ownership percentage would be approximately 15.9% of the outstanding common stock of ApolloMed, and the former NMM shareholders would own 31,802,587 shares of common stock, or approximately 84.1% of the outstanding common stock of ApolloMed.
Q: When and where is the ApolloMed special meeting?
A: The ApolloMed special meeting will be held on [●], 2017, at [●][a.m.][p.m.], Pacific Standard Time, at 700 N. Brand Blvd., Suite 1400, Glendale, California 91203.
Q: What is being voted on?
A: At the ApolloMed special meeting, ApolloMed stockholders will be asked to consider and vote in favor of the following:
(1) The ApolloMed Merger Proposal – to approve the Merger between Merger Sub and NMM pursuant to the terms and conditions of the Merger Agreement, the Merger Agreement and the transactions contemplated thereunder, including the issuance of shares of common stock and warrants of ApolloMed to NMM shareholders as merger consideration in the Merger (the “ApolloMed Merger Proposal”);
(2) The Board Classification Proposal – to approve amendments to the ApolloMed Restated Certificate of Incorporation (the “ApolloMed Charter”) and Restated Bylaws (the “ApolloMed Bylaws”) to divide the board of directors of ApolloMed into three classes (the “Board Classification Proposal”);
| 17 |
(3) The Election of Directors Proposal – to elect nine directors to serve as members of ApolloMed’s board for one-year, two-year or three-year terms (the “Election of Directors Proposal”);
(4) The ApolloMed Compensation Proposal – to consider and vote on a proposal to approve, in a non-binding advisory vote, certain compensation arrangements for ApolloMed’s named executive officers (the “ApolloMed Compensation Proposal”); and
(5) The ApolloMed Adjournment Proposal – to consider and vote upon a proposal to adjourn the special meeting to a later date or dates, if necessary, to permit the solicitation of additional proxies if, based upon the tabulated vote at the time of the special meeting, there are not sufficient votes to approve one or more proposals presented to stockholders for vote (the “ApolloMed Adjournment Proposal”).
Q: What constitutes a quorum for the ApolloMed special meeting?
A: Pursuant to the ApolloMed Bylaws, the presence of holders of at least a majority of the ApolloMed common stock, Series A preferred stock and Series B preferred stock, voting together as one class on as-converted basis, is required to constitute a quorum. Stockholders present in person or by proxy will be counted for purposes of determining whether a quorum is present.
In the absence of a quorum, the chair of the meeting or the holders of a majority of the shares of ApolloMed stock entitled to vote who are present, in person or by proxy, may adjourn the meeting to another place, date, and time. As of the record date for the special meeting, [●] shares of ApolloMed’s common stock (on an as-converted basis), would be required to achieve a quorum.
Q: What is the record date and what does it mean?
A: The record date to determine the stockholders entitled to notice of and to vote at the special meeting is the close of business on [●], 2017. The record date was established by the ApolloMed board of directors as required by Delaware law. As of the ApolloMed record date, there were [●] shares of ApolloMed common stock, [●] shares of Series A preferred stock and [●] shares of Series B preferred stock outstanding and entitled to vote at the ApolloMed special meeting held by [●] record holders. As of the ApolloMed record date all the outstanding shares of Series A preferred stock and Series B preferred stock were held by NMM.
Q: Who is entitled to vote at the special meeting?
A: Holders of ApolloMed common stock, Series A preferred stock and Series B preferred stock at the close of business on the ApolloMed record date may vote at the special meeting.
Q: How many votes do I have?
A: You are entitled to one vote on each proposal to be considered at the ApolloMed special meeting for each share of ApolloMed common stock, Series A preferred stock or Series B preferred stock that you owned as of the close of business on [●], 2017, which is the ApolloMed record date.
Q: Why is my vote important?
A: If you do not submit a proxy or vote in person, it may be more difficult for ApolloMed to obtain the necessary quorum to transact business at its special meeting. In addition, the Merger cannot be completed unless the requisite vote of the holders of ApolloMed common stock and Series A preferred stock and Series B preferred stock in favor of the ApolloMed Merger Proposal is obtained.
Q: How do I vote?
A: If you are a stockholder of record, you may vote your shares of ApolloMed common stock or Series A preferred stock or Series B preferred stock on the matters to be presented at the ApolloMed special meeting in any of the following ways:
In Person – To vote in person, come to the ApolloMed special meeting and you will be able to vote by ballot. To ensure that your shares of ApolloMed common stock or Series A preferred stock or Series B preferred stock are voted at the ApolloMed special meeting, the ApolloMed board of directors recommends that you submit a proxy even if you plan to attend the ApolloMed special meeting.
| 18 |
By Mail – To vote using the enclosed proxy card, simply complete, sign and date the enclosed proxy card and return it promptly in the enclosed return envelope. If you return your signed proxy card to ApolloMed before the ApolloMed special meeting, the persons named as proxies will vote your shares as you direct.
By Telephone – To vote by telephone, dial the toll-free telephone number located on the enclosed proxy card using a touch-tone phone and follow the recorded instructions. You will be asked to provide the ApolloMed number and control number from the enclosed proxy card.
By Internet – To vote over the Internet, go to the web address identified on the enclosed proxy card to complete an electronic proxy card. You will be asked to provide the ApolloMed number and control number from the enclosed proxy card.
If your shares are held in “street name” by a broker, bank or other nominee, please refer to the voting instructions provided by your bank, brokerage firm or other nominee to see which of the above choices are available to you. Your bank, brokerage firm or other nominee cannot vote your shares without instructions from you. Please note that if your shares are held in “street name” and you wish to vote in person at the ApolloMed special meeting, you must obtain a legal proxy from your bank, brokerage firm or other nominee.
Q: What is the vote required to approve each proposal?
A: Assuming a quorum is present, approval of the ApolloMed Merger Proposal, the Board Classification Proposal, and each of the directors in the Election of Directors Proposal requires the affirmative vote of (i) a majority of the shares of ApolloMed common stock, Series A preferred stock and Series B preferred stock, voting together as one class on an as-converted basis, and (ii) a majority of the shares of ApolloMed common stock, Series A preferred stock and Series B preferred stock, voting together as one class on an as-converted basis, not owned by NMM. Approval of the ApolloMed Compensation Proposal and approval of the ApolloMed Adjournment Proposal will require the affirmative vote of a majority of the shares of ApolloMed stock entitled to vote present in person or represented by proxy at the ApolloMed special meeting.
Each of the ApolloMed Merger Proposal, the Board Classification Proposal and each of the directors in the Election of Directors Proposal are all conditioned on each other. The ApolloMed Compensation Proposal and the ApolloMed Adjournment Proposal are not conditioned on any other proposal.
Q: Do I have any appraisal rights with respect to any of the matters to be voted on at the special meeting?
A: No. ApolloMed stockholders do not have any appraisal rights under Delaware law in connection with the matters to be voted on at the special meeting.
Q: How does ApolloMed’s board of directors recommend that I vote at the special meeting?
A: ApolloMed’s board of directors recommends that you vote “FOR” the ApolloMed Merger Proposal, “FOR” the Board Classification Proposal, “FOR” each of the directors in the Election of Directors Proposal, “FOR” the ApolloMed Compensation Proposal and “FOR” the ApolloMed Adjournment Proposal.
Q: What interests do ApolloMed’s current executive officers and directors have in the Merger?
A: ApolloMed’s directors and executive officers may have interests in the proposals that are different from, or in addition to or in conflict with, yours. These interests include:
| · | certain directors and officers of ApolloMed are expected to continue to serve as directors and officers of the combined company; |
| · | as current stockholders of ApolloMed, certain of ApolloMed’s directors and officers will retain an ownership stake in ApolloMed after the closing of the Merger, at which time the operations of the NMM business will comprise the majority of ApolloMed’s operations; |
| · | certain ApolloMed directors and officers have employment agreements with ApolloMed which are expected to remain in place following the Merger; |
| 19 |
| · | the Merger Agreement contemplates that Warren Hosseinion, M.D., the sole shareholder of Maverick Medical Group, Inc., a California professional corporation (“MMG”) and an affiliate of ApolloMed, will sell to APC-LSMA Designated Shareholder Medical Corporation, a California professional corporation (“APC-LSMA”), all the issued and outstanding shares of capital stock of MMG for $100 under the Stock Purchase Agreement between Warren Hosseinion and APC-LSMA (the “Maverick Stock Purchase Agreement”); and |
| · | the continued indemnification of current directors and officers of ApolloMed and the continuation of directors’ and officers’ liability insurance after the Merger. |
These interests may influence ApolloMed’s directors in making their recommendation that you vote in favor of the approval of the ApolloMed Merger Proposal and other proposals.
Q. Why am I being asked to consider and vote on the ApolloMed Compensation Proposal?
A. Under SEC rules, ApolloMed is required to seek a non-binding advisory vote with respect to the compensation that may be paid or become payable to its named executive officers that is based on or otherwise relates to the Merger, or so-called “golden parachute” compensation.
Q. What will happen if ApolloMed’s stockholders do not approve the ApolloMed Compensation Proposal?
A. The vote on the ApolloMed Compensation Proposal is a vote separate and apart from the vote to adopt the Merger Agreement and other related proposals. Accordingly, a stockholder may vote to approve the ApolloMed Compensation Proposal and vote not to approve the ApolloMed Merger Proposal, the Board Classification Proposal and each of the directors in the Election of Directors Proposal (which are conditioned on each other), or vote to approve such proposals and vote not to approve the ApolloMed Compensation Proposal. Because the vote on the ApolloMed Compensation Proposal is advisory only, it will not be binding on ApolloMed or the combined company after the Merger. Accordingly, if the ApolloMed Merger Proposal, the Board Classification Proposal and each of the directors in the Election of Directors Proposal are adopted by ApolloMed’s stockholders and the Merger is completed, the Merger-related compensation may be paid to ApolloMed’s named executive officers to the extent payable in accordance with the terms of their compensation agreements and arrangements even if ApolloMed’s stockholders do not approve the ApolloMed Compensation Proposal.
Q: What happens if I abstain from voting?
A: ApolloMed will count a properly executed proxy marked “ABSTAIN” with respect to a particular proposal as present for purposes of determining whether a quorum is present, but for purposes of approval an abstention will be counted toward the total vote and will have the same effect as a vote “AGAINST” the ApolloMed Merger Proposal, the Board Classification Proposal, each of the directors in the Election of Directors Proposal, the ApolloMed Compensation Proposal and the ApolloMed Adjournment Proposal.
Q: What will happen if I sign and return my proxy card without indicating how I wish to vote?
A: All proxies will be voted in accordance with the instructions contained therein. Signed and dated proxies received by ApolloMed without an indication of how the stockholder intends to vote on a proposal will be voted “FOR” each of the ApolloMed Merger Proposal, the Board Classification Proposal, each of the directors in the Election of Directors Proposal, the ApolloMed Compensation Proposal and the ApolloMed Adjournment Proposal.
Q: What happens if I sell my shares of ApolloMed stock before the special meeting?
A: Only holders of record of ApolloMed common stock and holders of Series A preferred stock and Series B preferred stock at the close of business on the record date are entitled to notice of the special meeting of stockholders and to vote at the special meeting and any adjournments or postponements of the special meeting. A complete list of stockholders of record entitled to vote at the special meeting will be available beginning 10 days before the special meeting at ApolloMed’s principal executive office for inspection by stockholders during ordinary business hours for any purpose germane to the special meeting.
| 20 |
Q: If my shares are held in “street name,” will my broker, bank or nominee automatically vote my shares for me?
A: No. Banks, brokers and other nominees that hold their customers’ shares in “street name” may not vote their customers’ shares on “non-routine” matters without instructions from their customers. As it is expected that each proposal is considered “non-routine,” such organizations do not have discretion to vote on any of the proposals. As a result, if you fail to provide your bank, broker or other nominee with instructions regarding how to vote your shares of ApolloMed capital stock, your shares will be counted for purposes of determining a quorum but will be considered a vote “AGAINST” the ApolloMed Merger Proposal, the Board Classification Proposal and each of the directors in the Election of Directors Proposal. For the ApolloMed Compensation Proposal and the ApolloMed Adjournment Proposal, broker non-votes will not be counted toward the total vote and will have no effect on either proposal.
Q: Can I attend the ApolloMed special meeting and vote my shares in person?
A: Yes. All holders of ApolloMed common stock, Series A preferred stock and Series B preferred stock as of the record date, including stockholders of record and stockholders who hold their shares through banks, brokers, nominees or any other holder of record, are invited to attend the ApolloMed special meeting. Holders of record of ApolloMed common stock, Series A preferred stock and Series B preferred stock can vote in person at the ApolloMed special meeting. If you are not a stockholder of record, you must obtain a legal proxy, executed in your favor, from the record holder of your shares, such as a broker, bank or other nominee, to be able to vote in person at the ApolloMed special meeting. If you plan to attend the ApolloMed special meeting, you must hold your shares in your own name or have a letter from the record holder of your shares confirming your ownership.
Q: Can I change or revoke my vote?
A: Yes. If you are a holder of record of ApolloMed common stock or a holder of Series A preferred stock or Series B preferred stock, you may revoke any proxy at any time prior or at the ApolloMed special meeting by:
| · | attending the ApolloMed special meeting and voting in person; |
| · | voting again by telephone or over the Internet (only your latest telephone or Internet vote submitted prior to the ApolloMed special meeting will be counted); |
| · | completing and submitting a new valid proxy card bearing a later date; or |
| · | sending written notice of revocation to ApolloMed at Apollo Medical Holdings, Inc., Attn: Secretary, 700 N. Brand Blvd., Suite 1400, Glendale, California 91203, which notice must be received before [●], Eastern Time, on [●], 2017. |
Q: What should I do if I receive more than one set of voting materials?
A: You may receive more than one set of voting materials, including multiple copies of this joint proxy statement/prospectus and multiple proxy cards or voting instruction cards. For example, if you hold your shares in more than one brokerage account, you will receive a separate voting instruction card for each brokerage account in which you hold shares. If you are a holder of record and your shares are registered in more than one name, you will receive more than one proxy card. Please complete, sign, date and return each proxy card and voting instruction card that you receive in order to cast your vote with respect to all of your shares.
Q: Who can help answer my questions?
A: The information provided above in this “Question and Answer” format is for your convenience only and is merely a summary of the information contained in this joint proxy statement/prospectus. ApolloMed urges you to carefully read this entire joint proxy statement/prospectus, including the documents referred to herein or otherwise incorporated by reference. If you have any questions, or need additional material, please feel free to contact:
Apollo Medical Holdings, Inc.:
700 N. Brand Blvd., Suite 1400
Glendale, CA 91203
Attention: Corporate Secretary
Telephone: (818) 396-8050
| 21 |
QUESTIONS AND ANSWERS FOR NMM SHAREHOLDERS
Q: What will I receive in the Merger?
A: Pursuant to the Merger Agreement, at the Effective Time, each issued and outstanding share of NMM common stock will be converted into the right to receive such number of fully paid and nonassessable ApolloMed shares of common stock that results in the NMM shareholders having a right to receive (A) an aggregate number of shares of ApolloMed common stock that represents 82% of the total issued and outstanding shares of ApolloMed common stock immediately following the Effective Time, assuming there are no NMM dissenting shareholder interests as of the Effective Time, calculated in accordance with the Merger Agreement (see “THE MERGER AGREEMENT – Effects of Merger; Merger Consideration” beginning on page 159), plus (B) an aggregate of 2,566,666 shares of ApolloMed common stock, assuming there are no NMM dissenting shareholder interests as of the Effective Time. In addition, each NMM shareholder shall be entitled to receive such shareholder’s pro rata portion of (i) warrants to purchase an aggregate of 850,000 shares of ApolloMed common stock, exercisable at $11.00 per share, and (ii) warrants to purchase an aggregate of 900,000 shares of ApolloMed common stock, exercisable at $10.00 per share. At the Effective Time, ApolloMed will hold back the Holdback Shares to secure indemnification of ApolloMed and its affiliates under the Merger Agreement. Separately, indemnification of pre-Merger NMM shareholders under the Merger Agreement will be made by the issuance by ApolloMed to pre-Merger NMM shareholders of new additional shares of common stock (capped at the same number of shares of ApolloMed common stock as the Holdback Shares).
Assuming the issuance of 30,052,587 shares of ApolloMed common stock to NMM shareholders in the Merger, the value of such shares is estimated to be $240,721,222 based upon a share price of $8.01 per share, the closing price of ApolloMed common stock on October 17, 2017. In addition, the estimated fair value of the warrants to be issued to NMM’s shareholders by ApolloMed in the Merger is $3,944,000, based on the estimated fair value of (i) $1,811,000 for the warrants to purchase an aggregate of 850,000 shares of ApolloMed common stock exercisable at $11.00 per share and (ii) $2,133,000 for the warrants to purchase an aggregate of 900,000 shares of ApolloMed common stock exercisable at $10.00 per share.
Q: When and where will the special meeting of NMM shareholders be held?
A: The NMM special meeting will be held on [●], 2017, at [●][a.m.][p.m.], Pacific Standard Time, at the offices of NMM, 1668 S. Garfield Ave. 3rd Floor, Alhambra, California 91801.
Q: What is being voted on?
A: At the NMM special meeting, NMM shareholders will be asked to consider and vote in favor of the following:
(1) The NMM Merger Proposal – to approve the Merger between NMM and Merger Sub pursuant to which Merger Sub will merge with and into NMM, with NMM continuing as the surviving corporation and a wholly owned subsidiary of ApolloMed, the Merger Agreement and the transactions contemplated thereunder (the “NMM Merger Proposal”); and
(2) The NMM Adjournment Proposal – to consider and vote upon a proposal to adjourn the special meeting to a later date or dates, if necessary, to permit the solicitation of additional proxies if, based upon the tabulated vote at the time of the special meeting, there are not sufficient votes to approve one or more proposals presented to stockholders for vote (the “NMM Adjournment Proposal”).
Q: What constitutes a quorum for the NMM special meeting?
A: Pursuant to the Amended and Restated NMM Bylaws (the “NMM Bylaws”), the presence of holders of at least a majority of the outstanding shares of NMM common stock is required to constitute a quorum. Shareholders present in person or by proxy will be counted for purposes of determining whether a quorum is present.
In the event that a quorum is not present, or if there are insufficient votes to approve the principal terms of the Merger and the Merger Agreement at the time of the special meeting, it is expected that the special meeting will be adjourned or postponed to solicit additional votes. As of the record date for the special meeting, [●] shares of NMM’s common stock would be required to achieve a quorum.
Q: What is the record date and what does it mean?
A: The record date to determine the NMM shareholders entitled to notice of and to vote at the special meeting is the close of business on [●], 2017. The record date is set by the NMM board of directors pursuant to the NMM Bylaws. As of the NMM record date, there were [●] shares of NMM common stock outstanding and entitled to vote at the NMM special meeting held by [●] record holders.
Q: Who is entitled to vote at the special meeting?
A: Holders of NMM common stock at the close of business on the NMM record date may vote at the special meeting.
| 22 |
Q: How many votes do I have?
A: You are entitled to one vote on each proposal to be considered at the NMM special meeting for each share of NMM common stock that you owned as of the close of business on [●], 2017, which is the NMM record date.
Q: Why is my vote important?
A: If you do not submit a proxy or vote in person, it may be more difficult for NMM to obtain the necessary quorum to transact business at its special meeting. In addition, the Merger cannot be completed unless the requisite vote of the holders of NMM common stock in favor of the NMM Merger Proposal is obtained.
Q: How do I vote?
A: If you are a shareholder of record, you may vote your shares of NMM common stock on the matters to be presented at the NMM special meeting in any of the following ways:
· In Person – To vote in person, come to the NMM special meeting and you will be able to vote by ballot. To ensure that your shares of NMM common stock are voted at the NMM special meeting, the NMM board recommends that you submit a proxy even if you plan to attend the NMM special meeting.
· By Mail – To vote using the enclosed proxy card, simply complete, sign and date the enclosed proxy card and return it promptly in the enclosed return envelope. If you return your signed proxy card to NMM before the NMM special meeting, the persons named as proxies will vote your shares of NMM common stock as you direct.
Q: What is the vote required to approve each proposal?
A: Assuming a quorum is present, approval of the NMM Merger Proposal requires the affirmative vote of NMM shareholders holding at least 95% of the outstanding shares of NMM common stock and representing at least 95% in number of the NMM shareholders. The NMM Adjournment Proposal requires the affirmative vote of a majority of the outstanding shares of NMM stock entitled to vote present in person or represented by proxy at the NMM special meeting.
If the NMM Merger Proposal does not receive the requisite vote for approval, then ApolloMed and NMM will not consummate the Merger.
Q: Do I have any appraisal rights with respect to any of the matters to be voted on at the special meeting?
A: Yes. You are entitled to the right to seek appraisal of the fair value of your shares of NMM common stock under Chapter 13 of the California Corporations Code. A summary of the dissenters’ rights that may be available to you are described in “THE MERGER – Dissenters’ Rights” on page 154.
Q: How does the NMM board recommend that I vote at the special meeting?
A: The NMM board recommends that you vote “FOR” the NMM Merger Proposal and “FOR” the NMM Adjournment Proposal.
Q: Have any NMM shareholders already agreed to vote in favor of the Merger?
A: Yes. Eddie Lam, M.D., Thomas Lam, M.D., Su Kin Lee, M.D., Kenneth Sim, M.D., Theresa Tseng, M.D., Yang Chern Tseng, M.D., and Albert Young, M.D. have each entered into an agreement with ApolloMed pursuant to which each has agreed to vote all of the shares of NMM common stock owned or controlled by them in favor of the Merger and the Merger Agreement. As of the close of business on [●], 2017, the record date for the special meeting, Eddie Lam, M.D., Thomas Lam, M.D., Su Kin Lee, M.D., Kenneth Sim, M.D., Theresa Tseng, M.D., Yang Chern Tseng, M.D., and Albert Young, M.D. collectively owned, directly or indirectly, [●] shares of NMM common stock, which represented approximately [●]% of the outstanding shares of NMM common stock.
Q: What interests do NMM’s current executive officers and directors have in the Merger?
A: NMM’s directors and executive officers may have interests in the proposals that are different from, or in addition to or in conflict with, yours. These interests include:
| 23 |
| · | certain current directors and officers of NMM expect the continuation of service as directors and officers of the combined company; |
| · | the Merger Agreement contemplates that Warren Hosseinion, M.D., the sole shareholder of MMG, will sell to APC-LSMA (an entity in which Dr. Thomas Lam is the sole shareholder and the sole executive officer, but which is controlled and consolidated by Allied Physicians of California IPA dba Allied Pacific IPA (“APC”)) all the issued and outstanding shares of capital stock of MMG for $100 under the Maverick Stock Purchase Agreement; and |
| · | the continued indemnification of current directors and officers of NMM and the continuation of directors’ and officers’ liability insurance after the Merger. |
These interests may influence NMM’s directors in making their recommendation that you vote in favor of the approval of the NMM Merger Proposal and the NMM Adjournment Proposal.
Q: What happens if I abstain from voting?
A: NMM will count a properly executed proxy marked “ABSTAIN” with respect to a particular proposal as present for purposes of determining whether a quorum is present, but for purposes of approval, an abstention will be counted toward the total vote and will have the same effect as a vote “AGAINST” the NMM Merger Proposal and the NMM Adjournment Proposal.
Q: What will happen if I sign and return my proxy card without indicating how I wish to vote?
A: All proxies will be voted in accordance with the instructions contained therein. Signed and dated proxies received by NMM without an indication of how the shareholder intends to vote on a proposal will be voted “FOR” each of the NMM Merger Proposal and the NMM Adjournment Proposal.
Q: What happens if I sell my shares of NMM common stock before the special meeting?
A: Only holders of record of NMM common stock at the close of business on the record date are entitled to notice of the special meeting of shareholders and to vote at the special meeting and any adjournments or postponements of the special meeting. A complete list of shareholders of record entitled to vote at the special meeting will be available beginning 10 days before the special meeting at NMM’s principal executive office for inspection by shareholders during ordinary business hours for any purpose germane to the special meeting.
Q: Can I attend the NMM special meeting and vote my shares in person?
A: Yes. All holders of NMM common stock as of the record date are invited to attend the NMM special meeting. Holders of record of NMM common stock can vote in person at the NMM special meeting. If you are not a shareholder of record, you must obtain a legal proxy, executed in your favor, from the record holder of your shares to be able to vote in person at the NMM special meeting. If you plan to attend the NMM special meeting, you must hold your shares in your own name or have a letter from the record holder of your shares confirming your ownership.
Q: Can I change or revoke my vote?
A: Yes. If you are a holder of record of NMM common stock, you may revoke any proxy at any time prior or at the NMM special meeting by:
| · | attending the NMM special meeting and voting in person; |
| · | completing and submitting a new valid proxy card bearing a later date; or |
| · | sending written notice of revocation to NMM at Network Medical Management, Inc., Attn: Secretary, 1668 S. Garfield Avenue, 3rd Floor, Alhambra, California 91801, which notice must be received before [●], Eastern Time, on [●], 2017. |
Q: What should I do if I receive more than one set of voting materials?
A: You may receive more than one set of voting materials, including multiple copies of this joint proxy statement/prospectus and multiple proxy cards or voting instruction cards. For example, if you are a holder of record and your shares are registered in more than one name, you will receive more than one proxy card. Please complete, sign, date and return each proxy card and voting instruction card that you receive in order to cast your vote with respect to all of your shares.
| 24 |
Q: Is the transaction expected to be taxable to NMM shareholders?
A: The Merger has been structured to qualify as a “reorganization” within the meaning of Section 368(a) of the Internal Revenue Code of 1986, as amended (the “Code”) and Treasury Regulations promulgated thereunder. As a result, NMM shareholders generally should not recognize gain or loss for U.S. federal income tax purposes upon the exchange of their shares of NMM stock for shares of ApolloMed common stock and warrants in connection with the Merger. To the extent, however, NMM distributes existing ApolloMed warrants to NMM shareholders prior to the consummation of the Merger, such distribution will constitute a dividend for U.S. federal income tax purposes to the extent of NMM’s current or accumulated earnings and profits as determined under U.S. federal income tax principles. See “CERTAIN MATERIAL U.S. FEDERAL INCOME TAX CONSEQUENCES OF THE MERGER” on page 214 of this joint proxy statement/prospectus for information.
Q: When can I expect to receive the merger consideration?
A: As soon as reasonably practicable after the Effective Time of the Merger, NMM shareholders will receive a letter of transmittal with instructions informing you how to effect the surrender of your shares of NMM common stock in exchange for the merger consideration.
Q: Where can I find more information on ApolloMed?
A: ApolloMed files annual, quarterly and current reports, proxy statements and other information with the U.S. Securities and Exchange Commission (the “SEC”). ApolloMed’s SEC filings are available to the public from the SEC’s website at http://www.sec.gov. Information about ApolloMed, including its SEC filings, is also available through its website at http://Apollomed.net. The information contained on, or that can be accessed through, such websites is not part of this joint proxy statement/prospectus.
Q: Who can help answer my questions?
A: The information provided above in this “Question and Answer” format is for your convenience only and is merely a summary of the information contained in this joint proxy statement/prospectus. NMM urges you to carefully read this entire joint proxy statement/prospectus, including the documents referred to herein or otherwise incorporated by reference. If you have any questions, or need additional material, please feel free to contact:
Network Medical Management, Inc.
1668 S. Garfield Avenue, 3rd Floor
Alhambra, California 91801
Attention: Thomas Lam, M.D.
Chief Executive Officer
Telephone: (626) 282-0288
| 25 |
This summary highlights selected information from this joint proxy statement/prospectus and may not contain all of the information that is important to you. You are urged to carefully read this entire document, including the annexes, and the other documents to which ApolloMed and NMM refer for a more complete understanding of the Merger. In addition, ApolloMed and NMM encourage you to read the information about ApolloMed in the section entitled “Information About ApolloMed” beginning on page 212 of this joint proxy statement/prospectus, which includes important business and financial information about ApolloMed, and to read the information in the section entitled “Information About NMM” beginning on page 263 of this joint proxy statement/prospectus, which includes important business and financial information about NMM. Stockholders of ApolloMed and shareholders of NMM may obtain additional information about ApolloMed without charge by following the instructions in the section entitled “Where You Can Find More Information” beginning on page 314 of this joint proxy statement/prospectus.
This summary and the balance of this joint proxy statement/prospectus contain forward-looking statements about events that are not certain to occur, and you should not place undue reliance on those statements. Please carefully read “Cautionary Statement Regarding Forward-Looking Statements” on page 100 of this joint proxy statement/prospectus.
Apollo Medical Holdings, Inc.
700 N. Brand Blvd., Suite 1400
Glendale, CA 91203
Tel: (818) 396-8050
Apollo Medical Holdings, Inc. was incorporated in the State of Delaware on November 1, 1985 under the name McKinnely Investment, Inc. On November 5, 1986 McKinnely Investment, Inc. changed its name to Acculine Industries, Incorporated and Acculine Industries, Incorporated changed its name to Siclone Industries, Incorporated on May 24, 1988. On July 3, 2008, Apollo Medical Holdings, Inc. merged into Siclone Industries, Incorporated and Siclone Industries, Incorporated, as the surviving entity from the merger, simultaneously changed its name to Apollo Medical Holdings, Inc.
ApolloMed is a physician-centric, integrated population health management company working to provide coordinated outcomes-based medical care in a cost-effective manner. Led by a management team with over a decade of experience, ApolloMed has built a company and culture that is focused on physicians providing high-quality medical care, population health management and care coordination for patients, particularly senior patients and patients with multiple chronic conditions. ApolloMed believes it is well-positioned to take advantage of changes in the rapidly evolving U.S. healthcare industry, as there is a growing national movement towards more results-oriented healthcare centered on the triple aim of patient satisfaction, high-quality care and cost efficiency.
ApolloMed’s common stock is currently quoted on OTC Pink and traded under the symbol “AMEH.” ApolloMed has applied for listing of its common stock on the NASDAQ Global Market effective as of the closing of the Merger. No assurance can be given that ApolloMed’s application will be approved. On December 21, 2016, the last full trading day before the announcement of the Merger, the last reported sale price of ApolloMed common stock was $3.99 per share, and, on [●], 2017, the latest practicable date prior to the date of this joint proxy statement/prospectus, the last reported sale price of ApolloMed common stock was $[●] per share.
Additional information about ApolloMed can be found in the sections titled “INFORMATION ABOUT APOLLOMED — Overview” beginning on page 212, “INFORMATION ABOUT APOLLOMED — ApolloMed Management’s Discussion and Analysis of Financial Condition and Results of Operations” beginning on page 240 and ApolloMed’s financial statements included elsewhere in this joint proxy statement/prospectus.
ApolloMed’s principal website is www.apollomed.net. The information contained on, or that can be accessed through, ApolloMed’s website is specifically not incorporated by reference into this joint proxy statement/prospectus, and is not a part of this joint proxy statement/prospectus.
Apollo Acquisition Corp.
700 N. Brand Blvd., Suite 1400
Glendale, CA 91203
Tel: (818) 396-8050
Apollo Acquisition Corp., a California corporation, is a wholly owned subsidiary of ApolloMed that was recently formed solely for the purpose of entering into the Merger Agreement and consummating the Merger and the other transactions contemplated by the Merger Agreement. It is not engaged in any business and has no material assets. In the Merger, Merger Sub will merge with and into NMM, with NMM surviving the Merger as ApolloMed’s wholly owned subsidiary, and Merger Sub will cease to exist.
| 26 |
Network Medical Management, Inc.
1668 S. Garfield Avenue
Alhambra, CA 91801
(626) 282-0288
Network Medical Management, Inc. is a California corporation formed in 1994. NMM, together with its subsidiaries and affiliated physician groups, constitutes a patient- and physician-centric, integrated health care delivery and management services company focused on providing coordinated, outcomes-based medical care in a cost-effective manner. Through capitation agreements between NMM’s affiliated physician groups and various health plans, NMM is responsible for coordinating the care for over 600,000 covered patients in southern and central California through a network of over 10 independent practice associations (“IPAs”) with approximately 4,000 contracted physicians. These covered patients are comprised of managed care members whose health coverage is provided through their employer or who have individually acquired health coverage directly from a health plan or as a result of their eligibility for Medicaid or Medicare benefits.
The patients of NMM’s affiliated physician groups and IPAs benefit from an integrated approach to medical care that places the physician at the center of patient care. NMM manages the delivery of healthcare services to patients via a network of affiliated physician groups and other network primary care physicians, network hospitals, and affiliated group and network specialists. Together with case managers, registered nurses and other care coordinators, these medical professionals utilize a comprehensive data analysis engine, sophisticated risk management techniques and clinical protocols to provide high-quality, cost effective care to NMM’s managed members. NMM monitors certain control metrics, such as the number of inpatient acute bed days per 1,000 patients and hospital readmission rates, as they are contributors to quality clinical outcomes and financial performance. Additionally, in an effort to identify changes or trends with respect to its commercial, senior and Medicaid payer classifications, NMM closely monitors the number of managed care members who have enrolled with a NMM affiliated physician group as such member’s primary care physician.
NMM is headquartered in, and primarily operates from, Los Angeles County, California.
Additional information about NMM can be found in the sections titled “INFORMATION ABOUT NMM” beginning on page 263 and “INFORMATION ABOUT NMM — NMM Management’s Discussion and Analysis of Financial Condition and Results of Operations” beginning on page 285 and NMM’s financial statements included elsewhere in this joint proxy statement/prospectus.
NMM’s principal website is www.nmm.cc. The information contained on, or that can be accessed through, NMM’s website is specifically not incorporated by reference into this joint proxy statement/prospectus, and is not a part of this joint proxy statement/prospectus.
The Merger Agreement (Page 158)
On December 21, 2016, ApolloMed, Merger Sub, NMM and the Shareholders’ Representative entered into the Merger Agreement. The Merger Agreement was subsequently amended on March 30, 2017 and October 17, 2017. The Merger Agreement is the legal document governing the Merger and is included in this joint proxy statement/prospectus as Annex A. All descriptions in this Summary and elsewhere in this joint proxy statement/prospectus of the terms and conditions of the Merger are qualified in their entirety by reference to the full text of the Merger Agreement. Please read the Merger Agreement carefully for a more complete understanding of the Merger.
The Merger (Page 120)
At the Effective Time of the Merger, Merger Sub, a wholly owned subsidiary of ApolloMed, will merge with and into NMM. Upon completion of the Merger, the separate corporate existence of Merger Sub will cease, and NMM will continue as the surviving entity and as a wholly owned subsidiary of ApolloMed.
Effects of Merger; Merger Consideration (Page 159)
Pursuant to the Merger Agreement, at the Effective Time, each issued and outstanding share of NMM common stock will be converted into the right to receive such number of fully paid and nonassessable ApolloMed shares of common stock that results in the NMM shareholders having a right to receive (A) an aggregate number of shares of ApolloMed common stock that represents 82% of the total issued and outstanding shares of ApolloMed common stock immediately following the Effective Time, assuming there are no NMM dissenting shareholder interests as of the Effective Time, calculated in accordance with the Merger Agreement (see “THE MERGER AGREEMENT – Effects of Merger; Merger Consideration” beginning on page 159), plus (B) an aggregate of 2,566,666 shares of ApolloMed common stock, assuming there are no NMM dissenting shareholder interests as of the Effective Time. In addition, each NMM shareholder shall be entitled to receive such shareholder’s pro rata portion of (i) warrants to purchase an aggregate of 850,000 shares of ApolloMed common stock, exercisable at $11.00 per share and (ii) warrants to purchase an aggregate of 900,000 shares of ApolloMed common stock, exercisable at $10.00 per share. At the Effective Time, ApolloMed will hold back the Holdback Shares to secure indemnification of ApolloMed and its affiliates under the Merger Agreement. Separately, indemnification of pre-Merger NMM shareholders under the Merger Agreement will be made by the issuance by ApolloMed to pre-Merger NMM shareholders of new additional shares of common stock (capped at the same number of shares of ApolloMed common stock as the Holdback Shares).
| 27 |
There will be no adjustment to the total number of shares of ApolloMed common stock that NMM shareholders will be entitled to receive for changes in the market price of ApolloMed common stock. Accordingly, the market value of the shares of ApolloMed common stock issued pursuant to the Merger will depend on the market value of the shares of ApolloMed common stock at the time the Merger closes, and could vary significantly from the market value on the date of this proxy statement/prospectus/information statement.
For a full description of the Merger Consideration, see the sections titled “THE MERGER” beginning on page 120 and “THE MERGER AGREEMENT — Effects of Merger; Merger Consideration” beginning on page 159 of this joint proxy statement/prospectus.
ApolloMed’s Reasons for the Merger
In approving and authorizing the Merger Agreement and the Merger, the ApolloMed board of directors considered a number of factors. In light of the number and wide variety of factors considered in connection with its evaluation of the Merger Agreement and the Merger, the ApolloMed board of directors did not consider it practicable to, and did not attempt to, quantify or otherwise assign relative weights to the specific factors it considered in reaching its determination. The ApolloMed board of directors viewed its position and determinations as being based on all of the information available and the factors presented to and considered by it. In addition, individual directors may have given different weight to different factors.
In evaluating the Merger Agreement and the Merger, the ApolloMed board of directors consulted with ApolloMed’s management and legal and financial advisors, reviewed a significant amount of information, and considered a number of factors, including, among others, the factors that the ApolloMed board viewed as supportive of its decision, to approve the Merger Agreement and the Merger, as being advisable, fair and in the best interests of ApolloMed and ApolloMed’s stockholders.
The ApolloMed board of directors also carefully considered and discussed a number of risks, uncertainties, and other countervailing factors in its deliberations regarding entering into the Merger Agreement and consummating the Merger.
The ApolloMed board of directors believes that, overall, the potential benefits to ApolloMed stockholders of the Merger Agreement, the Merger and the other transactions contemplated thereby outweigh the risks and uncertainties.
For a more complete description of these reasons, see “THE MERGER — ApolloMed’s Reasons for the Merger” beginning on page 128 of this joint proxy statement/prospectus.
In approving and authorizing the Merger Agreement and the Merger, the NMM board of directors considered a number of factors. In light of the number and wide variety of factors considered in connection with its evaluation of the Merger Agreement and the Merger, the NMM board of directors did not consider it practicable to, and did not attempt to, quantify or otherwise assign relative weights to the specific factors it considered in reaching its determination. The NMM board of directors viewed its position and determinations as being based on all of the information available and the factors presented to and considered by it. In addition, individual directors may have given different weight to different factors.
In evaluating the Merger Agreement and the Merger, the NMM board of directors consulted with NMM’s management and legal and financial advisors, reviewed a significant amount of information, and considered a number of factors, including, among others, the factors that the NMM board viewed as supportive of its decision, to approve the Merger Agreement and the Merger, as being advisable, fair and in the best interests of NMM and NMM’s shareholders.
The NMM board of directors also carefully considered and discussed a number of risks, uncertainties, and other countervailing factors in its deliberations regarding entering into the Merger Agreement and consummating the Merger.
| 28 |
The NMM board of directors believes that, overall, the potential benefits to NMM shareholders of the Merger Agreement, the Merger and the other transactions contemplated thereby outweigh the risks and uncertainties.
For a more complete description of these reasons, see “THE MERGER — NMM’s Reasons for the Merger” beginning on page 44 of this joint proxy statement/prospectus.
In evaluating the Merger Agreement and the Merger and related transactions contemplated by the Merger Agreement, you should carefully consider all of the information into this joint proxy statement/prospectus. In particular, you are urged to read and consider all of the factors discussed in the section entitled “RISK FACTORS” beginning on page 44.
Recommendation of ApolloMed’s Board of Directors (Page 103)
ApolloMed’s board of directors has determined that the Merger Agreement and the transactions contemplated thereby, including the Merger and the issuance of shares of common stock and warrants of ApolloMed to NMM shareholders pursuant to the terms of the Merger Agreement, are just, equitable and fair to ApolloMed and its stockholders and that it is in the best interests of ApolloMed and its stockholders that ApolloMed complete the Merger and has adopted and approved the Merger Agreement and the transactions contemplated thereby, including the Merger and the other transactions contemplated thereby. ApolloMed’s board of directors believes that each of the ApolloMed Merger Proposal, the Board Classification Proposal, each of the directors in the Election of Directors Proposal and the ApolloMed Adjournment Proposal to be presented at the special meeting is in the best interests of ApolloMed and its stockholders, and recommends that its stockholders vote “FOR” each of the proposals. For the factors considered by ApolloMed’s board of directors in reaching its decision to approve the Merger and Merger Agreement, see the section entitled “THE MERGER — ApolloMed’s Reasons for the Merger” beginning on page 128 of this joint proxy statement/prospectus.
Recommendation of NMM’s Board of Directors (Page 114)
NMM’s board of directors has determined that the Merger Agreement and the transactions contemplated thereby, including the Merger and the issuance of shares of common stock and warrants of ApolloMed to NMM shareholders pursuant to the terms of the Merger Agreement, are just, equitable and fair to NMM and its shareholders and that it is in the best interests of NMM and its shareholders that NMM complete the Merger and has adopted and approved the Merger Agreement and the transactions contemplated thereby. NMM’s board of directors believes that both the NMM Merger Proposal and the NMM Adjournment Proposal to be presented at the special meeting is in the best interests of NMM and its shareholders, and recommends that its shareholders vote “FOR” both of the proposals. For the factors considered by NMM’s board of directors in reaching its decision to approve the Merger and Merger Agreement, see the section entitled “THE MERGER — NMM’s Reasons for the Merger” beginning on page 130 of this joint proxy statement/prospectus.
The ApolloMed Special Meeting (Page 103)
The ApolloMed special meeting will be held on [●], 2017, at [●][a.m.][p.m.], Pacific Standard Time, at 700 N. Brand Blvd., Suite 1400, Glendale, California 91203. At the special meeting, ApolloMed stockholders will be asked to consider and vote on the following:
(1) The ApolloMed Merger Proposal — to approve the Merger between Merger Sub and NMM pursuant to the terms and conditions of the Merger Agreement and the transactions contemplated thereunder, including the issuance of shares of common stock of ApolloMed to NMM shareholders as merger consideration in the Merger;
(2) The Board Classification Proposal — to approve amendments to the ApolloMed Charter and ApolloMed Bylaws to divide the board of directors of ApolloMed into three classes;
(3) The Election of Directors Proposal — to elect nine directors to serve as members of ApolloMed’s board for one-year, two-year or three-year terms;
(4) The ApolloMed Compensation Proposal – to consider and vote on a proposal to approve, in a non-binding advisory vote, certain compensation arrangements for ApolloMed’s named executive officers; and
(5) The ApolloMed Adjournment Proposal — to consider and vote upon a proposal to adjourn the special meeting to a later date or dates, if necessary, to permit the solicitation of additional proxies if, based upon the tabulated vote at the time of the special meeting, there are not sufficient votes to approve one or more proposals presented to stockholders for the vote.
| 29 |
Only the holders of record of shares of ApolloMed common stock, Series A preferred stock and Series B preferred stock, voting together as one class on an as-converted basis, on the ApolloMed record date are entitled to receive notice of and to vote at the ApolloMed special meeting. Each share of ApolloMed common stock entitles the holder to one vote at the ApolloMed special meeting on each proposal to be considered at the ApolloMed special meeting. Holders of shares of Series A preferred stock and Series B preferred stock vote with holders of shares of common stock as one class, on an as-converted basis. Each share of Series A preferred stock and Series B preferred stock entitles the holder to one vote at the ApolloMed special meeting on each proposal to be considered at the ApolloMed special meeting.
As of the ApolloMed record date, there were [●] shares of ApolloMed common stock, [●] shares of Series A preferred stock and [●] shares of Series B preferred stock outstanding and entitled to vote at the ApolloMed special meeting.
At the close of business on the ApolloMed record date, directors and executive officers of ApolloMed and their affiliates were entitled to vote [●] shares of ApolloMed common stock (on an as-converted basis), or approximately [●]% of the issued and outstanding shares of ApolloMed common stock (on an as-converted basis) on that date. ApolloMed currently expects that the ApolloMed directors and executive officers will vote their shares of ApolloMed common stock in favor of the proposed proposals, although none of them is obligated to do so. In addition, on the ApolloMed record date, NMM was entitled to vote [●] shares of ApolloMed common stock (on an as-converted basis), or approximately [●]% of the issued and outstanding shares of ApolloMed common stock (on an as-converted basis) on that date. ApolloMed currently expects that the NMM will vote their shares of ApolloMed common stock in favor of the proposed proposals, although it is not obligated to do so.
Assuming a quorum is present, approval of the ApolloMed Merger Proposal, the Board Classification Proposal, and each of the directors in the Election of Directors Proposal requires the affirmative vote of (i) a majority of the shares of ApolloMed common stock, Series A preferred stock and Series B preferred stock, voting together as one class on an as-converted basis, and (ii) a majority of the shares of ApolloMed common stock, Series A preferred stock and Series B preferred stock, voting together as one class on an as-converted basis, not owned by NMM. Approval of the ApolloMed Compensation Proposal and approval of the ApolloMed Adjournment Proposal will require the affirmative vote of a majority of the shares of ApolloMed stock entitled to vote present in person or represented by proxy at the ApolloMed special meeting.
The ApolloMed Merger Proposal, the Board Classification Proposal and each of the directors in the Election of Directors Proposal are all conditioned on each other. The ApolloMed Compensation Proposal and the ApolloMed Adjournment Proposal are not conditioned on any other proposal.
ApolloMed will count a properly executed proxy marked “ABSTAIN” with respect to a particular proposal as present for purposes of determining whether a quorum is present, but for purposes of approval an abstention will be counted toward the total vote and will have the same effect as a vote “AGAINST” the ApolloMed Merger Proposal, the Board Classification Proposal, each of the directors in the Election of Directors Proposal, the ApolloMed Compensation Proposal and the ApolloMed Adjournment Proposal. If you fail to provide your bank, broker or other nominee with instructions regarding how to vote your shares of ApolloMed capital stock, your shares will be counted for purposes of determining a quorum but will be considered a vote “AGAINST” the ApolloMed Merger Proposal, the Board Classification Proposal and each of the directors in the Election of Directors Proposal. For the ApolloMed Compensation Proposal and the ApolloMed Adjournment Proposal, broker non-votes will not be counted toward the total vote and will have no effect on either proposal.
The NMM Special Meeting (Page 114)
The NMM special meeting will be held on [●], 2017, at [●][a.m.][p.m.], Pacific Standard Time, at 1668 S. Garfield Ave. 3rd Floor, Alhambra, California 91801. At the special meeting, NMM shareholders will be asked to consider and vote on the following proposals:
(1) The NMM Merger Proposal – to approve the Merger between NMM and Merger Sub pursuant to which Merger Sub will merge with and into NMM, with NMM continuing as the surviving corporation and a wholly owned subsidiary of ApolloMed, the Merger Agreement and the transactions contemplated thereunder; and
(2) The NMM Adjournment Proposal – to consider and vote upon a proposal to adjourn the special meeting to a later date or dates, if necessary, to permit the solicitation of additional proxies if, based upon the tabulated vote at the time of the special meeting, there are not sufficient votes to approve one or more proposals presented to shareholders for vote.
| 30 |
The NMM board of directors has fixed the close of business on [●], 2017 as the record date for the NMM special meeting. Only holders of record of shares of NMM common stock on the NMM record date are entitled to vote at the NMM special meeting. Each share of NMM common stock entitles the holder to one vote at the NMM special meeting on each proposal or action to be considered at the NMM special meeting.
As of the NMM record date, there were [●] shares of NMM common stock outstanding and entitled to vote at the NMM special meeting.
Eddie Lam, M.D., Thomas Lam, M.D., Su Kin Lee, M.D., Kenneth Sim, M.D., Theresa Tseng, M.D., Yang Chern Tseng, M.D., and Albert Young, M.D. have each entered into an agreement with ApolloMed pursuant to which each has agreed to vote all of the shares of NMM common stock owned or controlled by them in favor of the Merger and the Merger Agreement. As of the close of business on [●], 2017, the record date for the special meeting, Eddie Lam, M.D., Thomas Lam, M.D., Su Kin Lee, M.D., Kenneth Sim, M.D., Theresa Tseng, M.D., Yang Chern Tseng, M.D., and Albert Young, M.D. collectively owned, directly or indirectly, 106,461,067 shares of NMM common stock, which represented approximately [●]% of the outstanding shares of NMM common stock.
Assuming a quorum is present, approval of the NMM Merger Proposal requires the affirmative vote of NMM shareholders holding at least 95% of the outstanding shares of NMM common stock and representing at least 95% in number of the NMM shareholders. The NMM Adjournment Proposal requires the affirmative vote of a majority of the outstanding shares of NMM stock entitled to vote present in person or represented by proxy at the NMM special meeting.
If the NMM Merger Proposal does not receive the requisite vote for approval, then ApolloMed and NMM will not consummate the Merger.
NMM will count a properly executed proxy marked “ABSTAIN” with respect to a particular proposal as present for purposes of determining whether a quorum is present, but for purposes of approval an abstention will be counted toward the total vote and will have the same effect as a vote “AGAINST” the NMM Merger Proposal and the NMM Adjournment Proposal.
Interests of ApolloMed’s Directors and Executive Officers in the Merger (Page 151)
In considering the recommendation of the ApolloMed board of directors that ApolloMed stockholders vote to approve all of the presented proposals, ApolloMed stockholders should be aware that some of ApolloMed’s directors and officers have interests in the Merger and have arrangements that are different from, or in addition to, those of ApolloMed stockholders generally. These interests and arrangements may create potential conflicts of interest. ApolloMed’s board of directors was aware of these interests and considered these interests, among other matters, in adopting and approving the Merger Agreement and the transactions contemplated thereby, including the Merger, and in recommending that ApolloMed stockholders approve the ApolloMed Merger Proposal, the Board Classification Proposal, each of the directors in the Election of Directors Proposal, the ApolloMed Compensation Proposal and the ApolloMed Adjournment Proposal.
When ApolloMed’s stockholders consider the recommendation of ApolloMed’s board of directors in favor of approval of the ApolloMed Merger Proposal, the Board Classification Proposal, each of the directors in the Election of Directors Proposal, the ApolloMed Compensation Proposal and the ApolloMed Adjournment Proposal, ApolloMed’s stockholders should keep in mind that ApolloMed’s directors and officers have interests in the proposals that are different from, or in addition to or in conflict with, the interests of its stockholders. These interests include:
| · | certain directors and officers of ApolloMed are expected to continue to serve as directors and officers of the combined company; |
| · | as current stockholders of ApolloMed, certain of ApolloMed’s directors and officers will retain an ownership stake in ApolloMed after the closing of the Merger, at which time the operations of the NMM business will comprise the majority of ApolloMed’s operations; |
| · | certain ApolloMed directors and officers have employment agreements with ApolloMed which are expected to remain in place following the Merger; |
| · | the Merger Agreement contemplates that Warren Hosseinion, M.D., the sole shareholder of MMG, will sell to APC-LSMA all the issued and outstanding shares of capital stock of MMG for $100 under the Maverick Stock Purchase Agreement; and |
| 31 |
| · | the continued indemnification of current directors and officers of ApolloMed and the continuation of directors’ and officers’ liability insurance after the Merger. |
For a more complete description of these interests, see “THE MERGER — Interests of ApolloMed’s Directors and Executive Officers in the Merger” beginning on page 151 of this joint proxy statement/prospectus.
Interests of NMM’s Directors and Executive Officers in the Merger (Page 153)
In considering the recommendation of the NMM board of directors that NMM shareholders vote to approve both of the presented proposals, NMM shareholders should be aware that some of NMM’s directors and officers have interests in the Merger and have arrangements that are different from, or in addition to, those of NMM shareholders generally. These interests and arrangements may create potential conflicts of interest. NMM’s board of directors was aware of these interests and considered these interests, among other matters, in adopting and approving the Merger Agreement and the transactions contemplated thereby, including the Merger, and in recommending that NMM shareholders approve the NMM Merger Proposal and the NMM Adjournment Proposal. For a more complete description of these interests, see “THE MERGER — Interests of NMM’s Directors and Executive Officers in the Merger” beginning on page 153 of this joint proxy statement/prospectus.
When NMM’s shareholders consider the recommendation of NMM’s board of directors in favor of approval of the NMM Merger Proposal and the NMM Adjournment Proposal, NMM’s shareholders should keep in mind that NMM’s directors and officers have interests in the proposals that are different from, or in addition to or in conflict with, the interests of its shareholders. These interests include:
| · | certain directors and officers of NMM are expected to continue to serve as directors and officers of the combined company; |
| · | the Merger Agreement contemplates that Warren Hosseinion, M.D., the sole shareholder of MMG, will sell to APC-LSMA (an entity in which Dr. Thomas Lam is the sole shareholder and the sole executive officer, but which is controlled and consolidated by APC) all the issued and outstanding shares of capital stock of MMG for $100 under the Maverick Stock Purchase Agreement; and |
| · | the continued indemnification of current directors and officers of NMM and the continuation of directors’ and officers’ liability insurance after the Merger. |
For a more complete description of these interests, see “THE MERGER — Interests of NMM’s Directors and Executive Officers in the Merger” beginning on page 153 of this joint proxy statement/prospectus.
Treatment of Existing ApolloMed Warrants Held by NMM Shareholders (Page 169)
Currently, NMM has an outstanding Series A warrant to purchase 1,111,111 shares of ApolloMed common stock and Series B warrant to purchase 555,555 shares of ApolloMed common stock (the “ApolloMed Warrants”), which were previously issued by ApolloMed to NMM. Immediately prior to the consummation of the Merger, NMM may distribute the ApolloMed Warrants, in-kind, to the NMM shareholders such that the ApolloMed Warrants shall not be exercised prior to the consummation of the Merger.
Board Composition and Management of ApolloMed after the Merger (Page 177)
Board of Directors
The ApolloMed board of directors at the Effective Time will consist of nine directors divided into three classes. At or immediately following the Effective Time, the ApolloMed board of directors will be designated as follows:
Class I Directors
| · | Michael F. Eng (NMM designee) |
| · | Thomas Lam, M.D. (NMM designee) |
| · | David G. Schmidt (ApolloMed designee) |
| 32 |
Class II Directors
| · | Mitchell W. Kitayama (NMM designee) |
| · | Kenneth Sim, M.D. (NMM designee) |
| · | Mark Fawcett (ApolloMed designee) |
Class III Directors
| · | Li Yu (NMM designee) |
| · | Warren Hosseinion, M.D. (ApolloMed designee) |
| · | Gary Augusta (ApolloMed designee) |
Management
At or immediately following the Effective Time, the ApolloMed executive officers will be appointed as follows:
| Officer Name: | Position: | |
| Kenneth Sim, M.D. | Executive Chairman | |
| Thomas Lam, M.D. | Co-Chief Executive Officer | |
| Warren Hosseinion, M.D. | Co-Chief Executive Officer | |
| Gary Augusta | President | |
| Hing Ang | Chief Operating Officer | |
| Mihir Shah | Chief Financial Officer | |
| Adrian Vazquez, M.D. | Co-Chief Medical Officer | |
| Albert Young, M.D. | Co-Chief Medical Officer |
ApolloMed stockholders will not have any appraisal rights under Delaware law in connection with the matters to be voted on at the ApolloMed special meeting.
NMM shareholders have the right to dissent from the Merger and assert dissenters’ rights, provided the requirements of the California Corporations Code are followed. Any NMM shareholder electing to exercise dissenters’ rights must strictly comply with the provisions of Chapter 13 of the California Corporations Code.
The failure of a NMM shareholder to comply strictly with the California Corporations Code requirements will result in a loss of dissenters’ rights. A copy of the relevant statutory provisions is attached as Annex I. See the section titled “THE MERGER – Dissenters’ Rights” beginning on page 144 of this joint proxy statement/prospectus.
Pursuant to the terms of the Merger Agreement, prior to the closing of the Merger, NMM has agreed to repurchase and cancel all NMM common stock (including any other securities exercisable for or convertible into NMM common stock, or rights to acquire NMM common stock) that are held by dissenting shareholders or by other shareholders who have exercised their dissenters’ rights in accordance with Chapter 13 of the California Corporations Code.
The Merger Agreement contains provisions that restrict each of ApolloMed and NMM from encouraging, soliciting, initiating or knowingly facilitating inquiries or proposals with respect to, or engaging in negotiations or discussions with, or providing confidential or non-public information to, any person concerning a merger, consolidation, sale of substantially all assets or other similar transaction involving ApolloMed or NMM that would result in the acquisition in any manner of more than 15% of the voting power in, or more than 15% of the fair market value of the applicable entity.
| 33 |
Conditions to Completion of the Merger (Page 166)
Currently, ApolloMed and NMM expect to complete the Merger during the fourth quarter of 2017. As set forth in this joint proxy statement/prospectus and in the Merger Agreement, each party’s obligation to complete the Merger depends on a number of conditions being satisfied or, where legally permissible, waived, including the following:
| · | the absence of any legal restraint or governmental order that would prevent or prohibit the completion of the Merger and the other transactions contemplated by the Merger Agreement; |
| · | the approval of the ApolloMed stockholders of the ApolloMed Merger Proposal, the Board Classification Proposal and each of the directors in the Election of Directors Proposal; |
| · | the approval of the Merger Agreement and the transactions contemplated thereby by NMM shareholders holding at least 95% of the outstanding shares of NMM common stock and representing at least 95% in number of the NMM shareholders; and |
| · | the effectiveness of the registration statement of which this joint proxy statement/prospectus is a part and the absence of any stop order or related proceeding initiated or threatened by the SEC and not concluded or withdrawn. |
The obligation of ApolloMed and Merger Sub to complete the Merger is subject to the satisfaction or waiver of the following additional conditions:
| · | NMM’s representations and warranties being true in all respects (to the extent qualified by materiality or material adverse effect) and being true in all material respects (to the extent not qualified by materiality or material adverse effect) as of the date of the Merger Agreement and closing, except for those otherwise qualified as to a specified date; |
| · | the performance, in all material respects, by NMM and the Shareholders’ Representative, of its covenants and agreements required to be performed or complied with before or on the closing date of the Merger; |
| · | no action commenced or threatened in writing by a governmental authority, in effect, that would restrain or prevent the closing of the Merger or transactions contemplated by the Merger Agreement or seeks damages in connection with such transactions; |
| · | delivery to ApolloMed at or before closing of all required approvals, consents and waivers from NMM and all other closing deliverables from NMM, including, but not limited to, delivery by all NMM shareholders of executed shareholder lock-up agreements (each, a “Lock-Up Agreement” and together, the “Lock-Up Agreements”); |
| · | the absence of any material adverse effect on NMM and no event will have occurred or circumstance will exist that, individually or in combination with any other events or circumstances, would reasonably be expected to have a material adverse effect on NMM. For a more complete discussion on what constitutes a material adverse effect on NMM, see the section titled “THE MERGER AGREEMENT — Representations and Warranties” beginning on page 161 of this joint proxy statement/prospectus; |
| · | NMM’s repurchase and cancellation of all shares of NMM common stock that will not be voted in favor of the Merger or the other transactions contemplated by the Merger Agreement such that there shall be no NMM shareholders who have exercised their dissenters’ rights in respect of the Merger or any other dissenting shareholders; and |
| · | satisfaction or waiver of all conditions precedent to APC-LSMA’s purchase of all of the issued and outstanding capital stock of MMG. |
The obligation of NMM to complete the Merger is subject to the satisfaction or waiver of the following additional conditions:
| 34 |
| · | the representations and warranties of ApolloMed and Merger Sub being true in all respects, to the extent qualified by materiality or material adverse effect, and otherwise will be true in all material respects as of the date of the Merger Agreement and closing, except for those otherwise qualified as to a specified date; |
| · | the performance, in all material respects, by ApolloMed and Merger Sub of their covenants and agreements required to be performed or complied with before or on the closing date of the Merger; |
| · | no action commenced or threatened in writing by a governmental authority, in effect, that would restrain or prevent the closing of the Merger or transactions contemplated by the Merger Agreement or seeks damages in connection with such transactions; |
| · | receipt by, and delivery to, NMM at or before closing of all required approvals, consents and waivers from ApolloMed and Merger Sub and all closing deliverables and payments from ApolloMed; |
| · | the absence of any material adverse effect on ApolloMed and no event will have occurred or circumstance will exist that, individually or in combination with any other events or circumstances, would reasonably be expected to have a material adverse effect on NMM. For a more complete discussion on what constitutes a material adverse effect on NMM, see the section titled “THE MERGER AGREEMENT — Representations and Warranties” beginning on page 161 of this joint proxy statement/prospectus; and |
| · | satisfaction or waiver of all conditions precedent to APC-LSMA’s purchase of all of the issued and outstanding capital stock of MMG. |
Neither ApolloMed nor NMM can be certain when, or if, the conditions to the Merger will be satisfied or waived, or that the Merger will be completed. See “THE MERGER AGREEMENT — Conditions to Completion of the Merger” on page 166 of this joint proxy statement/prospectus for a more complete summary of the conditions that must be satisfied prior to closing.
Termination of Merger Agreement (Page 167)
The Merger Agreement may be terminated at any time prior to the closing of the Merger by mutual written consent of the parties. The Merger Agreement may also generally be terminated by either party, prior to closing of the Merger, in the following circumstances:
| · | if the Merger and other transactions contemplated by the Merger Agreement have not been consummated on or before March 31, 2018 (the “End Date”); |
| · | any law, order or legal restraint (a) makes the consummation of the Merger and the other transactions contemplated by the Merger Agreement illegal or otherwise prohibited or (b) enjoins a party from consummating the Merger and the other transactions contemplated by the Merger Agreement and such injunction, other legal restraint or order shall have become final and non-appealable; |
| · | if either party (i) withdraws its approval, recommendation or declaration of advisability of the Merger, the Merger Agreement or the consummation of the transactions contemplated thereunder, (ii) adopts, approves or declares advisable the adoption of any offer, proposal for merger, acquisition of assets or other business combination that would result in the acquisition of more than 15% of the voting power in, or more than 15% of the fair market value of the business, assets or deposits of such party (an “Acquisition Proposal”) or (iii) agree or propose to take any such actions (each such action, an “Adverse Recommended Change”); |
| · | if ApolloMed fails to obtain the requisite approval of the ApolloMed Merger Proposal, the Board Classification Proposal or each of the directors in the Election of Directors Proposal at its special meeting of stockholders or any adjournment or postponement thereof; |
| · | if NMM fails to obtain the requisite approval of the NMM Merger Proposal at its special meeting of shareholders or any adjournment or postponement thereof; |
| · | if there has been a material adverse effect by either party and such material adverse effect is not cured within 10 business days after receipt of written notice by the other party; |
| 35 |
| · | if there is a material breach by either party of the non-solicitation provisions or approval provisions in the Merger Agreement; or |
| · | if there has been a material breach by either party of any representation, warranty, covenant or agreement contained in Merger Agreement that has prevented or would prevent the satisfaction of any condition to the obligations of such party at the closing and such breach has not been waived or cured within 10 business days after written notice by the other party. |
In the event that the Merger Agreement is terminated pursuant to the above, the Merger Agreement will be void without further obligation or liability of any party (except for certain parties’ obligations of confidentiality and non-use of the other party’s confidential information) and no party will be entitled to any monetary damages, injunctive relief or any indemnification subject to certain limited exceptions; provided, that no party will be relieved from liability resulting from a knowing and intentional breach prior to such termination of any of its representations, warranties, covenants or agreements set forth in the Merger Agreement or any other transaction contemplated thereunder.
Notwithstanding the above, ApolloMed and NMM are each subject to a $1,500,000 termination fee in certain circumstances where the Merger Agreement is terminated and it enters into any definitive agreement with respect to, or consummates, any Acquisition Proposal within twelve months of the date of any such termination.
See “THE MERGER AGREEMENT — Termination of the Merger Agreement” on page 167 of this joint proxy statement/prospectus for a more complete summary of the termination options of either party.
Comparison of the Rights of ApolloMed Stockholders and NMM Shareholders (Page 309)
ApolloMed is incorporated under the laws of the State of Delaware and NMM is formed under the laws of the State of California. If the Merger is completed, NMM shareholders will become stockholders of ApolloMed, and their rights will be governed by Delaware General Corporation Law (the “DGCL”), as well as the ApolloMed Charter and ApolloMed Bylaws, each as amended to reflect the proposals being voted on at the ApolloMed special meeting. The rights of ApolloMed stockholders contained in the ApolloMed Charter and the ApolloMed Bylaws, as amended, and the DGCL differ from the rights of NMM shareholders under NMM’s Articles of Incorporation (as amended from time to time, the “NMM Articles”) and the California Corporations Code, as more fully described under the section entitled “COMPARISON OF RIGHTS OF APOLLOMED STOCKHOLDERS AND NMM SHAREHOLDERS” on page 309 of this joint proxy statement/prospectus.
Accounting Treatment (Page 157)
Although ApolloMed is the legal acquirer and will issue shares of its common stock to effect the Merger with NMM, the business combination will be accounted for as a “reverse merger” under the acquisition method of accounting principles generally accepted in the United States (“GAAP”). Under the “acquisition” method of accounting, the assets and liabilities of ApolloMed will be recorded, as of the completion of the Merger, at their respective fair values in the financial statements of NMM. The financial statements of NMM issued after the completion of the Merger will reflect these values but will not be restated retroactively to reflect the historical financial position or results of operations of ApolloMed.
For a more complete discussion of the accounting treatment of the Merger, see the section entitled “The Merger — Accounting Treatment.”
Considerations with Respect to U.S. Federal Income Tax Consequences of the Merger (Page 208)
The Merger has been structured to qualify as a reorganization within the meaning of Section 368(a) of the Code. Assuming the Merger qualifies as a reorganization and subject to the qualifications and limitations set forth in the section entitled “The Merger — Considerations with Respect to U.S. Federal Income Tax Consequences of the Merger,” the material U.S. federal income tax consequences to U.S. Holders (as defined herein) of NMM common stock should be as follows:
| · | an NMM shareholder should not recognize gain or loss upon the exchange of NMM common stock for ApolloMed common stock and warrants pursuant to the Merger, except to the extent of cash received in lieu of a fractional share of ApolloMed common stock as described below or to the extent of any imputed interest with respect to the Holdback Shares as described below; |
| 36 |
| · | an NMM shareholder’s aggregate tax basis for the shares of ApolloMed common stock and warrants received in the Merger (including any fractional share interest for which cash is received) should equal the shareholder’s aggregate tax basis in the shares of NMM common stock surrendered upon completion of the Merger (such aggregate tax basis to be allocated to such shares of ApolloMed common stock and warrants based on their relative fair market values); |
| · | the holding period of the shares of ApolloMed common stock and warrants received by an NMM shareholder in the Merger should include the holding period of the shares of NMM common stock surrendered in exchange therefor provided the surrendered NMM common stock is held as a capital asset (generally, property held for investment) at the time of the Merger; and |
| · | an NMM shareholder who receives cash in lieu of a fractional share of ApolloMed common stock in the Merger should recognize capital gain or loss in an amount equal to the difference between the amount of cash received instead of a fractional share and the shareholder’s tax basis allocable to such fractional share. |
Completion of the Merger, however, is not conditioned upon a receipt of an opinion from counsel that the Merger qualifies as a reorganization, and the Merger will occur even if the Merger does not qualify as a reorganization and NMM shareholders are fully taxed on the shares of ApolloMed common stock and warrants they receive in the Merger.
To the extent NMM distributes existing ApolloMed Warrants held thereby to NMM shareholders prior to the consummation of the Merger, such distribution will constitute a dividend for U.S. federal income tax purposes to the extent of NMM’s current or accumulated earnings and profits, as determined under U.S. federal income tax principles. See “CERTAIN MATERIAL U.S. FEDERAL INCOME TAX CONSEQUENCES OF THE MERGER” on page 208 of this joint proxy statement/prospectus for more information.
A portion of each Holdback Share issued to an NMM shareholder will be treated as “imputed interest” under Section 483 of the Code, with the amount of such imputed interest being based upon the applicable federal rate at the time of Merger and the period between the closing date of the Merger and the date on which the Holdback Share is issued to the NMM shareholder. The portion of such Holdback Share treated as imputed interest will be ordinary income to the NMM shareholder, rather than capital gain, and will be taxable to the NMM shareholder upon receipt.
Tax matters are very complicated, and the tax consequences of the Merger to a particular NMM shareholder will depend on such shareholder’s circumstances. Accordingly, you should consult your tax advisor for a full understanding of the tax consequences of the Merger to you, including the applicability and effect of federal, state, local and non-U.S. income and other tax laws. For more information, please see the section entitled “CONSIDERATIONS WITH RESPECT TO U.S. FEDERAL INCOME TAX CONSEQUENCES OF THE MERGER” beginning on page 36 of this joint proxy statement/prospectus.
Regulatory Approvals (Page 154)
ApolloMed must comply with the applicable federal and state securities laws in connection with the issuance of the securities in the Merger and the filing with the SEC of the registration statement of which this joint proxy statement/prospectus forms a part.
In addition, completion of the Merger is subject to the expiration or termination of the waiting period applicable to the Merger under the Hart-Scott-Rodino Antitrust Improvements Act of 1976, as amended (the “HSR Act”). Under the HSR Act, the Merger may not be completed until the expiration of a 30-calendar day waiting period, which began when ApolloMed and NMM each filed a Premerger Notification and Report Form under the HSR Act with the Federal Trade Commission (the “FTC”) and the Antitrust Division of the Department of Justice (the “Antitrust Division”) on June 7, 2017, unless the FTC and Antitrust Division grant early termination of such waiting period. The required waiting period with respect to the Merger expired at 11:59 p.m., New York City time, on July 7, 2017. The parties to the Merger Agreement are required to use their respective reasonable best efforts to consummate the offer and the Merger, including by taking all reasonable actions necessary to obtain any antitrust or other regulatory approvals.
For a more complete discussion of the regulatory approvals required in connection with the Merger, see the section entitled “THE MERGER — Regulatory Approvals Required for the Merger” on page 154 of this joint proxy statement/prospectus.
| 37 |
Opinion of ApolloMed’s Financial Advisor (Page 132)
In connection with the Merger, Merrill Lynch, Pierce, Fenner & Smith Incorporated (“BofA Merrill Lynch”), ApolloMed’s financial advisor, delivered to ApolloMed’s board of directors a written opinion, dated December 21, 2016, as to the fairness, from a financial point of view and as of the date of the opinion, of the exchange ratio to ApolloMed, assuming, at the direction of ApolloMed, that the exchange ratio would be 0.07002656301. The full text of the written opinion, dated December 21, 2016, of BofA Merrill Lynch, which describes, among other things, the assumptions made, procedures followed, factors considered and limitations on the review undertaken, is attached as Annex G to this document and is incorporated by reference herein in its entirety. BofA Merrill Lynch provided its opinion to ApolloMed’s board of directors (in its capacity as such) for the benefit and use of ApolloMed’s board of directors in connection with and for purposes of its evaluation of the exchange ratio from a financial point of view, assuming, at the direction of ApolloMed, that the exchange ratio would be 0.07002656301. BofA Merrill Lynch’s opinion does not address any other aspect of the Merger and no opinion or view was expressed as to the relative merits of the Merger in comparison to other strategies or transactions that might be available to ApolloMed or in which ApolloMed might engage or as to the underlying business decision of ApolloMed to proceed with or effect the Merger. BofA Merrill Lynch’s opinion does not address any other aspect of the Merger and does not constitute a recommendation to any stockholder as to how to vote or act in connection with the proposed Merger or any related matter.
For further information, see the section entitled “THE MERGER — Opinion of ApolloMed’s Financial Advisor” beginning on page 132 and the full text of the opinion attached as Annex G to this joint proxy statement/prospectus.
Opinion of NMM’s Financial Advisor (Page 138)
On December 20, 2016, at a meeting of the NMM board of directors held to evaluate the Merger, Vantage Point Advisors, Inc. (“Vantage Point”) rendered to the NMM board of directors an oral opinion, which was confirmed by delivery of a written opinion signed and dated December 21, 2016, to the effect that, as of the date of the opinion, and based upon and subject to the factors, assumptions and limitations set forth therein, the Merger was fair, from a financial point of view, to NMM and its common shareholders.
Vantage Point’s opinion was directed to the NMM board of directors and only addressed the fairness, from a financial point of view, of the exchange ratio and did not address any other terms of the Merger. The summary of Vantage Point’s opinion as set forth in this joint proxy statement/prospectus is qualified in its entirety by reference to the full text of the written opinion, which is attached as Annex H to this joint proxy statement/prospectus, and sets forth the procedures followed, assumptions made, qualifications and limitations of the review undertaken and other matters considered by Vantage Point in preparing its opinion. Vantage Point has consented to the inclusion of its fairness opinion as Annex H to this joint proxy statement/prospectus. Neither Vantage Point’s opinion nor the summary of its opinion and the related analyses set forth in this joint proxy statement/prospectus are intended to be, or constitute, advice or a recommendation to the NMM board of directors, NMM or any shareholder as to how to vote or act in connection with the Merger or any related matter.
For further information, see the section entitled “THE MERGER — Opinion of NMM’s Financial Advisor” beginning on page 138 and the full text of the opinion attached as Annex H to this joint proxy statement/prospectus.
Surrender of NMM Stock Certificates (Page 160)
Stock certificates representing shares of NMM common stock shall be surrendered to the exchange agent as further set forth on the letter of transmittal, unless any of such certificate(s) are held by NMM or any of its representatives, in which case such certificate(s) shall be delivered to the exchange agent on the NMM shareholder’s behalf.
See “THE MERGER AGREEMENT — Exchange Procedures” on page 160 of this joint proxy statement/prospectus for a more detailed description of the surrendering of NMM stock certificates.
| 38 |
SELECTED HISTORICAL FINANCIAL INFORMATION OF APOLLOMED
The following table sets forth selected historical financial information of ApolloMed for each of the periods presented. Such information has been derived from ApolloMed’s audited financial statements as of and for the fiscal years ended March 31, 2017 and 2016 and the three months ended June 30, 2017 and June 30, 2016, which is included elsewhere in this joint proxy statement/prospectus.
The following table should be read together with “INFORMATION ABOUT APOLLOMED — ApolloMed Management’s Discussion and Analysis of Financial Condition and Results of Operations” beginning on page 240 of this joint proxy statement/prospectus and ApolloMed’s audited financial statements for the fiscal years ended March 31, 2017 and 2016 and the three months ended June 30, 2017 and 2016 and related notes beginning on page 240 of this joint proxy statement/prospectus.
ApolloMed’s historical results are not necessarily indicative of results to be expected in any future period.
| Fiscal Year Ended March 31, | ||||||||
| 2017 | 2016 | |||||||
| Statement of Operations Data: | ||||||||
| Net Revenues | $ | 57,427,701 | $ | 44,048,740 | ||||
| Costs and Expenses | ||||||||
| Cost of services | 48,735,537 | 34,000,786 | ||||||
| General and administrative | 18,583,372 | 16,962,687 | ||||||
| Depreciation and amortization | 645,742 | 351,396 | ||||||
| Total costs and expenses | 67,964,651 | 51,314,869 | ||||||
| Loss from Operations | (10,536,950 | ) | (7,266,129 | ) | ||||
| Other (expense) Income | ||||||||
| Interest expense | (82,905 | ) | (542,296 | ) | ||||
| Gain (loss) on change in fair value of warrant and conversion feature liabilities, net | 1,633,333 | (408,692 | ) | |||||
| Gain on deconsolidation of variable interest entity | 242,411 | - | ||||||
| Loss on debt extinguishment, net | - | (266,366 | ) | |||||
| Other income | 14,701 | 239,057 | ||||||
| Total other expense, net | 1,807,540 | (978,297 | ) | |||||
| Net loss | (8,681,915 | ) | (8,173,389 | ) | ||||
| Net loss per share: | ||||||||
| Basic and diluted | $ | (1.49 | ) | $ | (1.79 | ) | ||
| Weighted average shares of common stock outstanding: | ||||||||
| Basic and diluted | 6,001,680 | 5,212,927 | ||||||
| Balance Sheet Data: | ||||||||
| Cash and cash equivalents | $ | 8,664,211 | $ | 9,270,010 | ||||
| Total assets | $ | 20,644,557 | $ | 19,566,533 | ||||
| Total liabilities | 20,374,189 | 11,015,247 | ||||||
| Total liabilities, mezzanine equity and stockholders’ equity | $ | 20,644,557 | $ | 19,566,533 | ||||
| Three
Months Ended June 30, |
||||||||
| 2017 | 2016 | |||||||
| Statement of Operations Data | ||||||||
| Net revenues | $ | 41,575,480 | $ | 12,371,673 | ||||
| Costs and expenses | ||||||||
| Cost of services | 40,239,642 | 10,133,005 | ||||||
| General and administrative | 4,889,184 | 3,836,475 | ||||||
| Depreciation and amortization | 155,267 | 164,658 | ||||||
| Total costs and expenses | 45,284,093 | 14,134,138 | ||||||
| Loss from operations | (3,708,613 | ) | (1,762,465 | ) | ||||
| Other (expense) income: | ||||||||
| Interest expense | (192,989 | ) | (2,659 | ) | ||||
| Gain on change in fair value of warrant liability | - | 822,222 | ||||||
| Other income | 38,657 | 1,971 | ||||||
| Total other (expense) income, net | (154,332 | ) | 821,534 | |||||
| Loss before benefit from income taxes | (3,862,945 | ) | (940,931 | ) | ||||
| Benefit from income taxes | (29,891 | ) | (41,553 | ) | ||||
| Net loss | (3,833,054 | ) | (899,378 | ) | ||||
| Net loss (income) attributable to non-controlling interest | 221,242 | (415,879 | ) | |||||
| Net loss attributable to Apollo Medical Holdings, Inc. | $ | (3,611,812 | ) | $ | (1,315,257 | ) | ||
| Net loss per share: | ||||||||
| Basic and diluted | $ | (0.60 | ) | $ | (0.22 | ) | ||
| Weighted average number of shares of common stock outstanding: | ||||||||
| Basic and diluted | ||||||||
| Balance Sheet Data: | ||||||||
| Cash and cash equivalents | $ | 31,206,495 | ||||||
| Total assets | $ | 43,298,794 | ||||||
| Total liabilities | $ | 46,637,914 | ||||||
| Total liabilities, mezzanine equity and stockholders’ equity | $ | 43,298,794 | ||||||
| 39 |
SELECTED HISTORICAL FINANCIAL INFORMATION OF NMM
The following table sets forth selected historical financial information of NMM for each of the periods presented. The historical financial information for the fiscal years ended December 31, 2016, 2015 and 2014 and for the six months ended June 30, 2017 and 2016 has been derived from NMM’s audited financial statements as of and for the fiscal years ended December 31, 2016, 2015 and 2014, and from NMM’s unaudited financial statements as of and for the six months ended June 30, 2017 and 2016, respectively, each of which is included elsewhere in this joint proxy statement/prospectus. The historical financial information for the fiscal years ended December 31, 2013 and 2012 has been derived from NMM’s unaudited historical consolidated financial statements that are not included in this joint proxy statement/prospectus. The results of operations for the six months ended June 30, 2017 and June 30, 2016 are not necessarily indicative of the results of operations for the full year or any other interim period. NMM management prepared the unaudited information as of and for the six months ended June 30, 2017 and 2016 on the same basis as it prepared NMM’s audited consolidated financial statements. In the opinion of NMM management, this information reflects all adjustments consisting of only normal recurring adjustments necessary for a fair presentation of this data for those dates.
The following table should be read together with “INFORMATION ABOUT NMM — NMM Management’s Discussion and Analysis of Financial Condition and Results of Operations” beginning on page 285 of this joint proxy statement/prospectus and NMM’s audited financial statements for the fiscal years ended December 31, 2016, 2015 and 2014 and related notes and unaudited financial statements as of and for the six months ended June 30, 2017 and 2016 and related notes beginning on page 285 of this joint proxy statement/prospectus.
NMM’s historical results are not necessarily indicative of results to be expected in any future period.
| 40 |
| As of or For the | ||||||||||||||||||||||||||||
| Six Months Ended | ||||||||||||||||||||||||||||
| June 30, | As of or For the Years Ended December 31, | |||||||||||||||||||||||||||
| 2017 | 2016 | 2016 | 2015 | 2014 | 2013 | 2012 | ||||||||||||||||||||||
| Balance Sheet Data: | (unaudited) | (unaudited) | [3] | [2] | [1] | [1] | ||||||||||||||||||||||
| Total assets | $ | 343,781,492 | $ | 355,303,468 | $ | 349,998,962 | $ | 362,486,567 | $ | 176,650,244 | $ | 28,611,785 | $ | 24,790,511 | ||||||||||||||
| Total non-current liabilities | 44,935,181 | 52,733,098 | 48,929,857 | 52,394,197 | 32,627,220 | 608,779 | 4,620,183 | |||||||||||||||||||||
| Total liabilities | 89,097,134 | 95,018,272 | 99,555,688 | 116,958,729 | 73,125,287 | 13,763,670 | 12,541,748 | |||||||||||||||||||||
| Total mezzanine equity - noncontrolling interest | 160,407,386 | 163,531,239 | 162,855,554 | 161,028,806 | 105,067,503 | 13,189,607 | 11,798,472 | |||||||||||||||||||||
| Total mezzanine equity - redeemable common stock | 88,217,116 | 82,234,601 | 87,979,414 | 76,318,873 | 1,971,658 | 4,475,331 | 4,475,331 | |||||||||||||||||||||
| Total Network Medical Management, Inc. shareholders’ equity (deficit) | 5,571,093 | 14,074,149 | (773,311 | ) | 7,773,162 | (4,108,304 | ) | (3,479,567 | ) | (4,150,652 | ) | |||||||||||||||||
| Allied Pacific of California IPA's noncontrolling interest in Concourse Diagnostic Surgery Center, LLC | 448,763 | 445,207 | 381,617 | 406,997 | 594,100 | 662,744 | 125,612 | |||||||||||||||||||||
| Total shareholders' equity (deficit) | 6,059,856 | 14,519,356 | (391,694 | ) | 8,180,159 | (3,514,204 | ) | (2,816,823 | ) | (4,025,040 | ) | |||||||||||||||||
| Total liabilities, mezzanine equity and shareholders' equity (deficit) | 343,781,492 | 355,303,468 | 349,998,962 | 362,486,567 | 176,650,244 | 28,611,785 | 24,790,511 | |||||||||||||||||||||
| Results of Operations: | ||||||||||||||||||||||||||||
| Total revenue | $ | 166,647,762 | $ | 149,121,384 | $ | 305,934,915 | $ | 313,124,705 | $ | 134,340,089 | $ | 84,090,680 | $ | 60,086,562 | ||||||||||||||
| Total expenses | 146,910,900 | 140,697,021 | 294,246,302 | 269,451,579 | 147,427,362 | 82,402,221 | 59,763,629 | |||||||||||||||||||||
| Income (loss) from operations | 19,736,862 | 8,424,363 | 11,688,613 | 43,673,126 | (13,087,273 | ) | 1,688,459 | 322,933 | ||||||||||||||||||||
| Net income (loss) | 13,089,250 | 8,102,517 | 10,019,797 | 26,679,623 | (13,702,710 | ) | 1,397,633 | 120,053 | ||||||||||||||||||||
| Net income (loss) attributable to noncontrolling interests | 6,744,846 | 1,801,530 | (1,433,730 | ) | 13,862,522 | (13,073,974 | ) | 726,548 | (578,534 | ) | ||||||||||||||||||
| Net income (loss) attributable to Network Medical Management, Inc. | 6,344,404 | 6,300,987 | 11,453,527 | 12,817,101 | (628,736 | ) | 671,085 | 698,587 | ||||||||||||||||||||
| Per Share Data: | ||||||||||||||||||||||||||||
| Earnings per common share - basic | $ | 0.02 | $ | 0.02 | $ | 0.03 | $ | 0.05 | $ | (0.00 | ) | $ | 0.00 | $ | 0.00 | |||||||||||||
| Earnings per common share - diluted | 0.02 | 0.02 | 0.03 | 0.05 | (0.00 | ) | 0.00 | 0.00 | ||||||||||||||||||||
| Weighted average shares of common stock outstanding - basic | 366,343,818 | 359,724,706 | 360,634,339 | 256,619,159 | 175,818,798 | 175,933,710 | 175,933,710 | |||||||||||||||||||||
| Weighted average shares of common stock outstanding - diluted | 373,769,718 | 366,861,151 | 367,945,833 | 263,734,916 | 175,818,798 | 175,933,710 | 175,933,710 | |||||||||||||||||||||
| [1] | Certain reclassifications have been made to the 2013 and 2012 unaudited consolidated financial statements to conform to the current period presentation. |
| [2] | In October 2014, APC merged with Pacific Independent Physician Association ("PIPA'), which resulted in significant changes to the results of operations. |
| [3] | In April 2015, APC merged with Physicians Healthways Medical Corporation ("PHW") and in July 2015, NMM merged with Pacific Independent Physician Association Management Service Organization ("PIPA MSO"), which resulted in significant changes to the results of operations. |
| 41 |
SELECTED UNAUDITED PRO FORMA CONDENSED COMBINED FINANCIAL DATA
The following selected unaudited pro forma condensed combined financial data gives effect to the proposed Merger of Merger Sub with and into NMM, which will be accounted for as a “reverse merger” business combination under the acquisition method of accounting with NMM treated as the accounting acquirer. NMM was determined to be the accounting acquirer based upon the terms of the Merger and other factors, such as relative voting rights and the composition of the combined company’s board and senior management. The selected unaudited pro forma condensed combined financial data presented below is based on, and should be read in conjunction with, the historical financial statements of ApolloMed that appear elsewhere in this joint proxy statement/prospectus, the unaudited pro forma condensed combined financial statements which include ApolloMed and NMM that appear elsewhere in this joint proxy statement/prospectus, including the footnotes thereto, and the historical financial statements of NMM and ApolloMed that appear elsewhere in this joint proxy statement/prospectus. See the sections entitled, “Where You Can Find More Information” and “Unaudited Pro Forma Condensed Combined Financial Statements,” for additional information.
The following selected unaudited pro forma condensed combined balance sheet data as of June 30, 2017 combines the historical unaudited condensed balance sheet of NMM as of June 30, 2017 and the historical unaudited condensed consolidated balance sheet of ApolloMed as of June 30, 2017, giving pro forma effect to the Merger as if the Merger had been completed on June 30, 2017. In addition, because NMM has a fiscal year end of December 31 and ApolloMed has a fiscal year end of March 31, the following selected unaudited pro forma condensed combined statements of operations for the fiscal year ended March 31, 2017 combine the historical condensed statement of operations of ApolloMed for the year ended March 31, 2017 and for the fiscal year ended December 31, 2016 for NMM, and for the three months ended June 30, 2017 combine the historical condensed statement of operations of ApolloMed for the three months ended June 30, 2017 and the historical condensed statement of operations of NMM for its three months ended March 31, 2017, giving pro forma effect to the Merger as if it had been completed on April 1, 2017.
The selected unaudited pro forma condensed combined financial data is presented for illustrative purposes only and is not necessarily indicative of the actual or future financial position or results of operations that would have been realized if the proposed Merger had been completed as of the dates indicated in the unaudited pro forma condensed combined financial statements or that will be realized upon the consummation of the proposed Merger.
Unaudited Pro Forma Condensed Combined Statements of Operations, Balance Sheet and Other Data:
| As of June 30, 2017 |
||||
| (in thousands) | ||||
| Balance Sheet Data | ||||
| Cash and cash equivalents | $ | 88,528 | ||
| Working capital | $ | 24,352 | ||
| Total assets | $ | 432,628 | ||
| Total liabilities | $ | 127,558 | ||
| Retained earnings | $ | 10,900 | ||
| Total stockholders' equity | $ | 134,425 | ||
| For the Three Months Ended June 30, 2017 |
||||
| (in thousands, except per share amounts) | ||||
| Statements of Operations Data | ||||
| Total revenue | $ | 125,749 | ||
| Income from operations | $ | 11,629 | ||
| Net income | $ | 7,687 | ||
| Net income attributable to common stockholders | $ | 1,481 | ||
| Net income per share attributable to common stockholders, basic | $ | 0.04 | ||
| Net income per share attributable to common stockholders, diluted | $ | 0.04 | ||
| 42 |
COMPARATIVE HISTORICAL AND UNAUDITED PRO FORMA PER SHARE DATA
The information below reflects the historical net loss and book value per share of ApolloMed common stock and the historical net loss and book value per share of NMM common stock in comparison with the unaudited pro forma net loss and book value per share after giving effect to the Merger on a pro forma basis.
Because NMM has a fiscal year end of December 31 and ApolloMed has a fiscal year end of March 31, the following unaudited pro forma net loss and book value per share data for the fiscal year ended March 31, 2017 was calculated using the historical condensed combined statement of operations data of ApolloMed for its three months ended June 30, 2017, and the historical condensed combined statement of operations data of NMM for its three months ended March 31, 2017, giving pro forma effect to the Merger as if it had been completed on April 1, 2017.
The unaudited pro forma per share data is presented for illustrative purposes only and is not necessarily indicative of actual or future financial position or results of operations that would have been realized if the proposed Merger had been completed as of the dates indicated or will be realized upon the completion of the proposed Merger. Although ApolloMed has not declared or paid any dividends during the periods presented, NMM has declared and paid dividends during such periods.
| As of June 30, 2017 and for the three months ended June 30, 2017 |
||||
| NMM: | ||||
| Book value per share – historical | $ | 0.02 | ||
| Basic net loss per share – historical | $ | 0.01 | ||
| Diluted net loss per share – historical | $ | 0.01 | ||
|
ApolloMed: |
||||
| Book value per share – historical | $ | (0.55 | ) | |
| Basic and diluted net loss per share – historical | $ | (0.60 | ) | |
| Combined: | ||||
| Book value per share – pro forma | 3.67 | |||
| Basic and diluted net income per share – pro forma | $ | 0.04 | ||
| Basic and diluted net income per share – pro forma | $ | 0.04 | ||
| 43 |
You should carefully consider the risks described below in evaluating whether to vote for the proposals discussed herein. The risks and uncertainties described below are not the only ones ApolloMed and NMM face, and these factors should be considered in conjunction with general investment risks and other information included in this joint proxy statement/prospectus, including the matters addressed in the section entitled “CAUTIONARY STATEMENT REGARDING FORWARD-LOOKING STATEMENTS” beginning on page 100 of this joint proxy statement/prospectus.
Risks Related to the Proposed Merger
The issuance of shares of ApolloMed common stock and warrants to purchase ApolloMed common stock to NMM shareholders in the Merger will substantially dilute the voting power of current ApolloMed stockholders. Having this diluted share position may reduce the influence that current ApolloMed stockholders have on the management of ApolloMed.
Pursuant to the Merger Agreement, at the Effective Time, each issued and outstanding share of NMM common stock will be converted into the right to receive such number of fully paid and nonassessable ApolloMed shares of common stock that results in the NMM shareholders having a right to receive (A) an aggregate number of shares of ApolloMed common stock that represents 82% of the total issued and outstanding shares of ApolloMed common stock immediately following the Effective Time, assuming there are no NMM dissenting shareholder interests as of the Effective Time, calculated in accordance with the Merger Agreement (see “THE MERGER AGREEMENT – Effects of Merger; Merger Consideration” beginning on page 159), plus (B) an aggregate of 2,566,666 shares of ApolloMed common stock, assuming there are no NMM dissenting shareholder interests as of the Effective Time. In addition, each NMM shareholder shall be entitled to receive such shareholder’s pro rata portion of (i) warrants to purchase an aggregate of 850,000 shares of ApolloMed common stock, exercisable at $11.00 per share and (ii) warrants to purchase an aggregate of 900,000 shares of ApolloMed common stock, exercisable at $10.00 per share. Accordingly, the issuance of the shares of ApolloMed common stock to NMM shareholders in the Merger or the exercise of warrants to purchase ApolloMed common stock issued to such NMM shareholders will significantly reduce the ownership stake and relative voting power of each share of ApolloMed common stock held by current ApolloMed stockholders. Consequently, following the Merger, the ability of ApolloMed’s current stockholders to influence the management of ApolloMed will be substantially reduced.
Any release or issuance of the Holdback Shares following the consummation of the Merger may dilute the voting power of the current ApolloMed stockholders.
The Merger Agreement requires that at the Effective Time, ApolloMed will hold back the Holdback Shares to secure indemnification of ApolloMed and its affiliates under the Merger Agreement. The Holdback Shares will be held for a period of up to 24 months after the closing of the Merger, during which ApolloMed may seek indemnification for any breach of, or noncompliance with, any provision of the Merger Agreement by NMM. At the end of the first year following the closing of the Merger, 50% of the Holdback Shares will be released to the pre-Merger NMM shareholders (subject to any reduction for any indemnification claims) and at the end of the second year following the closing of the Merger, the remainder of the Holdback Shares will be released to the pre-Merger NMM shareholders (subject to any reduction for any indemnification claims). Separately, indemnification of pre-Merger NMM shareholders under the Merger Agreement will be made by the issuance by ApolloMed to pre-Merger NMM shareholders of new additional shares of common stock (capped at the same number of shares of ApolloMed common stock as the Holdback Shares). To the extent Holdback Shares are released or issued, the ownership stake and relative voting power of each share of ApolloMed common stock held by the current ApolloMed stockholders will be reduced.
The exchange ratio is not adjustable based on the market price of ApolloMed common stock so the merger consideration at the closing may have a greater or lesser value than at the time the Merger Agreement was signed.
Upon completion of the Merger, each share of NMM common stock will be converted into the right to receive shares of ApolloMed common stock based on an exchange ratio that will be fixed at the time of the closing of the Merger based on the number of issued and outstanding shares of ApolloMed calculated in accordance with the Merger Agreement. See the section entitled “THE MERGER AGREEMENT — Effects of Merger; Merger Consideration.” The exchange ratio in the Merger Agreement will not be adjusted in the event of any change in the stock price of ApolloMed prior to the Merger. Any changes in the market price of ApolloMed common stock before the completion of the Merger will not affect the number of shares NMM shareholders will be entitled to receive pursuant to the Merger Agreement. Therefore, if before the completion of the Merger the market price of ApolloMed common stock declines from the market price on the date of the Merger Agreement, then NMM shareholders could receive merger consideration with substantially lower value. Similarly, if before the completion of the Merger the market price of ApolloMed common stock increases from the market price on the date of the Merger Agreement, then NMM shareholders could receive merger consideration with substantially more value for their shares of NMM common stock. Because the exchange ratio does not adjust as a result of changes in the value of ApolloMed common stock, for each one percentage point that the market value of ApolloMed common stock rises or declines, there is a corresponding one percentage point rise or decline, respectively, in the value of the total merger consideration issued to NMM shareholders.
| 44 |
The merger consideration to be received by NMM shareholders in the Merger is not consistent with the assumed exchange ratio on which BofA Merrill Lynch based its fairness opinion.
The exchange ratio set forth in the Merger Agreement is based in part on the number of shares of ApolloMed’s common stock issued and outstanding at the closing rather than a fixed ratio. At the direction of ApolloMed, BofA Merrill Lynch based its fairness opinion on the assumption that the exchange ratio would be 0.07002656301 at the closing. On December 21, 2016, the date of issuance of the BofA Merrill Lynch fairness opinion, there were 5,956,877 shares of common stock of ApolloMed outstanding. On [●], 2017, the latest practicable date prior to the date of this proxy statement/prospectus, there were 6,033,495 shares of common stock of ApolloMed outstanding. In addition, as a result of the amendments to the Merger Agreement entered into on March 30, 2017 and October 17, 2017, NMM shareholders will receive as additional merger consideration, (i) an aggregate of 2,566,666 shares of ApolloMed common stock, (ii) warrants to purchase an aggregate of 850,000 shares of ApolloMed common stock, exercisable at $11.00 per share and (iii) warrants to purchase an aggregate of 900,000 shares of ApolloMed common stock, exercisable at $10.00 per share, none of which were factored into the calculation of the exchange ratio that ApolloMed instructed BofA Merrill Lynch to assume at the time of issuance of the BofA Merrill Lynch fairness opinion. The actual exchange ratio at the closing is not consistent with the exchange ratio on which BofA Merrill Lynch based its fairness opinion.
The fairness opinion delivered to the ApolloMed and NMM board of directors by their respective financial advisors prior to signing the Merger Agreement does not reflect changes in circumstances between signing the Merger Agreement and the completion of the Merger, including the amendment to the Merger Agreement.
Neither ApolloMed nor NMM obtained an updated fairness opinion nor do they intend to obtain an updated fairness opinion reflecting any changes in circumstances between signing the Merger Agreement and the completion of the Merger, including the amendments to the Merger Agreement on March 30, 2017 and October 17, 2017. As such, the fairness opinions do not reflect the amendments to the Merger Agreement as well as any changes that may occur or may have already occurred after December 21, 2016 to the operations and prospects of ApolloMed or NMM, general market and economic conditions and other factors that may be beyond the control of ApolloMed or NMM, and on which the respective original fairness opinion was based. As a result, the current value of the common stock of ApolloMed and NMM may not be reflected in the fairness opinion. The fairness opinions do not speak as of the time the Merger will be completed or as of any date other than the date set forth in the fairness opinions. Because ApolloMed and NMM do not currently intend to request an updated fairness opinion, the fairness opinions will not address the fairness of the merger consideration, from a financial point of view, at the time the Merger is completed.
Because the Merger will be completed after the date of the ApolloMed special meeting of stockholders and the NMM special meeting of shareholders, at the time of the meetings, the exact number of shares of ApolloMed common stock that the NMM shareholders will receive upon completion of the Merger will be unknown.
Subject to the terms of the Merger Agreement, each issued and outstanding share of NMM common stock will be converted into the right to receive such number of fully paid and nonassessable ApolloMed shares of common stock that results in the NMM shareholders having a right to receive (A) an aggregate number of shares of ApolloMed common stock that represents 82% of the total issued and outstanding shares of ApolloMed common stock immediately following the Effective Time, assuming there are no NMM dissenting shareholder interests as of the Effective Time, calculated in accordance with the Merger Agreement (see “THE MERGER AGREEMENT – Effects of Merger; Merger Consideration” beginning on page 159), plus (B) an aggregate of 2,566,666 shares of ApolloMed common stock, assuming there are no NMM dissenting shareholder interests as of the Effective Time. In addition, each NMM shareholder shall be entitled to receive such shareholder’s pro rata portion of (i) warrants to purchase an aggregate of 850,000 shares of ApolloMed common stock, exercisable at $11.00 per share and (ii) warrants to purchase an aggregate of 900,000 shares of ApolloMed common stock, exercisable at $10.00 per share. Please see the section entitled “THE MERGER AGREEMENT — Effects of Merger; Merger Consideration”. Accordingly, the exact number of shares of ApolloMed common stock that NMM shareholders will receive upon completion of the Merger will not be available at the time of the ApolloMed special meeting of stockholders and the NMM special meeting of shareholders.
There is no assurance when or if the Merger will be completed. Any delay in completing the Merger may substantially reduce the benefits that ApolloMed and NMM expect to obtain from the Merger and any failure to complete the Merger could harm ApolloMed and NMM’s future business and operations.
Completion of the Merger is subject to the satisfaction or waiver of a number of conditions as set forth in the Merger Agreement. There can be no assurance that ApolloMed and NMM will be able to satisfy the closing conditions or that closing conditions beyond their control will be satisfied or waived. For a discussion of the conditions to the completion of the Merger, see the section entitled “THE MERGER AGREEMENT — Conditions to Completion of the Merger” beginning on page 166 of this joint proxy statement/prospectus. In addition, ApolloMed and NMM can agree at any time to terminate the Merger Agreement. ApolloMed and NMM can also terminate the Merger Agreement under other specified circumstances. See the section entitled “THE MERGER AGREEMENT — Termination of the Merger Agreement” beginning on page 167 of this joint proxy statement/prospectus.
If the Merger is not completed within the expected timeframe, such delay could result in additional transaction costs or other effects associated with uncertainty about the Merger. Furthermore, if the Merger is not completed, the ongoing businesses of ApolloMed and NMM could be adversely affected and each of ApolloMed and NMM will be subject to a variety of risks associated with the failure to complete the Merger, including without limitation the following:
| · | certain costs related to the Merger, such as legal and accounting fees, must be paid even if the Merger is not completed; |
| · | if the Merger Agreement is terminated under certain circumstances, either ApolloMed or NMM may be required to pay the other party a termination fee of $1.5 million, as applicable; |
| · | the attention of management of ApolloMed and NMM may have been diverted to the Merger rather than to each company’s own operations and the pursuit of other opportunities that could have been beneficial to each company; |
| · | the potential loss of key personnel during the pendency of the Merger as employees may experience uncertainty about their future roles with the combined company; |
| 45 |
| · | reputational harm due to the adverse perception of any failure to successfully complete the Merger; |
| · | the price of ApolloMed stock may decline and remain volatile; |
| · | ApolloMed and NMM will have been subject to certain restrictions on the conduct of their businesses which may have prevented them from making certain acquisitions or dispositions or pursuing certain business opportunities while the Merger was pending; and |
| · | each of ApolloMed and NMM may be subject to litigation related to the Merger or any failure to complete the Merger. |
In addition, if the Merger Agreement is terminated ApolloMed is likely to have an immediate financial need to raise additional capital to fund ApolloMed’s business and meet ApolloMed’s expenses, including both transactional and operational expenses.
Because the lack of a public market for NMM’s outstanding shares makes it difficult to evaluate the fairness of the Merger, NMM shareholders may receive consideration in the Merger that is greater than or less than the fair market value of the shares of NMM common stock.
The outstanding capital stock of NMM is privately held and is not traded in any public market. The lack of a public market makes it extremely difficult to determine the fair market value of shares of NMM common stock. Since the percentage of ApolloMed’s common stock to be issued to NMM shareholders was determined based on negotiations between the parties, it is possible that the value of the ApolloMed common stock to be issued in connection with the Merger will be greater than the fair market value of shares of NMM common stock. Alternatively, it is possible that the value of the shares of ApolloMed common stock to be issued in connection with the Merger will be less than the fair market value of shares of NMM common stock.
Some ApolloMed and NMM executive officers and directors have interests in the Merger that are different from your interests and such differing interests of such officers and directors may influence them to support or approve the Merger without regard to your interests.
When considering the recommendation by the ApolloMed board of directors that the ApolloMed stockholders vote “for” each of the proposals being submitted to the ApolloMed stockholders at the ApolloMed special meeting and the recommendation by the NMM board of directors that the NMM shareholders vote “for” each of the proposals being submitted to the NMM shareholders at the NMM special meeting, the ApolloMed stockholders and NMM shareholders should be aware that certain of the directors and executive officers of ApolloMed and NMM have arrangements that provide them with interests in the Merger that are different from, or in addition to, those of the stockholders of ApolloMed and NMM. For instance, certain directors and officers of ApolloMed and NMM are expected to continue to serve as directors and officers of the combined company and certain ApolloMed directors and officers have employment agreements with ApolloMed which are expected to remain in place following the Merger. The directors and executive officers ApolloMed and NMM also have certain rights to indemnification and to directors' and officers' liability insurance that will be provided by the combined company following completion of the Merger. These interests may have influenced the directors and executive officers of ApolloMed and NMM to support or recommend the proposals presented to ApolloMed stockholders and NMM shareholders, respectively. See the sections entitled “THE MERGER — Interests of ApolloMed’s Directors and Executive Officers in the Merger” and “THE MERGER — Interests of NMM’s Directors and Executive Officers in the Merger” beginning on page 151 and 153, respectively, of this joint proxy statement/prospectus.
| 46 |
The Merger has not yet been consummated and the failure to consummate the Merger could have a material adverse effect on ApolloMed’s business.
Consummation of the Merger is subject to antitrust regulatory clearance and other closing conditions, as well as approval by NMM’s shareholders and ApolloMed’s stockholders, none of which has yet occurred. If for any reason the Merger is not consummated, ApolloMed would have significant financial obligations to NMM in connection with previous financing transactions in which ApolloMed has engaged. Additionally, as ApolloMed anticipates that NMM will be an important future source of working capital for ApolloMed after the consummation of the Merger, ApolloMed might lose such additional funding. Furthermore, there are several areas of operations in which NMM and ApolloMed work together, including APA ACO, Inc., a Delaware corporation (“APAACO”), which is owned 50% by NMM and 50% by ApolloMed, as well as management services agreements (“MSAs”) ApolloMed has with certain NMM affiliates. If for any reason the Merger is not consummated, ApolloMed cannot predict the effect this would have on areas where ApolloMed operates together with NMM and for which ApolloMed is dependent upon significant revenue.
The pendency of the Merger could have an adverse effect on the business, financial condition, and results of operations or business prospects of ApolloMed or NMM.
The pendency of the Merger could disrupt ApolloMed’s business in the following ways, among others:
| · | Employees of ApolloMed or NMM might experience uncertainty regarding their future roles in the combined company, which might adversely affect the ability of ApolloMed or NMM to retain, recruit and motivate key personnel; and |
| · | the attention of management of ApolloMed or NMM might be directed toward the completion of the Merger and other transaction-related considerations and might be diverted from the day-to-day business operations of ApolloMed or NMM, as applicable, and matters related to the Merger may require management of time and resources management that could otherwise have been devoted to other potentially beneficial opportunities. |
Should they occur, any of these matters could adversely affect the business of, or harm the financial condition, results of operations or business prospects of ApolloMed and/or NMM.
Covenants in the Merger Agreement place certain restrictions on each of ApolloMed’s and NMM’s conduct of business prior to the closing of the Merger, including entering into a business combination with another party.
The Merger Agreement restricts each of NMM and ApolloMed from taking certain specified actions with respect to the conduct of its business without the other party’s consent while the Merger is pending. These restrictions may prevent each of NMM and ApolloMed from pursuing otherwise attractive business opportunities or other capital structure alternatives and making other changes to business or executing certain of its business strategies prior to the completion of the Merger, which opportunities, alternatives or other changes could be favorable to ApolloMed’s stockholders. See the section entitled “THE MERGER AGREEMENT — Covenants and Agreements — No Solicitation” beginning on page 163 of this joint proxy statement/prospectus.
Certain provisions of the Merger Agreement may discourage third parties from submitting alternative takeover proposals, including proposals that may be superior to the arrangements contemplated by the Merger Agreement.
The terms of the Merger Agreement prohibit each of ApolloMed and NMM from soliciting alternative takeover proposals or cooperating with persons making unsolicited takeover proposals, except in limited circumstances when such party’s board of directors determines in good faith that an unsolicited alternative takeover proposal is or is reasonably likely to lead to a superior takeover proposal and is reasonably capable of being consummated and that failure to cooperate with the proponent of the proposal is reasonably likely to result in a breach of the board’s fiduciary duties. In addition, if ApolloMed or NMM terminate the Merger Agreement under certain circumstances, including terminating because of a decision of a board of directors to recommend a superior proposal, each party would be required to pay a termination fee of $1.5 million to the other. This termination fee may discourage third parties from submitting alternative takeover proposals to ApolloMed or NMM or their shareholders, and may cause the respective boards of directors to be less inclined to recommend an alternative proposal.
| 47 |
The financial information presented in this joint proxy statement/prospectus for ApolloMed and NMM may not be fully comparable due to the different fiscal year-ends of each company.
ApolloMed has a fiscal year-end of March 31 and NMM has a fiscal year-end of December 31. Therefore, the historical financial statements and other financial information pertaining to ApolloMed and NMM cannot be directly compared in any given period. Moreover, because of the different fiscal years of ApolloMed and NMM, any cyclical trends in financial condition or results of operations of the two companies may not be fully comparable.
The Merger may not be tax-free to NMM shareholders.
The Merger has been structured to qualify as a reorganization within the meaning of Section 368(a) of the Code, but there can be no assurance that the Internal Revenue Service (“IRS”) would not assert, or that a court would not sustain, a position contrary to any described herein. The parties did not seek a ruling from the IRS regarding the tax consequences of the Merger. Therefore, if the Merger does not qualify as a reorganization, then the exchange of ApolloMed stock and warrants for stock of NMM pursuant to the Merger may be taxable to the NMM shareholders. Therefore, each holder of NMM stock is urged to consult with such holder’s own tax advisor with respect to the tax consequences of the Merger.
The rights of NMM shareholders who become ApolloMed stockholders in the Merger will be governed by the ApolloMed Charter and the ApolloMed Bylaws, as amended.
Upon the consummation of the Merger, NMM’s outstanding shares of common stock will be converted into the right to receive shares of ApolloMed common stock. NMM shareholders who receive shares of ApolloMed common stock in the Merger will become ApolloMed stockholders. As a result, NMM shareholders who become shareholders in ApolloMed will be governed by the ApolloMed Charter and the ApolloMed Bylaws, each as amended to reflect the proposals being voted on at the ApolloMed special meeting, and the DGCL rather than being governed by the NMM Articles and the California Corporations Code. See the section entitled “COMPARISON OF RIGHTS OF APOLLOMED STOCKHOLDERS AND NMM SHAREHOLDERS” beginning on page 309 of this joint proxy statement/prospectus.
Risks Related to the Combined Company Following the Merger
If ApolloMed and NMM are not successful in integrating their businesses and organizations, the anticipated benefits of the Merger may not be realized.
Historically, ApolloMed and NMM have operated as independent companies and will do so until the completion of the Merger. Achieving the anticipated benefits of the Merger will depend, in part, on the integration of technology, operations and personnel of ApolloMed and NMM. ApolloMed and NMM cannot assure you that the integration will be successful or that the anticipated benefits of the Merger will be fully realized. The challenges involved in this integration include the following:
| · | persuading the employees that ApolloMed’s and NMM’s business cultures are compatible and retaining the combined company’s key personnel; |
| · | maintaining the dedication of management resources to integration activities without diverting attention from the day-to-day business of the combined company; |
| · | maintaining management’s ability to focus on anticipating, responding to or utilizing changing technologies in the healthcare industry; |
| · | demonstrating to customers that the Merger will not result in adverse changes to the ability of the combined company to address the needs of customers of the loss of attention or business focus; and |
| · | keeping and retaining key ApolloMed and NMM employees after the Merger. |
| 48 |
The concentration of capital stock ownership with insiders of ApolloMed after the Merger will likely limit the ability of ApolloMed stockholders to influence corporate matters.
Following the Merger, the executive officers, directors, five percent or greater stockholders and their respective affiliated entities of ApolloMed will in the aggregate beneficially own approximately [●]% of ApolloMed’s outstanding common stock. As a result, these stockholders, acting together, have control over matters that require approval by ApolloMed’s stockholders, including the election of directors and approval of significant corporate transactions. Corporate actions might be taken even if other stockholders oppose them. This concentration of ownership might also have the effect of delaying or preventing a corporate transaction that other stockholders may view as beneficial.
ApolloMed may issue additional equity securities in the future, which may result in dilution to existing investors.
To the extent ApolloMed raises additional capital by issuing equity securities, including in a debt financing where ApolloMed issues convertible notes or notes with warrants and any shares of ApolloMed’s common stock to be issued in a private placement, ApolloMed’s stockholders may experience substantial dilution. ApolloMed may, from time to time, sell additional equity securities in one or more transactions at prices and in a manner it determines. If ApolloMed sells additional equity securities, existing stockholders may be materially diluted. In addition, new investors could gain rights superior to existing stockholders, such as liquidation and other preferences. In addition, the number of shares available for future grant under ApolloMed’s equity compensation plans may be increased in the future. In addition, the exercise or conversion of outstanding options or warrants to purchase shares of capital stock may result in dilution to ApolloMed’s stockholders upon any such exercise or conversion.
The market price of the combined company’s common stock after the Merger may be subject to significant fluctuations and volatility, and the stockholders of the combined company may be unable to sell their shares at a profit and might incur losses.
The market price of the combined company’s common stock could be subject to significant fluctuation following the Merger. The results of operations of the combined company and the market price of the combined company common stock following the Merger may be affected by factors different from those currently affecting the independent results of operations of ApolloMed and the stock price of ApolloMed. Some of the factors that may cause the market price of the combined company’s common stock to fluctuate include:
| · | actual or anticipated quarterly increases or decreases in revenue, gross margin or earnings and changes in the combined company’s business, operations or prospects; |
| · | announcements relating to strategic relationships, mergers, acquisitions, partnerships, collaborations, joint ventures, capital commitments, or other events by the combined company or the combined company’s competitors; |
| · | conditions or trends in the healthcare industry; |
| · | changes in the economic performance or market valuations of other healthcare-related companies; |
| · | general market conditions or domestic or international macroeconomic and geopolitical factors unrelated to the combined company’s performance or financial condition; |
| · | sale of the combined company’s common stock by stockholders, including executives and directors; |
| · | volatility and limitations in trading volumes of the combined company’s common stock; |
| · | the combined company’s ability to obtain financings; |
| · | failures to meet external expectations or management guidance; |
| · | changes in the combined company’s capital structure, future issuances of securities, sales or distributions of large blocks of common stock by stockholders; |
| · | the combined company’s cash position; |
| · | announcements and events surrounding financing efforts, including debt and equity securities; |
| · | analyst research reports, recommendation and changes in recommendations, price targets, and withdrawals of coverage; |
| 49 |
| · | departures and additions of key personnel; |
| · | disputes and litigations related to intellectual properties, proprietary rights, and contractual obligations; |
| · | changes in applicable laws, rules, regulations, or accounting practices and other dynamics; and |
| · | other events or factors, many of which may be out of the combined company’s control. |
The unaudited pro forma combined financial statements are presented for illustrative purposes only, and future results of the combined company may differ materially from the unaudited pro forma financial statements presented in this joint proxy statement/prospectus.
The unaudited pro forma combined financial statements contained in this joint proxy statement/prospectus are presented for illustrative purposes only and for several reasons, may not be an indication of the combined company’s financial condition or results of operations following the completion of the Merger. The unaudited pro forma combined financial statements have been derived from the historical financial statements of ApolloMed and NMM and adjustments and assumptions have been made regarding the combined company after giving effect to the Merger. The information upon which these adjustments and assumptions have been made is preliminary, and these kinds of adjustments and assumptions are difficult to make with accuracy. Moreover, the pro forma financial statements do not reflect all costs that are expected to be incurred by the combined company in connection with the merger. For example, the impact of any incremental costs incurred in integrating ApolloMed and NMM are not reflected in the pro forma financial statements. As a result, the actual financial condition and results of operations of the combined company following the completion of the Merger may not be consistent with, or evident from, these pro forma financial statements. The assumptions used in preparing the pro forma financial information may prove to be inaccurate, and other factors may affect the combined company’s financial condition or results of operations following the Merger. Any decline or potential decline in the combined company’s financial condition or results of operations may cause significant variations in the market price of ApolloMed common stock.
Subsequent to the consummation of the Merger, ApolloMed may be required to take write-downs or write-offs, restructuring and impairment or other charges that could have a significant negative effect on its financial condition, results of operations and stock price, which could cause you to lose some or all of your investment.
Although ApolloMed and NMM have conducted due diligence on each other, there can be no assurances that their diligence revealed all material issues that may be present in the other company’s business, that all material issues through a customary amount of due diligence will be uncovered, or that factors outside of ApolloMed’s and NMM’s control will not later arise. As a result, ApolloMed may be forced to later write-down or write-off assets, restructure operations, or incur impairment or other charges that could result in losses. Even if due diligence successfully identifies certain risks, unexpected risks may arise and previously known risks may materialize in a manner not consistent with each company’s preliminary risk analysis. Even though these charges may be non-cash items and not have an immediate impact on liquidity, the fact that ApolloMed reports charges of this nature could contribute to negative market perceptions about ApolloMed’s or its securities. In addition, charges of this nature may make future financing difficult to obtain on favorable terms or at all.
In the recent past, ApolloMed has identified material weaknesses in ApolloMed’s internal controls. ApolloMed cannot provide assurances that these weaknesses will not recur or that additional material weaknesses will not occur in the future. If ApolloMed’s internal control over financial reporting or ApolloMed’s disclosure controls and procedures are not effective, ApolloMed may not be able to accurately report its financial results, file its periodic reports in a timely manner or prevent fraud, which could cause investors to lose confidence in ApolloMed’s reported financial information and could lead to a decline in ApolloMed’s stock price or result in regulatory or legal actions against ApolloMed.
ApolloMed’s management is responsible for establishing and maintaining adequate internal control over ApolloMed’s financial reporting, as defined in Rule 13a-15(f) under the Securities and Exchange Act of 1934, as amended (“the “Exchange Act”). In the recent past, ApolloMed has identified a number of material weaknesses in ApolloMed’s disclosure controls and procedures. These material weaknesses could have allowed the reporting of inaccurate or incomplete information regarding ApolloMed’s business in ApolloMed’s public filings and required ApolloMed to devote substantial resources to mitigating and resolving the weaknesses ApolloMed identified. Despite these efforts, ApolloMed cannot provide assurances that these weaknesses will not recur or that additional material weaknesses will not occur in the future.
Additionally, ApolloMed intends to continue to grow ApolloMed’s business, in part, through the acquisition of new entities and the consummation of the Merger. If and when ApolloMed acquires such existing entities, or consummates the Merger, ApolloMed’s due diligence may fail to discover defects or deficiencies in the design and operations of the internal controls over financial reporting of such entities, or defects or deficiencies in the internal controls over financial reporting may arise when ApolloMed tries to integrate the operations of these newly acquired companies with itself. ApolloMed can provide no assurances that it will not experience such issues in future acquisitions, the result of which could have a material adverse effect on ApolloMed’s financial statements.
| 50 |
NMM has identified material weaknesses in its internal controls, and NMM cannot provide assurances that these weaknesses will be effectively remediated or that additional material weaknesses will not occur in the future. If NMM’s internal control over financial reporting or its disclosure controls and procedures are not effective, the combined company may not be able to accurately report its financial results or prevent fraud, which may cause investors to lose confidence in the combined company’s reported financial information and could lead to a decline in the combined company’s stock price.
NMM has identified material weaknesses in its internal controls over financial reporting. These material weaknesses include (i) inability to appropriately address and account for technical accounting matters, (ii) lack of adequate supervision and review, (iii) insufficient formal documentation of agreements and contractual terms, (iv) inadequate controls over financial reporting and (v) a lack of formal documentation of internal control procedures, policies and processes supporting the internal control environment. These material weaknesses could allow the reporting of inaccurate or incomplete information regarding the combined company’s financial results and will require the combined company to devote substantial resources to mitigating and resolving the weaknesses NMM has identified. NMM has implemented the following remediation efforts: (i) engaged outside accounting consultants to assist with technical accounting matters and financial reporting; (ii) implemented policies and procedures to require supervision and review of significant transactions prior to posting into the accounting system; (iii) implemented policies and procedures to require agreements to be signed; and (iv) added formal documentation of internal control procedures, policies and processes.
ApolloMed may not be able to timely and effectively implement controls and procedures required by Section 404 of the Sarbanes-Oxley Act of 2002 that will be applicable to the combined company after the Merger.
NMM is not currently subject to Section 404 of the Sarbanes-Oxley Act of 2002. The standards required for a public company under Section 404 of the Sarbanes-Oxley Act of 2002 are significantly more stringent than those required of NMM. Management may not be able to effectively and timely implement controls and procedures that adequately respond to the increased regulatory compliance and reporting requirements that will be applicable to ApolloMed after the Merger. If management is not able to implement the additional requirements of Section 404 of the Sarbanes-Oxley Act of 2002 in a timely manner or with adequate compliance, it may not be able to assess whether its internal control over financial reporting is effective, which may subject ApolloMed to adverse regulatory consequences and could harm investor confidence and the market price of ApolloMed’s common stock.
While ApolloMed has historically been a non-accelerated filer, the combined company expects to become an accelerated filer following the consummation of the Merger. As a result, the combined company might incur additional expense to obtain and utilize resources for management to perform its evaluation of the effectiveness of the combined company’s internal controls over financial reporting, as well as the related audit fees to have its independent auditors attest to management’s evaluation of the effectiveness of its internal controls over financial reporting in accordance with Section 404(b) of the Sarbanes-Oxley Act.
Anti-takeover provisions under Delaware law could make an acquisition of the combined company, which may be beneficial to the stockholders of the combined company, more difficult and may prevent attempts by the stockholders to replace or remove management.
The combined company will be subject to the anti-takeover provisions of the DGCL, including Section 203. Under these provisions, if anyone becomes an “interested stockholder,” the combined company may not enter into a “business combination” with that person for three years without special approval, which could discourage a third party from making a takeover offer and could delay or prevent a change of control. For purposes of Section 203 of the DGCL, “interested stockholder” means, generally, someone owning 15% or more of the combined company’s outstanding voting stock or an affiliate of the combined company that owned 15% or more of the combined company’s outstanding voting stock during the past three years, subject to certain exceptions as described in Section 203 of the DGCL.
As such, Section 203 of the DGCL could prohibit or delay mergers or a change in control and may discourage attempts by other companies to acquire the combined company.
| 51 |
Additionally, certain provisions in ApolloMed’s Charter could make it more difficult for a third party to acquire control of ApolloMed, even if such change in control would be beneficial to ApolloMed stockholders. Upon consummation of the Merger, the ApolloMed Charter and Bylaws will be amended to provide for the ApolloMed board to be divided into three classes serving staggered terms. The directors in each class will be elected to serve three-year terms. The provisions for a classified board could prevent a party that acquires control of a majority of the outstanding voting stock from obtaining control of the board of directors until the second annual stockholders meeting following the date the acquirer obtains the controlling stock interest. The classified board provisions and NMM shareholder Lock-Up Agreements could discourage a potential acquirer from making a tender offer or otherwise attempting to obtain control of ApolloMed and could increase the likelihood that incumbent directors will retain their positions. In addition, ApolloMed Charter and Bylaws contain provisions, such as blank check preferred stock, special meetings of stockholders and stockholder action by written consent, which could make it more difficult for a third party to acquire the combined company. These provisions may have the effect of preventing or hindering any attempts by the stockholders of the combined company to replace its board of directors or management.
If securities analysts do not publish research or reports about the business of the combined company, or if they publish negative evaluations, the price of the combined company’s common stock could decline.
The trading market for the combined company’s common stock will rely in part on the availability of research and reports that third-party industry or financial analysts publish about the combined company. There are many large, publicly traded companies active in the healthcare industry, which may mean it will be less likely that the combined company receives widespread analyst coverage. Furthermore, if one or more of the analysts who do cover the combined company downgrade its stock, its stock price would likely decline. If one or more of these analysts cease coverage of the combined company, the combined company could lose visibility in the market, which in turn could cause its stock price to decline.
ApolloMed needs to raise additional capital, which might not be available.
ApolloMed requires significant additional capital for general working capital and liquidity needs. If ApolloMed’s cash flow and existing working capital are not sufficient to fund its general working capital and liquidity requirements, as well as any debt service requirements, ApolloMed will have to raise additional funds by selling equity, issuing debt, borrowings, refinancing some or all of its existing debt or selling assets or subsidiaries. None of these alternatives for raising additional funds may be available, or available on acceptable terms to ApolloMed, in amounts sufficient for ApolloMed to meet its requirements. ApolloMed’s failure to obtain any required new financing may, if needed, require ApolloMed to reduce or curtail certain existing operations or make ApolloMed unable to continue to operate its business.
Because the Merger will likely result in an ownership change under Section 382 of the Code for ApolloMed, ApolloMed’s pre-Merger net operating loss carryforwards and certain other tax attributes will be subject to limitation. The net operating loss carryforwards and certain other tax attributes of NMM and of the combined company may also be subject to limitations as a result of ownership changes.
If a corporation undergoes an “ownership change” within the meaning of Section 382 of the Code, the corporation’s net operating loss carryforwards and certain other tax attributes arising from before the ownership change are subject to limitations on use after the ownership change. In general, an ownership change occurs if there is a cumulative change in the corporation’s equity ownership by certain stockholders that exceeds 50 percentage points over a rolling three-year period. Similar rules may apply under state tax laws. The Merger will likely result in an ownership change for ApolloMed and, accordingly, ApolloMed’s net operating loss carryforwards and certain other tax attributes will be subject to use limitations after the Merger. The Merger may also result in an ownership change for NMM, in which case, NMM’s net operating loss carryforwards and certain other tax attributes would also be subject to limitations. Additional ownership changes in the future could result in additional limitations on the net operating loss carryforwards of ApolloMed, NMM and the combined company. Consequently, even if the combined company achieves profitability, it may not be able to utilize a material portion of the net operating loss carryforwards and other tax attributes of ApolloMed, NMM and the combined company, which could have a material adverse effect on the combined company’s cash flow and results of operations.
Risks Related to the Business of ApolloMed
ApolloMed has a history of losses, and may have to further reduce costs by curtailing future operations to continue as a business.
Historically, ApolloMed has had operating losses and cash flow has been inadequate to support ongoing operations. For the three months ended June 30, 2017, and for the year ended March 31, 2017, ApolloMed had a net loss of approximately $3.8 million and $8.7 million, respectively, and as of June 30, 2017, ApolloMed had an accumulated deficit of approximately $41.3 million. ApolloMed’s ability to fund its capital requirements out of available cash and cash generated from its operations depends on a number of factors, including ApolloMed’s ability to integrate recently acquired businesses and continue growing its existing operations. If ApolloMed cannot generate positive cash flow from operations, it will have to reduce costs and/or try to raise working capital from other sources. These measures could materially and adversely affect ApolloMed’s ability to operate its business as presently conducted and execute ApolloMed’s business model.
| 52 |
ApolloMed may not be able to continue as a going concern.
As shown in the accompanying consolidated financial statements, ApolloMed has incurred a net loss of approximately $3.8 million and $8.7 million for the three months ended June 30, 2017 and for the year ended March 31, 2017, respectively, and used approximately $8.1 million in cash from operating activities during the year ended March 31, 2017 and, as of June 30, 2017, has an accumulated deficit and a stockholders’ deficit of approximately $41.3 million and $3.3 million, respectively. These factors raise substantial doubt about ApolloMed’s ability to continue as a going concern. ApolloMed’s consolidated financial statements do not include any adjustments relating to the recoverability and classification of recorded assets, or the amounts and classification of liabilities that might be necessary in the event that ApolloMed cannot continue as a going concern.
ApolloMed may encounter difficulties in managing its growth.
ApolloMed may not be able to successfully grow and expand. Successful implementation of its business plan will require management of growth, including potentially rapid and substantial growth, which could result in an increase in the level of responsibility for management personnel and strain on ApolloMed’s human and capital resources. To manage growth effectively, ApolloMed will be required, among other things, to continue to implement and improve its operating and financial systems and controls to expand, train and manage its employee base. ApolloMed’s ability to manage its operations and growth effectively requires ApolloMed to continue to expend funds to enhance its operational, financial and management controls, reporting systems and procedures and to attract and retain sufficient numbers of talented personnel. If ApolloMed is unable to implement and scale improvements to all of its control systems in an efficient and timely manner or if ApolloMed encounters deficiencies in existing systems and controls, then it will not be able to make available the services required to successfully execute its business plan. Failure to attract and retain sufficient numbers of qualified personnel could further strain its human resources and impede its growth or result in ineffective growth. Moreover, the management, systems and controls currently in place or to be implemented may not be adequate for such growth, and the steps taken to hire personnel and to improve such systems and controls might not be sufficient. If ApolloMed is unable to manage its growth effectively, it will have a material adverse effect on its business, results of operations and financial condition.
The terms of debt agreements could restrict ApolloMed’s operations, particularly ApolloMed’s ability to respond to changes in its business or to take specified actions and an event of default under ApolloMed’s debt agreements could harm its business.
Agreements for any indebtedness would likely contain a number of restrictive covenants that impose significant operating and financial restrictions on ApolloMed, including restrictions on ApolloMed’s ability to take actions that may be in its best interests. Debt agreements often include covenants that, among other things, generally:
| · | do not allow the borrower to borrow additional amounts or additional amounts above a certain limit, or that are senior to the existing debt, without the approval of the creditor; |
| · | require the borrower to obtain the consent of the creditor for acquisitions in excess of an agreed upon amount and/or grant security interests in newly-acquired companies; |
| · | do not allow the borrower to dispose of assets; |
| · | do not allow the borrower to liquidate, wind up or dissolve any of its subsidiaries without the creditor’s approval; |
| · | do not allow the borrower to create any liens on any of its assets; |
| · | require the borrower not to impair any security interests that the creditor has in the borrower’s assets; and |
| · | require the borrower to meet, on an ongoing basis, certain financial covenants, which may include targets as to consolidated earnings before interest, taxes, depreciation and amortization (“EBITDA”), leverage ratio, fixed charge coverage ratio and consolidated tangible net worth. |
| 53 |
No assurances can be given that ApolloMed will be able to meet any of the financial covenants in favor of a creditor, and, if ApolloMed were to fail to meet any financial covenants, there would be an event of default and no assurance can be given that a creditor would waive such default, which in turn could result in a material adverse effect on ApolloMed’s financial condition and ability to continue its operations.
ApolloMed is required to prepare and file with the SEC a registration statement covering the sale of a former creditor’s registrable securities by March 31, 2018.
On March 28, 2014, ApolloMed entered into a Credit Agreement (the “Credit Agreement”) with NNA of Nevada, Inc. (“NNA”), an affiliate of Fresenius SE & Co. KGaA (“Fresenius”), which has been amended from time to time. Presently, ApolloMed is required to prepare and file with the SEC a registration statement covering the sale of NNA’s registrable securities issued pursuant to the Credit Agreement by March 31, 2018. If ApolloMed fails to do so by such date, for each month thereafter until it files the registration statement registering NNA’s registrable securities ApolloMed must pay NNA liquidated damages of 1.5% of the total purchase price of the registrable securities owned by NNA, payable in shares of ApolloMed common stock. This may result in the dilution of the ownership interests of ApolloMed’s stockholders.
The nature of ApolloMed’s business and rapid changes in the healthcare industry makes it difficult to reliably predict future growth and operating results.
Rapidly changing Federal and state healthcare laws, and the regulations thereunder, make it difficult to anticipate the nature and amount of medical reimbursements, third party private payments and participation in certain government programs. For example, ApolloMed was awarded a participation agreement under the Centers for Medicare & Medicaid Services (“CMS”) Medicare Shared Savings Program (“MSSP”) in July 2012, to operate as an Accountable Care Organization (“ACO”). The ACO has received an “all or nothing” payment under the MSSP program for services rendered in fiscal 2015, but did not receive such a payment for fiscal 2016 or fiscal 2017. This makes it difficult to forecast ApolloMed’s future earnings, cash flow and results of operations. The evolving nature of the current medical services industry increases these uncertainties.
ApolloMed may be unable to successfully integrate recently acquired and launched entities and may have difficulty predicting the future needs of those entities.
In fiscal 2015, ApolloMed acquired AKM Medical Group, Inc., a California corporation (“AKM”), Southern California Heart Centers, a California medical corporation (“SCHC”), Best Choice Hospice Care, LLC, a California limited liability company (“BCHC”), and Holistic Care Home Health Agency, Inc., a California corporation (“HCHHA”), and launched ApolloMed Care Clinic, a California professional corporation (“ACC”), and Apollo Palliative Services LLC, a California limited liability company (“ApolloMed Palliative” or “APS”). In fiscal 2016, ApolloMed formed Apollo Care Connect, Inc., a Delaware corporation (“Apollo Care Connect”), and combined the operations of AKM into those of MMG, and disposed of substantially all of the assets of ACC. In fiscal 2017, ApolloMed acquired Bay Area Hospitalist Associates (“BAHA”) and also formed APAACO to operate under CMS’ Next Generation Accountable Care Organization Model Program (the “NGACO Model”).
As a result of ApolloMed’s rapid expansion ApolloMed may be unable to successfully integrate the various entities it has acquired or formed. Additionally, these entities operate in different areas of the health care industry and ApolloMed cannot accurately predict how these acquired entities will perform in the future, integrate into its entire operations or result in a diversion of management focus and attention to other parts of ApolloMed’s business.
ApolloMed’s growth strategy may not prove viable and expected growth and value may not be realized.
ApolloMed’s business strategy is to grow rapidly by managing a network of medical groups providing certain hospital-based services and integrated inpatient and outpatient physician networks. ApolloMed also seeks growth opportunities both organically and through the acquisition of target medical groups and other service providers. Identifying quality acquisition candidates is a time-consuming and costly process. There can be no assurance that ApolloMed will be successful in identifying and establishing relationships with these and other candidates. If ApolloMed is not successful in identifying and acquiring other entities, its ability to successfully implement its business plan and achieve targeted financial results could be adversely affected. The process of integrating acquired entities involves significant risks, which include, but are not limited to:
| · | demands on ApolloMed’s management team related to the significant increase in the size of its business; |
| · | diversion of management’s attention from the management of daily operations; |
| 54 |
| · | difficulties in the assimilation of different corporate cultures and business practices; |
| · | difficulties in conforming the acquired entities’ accounting policies to ApolloMed’s; |
| · | retaining employees who may be vital to the integration of departments, information technology systems, including accounting; |
| · | systems, technologies, books and records, procedures and maintaining uniform standards, such as internal accounting controls; |
| · | procedures, and policies; and |
| · | costs and expenses associated with any undisclosed or potential liabilities. |
There can be no assurance that ApolloMed will be able to manage the integration of its acquisitions or the growth of such acquisitions effectively.
An element of ApolloMed’s growth strategy is also the expansion of its business by developing new palliative care programs in its existing markets and in new markets. This aspect of ApolloMed’s growth strategy may not be successful, which could adversely impact its overall growth and profitability. ApolloMed cannot assure that it will be able to:
| · | identify markets that meet ApolloMed’s selection criteria for new palliative care programs; |
| · | hire and retain a qualified management team to operate each of ApolloMed’s new palliative care programs; |
| · | manage a large and geographically diverse group of palliative care programs; |
| · | become Medicare and Medicaid certified in new markets; |
| · | generate a sufficient patient base in new markets to operate profitably in these new markets; or |
| · | compete effectively with existing programs. |
ApolloMed may not make appropriate acquisitions, may fail to integrate them into its business, or these acquisitions could alter ApolloMed’s current payor mix and reduce its revenue.
ApolloMed’s business is significantly dependent on locating and acquiring or partnering with medical practices or individual physicians to provide health care services. As part of ApolloMed’s growth strategy, it regularly reviews potential acquisition opportunities. ApolloMed cannot predict whether it will be successful in pursuing such acquisition opportunities or what the consequences of any such acquisitions would be. If ApolloMed is not successful in finding attractive acquisition candidates that it can acquire on satisfactory terms, or if it cannot successfully complete and efficiently integrate those acquisitions that it identifies, ApolloMed may not be able to implement its business model, which would likely negatively impact its revenues, results of operations and financial condition. Furthermore, ApolloMed’s acquisition strategy involves a number of risks and uncertainties, including:
| · | ApolloMed may not be able to identify suitable acquisition candidates or strategic opportunities or successfully implement or realize the expected benefits of any suitable opportunities. In addition, ApolloMed competes for acquisitions with other potential acquirers, some of which may have greater financial or operational resources than it does. This competition may intensify due to the ongoing consolidation in the healthcare industry, which may increase ApolloMed’s acquisition costs. |
| · | ApolloMed may be unable to successfully and efficiently integrate completed acquisitions, including its recently completed acquisitions and such acquisitions may fail to achieve the financial results it expected. Integrating completed acquisitions into ApolloMed’s existing operations involves numerous short-term and long-term risks, including diversion of its management’s attention, failure to retain key personnel, failure to retain payor contracts and failure of the acquired practice to be financially successful. |
| · | ApolloMed cannot be certain of the extent of any unknown or contingent liabilities of any acquired business, including liabilities for failure to comply with applicable laws. ApolloMed may incur material liabilities for past activities of acquired entities. Also, depending on the location of the acquisition, it may be required to comply with laws and regulations that may differ from those of the states in which ApolloMed’s operations are currently conducted. |
| 55 |
| · | ApolloMed may acquire individual or group medical practices that operate with lower profit margins as compared with its current or expected profit margins or which have a different payor mix than ApolloMed’s other practice groups, which would reduce its profit margins. Depending upon the nature of the local healthcare market, ApolloMed may not be able to implement its business model in every local market that it enters, which may negatively impact ApolloMed’s revenues and financial condition. |
| · | If ApolloMed finances acquisitions by issuing equity securities or securities convertible into equity securities, its existing stockholders could be diluted, which, in turn, could adversely affect the market price of ApolloMed’s stock. If ApolloMed finances an acquisition with debt, it could result in higher leverage and interest costs. As a result, if it fails to evaluate and execute acquisitions properly, ApolloMed might not achieve the anticipated benefits of these acquisitions, and it may increase its acquisition costs. |
Changes to the fair value of contingent compensation payments to be paid in connection with ApolloMed’s acquisitions may result in significant fluctuations to its results of operations.
In connection with some of ApolloMed’s recent acquisitions, ApolloMed is required to make certain contingent compensation payments. The fair value of such payments is re-evaluated periodically based on changes in ApolloMed’s estimate of future operating results and changes in market discount rates. Any changes in ApolloMed’s estimated fair value is recognized in its results of operations. Increases in the amount of contingent compensation payments ApolloMed is required to make may have an adverse effect on its financial condition.
ApolloMed’s management team’s attention may be diverted by recent acquisitions and searches for new acquisition targets, and its business and operations may suffer adverse consequences as a result.
Mergers and acquisitions are time-intensive, requiring significant commitment of ApolloMed’s management team’s focus and resources. If ApolloMed’s management team spends too much time focused on recent acquisitions or on potential acquisition targets, its management team may not have sufficient time to focus on its existing business and operations. This diversion of attention could have material and adverse consequences on ApolloMed’s operations and its ability to be profitable.
ApolloMed’s growth strategy incurs significant costs, which could adversely affect its financial condition.
ApolloMed’s growth-by-acquisition strategy involves significant costs, including financial advisory, legal and accounting fees, and may include additional costs, including costs of fairness opinions, labor costs, termination payments, contingent payments and bonuses, among others. These costs could put a strain on ApolloMed’s available cash and cash flow, which in turn could adversely affect its overall financial condition.
ApolloMed may be unable to scale its operations successfully.
ApolloMed’s growth strategy will place significant demands on its management and financial, administrative and other resources. Operating results will depend substantially on the ability of ApolloMed’s officers and key employees to manage changing business conditions and to implement and improve its financial, administrative and other resources. If ApolloMed is unable to respond to and manage changing business conditions, or the scale of its operations and the quality of its services, ApolloMed’s ability to retain key personnel and its business could be adversely affected.
ApolloMed could experience significant losses under its capitation-based contracts if the medical expenses it incurs exceed revenues.
In California, health plans typically prospectively pay an IPA a fixed per member per month (“PMPM”) amount, or capitation payment, which is often based on a percentage of the amount received by the health plan. Capitation payments to IPAs, in the aggregate, represent a prospective budget from which the IPA manages care-related expenses on behalf of the population enrolled with that IPA. If ApolloMed’s IPAs are able to manage care-related expenses under the capitated levels, ApolloMed realizes an operating profit on its capitation contracts. However, if ApolloMed’s care-related expenses exceed projected levels, its IPAs may realize substantial operating deficits, which are not capped and could lead to substantial losses.
| 56 |
ApolloMed’s future growth could be harmed if it loses the services of Dr. Hosseinion.
ApolloMed’s success depends to a significant extent on the continued contributions of its key management personnel, particularly ApolloMed’s Chief Executive Officer, Warren Hosseinion, M.D., for the management of ApolloMed’s business and implementation of its business strategy. ApolloMed has entered into an employment agreement with Dr. Hosseinion and it holds a $5 million key man life insurance policy. The loss of Dr. Hosseinion’s services could have a material adverse effect on ApolloMed’s business, financial condition and results of operations.
ApolloMed’s current principal stockholders have significant influence over ApolloMed and the stockholders could delay, deter or prevent a change of control or other business combination or otherwise cause ApolloMed to take action with which stockholders might not agree. This includes that ApolloMed’s founders, Warren Hosseinion, M.D. and Adrian Vazquez, M.D., combined currently own more than 35% of ApolloMed’s shares and have significant influence over ApolloMed’s operations and strategic direction.
ApolloMed’s executive officers and directors, together with holders of greater than 5% of its outstanding common stock, as a group, currently beneficially own approximately 70% of ApolloMed’s outstanding common stock. As a result, ApolloMed’s executive officers, directors and holders of greater than 5% of its outstanding common stock have the ability to control all matters submitted to ApolloMed’s stockholders for approval, including among other things:
| · | changes to the composition of ApolloMed’s ApolloMed board, which has the authority to direct its business and appoint and remove ApolloMed’s officers; |
| · | proposed mergers, consolidations or other business combinations; and |
| · | amendments to the ApolloMed Charter and Bylaws which govern the rights attached to ApolloMed’s shares of common stock. |
This concentration of ownership of shares of ApolloMed’s common stock could delay or prevent proxy contests, mergers, tender offers, open market purchase programs or other purchases of shares of ApolloMed’s common stock that might otherwise give its stockholders the opportunity to realize a premium over the then prevailing market price of ApolloMed’s common stock. The interests of ApolloMed’s executive officers, directors and holders of greater than 5% of its outstanding common stock may not always coincide with the interests of the other stockholders. This concentration of ownership may also adversely affect ApolloMed’s stock price.
This concentration of ownership is underscored by the fact that Dr. Hosseinion (who currently owns approximately 19% of ApolloMed’s common stock) and Dr. Vazquez (who currently owns approximately 16% of ApolloMed’s common stock) together currently own more than 35% of ApolloMed’s common stock and exert a significant degree of influence over ApolloMed’s management and affairs and over matters requiring stockholder approval, including the election of directors and approval of significant corporate transactions. As stockholders, Drs. Hosseinion and Vazquez are entitled to vote their shares in their own interests, which may not always be in the interests of ApolloMed’s stockholders generally. Their concentrated holdings of so much of ApolloMed’s common stock may harm the value of ApolloMed’s shares and discourage investors from investing in ApolloMed. Drs. Hosseinion and Vazquez could also seek to delay, defer or prevent a change of control, merger, consolidation or sale of all or substantially all of ApolloMed’s assets that other stockholders may support, or conversely this concentrated control could result in the consummation of a transaction that other stockholders may not support.
If ApolloMed’s agreements or arrangements with Dr. Hosseinion or physician groups are deemed invalid under state corporate practice of medicine and similar laws, or Federal law, or are terminated as a result of changes in state law, it could have a material impact on ApolloMed’s results of operations and financial condition.
There are various state laws, including laws in California, regulating the corporate practice of medicine which prohibits ApolloMed from owning various healthcare entities. This corporate practice of medicine prohibitions are intended to prevent unlicensed persons from interfering with or inappropriately influencing a physician’s professional judgment. These and other laws may also prevent fee-splitting, which is the sharing of professional service income with non-professional or business interests. The interpretation and enforcement of these laws vary significantly from state to state. As a result, ApolloMed has structured other agreements and arrangements with these entities, such as having Dr. Hosseinion hold shares in such practices as nominee shareholder for ApolloMed’s benefit. If these agreements and arrangements were held to be invalid under state laws prohibiting the corporate practice of medicine, a significant portion of ApolloMed’s revenues would be affected, which may result in a material adverse effect on ApolloMed’s results of operations and financial condition. Additionally, any changes to Federal or state law that prohibit such agreements or arrangements could also have a material adverse effect upon ApolloMed’s results of operations and financial condition.
| 57 |
If ApolloMed lost the services of Dr. Hosseinion for any reason, the contractual arrangements with ApolloMed’s variable interest entities (“VIEs”) could be in jeopardy.
Because of corporate practice of medicine laws, many of ApolloMed’s affiliated physician practice groups are either wholly-owned or primarily owned by Dr. Hosseinion as nominee shareholder for ApolloMed’s benefit. If Dr. Hosseinion died, was incapacitated or otherwise was no longer affiliated with ApolloMed, there could be a material adverse effect on the relationship between each of those VIEs and ApolloMed and, therefore, ApolloMed’s business as a whole could be adversely affected.
The contractual arrangements ApolloMed has with its VIEs is not as secure as direct ownership of such entities.
Because of corporate practice of medicine laws, ApolloMed enters into contractual arrangements to manage certain affiliated physician practice groups, which allows ApolloMed to consolidate those groups for financial reporting purposes. If ApolloMed had direct ownership of certain of ApolloMed’s affiliated entities, it would be able to exercise its rights as an equity holder directly to effect changes in the boards of directors of those entities, which could effect changes at the management and operational level. Under ApolloMed’s contractual arrangements, it may not be able to directly change the members of the boards of directors of these entities and would have to rely on the entities and the entities’ equity holders to perform its obligations in order to exercise ApolloMed’s control over the entities. If any of these affiliated entities or its equity holders fail to perform its respective obligations under the contractual arrangements, ApolloMed may have to incur substantial costs and expend additional resources to enforce such arrangements.
Any failure by ApolloMed’s key affiliated entities or its equity holders to perform its obligations under the contractual arrangements it has with ApolloMed would have a material adverse effect on ApolloMed’s business, results of operations and financial condition. ApolloMed also owns the majority, and not all, of the equity of certain subsidiaries.
Several of ApolloMed’s affiliated physician practice groups are owned by other physicians who could die, become incapacitated or otherwise become no longer affiliated with ApolloMed. Although the terms of the MSAs ApolloMed has with these affiliates provide that the MSA will be binding on the successors of such affiliates’ equity holders, as those successors are not parties to the MSAs, it is uncertain whether the successors in case of the death, bankruptcy or divorce of an equity holder would be subject to such MSAs.
In addition, although ApolloMed consolidates in ApolloMed’s financial reporting and business structure ApolloMed Accountable Care Organization, Inc., a California corporation (“ApolloMed ACO”), and ApolloMed Palliative, individuals other than Dr. Hosseinion, who acts as nominee stockholder for the benefit of Apollo Medical Management, Inc., a Delaware corporation and wholly-owned subsidiary of ApolloMed (“AMM”), also own approximately 20% of the equity of ApolloMed ACO and 44% of the equity in ApolloMed Palliative. Additionally, ApolloMed consolidates APAACO in ApolloMed’s financial reporting, although it owns 50% of the equity in that entity.
ApolloMed’s operations are dependent on a limited number of key payors.
ApolloMed had one payor during the three months ended June 30, 2017 that accounted for 72.1% of net revenues. Four payors accounted for 18.8%, 13.1%, 8.5% and 6.8% of ApolloMed’s net revenues for ApolloMed’s fiscal year ended March 31, 2017, respectively. ApolloMed had three payors during the fiscal year ended March 31, 2016 that accounted for 29.8%, 15.7% and 9.9% of net revenues, respectively. ApolloMed believes that a majority of its revenue will continue to be derived from a few payors. Each payor may immediately terminate any of ApolloMed’s contracts or any individual credentialed physician upon the occurrence of certain events. They may also amend the material terms of the contracts under certain circumstances. Failure to maintain the contracts on favorable terms or at all, for any reason, would materially and adversely affect ApolloMed’s results of operations and financial condition.
A decline in the number of patients ApolloMed serves could have a material adverse effect on ApolloMed’s results of operations.
Like any business, a material decline in the number of patients ApolloMed serves, whether it or a third party government or private entity is paying for its healthcare, could have a material adverse effect on ApolloMed’s results of operations and financial condition.
ACOs are relatively new and undergoing changes and CMS may change or discontinue the MSSP program.
ApolloMed has invested resources in both applying to participate in the MSSP and in establishing initial infrastructure. The MSSP program and the rules regarding ACOs have been altered and may be further altered in the future. Any material change to the MSSP program and ACO requirements, governance and operating rules, could provide a significant financial risk for ApolloMed and alter its strategic direction, thereby producing stockholder risk and uncertainty. In addition, ApolloMed could be terminated from the MSSP if it does not comply with the MSSP participation requirements.
| 58 |
ApolloMed ACO may not generate savings through its participation in the MSSP revenue, if any, earned by such participation will occur, only once annually on an “all or nothing” basis.
ApolloMed ACO participates in the MSSP sponsored by CMS. The MSSP is a relatively new program with limited history of payments to ACO participants. As a result of the uncertain nature of the MSSP program, ApolloMed considers revenue, if any, under the MSSP, as contingent upon the realization of program savings as determined by CMS, and revenues are not considered earned and therefore are not recognized until notice from CMS that cash payments are to be imminently received.
In addition, there is no assurance that ApolloMed will meet the conditions necessary for receipt of future payments. Furthermore, ApolloMed’s ability to continue to generate savings for the MSSP program depends on many factors, many of which are outside ApolloMed’s control, including, among others, how CMS elects to administer the MSSP program, how savings levels are calculated and continued political support of the MSSP program. As a result, whether future revenues will be earned by ApolloMed ACO is uncertain and will be contingent on various factors, including whether savings were determined to be achieved in 2015 or in any other period during which savings are measured.
During the fiscal year ended March 31, 2015, ApolloMed was awarded and received approximately a $5.4 million payment related to savings achieved from July 1, 2012, through December 31, 2013, which represented 16% of ApolloMed’s net revenue during the year ended March 31, 2015. During the fiscal years ended March 31, 2016 and 2017, ApolloMed did not receive any MSSP payment. ApolloMed is eligible to be considered for an all-or-nothing payment under this program for performance year 2016 (which, if it is paid, would be paid to ApolloMed in fiscal 2018). ApolloMed does not expect to receive any such payments for performance years beginning 2017 because of ApolloMed’s transition to, and business focus on, the NGACO Model, in which it has been participating since January 1, 2017.
Moreover, if amounts are payable to ApolloMed under the MSSP, it will be paid on an annual basis significantly after the time it is earned. Additionally, since MSSP payments, if any, are made once annually, ApolloMed would not receive such payments spread out over its fiscal year and, consequently, revenue may be materially lower in quarters when any MSSP-related payments are not received by ApolloMed.
The success of ApolloMed’s emphasis on the new NGACO Model is uncertain.
To position ApolloMed to participate in the NGACO Model, it has devoted, and intends to continue to devote, significant effort and resources, financial and otherwise, to the NGACO Model, and refocus away from certain other parts of ApolloMed’s historic business and revenue streams, which will receive less emphasis in the future and could result in reduced revenue from these activities. It is unknown at this time if this strategic decision will be successful in terms of ApolloMed’s emphasis on the NGACO Model and/or placing less emphasis on certain other parts of ApolloMed’s core business and revenue streams.
The results of the NGACO Model are unknown.
The NGACO Model is a new CMS program that builds upon previous ACO programs, including the MSSP program. Through the NGACO Model, CMS will provide an opportunity to APAACO and other NGACOs experienced in coordinating care for populations of patients, and whose provider groups are willing to assume higher levels of financial risk and reward, to participate in this new attribution-based risk sharing model. In January 2017, CMS approved APAACO to participate in the NGACO Model and CMS and APAACO have entered into a Next Generation ACO Model Participation Agreement (the “Participation Agreement”) with a term of two performance years through December 31, 2018. CMS may offer to renew the Participation Agreement for an additional two performance years. Additionally, the Participation Agreement may be terminated sooner by CMS as specified therein and CMS has the flexibility to alter or change the program over this time period. The number of Medicare ACOs continues to rise in total but there are still a growing number of program types and demonstrations that could be consolidated and impact APAACO.
APAACO’s future participation in the AIPBP Payment Mechanism is uncertain.
APAACO chose to participate in the All-Inclusive Population-Based Payment (“AIPBP”) payment mechanism, and became the only NGACO to have chosen this payment mechanism. Under the AIPBP payment mechanism, CMS estimates the total annual Part A and Part B Medicare expenditures of APAACO’s assigned Medicare beneficiaries and pays that projected amount in per beneficiary per month payments. In October 2017, CMS notified APAACO that it has not been renewed for participation in the AIPBP payment mechanism of the NGACO Model for performance year 2018 due to certain alleged deficiencies in performance by APAACO. APAACO does not believe the allegations by CMS of performance deficiencies are valid or justify the CMS non-renewal determination and is in discussions with CMS regarding possible reversal of such determination. If APAACO is not successful in convincing CMS to reverse its decision then the payment mechanism under the NGACO Model would default to traditional Fee For Service (“FFS”). This would result in the loss in monthly revenues of cash flow currently being generated by APAACO and would thus have a material adverse effect on ApolloMed’s future revenues and potential cash flow.
In addition, APAACO chose “Risk Arrangement A,” comprising 80% risk for Part A and Part B Medicare expenditures and a shared savings and losses cap of 5%, or as a result a 4% effective shared savings and losses cap when factoring in 80% risk impact. APAACO’s benchmark Medicare Part A and Part B expenditures for beneficiaries for its 2017 performance year are approximately $335 million, and under “Risk Arrangement A” of the AIPBP payment mechanism APAACO could therefore have profits or be liable for losses of up to 4% of such benchmarked expenditures, or approximately $13.4 million. While performance can be monitored throughout the year, end results will not be known until 2018. ApolloMed cannot accurately predict and monitor performance under the AIPBP payment mechanism for 2017 because, among other factors, end results are released annually rather than on a more frequent basis.
The NGACO Model program has certain political risks.
If the Patient Protection and Affordable Care Act (the “ACA”) is amended or repealed and replaced, or if CMMI is terminated, the NGACO Model program could be discontinued or significantly altered. In addition, CMS leadership could be changed and influenced by Congress or the current Administration. Additionally, CMS or Center for Medicare and Medicaid Innovation (“CMMI”) may elect to combine any existing programs, including bundled payments, which could greatly alter the NGACO Model program.
| 59 |
APAACO’s participation in the NGACO Model program subjects it to certain regulatory risks.
Among many requirements to be eligible to participate in the NGACO Model program, APAACO must have at least 10,000 assigned Medicare beneficiaries and must maintain that number throughout each performance year. Although APAACO started its 2017 performance year with more than 32,000 assigned Medicare beneficiaries, there can be no assurance that APAACO will maintain the required number of assigned Medicare beneficiaries, and, if that number were not maintained, APAACO would become ineligible for the program.
APAACO is subject to changing state laws and regulations.
NGACOs are required to comply with all applicable state laws and regulations regarding provider-based risk-bearing entities. If these laws or regulations change, for example, to require a Knox-Keene license in California, which ApolloMed does not have, APAACO could be required to cease its NGACO operations.
APAACO may experience losses due to the NGACO Model Program.
APAACO is responsible for savings and losses from claims. The NGACO Model uses a prospectively-set cost benchmark, which is established prior to the start of each performance year. The benchmark is based on various factors, including baseline expenditures with the baseline updated each year to reflect the NGACO’s participant list for the given year. The 2017 performance year NGACO Model baseline for APAACO is based on calendar year 2014 expenditures that are risk-adjusted and trended. A discount is then applied that incorporates regional and national efficiency. The final benchmark could potentially underestimate APAACO’s actual expenditures for its Medicare beneficiaries.
If claims cost rise from benchmark, or 2014 and/or 2017 are statistical anomalies, APAACO could experience losses due to the NGACO Model program, which could be significant prior to any adjustment in benchmarked expenditures.
Additionally, given that APAACO is providing care coordination but does not employ any physicians nor provide direct patient care, the degree of influence APAACO has could be limited and out of its direct control. Because of APAACO’s limited influence, it is possible APAACO may not be able to influence provider and preferred provider behavior, utilization and patient costs.
APAACO’s dependence on CMS creates uncertainty and subjects APAACO to potential liability.
APAACO relies on CMS for design, oversight and governance of the NGACO Model program. Accurate data, claims benchmarking and calculations, timely payments and periodic process reviews are key to program success. In addition to APAACO’s administrative and care coordination operating costs, APAACO may not generate savings through its participation in the NGACO Model. Any savings generated, if at all, will be earned in arrears and uncertain in both timing and amount.
APAACO chose to participate in the All-Inclusive Population-Based Payment (“AIPBP”) payment mechanism, which entails certain special risks.
APAACO chose to participate in the AIPBP payment mechanism, and is the only NGACO to have chosen this payment mechanism. Under the AIPBP payment mechanism, CMS will estimate the total annual Part A and Part B Medicare expenditures of APAACO’s assigned Medicare beneficiaries and pay that projected amount in per beneficiary per month payments. APAACO chose “Risk Arrangement A,” comprising 80% risk for Part A and Part B Medicare expenditures and a shared savings and losses cap of 5%, or as a result a 4% effective shared savings and losses cap when factoring in 80% risk impact. APAACO’s benchmark Medicare Part A and Part B expenditures for beneficiaries for its 2017 performance year are approximately $335 million, and under “Risk Arrangement A” of the AIPBP payment mechanism APAACO could therefore have profits or be liable for losses of up to 4% of such benchmarked expenditures, or approximately $13.4 million. While performance can be monitored throughout the year, end results will not be known until 2018. ApolloMed cannot accurately predict and monitor performance under the AIPBP payment mechanism because, among other factors, end results are released annually rather than on a more frequent basis.
| 60 |
CMS has indicated that its initial financial reports to participants in the NGACO Model may not be complete.
The NGACO Model is new and CMS is implementing extensive reporting protocols in connection therewith. CMS has indicated that it does not anticipate initial reports under the NGACO Model to be indicative of final results of actual risk-sharing and revenues to which ApolloMed is entitled, especially for the period April 1, 2017 through June 30, 2017, which is the second quarter of the NGACO program and the first quarter of ApolloMed’s 2018 fiscal year. This is because there are inherent biases in reporting the results at such an early juncture. Were that to be the case, ApolloMed might not report accurately ApolloMed’s revenues for this period, which could be subject to adjustment in a later period once ApolloMed receives final results from CMS.
APAACO requires significant capital reserves for program participation.
NGACOs must provide a financial guarantee to CMS. The financial guarantee must be in an amount of 2% of the NGACO’s benchmark Medicare Part A and Part B expenditures. APAACO’s benchmark Medicare Part A and Part B expenditures for beneficiaries for its 2017 performance year being approximately $335 million, APAACO submitted a letter of credit for $6.7 million for the 2017 program year. If APAACO reaches the maximum of its shared losses of $13.4 million, it may need to pay another $6.7 million to CMS or CMS may change or alter the risk reserve process or amount. Additionally, the incurred but not reported (“IBNR”) methodology utilized by CMS could have a negative impact on APAACO and affect working capital and capital requirements.
APAACO is responsible for savings and losses related to care received by its patients at Out-of-Network Providers, which could negatively impact ApolloMed’s ability to control claim costs.
Medicare beneficiaries in a NGACO Model program are permitted to receive care from a wide network of contracted providers and facilities, which could make it challenging for APAACO to control financial risks associated with those beneficiaries. CMS notified APAACO that its Medicare beneficiaries historically have received approximately 62% of its care at non-contracted, out-of-network ("OON") providers. While not responsible for paying claims for OON providers, APAACO may have difficulty managing patient care and costs as compared to in-network providers. Additionally, APAACO is responsible for savings and losses of this population using OON providers, which could adversely impact ApolloMed’s financial results.
In addition, if APAACO is successful under its Participation Agreement with CMS in encouraging more of its patients to receive care with contracted, in-network providers, there is the possibility that the monthly AIPBP payments will be insufficient to cover current expenditures, since the AIPBP payments will be based on historical in-network/out-of-network ratios. This could potentially result in negative cash-flow problems for APAACO, if increased payments need to be made to contracted, in-network providers, especially if CMS fails to monitor this in-network/OON ratio on a frequent periodic basis and reconciliation payments are materially delayed.
There is uncertainty regarding the initial design and administration of the NGACO Model program.
Due to the newness of the NGACO Model program and the fact that APAACO is the only company participating in the AIPBP track, APAACO is subject to initial program challenges including, but not limited to, process design, data and other related program aspects. APAACO has already experienced various apparent errors in the NGACO Model program and APAACO has been working with CMS, including senior CMS management, on these issues, but the resolution and impact on APAACO remains uncertain. Moreover, there is the potential for new or additional issues to be experienced with CMS which could negatively impact APAACO. Among other things, the AIPBP claims processing methodology is complex and could create reimbursement delays to contracted APAACO providers which could in turn terminate their agreements with APAACO. For example, services provided by contracted APAACO providers with Dates of Service (“DOS”) from January 1, 2017 to March 31, 2017 were to be paid by CMS. All services provided by in-network, providers with DOS from April 1, 2017 onward were to be paid by APAACO. But a flaw in the claims processing system of one of CMS’ contractors caused payments to contracted APAACO providers to be unpaid or to be paid at a reduced rate from January 1, 2017 to March 31, 2017. Various providers expressed dissatisfaction about this and several decided to terminate their agreements with APAACO. Consequently, there is the actual and potential risk of damaging goodwill with APAACO’s contracted providers, which could have a material adverse effect on the operations and financial condition of APAACO in particular and ApolloMed’s results of operations and financial condition on a consolidated basis.
APAACO has also experienced weaknesses in the NGACO Model program beneficiary alignment methodology. For example, some patients see more than one primary care provider (“PCP”) in a calendar year. CMS could attribute a patient to one PCP rather than another, which could create potential liability for APAACO. For example, when APAACO sent letters to its patients, as required by CMS, it received several calls from PCPs who did not join APAACO, but whose patients were attributed to another PCP. There could also be liability where a PCP has a capitated contract with APAACO, but the PCP’s patient also sees another PCP, whether that PCP was contracted with APAACO or not. APAACO’s expenditures could increase due to payments by CMS of the out-of-network, non-contracted PCP.
| 61 |
AIPBP operations and benchmarking calculations are complex.
AIPBP operations and benchmarking calculations are complex and can lead to errors in the application of the NGACO Model program, which could create reimbursement delays to ApolloMed’s providers and adversely affect APAACO’s performance and results of operations. For example, APAACO has discovered a feature in the AIPBP claims files that do not allow APAACO to break down certain claims amounts by individual patient codes. This feature has created confusion for APAACO contracted providers in reconciling its payments, causing some providers to terminate their agreements with APAACO. This feature could also create uncertainty regarding those agreements with providers that include capitation plus carve-outs for certain procedures. APAACO has sought to address its concerns about such features with CMS and CMS has informed APAACO that CMS’ contractor is unable to remedy this situation for at least the foreseeable future.
CMS relies on multiple third-party contractors to manage the NGACO Model program, which could hinder performance.
In addition to CMS reliance, CMS relies on various third parties to effect the NGACO program. This may be other departments of the U.S. government, such as CMMI. CMS relies on multiple third party contractors to manage the NGACO Model program, including claims and auditing. Due to such reliance, there is the potential for errors, delays and poor communication among the differing entities involved, which are beyond the control of APAACO. This could negatively impact APAACO’s results of operations specifically and ApolloMed’s results of operations on a consolidated basis.
Third parties used by APAACO could hinder performance.
APAACO uses select third parties. This could create operational and performance risk if, for example, the third party does not perform its responsibilities properly. Additionally, APAACO has contracted with participating Part A and Part B providers and was able to contract discounted Medicare, Diagnosis-Related Group and Resource Utilization Group rates with multiple providers. However, APAACO providers could decide to change or discontinue these contractual rates or to terminate its agreements with APAACO.
Risk-sharing arrangements that MMG has with health plans and hospitals could result in its costs exceeding the corresponding revenues, which could reduce or eliminate any shared risk profitability. MMG also has a key contract with Prospect Medical Group and its management service organization, which if terminated could materially affect ApolloMed’s business.
Under risk-sharing arrangements into which MMG has entered, MMG is responsible for a portion of the cost of hospital services or other services that are not capitated. These risk-sharing arrangements may require MMG to assume a portion of any loss sustained from such arrangements, thereby adversely affecting ApolloMed’s results of operations. The terms of the particular risk-sharing arrangement allocate responsibility to the respective parties when the cost of services exceeds the related revenue, which results in a deficit, or permit the parties to share in any surplus amounts when actual costs are less than the related revenue. The amount of non-capitated medical and hospital costs in any period could be affected by factors beyond the control of MMG, such as changes in treatment protocols, new technologies, longer lengths of stay by the patient, and inflation. To the extent that such non-capitated medical and hospital costs are higher than anticipated, revenue may not be sufficient to cover the risk-sharing deficits the health plans and MMG are responsible for, which could reduce ApolloMed’s revenue and adversely affect ApolloMed’s results of operations.
The Merger Agreement contemplates that Warren Hosseinion M.D., the sole shareholder of MMG, will sell to APC-LSMA all the issued and outstanding shares of capital stock of MMG for $100 under the Maverick Stock Purchase Agreement.
| 62 |
If MMG is not able to satisfy California Department of Managed Health Care’s (“DMHC”) requirements, MMG could become subject to sanctions and its ability to do business in California could be limited or terminated.
The DMHC has instituted financial solvency regulations. The regulations are intended to provide a formal mechanism for monitoring the financial solvency of a risk-bearing organization (“RBO”) in California, including capitated physician groups, such as MMG. Under DMHC regulations, ApolloMed’s affiliated physician groups are required to, among other things:
| · | Maintain, at all times, a minimum “cash-to-claims ratio” (where “cash-to-claims ratio” means the organization’s cash, marketable securities, and certain qualified receivables, divided by the organization’s total unpaid claims liability). The regulations currently require a cash-to-claims ratio of 0.75; and |
| · | Submit periodic reports to the DMHC containing various data and attestations regarding performance and financial solvency, including incurred but not reported calculations and documentation, and attestations as to whether or not the organization was in compliance with the Knox-Keene Health Care Service Plan Act of 1975, as amended (the “Knox-Keene Act”), requirements related to claims payment timeliness, had maintained positive tangible net equity (i.e. at least $1.00), and had maintained positive working capital (i.e. at least $1.00). |
In the event that a physician organization is not in compliance with any of the above criteria, the organization would be required to describe in a report submitted to the DMHC the reasons for non-compliance and actions to be taken to bring the organization into compliance. Additionally, under these regulations, the DMHC can make public some of the information contained in the reports, including, but not limited to, whether or not a particular physician organization met each of the criteria. In the event ApolloMed’s affiliated physician groups are not able to meet certain of the financial solvency requirements, and fail to meet subsequent corrective action plans, ApolloMed’s affiliated physician groups could be subject to sanctions, or limitations on, or removal of, its ability to do business in California.
MMG is currently attempting to confirm that it is in compliance with certain financial requirements of the DMHC.
ApolloMed’s IPA, MMG, was not in compliance with certain DMHC financial requirements, including tangible net equity (“TNE”). ApolloMed has increased its intercompany line of credit to MMG to provide additional capital in attempt to comply partially with the DMHC’s requirements. Through a plan of remediation that ApolloMed presented to the DMHC and which plan it approved, ApolloMed must contribute additional funds, cut costs, increase revenue or a combination of the above, which ApolloMed has done. As a result of the foregoing actions ApolloMed took, MMG had positive TNE as of the third quarter of fiscal 2017 and has maintained positive TNE to date. Since DMHC requirements are that an RBO should have positive TNE for one full quarter to be taken off a corrective action plan (“CAP”), ApolloMed believes that MMG is currently in compliance with DMHC requirements. The DMHC is currently reviewing filings ApolloMed has made to confirm this compliance. However, there can be no assurance that MMG will remain in compliance with DMHC requirements. To the extent that ApolloMed is required to contribute additional capital to MMG in the future, ApolloMed would have less available cash to use on other parts of its business.
ApolloMed may be subject to liability for failure to fully comply with federal and state securities laws.
ApolloMed has from time to time issued securities to investors to raise capital and as compensation to directors, employees and consultants to attract and retain talent. As a result, ApolloMed is subject to federal and state securities laws. Any failure to comply with such laws, such as ApolloMed’s failing to file information statements for two corporate actions taken by its majority stockholders in written consents in 2012 and 2013, could cause federal or state agencies to take action against ApolloMed, which could restrict its ability to issue securities and result in fines or penalties. Any claims brought by such an agency could also cause ApolloMed to expend resources to defend itself, would divert the attention of its management from ApolloMed’s core business and could significantly harm ApolloMed’s business, operating results and financial condition, even if the claims are resolved in ApolloMed’s favor.
In 2017, ApolloMed filed an application with the California Department of Business Oversight (“DBO”), seeking qualification of securities issued under its 2010 and 2015 Equity Incentive Plans (the “Plans”) under California securities laws. In connection with such application, DBO requested ApolloMed to demonstrate compliance with California securities laws for ApolloMed’s securities that have been previously issued. Other than the 2017 application, ApolloMed has not sought to qualify previously issued securities in California. ApolloMed believes that past sales and issuances of ApolloMed’s securities were conducted in reliance on exemptions from qualification under California law, but certain sales and issuances may not have qualified for a valid exemption. It is uncertain whether such inquiry will lead to any action by DBO, but such action could result in, among other things, financial sanctions against ApolloMed. Further, ApolloMed could be required to conduct a rescission offer of certain prior sales and issuances. If a security holder accepts such an offer, ApolloMed would have to pay such holder the purchase price plus interest and costs, which could adversely affect its financial condition. In addition, ApolloMed agreed with DBO not to grant any options in California until it issues an order qualifying the securities issued under the Plans. As a result, the forms of equity compensation that ApolloMed may pay our management, staff and advisors are significantly limited, which could adversely affect its ability to attract and retain talent because management members and advisors may view options as more attractive than other forms of compensation and may demand increased cash compensation while the DBO inquiry continues.
Further, at ApolloMed’s 2016 annual meeting, its stockholders voted on the frequency of their future votes on its executive compensation. ApolloMed inadvertently failed to file, within 150 days after the meeting, a Form 8-K amendment to disclose its decision as to how frequently it will hold such a vote. ApolloMed does not expect this failure to affect this joint proxy statement/prospectus but such failure may adversely affect the effectiveness of ApolloMed’s registration statement on Form S-8 filed in May 2016 and ApolloMed may need to refile such registration statement. This failure also hinders ApolloMed’s ability to issue securities in certain transactions and raise additional capital, including causing us to be unable to use Form S-3 at least 12 calendar months from the missed filing deadline.
Economic conditions or changing consumer preferences could adversely impact ApolloMed’s business.
A downturn in economic conditions in one or more of ApolloMed’s markets could have a material adverse effect on ApolloMed’s results of operations, financial condition, business and prospects. Historically, state budget limitations have resulted in reduced state spending. Given that Medicaid is a significant component of state budgets, an economic downturn would put continued cost containment pressures on Medicaid outlays for ApolloMed’s services in California. In addition, an economic downturn and/or sustained unemployment, may also impact the number of enrollees in managed care programs as well as the profitability of managed care companies, which could result in reduced reimbursement rates.
The existing Federal deficit, as well as deficit spending by the government as the result of adverse developments in the economy or other reasons, can lead to continuing pressure to reduce government expenditures for other purposes, including government-funded programs in which ApolloMed participates, such as Medicare and Medicaid. Such actions in turn may adversely affect ApolloMed’s results of operations.
Although ApolloMed attempts to stay informed of government and customer trends, any sustained failure to identify and respond to trends could have a material adverse effect on ApolloMed’s results of operations, financial condition, business and prospects.
ApolloMed’s success depends, to a significant degree, upon ApolloMed’s ability to adapt to a changing market and continued development of additional services.
Although ApolloMed expects to provide a broad and competitive range of services, there can be no assurance of acceptance by the marketplace. ApolloMed’s ability to procure new contracts may be dependent upon the continuing results achieved at the current facilities, upon pricing and operational considerations, and the potential need for continuing improvement to existing services. Moreover, the markets for such services may not develop as expected nor can there be any assurance that ApolloMed will be successful in its marketing of any such services.
| 63 |
Competition for physicians is intense, and ApolloMed may not be able to hire and retain qualified physicians to provide services.
ApolloMed is dependent on its affiliated physicians to provide services and generate revenue. ApolloMed competes with many types of healthcare providers, including teaching, research and government institutions, hospitals and other practice groups, for the services of clinicians. The limited number of residents entering the job market each year and the limited number of other licensed providers seeking to change employers makes it challenging to meet ApolloMed’s hiring needs and may require ApolloMed to contract locum tenens physicians or to increase physician compensation in a manner that decreases its profit margins. The limited number of residents and other licensed providers also impacts ApolloMed’s ability to recruit new physicians with the expertise necessary to provide services within ApolloMed’s business and its ability to renew contracts with existing physicians on acceptable terms. If ApolloMed does not do so, its ability to provide services could be adversely affected. Even though ApolloMed’s physician turnover rate has remained stable over at least the last three years, if the turnover rate were to increase significantly, ApolloMed’s growth could be adversely affected.
Moreover, unlike some of ApolloMed’s competitors who sometimes pay additional compensation to physicians who agree to provide services exclusively to that competitor, ApolloMed’s IPAs have historically not entered into such exclusivity agreements and have allowed its affiliated physicians to affiliate with multiple IPAs. This practice may place ApolloMed at a competitive disadvantage regarding the hiring and retention of physicians relative to those competitors who do enter into such exclusivity agreements.
The healthcare industry continues to experience shortages in qualified service employees and management personnel and ApolloMed may be unable to hire qualified employees.
ApolloMed competes with other healthcare providers for its employees, both clinical associates and management personnel. As the demand for health services continues to exceed the supply of available and qualified staff, ApolloMed and its competitors have been forced to offer more attractive wage and benefit packages to these professionals. Furthermore, the competition for this segment of the labor market has created turnover as many seek to take advantage of the supply of available positions, many of which offer new and more attractive wage and benefit packages. In addition to the wage pressures described above, the cost of training new employees amid the turnover rates may cause added pressure on ApolloMed’s operating margins. Lastly, the market for qualified nurses and therapists is highly competitive, which may adversely affect ApolloMed’s palliative, home health and hospice operations, which are particularly dependent on nurses for patient care.
The healthcare industry is highly competitive.
There are many other companies and individuals currently providing health care services, many of which have been in business longer than ApolloMed has been, and/or have substantially more financial and personnel resources than ApolloMed has. ApolloMed competes directly with national, regional and local providers of inpatient healthcare for patients and physicians. Other companies could enter the market in the future and divert some or all of ApolloMed’s business. On a national basis, ApolloMed’s competitors include, but are not limited to, Team Health, EmCare, DaVita and Heritage, each of which has greater financial and other resources available to them. ApolloMed also competes with physician groups and privately-owned health care companies in each of ApolloMed’s local markets. Existing or future competitors also may seek to compete with ApolloMed for acquisitions, which could have the effect of increasing the price and reducing the number of suitable acquisitions, which would have an adverse impact on ApolloMed’s growth strategy. Since there are virtually no capital expenditures required to enter the industry, there are few financial barriers to entry. Individual physicians, physician groups and companies in other healthcare industry segments, including hospitals with which ApolloMed has contracts, and some of which have greater financial, marketing and staffing resources, may become competitors in providing health care services, and this competition may have a material adverse effect on ApolloMed’s business operations and financial position. In addition, certain governmental payors contract for services with independent providers such that ApolloMed’s relationships with these payors are not exclusive, particularly in California, where all of ApolloMed’s operations, providers and patients are located.
Additionally, as ApolloMed has expanded into palliative, home health and hospice care through ApolloMed Palliative, ApolloMed faces competitors that have traditionally concentrated in this segment and that may have greater resources and specialized expertise than ApolloMed has. In many areas in which ApolloMed’s palliative, home health and hospice care programs are located, it competes with a large number of organizations, including:
| 64 |
| · | community-based home health and hospice providers; |
| · | national and regional companies; |
| · | hospital-based home health agencies, hospice and palliative care programs; and |
| · | nursing homes. |
ApolloMed may be unable to compete successfully with these competitors in palliative, home health and hospice care, and may expend significant resources without success.
ApolloMed relies on referrals from third parties for its services.
ApolloMed’s business relies in part on referrals from third parties for its services. ApolloMed receives referrals from community medical providers, emergency departments, payors, and hospitals in the same manner as other medical professionals receive patient referrals. ApolloMed does not provide compensation or other remuneration to its referral sources for referring patients to them. A decrease in these referrals due to competition, concerns about the quality of ApolloMed’s services and other factors could result in a significant decrease in ApolloMed’s revenues and adversely impact its financial condition. Similarly, ApolloMed cannot assure that it will be able to obtain or maintain preferred provider status with significant third-party payors in the communities where it operates. If ApolloMed is unable to maintain its referral base or ApolloMed’s preferred provider status with significant third-party payors, it may negatively impact its revenues and financial performance.
Hospitals and other inpatient and post-acute care facilities may terminate their agreements with ApolloMed or reduce the fees it pays them.
During the fiscal year ended March 31, 2017, ApolloMed derived approximately 49% of its net revenue for physician services from contracts directly with hospitals and other inpatient and post-acute care facilities. ApolloMed’s current partner facilities may decide not to renew ApolloMed’s contracts, introduce unfavorable terms, or reduce fees paid to ApolloMed. Any of these events may impact the ability of ApolloMed’s physician practice groups to operate at such facilities, which would negatively impact ApolloMed’s revenue, results of operations and financial condition.
Some of the hospitals where ApolloMed’s affiliated physicians provide services may have its medical staff closed to non-contracted physicians.
In general, ApolloMed’s affiliated physicians may only provide services in a hospital where it has certain credentials, called privileges, which are granted by the medical staff and controlled by the legally binding medical staff bylaws of the hospital. The medical staff decides who will receive privileges and the medical staff of the hospitals where ApolloMed currently provides services or wish to provide services could decide that non-contracted physicians can no longer receive privileges to practice there. Such a decision would limit ApolloMed’s ability to furnish services in a hospital, decrease the number of ApolloMed’s affiliated physicians who could provide services or preclude ApolloMed from entering new hospitals. In addition, hospitals may attempt to enter into exclusive contracts for physician services, which would reduce access to certain populations of patients within the hospital.
ApolloMed may have difficulty collecting payments from third-party payors in a timely manner.
ApolloMed derives significant revenue from third-party payors, and delays in payment or audits leading to refunds to payors may adversely impact ApolloMed’s net revenue. ApolloMed assumes the financial risks relating to uncollectible and delayed payments. In particular, ApolloMed relies on some key governmental payors. Governmental payors typically pay on a more extended payment cycle, which could result in ApolloMed incurring expenses prior to receiving corresponding revenue. In the current healthcare environment, payors are continuing its efforts to control expenditures for healthcare, including proposals to revise coverage and reimbursement policies. ApolloMed may experience difficulties in collecting revenue because third-party payors may seek to reduce or delay payment to which ApolloMed believes it is entitled. If ApolloMed is not paid fully and in a timely manner for such services or there is a finding that it was incorrectly paid, ApolloMed’s revenues, cash flows and financial condition could be adversely affected.
Decreases in payor rates could adversely affect ApolloMed.
Decreases in payor rates, either prospectively or retroactively, could have a significant adverse effect on ApolloMed’s revenue, cash flow and results of operations. For example, during fiscal 2016, Health Net, Inc. reduced payor rates to its payees, including ApolloMed, retroactive to July 1, 2015 and LA Care reduced payor rates to its payees, including ApolloMed, retroactive to January 1, 2016.
| 65 |
ApolloMed’s business model depends on numerous complex management information systems, and any failure to successfully maintain these systems or implement new systems could undermine ApolloMed’s ability to receive ACO payments and otherwise materially harm ApolloMed’s operations and result in potential violations of healthcare laws and regulations.
ApolloMed depends on a complex, specialized, integrated management information system and standardized procedures for operational and financial information, as well as for ApolloMed’s billing operations. ApolloMed may be unable to enhance its existing management information systems or implement new management information systems where necessary. Additionally, ApolloMed may experience unanticipated delays, complications or expenses in implementing, integrating and operating its systems. ApolloMed’s management information systems may require modifications, improvements or replacements that may require both substantial expenditures as well as interruptions in operations. ApolloMed’s ability to implement these systems is subject to the availability of information technology and skilled personnel to assist ApolloMed in creating and implementing these systems. ApolloMed’s failure to successfully implement and maintain all of its systems could undermine its ability to receive MSSP payments and otherwise have a material adverse effect on ApolloMed’s business, results of operations and financial condition. Additionally, ApolloMed’s failure to successfully operate its billing systems could lead to potential violations of healthcare laws and regulations.
The requirements of remaining a public company and the new requirements under the NASDAQ listing rules that ApolloMed will become subject to following its uplisting to NASDAQ may strain ApolloMed’s resources and distract ApolloMed’s management, which could make it difficult to manage its business.
As a public company, ApolloMed is required to comply with various regulatory and reporting requirements, including those required by the SEC. If ApolloMed uplists to NASDAQ, ApolloMed will become subject to NASDAQ listing rules. Complying with these requirements are time-consuming and expensive, creating pressure on ApolloMed’s financial resources and, accordingly, ApolloMed’s results of operations and financial condition.
From time to time ApolloMed may be required to write-off intangible assets, such as goodwill, due to impairment.
ApolloMed’s intangible assets are subject to annual impairment testing. Under current accounting standards, goodwill is tested for impairment on an annual basis and ApolloMed may be subject to impairment losses as circumstances change after an acquisition. If ApolloMed records an impairment loss related to ApolloMed’s goodwill, it could have a material adverse effect on its results of operations for the year in which the impairment is recorded.
ApolloMed currently derives 100% of its revenues in California and is vulnerable to changes in California healthcare laws and regulations.
ApolloMed’s business and operations is located in one state, California. Any material changes by California with respect to strategy, taxation and economics of healthcare delivery, reimbursements, financial requirements or other aspects of regulation of the healthcare industry could have an adverse effect on ApolloMed’s business, results of operations and financial condition.
A prolonged disruption of the capital and/or credit markets may adversely affect ApolloMed’s future access to capital, ApolloMed’s cost of capital and its ability to continue operations.
ApolloMed has relied substantially on the capital and credit markets for liquidity and to execute ApolloMed’s business strategies, which includes a combination of internal growth and acquisitions. Volatility and disruption of the U.S. capital and credit markets may adversely affect ApolloMed’s access to capital and/or increase its cost of capital. Should current economic and market conditions deteriorate, ApolloMed’s ability to finance its ongoing operations and its expansion may be adversely affected, it may be unable to raise necessary funds, its cost of debt or equity capital may increase significantly and future access to capital markets may be adversely affected.
| 66 |
Uncertain or adverse economic conditions may have a negative impact on ApolloMed’s industry, business, results of operations or financial position.
Uncertain or adverse economic conditions could have a negative effect on the fundamentals of ApolloMed’s business, results of operations and/or financial position. These conditions could have a negative impact on ApolloMed’s industry. There can be no assurance that ApolloMed will not experience any material adverse effect on its business as a result of future economic conditions or that the actions of the U.S. Government, Federal Reserve or other governmental and regulatory bodies, for the purpose of stimulating the economy or financial markets will achieve its intended effect. Additionally, some of these actions may adversely affect financial institutions, capital providers, ApolloMed’s customers or ApolloMed’s financial condition, results of operations or the price of ApolloMed’s securities. Potential consequences of the foregoing include:
| · | ApolloMed’s ability to issue equity and/or borrow capital on terms and conditions that ApolloMed finds acceptable, or at all, may be limited, which could limit ApolloMed’s ability to access capital; |
| · | potential increased costs of borrowing capital if interest rates rise; |
| · | adverse terms imposed on ApolloMed by any equity investor; |
| · | the possible impairment of some or all of the value of ApolloMed’s goodwill and other intangible assets; and |
| · | the possibility that any then-existing lenders could refuse to fund any commitment to ApolloMed or could fail, and ApolloMed may not be able to replace or refinance the financing commitment of any such lender on satisfactory terms, or at all. |
Actual or perceived difficulties in the global capital and credit markets have adversely affected, and uncertain or adverse economic conditions may negatively affect, ApolloMed’s business. Ongoing uncertain economic conditions may affect ApolloMed’s financial performance or ApolloMed’s ability to forecast its business with accuracy.
ApolloMed’s operations and performance depend primarily on California and U.S. economic conditions and its impact on purchases of, or capitated rates for, ApolloMed’s delivery of healthcare services. As a result of the global financial crisis that began in 2008, which was experienced on a broad and extensive scope and scale, and the last recession in the United States, general economic conditions deteriorated significantly, and, although the markets have improved significantly, the overall economic recovery since that time has been uneven. Declines in consumer and business confidence and private as well as government spending during and since the last recession, together with significant reductions in the availability and increases in the cost of credit and volatility in the capital and credit markets, as well as government budgeting, have adversely affected the business and economic environment in which ApolloMed operates and can affect the profitability of ApolloMed’s business. ApolloMed’s business is significantly exposed to risks associated with government spending and private payor reimbursement rates. Economic conditions may remain uncertain for the foreseeable future. ApolloMed believes that this general economic uncertainty may continue in future periods, as ApolloMed’s patients, private payors and government payors alter their purchasing activities in response to the new economic reality, and, among other things, ApolloMed’s patients may change or scale back healthcare spending, and private and government payors could reduce reimbursement rates. Additional consequences of such adverse effects could include the delay or cancellation of consumer spending for discretionary and non-reimbursed healthcare. Future disruption of the credit markets, increases in interest rates and/or sluggish economic growth in future periods could adversely affect ApolloMed’s patients’ spending habits, private payors’ access to capital (which supports the continuation and expansion of its businesses) and governmental budgetary processes, and, in turn, could result in reduced revenue to ApolloMed. The continuation or recurrence of any of these conditions may adversely affect ApolloMed’s cash flow, results of operations and financial condition. This uncertainty may also affect ApolloMed’s ability to prepare accurate financial forecasts or meet specific forecasted results. If ApolloMed is unable to adequately respond to or forecast further changes in demand for healthcare services, ApolloMed’s results of operations, financial condition and business prospects may be materially and adversely affected.
| 67 |
Many of ApolloMed’s agreements with hospitals and medical groups are relatively short term or may be terminated without cause by providing advance notice, and any such termination could have a material adverse effect on ApolloMed’s financial results, operations and future business plans.
Many of ApolloMed’s hospitalist and other operating agreements are relatively short term or may be terminated without cause by providing advance notice. If these agreements are terminated before the end of its terms, at the end of its term or are not renewed, ApolloMed would lose the revenue generated by those agreements. Any such terminations could have a material adverse effect on ApolloMed’s results of operations, financial condition and future business plans.
Many of ApolloMed’s agreements with hospitals and medical groups include prohibitions against ApolloMed’s hiring physicians or patients or competing with the hospital or medical group, which limits ApolloMed’s ability to implement its business plan in certain areas.
Because many of ApolloMed’s hospitalist and other operating agreements include prohibitions on ApolloMed’s hiring physicians or patients or competing with the hospital or medical group, ApolloMed’s ability to hire physicians, attract patients or conduct business in certain areas may be limited in some cases.
If there is a change in accounting principles or the interpretation thereof by the Financial Accounting Standards Board (“FASB”) affecting consolidation of VIEs, it could impact ApolloMed’s consolidation of total revenues derived from such affiliated physician groups.
ApolloMed’s financial statements are consolidated and include the accounts of ApolloMed’s majority-owned subsidiaries and various non-owned affiliated physician groups that are VIEs, which consolidation is effectuated in accordance with applicable accounting rules. In the event of a change in accounting principles promulgated by FASB or in FASB’s interpretation of its principles, or if there were an adverse determination by a regulatory agency or a court or a change in state or federal law relating to the ability to maintain present agreements or arrangements with such physician groups, ApolloMed may not be permitted to continue to consolidate the total revenues of such organizations.
Accounting rules require that under some circumstances the VIE consolidation model be applied when a reporting enterprise holds a variable interest (e.g., equity interests, debt obligations, certain management and service contracts) in a legal entity. Under this model, an enterprise must assess the entity in which it holds a variable interest to determine whether it meets the criteria to be consolidated as a VIE. If the entity is a VIE, the consolidation framework next identifies the party, if one exists, that possesses a controlling financial interest in a VIE, and requires that party to consolidate as the primary beneficiary. An enterprise’s determination of whether it has a controlling financial interest in a VIE requires that a qualitative determination be made, and is not solely based on voting rights.
If an enterprise determines the entity in which it holds a variable interest is not subject to the VIE guidance in Accounting Standards Codification (“ASC”) 810, the enterprise should apply the traditional voting control model (also outlined in ASC 810) which focuses on voting rights. In ApolloMed’s case, the VIE consolidation model applies to ApolloMed’s controlled, but not owned, physician affiliated entities. ApolloMed’s determination regarding the consolidation of its affiliates could be challenged, which could have a material adverse effect on ApolloMed’s operations.
The healthcare industry is complex and intensely regulated at the federal, state, and local levels and government authorities may determine that ApolloMed has failed to comply with applicable laws or regulations.
As a company involved in providing healthcare services, ApolloMed is subject to numerous federal, state and local laws and regulations. There are significant costs involved in complying with these laws and regulations. Moreover, if ApolloMed is found to have violated any applicable laws or regulations, ApolloMed could be subject to civil and/or criminal damages, fines, sanctions or penalties, including exclusion from participation in governmental healthcare programs, such as Medicare and Medicaid. ApolloMed may also be required to change its method of operations. These consequences could be the result of current conduct or even conduct that occurred a number of years ago. ApolloMed also could incur significant costs merely if it becomes the subject of an investigation or legal proceeding alleging a violation of these laws and regulations. ApolloMed cannot predict whether a federal, state or local government will determine that ApolloMed is not operating in accordance with law, or whether, when or how the laws will change in the future and impact its business. Any of these actions could have a material adverse effect on ApolloMed’s business, financial condition and results of operations.
| 68 |
The following is a non-exhaustive list of some of the more significant healthcare laws and regulations that affect ApolloMed:
| · | federal laws, including the federal False Claims Act, that provide for penalties against entities and individuals which knowingly or recklessly make claims to Medicare, Medicaid, and other governmental healthcare programs, as well as third-party payors, that contain or are based upon false or fraudulent information; |
| · | a provision of the Social Security Act, commonly referred to as the “Anti-Kickback Statute,” that prohibits the knowing and willful offering, payment, solicitation or receipt of any bribe, kickback, rebate or other remuneration, in cash or in kind, in return for the referral or recommendation of patients for items and services covered, in or in part, by federal healthcare programs such as Medicare and Medicaid; |
| · | a provision of the Social Security Act, commonly referred to as the Stark Law or physician self-referral law, that (subject to limited exceptions) prohibits physicians from referring Medicare patients to an entity for the provision of specific “designated health services” if the physician or a member of such physician’s immediate family has a direct or indirect financial relationship with the entity, and prohibits the entity from billing for services arising out of such prohibited referrals; |
| · | a provision of the Social Security Act that provides for criminal penalties on healthcare providers who fail to disclose known overpayments; |
| · | a provision of the Social Security Act that provides for civil monetary penalties on healthcare providers who fail to repay known overpayments within 60 days of identification or the date any corresponding cost report was due, if applicable, and also allows improper retention of known overpayments to serve as a basis for False Claims Act violations; |
| · | state law provisions pertaining to anti-kickback, self-referral and false claims issues, which typically are not limited to relationships involving governmental payors; |
| · | provisions of, and regulations relating to, the Health Insurance Portability and Accountability Act (“HIPAA”) that provide penalties for knowingly and willfully executing a scheme or artifice to defraud a health-care benefit program or falsifying, concealing or covering up a material fact or making any material false, fictitious or fraudulent statement in connection with the delivery of or payment for healthcare benefits, items or services; |
| · | provisions of HIPAA and the Health Information Technology for Economic and Clinical Health Act (“HITECH”) limiting how covered entities, business associates and business associate sub-contractors may use and disclose patient health information (“PHI”) and the security measures that must be taken in connection with protecting that information and related systems, as well as similar or more stringent state laws; |
| · | federal and state laws that provide penalties for providers for billing and receiving payment from a governmental healthcare program for services unless the services are medically necessary and reasonable, adequately and accurately documented, and billed using codes that accurately reflect the type and level of services rendered; |
| · | state laws that provide for financial solvency requirements relating to plan operations, plan-affiliate operations and transactions, plan-provider contractual relationships and provider-affiliate operations and transactions, such as California S.B. 260 (1999); |
| · | federal laws that provide for administrative sanctions, including civil monetary penalties for, among other violations, inappropriate billing of services to federal healthcare programs, payments by hospitals to physicians for reducing or limiting services to Medicare or Medicaid patients, or employing or contracting with individuals or entities who/which are excluded from participation in federal healthcare programs; |
| · | federal and state laws and policies that require healthcare providers to enroll in the Medicare and Medicaid programs before submitting any claims for services, to promptly report certain changes in its operations to the agencies that administer these programs, and to re-enroll in these programs when changes in direct or indirect ownership occur or in response to revalidation requests from Medicare and Medicaid; |
| 69 |
| · | state laws that prohibit general business entities from practicing medicine, controlling physicians’ medical decisions or engaging in certain practices, such as splitting fees with physicians; |
| · | state laws that require timely payment of claims, including California A.B. 1455 (1999) which imposes time limits for the payment of uncontested covered claims and required health care service plans to pay interest on uncontested claims not paid promptly within the required time period; |
| · | laws in some states that prohibit non-domiciled entities from owning and operating medical practices in its states; |
| · | provisions of the Social Security Act (emanating from the Deficit Reduction Act of 2005 (the “DRA”)) that require entities that make or receive annual Medicaid payments of $5 million or more from a single Medicaid program to provide its employees, contractors and agents with written policies and employee handbook materials on federal and state false claims acts and related statutes, that establish a new Medicaid Integrity Program designed to enhance federal and state efforts to detect Medicaid fraud, waste, and abuse, and that increase financial incentives for both states and individuals to bring fraud and abuse claims against healthcare companies; and |
| · | federal and state laws and regulations restricting the techniques that may be used to collect past due accounts from consumers, such as ApolloMed’s patients, for services provided to the consumer. |
ApolloMed cannot predict the effect that the ACA and its implementation, amendment, or repeal and replacement, may have on ApolloMed’s business, results of operations or financial condition.
The continued implementation of provisions of the ACA, the adoption of new regulations thereunder and ongoing legal challenges create an uncertain environment for how the ACA may affect ApolloMed’s business, results of operations and financial condition.
However, some of the reductions in Medicare spending, such as negative adjustments to the Medicare hospital inpatient and outpatient prospective payment system market basket updates and the incorporation of productivity adjustments to the Medicare program’s annual inflation updates, became effective starting in 2010. Although the expansion of health insurance coverage should increase revenues from providing care to previously uninsured individuals, many of these provisions of the ACA, as currently provided, will continue to become effective beyond 2017, and the impact of such expansion may be gradual and may not offset scheduled decreases in reimbursement.
On June 28, 2012, the U.S. Supreme Court upheld the constitutionality of the ACA, including the “individual mandate” provisions of the ACA that generally require all individuals to obtain healthcare insurance or pay a penalty. However, the U.S. Supreme Court also held that the provision of the ACA that authorized the Secretary of the U.S. Department of Health and Human Services (“HHS”) to penalize states that choose not to participate in the expansion of the Medicaid program by removing all of its existing Medicaid funding was unconstitutional. In response to the ruling, a number of U.S. governors opposed its state’s participation in the expanded Medicaid program, which resulted in the ACA not providing coverage to some low-income persons in those states. In addition, several bills have been, and are continuing to be, introduced in Congress to amend all or significant provisions of the ACA, or repeal and replace the ACA with another law.
The ACA changed how healthcare services are covered, delivered, and reimbursed. The net effect of the ACA on ApolloMed’s business is subject to numerous variables, including the law’s complexity, lack of complete implementing regulations and interpretive guidance, gradual and potentially delayed implementation or possible amendment, as well as the uncertainty as to the extent to which states will choose to participate in the expanded Medicaid program.
The ACA and the Health Care and Education Reconciliation Act of 2010 (collectively, the “Health Care Reform Acts”) mandated changes specific to home health and hospice benefits under Medicare. For home health, the Health Care Reform Acts mandated the creation of a value-based purchasing program, development of quality measures, a decrease in home health reimbursement beginning with federal year 2014 that will be phased-in over a four-year period, and a reduction in the outlier cap. In addition, the Health Care Reform Acts require the HHS Secretary to test different models for delivery of care, some of which would involve home health services. They also require the HHS Secretary to establish a national pilot program for integrated care for patients with specific conditions, bundling payment for acute hospital care, physician services, outpatient hospital services (including emergency department services), and post-acute care services, which would include home health. The Health Care Reform Acts further direct the HHS Secretary to rebase payments for home health, which will result in a decrease in home health reimbursement beginning in 2014 that is being phased-in over a four-year period. The HHS Secretary is also required to conduct a study to evaluate cost and quality of care among efficient home health agencies regarding access to care and treating Medicare beneficiaries with varying severity levels of illness and provide a report to Congress. Beginning October 1, 2012, the annual market basket rate increase for hospice providers was reduced by a formula that caused payment rates to be lower than in the prior year.
| 70 |
The impact that changes in healthcare laws could have on ApolloMed is uncertain but could be material.
Despite the enactment of the ACA and its being upheld by the U.S. Supreme Court as constitutional, continuing legal and political challenges to specific parts of the ACA have added uncertainty about the current state of healthcare laws in the United States. This uncertainty has intensified following the 2016 presidential election and the publicly announced intention of the leadership of the majority in the 115th Congress to “repeal and replace” the ACA, related Health Care Reform Acts and possibly other healthcare laws, and of the Administration to seek to have regulators amend or rescind certain regulations thereunder.
It is impossible to know what impact such efforts, assuming it is successful, will have on ApolloMed. However, any changes in healthcare laws or regulations that reduce, curtail or eliminate payments, government-subsidized programs, government-sponsored programs, and/or the expansion of Medicare or Medicaid, among other actions, could have a material adverse effect on ApolloMed’s business, results of operations and financial condition.
Just as the fate of the ACA is uncertain, so is the future of ACOs, which were established under the ACA to improve care and reduce costs. ApolloMed operates an ACO and has been approved by CMS to operate an ACO under the NGACO Model. Under the MSSP and NGACO programs and pursuant to the Participation Agreement ApolloMed has entered into with CMS for ApolloMed’s NGACO Model, ApolloMed’s ACO operations will always be subject to the nation’s healthcare laws, as amended, repealed or replaced from time to time.
It is impossible to know what impact such ‘repeal and replace” or similar efforts, assuming it is successful, will have on ApolloMed. However, any changes in healthcare laws or regulations that reduce, curtail or eliminate payments, reimbursements, government-subsidized programs, government-sponsored programs, and/or the expansion of Medicare or Medicaid, among other actions, could have a material adverse effect on ApolloMed’s business, results of operations and financial condition.
Providers in the healthcare industry are sometimes the subject of federal and state investigations, as well as payor audits.
Due to ApolloMed’s participation in government and private healthcare programs, ApolloMed is sometimes involved in inquiries, reviews, audits and investigations by governmental agencies and private payors of ApolloMed’s business practices, including assessments of ApolloMed’s compliance with coding, billing and documentation requirements. Federal and state government agencies have active civil and criminal enforcement efforts that include investigations of healthcare companies, and its executives and managers. Under some circumstances, these investigations can also be initiated by private individuals under whistleblower provisions which may be incentivized by the possibility for private recoveries. The Deficit Reduction Act revised federal law to further encourage these federal, state and individually-initiated investigations against healthcare companies.
Responding to these audit and enforcement activities can be costly and disruptive to ApolloMed’s business operations, even when the allegations are without merit. If ApolloMed is subject to an audit or investigation and a finding is made that ApolloMed was incorrectly reimbursed, it may be required to repay these agencies or private payors, or it may be subjected to pre-payment reviews, which can be time-consuming and result in non-payment or delayed payment for the services it provide. ApolloMed also may be subject to other financial sanctions or be required to modify ApolloMed’s operations.
| 71 |
Controls designed to reduce inpatient services may reduce ApolloMed’s revenues.
Controls imposed by Medicare, Medicaid and commercial third-party payors designed to reduce admissions and lengths of stay, commonly referred to as “utilization review”, have affected and are expected to continue to affect ApolloMed’s operations. Federal law contains numerous provisions designed to ensure that services rendered by hospitals to Medicare and Medicaid patients meet professionally recognized standards and are medically necessary and that claims for reimbursement are properly filed. These provisions include a requirement that a sampling of admissions of Medicare and Medicaid patients must be reviewed by quality improvement organizations, which review the appropriateness of Medicare and Medicaid patient admissions and discharges, the quality of care provided, and the appropriateness of cases of extraordinary length of stay or cost on a post-discharge basis. Quality improvement organizations may deny payment for services or assess fines and also have the authority to recommend to the U.S. Department of Health and Human Services that a provider which is in substantial noncompliance with the standards of the quality improvement organization be excluded from participation in the Medicare program. The ACA potentially expands the use of prepayment review by Medicare contractors by eliminating statutory restrictions on its use, and, as a result, efforts to impose more stringent cost controls are expected to continue. Utilization review is also a requirement of most non-governmental managed care organizations and other third-party payors. Inpatient utilization, average lengths of stay and occupancy rates continue to be negatively affected by payor-required preadmission authorization and utilization review and by third party payor pressure to maximize outpatient and alternative healthcare delivery services for less acutely ill patients. Although ApolloMed is unable to predict the effect these controls and changes will have on ApolloMed’s operations, significant limits on the scope of services reimbursed and on reimbursement rates and fees could have a material, adverse effect on ApolloMed’s business, financial position and results of operations.
Laws regulating the corporate practice of medicine could restrict the manner in which ApolloMed is permitted to conduct its business and the failure to comply with such laws could subject ApolloMed to penalties or require a corporate restructuring.
Some states have laws that prohibit business entities from practicing medicine, employing physicians to practice medicine, exercising control over medical decisions by physicians (also known collectively as the corporate practice of medicine) or engaging in some arrangements, such as fee-splitting, with physicians. In some states these prohibitions are expressly stated in a statute or regulation, while in other states the prohibition is a matter of judicial or regulatory interpretation. California is one of the states that prohibit the corporate practice of medicine.
In California, ApolloMed operates by maintaining contracts with its affiliated physician groups which are each owned and operated by physicians and which employ or contract with additional physicians to provide physician services. Under these arrangements, ApolloMed provides management services, receives a management fee for providing non-medical management services, does not represent that it offers medical services, and does not exercise influence or control over the practice of medicine by the physicians or the affiliated physician groups.
In addition to the above management arrangements, ApolloMed has some contractual rights relating to the transfer of equity interests in some of its affiliated physician groups to a nominee shareholder designated by them, through physician shareholder agreements, with Dr. Hosseinion, the controlling equity holder of such affiliated physician groups. However, such equity interests cannot be transferred to or held by ApolloMed or by any non-professional organization. Accordingly, ApolloMed does not directly own any equity interests in any physician groups in California. In the event that any of these affiliated physician groups fails to comply with the management arrangement or any management arrangement is terminated and/or ApolloMed is unable to enforce its contractual rights over the orderly transfer of equity interests in its affiliated physician groups, or California law is interpreted to invalidate these arrangements, there could be a material adverse effect on ApolloMed’s business, results of operations and financial condition.
ApolloMed’s palliative care business is subject to rules, prohibitions, regulations and reimbursement requirements that differ from those that govern its primary home health and hospice operations.
ApolloMed continues to develop its palliative care services, which is a type of care focused upon relieving pain and suffering in patients who do not qualify for, or who have not yet elected, hospice services. The continued development of this business line exposes ApolloMed to additional risks, in part because the business line requires them to comply with additional Federal and state laws and regulations that differ from those that govern its home health and hospice business. This line of business requires compliance with different Federal and state requirements governing licensure, enrollment, documentation, prescribing, coding, billing and collection of coinsurance and deductibles, among other requirements. Additionally, some states have prohibitions on the corporate practice of medicine and fee-splitting, which generally prohibit business entities from owning or controlling medical practices or may limit the ability of clinical professionals to share professional service income with non-professional or business interests. Reimbursement for palliative care and house calls services is generally conditioned on ApolloMed’s clinical professionals providing the correct procedure and diagnosis codes and properly documenting both the service itself and the medical necessity for the service. Incorrect or incomplete documentation and billing information, or the incorrect selection of codes for the level and type of service provided, could result in non-payment for services rendered or lead to allegations of billing fraud. Further, compliance with applicable regulations may cause ApolloMed to incur expenses that it has not anticipated, and if it is unable to comply with these additional legal requirements, ApolloMed may incur liability, which could have a material adverse effect on its business and consolidated financial condition, results of operations and cash flows.
| 72 |
ApolloMed’s home health, hospice and palliative care business line is subject to new licensing requirements, which will require ApolloMed to expend resources in order to comply with the changing requirements.
In October 2013, California enacted the Home Care Services Consumer Protection Act. The act establishes a licensing program for home care organizations, and requires background checks, basic training and tuberculosis screening for the aides that are employed by home care organizations. Home care organizations and aides had until January 1, 2015 to comply with the new licensing and background check requirements. Because ApolloMed operates in California, the requirements of the act are expected to impose additional costs on ApolloMed.
ApolloMed does not have a limited Knox-Keene license.
ApolloMed does not hold a limited Knox-Keene license, which is a managed care plan license in California. If the DMHC were to determine that ApolloMed has been inappropriately taking risk for institutional and professional services as a result of ApolloMed’s various hospital and physician arrangements without having a limited Knox-Keene license, it may be required to obtain a limited Knox-Keene license to resolve such violations and could be subject to civil and criminal liability, any of which could have a material adverse effect on ApolloMed’s business, results of operations and financial condition.
ApolloMed’s revenue may be negatively impacted by the failure of its affiliated physicians to appropriately document services it provides.
ApolloMed relies upon ApolloMed’s affiliated physicians to appropriately and accurately complete necessary medical record documentation and assign appropriate reimbursement codes for its services. Reimbursement to ApolloMed is conditioned upon, in part, ApolloMed’s affiliated physicians providing the correct procedure and diagnosis codes and properly documenting the services themselves, including the level of service provided and the medical necessity for the services. If ApolloMed’s affiliated physicians have provided incorrect or incomplete documentation or selected inaccurate reimbursement codes, this could result in nonpayment for services rendered or lead to allegations of billing fraud. This could subsequently lead to civil and criminal penalties, including exclusion from government healthcare programs, such as Medicare and Medicaid. In addition, third-party payors may disallow, in whole or in part, requests for reimbursement based on determinations that certain amounts are not covered, services provided were not medically necessary, or supporting documentation was not adequate. Retroactive adjustments may change amounts realized from third-party payors and result in recoupments or refund demands, affecting revenue already received.
Changes associated with reimbursement by third-party payors for ApolloMed’s services may adversely affect ApolloMed’s operating results and financial condition.
The medical services industry is undergoing significant changes with government and other third-party payors that are taking measures to reduce reimbursement rates or, in some cases, denying reimbursement altogether. There is no assurance that government or other third-party payors will continue to pay for the services provided by ApolloMed’s affiliated medical groups. Furthermore, there has been, and continues to be, a great deal of discussion and debate about the repeal and replacement of existing government reimbursement programs, such as the ACA. As a result, the future of healthcare reimbursement programs is uncertain, making long-term business planning difficult and imprecise. The failure of government or other third party payors to cover adequately the medical services provided by ApolloMed could have a material adverse effect on ApolloMed’s business, results of operations and financial condition.
Compliance with federal and state privacy and information security laws is expensive, and ApolloMed may be subject to government or private actions due to privacy and security breaches.
ApolloMed must comply with numerous federal and state laws and regulations governing the collection, dissemination, access, use, security and confidentiality of PHI, including HIPAA and HITECH. As part of ApolloMed’s medical record keeping, third-party billing, and other services, ApolloMed collects and maintains PHI in paper and electronic format. Therefore, new privacy or security laws, whether implemented pursuant to federal or state action, could have a significant effect on the manner in which ApolloMed handles healthcare-related data and communicates with payors. In addition, compliance with these standards could impose significant costs on ApolloMed or limit ApolloMed’s ability to offer services, thereby negatively impacting the business opportunities available to them. Despite ApolloMed’s efforts to prevent security and privacy breaches, it may still occur. If any non-compliance with existing or new laws and regulations related to PHI results in privacy or security breaches, ApolloMed could be subject to monetary fines, civil suits, civil penalties or even criminal sanctions.
| 73 |
As a result of the expanded scope of HIPAA through HITECH, ApolloMed may incur significant costs in order to minimize the amount of “unsecured PHI” it handles and retains or to implement improved administrative, technical or physical safeguards to protect PHI. ApolloMed may incur significant costs in order to demonstrate and document whether there is a low probability that PHI has been compromised in order to overcome the presumption that an impermissible use or disclosure of PHI results in a reportable breach. ApolloMed may incur significant costs to notify the relevant individuals, government entities and, in some cases, the media, in the event of a breach and to provide appropriate remediation and monitoring to mitigate the possible damage done by any such breach.
Providers must be properly enrolled in governmental healthcare programs, such as Medicare and Medicaid, before it can receive reimbursement for providing services, and there may be delays in the enrollment process.
Each time a new affiliated physician joins ApolloMed, ApolloMed must enroll the affiliated physician under ApolloMed’s applicable group identification number for Medicare and Medicaid programs and for certain managed care and private insurance programs before ApolloMed can receive reimbursement for services the physician renders to beneficiaries of those programs. The estimated time to receive approval for the enrollment is sometimes difficult to predict and, in recent years, the Medicare program carriers often have not issued these numbers to ApolloMed’s affiliated physicians in a timely manner. These practices result in delayed reimbursement that may adversely affect ApolloMed’s cash flow.
ApolloMed may face malpractice and other lawsuits that may not be covered by insurance.
Malpractice lawsuits are common in the healthcare industry. The medical malpractice legal environment varies greatly by state. The status of tort reform, availability of non-economic damages or the presence or absence of other statutes, such as elder abuse or vulnerable adult statutes, influence the incidence and severity of malpractice litigation. ApolloMed may also be subject to other types of lawsuits which may involve large claims and significant defense costs. Many states have joint and several liabilities for all healthcare providers who deliver care to a patient and are at least partially liable. As a result, if one healthcare provider is found liable for medical malpractice for the provision of care to a particular patient, all other healthcare providers who furnished care to that same patient, including possibly ApolloMed’s affiliated physicians, may also share in the liability, which may be substantial.
ApolloMed currently maintains malpractice liability insurance coverage to cover professional liability and other claims for certain hospitalists and clinic physicians. All of ApolloMed’s physicians are required to carry first dollar coverage with limits of coverage equal to $1,000,000 for all claims based on occurrence up to an aggregate of $3,000,000 per year. ApolloMed cannot be certain that its insurance coverage will be adequate to cover liabilities arising out of claims asserted against ApolloMed, ApolloMed’s affiliated professional organizations or ApolloMed’s affiliated physicians, and ApolloMed cannot provide assurance that any future liabilities will not have a material adverse impact on its results of operations, cash flows or financial position. Liabilities in excess of ApolloMed’s insurance coverage, including coverage for professional liability and other claims, could have a material adverse effect on ApolloMed’s business, financial condition, and results of operations. In addition, ApolloMed’s professional liability insurance coverage generally must be renewed annually and may not continue to be available to ApolloMed in future years at acceptable costs and on favorable terms.
ApolloMed has established reserves for potential medical liability losses which are subject to inherent uncertainties and a deficiency in the established reserves may lead to a reduction in ApolloMed’s net income.
ApolloMed establishes reserves for estimates of IBNR due to contracted physicians, hospitals, and other professional providers and risk-pool liabilities. IBNR estimates are developed using actuarial methods and are based on many variables, including the utilization of health care services, historical payment patterns, cost trends, product mix, seasonality, changes in membership, and other factors. Many of the medical contracts are complex in nature and may be subject to differing interpretations regarding amounts due for the provision of various services. Such differing interpretations may not come to light until a substantial period of time has passed following the contract implementation. The inherent difficulty in interpreting contracts and the estimated level of necessary reserves could result in significant fluctuations in ApolloMed’s estimates from period to period. It is possible that actual losses and related expenses may differ, perhaps substantially, from the reserve estimates reflected in ApolloMed’s financial statements. If subsequent claims exceed ApolloMed’s estimated reserves, ApolloMed may be required to increase reserves, which would lead to a reduction in ApolloMed’s assets or net income.
Litigation expenses may be material.
The defense of litigation, including fees of legal counsel, expert witnesses and related costs, is expensive and difficult to forecast accurately. In general, such costs are unrecoverable even if ApolloMed ultimately prevails in litigation and could represent a significant portion of ApolloMed’s limited capital resources. To defend lawsuits, it is also necessary for ApolloMed to divert officers and other employees from its normal business functions to gather evidence, give testimony and otherwise support litigation efforts. ApolloMed expects to experience higher than normal litigation costs until the lawsuits by ApolloMed’s competitor are decided.
| 74 |
If ApolloMed loses any material litigation, ApolloMed could face material judgments or awards against them. An unfavorable resolution of one or more of the proceedings in which ApolloMed is involved now or in the future could have a material adverse effect on ApolloMed’s business, assets, cash flow and financial condition.
ApolloMed may also in the future find it necessary to file lawsuits to recover damages or protect ApolloMed’s interests. The cost of such litigation could also be significant and unrecoverable, which may also deter ApolloMed from aggressively pursuing even legitimate claims.
ApolloMed may be subject to litigation related to the agreements that ApolloMed’s IPAs enter into with primary care physicians.
It is common in the medical services industry for primary care physicians to be affiliated with multiple IPAs. ApolloMed’s IPAs often enter into agreements with physicians who are also affiliated with ApolloMed’s competitors. However, some of ApolloMed’s competitors at times enter into agreements with physicians that require the physician to provide services exclusively to that competitor. ApolloMed’s IPAs often have no knowledge, and no way of knowing, whether a physician seeking to affiliate with ApolloMed is subject to an exclusivity agreement unless the physician informs ApolloMed of that agreement. ApolloMed’s IPAs rely on the physicians seeking to affiliate with ApolloMed to determine whether it is able to enter into the proposed agreement. Competitors have initiated lawsuits against ApolloMed based in part on interference with such exclusivity agreements, and may do so in the future. An adverse outcome in one or more of such lawsuits could adversely affect ApolloMed’s business, assets, cash flow and financial condition.
Changes in the rates or methods of Medicare reimbursements may adversely affect ApolloMed’s operations.
In order to participate in the Medicare program, ApolloMed must comply with stringent and often complex enrollment and reimbursement requirements. These programs generally provide for reimbursement on a fee-schedule basis rather than on a charge-related basis, meaning that generally ApolloMed cannot increase its revenue by increasing the amount it charge for its services. To the extent that ApolloMed’s costs increase, ApolloMed may not be able to recover its increased costs from these programs and cost containment measures and market changes in non-governmental insurance plans have generally restricted ApolloMed’s ability to recover, or shift to non-governmental payors, these increased costs. In attempts to limit federal and state spending, there have been, and ApolloMed expects that there will continue to be, a number of proposals to limit or reduce Medicare reimbursement for various services. In April of 2015, the Medicare Access and CHIP Reauthorization Act of 2015 (“MACRA”) was signed into law, which made numerous changes to Medicare, Medicaid, and other healthcare related programs. These changes include new systems for establishing the annual updates to payment rates for physicians’ services in Medicare. ApolloMed’s business may be significantly and adversely affected by MACRA and any changes in reimbursement policies and other legislative initiatives aimed at or having the effect of reducing healthcare costs associated with Medicare, TRICARE (which provides civilian health benefits for U.S. Armed Forces military personnel and military retirees and their dependents) and other government healthcare programs.
ApolloMed’s business also could be adversely affected by reductions in, or limitations of, reimbursement amounts or rates under these government programs, reductions in funding of these programs or elimination of coverage for certain individuals or treatments under these programs.
Overall payments made by Medicare for hospice services are subject to cap amounts. Total Medicare payments to ApolloMed for hospice services are compared to the cap amount for the hospice cap period, which runs from November 1 of one year through October 31 of the next year. CMS generally announces the cap amount in the month of July or August in the cap period and not at the beginning of the cap period. Accordingly, ApolloMed must estimate the cap amount for the cap period before CMS announces the cap amount. If ApolloMed’s estimate exceeds the later announced cap amount, ApolloMed may suffer losses. CMS can also make retroactive adjustments to cap amounts announced for prior cap periods, in which case payments to ApolloMed in excess of the cap amount must be returned to Medicare. A second hospice cap amount limits the number of days of inpatient care to not more than 20 percent of total patient care days within the cap period.
In addition, the Health Care Reform Acts includes several provisions that could adversely impact hospice providers, including a provision to reduce the annual market basket update for hospice providers by a productivity adjustment. ApolloMed cannot predict whether any healthcare reform initiatives will be implemented, or whether the Health Care Reform Acts or other changes in the administration of governmental healthcare programs or interpretations of governmental policies or other changes affecting the healthcare system will adversely affect ApolloMed’s revenues. Further, due to budgetary concerns, several states have considered or are considering reducing or eliminating the Medicaid hospice benefit. Reductions or changes in Medicare or Medicaid funding could significantly reduce ApolloMed’s net patient service revenue and ApolloMed’s profitability.
| 75 |
If ApolloMed inadvertently employs or contracts with an excluded person, ApolloMed may face government sanctions.
Individuals and entities can be excluded from participating in the Medicare and Medicaid programs for violating certain laws and regulations, or for other reasons such as the loss of a license in any state, even if the individual retains other licensure. This means that it (and all others) are prohibited from receiving payment for its services rendered to Medicare or Medicaid beneficiaries, and if the excluded individual is a physician, all services ordered (not just provided) by such physician are also non-covered and non-payable. Entities which employ or contract with excluded individuals are prohibited from billing the Medicare or Medicaid programs for the excluded individual’s services, and are subject to civil monetary penalties if it does. The U.S. Department of Health and Human Services Office of the Inspector General (“OIG”) maintains a list of excluded individuals and entities. Although ApolloMed has instituted policies and procedures through its compliance program to minimize the risks, there can be no assurance that ApolloMed will not inadvertently hire or contract with an excluded person, or that any of ApolloMed’s current employees or contracts will not become excluded in the future without ApolloMed’s knowledge. If this occurs, ApolloMed may be subject to substantial repayments and civil penalties, and the hospitals at which ApolloMed furnishes services also may be subject to repayments and sanctions, for which it may seek recovery from ApolloMed.
ApolloMed may be impacted by eligibility changes to government and private insurance programs.
Due to potential decreased availability of healthcare through private employers, the number of patients who are uninsured or participate in governmental programs may increase. A shift in payor mix from managed care and other private payors to government payors or the uninsured may result in a reduction in ApolloMed’s rates of reimbursement or an increase in ApolloMed’s uncollectible receivables or uncompensated care, with a corresponding decrease in ApolloMed’s net revenue. Changes in the eligibility requirements for governmental programs also could increase the number of patients who participate in such programs or the number of uninsured patients. Even for those patients who remain with private insurance, changes in those programs could increase patient responsibility amounts, resulting in a greater risk for ApolloMed of uncollectible receivables. Further, ApolloMed’s hospice related business could become subject to “quality star ratings” and, if sufficient quality is not achieved, reimbursement could be negatively impacted. These factors and events could have a material adverse effect on ApolloMed’s business, results of operations and financial condition.
Federal and state laws may limit ApolloMed’s effectiveness at collecting monies owed to ApolloMed from patients.
ApolloMed utilizes third parties whom ApolloMed does not and cannot control to collect from patients any co-payments and other payments for services that ApolloMed’s physicians provide to patients. The federal Fair Debt Collection Practices Act (the “FDCPA”) restricts the methods that third-party collection companies may use to contact and seek payment from consumer debtors regarding past due accounts. State laws vary with respect to debt collection practices, although most state requirements are similar to those under the FDCPA. If ApolloMed’s collection practices or those of ApolloMed’s collection agencies are inconsistent with these standards, ApolloMed may be subject to actual damages and penalties. These factors and events could have a material adverse effect on ApolloMed’s business, results of operations and financial condition.
If ApolloMed is unable to effectively adapt to changes in the healthcare industry, including changes to laws and regulations regarding or affecting healthcare reform or the healthcare industry, ApolloMed’s business may be harmed.
Due to the importance of the healthcare industry in the lives of all Americans, federal, state, and local legislative bodies frequently pass legislation and promulgate regulations relating to healthcare reform or that affect the healthcare industry. As has been the trend in recent years, it is reasonable to assume that there will continue to be increased federal oversight and regulation of the healthcare industry in the future. ApolloMed cannot assure its stockholders as to the ultimate content, timing or effect of any new healthcare legislation or regulations, nor is it possible at this time to estimate the impact of potential new legislation or regulations on ApolloMed’s business. It is possible that future legislation enacted by Congress or state legislatures, or regulations promulgated by regulatory authorities at the Federal or state level, could adversely affect ApolloMed’s business or could change the operating environment of the hospitals and other facilities where ApolloMed’s physicians provide services. It is possible that the changes to the Medicare or other governmental healthcare program reimbursements may serve as precedent to possible changes in other payors’ reimbursement policies in a manner averse to ApolloMed. Similarly, changes in private payor reimbursements could lead to adverse changes in Medicare and other governmental healthcare programs which could have a material adverse effect on ApolloMed’s business, financial condition and results of operations.
| 76 |
ApolloMed may incur significant costs to adopt certain provisions under HITECH.
HITECH was enacted into law on February 17, 2009 as part of the American Recovery and Reinvestment Act of 2009. Among the many provisions of HITECH are those relating to the implementation and use of certified electronic health records (“EHR”). ApolloMed’s patient medical records are maintained and under the custodianship of the healthcare facilities in which ApolloMed operates. However, to adopt the use of EHRs utilized by these healthcare facilities, determine to adopt certain EHRs, or comply with any related provisions of HITECH, ApolloMed may incur significant costs which could have a material adverse effect on ApolloMed’s business operations and financial position.
The healthcare industry is becoming increasingly reliant on use of technology.
The role of technology is greatly increasing in the delivery of healthcare, which provides risk to traditional physician-driven healthcare delivery companies such as ApolloMed. ApolloMed needs to understand and integrate with electronic health records, databases, cloud-based billing systems and many other technology applications in the delivery of ApolloMed’s services. Additionally, consumers are using mobile applications and care and cost research in selecting and usage of healthcare services. ApolloMed relies on employees and third parties with technology knowledge and expertise and could be at risk if resources are not properly established, maintained or secured.
ApolloMed may be exposed to cybersecurity risks.
While ApolloMed has not experienced any cybersecurity incidents, the nature of ApolloMed’s business and the requirements of healthcare privacy laws such as HIPAA and HITECH, impose significant obligations on ApolloMed to maintain the privacy and protection of patient medical information. Any cybersecurity incident could expose ApolloMed to violations of HIPAA and/or HITECH that, even unintended, could cause significant financial exposure to ApolloMed in the form of fines and costs of remediation of any such incident.
ApolloMed’s stock is thinly traded, the market price of ApolloMed’s common stock is volatile and the value of investments could fluctuate, and decline, significantly.
ApolloMed’s stock is thinly traded. In part because of that, and for other reasons, the trading price of ApolloMed’s common stock has been, and ApolloMed expects it to continue to be, volatile. The price at which ApolloMed’s common stock trades depends upon a number of factors, including ApolloMed’s results of operations, its financial situation, the announcement and consummation of certain transactions, ApolloMed’s ability or inability to raise the additional capital and the terms on which it raises capital and trading volume. Other factors include:
| · | variations in quarterly operating results; |
| · | developments in the hospitalists markets; |
| · | announcements of acquisitions dispositions and other corporate level transactions; |
| · | announcements of financings and other capital raising transactions; |
| · | sales of stock by ApolloMed’s stockholders generally and ApolloMed’s larger stockholders in particular; |
| · | general inefficiencies of trading on junior markets or quotations systems, including the need to comply on a state-by-state basis with state “blue sky” securities laws for the resale of ApolloMed’s common stock on OTC Pink; and |
| · | general stock market and economic conditions. |
There has been a limited trading market for ApolloMed’s common stock to date.
There has been limited trading volume in ApolloMed’s common stock, which is currently quoted on OTC Pink and traded under the symbol “AMEH.” Although ApolloMed has applied for listing of its common stock on the NASDAQ Global Market effective as of the closing of the Merger, it is anticipated that there will continue to be a limited trading market for ApolloMed’s common stock on NASDAQ, if ApolloMed’s application is approved. A lack of an active market may impair ApolloMed’s stockholders’ ability to sell shares at the time they wish to sell shares or at a price that ApolloMed’s stockholders consider reasonable. The lack of an active market may also reduce the fair market value of ApolloMed’s common stock. An inactive market may also impair ApolloMed’s ability to raise capital by selling shares of capital stock and may impair ApolloMed’s ability to acquire other companies by using common stock as consideration.
| 77 |
Investors may experience dilution of their ownership interests because of the future issuance of additional shares of ApolloMed’s common stock.
ApolloMed has issued some of its directors, officers, other employees, consultants, lenders and other third parties securities, including options, warrants, convertible preferred stock and convertible debt that such parties may exercise or convert into shares of ApolloMed’s common stock. Such conversions or exercises would result in the issuance of additional shares of ApolloMed’s common stock, resulting in dilution of the ownership interests of its present stockholders.
Moreover, ApolloMed may in the future issue additional authorized but previously unissued equity securities, resulting in further dilution of the ownership interests of ApolloMed’s present stockholders. ApolloMed may also issue additional shares of its common stock or other securities that are convertible into or exercisable for common stock in connection with hiring or retaining employees, future acquisitions, future sales of ApolloMed’s securities for capital raising purposes or for other business purposes. For example, ApolloMed will have to issue additional shares of common stock to NNA if ApolloMed fails to comply with NNA’s registration rights.
The future issuance of any such additional shares of common stock may create downward pressure on the trading price of ApolloMed’s common stock. There can be no assurance that ApolloMed will not be required to issue additional shares, warrants or other convertible securities in the future in conjunction with any capital raising efforts, including at a price (or exercise prices) below the price at which shares of ApolloMed’s common stock are currently traded at such time.
Delaware law and ApolloMed’s Charter could discourage a change in control, or an acquisition of us by a third party, even if the acquisition would be favorable to ApolloMed’s stockholders.
The DGCL contains provisions that may have the effect of making more difficult or delaying attempts by others to obtain control of us, even when these attempts may be in the best interests of ApolloMed’s stockholders. Delaware law imposes conditions on certain business combination transactions with “interested stockholders”. These provisions and others that could be adopted in the future could deter unsolicited takeovers or delay or prevent changes in ApolloMed’s control or management, including transactions in which stockholders might otherwise receive a premium for their shares over then current market prices. These provisions may also limit the ability of stockholders to approve transactions that they may deem to be in their best interests.
ApolloMed’s Charter empowers the ApolloMed board to establish and issue one or more classes of preferred stock, and to determine the rights, preferences and privileges of the preferred stock. These provisions give the ApolloMed board the ability to deter, discourage or make more difficult a change in control of ApolloMed, even if such a change in control could be deemed in the interest of ApolloMed’s stockholders or if such a change in control would provide ApolloMed’s stockholders with a substantial premium for their shares over the then-prevailing market price for the common stock.
In the past, ApolloMed’s common stock has been subject to the “penny stock” rules of the SEC, and it could become subject to that rule again. Additionally, trading in ApolloMed’s securities is very limited, which makes transactions in its common stock cumbersome, increases stock price volatility and may reduce the value of an investment in its securities.
The SEC has adopted Rule 3a51-1 under the Exchange Act, which establishes the definition of a “penny stock”, for the purposes relevant to us, as any equity security that has a market price of less than $5.00 per share or with an exercise price of less than $5.00 per share, subject to certain exceptions. During the last 52 weeks, ApolloMed’s common stock has traded at both below and above $5.00 per share. For any transaction involving a penny stock, unless exempt, Rule 15g-9 under the Exchange Act requires:
| · | a broker or dealer to approve a person’s account for transactions in penny stocks; and |
| · | a broker or dealer receives a written agreement for the transaction from the investor, setting forth the identity and quantity of the penny stock to be purchased. |
In order to approve a person’s account for transactions in penny stocks, the broker or dealer must:
| · | obtain financial information and investment experience objectives of the person; and |
| 78 |
| · | make a reasonable determination that the transactions in penny stocks are suitable for that person and the person has sufficient knowledge and experience in financial matters to be capable of evaluating the risks of transactions in penny stocks. |
The broker or dealer must also deliver, prior to any transaction in a penny stock, a disclosure schedule prescribed by the SEC relating to the penny stock market, which, among other things:
| · | sets forth the basis on which the broker or dealer made the suitability determination; and |
| · | that the broker or dealer received a signed, written agreement from the investor prior to the transaction. |
Disclosure also has to be made about the risks of investing in penny stocks in both public offerings and in secondary trading and about the commissions payable to both the broker-dealer and the registered representative, current quotations for the securities and the rights and remedies available to an investor in cases of fraud in penny stock transactions. Finally, monthly statements have to be sent disclosing recent price information for the penny stock held in the account and information on the limited market in penny stocks. Generally, brokers may be less willing to execute transactions in securities subject to the “penny stock” rules. This may make it more difficult for investors to purchase or sell ApolloMed’s common stock and cause a decline in the market value of its stock or underscore its stock’s volatility in the market.
Additionally, ApolloMed’s common stock is relatively thinly traded and on a number of days there are no market transactions in ApolloMed’s common stock. This could contribute to stock price volatility or supply/demand imbalances that could adversely affect the price of ApolloMed’s common stock from time to time, making an investment in ApolloMed’s common stock less attractive to certain investors.
Risks related to the Business of NMM
As a healthcare company, NMM is subject to many of the same risks to which ApolloMed is subject.
As a participant in the healthcare industry, NMM is subject to many of the same risks that ApolloMed is subject to as described in the ApolloMed risk factors, any of which could materially and adversely affect NMM’s revenues, earnings or cash flows. Among these risks are the following:
| · | the healthcare business is heavily regulated and changes in laws, regulations, or government programs could have a material impact on NMM’s business; |
| · | failure to comply with complex governmental regulations could have severe consequences to NMM, including, without limitation, exclusion from governmental payor programs like Medicare and Medicaid; |
| · | NMM could become the subject of governmental investigations, claims, and litigation; |
| · | NMM may be unable to continue to acquire or to successfully integrate acquisitions into its business, and such acquisitions may include liabilities of which NMM was not aware; and |
| · | as a result of the broad scope of NMM’s business, NMM may be exposed to medical malpractice claims, as well as claims for damages and other expenses, that may not be covered by insurance. |
NMM may encounter difficulties in managing its growth.
NMM may not be able to successfully grow and expand. Successful implementation of its business plan will require management of growth, including potentially rapid and substantial growth, which could result in an increase in the level of responsibility for management personnel and strain on NMM human and capital resources. To manage growth effectively, NMM will be required to continue to implement and improve its operating and financial systems and controls to expand, train and manage its employee base. NMM’s ability to manage its operations and growth effectively requires NMM to continue to expend funds to enhance its operational, financial and management controls, reporting systems and procedures and to attract and retain sufficient numbers of talented personnel. If NMM is unable to implement and scale improvements to all of its control systems in an efficient and timely manner or if NMM encounters deficiencies in existing systems and controls, then it will not be able to make available the services required to successfully execute its business plan. Failure to attract and retain sufficient numbers of qualified personnel could further strain its human resources and impede its growth or result in ineffective growth. Moreover, the management, systems and controls currently in place or to be implemented may not be adequate for such growth, and the steps taken to hire personnel and to improve such systems and controls might not be sufficient. If NMM is unable to manage its growth effectively, it will have a material adverse effect on its business, results of operations and financial condition.
| 79 |
The nature of NMM’s business and rapid changes in the healthcare industry makes it difficult to reliably predict future growth and operating results.
Rapidly changing Federal and state healthcare laws, and the regulations thereunder, make it difficult to anticipate the nature and amount of medical reimbursements, third party private payments and participation in certain government programs. This makes it difficult to forecast NMM’s future earnings, cash flow and results of operations. The evolving nature of the current medical services industry increases these uncertainties.
NMM’s growth strategy may not prove viable and expected growth and value may not be realized.
NMM’s business strategy is to grow rapidly by managing a network of medical groups and integrated physician networks. NMM also seeks growth opportunities both organically and through acquisitions of medical service providers. Identifying quality acquisition candidates is a time-consuming and costly process. There can be no assurance that NMM will be successful in identifying and establishing relationships with these and other candidates. If NMM is not successful in identifying and acquiring other entities, its ability to successfully implement its business plan and achieve targeted financial results could be adversely affected. The process of integrating acquired entities involves significant risks, which include, but are not limited to:
| · | demands on NMM’s management team related to the significant increase in the size of its business; |
| · | diversion of management’s attention from the management of daily operations; |
| · | difficulties in the assimilation of different corporate cultures and business practices; |
| · | difficulties in conforming the acquired entities’ accounting policies to NMM’s; |
| · | retaining employees who may be vital to the integration of departments, information technology systems, including accounting; |
| · | systems, technologies, books and records, procedures and maintaining uniform standards, such as internal accounting controls; |
| · | procedures, and policies; and |
| · | costs and expenses associated with any undisclosed or potential liabilities. |
There can be no assurance that NMM will be able to manage the integration of its acquisitions or the growth of such acquisitions effectively.
NMM may not make appropriate acquisitions, may fail to integrate them into its business, or these acquisitions could alter NMM’s current payor mix and reduce its revenue.
NMM’s business is significantly dependent on locating and acquiring, partnering or contracting with medical practices to provide health care services. As part of NMM’s growth strategy, it regularly reviews potential acquisition opportunities. NMM cannot predict whether it will be successful in pursuing such acquisition opportunities or what the consequences of any such acquisitions would be. If NMM is not successful in finding attractive acquisition candidates that it can acquire on satisfactory terms, or if it cannot successfully complete and efficiently integrate those acquisitions that it identifies, NMM may not be able to implement its business model, which would likely negatively impact its revenues, results of operations and financial condition. Furthermore, NMM’s acquisition strategy involves a number of risks and uncertainties, including:
| · | NMM may not be able to identify suitable acquisition candidates or strategic opportunities or successfully implement or realize the expected benefits of any suitable opportunities. In addition, NMM competes for acquisitions with other potential acquirers, some of which may have greater financial or operational resources than it does. This competition may intensify due to the ongoing consolidation in the healthcare industry, which may increase NMM’s acquisition costs. |
| 80 |
| · | NMM may be unable to successfully and efficiently integrate completed acquisitions, including its recently completed acquisitions and such acquisitions may fail to achieve the financial results it expected. Integrating completed acquisitions into NMM’s existing operations involves numerous short-term and long-term risks, including diversion of its management’s attention, failure to retain key personnel, failure to retain payor contracts and failure of the acquired practice to be financially successful. |
| · | NMM cannot be certain of the extent of any unknown or contingent liabilities of any acquired business, including liabilities for failure to comply with applicable laws. NMM may incur material liabilities for past activities of acquired entities. Also, depending on the location of the acquisition, it may be required to comply with laws and regulations that may differ from those of the states in which NMM’s operations are currently conducted. |
| · | NMM may acquire group medical practices that operate with lower profit margins as compared with its current or expected profit margins or which have a different payor mix than NMM’s other practice groups, which would reduce its profit margins. Depending upon the nature of the local healthcare market, NMM may not be able to implement its business model in every local market that it enters, which may negatively impact NMM’s revenues and financial condition. |
| · | If NMM finances acquisitions by issuing equity securities or securities convertible into equity securities, its existing stockholders could be diluted. If NMM finances an acquisition with debt, it could result in higher leverage and interest costs. As a result, if it fails to evaluate and execute acquisitions properly, NMM might not achieve the anticipated benefits of these acquisitions, and it may increase its acquisition costs. |
NMM management team’s attention may be diverted by recent acquisitions and searches for new acquisition targets, and its business and operations may suffer adverse consequences as a result.
Mergers and acquisitions are time-intensive, requiring significant commitment of NMM’s management team’s focus and resources. If NMM’s management team spends too much time focused on recent acquisitions or on potential acquisition targets, its management team may not have sufficient time to focus on its existing business and operations. This diversion of attention could have material and adverse consequences on NMM’s operations and its ability to be profitable.
NMM’s growth strategy incurs significant costs, which could adversely affect its financial condition.
NMM’s growth-by-acquisition strategy involves significant costs, including financial advisory, legal and accounting fees, and may include additional costs, including costs of fairness opinions, labor costs, termination payments, contingent payments and bonuses, among others. These costs could put a strain on NMM’s available cash and cash flow, which in turn could adversely affect its overall financial condition.
NMM may be unable to scale its operations successfully.
NMM’s growth strategy will place significant demands on its management and financial, administrative and other resources. Operating results will depend substantially on the ability of NMM’s officers and key employees to manage changing business conditions and to implement and improve its financial, administrative and other resources. If NMM is unable to respond to and manage changing business conditions, or the scale of its operations and the quality of its services, NMM’s ability to retain key personnel and its business could be adversely affected.
NMM could experience significant losses under its capitation-based contracts if the medical expenses it incurs exceed revenues.
In California, health plans typically prospectively pay an IPA a PMPM amount, or capitation payment, which is often based on a percentage of the amount received by the health plan. Capitation payments to IPAs, in the aggregate, represent a prospective budget from which the IPA manages care-related expenses on behalf of the population enrolled with that IPA. If NMM’s IPAs are able to manage care-related expenses under the capitated levels, NMM realizes an operating profit on its capitation contracts. However, if NMM’s care-related expenses exceed projected levels, its IPAs may realize substantial operating deficits, which are not capped and could lead to substantial losses.
| 81 |
If NMM’s agreements or arrangements with its affiliated physician groups are deemed invalid under state corporate practice of medicine and similar laws, or Federal law, or are terminated as a result of changes in state law, it could have a material impact on NMM’s results of operations and financial condition.
There are various state laws, including laws in California, regulating the corporate practice of medicine which prohibits NMM from owning various healthcare entities. This corporate practice of medicine prohibitions are intended to prevent unlicensed persons from interfering with or inappropriately influencing a physician’s professional judgment. These and other laws may also prevent fee-splitting, which is the sharing of professional service income with non-professional or business interests. The interpretation and enforcement of these laws vary significantly from state to state. If these agreements and arrangements were held to be invalid under state laws prohibiting the corporate practice of medicine, a significant portion of NMM’s revenues would be affected, which may result in a material adverse effect on NMM’s results of operations and financial condition. Additionally, any changes to Federal or state law that prohibit such agreements or arrangements could also have a material adverse effect upon NMM’s results of operations and financial condition.
The contractual arrangements NMM has with its VIEs is not as secure as direct ownership of such entities.
Because of corporate practice of medicine laws, NMM enters into contractual arrangements to manage certain affiliated physician practice groups, which allows NMM to consolidate those groups for financial reporting purposes. If NMM had direct ownership of certain of NMM’s affiliated entities, it would be able to exercise its rights as an equity holder directly to effect changes in the boards of directors of those entities, which could effect changes at the management and operational level. Under NMM’s contractual arrangements, it may not be able to directly change the members of the boards of directors of these entities and would have to rely on the entities and the entities’ equity holders to perform its obligations in order to exercise NMM’s control over the entities. If any of these affiliated entities or its equity holders fail to perform its respective obligations under the contractual arrangements, NMM may have to incur substantial costs and expend additional resources to enforce such arrangements.
Any failure by NMM’s key affiliated entities or its equity holders to perform its obligations under the contractual arrangements it has with NMM would have a material adverse effect on NMM’s business, results of operations and financial condition. NMM also owns the majority, and not all, of the equity of certain subsidiaries.
Several of NMM’s affiliated physician practice groups are owned by other physicians who could die, become incapacitated or otherwise become no longer affiliated with NMM. Although the terms of the MSAs NMM has with these affiliates provide that the MSA will be binding on the successors of such affiliates, as those successors are not parties to the MSAs, it is uncertain whether the successors in case of the death, bankruptcy or divorce of an equity holder would be subject to such MSAs.
| 82 |
NMM’s operations are dependent on a limited number of key payors.
NMM’s operations are dependent on Blue Cross, Central Health, Health Net, LA Care and Blue Shield. Four of these HMO’s accounted for 69% and 71% of NMM’s total capitation and claims revenue for the years ended December 31, 2016 and 2015, respectively. Three and four HMO’s accounted for 96% and 99% of the total risk pool settlement revenue for the years ended December 31, 2016 and 2015, respectively. Three HMO’s accounted for 83% and 85% of the total fee for services revenue for the years ended December 31, 2016 and 2015, respectively. NMM believes that a majority of its revenue will continue to be derived from a limited number of key payors. Each payor may immediately terminate any of NMM’s contracts or any individual credentialed physician upon the occurrence of certain events. They may also amend the material terms of the contracts under certain circumstances. Failure to maintain the contracts on favorable terms or at all, for any reason, would materially and adversely affect NMM’s results of operations and financial condition.
A decline in the number of patients NMM and its affiliated physician groups serve could have a material adverse effect on NMM’s results of operations.
Like any business, a material decline in the number of patients NMM and its affiliated physician groups serve, whether it or a third party government or private entity is paying for its healthcare, could have a material adverse effect on NMM’s results of operations and financial condition.
ACOs are relatively new and undergoing changes and CMS may change or discontinue the MSSP program.
NMM has invested resources in both applying to participate in the MSSP and in establishing initial infrastructure. The MSSP program and the rules regarding ACOs has been altered and may be further altered in the future. Any material change to the MSSP program and ACO requirements, governance and operating rules, could provide a significant financial risk for NMM and alter its strategic direction, thereby producing stockholder risk and uncertainty. In addition, NMM could be terminated from the MSSP if it does not comply with the MSSP participation requirements.
NMM’s ACOs may not generate savings through its participation in the MSSP revenue, if any, earned by such participation will occur, only once annually on an “all or nothing” basis.
NMM operates two ACOs that participate in the MSSP sponsored by CMS. The MSSP is a relatively new program with limited history of payments to ACO participants. As a result of the uncertain nature of the MSSP program, NMM considers revenue, if any, under the MSSP, as contingent upon the realization of program savings as determined by CMS, and revenues are not considered earned and therefore are not recognized until notice from CMS that cash payments are to be imminently received.
In addition, there is no assurance that NMM will meet the conditions necessary for receipt of future payments. Furthermore, NMM’s ability to continue to generate savings for the MSSP program depends on many factors, many of which are outside NMM’s control, including, among others, how CMS elects to administer the MSSP program, how savings levels are calculated and continued political support of the MSSP program. As a result, whether future revenues will be earned by NMM’s ACOs is uncertain and will be contingent on various factors, including whether savings were determined to be achieved in 2015 or in any other period during which savings are measured.
Moreover, if amounts are payable to NMM under the MSSP, it will be paid on an annual basis significantly after the time it is earned. Additionally, since MSSP payments, if any, are made once annually, NMM would not receive such payments spread out over its fiscal year and, consequently, revenue may be materially lower in quarters when any MSSP-related payments are not received by NMM.
The success of NMM’s emphasis on the new NGACO Model is uncertain.
To position NMM to participate in the NGACO Model, it has devoted, and intends to continue to devote, significant effort and resources, financial and otherwise, to the NGACO Model, and refocus away from certain other parts of NMM’s historic business and revenue streams, which will receive less emphasis in the future and could result in reduced revenue from these activities. It is unknown at this time if this strategic decision will be successful in terms of NMM’s emphasis on the NGACO Model and/or placing less emphasis on certain other parts of NMM’s core business and revenue streams.
| 83 |
The results of the NGACO Model are unknown.
The NGACO Model is a new CMS program that builds upon previous ACO programs, including the MSSP program. Through the NGACO Model, CMS will provide an opportunity to APAACO and other NGACOs experienced in coordinating care for populations of patients, and whose provider groups are willing to assume higher levels of financial risk and reward, to participate in this new attribution-based risk sharing model. In January 2017, CMS approved APAACO to participate in the NGACO Model and CMS and APAACO have entered into the Participation Agreement with a term of two performance years through December 31, 2018. CMS may offer to renew the Participation Agreement for an additional two performance years. Additionally, the Participation Agreement may be terminated sooner by CMS as specified therein and CMS has the flexibility to alter or change the program over this time period. The number of Medicare ACOs continues to rise in total but there are still a growing number of program types and demonstrations that could be consolidated and impact APAACO.
The NGACO Model program has certain political risks.
If the ACA is amended or repealed and replaced, or if CMMI is terminated, the NGACO Model program could be discontinued or significantly altered. In addition, CMS leadership could be changed and influenced by Congress and/or the current Administration. Additionally, CMS or CMMI may elect to combine any existing programs, including bundled payments, which could greatly alter the NGACO Model program.
APAACO’s participation in the NGACO Model program subjects it to certain regulatory risks.
Among many requirements to be eligible to participate in the NGACO Model program, APAACO must have at least 10,000 assigned Medicare beneficiaries and must maintain that number throughout each performance year. Although APAACO started its 2017 performance year with more than 32,000 assigned Medicare beneficiaries, there can be no assurance that APAACO will maintain the required number of assigned Medicare beneficiaries, and, if that number were not maintained, APAACO would become ineligible for the program.
APAACO is subject to changing state laws and regulations.
NGACOs are required to comply with all applicable state laws and regulations regarding provider-based risk-bearing entities. If these laws or regulations change, for example, to require a Knox-Keene license in California, which NMM does not have, APAACO could be required to cease its NGACO operations.
APAACO may experience losses due to the NGACO Model Program.
APAACO is responsible for savings and losses from claims. The NGACO Model uses a prospectively-set cost benchmark, which is established prior to the start of each performance year. The benchmark is based on various factors, including baseline expenditures with the baseline updated each year to reflect the NGACO’s participant list for the given year. The 2017 performance year NGACO Model baseline for APAACO is based on calendar year 2014 expenditures that are risk adjusted and trended. A discount is then applied that incorporates regional and national efficiency. The final benchmark could potentially underestimate APAACO’s actual expenditures for its Medicare beneficiaries.
If claims cost rise from benchmark, or 2014 and/or 2017 are statistical anomalies, APAACO could experience losses due to the NGACO Model program, which could be significant prior to any adjustment in benchmarked expenditures.
Additionally, given that APAACO is providing care coordination but does not employ any physicians nor provide direct patient care, the degree of influence APAACO has could be limited and out of its direct control. Because of APAACO’s limited influence, it is possible APAACO may not be able to influence provider and preferred provider behavior, utilization and patient costs.
| 84 |
APAACO’s dependence on CMS creates uncertainty and subjects APAACO to potential liability.
APAACO relies on CMS for design, oversight and governance of the NGACO Model program. Accurate data, claims benchmarking and calculations, timely payments and periodic process reviews are key to program success. In addition to APAACO’s administrative and care coordination operating costs, APAACO may not generate savings through its participation in the NGACO Model. Any savings generated, if at all, will be earned in arrears and uncertain in both timing and amount.
APAACO chose to participate in the AIPBP payment mechanism, which entails certain special risks.
APAACO chose to participate in the AIPBP payment mechanism, and is the only NGACO to have chosen this payment mechanism. Under the AIPBP payment mechanism, CMS will estimate the total annual Part A and Part B Medicare expenditures of APAACO’s assigned Medicare beneficiaries and pay that projected amount in per beneficiary per month payments. APAACO chose “Risk Arrangement A,” comprising 80% risk for Part A and Part B Medicare expenditures and a shared savings and losses cap of 5%, or as a result a 4% effective shared savings and losses cap when factoring in 80% risk impact. APAACO’s benchmark Medicare Part A and Part B expenditures for beneficiaries for its 2017 performance year are approximately $335 million, and under “Risk Arrangement A” of the AIPBP payment mechanism APAACO could therefore have profits or be liable for losses of up to 4% of such benchmarked expenditures, or approximately $13.4 million. While performance can be monitored throughout the year, end results will not be known until 2018.
CMS has indicated that its initial financial reports to participants in the NGACO Model may not be complete.
The NGACO Model is new and CMS is implementing extensive reporting protocols in connection therewith. CMS has indicated that it does not anticipate initial reports under the NGACO Model to be indicative of final results of actual risk-sharing and revenues to which NMM is entitled, especially for the period April 1, 2017 through June 30, 2017, which is the second quarter of the NGACO program and the second quarter of NMM’s 2017 fiscal year. This is because there are inherent biases in reporting the results at such an early juncture. Were that to be the case, NMM might not report accurately NMM’s revenues for this period, which could be subject to adjustment in a later period once NMM receives final results from CMS.
APAACO requires significant capital reserves for program participation.
NGACOs must provide a financial guarantee to CMS. The financial guarantee must be in an amount of 2% of the NGACO’s benchmark Medicare Part A and Part B expenditures. APAACO’s benchmark Medicare Part A and Part B expenditures for beneficiaries for its 2017 performance year being approximately $335 million, APAACO submitted a letter of credit for $6.7 million for the 2017 program year. If APAACO reaches the maximum of its shared losses of $13.4 million, it may need to pay another $6.7 million to CMS or CMS may change or alter the risk reserve process or amount. Additionally, the IBNR methodology utilized by CMS could have a negative impact on APAACO and affect working capital and capital requirements.
APAACO is responsible for savings and losses related to care received by its patients at Out-of-Network Providers which could negatively impact NMM’s ability to control claim costs.
Medicare beneficiaries in a NGACO Model program are not required to receive its care from a narrow network of contracted providers and facilities, which could make it challenging for APAACO to control the financial risks of those beneficiaries. CMS notified APAACO that its Medicare beneficiaries historically have received approximately 62% of its care at non-contracted, OON providers. While not responsible for paying claims for OON providers, APAACO may have difficulty managing patient care and costs as compared to in-network providers. Additionally, APAACO is responsible for savings and losses of this population using OON providers, which could adversely impact NMM’s financial results.
In addition, if APAACO is successful under its Participation Agreement with CMS in encouraging more of its patients to receive care with contracted, in-network providers, there is the possibility that the monthly AIPBP payments will be insufficient to cover current expenditures, since the AIPBP payments will be based on historical in-network/out-of-network ratios. This could potentially result in negative cash-flow problems for APAACO, if increased payments need to be made to contracted, in-network providers, especially if CMS fails to monitor this in-network/OON ratio on a frequent periodic basis and reconciliation payments are materially delayed.
| 85 |
There is uncertainty regarding the initial design and administration of the NGACO Model program.
Due to the newness of the NGACO Model program and the fact that APAACO is the only company participating in the AIPBP track, APAACO is subject to initial program challenges including, but not limited to, process design, data and other related program aspects. APAACO has already experienced various apparent errors in the NGACO Model program and APAACO has been working with CMS, including senior CMS management, on these issues, but the resolution and impact on APAACO remains uncertain. Moreover, there is the potential for new or additional issues to be experienced with CMS which could negatively impact APAACO. Among other things, the AIPBP claims processing methodology is complex and could create reimbursement delays to contracted APAACO providers, which could cause some providers to terminate its agreements with APAACO. For example, services provided by contracted APAACO providers with DOS from January 1, 2017 to March 31, 2017 were to be paid by CMS. All services provided with DOS from April 1, 2017 onward were to be paid by APAACO. But a flaw in the claims processing system of one of CMS’ contractors caused payments to contracted APAACO providers to be unpaid or to be paid at a reduced rate from January 1, 2017 to March 31, 2017. Various providers expressed dissatisfaction about this and several decided to terminate its agreements with APAACO. Consequently, there is the actual and potential risk of damaging goodwill with APAACO’s contracted providers, which could have a material adverse effect on the operations and financial condition of APAACO in particular and NMM’s results of operations and financial condition on a consolidated basis.
APAACO has also experienced weaknesses in the NGACO Model program beneficiary alignment methodology. For example, some patients see more than one PCP in a calendar year. CMS could attribute a patient to one PCP rather than another, which could create potential liability for APAACO. For example, when APAACO sent letters to its patients, as required by CMS, it received several calls from PCPs who did not join APAACO, but whose patients were attributed to another PCP. There could also be liability where a PCP has a capitated contract with APAACO, but the PCP’s patient also sees another PCP, whether that PCP was contracted with APAACO or not. APAACO’s expenditures could increase due to CMS having paid an additional PCP, or to the extent that APAACO has to pay for a PCP that is not an APAACO contracted provider.
AIPBP operations and benchmarking calculations are complex.
AIPBP operations and benchmarking calculations are complex and can lead to errors in the application of the NGACO Model program, which could create reimbursement delays to NMM’s providers and adversely affect APAACO’s performance and results of operations. For example, APAACO has discovered a feature in the AIPBP claims files that do not allow APAACO to break down certain claims amounts by individual patient codes. This feature has created confusion for APAACO contracted providers in reconciling its payments, causing some providers to terminate its agreements with APAACO. This feature could also create uncertainty with those agreements with providers that include capitation plus carve-outs for certain procedures. APAACO has sought to address its concerns about such feature with CMS and CMS has informed APAACO that CMS’ contractor is unable to remedy this situation for at least the foreseeable future.
CMS relies on multiple third-party contractors to manage the NGACO Model program, which could hinder performance.
In addition to CMS reliance, CMS relies on various third parties to effect the NGACO program. This may be other departments of the U.S. government, such as CMMI. CMS relies on multiple third party contractors to manage the NGACO Model program, including claims and auditing. Due to such reliance, there is the potential for errors, delays and poor communication among the differing entities involved, which are beyond the control of APAACO. This could negatively impact APAACO’s results of operations specifically and NMM’s results of operations on a consolidated basis.
Third parties used by APAACO could hinder performance.
APAACO uses select third parties. This could create operational and performance risk if, for example, the third party does not perform its responsibilities properly. Additionally, APAACO has contracted with participating Part A and Part B providers and was able to contract discounted Medicare, Diagnosis-Related Group and Resource Utilization Group rates with multiple providers. However, APAACO providers could decide to change or discontinue these contractual rates or to terminate its agreements with APAACO.
| 86 |
Risk-sharing arrangements that NMM’s affiliated physician groups have with health plans and hospitals could result in its costs exceeding the corresponding revenues, which could reduce or eliminate any shared risk profitability.
Under risk-sharing arrangements into which NMM’s affiliated physician groups have entered, NMM’s affiliated physician groups are responsible for a portion of the cost of hospital services or other services that are not capitated. These risk-sharing arrangements may require NMM to assume a portion of any loss sustained from such arrangements, thereby adversely affecting NMM’s results of operations. The terms of the particular risk-sharing arrangement allocate responsibility to the respective parties when the cost of services exceeds the related revenue, which results in a deficit, or permit the parties to share in any surplus amounts when actual costs are less than the related revenue. The amount of non-capitated medical and hospital costs in any period could be affected by factors beyond the control of NMM, such as changes in treatment protocols, new technologies, longer lengths of stay by the patient, and inflation. To the extent that such non-capitated medical and hospital costs are higher than anticipated, revenue may not be sufficient to cover the risk-sharing deficits the health plans and NMM are responsible for, which could reduce NMM’s revenue and adversely affect NMM’s results of operations.
If NMM’s affiliated physician groups are not able to satisfy DMHC’s requirements, NMM’s affiliated physician groups could become subject to sanctions and its ability to do business in California could be limited or terminated.
The DMHC has instituted financial solvency regulations. The regulations are intended to provide a formal mechanism for monitoring the financial solvency of an RBO in California, including capitated physician groups, such as APC. Under DMHC regulations, NMM’s affiliated physician groups are required to, among other things:
| · | Maintain, at all times, a minimum “cash-to-claims ratio” (where “cash-to-claims ratio” means the organization’s cash, marketable securities, and certain qualified receivables, divided by the organization’s total unpaid claims liability). The regulations currently require a cash-to-claims ratio of 0.75; and |
| · | Submit periodic reports to the DMHC containing various data and attestations regarding performance and financial solvency, including incurred but not reported calculations and documentation, and attestations as to whether or not the organization was in compliance with the Knox-Keene Act, requirements related to claims payment timeliness, had maintained positive tangible net equity (i.e. at least $1.00), and had maintained positive working capital (i.e. at least $1.00). |
In the event that a physician organization is not in compliance with any of the above criteria, the organization would be required to describe in a report submitted to the DMHC the reasons for non-compliance and actions to be taken to bring the organization into compliance. Additionally, under these regulations, the DMHC can make public some of the information contained in the reports, including, but not limited to, whether or not a particular physician organization met each of the criteria. In the event NMM’s affiliated physician groups are not able to meet certain of the financial solvency requirements, and fail to meet subsequent corrective action plans, NMM’s affiliated physician groups could be subject to sanctions, or limitations on, or removal of, its ability to do business in California.
Economic conditions or changing consumer preferences could adversely impact NMM’s business.
A downturn in economic conditions in one or more of NMM’s markets could have a material adverse effect on NMM’s results of operations, financial condition, business and prospects. Historically, state budget limitations have resulted in reduced state spending. Given that Medicaid is a significant component of state budgets, an economic downturn would put continued cost containment pressures on Medicaid outlays for NMM’s services in California. In addition, an economic downturn and/or sustained unemployment, may also impact the number of enrollees in managed care programs as well as the profitability of managed care companies, which could result in reduced reimbursement rates.
The existing Federal deficit, as well as deficit spending by the government as the result of adverse developments in the economy or other reasons, can lead to continuing pressure to reduce government expenditures for other purposes, including government-funded programs in which NMM participates, such as Medicare and Medicaid. Such actions in turn may adversely affect NMM’s results of operations.
| 87 |
Although NMM attempts to stay informed of government and customer trends, any sustained failure to identify and respond to trends could have a material adverse effect on NMM’s results of operations, financial condition, business and prospects.
NMM’s success depends, to a significant degree, upon NMM’s ability to adapt to a changing market and continued development of additional services.
Although NMM expects to provide a broad and competitive range of services, there can be no assurance of acceptance by the marketplace. NMM’s ability to procure new contracts may be dependent upon the continuing results achieved at the current facilities, upon pricing and operational considerations, and the potential need for continuing improvement to existing services. Moreover, the markets for such services may not develop as expected nor can there be any assurance that NMM will be successful in its marketing of any such services.
NMM’s revenues and profits could be diminished if NMM fails to retain and attract the services of key primary care physicians.
Key primary care physicians with large patient enrollment could retire, become disabled, terminate their provider contracts, get lured away by a competing independent physician association or medical group, or otherwise become unable or unwilling to continue practicing medicine or contracting with NMM or its affiliated physicians, physician groups, or IPAs. Moreover, given limitations relating to the enforcement of post-termination noncompetition covenants in California, it would be difficult to restrict a primary care physician from competing with NMM’s affiliated physicians, physician groups, or IPAs. As a result, members who have been served by such physicians could choose to enroll with competitors’ physician organizations or could seek medical care elsewhere, which could reduce NMM’s affiliated physician group revenues and profits. Moreover, NMM’s affiliated physician groups may not be able to attract new physicians to replace the services of terminating physicians or to service its growing membership.
The healthcare industry continues to experience shortages in qualified service employees and management personnel and NMM may be unable to hire qualified employees.
NMM and its affiliated physician groups compete with other healthcare providers for its employees, both clinical associates and management personnel. As the demand for health services continues to exceed the supply of available and qualified staff, NMM and its competitors have been forced to offer more attractive wage and benefit packages to these professionals. Furthermore, the competition for this segment of the labor market has created turnover as many seek to take advantage of the supply of available positions, many of which offer new and more attractive wage and benefit packages. In addition to the wage pressures described above, the cost of training new employees amid the turnover rates may cause added pressure on NMM’s operating margins.
The healthcare industry is highly competitive.
There are many other companies and individuals currently providing health care services, many of which have been in business longer than NMM has been, and/or have substantially more financial and personnel resources than NMM has. NMM competes directly with national, regional and local providers of inpatient healthcare for patients and physicians. Other companies could enter the market in the future and divert some or all of NMM’s business. On a national basis, NMM’s competitors include, but are not limited to, DaVita and Heritage, each of which has greater financial and other resources available to them. NMM also competes with physician groups and privately-owned health care companies in each of NMM’s local markets. Existing or future competitors also may seek to compete with NMM for acquisitions, which could have the effect of increasing the price and reducing the number of suitable acquisitions, which would have an adverse impact on NMM’s growth strategy. Since there are virtually no capital expenditures required to enter the industry, there are few financial barriers to entry. Individual physicians, physician groups and companies in other healthcare industry segments, including hospitals with which NMM has contracts, and some of which have greater financial, marketing and staffing resources, may become competitors in providing health care services, and this competition may have a material adverse effect on NMM’s business operations and financial position. In addition, certain governmental payors contract for services with independent providers such that NMM’s relationships with these payors are not exclusive, particularly in California, where all of NMM’s operations, providers and patients are located.
| 88 |
Hospitals may terminate their agreements with NMM’s affiliated physician groups or reduce the fees they pay to NMM.
In California, NMM’s affiliated physician groups maintain significant hospital arrangements designed to facilitate the provision of coordinated hospital care with those services provided to members by NMM’s affiliated physician groups. Through contractual arrangements with certain key hospitals, NMM’s affiliated physician groups provide utilization review, quality assurance, and other management services related to the provision of patient care services to members by the contracted hospitals and downstream hospital contractors. In the event that any one of these key hospital agreements is amended in a financially unfavorable manner or is otherwise terminated, any of such events may negatively impact NMM’s revenue, results of operations and financial condition.
Some of the hospitals where NMM’s affiliated physicians provide services may have its medical staff closed to non-contracted physicians.
In general, NMM’s affiliated physicians may only provide services in a hospital where it has certain credentials, called privileges, which are granted by the medical staff and controlled by the legally binding medical staff bylaws of the hospital. The medical staff decides who will receive privileges and the medical staff of the hospitals where NMM’s affiliated physicians currently provide services or wish to provide services could decide that non-contracted physicians can no longer receive privileges to practice there. Such a decision would limit the ability of NMM’s affiliated physicians to furnish services in a hospital, decrease the number of NMM’s affiliated physicians who could provide services or preclude NMM’s from entering new hospitals. In addition, hospitals may attempt to enter into exclusive contracts for physician services, which would reduce access to certain populations of patients within the hospital.
NMM may have difficulty collecting payments from third-party payors in a timely manner.
NMM and its affiliated physician groups derive significant revenue from third-party payors, and delays in payment or audits leading to refunds to payors may adversely impact NMM’s net revenue. NMM assumes the financial risks relating to uncollectible and delayed payments. In particular, NMM and its affiliated physician groups rely on some key governmental payors. Governmental payors typically pay on a more extended payment cycle, which could result in NMM incurring expenses prior to receiving corresponding revenue. In the current healthcare environment, payors are continuing its efforts to control expenditures for healthcare, including proposals to revise coverage and reimbursement policies. NMM may experience difficulties in collecting revenue because third-party payors may seek to reduce or delay payment to which NMM believes it is entitled. If NMM and its affiliated physician groups are not paid fully and in a timely manner for such services or there is a finding that it was incorrectly paid, NMM’s revenues, cash flows and financial condition could be adversely affected.
Decreases in payor rates could adversely affect NMM.
Decreases in payor rates, either prospectively or retroactively, could have a significant adverse effect on NMM’s revenue, cash flow and results of operations. For example, during fiscal 2016, Health Net, Inc. reduced payor rates to its payees, retroactive to July 1, 2015 and LA Care reduced payor rates to its payees, retroactive to January 1, 2016.
NMM’s business model depends on numerous complex management information systems, and any failure to successfully maintain these systems or implement new systems could undermine NMM’s ability to receive ACO payments and otherwise materially harm NMM’s operations and result in potential violations of healthcare laws and regulations.
NMM depends on a complex, specialized, integrated management information system and standardized procedures for operational and financial information, as well as for NMM’s billing operations. NMM may be unable to enhance its existing management information systems or implement new management information systems where necessary. Additionally, NMM may experience unanticipated delays, complications or expenses in implementing, integrating and operating its systems. NMM’s management information systems may require modifications, improvements or replacements that may require both substantial expenditures as well as interruptions in operations. NMM’s ability to implement these systems is subject to the availability of information technology and skilled personnel to assist NMM in creating and implementing these systems. NMM’s failure to successfully implement and maintain all of its systems could undermine its ability to receive MSSP payments and otherwise have a material adverse effect on NMM’s business, results of operations and financial condition. Additionally, NMM’s failure to successfully operate its billing systems could lead to potential violations of healthcare laws and regulations.
| 89 |
From time to time NMM may be required to write-off intangible assets, such as goodwill, due to impairment.
NMM’s intangible assets are subject to annual impairment testing. Under current accounting standards, goodwill is tested for impairment on an annual basis and NMM may be subject to impairment losses as circumstances change after an acquisition. If NMM records an impairment loss related to NMM’s goodwill, it could have a material adverse effect on its results of operations for the year in which the impairment is recorded.
NMM currently derives 100% of its revenues in California and is vulnerable to changes in California healthcare laws and regulations.
NMM’s business and operations is located in one state, California. Any material changes by California with respect to strategy, taxation and economics of healthcare delivery, reimbursements, financial requirements or other aspects of regulation of the healthcare industry could have an adverse effect on NMM’s business, results of operations and financial condition.
A prolonged disruption of the capital and/or credit markets may adversely affect NMM’s future access to capital, NMM’s cost of capital and its ability to continue operations.
Volatility and disruption of the U.S. capital and credit markets may adversely affect NMM’s access to capital and/or increase its cost of capital. Should current economic and market conditions deteriorate, NMM’s ability to finance its ongoing operations and its expansion may be adversely affected, it may be unable to raise necessary funds, its cost of debt or equity capital may increase significantly and future access to capital markets may be adversely affected.
Uncertain or adverse economic conditions may have a negative impact on NMM’s industry, business, results of operations or financial position.
Uncertain or adverse economic conditions could have a negative effect on the fundamentals of NMM’s business, results of operations and/or financial position. These conditions could have a negative impact on NMM’s industry. There can be no assurance that NMM will not experience any material adverse effect on its business as a result of future economic conditions or that the actions of the U.S. Government, Federal Reserve or other governmental and regulatory bodies, for the purpose of stimulating the economy or financial markets will achieve its intended effect. Additionally, some of these actions may adversely affect financial institutions, capital providers, NMM’s customers or NMM’s financial condition, results of operations or the price of NMM’s securities. Potential consequences of the foregoing include:
| · | NMM’s ability to issue equity and/or borrow capital on terms and conditions that NMM finds acceptable, or at all, may be limited, which could limit NMM’s ability to access capital; |
| · | potential increased costs of borrowing capital if interest rates rise; |
| · | adverse terms imposed on NMM by any equity investor; |
| · | the possible impairment of some or all of the value of NMM’s goodwill and other intangible assets; and |
| · | the possibility that any then-existing lenders could refuse to fund any commitment to NMM or could fail, and NMM may not be able to replace or refinance the financing commitment of any such lender on satisfactory terms, or at all. |
| 90 |
Actual or perceived difficulties in the global capital and credit markets have adversely affected, and uncertain or adverse economic conditions may negatively affect, NMM’s business. Ongoing uncertain economic conditions may affect NMM’s financial performance or NMM’s ability to forecast its business with accuracy.
NMM’s operations and performance depend primarily on California and U.S. economic conditions and its impact on purchases of, or capitated rates for, NMM’s delivery of healthcare services. As a result of the global financial crisis that began in 2008, which was experienced on a broad and extensive scope and scale, and the last recession in the United States, general economic conditions deteriorated significantly, and, although the markets have improved significantly, the overall economic recovery since that time has been uneven. Declines in consumer and business confidence and private as well as government spending during and since the last recession, together with significant reductions in the availability and increases in the cost of credit and volatility in the capital and credit markets, as well as government budgeting, have adversely affected the business and economic environment in which NMM operates and can affect the profitability of NMM’s business. NMM’s business is significantly exposed to risks associated with government spending and private payor reimbursement rates. Economic conditions may remain uncertain for the foreseeable future. NMM believes that this general economic uncertainty may continue in future periods, as NMM’s patients, private payors and government payors alter their purchasing activities in response to the new economic reality, and, among other things, NMM’s patients may change or scale back healthcare spending, and private and government payors could reduce reimbursement rates. Additional consequences of such adverse effects could include the delay or cancellation of consumer spending for discretionary and non-reimbursed healthcare. Future disruption of the credit markets, increases in interest rates and/or sluggish economic growth in future periods could adversely affect NMM’s patients’ spending habits, private payors’ access to capital (which supports the continuation and expansion of its businesses) and governmental budgetary processes, and, in turn, could result in reduced revenue to NMM. The continuation or recurrence of any of these conditions may adversely affect NMM’s cash flow, results of operations and financial condition. This uncertainty may also affect NMM’s ability to prepare accurate financial forecasts or meet specific forecasted results. If NMM is unable to adequately respond to or forecast further changes in demand for healthcare services, NMM’s results of operations, financial condition and business prospects may be materially and adversely affected.
Many of NMM’s agreements with medical groups are relatively short term or may be terminated without cause by providing advance notice, and any such termination could have a material adverse effect on NMM’s financial results, operations and future business plans.
Many of NMM’s management services agreements are relatively short term or may be terminated without cause by providing advance notice. If these agreements are terminated before the end of its terms, at the end of its term or are not renewed, NMM would lose the revenue generated by those agreements. Any such terminations could have a material adverse effect on NMM’s results of operations, financial condition and future business plans.
NMM and its affiliated physicians, physician groups may be required to continue providing services following termination or renegotiation of certain agreements with health plans.
There are circumstances under federal and state law pursuant to which NMM’s affiliated physician groups could be obligated to continue to provide medical services to members in their care following a termination of their applicable risk agreement with health plans and termination of the receipt of payments thereunder. In certain cases, this obligation could require the physician group or IPA to provide care to such member following the bankruptcy or insolvency of a health plan. Accordingly, the obligations to provide medical services to NMM’s affiliated physician groups members (and the associated costs) may not terminate at the time the applicable agreement with the health plan terminates, and NMM’s affiliated physician groups may not be able to recover its cost of providing those services from the health plan, which could have a material adverse effect on NMM’s financial condition, results of operations, and/or cash flows.
If there is a change in accounting principles or the interpretation thereof by the FASB affecting consolidation of VIEs, it could impact NMM’s consolidation of total revenues derived from APC.
NMM’s financial statements are consolidated and include the accounts of NMM’s majority-owned subsidiaries and various non-owned affiliated physician groups that are VIEs, which consolidation is effectuated in accordance with applicable accounting rules. In the event of a change in accounting principles promulgated by FASB or in FASB’s interpretation of its principles, or if there were an adverse determination by a regulatory agency or a court or a change in state or federal law relating to the ability to maintain present agreements or arrangements with such physician groups, NMM may not be permitted to continue to consolidate the total revenues of such organizations.
| 91 |
Accounting rules require that under some circumstances the VIE consolidation model be applied when a reporting enterprise holds a variable interest (e.g., equity interests, debt obligations, certain management and service contracts) in a legal entity. Under this model, an enterprise must assess the entity in which it holds a variable interest to determine whether it meets the criteria to be consolidated as a VIE. If the entity is a VIE, the consolidation framework next identifies the party, if one exists, that possesses a controlling financial interest in a VIE, and requires that party to consolidate as the primary beneficiary. An enterprise’s determination of whether it has a controlling financial interest in a VIE requires that a qualitative determination be made, and is not solely based on voting rights.
If an enterprise determines the entity in which it holds a variable interest is not subject to the VIE guidance in ASC 810, the enterprise should apply the traditional voting control model (also outlined in ASC 810) which focuses on voting rights. In NMM’s case, the VIE consolidation model applies to NMM’s controlled, but not owned, physician affiliated entities. NMM’s determination regarding the consolidation of its affiliates could be challenged, which could have a material adverse effect on NMM’s operations.
The healthcare industry is complex and intensely regulated at the federal, state, and local levels and government authorities may determine that NMM has failed to comply with applicable laws or regulations.
As a company involved in providing healthcare services, NMM and its affiliated physician groups are subject to numerous federal, state and local laws and regulations. There are significant costs involved in complying with these laws and regulations. Moreover, if NMM is found to have violated any applicable laws or regulations, NMM could be subject to civil and/or criminal damages, fines, sanctions or penalties, including exclusion from participation in governmental healthcare programs, such as Medicare and Medicaid. NMM may also be required to change its method of operations. These consequences could be the result of current conduct or even conduct that occurred a number of years ago. NMM also could incur significant costs merely if it becomes the subject of an investigation or legal proceeding alleging a violation of these laws and regulations. NMM cannot predict whether a federal, state or local government will determine that NMM is not operating in accordance with law, or whether, when or how the laws will change in the future and impact its business. Any of these actions could have a material adverse effect on NMM’s business, financial condition and results of operations.
The following is a non-exhaustive list of some of the more significant healthcare laws and regulations that affect NMM:
| · | federal laws, including the federal False Claims Act, that provide for penalties against entities and individuals which knowingly or recklessly make claims to Medicare, Medicaid, and other governmental healthcare programs, as well as third-party payors, that contain or are based upon false or fraudulent information; |
| · | a provision of the Social Security Act, commonly referred to as the “Anti-Kickback Statute,” that prohibits the knowing and willful offering, payment, solicitation or receipt of any bribe, kickback, rebate or other remuneration, in cash or in kind, in return for the referral or recommendation of patients for items and services covered, in or in part, by federal healthcare programs such as Medicare and Medicaid; |
| · | a provision of the Social Security Act, commonly referred to as the Stark Law or physician self-referral law, that (subject to limited exceptions) prohibits physicians from referring Medicare patients to an entity for the provision of specific “designated health services” if the physician or a member of such physician’s immediate family has a direct or indirect financial relationship with the entity, and prohibits the entity from billing for services arising out of such prohibited referrals; |
| · | a provision of the Social Security Act that provides for criminal penalties on healthcare providers who fail to disclose known overpayments; |
| · | a provision of the Social Security Act that provides for civil monetary penalties on healthcare providers who fail to repay known overpayments within 60 days of identification or the date any corresponding cost report was due, if applicable, and also allows improper retention of known overpayments to serve as a basis for False Claims Act violations; |
| · | state law provisions pertaining to anti-kickback, self-referral and false claims issues, which typically are not limited to relationships involving governmental payors; |
| 92 |
| · | provisions of, and regulations relating to, HIPAA that provide penalties for knowingly and willfully executing a scheme or artifice to defraud a health-care benefit program or falsifying, concealing or covering up a material fact or making any material false, fictitious or fraudulent statement in connection with the delivery of or payment for healthcare benefits, items or services; |
| · | provisions of HIPAA and HITECH limiting how covered entities, business associates and business associate sub-contractors may use and disclose PHI and the security measures that must be taken in connection with protecting that information and related systems, as well as similar or more stringent state laws; |
| · | federal and state laws that provide penalties for providers for billing and receiving payment from a governmental healthcare program for services unless the services are medically necessary and reasonable, adequately and accurately documented, and billed using codes that accurately reflect the type and level of services rendered; |
| · | state laws that provide for financial solvency requirements relating to plan operations, plan-affiliate operations and transactions, plan-provider contractual relationships and provider-affiliate operations and transactions, such as California S.B. 260 (1999); |
| · | federal laws that provide for administrative sanctions, including civil monetary penalties for, among other violations, inappropriate billing of services to federal healthcare programs, payments by hospitals to physicians for reducing or limiting services to Medicare or Medicaid patients, or employing or contracting with individuals or entities who/which are excluded from participation in federal healthcare programs; |
| · | federal and state laws and policies that require healthcare providers to enroll in the Medicare and Medicaid programs before submitting any claims for services, to promptly report certain changes in its operations to the agencies that administer these programs, and to re-enroll in these programs when changes in direct or indirect ownership occur or in response to revalidation requests from Medicare and Medicaid; |
| · | state laws that prohibit general business entities from practicing medicine, controlling physicians’ medical decisions or engaging in certain practices, such as splitting fees with physicians; |
| · | state laws that require timely payment of claims, including California A.B. 1455 (1999) which imposes time limits for the payment of uncontested covered claims and required health care service plans to pay interest on uncontested claims not paid promptly within the required time period; |
| · | laws in some states that prohibit non-domiciled entities from owning and operating medical practices in its states; |
| · | provisions of the Social Security Act (emanating from the DRA) that require entities that make or receive annual Medicaid payments of $5 million or more from a single Medicaid program to provide its employees, contractors and agents with written policies and employee handbook materials on federal and state false claims acts and related statutes, that establish a new Medicaid Integrity Program designed to enhance federal and state efforts to detect Medicaid fraud, waste, and abuse, and that increase financial incentives for both states and individuals to bring fraud and abuse claims against healthcare companies; and |
| · | federal and state laws and regulations restricting the techniques that may be used to collect past due accounts from consumers, such as NMM’s patients, for services provided to the consumer. |
NMM cannot predict the effect that the ACA and its implementation, amendment, or repeal and replacement, may have on NMM’s business, results of operations or financial condition.
The continued implementation of provisions of the ACA, the adoption of new regulations thereunder and ongoing legal challenges create an uncertain environment for how the ACA may affect NMM’s business, results of operations and financial condition.
However, some of the reductions in Medicare spending, such as negative adjustments to the Medicare hospital inpatient and outpatient prospective payment system market basket updates and the incorporation of productivity adjustments to the Medicare program’s annual inflation updates, became effective starting in 2010. Although the expansion of health insurance coverage should increase revenues from providing care to previously uninsured individuals, many of these provisions of the ACA, as currently provided, will continue to become effective beyond 2017, and the impact of such expansion may be gradual and may not offset scheduled decreases in reimbursement.
| 93 |
On June 28, 2012, the U.S. Supreme Court upheld the constitutionality of the ACA, including the “individual mandate” provisions of the ACA that generally require all individuals to obtain healthcare insurance or pay a penalty. However, the U.S. Supreme Court also held that the provision of the ACA that authorized the Secretary of the HHS to penalize states that choose not to participate in the expansion of the Medicaid program by removing all of its existing Medicaid funding was unconstitutional. In response to the ruling, a number of U.S. governors opposed its state’s participation in the expanded Medicaid program, which resulted in the ACA not providing coverage to some low-income persons in those states. In addition, several bills have been, and are continuing to be, introduced in Congress to amend all or significant provisions of the ACA, or repeal and replace the ACA with another law.
The ACA changed how healthcare services are covered, delivered, and reimbursed. The net effect of the ACA on NMM’s business is subject to numerous variables, including the law’s complexity, lack of complete implementing regulations and interpretive guidance, gradual and potentially delayed implementation or possible amendment, as well as the uncertainty as to the extent to which states will choose to participate in the expanded Medicaid program.
The impact that changes in healthcare laws could have on NMM is uncertain but could be material.
Despite the enactment of the ACA and its being upheld by the U.S. Supreme Court as constitutional, continuing legal and political challenges to specific parts of the ACA have added uncertainty about the current state of healthcare laws in the United States. This uncertainty has intensified following the 2016 presidential election and the publicly announced intention of the leadership of the majority in the 115th Congress to “repeal and replace” the ACA, related Health Care Reform Acts and possibly other healthcare laws, and of the Administration to seek to have regulators amend or rescind certain regulations thereunder.
It is impossible to know what impact such efforts, assuming it is successful, will have on NMM. However, any changes in healthcare laws or regulations that reduce, curtail or eliminate payments, government-subsidized programs, government-sponsored programs, and/or the expansion of Medicare or Medicaid, among other actions, could have a material adverse effect on NMM’s business, results of operations and financial condition.
Just as the fate of the ACA is uncertain, so is the future of ACOs, which were established under the ACA to improve care and reduce costs. NMM operates an ACO and has been approved by CMS to operate an ACO under the NGACO Model. Under the MSSP and NGACO programs and pursuant to the Participation Agreement NMM has entered into with CMS for NMM’s NGACO Model, NMM’s ACO operations will always be subject to the nation’s healthcare laws, as amended, repealed or replaced from time to time.
It is impossible to know what impact such “repeal and replace” or similar efforts, assuming it is successful, will have on NMM. However, any changes in healthcare laws or regulations that reduce, curtail or eliminate payments, reimbursements, government-subsidized programs, government-sponsored programs, and/or the expansion of Medicare or Medicaid, among other actions, could have a material adverse effect on NMM’s business, results of operations and financial condition.
Providers in the healthcare industry are sometimes the subject of federal and state investigations, as well as payor audits.
Due to NMM’s affiliated physician groups’ participation in government and private healthcare programs, NMM may be involved in inquiries, reviews, audits and investigations by governmental agencies and private payors of NMM’s business practices, including assessments of NMM’s compliance with coding, billing and documentation requirements. Federal and state government agencies have active civil and criminal enforcement efforts that include investigations of healthcare companies, and its executives and managers. Under some circumstances, these investigations can also be initiated by private individuals under whistleblower provisions which may be incentivized by the possibility for private recoveries. The Deficit Reduction Act revised federal law to further encourage these federal, state and individually-initiated investigations against healthcare companies.
Responding to these audit and enforcement activities can be costly and disruptive to NMM’s business operations, even when the allegations are without merit. If NMM is subject to an audit or investigation and a finding is made that NMM or its affiliated physician groups were incorrectly reimbursed, it may be required to repay these agencies or private payors, or it may be subjected to pre-payment reviews, which can be time-consuming and result in non-payment or delayed payment for the services it provide. NMM also may be subject to other financial sanctions or be required to modify NMM’s operations.
| 94 |
Laws regulating the corporate practice of medicine could restrict the manner in which NMM is permitted to conduct its business and the failure to comply with such laws could subject NMM to penalties or require a corporate restructuring.
Some states have laws that prohibit business entities from practicing medicine, employing physicians to practice medicine, exercising control over medical decisions by physicians (also known collectively as the corporate practice of medicine) or engaging in some arrangements, such as fee-splitting, with physicians. In some states these prohibitions are expressly stated in a statute or regulation, while in other states the prohibition is a matter of judicial or regulatory interpretation. California is one of the states that prohibit the corporate practice of medicine.
In California, NMM and its affiliated physician groups operate by maintaining contracts with its affiliated physician groups which are each owned and operated by physicians and which employ or contract with additional physicians to provide physician services. Under these arrangements, NMM provides management services, receives a management fee for providing non-medical management services, does not represent that it offers medical services, and does not exercise influence or control over the practice of medicine by the physicians or the affiliated physician groups. In the event that any of these affiliated physician groups fails to comply with the management arrangement or any management arrangement is terminated and/or NMM is unable to enforce its contractual rights, or California law is interpreted to invalidate these arrangements, there could be a material adverse effect on NMM’s business, results of operations and financial condition.
NMM does not have a limited Knox-Keene license.
NMM does not hold a limited Knox-Keene license, which is a managed care plan license in California. If the DMHC were to determine that NMM or its affiliated physician groups has been inappropriately taking risk for institutional and professional services as a result of NMM’s various hospital and physician arrangements without having a limited Knox-Keene license, it may be required to obtain a limited Knox-Keene license to resolve such violations and could be subject to civil and criminal liability, any of which could have a material adverse effect on NMM’s business, results of operations and financial condition.
NMM’s revenue may be negatively impacted by the failure of its affiliated physicians to appropriately document services it provides.
NMM relies upon NMM’s affiliated physicians to appropriately and accurately complete necessary medical record documentation and assign appropriate reimbursement codes for its services. Reimbursement to NMM is conditioned upon, in part, NMM’s affiliated physicians providing the correct procedure and diagnosis codes and properly documenting the services themselves, including the level of service provided and the medical necessity for the services. If NMM’s affiliated physicians have provided incorrect or incomplete documentation or selected inaccurate reimbursement codes, this could result in nonpayment for services rendered or lead to allegations of billing fraud. This could subsequently lead to civil and criminal penalties, including exclusion from government healthcare programs, such as Medicare and Medicaid. In addition, third-party payors may disallow, in whole or in part, requests for reimbursement based on determinations that certain amounts are not covered, services provided were not medically necessary, or supporting documentation was not adequate. Retroactive adjustments may change amounts realized from third-party payors and result in recoupments or refund demands, affecting revenue already received.
Changes associated with reimbursement by third-party payors for NMM’s services may adversely affect NMM’s operating results and financial condition.
The medical services industry is undergoing significant changes with government and other third-party payors that are taking measures to reduce reimbursement rates or, in some cases, denying reimbursement altogether. There is no assurance that government or other third-party payors will continue to pay for the services provided by NMM’s affiliated medical groups. Furthermore, there has been, and continues to be, a great deal of discussion and debate about the repeal and replacement of existing government reimbursement programs, such as the ACA. As a result, the future of healthcare reimbursement programs is uncertain, making long-term business planning difficult and imprecise. The failure of government or other third party payors to cover adequately the medical services provided by NMM’s affiliated physician groups could have a material adverse effect on NMM’s business, results of operations and financial condition.
| 95 |
Compliance with federal and state privacy and information security laws is expensive, and NMM or its affiliated physician groups may be subject to government or private actions due to privacy and security breaches.
NMM and its affiliated physician groups must comply with numerous federal and state laws and regulations governing the collection, dissemination, access, use, security and confidentiality of PHI, including HIPAA and HITECH. As part of NMM and its affiliated physician groups medical record keeping, third-party billing, and other services, NMM collects and maintains PHI in paper and electronic format. Therefore, new privacy or security laws, whether implemented pursuant to federal or state action, could have a significant effect on the manner in which NMM handles healthcare-related data and communicates with payors. In addition, compliance with these standards could impose significant costs on NMM or limit NMM’s ability to offer services, thereby negatively impacting the business opportunities available to them. Despite NMM’s efforts to prevent security and privacy breaches, it may still occur. If any non-compliance with existing or new laws and regulations related to PHI results in privacy or security breaches, NMM could be subject to monetary fines, civil suits, civil penalties or even criminal sanctions.
As a result of the expanded scope of HIPAA through HITECH, NMM may incur significant costs in order to minimize the amount of “unsecured PHI” it handles and retains or to implement improved administrative, technical or physical safeguards to protect PHI. NMM may incur significant costs in order to demonstrate and document whether there is a low probability that PHI has been compromised in order to overcome the presumption that an impermissible use or disclosure of PHI results in a reportable breach. NMM may incur significant costs to notify the relevant individuals, government entities and, in some cases, the media, in the event of a breach and to provide appropriate remediation and monitoring to mitigate the possible damage done by any such breach.
Providers must be properly enrolled in governmental healthcare programs, such as Medicare and Medicaid, before it can receive reimbursement for providing services, and there may be delays in the enrollment process.
NMM’s affiliated physicians must enroll under the Medicare and Medicaid programs and for certain managed care and private insurance programs before NMM can receive reimbursement for services the physician renders to beneficiaries of those programs. The estimated time to receive approval for the enrollment is sometimes difficult to predict and, in recent years, the Medicare program carriers often have not issued these numbers to NMM’s affiliated physicians in a timely manner. These practices result in delayed reimbursement that may adversely affect NMM’s cash flow.
NMM and its affiliated physician groups may face malpractice and other lawsuits that may not be covered by insurance.
Malpractice lawsuits are common in the healthcare industry. The medical malpractice legal environment varies greatly by state. The status of tort reform, availability of non-economic damages or the presence or absence of other statutes, such as elder abuse or vulnerable adult statutes, influence the incidence and severity of malpractice litigation. NMM may also be subject to other types of lawsuits which may involve large claims and significant defense costs. Many states have joint and several liabilities for all healthcare providers who deliver care to a patient and are at least partially liable. As a result, if one healthcare provider is found liable for medical malpractice for the provision of care to a particular patient, all other healthcare providers who furnished care to that same patient, including possibly NMM’s affiliated physicians, may also share in the liability, which may be substantial.
NMM cannot be certain that its insurance coverage will be adequate to cover liabilities arising out of claims asserted against NMM, NMM’s affiliated professional organizations or NMM’s affiliated physicians, and NMM cannot provide assurance that any future liabilities will not have a material adverse impact on its results of operations, cash flows or financial position. Liabilities in excess of NMM’s insurance coverage, including coverage for professional liability and other claims, could have a material adverse effect on NMM’s business, financial condition, and results of operations. In addition, NMM’s professional liability insurance coverage generally must be renewed annually and may not continue to be available to NMM in future years at acceptable costs and on favorable terms.
| 96 |
NMM has established reserves for potential medical liability losses which are subject to inherent uncertainties and a deficiency in the established reserves may lead to a reduction in NMM’s net income.
NMM establishes reserves for estimates of IBNR due to contracted physicians, hospitals, and other professional providers and risk-pool liabilities. IBNR estimates are developed using actuarial methods and are based on many variables, including the utilization of health care services, historical payment patterns, cost trends, product mix, seasonality, changes in membership, and other factors. Many of the medical contracts are complex in nature and may be subject to differing interpretations regarding amounts due for the provision of various services. Such differing interpretations may not come to light until a substantial period of time has passed following the contract implementation. The inherent difficulty in interpreting contracts and the estimated level of necessary reserves could result in significant fluctuations in NMM’s estimates from period to period. It is possible that actual losses and related expenses may differ, perhaps substantially, from the reserve estimates reflected in NMM’s financial statements. If subsequent claims exceed NMM’s estimated reserves, NMM may be required to increase reserves, which would lead to a reduction in NMM’s assets or net income.
Litigation expenses may be material.
The defense of litigation, including fees of legal counsel, expert witnesses and related costs, is expensive and difficult to forecast accurately. In general, such costs are unrecoverable even if NMM ultimately prevails in litigation and could represent a significant portion of NMM’s limited capital resources. To defend lawsuits, it is also necessary for NMM to divert officers and other employees from its normal business functions to gather evidence, give testimony and otherwise support litigation efforts.
If NMM loses any material litigation, NMM could face material judgments or awards against them. An unfavorable resolution of one or more of the proceedings in which NMM is involved now or in the future could have a material adverse effect on NMM’s business, assets, cash flow and financial condition.
NMM may also in the future find it necessary to file lawsuits to recover damages or protect NMM’s interests. The cost of such litigation could also be significant and unrecoverable, which may also deter NMM from aggressively pursuing even legitimate claims.
NMM may be subject to litigation related to the agreements that NMM’s IPAs enter into with primary care physicians.
It is common in the medical services industry for primary care physicians to be affiliated with multiple IPAs. NMM IPAs often enter into agreements with physicians who are also affiliated with NMM’s competitors. However, some of NMM’s competitors at times enter into agreements with physicians that require the physician to provide services exclusively to that competitor. NMM’s IPAs often have no knowledge, and no way of knowing, whether a physician seeking to affiliate with the IPA is subject to an exclusivity agreement unless the physician informs the IPA of that agreement. NMM’s IPAs rely on the physicians seeking to affiliate with the IPA to determine whether it is able to enter into the proposed agreement. Competitors may in the future initiate lawsuits against NMM based in part on interference with such exclusivity agreements. An adverse outcome in one or more of such lawsuits could adversely affect NMM’s business, assets, cash flow and financial condition.
Changes in the rates or methods of Medicare reimbursements may adversely affect NMM’s operations.
In order to participate in the Medicare program, NMM must comply with stringent and often complex enrollment and reimbursement requirements. These programs generally provide for reimbursement on a fee-schedule basis rather than on a charge-related basis, meaning that generally NMM cannot increase its revenue by increasing the amount it charge for its services. To the extent that NMM’s costs increase, NMM may not be able to recover its increased costs from these programs and cost containment measures and market changes in non-governmental insurance plans have generally restricted NMM’s ability to recover, or shift to non-governmental payors, these increased costs. In attempts to limit federal and state spending, there have been, and NMM expects that there will continue to be, a number of proposals to limit or reduce Medicare reimbursement for various services. In April of 2015, MACRA was signed into law, which made numerous changes to Medicare, Medicaid, and other healthcare related programs. These changes include new systems for establishing the annual updates to payment rates for physicians’ services in Medicare. NMM’s business may be significantly and adversely affected by MACRA and any changes in reimbursement policies and other legislative initiatives aimed at or having the effect of reducing healthcare costs associated with Medicare, TRICARE (which provides civilian health benefits for U.S. Armed Forces military personnel, military retirees, and its dependents) and other government healthcare programs.
| 97 |
NMM’s business also could be adversely affected by reductions in, or limitations of, reimbursement amounts or rates under these government programs, reductions in funding of these programs or elimination of coverage for certain individuals or treatments under these programs.
If NMM or its affiliated physician groups inadvertently employs or contracts with an excluded person, NMM may face government sanctions.
Individuals and entities can be excluded from participating in the Medicare and Medicaid programs for violating certain laws and regulations, or for other reasons such as the loss of a license in any state, even if the individual retains other licensure. This means that it (and all others) are prohibited from receiving payment for its services rendered to Medicare or Medicaid beneficiaries, and if the excluded individual is a physician, all services ordered (not just provided) by such physician are also non-covered and non-payable. Entities which employ or contract with excluded individuals are prohibited from billing the Medicare or Medicaid programs for the excluded individual’s services, and are subject to civil monetary penalties if it does. The OIG maintains a list of excluded individuals and entities. Although NMM has instituted policies and procedures through its compliance program to minimize the risks, there can be no assurance that NMM and its affiliated physician groups will not inadvertently hire or contract with an excluded person, or that any of NMM’s current employees or contractors will not become excluded in the future without NMM’s knowledge. If this occurs, NMM may be subject to substantial repayments and civil penalties, and the hospitals at which NMM and its affiliated physician groups furnishes services also may be subject to repayments and sanctions, for which it may seek recovery from NMM.
NMM may be impacted by eligibility changes to government and private insurance programs.
Due to potential decreased availability of healthcare through private employers, the number of patients who are uninsured or participate in governmental programs may increase. A shift in payor mix from managed care and other private payors to government payors or the uninsured may result in a reduction in NMM’s rates of reimbursement or an increase in NMM’s uncollectible receivables or uncompensated care, with a corresponding decrease in NMM’s net revenue. Changes in the eligibility requirements for governmental programs also could increase the number of patients who participate in such programs or the number of uninsured patients. Even for those patients who remain with private insurance, changes in those programs could increase patient responsibility amounts, resulting in a greater risk for NMM of uncollectible receivables. These factors and events could have a material adverse effect on NMM’s business, results of operations and financial condition.
If NMM is unable to effectively adapt to changes in the healthcare industry, including changes to laws and regulations regarding or affecting healthcare reform or the healthcare industry, NMM’s business may be harmed.
Due to the importance of the healthcare industry in the lives of all Americans, federal, state, and local legislative bodies frequently pass legislation and promulgate regulations relating to healthcare reform or that affect the healthcare industry. As has been the trend in recent years, it is reasonable to assume that there will continue to be increased federal oversight and regulation of the healthcare industry in the future. NMM cannot assure its stockholders as to the ultimate content, timing or effect of any new healthcare legislation or regulations, nor is it possible at this time to estimate the impact of potential new legislation or regulations on NMM’s business. It is possible that future legislation enacted by Congress or state legislatures, or regulations promulgated by regulatory authorities at the Federal or state level, could adversely affect NMM’s business. It is possible that the changes to the Medicare or other governmental healthcare program reimbursements may serve as precedent to possible changes in other payors’ reimbursement policies in a manner averse to NMM. Similarly, changes in private payor reimbursements could lead to adverse changes in Medicare and other governmental healthcare programs which could have a material adverse effect on NMM’s business, financial condition and results of operations.
| 98 |
NMM may incur significant costs to adopt certain provisions under HITECH.
HITECH was enacted into law on February 17, 2009 as part of the American Recovery and Reinvestment Act of 2009. Among the many provisions of HITECH are those relating to the implementation and use of certified EHR. NMM’s patient medical records are maintained and under the custodianship of NMM’s affiliated physicians and physician groups. However, to determine to adopt certain EHRs, or comply with any related provisions of HITECH, NMM may incur significant costs which could have a material adverse effect on NMM’s business operations and financial position.
The healthcare industry is becoming increasingly reliant on use of technology.
The role of technology is greatly increasing in the delivery of healthcare, which provides risk to traditional physician-driven healthcare delivery companies such as NMM. NMM needs to understand and integrate with electronic health records, databases, cloud-based billing systems and many other technology applications in the delivery of NMM’s services. Additionally, consumers are using mobile applications and care and cost research in selecting and usage of healthcare services. NMM relies on employees and third parties with technology knowledge and expertise and could be at risk if resources are not properly established, maintained or secured.
NMM may be exposed to cybersecurity risks.
While NMM has not experienced any cybersecurity incidents, the nature of NMM’s business and the requirements of healthcare privacy laws such as HIPAA and HITECH, impose significant obligations on NMM and its affiliated physician groups to maintain the privacy and protection of patient medical information. Any cybersecurity incident could expose NMM and its affiliated physician groups to violations of HIPAA and/or HITECH that, even unintended, could cause significant financial exposure to NMM in the form of fines and costs of remediation of any such incident.
| 99 |
CAUTIONARY STATEMENT REGARDING FORWARD-LOOKING STATEMENTS
This joint proxy statement/prospectus and other documents incorporated by reference into this joint proxy statement/prospectus contain forward-looking statements within the meaning of the safe harbor provisions of the Private Securities Litigation Reform Act of 1995. Forward-looking statements may be identified by the use of forward-looking terms such as “anticipates,” “assumes,” “believes,” “can,” “could,” “estimates,” “expects,” “forecasts,” “guides,” “intends,” “is confident that,” “may,” “plans,” “seeks,” “projects,” “targets,” and “would” or the negative of such terms or other variations on such terms or comparable terminology. Such forward-looking statements include, but are not limited to, statements about the benefits of the proposed Merger between ApolloMed and NMM including future financial and operating results, ApolloMed’s plans post-Merger, objectives, expectations and intentions, the expected timing of completion of the Merger and other statements that are not historical facts. Such statements are based upon the current beliefs and expectations of the respective managements of ApolloMed and NMM and are subject to significant risks and uncertainties that could cause actual outcomes and results to differ materially. Important factors that could cause actual results to differ materially from those indicated by such forward-looking statements include, without limitation, the risks and uncertainties set forth under the section entitled “RISK FACTORS” beginning on page 44 of this joint proxy statement/prospectus. These risks and uncertainties include, but are not limited to:
| · | the occurrence of any event, change or other circumstances that could give rise to the termination of the Merger Agreement; |
| · | the inability to complete the Merger due to the failure to obtain stockholder approval or governmental or regulatory clearances or the failure to satisfy other conditions to the closing of the Merger or for any other reason; |
| · | legal or regulatory proceedings or other matters that affect the timing or ability to complete the Merger as contemplated; |
| · | the risk that the proposed Merger disrupts current plans and operations; |
| · | fluctuations in the market value of ApolloMed common stock; |
| · | the effects of the Merger on ApolloMed’s and NMM’s financial results; |
| · | disruption from the Merger making it difficult to maintain business and operational relationships; |
| · | diversion of management time on issues related to the Merger; |
| · | the risk that the businesses will not be integrated successfully, or that the integration will be more costly or more time consuming and complex than anticipated; |
| · | the risk that synergies anticipated to be realized from the Merger may not be fully realized or may take longer to realize than expected; |
| · | adverse developments in general market, business, economic, labor, regulatory and political conditions; |
| · | the amount of any costs, fees, expenses, impairments and charges related to the Merger; |
| · | the uncertainty regarding the adequacy of ApolloMed’s and NMM’s liquidity to pursue its business objectives; |
| · | the impact of any outbreak or escalation of hostilities on a national, regional or international basis, acts of terrorism or natural disasters; and |
| · | the impact of any change to applicable laws and regulations affecting domestic and foreign operations, including those relating to trade, monetary and fiscal policies, taxes, price controls, regulatory approval of new products, licensing and healthcare reform. |
| 100 |
For a further list and description of such risks and uncertainties, see “RISK FACTORS” beginning on page 44, “INFORMATION ABOUT APOLLOMED — ApolloMed Management’s Discussion and Analysis of Financial Condition and Results of Operations” and “INFORMATION ABOUT NMM — NMM Management’s Discussion and Analysis of Financial Condition and Results of Operations” of this joint proxy statement/prospectus. ApolloMed and NMM do not undertake any obligation to update or revise any forward-looking statements, whether as a result of new information, future events or otherwise, except as required by law. You are cautioned not to place undue reliance on these forward-looking statements, because, while the respective managements of ApolloMed and NMM believe the assumptions on which the forward-looking statements are based are reasonable, there can be no assurance that these forward-looking statements will prove to be accurate. This cautionary statement is applicable to all forward-looking statements contained in this joint proxy statement/prospectus.
ApolloMed was incorporated in the State of Delaware on November 1, 1985 under the name McKinnely Investment, Inc. On November 5, 1986 McKinnely Investment, Inc. changed its name to Acculine Industries, Incorporated and Acculine Industries, Incorporated changed its name to Siclone Industries, Incorporated on May 24, 1988. On July 3, 2008, Apollo Medical Holdings, Inc. merged into Siclone Industries, Incorporated and Siclone Industries, Incorporated, as the surviving entity from the merger, simultaneously changed its name to Apollo Medical Holdings, Inc.
ApolloMed is a physician-centric, integrated population health management company working to provide coordinated outcomes-based medical care in a cost-effective manner. Led by a management team with over a decade of experience, ApolloMed has built a company and culture that is focused on physicians providing high-quality medical care, population health management and care coordination for patients, particularly senior patients and patients with multiple chronic conditions. ApolloMed believes it is well-positioned to take advantage of changes in the rapidly evolving U.S. healthcare industry, as there is a growing national movement towards more results-oriented healthcare centered on the triple aim of patient satisfaction, high-quality care and cost efficiency.
ApolloMed’s common stock is currently quoted on OTC Pink and traded under the symbol “AMEH.” On December 21, 2016, the last full trading day before the announcement of the Merger, the last reported sale price of ApolloMed common stock was $3.99 per share, and, on [·], 2017, the latest practicable date prior to the date of this joint proxy statement/prospectus, the last reported sale price of ApolloMed common stock was $[·] per share. ApolloMed has applied for listing of its common stock on the NASDAQ Global Market effective as of the closing of the Merger.
ApolloMed’s principal executive offices are located at 700 N. Brand Blvd., Suite 1400, Glendale, CA 91203, its telephone number is (818) 396-8050, and its website is www.apollomed.net. This website is an inactive textual reference only and not an active hyperlink. The information on or that can be accessed through ApolloMed’s website is specifically not incorporated by reference into this joint proxy statement/prospectus, and is not a part of this joint proxy statement/prospectus.
Additional information about ApolloMed can be found in the sections titled “INFORMATION ABOUT APOLLOMED — Overview” beginning on page 212 and “INFORMATION ABOUT APOLLOMED — ApolloMed Management’s Discussion and Analysis of Financial Condition and Results of Operations” beginning on page 240 and ApolloMed’s financial statements included elsewhere in this joint proxy statement/prospectus.
Apollo Acquisition Corp. is a wholly owned subsidiary of ApolloMed that was formed in California on December 13, 2016, solely for the purpose of entering into the Merger Agreement and affecting the Merger and the other transactions contemplated by the Merger Agreement. Merger Sub is not engaged in any business and has no material assets. Its principal executive offices have the same address and telephone number as ApolloMed set forth above.
Network Medical Management, Inc.
Network Medical Management, Inc. is a California corporation formed in 1994. NMM, together with its subsidiaries and affiliated physician groups, is a patient- and physician-focused, integrated health care delivery and management company with 23 years of providing coordinated, outcomes-based medical care in a cost-effective manner.
Through capitation agreements with leading health plans, NMM is responsible for coordinating the care for over 600,000 covered patients in southern and central California through a network of more than 10 IPAs with approximately 4,000 contracted physicians. These covered patients are comprised of managed care members whose health coverage is provided through their employer or who have individually acquired health coverage directly from a health plan or as a result of their eligibility for Medicaid or Medicare benefits.
| 101 |
The patients of NMM’s affiliated physician groups and IPAs benefit from an integrated approach to medical care that places the physician at the center of patient care. NMM manages the delivery of healthcare services to patients via a network of affiliated physician groups and other network primary care physicians, network hospitals, and affiliated group and network specialists. Together with case managers, registered nurses and other care coordinators, these medical professionals utilize a comprehensive data analysis engine, sophisticated risk management techniques and clinical protocols to provide high-quality, cost effective care to NMM’s managed members. NMM monitors certain control metrics, such as the number of inpatient acute bed days per 1,000 patients and hospital readmission rates, as they are contributors to quality clinical outcomes and financial performance. Additionally, NMM closely monitors the number of managed care members who have enrolled with an NMM affiliated physician group as their primary care physicians in an effort to identify changes or trends with respect to its commercial, senior and Medicaid payer classifications.
NMM is headquartered in, and primarily operates from, Los Angeles County, California.
NMM’s principal executive offices are located at 1668 S. Garfield Avenue, 3rd Floor, Alhambra, California 91801, its telephone number is (626) 282-0288 and its website is www.nmm.cc. This website is an inactive textual reference only and not an active hyperlink. The information on or that can be accessed through NMM’s website is specifically not incorporated by reference into this joint proxy statement/prospectus, and is not a part of this joint proxy statement/prospectus.
Additional information about NMM can be found in the sections titled “INFORMATION ABOUT NMM ” beginning on page 263 and “INFORMATION ABOUT NMM — NMM Management’s Discussion and Analysis of Financial Condition and Results of Operations” beginning on page 285 and NMM’s financial statements included elsewhere in this joint proxy statement/prospectus.
Post-Merger Organizational Structure
The following is an organizational chart showing the anticipated intercorporate relationships of ApolloMed and NMM immediately following the completion of the Merger:
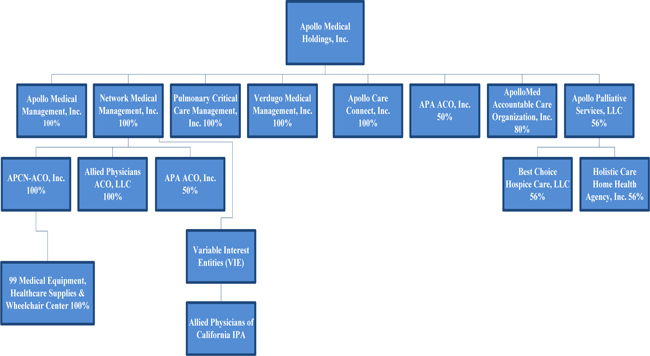
| 102 |
THE SPECIAL MEETING OF APOLLOMED STOCKHOLDERS
This section contains information for ApolloMed’s stockholders regarding the special meeting of ApolloMed stockholders that has been called to consider the approval of the ApolloMed Merger Proposal, the Board Classification Proposal, each of the directors in the Election of Directors Proposal, the ApolloMed Compensation Proposal and the ApolloMed Adjournment Proposal.
ApolloMed is furnishing this joint proxy statement/prospectus to the holders of ApolloMed capital stock as of the record date in connection with the solicitation of proxies by the ApolloMed board of directors for use at the ApolloMed special meeting of stockholders and any adjournment or postponement of the special meeting.
The ApolloMed special meeting of stockholders will be held on [●], 2017, at [●][a.m.][p.m.], Pacific Standard Time, at 700 N. Brand Blvd., Suite 1400, Glendale, California 91203.
Purpose of the ApolloMed Special Meeting
At the ApolloMed special meeting, ApolloMed stockholders will be asked to consider and vote upon the following matters:
(1) The ApolloMed Merger Proposal
(2) The Board Classification Proposal
(3) The Election of Directors Proposal;
(4) The ApolloMed Compensation Proposal; and
(5) The ApolloMed Adjournment Proposal.
ApolloMed stockholders also will consider and act on any other matters as may properly come before the ApolloMed special meeting or any adjournment or postponement of the meeting, including any procedural matters incident to the conduct of the meeting.
Recommendation of the ApolloMed Board of Directors
The ApolloMed board of directors has determined that it is advisable and in the best interest of ApolloMed and its stockholders to enter into the Merger Agreement and the ApolloMed board of directors has authorized and approved the terms of the Merger Agreement and the transactions contemplated thereby. Certain factors considered by the ApolloMed board of directors in reaching its decision to adopt and approve the Merger Agreement and the Merger can be found in the section of this joint proxy statement/prospectus entitled “THE MERGER — ApolloMed Reasons for the Merger” beginning on page 128.
The ApolloMed board of directors recommends that ApolloMed stockholders vote “FOR” the ApolloMed Merger Proposal, “FOR” the Board Classification Proposal, “FOR” each of the directors in the Election of Directors Proposal, “FOR” the ApolloMed Compensation Proposal and “FOR” the ApolloMed Adjournment Proposal.
ApolloMed Record Date and Quorum
The ApolloMed board of directors has fixed as of the close of business [●], 2017 as the record date for the ApolloMed special meeting. Only the holders of record of shares of ApolloMed common stock, Series A preferred stock and Series B preferred stock as of the close of business on the ApolloMed record date are entitled to receive notice of and to vote at the ApolloMed special meeting or at any postponement or adjournment of the ApolloMed special meeting.
As of the ApolloMed record date, there were [●] shares of ApolloMed common stock, [●] shares of Series A preferred stock and [●] shares of Series B preferred stock outstanding and entitled to vote at the ApolloMed special meeting held by [●] record holders. Each share of ApolloMed common stock entitles the holder to one vote at the ApolloMed special meeting on each proposal to be considered at the ApolloMed special meeting. Holders of shares of Series A preferred stock and Series B preferred stock vote with holders of shares of common stock as one class, on an as-converted basis. Each share of Series A preferred stock and Series B preferred stock entitles the holder to one vote at the ApolloMed special meeting on each proposal to be considered at the ApolloMed special meeting. As of the ApolloMed record date all the shares of Series A preferred stock and Series B preferred stock were held by NMM.
| 103 |
Pursuant to the ApolloMed Bylaws, the presence of holders of a majority of all the shares of ApolloMed stock entitled to vote at the special meeting is necessary to constitute a quorum, unless or except to the extent that the presence of a larger number may be required by law.
In the absence of a quorum, the chair of the meeting or the holders of a majority of the shares of ApolloMed stock entitled to vote who are present, in person or by proxy, may adjourn the meeting to another place, date, and time. As of the record date for the special meeting, [●] shares of ApolloMed’s common stock (on an as-converted basis), would be required to achieve a quorum.
At the close of business on the ApolloMed record date, directors and executive officers of ApolloMed and their affiliates were entitled to vote [●] shares of ApolloMed common stock (on an as-converted basis), or approximately [●]% of the issued and outstanding shares of ApolloMed common stock (on an as-converted basis) on that date. ApolloMed currently expects that the ApolloMed directors and executive officers will vote their shares of ApolloMed common stock in favor of the proposed proposals, although none of them is obligated to do so. In addition, on the ApolloMed record date, NMM was entitled to vote [●] shares of ApolloMed common stock (on an as-converted basis), or approximately [●]% of the issued and outstanding shares of ApolloMed common stock (on an as-converted basis) on that date. ApolloMed currently expects that NMM will vote its shares of ApolloMed common stock in favor of the proposals although NMM is not obligated to do so.
In accordance with Delaware law, a list of stockholders entitled to vote at the meeting will be available at the meeting, and for 10 days prior to the meeting, at ApolloMed’s offices, 700 N. Brand Blvd., Suite 1400, Glendale, CA 91203, between the hours of 9:00 a.m. and 5:00 p.m., Pacific Standard Time.
Assuming a quorum is present, approval of the ApolloMed Merger Proposal, the Board Classification Proposal, and each of the directors in the Election of Directors Proposal requires the affirmative vote of (i) a majority of the shares of ApolloMed common stock, Series A preferred stock and Series B preferred stock, voting together as one class on an as-converted basis, and (ii) a majority of the shares of ApolloMed common stock, Series A preferred stock and Series B preferred stock, voting together as one class on an as-converted basis, not owned by NMM. Approval of each of the ApolloMed Compensation Proposal and approval of the ApolloMed Adjournment Proposal will require the affirmative vote of a majority of the shares of ApolloMed capital stock entitled to vote present in person or represented by proxy at the ApolloMed special meeting.
Each of the ApolloMed Merger Proposal, the Board Classification Proposal and each of the directors in the Election of Directors Proposal are all conditioned on each other. The ApolloMed Compensation Proposal and the ApolloMed Adjournment Proposal are not conditioned on any other proposal.
Abstentions, Failure to Vote and Broker Non-Votes
If you are an ApolloMed stockholder and mark “ABSTAIN” on your proxy with respect to any of the proposals, your proxy will be counted toward the vote total for such proposal and will have the same effect as an “AGAINST” vote. Abstentions will be considered present for the purpose of determining the presence of a quorum.
If you are an ApolloMed stockholder of record and fail to submit a proxy card or vote at the special meeting, your shares will not be counted toward the total vote and will have no effect on the ApolloMed Compensation Proposal and the ApolloMed Adjournment Proposal but will be considered a vote “AGAINST” the ApolloMed Merger Proposal, the Board Classification Proposal and each of the directors in the Election of Directors Proposal. If you fail to submit a proxy card or vote at the special meeting, your shares will not be counted for purposes of determining a quorum.
Banks, brokers and other nominees that hold their customers’ shares in “street name” may not vote their customers’ shares on “non-routine” matters without instructions from their customers. As it is expected that each proposal is considered “non-routine,” such organizations do not have discretion to vote on any of the proposals. As a result, if you fail to provide your bank, broker or other nominee with any instructions regarding how to vote your shares of ApolloMed capital stock, your shares will be counted for purposes of determining a quorum but will be considered a vote “AGAINST” the ApolloMed Merger Proposal, the Board Classification Proposal and each of the directors in the Election of Directors Proposal. For the ApolloMed Compensation Proposal and the ApolloMed Adjournment Proposal, broker non-votes will not be counted toward the total vote and will have no effect.
| 104 |
Whether or not you plan to attend the ApolloMed special meeting in person, you should submit your proxy as soon as possible. If you own shares of ApolloMed common stock, Series A preferred stock or Series B preferred stock in your own name, you are an owner or holder of record. This means that you may use the enclosed proxy card or the Internet or telephone voting options to tell the persons named as proxies how to vote your shares of ApolloMed capital stock. You may vote your shares of ApolloMed capital stock held of record in any of the following ways:
In Person — To vote in person, come to the ApolloMed special meeting and you will be able to vote by ballot. To ensure that your shares of ApolloMed capital stock are voted at the ApolloMed special meeting, the ApolloMed board of directors recommends that you submit a proxy even if you plan to attend the ApolloMed special meeting.
By Mail — To vote using the enclosed proxy card, simply complete, sign and date the enclosed proxy card and return it promptly in the enclosed return envelope. If you return your signed proxy card to ApolloMed before the ApolloMed special meeting, the persons named as proxies will vote your shares of ApolloMed capital stock as you direct.
By Telephone — To vote by telephone, dial the toll free telephone number located on the enclosed proxy card using a touch-tone phone and follow the recorded instructions. You will be asked to provide ApolloMed number and control number from the enclosed proxy card.
By Internet — To vote over the Internet, go to the web address identified on the enclosed proxy card to complete an electronic proxy card. You will be asked to provide ApolloMed number and control number from the enclosed proxy card.
The telephone and Internet voting procedures are designed to authenticate stockholders’ identities, to allow stockholders to vote their shares, and to confirm that their instructions have been recorded properly. Submitting a proxy will not affect your right to vote in person if you decide to attend the ApolloMed special meeting.
The ApolloMed board of directors has appointed Warren Hosseinion and Gary Augusta to serve as proxies for the ApolloMed special meeting.
If a proxy card is signed and returned without an indication as to how the shares of ApolloMed capital stock represented by the proxy are to be voted with regard to a particular proposal, the ApolloMed capital stock represented by the proxy will be voted “FOR” each such proposal. As of the date of this joint proxy statement/prospectus, ApolloMed has no knowledge of any business that will be presented for consideration at the ApolloMed special meeting and which would be required to be set forth in this joint proxy statement/prospectus other than the matters set forth in the accompanying Notice of Special Meeting of Stockholders of ApolloMed. In accordance with the ApolloMed Bylaws and Delaware law, business transacted at the ApolloMed special meeting will be limited to those matters set forth in such notice.
Your vote as an ApolloMed stockholder is very important. Please submit your proxy as soon as possible, whether or not you plan to attend the ApolloMed special meeting in person.
If you are an ApolloMed stockholder and your shares are held in “street name” by a broker, bank or other nominee, you will receive instructions from your bank, brokerage firm or other nominee that you must follow in order to have your shares of ApolloMed capital stock voted. Those instructions will identify which of the above choices are available to you in order to have your shares voted.
You may not vote shares held in “street name” by returning a proxy card directly to ApolloMed or by voting in person at the ApolloMed special meeting unless you provide a “legal proxy,” which you must obtain from your broker, bank or other nominee. Further, brokers, banks or other nominees who hold shares of ApolloMed capital stock on behalf of their customers may not give a proxy to ApolloMed to vote those shares with respect to any of the proposals without specific instructions from their customers, as brokers, banks and other nominees do not have discretionary voting power on these matters. Therefore, if you are an ApolloMed stockholder and you do not instruct your broker, bank or other nominee on how to vote your shares during the ApolloMed special meeting, it will have the same effect as described above under “— Abstentions and Broker Non-Votes.”
| 105 |
Revocation of Proxies and Voting Instructions
If your shares of ApolloMed capital stock are registered in your own name, you may revoke your proxy in one of the following ways by:
| · | Attending the ApolloMed special meeting and voting in person. Your attendance at the ApolloMed special meeting will not by itself revoke a proxy. You must vote your shares by ballot at the ApolloMed special meeting to revoke your proxy; |
| · | Voting again by telephone or over the Internet (only your latest telephone or Internet vote submitted prior to the ApolloMed special meeting will be counted); |
| · | Completing and submitting a new valid proxy card bearing a later date; or |
| · | Sending written notice of revocation to ApolloMed at Apollo Medical Holdings, Inc., Attn: Secretary, 700 N. Brand Blvd., Suite 1400, Glendale, California 91203, which notice must be received before [●], Eastern Time, on [●], 2017. |
If your shares of ApolloMed capital stock are held in “street name”, your bank, broker or other nominee should provide instructions explaining how you may change or revoke your voting instructions.
ApolloMed will have a representative of Broadridge Financial Solutions appointed as the inspector of election for the ApolloMed special meeting to tabulate the affirmative and negative votes, broker non-votes and abstentions.
The cost of solicitation of proxies from ApolloMed stockholders will be borne by ApolloMed. In addition to solicitation by use of the mail, proxies may be solicited by directors, officers and employees of ApolloMed in person or by telephone, telegram or other means of communication. These directors, officers and employees will not receive additional compensation for their efforts but will be reimbursed for reasonable out-of-pocket expenses they incur in connection with the solicitation. ApolloMed will reimburse brokerage firms and other custodians, nominees and fiduciaries for their reasonable out-of-pocket expenses incurred in forwarding of solicitation materials to the beneficial owners of ApolloMed capital stock and collecting voting instructions.
If you need assistance in completing your proxy card or have questions regarding the various voting options with respect to the ApolloMed special meeting, please contact:
Apollo Medical Holdings, Inc.
Attn: Secretary
700 N. Brand Blvd., Suite 1400,
Glendale, California 91203
(818) 396-8050
| 106 |
PROPOSALS SUBMITTED TO APOLLOMED STOCKHOLDERS
APOLLOMED PROPOSAL 1 — APPROVAL OF THE APOLLOMED MERGER PROPOSAL
As discussed in this joint proxy statement/prospectus, ApolloMed is asking its stockholders to adopt and approve the ApolloMed Merger Proposal, which includes an approval of the Merger Agreement and the Merger and the other transactions contemplated thereby, including the issuance of shares of ApolloMed common stock and warrants in connection therewith.
For a summary of and detailed information regarding this proposal, see the information about the Merger Agreement and the Merger elsewhere in this joint proxy statement/prospectus, including the information set forth in sections entitled “THE MERGER” beginning on page 120 and “THE MERGER AGREEMENT” beginning on page 158. A copy of the Merger Agreement is attached as Annex A to this joint proxy statement/prospectus and incorporated herein by reference. You are urged to read carefully this joint proxy statement/prospectus and the Merger Agreement attached hereto in their entirety before voting on this proposal.
Under the terms of the Merger Agreement, Merger Sub will merge with and into NMM, with NMM becoming a wholly-owned subsidiary of ApolloMed. The Merger has been structured to qualify for federal income tax purposes as a tax-deferred reorganization under the provisions of Section 368(a) of the Internal Revenue Code of 1986.
Pursuant to the Merger Agreement, at the Effective Time, each issued and outstanding share of NMM common stock will be converted into the right to receive such number of fully paid and nonassessable ApolloMed shares of common stock that results in the NMM shareholders having a right to receive (A) an aggregate number of shares of ApolloMed common stock that represents 82% of the total issued and outstanding shares of ApolloMed common stock immediately following the Effective Time, assuming there are no NMM dissenting shareholder interests as of the Effective Time, calculated in accordance with the Merger Agreement (see “THE MERGER AGREEMENT – Effects of Merger; Merger Consideration” beginning on page 159), plus (B) an aggregate of 2,566,666 shares of ApolloMed common stock, assuming there are no NMM dissenting shareholder interests as of the Effective Time. In addition, each NMM shareholder shall be entitled to receive such shareholder’s pro rata portion of (i) warrants to purchase an aggregate of 850,000 shares of ApolloMed common stock, exercisable at $11.00 per share and (ii) warrants to purchase an aggregate of 900,000 shares of ApolloMed common stock, exercisable at $10.00 per share. At the Effective Time, pre-Merger ApolloMed stockholders will continue to own and hold their existing shares of ApolloMed common stock. At the Effective Time, ApolloMed will hold back the Holdback Shares to secure certain indemnification rights of ApolloMed and its affiliates under the Merger Agreement. Separately, indemnification of pre-Merger NMM shareholders under the Merger Agreement, if any, will be made by the issuance by ApolloMed to pre-Merger NMM shareholders of new additional ApolloMed shares of common stock (capped at the same number of shares of ApolloMed common stock as the Holdback Shares).
The terms of, and reasons for and other aspects of the Merger Agreement, the Merger and the issuance of shares of ApolloMed common stock and warrants pursuant to the Merger Agreement are described in detail elsewhere in this joint proxy statement/prospectus.
Required Vote
Assuming a quorum is present, approval of the ApolloMed Merger Proposal requires the affirmative vote of (i) a majority of the shares of ApolloMed common stock, Series A preferred stock and Series B preferred stock, voting together as one class on an as-converted basis, and (ii) a majority of the shares of ApolloMed common stock, Series A preferred stock and Series B preferred stock, voting together as one class on an as-converted basis, not owned by NMM.
Each of the ApolloMed Merger Proposal, the Board Classification Proposal and each of the directors in the Election of Directors Proposal are all conditioned on each other. The Compensation Proposal and the ApolloMed Adjournment Proposal are not conditioned on any other proposal.
Recommendation of the ApolloMed Board of Directors
THE APOLLOMED BOARD OF DIRECTORS RECOMMENDS THAT APOLLOMED STOCKHOLDERS VOTE “FOR” THE APOLLOMED MERGER PROPOSAL
| 107 |
APOLLOMED PROPOSAL 2 — APPROVAL OF THE BOARD CLASSIFICATION PROPOSAL
General
The Board Classification Proposal will only be presented to the special meeting of ApolloMed if the ApolloMed Merger Proposal is approved.
After careful consideration, ApolloMed’s board of directors consented to approve, and to recommend to its stockholders to approve, if the ApolloMed Merger Proposal is approved, a proposal to amend the ApolloMed Charter and ApolloMed Bylaws to classify ApolloMed’s board of directors into three classes of directors.
ApolloMed currently has a declassified board, which means that pursuant to the ApolloMed Bylaws, ApolloMed’s directors must stand for election each year at ApolloMed’s annual stockholder meeting. If adopted, this proposal would approve the amendment to the ApolloMed Charter as set forth in Annex E and the ApolloMed Bylaws as set forth in Annex F to divide ApolloMed’s directors into three classes, with the terms of office of one class expiring each year. Class I would hold office initially for a term expiring at the first annual meeting of stockholders after effectiveness of the Board Classification Proposal; Class II would hold office initially for a term expiring at the second annual meeting of stockholders after effectiveness of the Board Classification Proposal; and Class III would hold office initially for a term expiring at the third annual meeting of stockholders after effectiveness of the Board Classification Proposal. The board has identified both the size of each class and nominees who would initially serve in each of the classes. If the proposed amendment is approved, then it is intended that the following classifications would be applied, subject to the election of any director nominee at the meeting.
Class I Directors
| · | Michael F. Eng |
| · | Thomas Lam, M.D. |
| · | David G. Schmidt |
Class II Directors
| · | Mitchell W. Kitayama |
| · | Kenneth Sim, M.D. |
| · | Mark Fawcett |
Class III Directors
| · | Li Yu |
| · | Warren Hosseinion, M.D. |
| · | Gary Augusta |
At each annual meeting of stockholders following the initial classification and election, the successors to the class of directors whose terms expire at each future meeting would be elected for a term of office to expire at the third succeeding annual meeting after their election and until their successors have been duly elected and qualified.
If the Board Classification Proposal is approved, it will become effective upon the filing of the amendment to the ApolloMed Charter with the State of Delaware in connection with the closing of the Merger.
Rationale for Classification
Classified boards provide protection against unwanted takeovers and proxy contests because they make it difficult for a substantial stockholder to gain control of the board of directors without the cooperation or approval of incumbent directors. Other than with respect to the Merger, the board is not aware of any planned or actual attempt to accumulate the common stock or to obtain control of ApolloMed but rather is recommending the Board Classification Proposal to ensure fair treatment of ApolloMed’s stockholders in any future takeover attempt.
| 108 |
The board believes that the Board Classification Proposal will reduce the possibility that a third party could effect a sudden change in the majority control of the board of directors without the support of the incumbent directors. However, the Board Classification Proposal may have significant effects on the ability of stockholders of ApolloMed to effect an immediate change in the composition of the ApolloMed board and otherwise to exercise their voting power to affect the composition of the board. Accordingly, stockholders are urged to read carefully the following portions of this section of this proxy statement and the relevant annexes hereto, which set forth the full text of the Board Classification Proposal, before voting on this proposal.
The board also believes a classified board will help ensure some continuity of management of the business and affairs of ApolloMed by minimizing the potential turnover of directors in a particular year and making it more time-consuming for a potential acquirer, or a substantial stockholder or stockholders to gain control of the board or ApolloMed without the consent of the incumbent board, and provide the board with sufficient time to review any proposal from the potential acquirer or substantial stockholders. Specifically, the proposed classified board amendment will significantly extend the time required to effect a change in control of the board and may discourage hostile takeover bids. Currently, changes in control of the board can be made by stockholders holding a majority of the votes cast at a single annual meeting. If ApolloMed implements a classified board, it will take at least two annual meetings for a majority of stockholders to make a change in control of the board, because only a minority of the directors would be eligible for election at each meeting.
Vote Required for Approval.
Assuming a quorum is present, approval of the Board Classification Proposal requires the affirmative vote of (i) a majority of the shares of ApolloMed common stock, Series A preferred stock and Series B preferred stock, voting together as one class on an as-converted basis, and (ii) a majority of the shares of ApolloMed common stock, Series A preferred stock and Series B preferred stock, voting together as one class on an as-converted basis, not owned by NMM.
Each of the ApolloMed Merger Proposal, the Board Classification Proposal and each of the directors in the Election of Directors Proposal are all conditioned on each other. The ApolloMed Compensation Proposal and the ApolloMed Adjournment Proposal are not conditioned on any other proposal.
Recommendation of the ApolloMed Board of Directors
THE APOLLOMED BOARD OF DIRECTORS RECOMMENDS THAT THE APOLLOMED STOCKHOLDERS VOTE “FOR” THE BOARD CLASSIFICATION PROPOSAL
| 109 |
APOLLOMED PROPOSAL 3 — APPROVAL OF EACH OF THE DIRECTORS IN THE ELECTION OF DIRECTORS PROPOSAL
General
The Election of Directors Proposal will only be presented to the special meeting of ApolloMed if the ApolloMed Merger Proposal and Board Classification Proposal are approved.
As currently in effect, ApolloMed’s Bylaws provide that the authorized number of directors shall be fixed from time to time by the ApolloMed board, provided that the authorized number of directors shall not be less than one. The ApolloMed board of directors currently consists of seven members. Pursuant to the Merger Agreement, the board has nominated nine individuals for election at the special meeting, of which five are currently serving on the board, and has set the number of directors at nine, with a three-class board.
There are no family relationships among any of the current directors, the nominees for directors and ApolloMed’s executive officers.
ApolloMed is asking its stockholders to approve the election of nine nominees to the board of directors of ApolloMed, each of whom shall be designated a class and shall serve until the expiration of the term with respect to such designated class. If the election of the nine nominees is approved, such election will become effective upon the classification of the ApolloMed board in connection with closing of the Merger.
Nominees for Election as Directors
The following are the nominees for election as directors to the ApolloMed board of directors and their designated classes:
Class I Directors
| · | Michael F. Eng (NMM designee) |
| · | Thomas Lam, M.D. (NMM designee) |
| · | David G. Schmidt (ApolloMed designee) |
Class II Directors
| · | Mitchell W. Kitayama (NMM designee) |
| · | Kenneth Sim, M.D. (NMM designee) |
| · | Mark Fawcett (ApolloMed designee) |
Class III Directors
| · | Li Yu (NMM designee) |
| · | Warren Hosseinion, M.D. (ApolloMed designee) |
| · | Gary Augusta (ApolloMed designee) |
The biographies and other information regarding the above nominees are described in detail in the other sections in this joint proxy statement/prospectus.
Vote Required for Approval.
Assuming a quorum is present, approval of each of the directors in the Election of Directors Proposal requires the affirmative vote of (i) a majority of the shares of ApolloMed common stock, Series A preferred stock and Series B preferred stock, voting together as one class on an as-converted basis, and (ii) a majority of the shares of ApolloMed common stock, Series A preferred stock and Series B preferred stock, voting together as one class on an as-converted basis, not owned by NMM.
| 110 |
Each of the ApolloMed Merger Proposal, the Board Classification Proposal and each of the directors in the Election of Directors Proposal are all conditioned on each other. The ApolloMed Compensation Proposal and the ApolloMed Adjournment Proposal are not conditioned on any other proposal.
Recommendation of the ApolloMed Board of Directors
THE APOLLOMED BOARD OF DIRECTORS RECOMMENDS THAT THE APOLLOMED STOCKHOLDERS VOTE “FOR” EACH OF THE DIRECTORS IN THE ELECTION OF DIRECTORS PROPOSAL
| 111 |
APOLLOMED PROPOSAL 4 – APPROVAL OF THE APOLLOMED COMPENSATION PROPOSAL
The Dodd-Frank Act and Rule 14a-21(c) under the Exchange Act require that ApolloMed seek a non-binding advisory vote from ApolloMed’s stockholders to approve certain merger-related executive compensation, as disclosed in the section entitled “The Merger – Interests of ApolloMed’s Directors and Executive Officers in the Merger”, beginning on page 151, including the table entitled “Merger-Related Compensation for ApolloMed’s Named Executive Officers” and accompanying footnotes and narrative discussion. Accordingly, ApolloMed is asking its stockholders to vote in favor of the adoption of the following Resolution, on a non-binding advisory basis:
“RESOLVED, that the compensation that may be paid or become payable to ApolloMed’s named executive officers, as disclosed pursuant to Item 402(t) of Regulation S-K, including the compensation tables and any related information disclosed in this joint proxy statement/prospectus is hereby APPROVED”.
Vote Required for Approval
The approval, by non-binding advisory vote, of the ApolloMed Compensation Proposal requires the affirmative vote of holders of a majority of the number of shares of ApolloMed common stock entitled to vote present or represented by proxy at the ApolloMed special meeting. Votes to “ABSTAIN” are counted for purposes of determining a quorum and will be considered a vote “AGAINST” the ApolloMed Compensation Proposal.
The vote on the ApolloMed Compensation Proposal is a vote separate and apart from the vote to adopt the Merger Agreement and other related proposals. Accordingly, a stockholder may vote to approve the ApolloMed Compensation Proposal and vote not to approve the ApolloMed Merger Proposal, the Board Classification Proposal and each of the directors in the Election of Directors Proposal (which are conditioned on each other), or vote to approve such proposals and vote not to approve the ApolloMed Compensation Proposal. Because the vote on the ApolloMed Compensation Proposal is advisory only, it will not be binding on ApolloMed or the combined company after the Merger. Accordingly, if the ApolloMed Merger Proposal, the Board Classification Proposal and each of the directors in the Election of Directors Proposal are adopted by ApolloMed’s stockholders and the Merger is completed, the Merger-related compensation may be paid to ApolloMed’s named executive officers to the extent payable in accordance with the terms of their compensation agreements and arrangements even if ApolloMed’s stockholders do not approve the ApolloMed Compensation Proposal.
Recommendation of the ApolloMed Board of Directors
THE APOLLOMED BOARD OF DIRECTORS RECOMMENDS THAT APOLLOMED STOCKHOLDERS VOTE “FOR” THE APOLLOMED COMPENSATION PROPOSAL
| 112 |
APOLLOMED PROPOSAL 5 — APPROVAL OF THE APOLLOMED ADJOURNMENT PROPOSAL
The ApolloMed Adjournment Proposal, if adopted, will allow ApolloMed’s board of directors to adjourn the special meeting of stockholders to a later date or dates, if necessary or appropriate, to permit further solicitation of proxies in the event, based on the tabulated votes, there are not sufficient votes at the time of the special meeting to approve one or more of the proposals presented at the special meeting. In no event will ApolloMed’s board of directors adjourn the special meeting without further notice, to a date that is more than 30 days after the date for which the special meeting was originally noticed or if a new record date is fixed for the adjourned meeting.
In the ApolloMed Adjournment Proposal, ApolloMed is asking its stockholders to authorize the holder of any proxy solicited by its board of directors to vote in favor of granting discretionary authority to ApolloMed’s board of directors to adjourn the special meeting to another time and place for the purpose of soliciting additional proxies. If ApolloMed’s stockholders approve the ApolloMed Adjournment Proposal, ApolloMed could adjourn the special meeting and any adjourned session of the special meeting and use the additional time to solicit additional proxies, including the solicitation of proxies from ApolloMed stockholders who have previously voted. If ApolloMed adjourns the special meeting, it will not give notice of the time and place of the adjourned meeting other than by an announcement of such time and place at the special meeting.
Vote Required for Approval
Assuming a quorum is present, approval of the ApolloMed Adjournment Proposal requires the affirmative vote of holders of a majority of the number of shares of ApolloMed stock entitled to vote present in person or represented by proxy at the ApolloMed special meeting. Adoption of the ApolloMed Adjournment Proposal is not conditioned upon the approval of any of the other proposals.
Recommendation of the ApolloMed Board of Directors
THE APOLLOMED BOARD OF DIRECTORS RECOMMENDS THAT APOLLOMED STOCKHOLDERS VOTE “FOR” THE APOLLOMED ADJOURNMENT PROPOSAL.
| 113 |
THE SPECIAL MEETING OF NMM SHAREHOLDERS
This section contains information for NMM’s shareholders regarding this special meeting of NMM shareholders that has been called to consider the approval of the NMM Merger Proposal and the NMM Adjournment Proposal.
NMM is furnishing this joint proxy statement/prospectus to the holders of NMM common stock of the record date in connection with the solicitation of proxies by the NMM board of directors for use at the NMM special meeting and any adjournment or postponement of its special meeting.
The NMM special meeting will be held on [●], 2017, at [●][a.m.][p.m.], Pacific Standard Time, at 1668 S. Garfield Avenue, 3rd Floor, Alhambra, California 91801.
Purpose of the NMM Special Meeting
At the NMM special meeting, NMM shareholders will be asked to consider and vote upon the following matters:
(1) The NMM Merger Proposal; and
(2) The NMM Adjournment Proposal.
Recommendation of the NMM Board of Directors
The NMM board of directors has determined that it is advisable and in the best interest of NMM and its shareholders to enter into the Merger Agreement and the NMM board of directors has authorized and approved the terms of the Merger Agreement and the transactions contemplated thereby. Certain factors considered by the NMM board of directors in reaching its decision to adopt and approve the Merger Agreement and the Merger can be found in the section of this joint proxy statement/prospectus entitled “THE MERGER – NMM Reasons for the Merger” beginning on page 130.
The NMM board of directors recommends that NMM shareholders vote “FOR” the NMM Merger Proposal and “FOR” the NMM Adjournment Proposal.
The NMM board of directors has fixed the close of business on [●], 2017 as the record date for the NMM special meeting. Only holders of record of shares of NMM common stock on the NMM record date are entitled to vote at the NMM special meeting. Each share of NMM common stock entitles the holder to one vote at the NMM special meeting on each proposal or action to be considered at the NMM special meeting.
As of the NMM record date, there were [●] shares of NMM common stock outstanding and entitled to vote at the NMM special meeting held by approximately [●] holders of record. Each share of NMM common stock entitles the holder to one vote at the NMM special meeting on each proposal to be considered at the NMM special meeting.
The presence of holders of at least a majority of the outstanding shares of NMM common stock is required to constitute a quorum. Shareholders present in person or by proxy will be counted for purposes of determining whether a quorum is present.
In the event that a quorum is not present, or if there are insufficient votes to approve the principal terms of the Merger and the Merger Agreement at the time of the special meeting, it is expected that the special meeting will be adjourned or postponed to solicit additional votes. As of the record date for the special meeting, [●] shares of NMM’s common stock would be required to achieve a quorum.
| 114 |
Eddie Lam, M.D., Thomas Lam, M.D., Su Kin Lee, M.D., Kenneth Sim, M.D., Theresa Tseng, M.D., Yang Chern Tseng, M.D., and Albert Young, M.D. have each entered into an agreement with ApolloMed pursuant to which each has agreed to vote all of the shares of NMM common stock owned or controlled by them in favor of the Merger and the Merger Agreement. As of the close of business on [●], 2017, the record date for the special meeting, Eddie Lam, M.D., Thomas Lam, M.D., Su Kin Lee, M.D., Kenneth Sim, M.D., Theresa Tseng, M.D., Yang Chern Tseng, M.D., and Albert Young, M.D. collectively owned, directly or indirectly, [●] shares of NMM common stock, which represented approximately [●]% of the outstanding shares of NMM common stock.
A complete list of shareholders of record entitled to vote at the special meeting will be available for 10 days before the special meeting at NMM’s principal executive office for inspection by shareholders during ordinary business hours for any purpose germane to the special meeting.
Assuming a quorum is present, approval of the NMM Merger Proposal requires the affirmative vote of NMM shareholders holding at least 95% of the outstanding shares of NMM common stock and representing at least 95% in number of the NMM shareholders. The NMM Adjournment Proposal requires the affirmative vote of a majority of the outstanding shares of NMM stock entitled to vote present in person or represented by proxy at the NMM special meeting.
The NMM Merger Proposal and the NMM Adjournment Proposal are not conditioned on each other. If the NMM Merger Proposal does not receive the requisite vote for approval, then ApolloMed and NMM will not consummate the Merger.
NMM shareholders are entitled to the right to seek appraisal of the fair value of their shares of NMM common stock under Chapter 13 of the California Corporations Code. See the section titled “THE MERGER – Dissenters’ Rights” beginning on page 154 of this joint proxy statement/prospectus.
Abstentions and Failure to Vote
If you are a NMM shareholder and mark “ABSTAIN” on your proxy with respect to the NMM Merger Proposal and the NMM Adjournment Proposal, NMM will count the proxy with respect to the NMM Merger Proposal and NMM Adjournment Proposal as present for purposes of determining whether a quorum is present, but for purposes of approval an abstention will have the same effect as a vote “AGAINST” the NMM Merger Proposal and the NMM Adjournment Proposal.
If you fail to submit a proxy card or vote at the special meeting, your shares will not be counted for purposes of determining a quorum. If you are a NMM shareholder of record and fail to submit a proxy card or vote at the special meeting, your shares will not be counted toward the total vote and will have no effect on the NMM Adjournment Proposal but will be considered a vote “AGAINST” the NMM Merger Proposal.
Whether or not you plan to attend the NMM special meeting in person, you should submit your proxy as soon as possible. If you own shares of NMM common stock in your own name, you are an owner or holder of record. This means that you may use the enclosed proxy card to tell the persons named as proxies how to vote your shares of NMM common stock. You may vote your shares of NMM common stock held of record in any of the following ways:
In Person — To vote in person, come to the NMM special meeting and you will be able to vote by ballot. To ensure that your shares of NMM capital stock are voted at the NMM special meeting, the NMM board of directors recommends that you submit a proxy even if you plan to attend the NMM special meeting.
| 115 |
By Mail — To vote using the enclosed proxy card, simply complete, sign and date the enclosed proxy card and return it promptly in the enclosed return envelope. If you return your signed proxy card to NMM before the NMM special meeting, the persons named as proxies will vote your shares of NMM common stock as you direct.
Submitting a proxy will not affect your right to vote in person if you decide to attend the NMM special meeting.
The NMM board of directors has appointed Kenneth Sim and Thomas Lam to serve as proxies for the NMM special meeting.
If a proxy card is signed and returned without an indication as to how the shares of NMM common stock represented by the proxy are to be voted with regard to the proposal, the NMM common stock represented by the proxy will be voted “FOR” such proposal. As of the date of this joint proxy statement/prospectus, NMM has no knowledge of any business that will be presented for consideration at the NMM special meeting and which would be required to be set forth in this joint proxy statement/prospectus other than the matters set forth in the accompanying Notice of Special Meeting of Shareholders of NMM. In accordance with the NMM Bylaws and California law, business transacted at the NMM special meeting will be limited to those matters set forth in such notice.
Your vote as an NMM shareholder is very important. Please submit your proxy as soon as possible, whether or not you plan to attend the NMM special meeting in person.
Revocation of Proxies and Voting Instructions
If your shares of NMM common stock are registered in your own name, you may revoke your proxy in one of the following ways by:
| · | Attending the NMM special meeting and voting in person. Your attendance at the NMM special meeting will not by itself revoke a proxy. You must vote your shares by ballot at the NMM special meeting to revoke your proxy; |
| · | Completing and submitting a new valid proxy card bearing a later date; or |
| · | Sending written notice of revocation to NMM at Network Medical Management, Inc., Attn: Secretary, 700 1668 S. Garfield Avenue, 3rd Floor, Alhambra, California 91801, which notice must be received before [●], Eastern Time, on [●], 2017. |
NMM will appoint Sue Kin Lee as inspector of election for the NMM special meeting to tabulate the affirmative and negative votes and abstentions.
The cost of solicitation of proxies from NMM shareholders will be borne by NMM. In addition to solicitation by use of the mail, proxies may be solicited by directors, officers and employees of NMM in person. These directors, officers and employees will not receive additional compensation for their efforts but will be reimbursed for reasonable out-of-pocket expenses they incur in connection with the solicitation. NMM will reimburse custodians, nominees and fiduciaries for their reasonable out-of-pocket expenses incurred in forwarding of solicitation materials to the beneficial owners of NMM common stock and collecting voting instructions.
| 116 |
If you need assistance in completing your proxy card or have questions regarding the various voting options with respect to the NMM special meeting, please contact:
Network Medical Management, Inc.
1668 S. Garfield Avenue, 3rd Floor
Alhambra, California 91801
Attention: Thomas Lam, M.D.
Chief Executive Officer
Telephone: (626) 282-0288
| 117 |
PROPOSALS SUBMITTED TO NMM SHAREHOLDERS
NMM PROPOSAL 1 – APPROVAL OF THE NMM MERGER PROPOSAL
As discussed in this joint proxy statement/prospectus, NMM is asking its shareholders to approve the NMM Merger Proposal, which includes an approval of the Merger, the Merger Agreement and the transactions contemplated thereby, including the issuance of shares of ApolloMed common stock and warrants in connection therewith.
For a summary of and detailed information regarding this proposal, see the information about the Merger Agreement and the issuance of shares of ApolloMed common stock and warrants in the Merger throughout this joint proxy statement/prospectus, including the information set forth in sections entitled “THE MERGER” beginning on page 120 and “THE MERGER AGREEMENT” beginning on page 158. A copy of the Merger Agreement is attached as Annex A to this joint proxy statement/prospectus and incorporated herein by reference. You are urged to read carefully this joint proxy statement/prospectus and the Merger Agreement attached hereto in their entirety before voting on this proposal.
Under the terms of the Merger Agreement, Merger Sub will merge with and into NMM, with NMM becoming a wholly-owned subsidiary of ApolloMed. The Merger has been structured to qualify for federal income tax purposes as a tax-deferred reorganization under the provisions of Section 368(a) of the Internal Revenue Code of 1986.
Pursuant to the Merger Agreement, at the Effective Time, each issued and outstanding share of NMM common stock will be converted into the right to receive such number of fully paid and nonassessable ApolloMed shares of common stock that results in the NMM shareholders having a right to receive (A) an aggregate number of shares of ApolloMed common stock that represents 82% of the total issued and outstanding shares of ApolloMed common stock immediately following the Effective Time, assuming there are no NMM dissenting shareholder interests as of the Effective Time, calculated in accordance with the Merger Agreement (see “THE MERGER AGREEMENT – Effects of Merger; Merger Consideration” beginning on page 159), plus (B) an aggregate of 2,566,666 shares of ApolloMed common stock, assuming there are no NMM dissenting shareholder interests as of the Effective Time. In addition, each NMM shareholder shall be entitled to receive such shareholder’s pro rata portion of (i) warrants to purchase an aggregate of 850,000 shares of ApolloMed common stock, exercisable at $11.00 per share and (ii) warrants to purchase an aggregate of 900,000 shares of ApolloMed common stock, exercisable at $10.00 per share. At the Effective Time, ApolloMed will hold back the Holdback Shares to secure indemnification of ApolloMed and its affiliates under the Merger Agreement. Separately, indemnification of pre-Merger NMM shareholders under the Merger Agreement will be made by the issuance by ApolloMed to pre-Merger NMM shareholders of new additional shares of common stock (capped at the same number of shares of ApolloMed common stock as the Holdback Shares).
The terms of, reasons for and other aspects of the Merger Agreement, the Merger and the issuance of shares of ApolloMed common stock and warrants pursuant to the Merger Agreement are described in detail in the other sections in this joint proxy statement/prospectus.
Vote Required for Approval.
Assuming a quorum is present, approval of the NMM Merger Proposal requires the affirmative vote of NMM shareholders holding at least 95% of the outstanding shares of NMM common stock and representing at least 95% in number of the NMM shareholders.
The NMM Merger Proposal and the NMM Adjournment Proposal are not conditioned on each other. If the NMM Merger Proposal does not receive the requisite vote for approval, then ApolloMed and NMM will not consummate the Merger.
Dissenters’ Rights
NMM shareholders are entitled to the right to seek appraisal of the fair value of their shares of NMM common stock under Chapter 13 of the California Corporations Code. See the section titled “THE MERGER – Dissenters’ Rights” beginning on page 154 of this joint proxy statement/prospectus.
Recommendation of the NMM Board of Directors
THE NMM BOARD OF DIRECTORS RECOMMENDS THAT NMM SHAREHOLDERS VOTE “FOR” THE NMM MERGER PROPOSAL.
| 118 |
NMM PROPOSAL 2 — APPROVAL OF THE NMM ADJOURNMENT PROPOSAL
The NMM Adjournment Proposal, if adopted, will allow NMM’s board of directors to adjourn the special meeting to a later date or dates, if necessary or appropriate, to permit further solicitation of proxies in the event, based on the tabulated votes, there are not sufficient votes at the time of the special meeting to approve one or more of the proposals presented at the special meeting. In no event will NMM’s board of directors adjourn the special meeting without further notice, to a date that is more than 30 days after the date for which the special meeting was originally noticed or if a new record date is fixed for the adjourned meeting.
In the NMM Adjournment Proposal, NMM is asking its shareholders to authorize the holder of any proxy solicited by its board of directors to vote in favor of granting discretionary authority to NMM’s board of directors to adjourn the special meeting to another time and place for the purpose of soliciting additional proxies. If NMM’s shareholders approve the NMM Adjournment Proposal, NMM could adjourn the special meeting and any adjourned session of the special meeting and use the additional time to solicit additional proxies, including the solicitation of proxies from NMM shareholders who have previously voted. If NMM adjourns the special meeting, it will not give notice of the time and place of the adjourned meeting other than by an announcement of such time and place at the special meeting.
Vote Required for Approval
Assuming a quorum is present, approval of the NMM Adjournment Proposal requires the affirmative vote of holders of a majority of the number of shares of NMM stock entitled to vote present in person or represented by proxy at the NMM special meeting. Adoption of the NMM Adjournment Proposal is not conditioned upon the approval of any of the other proposals.
Recommendation of the NMM Board of Directors
THE NMM BOARD OF DIRECTORS RECOMMENDS THAT NMM SHAREHOLDERS VOTE “FOR” THE NMM ADJOURNMENT PROPOSAL.
| 119 |
The following discussion contains certain information about the Merger. The discussion is subject, and qualified in its entirety by reference, to the Merger Agreement and Amendments attached as Annex A to this joint proxy statement/prospectus. NMM and ApolloMed urge you to read carefully this entire joint proxy statement/prospectus, including the Merger Agreement and Amendments attached as Annex A for a more complete understanding of the Merger.
Each of the respective boards of directors of ApolloMed and NMM has approved the Merger Agreement and the transactions contemplated therein, including the Merger. Pursuant to the Merger Agreement, Merger Sub, a wholly owned subsidiary of ApolloMed, will merge with and into NMM, with NMM continuing as the surviving entity and a wholly owned subsidiary of ApolloMed. The Merger will be effective upon the filing of the Certificate of Merger with the Secretary of State of the State of California or at such later time as is agreed to by the parties and specified in the Certificate of Merger. The time at which the Merger becomes effective is referred to as the “Effective Time”.
At the Effective Time, each issued and outstanding share of NMM common stock will be converted into the right to receive such number of fully paid and nonassessable ApolloMed shares of common stock that results in the NMM shareholders having a right to receive (A) an aggregate number of shares of ApolloMed common stock that represents 82% of the total issued and outstanding shares of ApolloMed common stock immediately following the Effective Time, assuming there are no NMM dissenting shareholder interests as of the Effective Time, calculated in accordance with the Merger Agreement (see “THE MERGER AGREEMENT – Effects of Merger; Merger Consideration” beginning on page 159), plus (B) an aggregate of 2,566,666 shares of ApolloMed common stock, assuming there are no NMM dissenting shareholder interests as of the Effective Time. In addition, each NMM shareholder shall be entitled to receive such shareholder’s pro rata portion of (i) warrants to purchase an aggregate of 850,000 shares of ApolloMed common stock, exercisable at $11.00 per share and (ii) warrants to purchase an aggregate of 900,000 shares of ApolloMed common stock, exercisable at $10.00 per share.
For purposes of calculating the exchange ratio, (A) the aggregate number of shares of ApolloMed common stock held by the NMM shareholders immediately following the Effective Time will exclude (i) any shares of ApolloMed common stock owned by NMM shareholders immediately prior to the Effective Time, (ii) the Additional Shares and (iii) any ApolloMed common stock issuable to NMM shareholders pursuant to the exercise of the ApolloMed Warrants and/or the Warrant Consideration and (B) the total number of issued and outstanding shares of ApolloMed common stock immediately following the Effective Time shall exclude 499,000 shares of ApolloMed common stock issued or issuable to Alliance under the Alliance Note pursuant to the Securities Purchase Agreement between ApolloMed and Alliance dated as of March 30, 2017 (the “Securities Purchase Agreement”).
In connection with the Merger Agreement, it is contemplated that Warren Hosseinion, M.D., the sole shareholder of MMG, will sell to APC-LSMA (an entity in which Dr. Thomas Lam is the sole shareholder and the sole executive officer, but which is controlled and consolidated by APC) all the issued and outstanding shares of capital stock of MMG for $100 under the Maverick Stock Purchase Agreement.
The closing price of ApolloMed common stock on the OTC Pink on December 21, 2016, the last full trading day prior to the public announcement of the Merger, was $3.99. The closing price of ApolloMed common stock on the OTC Pink on [●], 2017, the last practicable full trading day prior to the date of this joint proxy /prospectus, was $[●].
ApolloMed Overview
Apollo Medical Holdings, Inc. was incorporated in the State of Delaware on November 1, 1985 under the name McKinnely Investment, Inc. On November 5, 1986 McKinnely Investment, Inc. changed its name to Acculine Industries, Incorporated and Acculine Industries, Incorporated changed its name to Siclone Industries, Incorporated on May 24, 1988. On July 3, 2008, Apollo Medical Holdings, Inc. merged into Siclone Industries, Incorporated and Siclone Industries, Incorporated, as the surviving entity from the merger, simultaneously changed its name to Apollo Medical Holdings Inc.
ApolloMed is a physician-centric, integrated population health management company working to provide coordinated outcomes-based medical care in a cost-effective manner. Led by a management team with over a decade of experience, ApolloMed has built a company and culture that is focused on physicians providing high-quality medical care, population health management and care coordination for patients, particularly senior patients and patients with multiple chronic conditions. ApolloMed believes it is well-positioned to take advantage of changes in the rapidly evolving U.S. healthcare industry, as there is a growing national movement towards more results-oriented healthcare centered on the triple aim of patient satisfaction, high-quality care and cost efficiency.
| 120 |
NMM Overview
Network Medical Management, Inc. is a California corporation formed in 1994. NMM, together with its subsidiaries and affiliated physician groups, constitutes a patient- and physician-centric, integrated health care delivery and management services company focused on providing coordinated, outcomes-based medical care in a cost-effective manner. Through capitation agreements between NMM’s affiliated physician groups and various health plans, NMM is responsible for coordinating the care for over 600,000 covered patients in southern and central California through a network of over 10 IPAs with approximately 4,000 contracted physicians. These covered patients are comprised of managed care members whose health coverage is provided through their employer or who have individually acquired health coverage directly from a health plan or as a result of their eligibility for Medicaid or Medicare benefits.
The patients of NMM’s affiliated physician groups and IPAs benefit from an integrated approach to medical care that places the physician at the center of patient care. NMM manages the delivery of healthcare services to patients via a network of affiliated physician groups and other network primary care physicians, network hospitals, and affiliated group and network specialists. Together with case managers, registered nurses and other care coordinators, these medical professionals utilize a comprehensive data analysis engine, sophisticated risk management techniques and clinical protocols to provide high-quality, cost effective care to NMM’s managed members. NMM monitors certain control metrics, such as the number of inpatient acute bed days per 1,000 patients and hospital readmission rates, as they are contributors to quality clinical outcomes and financial performance. Additionally, in an effort to identify changes or trends with respect to its commercial, senior and Medicaid payer classifications, NMM closely monitors the number of managed care members who have enrolled with a NMM affiliated physician group as such member’s primary care physician.
NMM is headquartered in, and primarily operates from, Los Angeles County, California.
Background of the Merger between ApolloMed and NMM
The management teams and boards of directors of each of ApolloMed and NMM have been actively monitoring and assessing developments in the population health management industry and are generally aware of the business activities of other major health management companies, especially those companies located in California. As a result, executives and board members from each of ApolloMed and NMM are generally familiar with the other company’s business and operations.
In addition, in light of the economic and regulatory landscape and trends in the U.S. healthcare system and ApolloMed’s need for additional financing to succeed, ApolloMed management has from time to time reviewed and considered potential strategic alternatives to grow the company’s business, including mergers and strategic combinations with other industry participants with a strong financial position. These strategic alternatives have been reviewed by the ApolloMed board periodically since ApolloMed became a publicly held company in June 2008 through a reverse merger. The ApolloMed board also has explored financing opportunities periodically to satisfy the company’s requirements. In reviewing different strategic opportunities, the ApolloMed board has prioritized long-term value for stockholders and directed management to focus on identifying companies with complementary service capabilities and management expertise which, if combined with ApolloMed, could offer synergies, including increased operational scale, reduced risk and administrative costs, potential for introducing ApolloMed’s core capabilities (including management of chronically ill, high-risk patients, hospitalist medicine, hospice/palliative care, home-health care and population health management consulting services) to another network of IPAs, addition of new expertise (such as NMM’s management services and case management system), increased demand for “bundled” services, transitioning to a value-based reimbursement business model, and ApolloMed’s NGACO program. The ApolloMed board and management also shared the view that any potential pursuit of a strategic combination should strengthen the combined company’s balance sheet and enable a post-transaction uplisting to a major stock exchange (such as NASDAQ) and thus enhancing ApolloMed’s ability to raise additional financing in the public markets. Since 2008, ApolloMed management has had multiple interactions with different parties, including NMM. Following is a chronological record of material events leading up to event of the Merger Agreement and announcement of the pending Merger.
On August 19, 2014, Mr. Gary Augusta, ApolloMed’s current Executive Chairman, outlined to the ApolloMed board a plan to raise capital in the public equity markets through a mid-sized broker dealer (“Broker”). In August 2014, management entered into discussions with the Broker, who was formally engaged in November 2014.
| 121 |
In early 2015, to continue exploring alternatives, ApolloMed entered into non-disclosure agreements with certain private equity groups for ApolloMed management to exchange information and discuss potential strategic opportunities with them. These discussions did not lead to any concrete proposal.
On March 9, 2015, ApolloMed filed a registration statement on Form S-1 in connection with the proposed public offering. After review and pre-effective amendments, the S-1 was declared effective by the staff of the SEC on May 14, 2015.
In May 2015, ApolloMed management had a series of meetings with potential investors as part of an investor roadshow for a proposed underwritten public offering and on May 7, 2015, ApolloMed filed, and the SEC declared effective, a Form S-1 Registration Statement in connection therewith. On June 1, 2015, ApolloMed management updated the board of directors on progress of the public offering. In early June 2015, the Broker that had been engaged to manage the proposed ApolloMed public offering communicated to ApolloMed management that, to consummate the public offering, ApolloMed would need to increase the amount of previously-discussed warrant coverage, with freely tradable warrants having their own ticker symbol, to be offered in addition to its common stock. On June 9, 2015, ApolloMed management engaged in a discussion with the ApolloMed board regarding ApolloMed’s financing efforts (including an overview by Mr. Augusta of the investor roadshow) and management determined that it was not in the best interests of ApolloMed’s stockholders to complete the public offering on the basis proposed by Broker.
On July 27, 2015, after several discussions and a meeting in New York City with Warren Hosseinion, M.D., ApolloMed’s Chief Executive Officer, Private Equity Firm A sent a proposal to Dr. Hosseinion to indicate its interest in investing in newly-issued capital stock of ApolloMed. As part of its proposal, Private Equity Firm A expected the securities to feature certain preemptive rights, negative controls and exit rights. Certain of the terms of Private Equity Firm A’s proposal were determined to be unacceptable to ApolloMed.
On July 28, 2015, the ApolloMed board discussed various positive and negative aspects of both public and private capital structures, as well as NASDAQ uplisting requirements.
On August 12, 2015, Dr. Hosseinion held a meeting with Kenneth Sim, M.D. and Thomas Lam, M.D., NMM’s current Chairman and Chief Executive Officer, respectively. At that meeting, Dr. Hosseinion, Dr. Sim and Dr. Lam first discussed a possible investment by NMM in ApolloMed, which could be a prelude to a possible business combination, as well as the potential advantages of a combined company, including increased and synergistic operational expertise, capabilities and scale, an experienced management team with complementary skills and the potential to access additional sources of capital.
On August 20, 2015, ApolloMed management discussed with the ApolloMed board of directors the option of pursuing private investment in ApolloMed, as well as the possibility of relaunching a public offering. A stock purchase agreement for use in connection with a private investment was prepared and circulated. The private offering was delayed and ultimately not pursued after preliminary outreach to select individual investors.
On August 24, 2015, Dr. Sim informed the NMM board of a possible business combination with ApolloMed. The NMM board approved Drs. Sim and Lam to continue to pursue a possible business combination with ApolloMed.
On September 13, 2015, Dr. Hosseinion made a presentation to the NMM board, setting forth a rationale for NMM investment in ApolloMed and to raise the possibility of forming a combined patient-centered, physician-centric integrated healthcare delivery company focused on cutting costs, improving care and preparing for challenges and opportunities presented by the future of U.S. healthcare.
On September 15, 2015, the ApolloMed board discussed various strategic alternatives (including possibly renewing efforts to complete a public offering) and discussed the status of management’s discussions with Private Equity Firm A. ApolloMed management examined options for capital raises with the ApolloMed board and determined that, as Private Equity Firm A was seeking preferential rights akin to those granted by private companies in early-stage preferred stock financings, its proposal was not practically viable and was not in the best interest of ApolloMed and its stockholders. After a discussion with the ApolloMed board, ApolloMed management determined to continue discussions regarding the potential investment from NMM.
| 122 |
On September 17, 2015, Dr. Hosseinion made a presentation to the NMM executive board regarding ApolloMed’s history, structures, financial picture, strategy and direction. A possible business combination and preliminary deal points were also discussed.
On September 18, 2015, NMM and ApolloMed signed a non-disclosure agreement with ApolloMed in order to exchange information and documents and to conduct due diligence on each other. Subsequently, the parties negotiated the key terms of an approximately $10 million investment by NMM in ApolloMed in the form of units consisting of Series A preferred stock at a price of $9.00 per share (which was consistent with the pricing of a prior investment that ApolloMed received from an investing unit of Fresenius Medical Care), and 100% warrant coverage. ApolloMed management discussed with the board of directors that the NMM investment could be used to pay off the Fresenius debt, and that NMM considered such a financing to be the first step toward a merger of the companies.
On September 21, 2015, the NMM board discussed the proposed business combination, including due diligence.
On October 12, 2015, the NMM board reviewed with management the key terms of the proposed $10 million investment in ApolloMed by NMM.
On October 13, 2015, the ApolloMed board approved (i) the proposed $10 million investment in ApolloMed by NMM, and (ii) the repayment of the NNA debt.
On October 14, 2015, ApolloMed and NMM entered into a Securities Purchase Agreement, pursuant to which NMM purchased investment units from ApolloMed consisting of 1,111,111 shares of ApolloMed’s Series A Preferred Stock and warrants to purchase 1,111,111 shares of ApolloMed’s common stock at an exercise price of $9.00 per share, for an aggregate $10,000,000. See “Related Party Transactions” beginning on page 198 for additional information.
On October 16, 2015, ApolloMed received a pay-off letter from NNA relating to its debt, and negotiations continued regarding the conversion of NNA securities into ApolloMed common stock, which was completed on November 17, 2015.
On October 19, 2015, the NMM board discussed the proposed business combination. NMM has been represented by Tin Kin Lee Law Offices for the proposed business combination.
Dr. Hosseinion discussed and met with NMM management and the parties reached a consensus that, before pursuing a potential business combination, the companies should first deepen their collaboration through ApolloMed providing services to entities affiliated with NMM, including hospitalist services for APC and management services for NMM’s two MSSP ACOs.
On November 17, 2015, management briefed the ApolloMed board on ongoing capital raising possibilities and NASDAQ uplisting, and in subsequent meetings ApolloMed management continued to consider and explore capital-raising opportunities (including by public offering and NASDAQ uplisting).
In addition to exploring a possible business combination with NMM, ApolloMed management was also examining other strategic opportunities. On December 18, 2015, Dr. Hosseinion had a conference call with the Chief Executive Officer of Company X, a NASDAQ-listed healthcare company, to assess the parties’ interest in exploring a potential business combination. To facilitate exchange of information and documents, on December 19, 2015, ApolloMed and Company X entered into a non-disclosure agreement. On January 1, 2016, Dr. Hosseinion met several members of Company X’s senior management team at its offices. On January 12, 2016, Dr. Hosseinion and Mr. Augusta held a meeting with executives of Company X during the J.P. Morgan 34th Annual Healthcare Conference in San Francisco. To continue exploring this opportunity, on January 19, 2016, based on Company X’s financial condition and the perceived value of Company X and ApolloMed, respectively, Dr. Hosseinion emailed a preliminary proposal to Company X. Under that proposal, if the potential business combination were consummated, ApolloMed’s stockholders would acquire a substantial majority of the combined company. This offer was subsequently rejected. On June 2, 2016, Dr. Hosseinion had a follow-up meeting with executives of Company X. Afterwards, discussions with Company X were discontinued. ApolloMed management also held discussions at that time with Company Y regarding possible strategic and investment opportunities between the companies, which ultimately were discontinued.
| 123 |
On January 19, 2016, pursuant to ApolloMed’s agreements with NMM and an investing unit of Fresenius, the ApolloMed board appointed Dr. Lam to the board after having appointed a few days earlier another director, Mr. Mark Fawcett, a senior executive with Fresenius.
On February 1, 2016, ApolloMed started to provide hospitalist services for APC, an affiliate of NMM, at seven hospitals.
Subsequently, Dr. Hosseinion and NMM began discussions about the possibility of a second round of financing to be provided by NMM, including the basic terms and conditions of such financing.
On February 18, 2016, ApolloMed management discussed with the ApolloMed board how to expand its relationship with NMM, including potentially through a further investment management had been discussing with NMM and continued exploration of a business combination transaction with NMM.
On February 22, 2016, Dr. Hosseinion presented to the NMM board regarding the possibility of NMM making an additional investment in ApolloMed as well as the possibility of a business combination between the two companies.
On February 25, 2016, Dr. Hosseinion and Mr. Augusta met with Drs. Sim and Lam to discuss further the terms and conditions of an additional investment in ApolloMed by NMM.
On March 17, 2016, management briefed the ApolloMed board on the terms of the proposed Series B investment by NMM and discussed that NMM communicated its desire to continue to explore a business combination transaction.
On March 19, 2016, Dr. Hosseinion made a presentation at a shareholder meeting of NMM, where he introduced ApolloMed’s population health management platform and discussed CMS’ NGACO initiative.
Subsequently, the parties negotiated the key terms of an approximately $5 million investment in ApolloMed by NMM, including pricing at $10.00 per share of preferred stock and 100% warrant coverage.
On March 28, 2016, the ApolloMed board authorized the investment transaction with NMM.
On March 30, 2016, ApolloMed and NMM entered into a Securities Purchase Agreement, pursuant to which NMM purchased investment units from ApolloMed consisting of 555,555 shares of ApolloMed’s Series B Preferred Stock and warrants to purchase 555,555 shares of ApolloMed’s common stock at an exercise price of $10.00 per share, for an aggregate $4,999,995. See “Related Party Transactions” beginning on page 198 for additional information.
Dr. Hosseinion, Dr. Sim and Dr. Lam met again on April 4, 2016 to discuss further a potential business combination. Later that day, Dr. Hosseinion emailed a detailed due diligence list to Dr. Sim. At the April 4, 2016 meeting, the three executives also agreed to form a joint venture that would apply to CMS to participate in CMS’ NGACO Model in the name of the joint venture and include certain MSSP ACOs affiliated with NMM. The 50/50 joint venture, APAACO, was formed by ApolloMed and NMM on April 29, 2016. Beginning in May 2016, ApolloMed started to provide management services to two MSSP ACOs affiliated with NMM. See “INFORMATION ABOUT APOLLOMED – Business Description” beginning on page 219 for additional information.
On April 5, 2016, each of ApolloMed and NMM set up electronic data rooms for the other company and its representatives to access due diligence materials. Over the course of the succeeding months, each of the ApolloMed and NMM teams (including their respective legal counsel) performed the due diligence on the other company.
On April 21, 2016, management briefed the ApolloMed board on the overall merger process, including discussion of a proposed timeline, responsibilities and initial due diligence results.
On April 26, 2016, the ApolloMed board discussed various procedural and legal aspects of the proposed business combination. ApolloMed’s outside general counsel advised the ApolloMed board on certain legal considerations for its review and consideration of the proposed business combination.
| 124 |
On May 13, 2016, the ApolloMed board, in the absence of Dr. Lam, followed up on prior discussions regarding the potential business combination with NMM. At the meeting, Dr. Hosseinion made a presentation about NMM to the ApolloMed board, including in relation to NMM’s financial strength and performance. Dr. Hosseinion next outlined management’s rationale for combining the two companies, including operational synergies leading to a value-based-reimbursement business model, an important industry trend, differentiated but complementary expertise allowing each to help the other’s business and operations, and combined market and financial strengths for further expansion and capital raising. The ApolloMed board reviewed these benefits against compliance and other costs that could potentially increase as a result of the potential business combination. The ApolloMed board then reviewed with ApolloMed’s outside general counsel, SEC Law Firm, the overall legal process and considerations in evaluating and approving the proposed business combination.
On May 19, 2016, the ApolloMed board met and, in the absence of Dr. Lam, Dr. Hosseinion and Mr. Augusta, made a presentation regarding additional information about NMM and the potential transaction and then the ApolloMed board further discussed the proposed business combination, including due diligence topics and the advisability of retaining an investment banking firm for the proposed business combination (as well as the potential firms to take on this role). ApolloMed’s outside general counsel again advised the ApolloMed board on certain legal considerations for its review and consideration of the proposed business combination. The meeting was then adjourned to allow the ApolloMed board to visit NMM’s offices and to reconvene there. At NMM’s offices, Dr. Lam made a presentation to the ApolloMed board on NMM’s business, operations and history, the two companies’ competitive landscape and benefits created by the proposed business combination.
On June 25, 2016, Dr. Sim updated the NMM board on the status of the proposed business combination.
On July 21, 2016, in the absence of Dr. Lam, the ApolloMed board received from Mr. Augusta updates on the proposed business combination, including the continuing due diligence, the estimated closing schedule and the preliminary plan on post-merger integration. Mr. Augusta reported that after meeting with several financial advisory firms, management recommended BofA Merrill Lynch to serve as financial advisor for ApolloMed in connection with the transaction. After considering the advisory fee proposed by BofA Merrill Lynch and other key terms of the engagement and having a lengthy discussion with all questions being answered, the ApolloMed board authorized management to engage BofA Merrill Lynch.
On July 28, 2016, Dr. Hosseinion met with Dr. Sim and Dr. Lam to discuss the post-merger structure of the combined company and what percentages of the combined company would be owned by former shareholders of NMM and by existing stockholders of ApolloMed, respectively.
On August 15, 2016, Dr. Hosseinion and Mr. Augusta conferred with Dr. Sim and Dr. Lam in person to discuss on-going due diligence. At the meeting, they also exchanged views on the appropriate ownership split and share exchange ratio.
On August 18, 2016, ApolloMed management updated the ApolloMed board, in the absence of Dr. Lam, on the progress of ApolloMed’s due diligence review of NMM and management’s prior discussions with NMM about the preliminary terms of the proposed business combination. The ApolloMed board reviewed the preliminary terms of the proposed business combination with management. On the same day, ApolloMed formally engaged McDermott Will & Emery LLP (“MWE”) as its legal counsel for the proposed business combination. Subsequently, MWE began to draft the Merger Agreement and assist ApolloMed with legal due diligence.
On August 25 and 26, 2016, Dr. Hosseinion and Mr. Augusta attended NMM’s board retreat in San Diego where they discussed and negotiated certain material terms of the proposed business combination with members of the NMM board, including a roughly 80% (for NMM’s former shareholders) / 20% (for ApolloMed’s existing stockholders) ownership split on a fully diluted basis for the combined company and the mechanism and timing for setting the final exchange ratio, the composition of the initial board of directors of the combined company, as well as a termination fee to the non-defaulting party if the business combination is not consummated. Dr. Hosseinion also presented updates on the NGACO program.
On September 14, 2016, ApolloMed held its 2016 annual stockholders meeting. At the ApolloMed board’s meeting following the annual meeting (at which Dr. Lam was not present) representatives from BofA Merrill Lynch reviewed its preliminary financial analyses of the proposed transaction.
On October 1, 2016, Dr. Sim made a presentation to the NMM board regarding the proposed business combination and the mechanics of a reverse merger transaction.
| 125 |
On October 2, 2016, the NMM board reviewed the financials terms of the proposed transaction.
On October 7, 2016, MWE sent a preliminary version of the Merger Agreement to NMM’s legal counsel. Over the course of the following weeks, the parties and their representatives exchanged various drafts of the Merger Agreement.
In parallel with pursuing the potential business combination with NMM, ApolloMed management was also actively seeking other strategic options in order to maximize stockholder value. On October 7, 2016, Dr. Hosseinion had a conference call with representatives from Private Equity Firm B, which had invested in healthcare services companies, and discussed its potential interest in a possible investment in ApolloMed. On October 22 and 23, 2016, Dr. Hosseinion had an email exchange with the Vice President of Corporate Development at Company Y, a publicly traded healthcare development and management company, to share information about the two companies and explore the possibility of any strategic transaction between them. On November 2, 2016, Mr. Augusta met with representatives from Private Equity Firm C, a global leading private equity firm in New York City to explore potential investment and acquisition opportunities. On November 7, 2016, Dr. Hosseinion had separate face-to-face discussions with representatives from private equity firms A and B in New York City, to seek potential growth capital investments. These discussions did not lead to any concrete proposal from Company Y or private equity firms A, B and C.
On November 17, 2016, Mr. Augusta provided a status update on the proposed business combination and the due diligence process, and Dr. Sim and Dr. Lam made a further presentation on NMM and its affiliated organizations to the ApolloMed board. Dr. Hosseinion and Mr. Augusta then discussed the two companies’ financial performance and answered questions and comments from the ApolloMed board of directors.
On December 11, 2016, Dr. Hosseinion and Mr. Augusta discussed additional details of the Merger Agreement with NMM executives.
On December 12, 2016, a draft of the Merger Agreement was provided to the ApolloMed board. On the next day, the ApolloMed board received a revised draft of the Merger Agreement.
On December 14, 2016, Dr. Hosseinion and Dr. Sim had a telephonic discussion to negotiate certain key items under the Merger Agreement, including the break-up mechanism, the holdback shares, the minimum level of cash to be maintained by NMM at closing, and the final exchange ratio, as well as the terms of the $5 million working capital loan to be provided to ApolloMed after closing.
On December 15, 2016, Dr. Hosseinion and Mr. Augusta provided the ApolloMed board, in the absence of Dr. Lam, an update on BofA Merrill Lynch’s preliminary financial analyses of the proposed business combination. On the same day, ApolloMed formally engaged BofA Merrill Lynch as its financial advisor for the proposed business combination. On December 19, 2016, a further revised draft of the Merger Agreement and drafts of other transaction documents, including a voting agreement by and among ApolloMed and certain NMM shareholders (each, a “Voting Agreement” and together, the “Voting Agreements”), the Lock-Up Agreements to be entered into by all shareholders of NMM (other than any dissenting shareholders), a Consent and Waiver Agreement, the Working Capital Loan, the amendment to the ApolloMed Bylaws and the amendment to the ApolloMed Charter (collectively with the Merger Agreement, “Transaction Documents”), were provided to the ApolloMed board. See “AGREEMENTS RELATED TO THE MERGER” beginning on page 171 for additional information.
On December 20, 2016, the ApolloMed board of directors met for the purpose of considering the proposed business combination. At the meeting, representatives from BofA Merrill Lynch reviewed its preliminary financial analyses of the proposed business combination. The ApolloMed board then received updated reports on the proposed business combination including the status of negotiations with NMM on the Merger Agreement, and reviewed with representatives from MWE, outside legal counsel for the proposed business combination, directors’ fiduciary duties and the best practices in connection with considering approval of the Merger Agreement and the underlying transaction and key provisions of the Merger Agreement. A representative from MWE further explained the general framework of the stock-for-stock consideration in the proposed business combination, certain key terms of the Merger Agreement, including transaction structure, closing conditions, transaction consideration (including the exchange ratio) and termination provisions, as well as corporate governance changes that would apply to the combined company following the closing of the Merger, including the future composition of the ApolloMed board and amendments to ApolloMed’s Charter and Bylaws. The representative from MWE also discussed various aspects of the Transaction Documents and responded to questions posed by the ApolloMed board. The ApolloMed board then discussed issues related to the then-current versions of the Transaction Documents, including the provision stating that the exchange ratio would be calculated based on the number of shares of ApolloMed’s common stock issued and outstanding at closing (which was not likely to be consistent with the exchange ratio assumption that ApolloMed was directing BofA Merrill Lynch to base its fairness opinion on because the number of shares of ApolloMed’s common stock issued and outstanding at closing was likely to be different) as well as other recent revisions to the Merger Agreement.
| 126 |
The meeting was adjourned. After the meeting was reconvened later that evening, representatives from BofA Merrill Lynch reviewed its updated financial analyses and rendered its oral opinion, which was subsequently confirmed in writing on December 21, 2016, to the ApolloMed board that, as of the date of the meeting and based upon and subject to the various assumptions and limitations described in such opinion, including the assumption made at the direction of ApolloMed that the exchange ratio would be the assumed exchange ratio, the assumed exchange ratio was fair, from a financial point of view to ApolloMed. Following these presentations and the opportunity for further discussion among the directors about the transaction, after careful deliberation, the ApolloMed board determined that the proposed business combination, based on a 82% (for NMM’s former shareholders) / 18% (for ApolloMed’s existing stockholders) ownership split of the total issued and outstanding shares of ApolloMed’s common stock at closing (after giving effect to the Merger and assuming there would be no dissenting NMM shareholders at closing), was fair to and in the best interests of ApolloMed and its stockholders, approved the Merger Agreement and other Transaction Documents, authorized ApolloMed management to finalize and execute the Merger Agreement and other Transaction Documents (substantially in the form presented to the ApolloMed board) and to consummate the transactions contemplated thereby, and resolved to recommend that ApolloMed stockholders adopt and approve the Transaction Documents and the transactions contemplated hereby, including the Merger.
In reaching its decision, the ApolloMed board placed substantial weight on the benefit of the proximity of the two companies’ existing operations in post-merger integration and expansion, the prospect of bringing together two leading, complementary healthcare organizations to form one of the nation’s largest integrated population health management companies, which would be well positioned for the ongoing transition of U.S. healthcare to value-based reimbursements (fee for value) from volume-based care.
On December 20, 2016, at a meeting of the NMM board held to evaluate the business combination, Vantage Point rendered to the NMM board an oral opinion, which was confirmed by delivery of a written opinion signed and dated December 21, 2016, to the effect that, as of the date of the opinion, and based upon and subject to the factors, assumptions and limitations set forth therein, the exchange ratio pursuant to the Merger Agreement was fair, from a financial point of view, to NMM and its shareholders. At the meeting, the NMM board determined that the proposed business combination was in the best interests of NMM and its shareholders and authorized NMM management to finalize and execute the Merger Agreement, substantially in the form presented to the NMM board.
In reaching its decision, the NMM board took into consideration, among other factors, that the Merger would allow NMM shareholders to monetize their investment in NMM through owning stock in a publicly-traded company and would enable the combined company to pursue and execute growth opportunities at an expedited pace.
On December 21, 2016, ApolloMed and NMM executed the Merger Agreement. The entry into the Merger was announced on December 22, 2016 in a joint press release issued by ApolloMed and NMM.
On January 3, 2017, NMM provided the $5 million working capital loan to ApolloMed, which was evidenced by a promissory note requiring repayment on a quarterly basis from February 1, 2017 to the end of January 2019 (the “Original Note”).
On March 30, 2017, upon approval by their respective boards, ApolloMed and NMM executed an amendment to the Merger Agreement in connection with a third-party debt financing that ApolloMed entered into after execution of the Merger Agreement. In connection with such third-party debt financing, which included a guaranty to be provided by NMM, ApolloMed issued a convertible promissory note in consideration for an approximately $5 million working capital loan. Pursuant to the Merger Agreement amendment, certain shares of ApolloMed’s common stock, including shares issuable to such lender upon conversion of the note, would not be taken into account for purposes of calculating the final exchange ratio at closing of the Merger. In consideration for excluding the shares issuable upon conversion of the note from the calculation of the shares of ApolloMed’s common stock to be issued to NMM shareholders at closing of the Merger and NMM’s guaranty, ApolloMed agreed to issue to NMM shareholders, at closing of the Merger, as part of the merger consideration, warrants to purchase 850,000 shares of ApolloMed’s common stock at an exercise price of $11.00 per share.
| 127 |
The Merger had not closed by August 31, 2017, the date after which the Merger Agreement was terminable by either party under certain circumstances. Due to its financial condition, ApolloMed began seeking additional financing from NMM and an extension on the payment maturity date under its existing loan with NMM. In September 2017, the parties began discussing possible amendments to the Merger Agreement and a new convertible note to replace the existing five million dollar working capital loan between NMM and ApolloMed, evidenced by the Original Note. During the course of negotiations, ApolloMed received an unsolicited acquisition offer from a NASDAQ-listed company and both ApolloMed and NMM sought and received consent in connection with alternative acquisition proposals. The ApolloMed board met on various occasions throughout September to discuss the financial needs of ApolloMed, the status of negotiations with NMM and actions to be taken in connection with the unsolicited acquisition offer.
On October 15, 2017, a meeting of the ApolloMed board was held to evaluate the proposed (i) amendment to the Merger Agreement (“Amendment No. 2”), (ii) amendment to the existing Alliance Note (the “Alliance Note Amendment”) and (iii) restatement of the Original Note with NMM (the “Restated NMM Note”). At the meeting, the ApolloMed board determined that the proposed transactions were in the best interests of ApolloMed and its stockholders and authorized ApolloMed management to finalize and execute Amendment No. 2, the Restated NMM Note, the Alliance Note Amendment and related documentation.
In connection with the amendments to the Merger Agreement, neither ApolloMed nor NMM sought updated fairness opinions due to timing and cost considerations.
Pursuant to Amendment No. 2, the merger consideration was amended to provide that each outstanding share of NMM common stock will be converted into the right to receive such number of shares of ApolloMed common stock that would result in the NMM shareholders having a right to receive (i) an aggregate number of shares of ApolloMed common stock that represents 82% of the total issued and outstanding shares of ApolloMed common stock immediately following the consummation of the Merger (assuming there are no NMM dissenting shareholder interests as of the effective time of the Merger), plus (ii) an aggregate of 2,566,666 shares of ApolloMed common stock. In addition, Amendment No. 2 provides that each NMM shareholder will be entitled to receive such shareholder’s pro rata portion of (i) warrants to purchase an aggregate of 850,000 shares of ApolloMed common stock exercisable at $11.00 per share and (ii) warrants to purchase an aggregate of 900,000 shares of ApolloMed common stock exercisable at $10.00 per share. Amendment No. 2 contains other changes, including provisions extending the End Date to March 31, 2018.
Amendment No. 2 also contemplates NMM to provide a new working capital loan in the amount of $9,000,000, which is convertible into shares of common stock of ApolloMed at $10 per share. Of the principal amount, (A) $5,000,000 is required to be used to refinance the Original Note and (B) $4,000,000 is to be used for working capital. The Restated NMM Note cancels and replaces the Original Note.
In addition, under the terms of the Restated NMM Note, in the event that ApolloMed fails to repay the Alliance Note in full when due, NMM agrees and undertakes to pay Alliance all amounts owed by ApolloMed to Alliance or enter into another agreement with Alliance. The Restated NMM Note has also been amended and restated to include (i) an extension of the maturity date to the earlier of (A) March 31, 2019 or (B) 12 months after the date the Merger Agreement is terminated, (ii) the increase in the principal amount of the Restated NMM Note to $13,990,000 if ApolloMed fails to pay the Alliance Note and NMM either pays all amounts owed under the Alliance Note or enters into another agreement with Alliance (such that in either case the Alliance Note is cancelled) and (iii) a conversion feature allowing the Restated NMM Note to be converted into shares of ApolloMed common stock at $10.00 per share with such conversion, if exercised in accordance with the terms of the Restated NMM Note, becoming effective on the maturity date.
| 128 |
ApolloMed’s Reasons for the Merger
In approving and authorizing the Merger Agreement and the Merger, the ApolloMed board of directors considered a number of factors. Although the following discussion sets forth the material factors considered by the ApolloMed board of directors in reaching its determination, it may not include all of the factors considered by the ApolloMed board. In light of the number and wide variety of factors considered in connection with its evaluation of the Merger Agreement and the Merger, the ApolloMed board of directors did not consider it practicable to, and did not attempt to, quantify or otherwise assign relative weights to the specific factors it considered in reaching its determination. The ApolloMed board of directors viewed its position and determinations as being based on all of the information available and the factors presented to and considered by it. In addition, individual directors may have given different weight to different factors.
In evaluating the Merger Agreement and the Merger, the ApolloMed board of directors consulted with ApolloMed’s management and legal and financial advisors, reviewed a significant amount of information, and considered a number of factors, including, among others, the following factors that the ApolloMed board viewed as supportive of its decision, to approve the Merger Agreement and the Merger, as being advisable, fair and in the best interests of ApolloMed and the ApolloMed’s stockholders:
| · | the likelihood of increased scale, including financial, clinical, network size and operational attributes, which would create near and long-term value for both ApolloMed stockholders and NMM shareholders; |
| · | historical and current financial condition of ApolloMed and NMM and the ability to take on more strategic risk and have less stockholder risk; |
| · | the combined company’s increased management expertise following the Merger; |
| · | historical and current financial market conditions; |
| · | the highly strategic nature of the Merger, which would combine two physician-driven companies to create one of the nation’s leading physician services organizations, offering end-to-end solutions; |
| · | savings opportunity to migrate ApolloMed to value-based reimbursement; |
| · | ApolloMed’s liquidity position; |
| · | the likelihood of establishing a leading position in the population health management setting; |
| · | ApolloMed’s historical stock prices and trading volumes; |
| · | the capability to manage patient care and influence high-quality at lower costs across the continuum of care; |
| · | the possibility of geographic expansion; |
| · | the likelihood of growth opportunities from combining highly synergistic operational expertise and capabilities with highly complementary physician-centric cultures, management and clinical capabilities; |
| · | the ability to leverage technology and data expenditures and platforms; |
| · | historical and current information concerning NMM’s business, operations and management and the results of the due diligence investigation of NMM conducted by ApolloMed’s management and advisors; |
| 129 |
| · | increased demand for “bundled” services, hospitalist and post-acute care services; |
| · | the combined company’s steady EBITDA streams, which enables the combined company to uplist to NASDAQ in connection with the Merger; |
| · | the ability to raise additional capital; |
| · | the potential for increased cash flow; |
| · | ApolloMed’s ability to commence new CMS and payor programs while protecting against any reimbursement changes following the Merger; |
| · | the likelihood of retaining key NMM employees to manage the combined company; |
| · | the likelihood that the Merger will be consummated on a timely basis; |
| · | the possibility that the combined entity would be able to take advantage of the potential benefits resulting from the combination of the ApolloMed public company infrastructure and experienced NMM management team and board and business know-how; |
| · | the prospect of receiving a working capital loan in the principal amount of $5,000,000 from NMM within five business days following the execution of the Merger Agreement pursuant to the terms of the Merger Agreement; and |
| · | the opinion of BofA Merrill Lynch, dated December 21, 2016, to ApolloMed’s board of directors as to the fairness, from a financial point of view and as of the date of the opinion, of the exchange ratio to ApolloMed, assuming, at the direction of ApolloMed, that the exchange ratio would be 0.07002656301, as more fully described below in the section entitled “Opinion of ApolloMed’s Financial Advisor.” |
The ApolloMed board of directors also carefully considered and discussed a number of risks, uncertainties, and other countervailing factors in its deliberations regarding entering into the Merger Agreement and consummating the Merger, including, among others, the following:
| · | the risk that the conditions to the Merger will not be satisfied; |
| · | the risks and substantial costs, including public company costs, and the difficulty of obtaining additional financing on terms favorable to ApolloMed or at all to cover such costs of ApolloMed remaining a stand-alone publicly traded company, instead of agreeing to a transaction with NMM; |
| · | the uncertainty of the trading price of ApolloMed common stock after announcing the Merger and after closing the Merger; |
| · | the possibility that the anticipated benefits of the Merger may not be realized or may be lower than expected; |
| · | the potential limitations on ApolloMed’s operations due to pre-closing covenants in the Merger Agreement; |
| · | the effect of the public announcement of the Merger on ApolloMed’s operations, stock price, and employees; |
| · | the disruption that may be caused by failure to complete the Merger; |
| · | the substantial fees and expenses incurred by ApolloMed in connection with the Merger, which will be incurred whether or not the Merger is completed; and |
| · | other risks described in the sections entitled “Risk Factors” and “Forward-Looking Statements” beginning on page 44 and 100, respectively, of this joint proxy statement/prospectus. |
| 130 |
The ApolloMed board of directors believes that, overall, the potential benefits to ApolloMed stockholders of the Merger Agreement, the Merger and the other transactions contemplated thereby outweigh the risks and uncertainties.
Although this discussion of the information and factors considered by the ApolloMed board of directors is believed to include the material factors it considered, it is not intended to be exhaustive and may not include all of the factors considered by the ApolloMed board. The ApolloMed board of directors did not find it useful and did not attempt to quantify or assign any relative or specific weights to the various factors that it considered in reaching its determination that the Merger Agreement and the transactions contemplated thereby are fair to, advisable, and in the best interests of ApolloMed and its stockholders. The ApolloMed board of directors based its determination on the totality of the information presented to and factors considered by it. In addition, individual members of the ApolloMed board may have given differing weights to different factors.
In approving and authorizing the Merger Agreement and the Merger, the NMM board of directors considered a number of factors. Although the following discussion sets forth the material factors considered by the NMM board of directors in reaching its determination, it may not include all of the factors considered by the NMM board. In light of the number and wide variety of factors considered in connection with its evaluation of the Merger Agreement and the Merger, the NMM board of directors did not consider it practicable to, and did not attempt to, quantify or otherwise assign relative weights to the specific factors it considered in reaching its determination. The NMM board of directors viewed its position and determinations as being based on all of the information available and the factors presented to and considered by it. In addition, individual directors may have given different weight to different factors.
In evaluating the Merger Agreement and the Merger, the NMM board of directors consulted with NMM’s management and legal and financial advisors, reviewed a significant amount of information, and considered a number of factors, including, among others, the following factors that the NMM board viewed as supportive of its decision, to approve the Merger Agreement and the Merger, as being advisable, fair and in the best interests of NMM and the NMM’s shareholders:
| · | the Merger will allow NMM shareholders to monetize their investment in NMM, providing the NMM shareholders with the ability to obtain liquidity in the form of registered shares of ApolloMed common stock, subject to the restrictions set forth in the Merger Agreement; |
| · | the inclusion of ApolloMed common stock in the merger consideration provides NMM shareholders the ability to participate in the future results of the combined company; |
| · | the expectation that the combined company will provide additional and significant sources of capital growth essential to execute NMM’s vision of transforming the national healthcare delivery system; |
| · | NMM will be able to pursue growth opportunities more quickly and easily than it could as a private company, including: (1) market and geographic expansion and (2) enhanced business development capabilities; |
| · | the Merger presents an opportunity to partner with a mission and values driven organization that can augment NMM’s values and culture; |
| · | the possible strategic alternatives to the Merger, including continuing as a standalone company, an initial public offering, private equity financing, or a sale or merger with other parties, were evaluated by the NMM board with the assistance of management, and the NMM board determined such alternatives were less favorable to NMM and the NMM shareholders than the Merger given the potential risks, rewards, and uncertainties associated with those alternatives; |
| · | NMM management will stay in place following the consummation of the Merger; |
| 131 |
| · | the belief that the combined company will have an increased ability to attract and retain management and medical professionals; |
| · | the expectation that the combined company will have a greater opportunity to impact healthcare public policy than NMM has on a standalone basis; and |
| · | the likelihood that the Merger would be completed, based on, among other things: |
| o | the absence of significant required regulatory approvals, other than those relating to the HSR Act; |
| o | Apollo’s obligation to pay NMM a $1.5 million termination fee if the Merger Agreement is terminated under certain circumstances; and |
| o | the reputation and financial capacity of ApolloMed. |
In the course of its deliberations, the NMM board also considered a variety of risks and other countervailing factors related to entering into the Merger Agreement, including, without limitation, the following:
| · | the fact that NMM will no longer be an independent company and the concern that it will not have autonomy in its decision-making; |
| · | the risk that the Merger could compromise or diminish NMM’s distinctive physician-owned, physician-led culture and business model, including the potential impact on current employees, affiliated physicians, and physician group and IPA consolidation opportunities; |
| · | the potential negative consequences that could result from public visibility into NMM’s financial statements; |
| · | the fact that the number of shares of ApolloMed common stock offered as consideration is fixed and therefore the total merger consideration at the time of closing may have a greater or lesser value than at the time the Merger Agreement was signed; |
| · | the risk that the Merger might not be completed in a timely manner or at all; |
| · | the risks and costs to NMM if the Merger does not close, including the diversion of management and employee attention and the potential effect on NMM’s business and its relationships with payors and physicians; |
| · | the restrictions on the conduct of NMM’s business prior to the completion of the Merger, which may delay or prevent NMM from undertaking business opportunities that may arise and certain other actions it might otherwise take with respect to its operations pending completion of the Merger; |
| · | the risk that, while the Merger is expected to be completed, there can be no assurance that all conditions to the parties’ obligations to complete the Merger will be satisfied, and as a result, it is possible that the Merger may not be completed even if it is approved by the NMM shareholders; and |
| · | other risks described in the sections entitled “Risk Factors” and “Forward-Looking Statements” beginning on page 44 and 100, respectively, of this joint proxy statement/prospectus. |
The NMM board of directors believes that, overall, the potential benefits to NMM shareholders of the Merger Agreement, the Merger and the other transactions contemplated thereby outweigh the risks and uncertainties.
Although this discussion of the information and factors considered by the NMM board of directors is believed to include the material factors it considered, it is not intended to be exhaustive and may not include all of the factors considered by the NMM board. The NMM board of directors did not find it useful and did not attempt to quantify or assign any relative or specific weights to the various factors that it considered in reaching its determination that the Merger Agreement and the transactions contemplated thereby are fair to, advisable, and in the best interests of NMM and its shareholders. The NMM board of directors based its determination on the totality of the information presented to and factors considered by it. In addition, individual members of the NMM board may have given differing weights to different factors.
| 132 |
Opinion of ApolloMed’s Financial Advisor
ApolloMed has retained BofA Merrill Lynch to act as ApolloMed’s financial advisor in connection with the Merger. BofA Merrill Lynch is an internationally recognized investment banking firm which is regularly engaged in the valuation of businesses and securities in connection with mergers and acquisitions, negotiated underwritings, secondary distributions of listed and unlisted securities, private placements and valuations for corporate and other purposes. ApolloMed selected BofA Merrill Lynch to act as ApolloMed’s financial advisor in connection with the Merger on the basis of BofA Merrill Lynch’s experience in transactions similar to the Merger and its reputation in the investment community.
On December 21, 2016, at a meeting of ApolloMed’s board of directors held to evaluate the Merger, BofA Merrill Lynch delivered to ApolloMed’s board of directors an oral opinion, which was confirmed by delivery of a written opinion dated December 21, 2016 to the effect that, as of the date of the opinion and based on and subject to various assumptions and limitations described in its opinion (including the assumption, made at the direction of ApolloMed, of an exchange ratio would be 0.07002656301), the exchange ratio provided for in the Merger was fair, from a financial point of view, to ApolloMed.
The full text of BofA Merrill Lynch’s written opinion to ApolloMed’s board of directors, which describes, among other things, the assumptions made, procedures followed, factors considered and limitations on the review undertaken, is attached as Annex G to this document and is incorporated by reference herein in its entirety. The following summary of BofA Merrill Lynch’s opinion is qualified in its entirety by reference to the full text of the opinion. BofA Merrill Lynch delivered its opinion to ApolloMed’s board of directors for the benefit and use of ApolloMed’s board of directors (in its capacity as such) in connection with and for purposes of its evaluation of the assumed exchange ratio from a financial point of view. BofA Merrill Lynch’s opinion does not address any other aspect of the Merger and no opinion or view was expressed as to the relative merits of the Merger in comparison to other strategies or transactions that might be available to ApolloMed or in which ApolloMed might engage or as to the underlying business decision of ApolloMed to proceed with or effect the Merger. BofA Merrill Lynch’s opinion does not address any other aspect of the Merger and does not constitute a recommendation to any stockholder as to how to vote or act in connection with the proposed Merger or any related matter.
In connection with rendering its opinion, BofA Merrill Lynch:
| (i) | reviewed certain publicly available business and financial information relating to ApolloMed; |
| (ii) | reviewed certain internal financial and operating information with respect to the business, operations and prospects of NMM furnished to or discussed with BofA Merrill Lynch by the management of NMM, including certain financial forecasts relating to NMM prepared by the management of NMM, referred to herein as NMM management forecasts; |
| (iii) | reviewed certain internal financial and operating information with respect to the business, operations and prospects of ApolloMed (excluding the NGACO business and MMG IPA business) furnished to or discussed with BofA Merrill Lynch by the management of ApolloMed, including certain financial forecasts relating to ApolloMed (excluding the NGACO business and MMG IPA business) prepared by the management of ApolloMed, referred to herein as ApolloMed management forecasts; |
| (iv) | reviewed certain internal financial and operating information with respect to the business, operations and prospects of the NGACO business furnished to or discussed with BofA Merrill Lynch by the management of ApolloMed, including certain financial forecasts relating to the NGACO business prepared by the management of ApolloMed, referred to herein as NGACO forecasts; |
| (v) | reviewed certain estimates as to the amount and timing of cost savings and revenue enhancements anticipated by the management of ApolloMed to result from the Merger, referred to herein as cost savings; |
| 133 |
| (vi) | reviewed certain information, prepared by the management of ApolloMed, regarding the net operating losses held by ApolloMed and certain estimates regarding the utilization of such net operating losses for U.S. federal income tax purposes, referred to herein as the NOL utilization projections; |
| (vii) | discussed the past and current business, operations, financial condition and prospects of NMM with members of senior managements of NMM and ApolloMed, and discussed the past and current business, operations, financial condition and prospects of ApolloMed with members of senior management of ApolloMed; |
| (viii) | reviewed the potential pro forma financial impact of the Merger on the future financial performance of ApolloMed, including the potential effect on ApolloMed’s estimated earnings per share; |
| (ix) | compared certain financial information of NMM and ApolloMed with similar information of other companies BofA Merrill Lynch deemed relevant; |
| (x) | reviewed a draft, dated December 20, 2016, of the Merger Agreement; and |
| (xi) | performed such other analyses and studies and considered such other information and factors as BofA Merrill Lynch deemed appropriate. |
In arriving at its opinion, BofA Merrill Lynch assumed and relied upon, without independent verification, the accuracy and completeness of the financial and other information and data publicly available or provided to or otherwise reviewed by or discussed with it and relied upon the assurances of the managements of ApolloMed and NMM that they were not aware of any facts or circumstances that would make such information or data inaccurate or misleading in any material respect.
With respect to the NMM management forecasts, BofA Merrill Lynch was advised by NMM, and assumed, with ApolloMed’s consent, that they were reasonably prepared on bases reflecting the best currently available estimates and good faith judgments of the management of NMM as to the future financial performance of NMM. With respect to the NMM management forecasts, BofA Merrill Lynch was advised by ApolloMed, and assumed, that the NMM Forecasts reflect the best currently available estimates and good faith judgments of the management of ApolloMed as to the future financial performance of NMM. With respect to the ApolloMed management forecasts, NGACO forecasts, cost savings and NOL utilization projections, BofA Merrill Lynch was advised by ApolloMed, and assumed, that they were reasonably prepared on bases reflecting the best currently available estimates and good faith judgments of the management of ApolloMed as to the future financial performance of ApolloMed (excluding the NGACO business and MMG IPA business), the NGACO business and the other matters covered thereby. BofA Merrill Lynch relied, at the direction of ApolloMed, on the assessments of the management of ApolloMed as to ApolloMed’s ability to achieve the cost savings and was advised by ApolloMed, and assumed, that the cost savings would be realized in the amounts and at the times projected. BofA Merrill Lynch relied, at the direction of ApolloMed, on the assessments of the management of ApolloMed as to the availability to ApolloMed of the net operating losses set out in the NOL utilization projections and was advised by ApolloMed, and assumed, that the NOL utilization projections would be utilized in the amounts and at the times projected.
BofA Merrill Lynch did not make nor was provided with any independent evaluation or appraisal of the assets or liabilities (contingent or otherwise) of NMM or ApolloMed, nor did it make any physical inspection of the properties or assets of NMM or ApolloMed. BofA Merrill Lynch did not evaluate the solvency or fair value of NMM or ApolloMed under any state, federal or other laws relating to bankruptcy, insolvency or similar matters. BofA Merrill Lynch assumed, at the direction of ApolloMed, that the Merger would be consummated in accordance with its terms, without waiver, modification or amendment of any material term, condition or agreement and that, in the course of obtaining the necessary governmental, regulatory and other approvals, consents, releases and waivers for the Merger, no delay, limitation, restriction or condition, including any divestiture requirements or amendments or modifications, would be imposed that would have an adverse effect on ApolloMed, NMM or the contemplated benefits of the Merger. BofA Merrill Lynch also assumed, at the direction of ApolloMed, that the final executed Merger Agreement would not differ in any material respect from the draft Merger Agreement reviewed by BofA Merrill Lynch.
| 134 |
BofA Merrill Lynch expressed no opinion or view as to any terms or other aspects of the Merger (other than the exchange ratio to the extent expressly specified in its opinion), including, without limitation, the form or structure of the Merger or any ongoing obligations of the parties pursuant to the Merger Agreement. BofA Merrill Lynch’s opinion was limited to the fairness, from a financial point of view, to ApolloMed of the assumed exchange ratio provided for in the Merger and no opinion or view was expressed with respect to any consideration received in connection with the Merger by the holders of any class of securities, creditors or other constituencies of any party. In addition, no opinion or view was expressed with respect to the fairness (financial or otherwise) of the amount, nature or any other aspect of any compensation to any of the officers, directors or employees of any party to the Merger, or class of such persons, relative to the assumed exchange ratio. Furthermore, no opinion or view was expressed as to the relative merits of the Merger in comparison to other strategies or transactions that might be available to ApolloMed or in which ApolloMed might engage or as to the underlying business decision of ApolloMed to proceed with or effect the Merger. BofA Merrill Lynch did not express any opinion as to what the value of ApolloMed common stock actually would be when issued or the prices at which ApolloMed common stock would trade at any time, including following announcement or consummation of the Merger. In addition, BofA Merrill Lynch expressed no opinion or recommendation as to how any stockholder should vote or act in connection with the Merger or any related matter. Except as described above, ApolloMed imposed no other limitations on the investigations made or procedures followed by BofA Merrill Lynch in rendering its opinion.
BofA Merrill Lynch’s opinion was necessarily based on financial, economic, monetary, market and other conditions and circumstances as in effect on, and the information made available to BofA Merrill Lynch as of, the date of its opinion. It should be understood that subsequent developments may affect its opinion, and BofA Merrill Lynch does not have any obligation to update, revise or reaffirm its opinion. The issuance of BofA Merrill Lynch’s opinion was approved by a fairness opinion review committee of BofA Merrill Lynch.
The discussion set forth below in the sections entitled “Selected Publicly Traded Companies Analysis”, “Discounted Cash Flow Analysis”, and “Relative Valuation” below represents a brief summary of the material financial analyses presented by BofA Merrill Lynch to ApolloMed’s board of directors in connection with its opinion. The financial analyses summarized below include information presented in tabular format. In order to fully understand the financial analyses performed by BofA Merrill Lynch, the tables must be read together with the text of each summary. The tables alone do not constitute a complete description of the financial analyses performed by BofA Merrill Lynch. Considering the data set forth in the tables below without considering the full narrative description of the financial analyses, including the methodologies and assumptions underlying the analyses, could create a misleading or incomplete view of the financial analyses performed by BofA Merrill Lynch.
Selected Publicly Traded Companies Analysis
BofA Merrill Lynch reviewed the NMM management forecasts for NMM, the ApolloMed management forecasts for ApolloMed, the following four publicly traded companies in the physician services sector, and the following three publicly traded companies in the high growth healthcare services sector, that, in the professional judgment of BofA Merrill Lynch, have businesses that for the purposes of this analysis may be considered similar to those of ApolloMed:
Physician Services Sector (“PSS”)
| · | DaVita Inc.; |
| · | Envision Healthcare Corporation; |
| · | MEDNAX Inc; and |
| · | Team Health Holdings Inc.* |
| * | All TeamHealth Inc. statistics are as of October 3, 2016, the last trading day prior to news reports that TeamHealth was considering a possible sale of the Company. |
High Growth Healthcare Services Sector (“HG”)
| · | American Renal Associates LLC; |
| · | Diplomat Pharmacy, Inc.; and |
| · | ExamWorks, Inc.* |
| * | All ExamWorks statistics are as of April 26, 2016, the last trading day prior to an acquisition announcement. |
| 135 |
For purposes of the analysis, BofA Merrill Lynch analyzed the following operational and trading statistics for ApolloMed, NMM and each of the selected publicly traded companies for comparison purposes (other than 2017E EV / EBITDA for which no statistics were analyzed for ApolloMed or NMM):
| · | estimated calendar year 2016 to estimated calendar year 2018 revenue compound annual growth rate (“CAGR”), referred to as 2016E – 2018E Revenue CAGR; |
| · | estimated calendar year 2016 to estimated calendar year 2018 earnings before interest, taxes, depreciation and amortization (“EBITDA”) CAGR, referred to as 2016E – 2018E EBITDA CAGR; |
| · | estimated calendar year 2017 EBITDA margin, referred to as 2017E EBITDA Margin; |
| · | estimated calendar year 2016 to estimated calendar year 2018 estimated earnings per share CAGR, referred to as 2016E – 2018E EPS CAGR; and |
| · | enterprise value (“EV”), calculated as the market value of equity based on closing stock prices on December 20, 2016 on a fully diluted basis, plus debt, less cash and equivalents, plus non-controlling interests, as a multiple of calendar year 2017 estimated EBITDA, referred to as 2017E EV / EBITDA. |
| High* | Low* | Median* | ||||||||||||||||||||||||||||||
| PSS | HG | PSS | HG | PSS | HG | ApolloMed | NMM | |||||||||||||||||||||||||
| 2016E – 2018E Revenue CAGR | 9.7 | % | 15.7 | % | 5.4 | % | 10.7 | % | 8.0 | % | 14.6 | % | 291.7 | % | 8.0 | % | ||||||||||||||||
| 2016E – 2018E EBITDA CAGR | 11.9 | % | 15.9 | % | 4.8 | % | 9.6 | % | 10.9 | % | 14.4 | % | 145.9 | % | 19.4 | % | ||||||||||||||||
| 2017E EBITDA Margin | 21.5 | % | 27.6 | % | 10.9 | % | 2.1 | % | 17.1 | % | 17.7 | % | 2.9 | % | 14.4 | % | ||||||||||||||||
| 2016E – 2018E EPS CAGR | 15.9 | % | 45.0 | % | 7.5 | % | 9.3 | % | 12.0 | % | 14.7 | % | 151.9 | % | 22.5 | % | ||||||||||||||||
| 2017E EV / EBITDA | 10.4 | x | 11.1 | x | 8.4 | x | 8.7 | x | 8.9 | x | 9.0 | x | - | - | ||||||||||||||||||
Notes: * = excludes ApolloMed and NMM.
After taking into consideration the observed data for the selected publicly traded companies, ApolloMed and NMM, BofA Merrill Lynch then applied 2017E EV / EBITDA multiples of 8.0x to 9.0x derived from the selected publicly traded companies to calendar year 2017 estimated EBITDA for ApolloMed and NMM from the ApolloMed management forecasts and NGACO forecasts in respect of ApolloMed, and the NMM management forecasts in respect of NMM.
This analysis indicated the following approximate implied equity per share value reference range (rounded to the nearest $0.05) for ApolloMed and implied equity value reference ranges for ApolloMed and NMM, as compared to the price of ApolloMed’s shares as of December 20, 2016:
| Implied Per Share Equity Value Reference Range |
Implied Equity Value Reference Range (mm) |
Share Price as of December 20, 2016 |
||||||
| ApolloMed | $4.75 - $5.20 | $37.2 - $41.5 | $3.99 | |||||
| NMM | - | $280 - $313 | - | |||||
No company used in this analysis is identical or directly comparable to NMM or ApolloMed. Accordingly, an evaluation of the results of this analysis is not entirely mathematical. Rather, this analysis involves complex considerations and judgments concerning differences in financial and operating characteristics and other factors that could affect the public trading or other values of the companies to which ApolloMed and NMM were compared.
Discounted Cash Flow Analysis
BofA Merrill Lynch performed a discounted cash flow analysis of ApolloMed and NMM to calculate the estimated present value of the standalone unlevered, after-tax free cash flows that ApolloMed and NMM were forecasted to generate during the last quarter of 2016 through calendar year 2025 based on the ApolloMed management forecasts and NGACO forecasts in respect of ApolloMed, and the NMM management forecasts in respect of NMM.
BofA Merrill Lynch calculated terminal values for ApolloMed (excluding the NGACO business) by applying a perpetuity growth rate of 3.0% to 4.0% to ApolloMed’s terminal year estimated unlevered, after-tax free cash flows (excluding the NGACO business). The unlevered free cash flows and range of terminal values were then discounted to present value as of September 30, 2016 using discount rates ranging from 17.50% to 19.00%, which were based on an estimate of ApolloMed’s discount rate (excluding the NGACO business).
| 136 |
BofA Merrill Lynch also calculated terminal values for the NGACO business by applying a perpetuity growth rate of 3.0% to 4.0% to the NGACO business’s terminal year estimated unlevered, after-tax free cash flows. The unlevered free cash flows and range of terminal values were then discounted to present value as of September 30, 2016 using discount rates ranging from 25.0% to 30.0%, which were based on an estimate of the NGACO business’ discount rate.
BofA Merrill Lynch also calculated terminal values for NMM by applying a perpetuity growth rate of 3.0% to 4.0% to NMM’s terminal year estimated unlevered, after-tax free cash flows. The unlevered free cash flows and range of terminal values were then discounted to present value as of September 30, 2016 using discount rates ranging from 8.50% to 9.50%, which were based on an estimate of NMM’s discount rate.
This analysis indicated the following approximate implied per share equity value reference ranges for 50% of the NGACO business, ApolloMed (excluding the NGACO business) and ApolloMed and implied equity value reference ranges for 50% of the NGACO business, ApolloMed, NMM (excluding the NGACO business) and, as compared to the price of ApolloMed’s shares as of December 20, 2016:
| Implied Per Share Equity Value Reference Range |
Implied Equity Value Reference Range (mm) |
Share Price as of December 20, 2016 |
||||||
| 50% of NGACO | $3.86 - $5.06 | $32 - $43 | - | |||||
| ApolloMed (ex-50% NGACO) | $3.73 - $4.15 | - | - | |||||
| ApolloMed | $7.60 - $9.20 | $63.1 - $77.9 | $3.99 | |||||
| NMM (ex-50% NGACO) | - | $242 - $336 | - | |||||
| NMM | - | $274 - $379 | - | |||||
Relative Valuation
Based on implied equity value reference ranges for ApolloMed and NMM calculated as described above in the sections entitled “Selected Publicly Traded Companies Analysis” and “Discounted Cash Flow Analysis”, BofA Merrill Lynch calculated implied exchange ratios resulting from one share of NMM being converted into shares of ApolloMed, with the top of the range being based on the highest NMM implied equity value and the lowest ApolloMed implied equity value and the bottom of the range based on the lowest NMM implied equity value and the highest ApolloMed implied equity value. These analyses indicated the following implied exchange ratio reference ranges, in each case as compared to the assumed exchange ratio of 0.07002656301 (rounded to 0.070x below):
| Implied exchange ratio reference ranges based on: | ||||
| Selected Publicly Traded Companies | Discounted Cash Flow Analysis | Assumed exchange ratio | ||
| 0.104x - 0.129x | 0.054x – 0.092x | 0.070x | ||
Contribution Analysis
BofA Merrill Lynch calculated the relative contributions of ApolloMed and NMM to the combined company of projected revenue, projected EBITDA, and net income, in each case less non-controlling interests (“NCI”), for calendar years 2017 through 2019 using the ApolloMed management forecasts and NGACO forecasts in respect of ApolloMed, and the NMM management forecasts in respect of NMM. Associated implied equity ownership and exchange ratios were derived from the relative contributions taking into account the capital structure of ApolloMed and NMM. Pro forma ownership was derived from the assumption made at the direction of ApolloMed that the exchange ratio would be 0.07002656301 and the equity data provided by ApolloMed management. The analysis indicated the following individually calculated contribution percentages for revenue, EBITDA, and GAAP net income, for each of the calendar years 2017 through 2019, in each case as compared to the assumed exchange ratio of 0.07002656301 (rounded to 0.070x below):
| 137 |
| Contribution | Implied % Equity Ownership |
Implied | Assumed exchange |
|||||||||||||||||||||||
| ApolloMed | NMM | ApolloMed | NMM | exchange ratio | ratio | |||||||||||||||||||||
| Revenue less NCI | 2017E | 53 | % | 47 | % | 42 | % | 58 | % | 0.021 | x | 0.070 | x | |||||||||||||
| 2018E | 52 | % | 48 | % | 42 | % | 58 | % | 0.021 | x | 0.070 | x | ||||||||||||||
| 2019E | 52 | % | 48 | % | 42 | % | 58 | % | 0.021 | x | 0.070 | x | ||||||||||||||
| EBITDA less NCI | 2017E | 11 | % | 89 | % | 11 | % | 89 | % | 0.122 | x | 0.070 | x | |||||||||||||
| 2018E | 24 | % | 76 | % | 22 | % | 78 | % | 0.055 | x | 0.070 | x | ||||||||||||||
| 2019E | 27 | % | 73 | % | 25 | % | 75 | % | 0.046 | x | 0.070 | x | ||||||||||||||
| Net Income less NCI | 2017E | 10 | % | 90 | % | 10 | % | 90 | % | 0.138 | x | 0.070 | x | |||||||||||||
| 2018E | 26 | % | 74 | % | 26 | % | 74 | % | 0.043 | x | 0.070 | x | ||||||||||||||
| 2019E | 31 | % | 69 | % | 31 | % | 69 | % | 0.034 | x | 0.070 | x | ||||||||||||||
| Pro Forma Ownership | 18 | % | 82 | % | 18 | % | 82 | % | 0.070 | x | 0.070 | x | ||||||||||||||
Pro Forma Accretion/Dilution Analysis
BofA Merrill Lynch reviewed the potential pro forma financial effect of the Merger on ApolloMed’s calendar years 2017 through 2019 estimated EPS. Estimated financial data of NMM were based on the NMM management forecasts and estimated financial data of ApolloMed were based on the ApolloMed management forecasts and NGACO forecasts. Based on the assumed exchange ratio, this analysis indicated that the Merger could be accretive to ApolloMed’s estimated EPS for calendar year 2017 by $0.35 and dilutive to ApolloMed’s estimated EPS for calendar year 2018 by $0.10 and calendar year 2019 by $0.33. The actual results achieved by the combined company may vary from projected results and the variations may be material.
Other Factors
In rendering its opinion, BofA Merrill Lynch also reviewed and considered other factors, including historical trading prices and trading volumes of ApolloMed common stock during the one-year period ended December 20, 2016.
Miscellaneous
As noted above, the discussion set forth above in the sections entitled “Selected Publicly Traded Companies Analysis”, “Discounted Cash Flow Analysis”, and “Relative Valuation” is a summary of the material financial analyses presented by BofA Merrill Lynch to ApolloMed’s board of directors in connection with its opinion and is not a comprehensive description of all analyses undertaken by BofA Merrill Lynch in connection with its opinion. The preparation of a financial opinion is a complex analytical process involving various determinations as to the most appropriate and relevant methods of financial analysis and the application of those methods to the particular circumstances and, therefore, a financial opinion is not readily susceptible to partial analysis or summary description. BofA Merrill Lynch believes that its analyses summarized above must be considered as a whole. BofA Merrill Lynch further believes that selecting portions of its analyses and the factors considered or focusing on information presented in tabular format, without considering all analyses and factors or the narrative description of the analyses, could create a misleading or incomplete view of the processes underlying BofA Merrill Lynch’s analyses and opinion. The fact that any specific analysis has been referred to in the summary above is not meant to indicate that such analysis was given greater weight than any other analysis referred to in the summary.
In performing its analyses, BofA Merrill Lynch considered industry performance, general business and economic conditions and other matters, many of which are beyond the control of ApolloMed and NMM. The estimates of the future performance of ApolloMed and NMM in or underlying BofA Merrill Lynch’s analyses are not necessarily indicative of actual values or actual future results, which may be significantly more or less favorable than those estimates or those suggested by BofA Merrill Lynch’s analyses. These analyses were prepared solely as part of BofA Merrill Lynch’s analysis of the fairness, from a financial point of view, of the assumed exchange ratio and were provided to ApolloMed’s board of directors in connection with the delivery of BofA Merrill Lynch’s opinion. The analyses do not purport to be appraisals or to reflect the prices at which a company might actually be sold or the prices at which any securities have traded or may trade at any time in the future. Accordingly, the estimates used in, and the ranges of valuations resulting from, any particular analysis described above are inherently subject to substantial uncertainty and should not be taken to be BofA Merrill Lynch’s view of the actual values of NMM or ApolloMed.
| 138 |
The type and amount of consideration payable in the Merger was determined through negotiations between ApolloMed and NMM, rather than by any financial advisor, and was approved by ApolloMed’s board of directors. The decision to enter into the Merger Agreement was solely that of ApolloMed’s board of directors. As described above, BofA Merrill Lynch’s opinion and analyses were only one of many factors considered by ApolloMed’s board of directors in its evaluation of the proposed Merger and should not be viewed as determinative of the views of ApolloMed’s board of directors or management with respect to the Merger or the exchange ratio.
ApolloMed has agreed to pay BofA Merrill Lynch for its services in connection with the Merger a fee of $750,000 that was payable on the rendering of the opinion, a fee of $2,000,000 that is payable immediately prior to or upon closing of the Merger, and an additional fee in an amount up to $500,000 as determined in the sole discretion of ApolloMed based on its good faith evaluation of the services provided by BofA Merrill Lynch under its engagement, payable immediately prior to or upon closing of the Merger. ApolloMed also has agreed to reimburse BofA Merrill Lynch for its expenses incurred in connection with BofA Merrill Lynch’s engagement and to indemnify BofA Merrill Lynch, any of its affiliates, its and their respective directors, officers, employees and agents and each other person controlling BofA Merrill Lynch or any of its affiliates against specified liabilities, including liabilities under the federal securities laws.
BofA Merrill Lynch and its affiliates comprise a full service securities firm and commercial bank engaged in securities, commodities and derivatives trading, foreign exchange and other brokerage activities, and principal investing as well as providing investment, corporate and private banking, asset and investment management, financing and financial advisory services and other commercial services and products to a wide range of companies, governments and individuals. In the ordinary course of their businesses, BofA Merrill Lynch and its affiliates may invest on a principal basis or on behalf of customers or manage funds that invest, make or hold long or short positions, finance positions or trade or otherwise effect transactions in equity, debt or other securities or financial instruments (including derivatives, bank loans or other obligations) of ApolloMed, NMM and certain of their respective affiliates (including Fresenius SE & Co KGaA and Fresenius Medical Care Corporation (each and together, “Fresenius”)), affiliates of NNA of Nevada, Inc., a shareholder in ApolloMed.
BofA Merrill Lynch and its affiliates in the past have provided, currently are providing, and in the future may provide, investment banking, commercial banking and other financial services to Fresenius and certain of its affiliates and have received or in the future may receive compensation for the rendering of these services, including having acted or acting as joint bookrunner, co-mandated arranger, administrative agent, and collateral agent for, and/or as a lender (including, in some cases, swing line lender and letter of credit lender) to Fresenius and/or certain of its affiliates and having provided or providing certain treasury, derivatives and foreign exchange trading services to Fresenius and certain of its affiliates. From December 1, 2014 through November 30, 2016, BofA Merrill Lynch and its affiliates derived aggregate revenues from Fresenius and its affiliates of approximately $25 million for investment and corporate banking services.
Opinion of NMM’s Financial Advisor
Vantage Point Advisors
On December 20, 2016, at a meeting of the NMM board of directors held to evaluate the Merger, Vantage Point Advisors rendered to the NMM board of directors an oral opinion, which was confirmed by delivery of a written opinion signed and dated December 21, 2016, to the effect that, as of the date of the opinion, and based upon and subject to the factors, assumptions and limitations set forth therein, the Merger was fair, from a financial point of view, to NMM and its common shareholders.
Vantage Point’s opinion was directed to the NMM board of directors and only addressed the fairness, from a financial point of view, of the exchange ratio and did not address any other terms of the Merger. The following summary of Vantage Point’s opinion is qualified in its entirety by reference to the full text of the written opinion, which is attached as Annex H to this joint proxy statement/prospectus, and sets forth the procedures followed, assumptions made, qualifications and limitations of the review undertaken and other matters considered by Vantage Point in preparing its opinion. Vantage Point has consented to the inclusion of its fairness opinion as Annex H to this joint proxy statement/prospectus. However, neither Vantage Point’s opinion nor the summary of its opinion and the related analyses set forth in this joint proxy statement/prospectus are intended to be, and do not constitute, advice or a recommendation to the NMM board of directors, NMM or any shareholder as to how to vote or act in connection with respect to the Merger or any related matter.
| 139 |
In the course of Vantage Point’s analyses for rendering its opinion, among other things, Vantage Point performed the following procedures:
| · | reviewed an execution copy of the Agreement received; |
| · | reviewed NMM’s financial statements, which included audited financial statements for the twelve month periods ended December 31, 2011 through December 31, 2014, unaudited financial statements for the twelve month period ended December 31, 2015 and its unaudited interim financial statements for the nine month periods ended September 30, 2015 and September 30, 2016 (collectively, the "Financial Statements"); |
| · | reviewed ApolloMed’s financial statements as contained in its Form 10-K SEC filings for the 12-month periods ended January 31, 2012 through January 31, 2014, March 31, 2015 and March 31, 2016 and Form 10-Q SEC filings for the 6-month period ended September 30, 2016; |
| · | reviewed NMM Shareholders’ Agreement; |
| · | reviewed an up-to-date list of the names of NMM’s shareholders, including the total number of shares of capital stock of NMM outstanding as of the date hereof; |
| · | reviewed NMM’s board of directors meeting minutes from 2014 through the date hereof; |
| · | reviewed the letter from the CMMI to APAACO dated August 1, 2016 regarding NGACO Model application; |
| · | reviewed various corporate documents related to APAACO; |
| · | reviewed NMM’s schedule of all dividends paid to stockholders and bonuses paid to employees for the period beginning January 1, 2014 and ending November 21, 2016; |
| · | read certain operating and financial information, including projections, provided to Vantage Point by management relating to the business prospects of NMM, ApolloMed and APAACO; |
| · | met with certain members of NMM’s and ApolloMed’s senior and operating management to discuss NMM’s operations, historical financial results and business prospects; |
| · | visited certain of NMM’s facilities in Alhambra, CA; |
| · | visited certain of ApolloMed’s facilities in Glendale, CA; |
| · | read other appraisals involving common stock of NMM; |
| · | evaluated the stock price history and press releases of ApolloMed; |
| · | analyzed certain financial, stock market and other publicly available information relating to the businesses of other companies whose operations and financings we considered relevant in evaluating those of NMM and ApolloMed; and |
| · | conducted such other studies, analyses, inquiries and investigations, as Vantage Point deemed appropriate. |
In arriving at its opinion, Vantage Point assumed and relied upon, without independent verification, the accuracy and completeness of the financial and other information and data publicly available or provided to or otherwise reviewed by or discussed with it and relied upon the assurances of the management of NMM that they were not aware of any facts or circumstances that would make such information or data inaccurate or misleading in any material respect. With respect to the NMM forecasts, Vantage Point was advised by NMM, and assumed that such forecasts were reasonably prepared on bases reflecting the best currently available estimates and good faith judgments of the management of NMM as to the future financial performance of NMM and the other matters covered thereby. Vantage Point did not make or was not provided with any independent evaluation or appraisal of the assets or liabilities (contingent or otherwise) of NMM, nor did it make any physical inspection of the properties or assets of NMM. Vantage Point did not evaluate the solvency or fair value of NMM under any state, federal or other laws relating to bankruptcy, insolvency or similar matters. Vantage Point assumed, at the direction of NMM, that the Merger would be consummated in accordance with its terms, without waiver, modification or amendment of any material term, condition or agreement.
| 140 |
Except as set forth in the opinion, Vantage Point expressed no view or opinion as to any terms or other aspects of the Merger. Vantage Point’s opinion was limited to the fairness, from a financial point of view, of the exchange ratio and no opinion or view was expressed with respect to any consideration received in connection with the Merger by the holders of any other class of securities, creditors or other constituencies of any party. In addition, no opinion or view was expressed with respect to the fairness (financial or otherwise) of the amount, nature or any other aspect of any compensation to any of the officers, directors or employees of any party to the Merger, or class of such persons, relative to the exchange ratio. Furthermore, no opinion or view was expressed as to the relative merits of the Merger in comparison to other strategies or transactions that might be available to NMM or in which NMM might engage or as to the underlying business decision of NMM to proceed with or effect the Merger. In addition, Vantage Point expressed no opinion or recommendation as to how any shareholder should vote or act in connection with the Merger or any related matter.
Vantage Point’s opinion was necessarily based on financial, economic, monetary, market and other conditions and circumstances as in effect on, and the information made available to Vantage Point as of, the date of its opinion. It should be understood that subsequent developments may affect its opinion, and Vantage Point does not have any obligation to update, revise or reaffirm its opinion.
NMM agreed to pay Vantage Point for its services in connection with the Merger an aggregate fee of $410,000. Vantage Point has received no other compensation from NMM or its affiliates during the last two years. NMM also agreed to reimburse Vantage Point for its reasonable expenses and to indemnify Vantage Point against certain liabilities arising out of its engagement. The fee payable to Vantage Point was not contingent on its issuance of a favorable fairness opinion.
NMM selected Vantage Point as a financial advisor in connection with the Merger because of its qualifications, expertise and reputation in valuation opinions related to mergers and acquisitions.
Financial Analyses by Vantage Point
The following is a summary of the material financial analyses delivered by Vantage Point to the NMM board of directors in connection with rendering the fairness opinion described above. The following summary, however, does not purport to be a complete description of the financial analyses performed by Vantage Point, nor does the order of analyses described represent relative importance or weight given to those analyses by Vantage Point. Some of the summaries of the financial analyses include information presented in tabular format. In order to fully understand the financial analyses performed by Vantage Point, the tables must be read together with the full text of each summary and are alone not a complete description of Vantage Point’s financial analyses. Considering the data set forth in the tables below without considering the narrative description of the financial analyses, including the methodologies and assumptions underlying the analyses, could create a misleading or incomplete view of Vantage Point’s financial analyses. Except as otherwise noted, the following quantitative information, to the extent that it is based on market data, is based on market data as it existed on or before December 19, 2016, and is not necessarily indicative of current market conditions.
The preparation of fairness opinions is a complex process involving various determinations as to the most appropriate and relevant methods of financial analysis and the application of those methods to particular circumstances and, therefore, is not necessarily susceptible to partial analysis or summary description. Selecting portions of the analyses or of the summary set forth above, without considering the analyses as a whole, could create an incomplete view of the processes underlying Vantage Point’s opinion. In arriving at its fairness determination, Vantage Point considered the results of all of its analyses and did not attribute any particular weight to any factor or analysis considered by it. Rather, Vantage Point made its determination as to fairness on the basis of its experience and professional judgment after considering the results of all of its analyses. No company or transaction used in the analyses below as a comparison is directly comparable to NMM or the Merger.
| 141 |
Vantage Point prepared these analyses solely for purposes of, and the analyses were delivered to the NMM board of directors in connection with, the provision of its opinion to the NMM board of directors as to the fairness to such holders, from a financial point of view, of the exchange ratio to be received by the holders of NMM common stock pursuant to the Merger Agreement. These analyses do not purport to be appraisals nor do they necessarily reflect or purport to reflect the prices at which businesses or securities actually may be sold or the prices at which any securities have traded or may trade at any time in the future. Analyses based upon forecasts of future results are not necessarily indicative of actual future results, which may be significantly more or less favorable than suggested by these analyses. Because these analyses are inherently subject to uncertainty, being based upon numerous factors or events beyond the control of NMM or its advisor, none of NMM, Vantage Point or any other person assumes responsibility if future results are materially different from those forecast.
The type and amount of consideration payable in the Merger was determined through arm’s-length negotiations between NMM and ApolloMed and its counsel, rather than by Vantage Point, and was approved by the NMM board of directors. Vantage Point did not recommend any specific exchange ratio to the NMM board of directors or to NMM or that any given exchange ratio constituted the only appropriate consideration for the Merger. The decision to enter into the Merger Agreement was solely that of the NMM board of directors. The opinion of financial advisor was one of many factors taken into consideration by the NMM board of directors in its evaluation of the proposed Merger. Consequently, the analyses described below should not be viewed as determinative of the opinion of the NMM board of directors with respect to the exchange ratio or of whether the NMM board of directors would have been willing to determine that a different exchange ratio was fair.
In its analysis of the exchange ratio, Vantage Point performed an analysis of the equity attributable to NMM shareholders before and after giving effect to the transaction and considered the value of the following entities:
| 1) | NMM |
| 2) | ApolloMed |
| 3) | The combined entity |
| 4) | The NGACO, which is a 50/50 joint venture between NMM and ApolloMed. |
Valuation of NMM
Discounted Cash Flow. Vantage Point performed an illustrative discounted cash flow (“DCF”), analysis on NMM using the stand-alone forecast prepared by NMM management to determine a range of implied values of NMM common stock. Vantage Point relied on management’s projections for the years ending December 31, 2016 through December 31, 2019. Vantage Point added an additional year to smooth the growth rate towards the sustainable growth rate and margins to sustainable levels. In estimating NMM’s value into perpetuity Vantage Point utilized the Gordon Growth Method (“GGM”) and the Exit Multiple Method. The GGM assumes the company will continue to grow and generate free cash flows at a consistent rate into perpetuity. The Exit Multiple Method assumes the company will be sold at the end of the projection period and value is estimated by applying an appropriate market multiple to a relevant metric such as EBITDA.
Gordon Growth Method: A sustainable growth rate of 3.0 percent was selected based on historical growth in gross domestic product and industry outlook. A concluded terminal period capitalization rate range of 11.0 percent to 13.0 percent was used, which was derived based on the discount rate range used in the analysis of 14.0 percent to 16.0 percent as reduced by the sustainable growth rate. The discount rate was derived using the weighted average cost of capital (“WACC”). The WACC estimates the weighted average of the cost of equity and the cost of debt. The weight of equity and weight of debt are determined by the target capital structure. The cost of equity was estimated as 18.9 percent and the after-tax cost of debt was estimated as 2.9 percent. The target capital structure was estimated to be 25.0 percent debt and 75.0 percent equity.
Exit Multiple Method: An EBITDA exit multiple range of 5.5 times to 6.5 times was applied to 2020 EBITDA of $35.0 million (as determined by Vantage Point adding an additional forecast year to smooth the growth rate towards the sustainable growth rate and margins to sustainable levels). The exit multiple was selected based on observations of market multiples in the Guideline Company Analysis and Market Transaction Analysis and expected financial performance.
| 142 |
Vantage Point also considered a tax amortization benefit for goodwill, depreciation and amortization, working capital requirements and capital expenditures as provided by management. Based on an income approach analysis, the business enterprise value range from operations was determined to be as follows: $153.0 million to $176.0 million. Adjustments were made by adding back cash of $35.0 million, the value of preferred stock of ApolloMed held by NMM of $17.1 million, the value of warrants in ApolloMed held by NMM of $5.5 million, and the value of NMM’s 50 percent interest in the NGACO of $43.0 million to $50.0 million, to arrive at an equity value range of: $254.0 million to $284.0 million.
Guideline Company Analysis. Vantage Point reviewed and compared certain financial information for NMM to corresponding financial information and multiples for 12 publicly traded corporations. The companies included were chosen because they are publicly traded companies with operations that for purposes of analysis may in certain respects be considered similar to those of NMM. Industries considered included healthcare services, healthcare facilities, and managed healthcare:
| · | AMN Healthcare Services, Inc. |
| · | Diversicare Healthcare Services, Inc. |
| · | Genesis Healthcare, Inc. |
| · | Kindred Healthcare, Inc. |
| · | LHC Group, Inc. |
| · | Pacific Health Care Organization, Inc. |
| · | Quorum Health Corporation |
| · | Select Medical Holdings Corporation |
| · | Surgical Care Affiliates, Inc. |
| · | Team Health Holdings, Inc. |
| · | The Ensign Group, Inc. |
| · | The Providence Service Corporation |
It is noted none of the selected companies are directly comparable to NMM.
The following table summarizes the range of observed valuation multiples utilized in Vantage Point’s guideline company analysis under the market approach.
| BEV / Revenue | BEV / EBITDA | |||||||||||||||||||||||||||||||
| Total LTM | FY LFY | Forward FY1 |
Forward FY2 |
LTM | LFY | Forward FY1 |
Forward FY2 |
|||||||||||||||||||||||||
| Minimum: | 0.35 | x | 0.35 | x | 0.54 | x | 0.57 | x | 4.98 | x | 1.92 | x | 4.20 | x | 4.30 | x | ||||||||||||||||
| Lower (First) Quartile: | 0.65 | x | 0.65 | x | 0.70 | x | 0.69 | x | 7.29 | x | 6.90 | x | 8.52 | x | 7.60 | x | ||||||||||||||||
| Median: | 0.98 | x | 0.96 | x | 0.97 | x | 0.93 | x | 10.29 | x | 10.12 | x | 10.30 | x | 9.32 | x | ||||||||||||||||
| Upper (Third) Quartile: | 1.15 | x | 1.34 | x | 1.16 | x | 1.09 | x | 10.77 | x | 12.52 | x | 12.01 | x | 13.94 | x | ||||||||||||||||
| Maximum: | 2.94 | x | 3.37 | x | 2.72 | x | 2.37 | x | 14.63 | x | 16.22 | x | 25.02 | x | 22.98 | x | ||||||||||||||||
Notes: Business Enterprise Value (“BEV”) equals Market Capitalization plus Book Value of Total Debt plus Book Value of Preferred Stock plus Book Value of Minority Interest minus Cash and Short Term Investments.
| 143 |
Trailing and forward revenue and EBITDA market multiples were calculated from the set of comparable guideline companies. The revenue and EBITDA multiples were used to obtain unadjusted business enterprise values in the range of $207.0 to $222.0 million. Adjustments were made by adding back cash of $35.0 million, the value of preferred stock of ApolloMed held by NMM of $18.0 million, the value of warrants in ApolloMed held by NMM of $6.1 million, and the value of NMM’s 50 percent interest in the NGACO of $43.0 million to $50.0 million, to arrive at an equity value range of: $309.0 million to $331.0 million.
Enterprise values derived from the selected companies analysis described below were calculated using the closing prices of the common stock of the selected companies listed below as of December 19, 2016. Estimates of EBITDA for the next two fiscal years, FY1 and FY2, for the selected companies listed below were based on consensus estimates.
Market Transaction Analysis. Vantage Point performed a market transaction analysis based on observed transactions involving the sale of entire companies, identifying thirty-one recent market transactions involving businesses reasonably similar to NMM. Industries considered included healthcare services, healthcare facilities, and managed healthcare.
Revenue and EBITDA market multiples were calculated from the set of selected comparable company transactions. The revenue and EBITDA multiples were used to obtain unadjusted business enterprise value in the range of $208.0 million to $224.0 million. Adjustments were made by adding back cash of $35.0 million, the value of preferred stock of ApolloMed held by NMM of $18.1 million, the value of warrants in ApolloMed held by NMM of $6.1 million, and the value of NMM’s 50 percent interest in the NGACO of $43.0 million to $50.0 million, to arrive at an equity value in the range of $310.0 to $333.0 million. The specific companies and data used to calculate the transaction values and resulting multiples are shown in the following table.
| 144 |
| Announcement Date | Target Company | Enterprise Value (EV)1 (US$ millions) |
EV
/ Revenue |
EV
/ EBITDA |
||||||||||
| Jun-15-2016 | Envision Healthcare Holdings, Inc. | $ | 7,935.9 | 1.37 | x | 12.59 | x | |||||||
| Aug-29-2016 | USMD Holdings, Inc. | $ | 298.8 | 0.91 | x | NMF | ||||||||
| Sep-23-2016 | VEGA Medical Professionals LLC | $ | 24.0 | 1.54 | x | 30.00 | x | |||||||
| Sep-16-2015 | Alliance Healthcare Services, Inc. | $ | 774.3 | 1.73 | x | 6.48 | x | |||||||
| Nov-17-2015 | B. E. Smith, Inc. | $ | 160.0 | 1.60 | x | N/A | ||||||||
| Dec-1-2015 | Allied Healthcare International Inc. | $ | 28.6 | 0.07 | x | N/A | ||||||||
| Jul-10-2015 | IPC Healthcare, Inc. | $ | 1,545.8 | 2.17 | x | 21.97 | x | |||||||
| Oct-13-2015 | Recruitment Group PS | $ | 16.0 | 2.11 | x | 26.67 | x | |||||||
| May-20-2015 | Omnicare Inc. | $ | 11,308.9 | 1.74 | x | 15.04 | x | |||||||
| Mar-22-2015 | Concentra, Inc. | $ | 1,055.0 | 1.06 | x | N/A | ||||||||
| May-14-2015 | Healthcare Business Insights, LLC | $ | 30.0 | 3.00 | x | N/A | ||||||||
| Mar-17-2015 | Physicians Practice Plus Inc. | $ | 20.0 | 1.87 | x | 9.09 | x | |||||||
| Jan-19-2015 | VISTA Staffing Solutions, Inc. | $ | 123.0 | 0.92 | x | N/A | ||||||||
| Nov-26-2014 | Athas Health, LLC | $ | 39.3 | 1.38 | x | 20.59 | x | |||||||
| Mar-13-2014 | Conemaugh Health System, Inc. | $ | 121.3 | 0.24 | x | N/A | ||||||||
| May-29-2014 | Sheridan Healthcare, Inc. | $ | 2,344.6 | 2.46 | x | 19.06 | x | |||||||
| Jun-2-2014 | Medical Staffing Network Healthcare, LLC | $ | 47.1 | 0.21 | x | N/A | ||||||||
| Jun-10-2014 | Phoenix Physicians, LLC | $ | 166.9 | 1.83 | x | 15.63 | x | |||||||
| May-16-2014 | Health Advocate, Inc. | $ | 265.0 | 3.08 | x | N/A | ||||||||
| Mar-31-2014 | CDMI, LLC | $ | 365.3 | 8.56 | x | 10.10 | x | |||||||
| Feb-27-2014 | KnowledgePoint360 Group LLC | $ | 144.0 | 1.36 | x | 7.20 | x | |||||||
| Dec-2-2013 | Allied Healthcare Staffing Division | $ | 28.7 | 0.73 | x | N/A | ||||||||
| Aug-19-2012 | Coventry Health Care Inc. | $ | 5,795.5 | 0.43 | x | 6.33 | x | |||||||
| May-20-2012 | HealthCare Partners, LLC | $ | 4,693.0 | 1.96 | x | 8.91 | x | |||||||
| Oct-24-2011 | HealthSpring Inc. | $ | 3,140.4 | 0.63 | x | 6.20 | x | |||||||
| Sep-18-2011 | Midwest Health Plan, Inc. | $ | 70.0 | 0.28 | x | N/A | ||||||||
| Aug-26-2010 | Bravo Health, Inc. | $ | 545.0 | 0.45 | x | 6.74 | x | |||||||
| 145 |
Notes: NMF = not meaningful. N/A = not available. Enterprise Value equals Consideration plus Net Assumed Liabilities (total debt plus total preferred and minority interest minus total cash and short-term investments reported no more than one year before the consideration offer date).
A valuation analysis of a subject company is a consideration in evaluating the fairness of a transaction. The Market Transactions Analysis was one of several widely accepted methodologies used to support valuation ranges for NMM. This market-facing approach established a value range based on what the market recognizes in the same or similar industries having similar operating characteristics.
Valuation of ApolloMed
Discounted Cash Flow. Vantage Point performed an illustrative DCF analysis on ApolloMed using the stand-alone, probability-adjusted forecast prepared by ApolloMed management to determine a range of implied values of ApolloMed common stock. Vantage Point relied on ApolloMed management’s projections for the years ending March 31, 2017 through March 31, 2019. Two additional years were added by Vantage Point to smooth the growth rate towards the sustainable growth rate and margins to sustainable levels.
In estimating ApolloMed’s value into perpetuity Vantage Point utilized the GGM and the Exit Multiple Method.
| · | Gordon Growth Method: A sustainable growth rate of 3.0 percent was selected based on historical growth in gross domestic product and industry outlook. A concluded terminal period capitalization rate range of 15.5 percent to 17.5 percent was used, which was derived based on the discount rate range used in the analysis of 18.5 percent to 19.5 percent as reduced by the terminal growth rate. The discount rate was derived using the WACC, in which the cost of equity was estimated as 23.9 percent and the after-tax cost of debt was estimated as 2.9 percent. The target capital structure was estimated to be 25.0 percent debt and 75.0 percent equity. |
| · | Exit Multiple Method: An EBITDA exit multiple range of 4.5 to 5.5 times was applied to 2021 EBITDA of $11.0 million (as determined by Vantage Point adding two additional forecast years to smooth the growth rate towards the sustainable growth rate and margins to sustainable levels). The exit multiple was selected based on observations of market multiples in the Guideline Company Analysis and Market Transaction Analysis and expected financial performance. |
Vantage Point also considered depreciation and amortization, working capital requirements and capital expenditures as provided by management. Based on an income approach analysis, the business enterprise value range from operations was determined to be as follows: $36.0 million to $41.0 million. Adjustments were made by adding back cash, which was assumed to be zero, less the related party payable of $201.0 thousand and plus the value of ApolloMed’s 50 percent interest in the NGACO of $43.0 million to $50.0 million, to arrive at an equity value range of: $79.0 million to $91.0 million.
Guideline Company Analysis. Vantage Point reviewed and compared certain financial information for ApolloMed to corresponding financial information and multiples for 12 publicly traded corporations. The companies included were chosen because they are publicly traded companies with operations that for purposes of analysis may in certain respects be considered similar to those of ApolloMed. Industries considered included healthcare services, healthcare facilities, and managed healthcare:
| · | AMN Healthcare Services, Inc. |
| 146 |
| · | Diversicare Healthcare Services, Inc. |
| · | Genesis Healthcare, Inc. |
| · | Kindred Healthcare, Inc. |
| · | LHC Group, Inc. |
| · | Pacific Health Care Organization, Inc. |
| · | Quorum Health Corporation |
| · | Select Medical Holdings Corporation |
| · | Surgical Care Affiliates, Inc. |
| · | Team Health Holdings, Inc. |
| · | The Ensign Group, Inc. |
| · | The Providence Service Corporation |
It is noted none of the selected companies are directly comparable to ApolloMed.
The following table summarizes the range of observed valuation multiples utilized in Vantage Point’s guideline company analysis under the market approach.
| BEV / Revenue | BEV / EBITDA | |||||||||||||||||||||||||||||||
| Total LTM | FY LFY |
Forward FY1 |
Forward FY2 |
LTM | LFY |
Forward FY1 |
Forward
FY2 |
|||||||||||||||||||||||||
| Minimum: | 0.35 | x | 0.35 | x | 0.54 | x | 0.57 | x | 4.98 | x | 1.92 | x | 4.20 | x | 4.30 | x | ||||||||||||||||
| Lower (First) Quartile: | 0.65 | x | 0.65 | x | 0.70 | x | 0.69 | x | 7.29 | x | 6.90 | x | 8.52 | x | 7.60 | x | ||||||||||||||||
| Median: | 0.98 | x | 0.96 | x | 0.97 | x | 0.93 | x | 10.29 | x | 10.12 | x | 10.30 | x | 9.32 | x | ||||||||||||||||
| Upper (Third) Quartile: | 1.15 | x | 1.34 | x | 1.16 | x | 1.09 | x | 10.77 | x | 12.52 | x | 12.01 | x | 13.94 | x | ||||||||||||||||
| Maximum: | 2.94 | x | 3.37 | x | 2.72 | x | 2.37 | x | 14.63 | x | 16.22 | x | 25.02 | x | 22.98 | x | ||||||||||||||||
Notes: BEV equals Market Capitalization plus Book Value of Total Debt plus Book Value of Preferred Stock plus Book Value of Minority Interest minus Cash and Short Term Investments.
Trailing and forward revenue and EBITDA market multiples were calculated from the set of comparable guideline companies. The revenue and EBITDA (for FY2) multiples were used to obtain unadjusted business enterprise values in the range of $40.0 to $48.0 million. Adjustments were made by adding back cash which was assumed to be zero, less the related party payable of $201.0 thousand and plus the value of ApolloMed’s 50 percent interest in the ACO of $43.0 million to $50.0 million, to arrive at an equity value range of: $83.0 million to $98.0 million.
Market Transaction Analysis. Vantage Point performed a market transaction analysis based on observed transactions involving the sale of entire companies, identifying thirty-one recent market transactions involving businesses reasonably similar to ApolloMed. Industries considered included healthcare services, healthcare facilities, and managed healthcare.
Revenue and EBITDA market multiples were calculated from the set of selected comparable company transactions. The revenue and EBITDA multiples were used to obtain unadjusted business enterprise value in the range of $40.0 million to $49.0 million. Adjustments were made by adding back cash which was assumed to be zero, less the related party payable of $201.0 thousand and plus the value of ApolloMed’s 50 percent interest in the ACO of $43.0 million to $50.0 million, to arrive at an equity value range of: $83.0 to $99.0 million. The specific companies and data used to calculate the transaction values and resulting multiples are shown in the following table.
| 147 |
| Announcement Date | Target Company |
Enterprise Value (EV)1 (US$ millions) |
EV / Revenue |
EV / EBITDA |
||||||||||
| Jun-15-2016 | Envision Healthcare Holdings, Inc. | $ | 7,935.9 | 1.37 | x | 12.59 | x | |||||||
| Aug-29-2016 | USMD Holdings, Inc. | $ | 298.8 | 0.91 | x | NMF | ||||||||
| Sep-23-2016 | VEGA Medical Professionals LLC | $ | 24.0 | 1.54 | x | 30.00 | x | |||||||
| Sep-16-2015 | Alliance Healthcare Services, Inc. | $ | 774.3 | 1.73 | x | 6.48 | x | |||||||
| Nov-17-2015 | B. E. Smith, Inc. | $ | 160.0 | 1.60 | x | N/A | ||||||||
| Dec-1-2015 | Allied Healthcare International Inc. | $ | 28.6 | 0.07 | x | N/A | ||||||||
| Jul-10-2015 | IPC Healthcare, Inc. | $ | 1,545.8 | 2.17 | x | 21.97 | x | |||||||
| Oct-13-2015 | Recruitment Group PS | $ | 16.0 | 2.11 | x | 26.67 | x | |||||||
| May-20-2015 | Omnicare Inc. | $ | 11,308.9 | 1.74 | x | 15.04 | x | |||||||
| Mar-22-2015 | Concentra, Inc. | $ | 1,055.0 | 1.06 | x | N/A | ||||||||
| May-14-2015 | Healthcare Business Insights, LLC | $ | 30.0 | 3.00 | x | N/A | ||||||||
| Mar-17-2015 | Physicians Practice Plus Inc. | $ | 20.0 | 1.87 | x | 9.09 | x | |||||||
| Jan-19-2015 | VISTA Staffing Solutions, Inc. | $ | 123.0 | 0.92 | x | N/A | ||||||||
| Nov-26-2014 | Athas Health, LLC | $ | 39.3 | 1.38 | x | 20.59 | x | |||||||
| Mar-13-2014 | Conemaugh Health System, Inc. | $ | 121.3 | 0.24 | x | N/A | ||||||||
| May-29-2014 | Sheridan Healthcare, Inc. | $ | 2,344.6 | 2.46 | x | 19.06 | x | |||||||
| Jun-2-2014 | Medical Staffing Network Healthcare, LLC | $ | 47.1 | 0.21 | x | N/A | ||||||||
| Jun-10-2014 | Phoenix Physicians, LLC | $ | 166.9 | 1.83 | x | 15.63 | x | |||||||
| May-16-2014 | Health Advocate, Inc. | $ | 265.0 | 3.08 | x | N/A | ||||||||
| Mar-31-2014 | CDMI, LLC | $ | 365.3 | 8.56 | x | 10.10 | x | |||||||
| Feb-27-2014 | KnowledgePoint360 Group LLC | $ | 144.0 | 1.36 | x | 7.20 | x | |||||||
| Dec-2-2013 | Allied Healthcare Staffing Division | $ | 28.7 | 0.73 | x | N/A | ||||||||
| Aug-19-2012 | Coventry Health Care Inc. | $ | 5,795.5 | 0.43 | x | 6.33 | x | |||||||
| May-20-2012 | HealthCare Partners, LLC | $ | 4,693.0 | 1.96 | x | 8.91 | x | |||||||
| Oct-24-2011 | HealthSpring Inc. | $ | 3,140.4 | 0.63 | x | 6.20 | x | |||||||
| Sep-18-2011 | Midwest Health Plan, Inc. | $ | 70.0 | 0.28 | x | N/A | ||||||||
| Aug-26-2010 | Bravo Health, Inc. | $ | 545.0 | 0.45 | x | 6.74 | x | |||||||
| 148 |
Notes: NMF = not meaningful. N/A = not available. Enterprise Value equals Consideration plus Net Assumed Liabilities (total debt plus total preferred and minority interest minus total cash and short-term investments reported no more than one year before the consideration offer date).
A valuation analysis of a subject company is a consideration in evaluating the fairness of a transaction. The Market Transactions Analysis was one of several widely accepted methodologies used to support valuation ranges for ApolloMed. This market-facing approach established a value range based on what the market recognizes in the same or similar industries having similar operating characteristics.
Public Stock Price
The public stock price does not appear to be a good indicator of value for ApolloMed for the following reasons:
| · | Lack of public information providing visibility into ApolloMed’s future prospects, primarily the value associated with the ACO. |
| · | Lack of trading liquidity. |
| · | Small public float outside of ApolloMed insiders. |
| · | No equity analyst coverage. |
Valuation of the combined entity.
Discounted Cash Flow. Vantage Point performed an illustrative DCF analysis on the combined entity using the combined, probability-adjusted forecast prepared by NMM and ApolloMed management to determine a range of implied values. Vantage Point relied on combined management’s projections for the years ending December 31, 2016 through December 31, 2019. One additional year was added by Vantage Point to smooth the growth rate towards the sustainable growth rate and margins to sustainable levels.
In estimating the combined entity’s value into perpetuity Vantage Point utilized the GGM and the Exit Multiple Method.
| · | Gordon Growth Method: A sustainable growth rate of 3.0 percent was selected based on historical growth in gross domestic product and industry outlook. A concluded terminal period capitalization rate range of 11.0 to 13.0 percent was used, which was derived based on the discount rate range used in the analysis of 14.0 percent to 16.0 percent as reduced by the terminal growth rate. The discount rate was derived using the WACC in which the cost of equity was estimated as 18.9 percent and the after-tax cost of debt was estimated as 2.9 percent. The target capital structure was estimated to be 25.0 percent debt and 75.0 percent equity. |
| · | Exit Multiple Method: An EBITDA exit multiple range of 6.0 times to 7.0 times was applied to 2020 EBITDA of $48.0 million. (as determined by Vantage Point adding an additional forecast year to smooth the growth rate towards the sustainable growth rate and margins to sustainable levels). The exit multiple was selected based on observations of market multiples in the Guideline Company Analysis and Market Transaction Analysis and expected financial performance. |
| 149 |
Vantage Point also considered a tax amortization benefit for goodwill, depreciation and amortization, working capital requirements and capital expenditures as provided by management. Based on an income approach analysis, the business enterprise value range from operations was determined to be as follows: $226.0 million to $274.0 million. Adjustments were made by adding the value of the ACO of $86.0 million to $100.0 million and cash of $10.0 million in order to arrive at an implied combined equity value of $322.0 million to $384.0 million. The exchange ratio was then applied by adjusting for the immediate post-deal share ownership of 72.0 percent plus the present value of the share holdback (10.0 percent) of $30.0 million to $35.7 million. Adjustments were also made for a cash dividend of $25.0 million, net value of the warrants held in ApolloMed of $3.4 million, and less option dilution of $6.3 million, to arrive at post deal consideration to NMM of: $284.0 million to $334.0 million.
Guideline Company Analysis.
The values calculated in the NMM and ApolloMed valuation sections were added to arrive at an enterprise value range $247.0 to $270.0 million. Adjustments were made for cash of $10.0 million and the value of the ACO of $86.0 million to $100.0 million in order to arrive at an implied combined equity value of $343.0 million to $380.0 million. The exchange ratio was then applied by adjusting for the immediate post-deal share ownership of 72.0 percent plus the present value of the share holdback (10 percent) of $32.0 million to $35.0 million, cash dividend of $25.0 million, net value of the warrants held in ApolloMed of $3.7 million, and less option dilution of $6.6 million, to arrive at post deal consideration to NMM of $301.0 million to $331.0 million.
Market Transaction Analysis. The values calculated in the NMM and ApolloMed valuation sections were added to arrive at an enterprise value range $248.0 to $273.0 million. Adjustments were made for cash of $10.0 million and the value of the ACO of $86.0 million to $100.0 million in order to arrive at an implied combined equity value of $344.0 million to $383.0 million. The exchange ratio was then applied by adjusting for the immediate post-deal share ownership of 72.0 percent plus the present value of the share holdback (10 percent) of $32.0 million to $36.0 million, cash dividend of $25.0 million, net value of the warrants held in ApolloMed of $3.6 million, and less option dilution of $6.6 million, to arrive at post deal consideration to NMM of $302.0 million to $333.0 million.
Valuation of The NGACO
Discounted Cash Flow. Vantage Point performed an illustrative DCF analysis on the NGACO using the stand-alone forecast prepared by NMM and ApolloMed management to determine a range of implied values. Vantage Point relied on NMM and ApolloMed management’s projections for the years ending December 31, 2017 through December 31, 2019. Two additional years were added by Vantage Point to smooth the growth rate towards the sustainable growth rate and margins to sustainable levels.
In estimating the NGACO’s value into perpetuity, Vantage Point utilized the GGM. A sustainable growth rate of 3.0 percent was selected based on historical gross domestic product growth and industry outlook. A concluded terminal period capitalization rate range of 17.0 percent to 19.0 percent was used, which was derived based on the discount rate range used in the analysis of 20.0 percent to 22.0 percent as reduced by the terminal growth rate. The discount rate was derived using the WACC, under which the cost of equity was estimated as 26.9 percent and the after-tax cost of debt was estimated as 2.9 percent. The target capital structure was estimated to be 25.0 percent debt and 75.0 percent equity.
Vantage Point also considered depreciation and amortization, working capital requirements and capital expenditures as provided by management. Based on an income approach analysis, the business enterprise value range from operations was determined to be as follows: $86.0 million to $100.0 million.
Summary
The summary of NMM’s equity value (before and after giving effect to the transaction), based on the valuation methodologies described above, is set forth below:
| 150 |
| $US millions | Before | After | ||||||||||||||
| Low | High | Low | High | |||||||||||||
| Discounted Cash Flow | $ | 254.0 | $ | 284.0 | $ | 284.0 | $ | 334.0 | ||||||||
| Guideline Company Analysis | $ | 309.0 | $ | 331.0 | $ | 301.0 | $ | 331.0 | ||||||||
| Market Transaction Analysis | $ | 310.0 | $ | 333.0 | $ | 302.0 | $ | 333.0 | ||||||||
Restrictions on Sales of Shares of ApolloMed Common Stock Received in the Merger
The shares of ApolloMed common stock to be issued in connection with the Merger will be registered under the Securities Act and will be subject to Lock-Up Agreements between ApolloMed and each of the NMM shareholders. Please see the section “AGREEMENTS RELATED TO THE MERGER AGREEMENT — Lock Up Agreements” in this joint proxy statement/prospectus.
Additional restrictions will apply to any NMM shareholder who may be deemed to be an “affiliate” of ApolloMed for purposes of Rule 144 under the Securities Act. Persons who may be deemed to be affiliates of ApolloMed include individuals or entities that control, are controlled by, or are under common control with, ApolloMed and may include the executive officers, directors and significant stockholders of ApolloMed.
U.S. Federal Income Tax Considerations
The Merger has been structured to qualify as a “reorganization” within the meaning of Section 368(a) of the Code and Treasury Regulations promulgated thereunder. As a result, NMM shareholders generally should not recognize gain or loss for U.S. federal income tax purposes upon the exchange of their shares of NMM stock for shares of ApolloMed common stock and warrants in connection with the Merger. ApolloMed stockholders will not recognize gain or loss for U.S. federal income tax purposes as a result of the Merger. In the event and to the extent NMM distributes existing ApolloMed Warrants held thereby to NMM shareholders prior to consummation of the Merger, such distribution will constitute a dividend for U.S. federal income tax purposes to the extent of NMM’s current or accumulated earnings and profits as determined under U.S. federal income tax principles.
For a more complete discussion of the material U.S. federal income tax consequences of the Merger, see the section titled “CERTAIN MATERIAL U.S. FEDERAL INCOME TAX CONSEQUENCES OF THE MERGER” beginning on page 214 of this joint proxy statement/prospectus.
Ownership of ApolloMed Following the Merger
Immediately following the Effective Time, ApolloMed and NMM anticipate that current NMM shareholders will own 83.3% of the total issued and outstanding shares of ApolloMed common stock, assuming there are no NMM dissenting shareholder interests as of the Effective Time, calculated in accordance with the Merger Agreement (see “THE MERGER AGREEMENT – Effects of Merger; Merger Consideration” beginning on page 159) and excluding the shares of ApolloMed common stock issuable upon exercise of the Warrant Consideration.
Board Composition and Management of ApolloMed after the Merger
At the Effective Time, the ApolloMed Charter and ApolloMed Bylaws will be amended to divide the board of directors into three classes, Class I, Class II and Class III, with three directors in each class.
NMM has selected, and ApolloMed has agreed to use reasonable efforts to elect, at or immediately following the Effective Time, Michael F. Eng as a Class I director, Mitchell W. Kitayama and Kenneth Sim M.D., as Class II directors and Li Yu as a Class III director, to the ApolloMed board of directors, subject to the approval of the ApolloMed stockholders. Except for Suresh Nihalani and Ted Schreck, the current directors of ApolloMed will serve as the remaining ApolloMed board members, subject to the approval of the ApolloMed stockholders, with Thomas Lam M.D. and David G. Schmidt designated as Class I directors, Mark Fawcett designated as a Class II director and Warren Hosseinion M.D. and Gary Augusta designated as Class III directors.
| 151 |
Under the terms of the Merger Agreement, ApolloMed will appoint Kenneth Sim M.D. to serve as Executive Chairman, Albert Young, M.D., to serve as Co-Chief Medical Officer, Thomas Lam, M.D., to serve as Co-Chief Executive Officer and Hing Ang to serve as Chief Operating Officer of ApolloMed at the Effective Time. Gary Augusta, current Executive Chairman of ApolloMed, will be President, Warren Hosseinion M.D. will be Co-Chief Executive Officer, Mihir Shah will continue as Chief Financial Officer and Adrian Vazquez M.D. will be Co-Chief Medical Officer of ApolloMed.
It is anticipated that Suresh Nihalani and Ted Schreck will resign as directors of ApolloMed effective as of the Effective Time.
Information about the individuals who will be directors and executive officers of ApolloMed, including biographical information, executive compensation and stock ownership, can be found in the sections titled “MANAGEMENT OF THE COMBINED COMPANY” beginning on page 177 “PRINCIPAL STOCKHOLDERS OF APOLLOMED AND THE COMBINED COMPANY” beginning on page 195 and “PRINCIPAL SHAREHOLDERS OF NMM AND THE COMBINED COMPANY” beginning on page 197 of this joint proxy statement/prospectus.
Interests of ApolloMed’s Directors and Executive Officers in the Merger
In considering the recommendation of ApolloMed’s board of directors to approve and adopt the ApolloMed Merger Proposal, as stockholders of ApolloMed, officers and directors owning shares of ApolloMed will be treated as other stockholders of ApolloMed and will experience the same stock appreciation, if any, as a result of the Merger. However, ApolloMed stockholders should be aware that certain of ApolloMed’s directors and executive officers have interests in the Merger that may be different from, or in addition to, the interests of ApolloMed stockholders generally. ApolloMed’s board of directors was aware of these interests and considered them, among other matters, in approving and declaring advisable the Merger Agreement and the transactions contemplated by the Merger Agreement. These interests are described below.
Continuing Service of Directors and Executive Officers of ApolloMed
ApolloMed’s current directors Warren Hosseinion M.D., who is also ApolloMed’s Chief Executive Officer, Gary Augusta, who is also ApolloMed’s Executive Chairman, Mark Fawcett, Thomas Lam, M.D. and David Schmidt are expected to continue to serve as directors of the combined company. Suresh Nihalani and Ted Schreck will resign as directors of ApolloMed immediately prior to the Effective Time from his position, effective immediately after the Effective Time.
In addition, Warren Hosseinion, M.D. is expected to serve as Co-Chief Executive Officer of the combined company together with Thomas Lam M.D. Gary Augusta is expected to serve as President of the combined company, Mihir Shah, ApolloMed’s Chief Financial Officer is expected to continue in the same role and Adrian Vazquez M.D., ApolloMed’s Chief Medical Officer is expected to serve as Co-Chief Medical Officer of the combined company with Albert Young M.D.
Ownership Interest
As of [●], 2017, the latest practicable date before the printing of this joint proxy statement/prospectus, the directors and executive officers of ApolloMed beneficially owned [●]% of the outstanding shares of ApolloMed common stock. See “Principal Stockholders of ApolloMed” for more information.
Employment Agreements
On December 20, 2016, AMM, a wholly-owned subsidiary of ApolloMed, entered into new employment agreements with each of Warren Hosseinion M.D., Adrian Vazquez M.D., Gary Augusta and Mihir Shah. Each of the new employment agreements have an initial term of three years with automatic renewals and are expected to remain in place following the Merger. The new employment agreements were approved by the Compensation Committee of the board of directors of ApolloMed and replace the employment agreements previously entered into with (i) Dr. Hosseinion and Dr. Vazquez on March 28, 2014, as amended on January 12, 2016 and as amended and restated on June 29, 2016, and (ii) Mr. Shah on July 21, 2016. Mr. Augusta’s consulting agreement through Flacane Advisers, Inc. has been terminated. Please see the section titled “MANAGEMENT OF THE COMBINED COMPANY – ApolloMed Executive Compensation” beginning on page 184 of this joint proxy statement/prospectus for further information about the new employment agreements.
| 152 |
Merger-Related Compensation
In accordance with Item 402(t) of the SEC’s Regulation S-K, the table below presents the estimated amounts of compensation for each “named executive officer” of ApolloMed that may be paid or become payable to ApolloMed’s named executive officers. The plans or arrangements pursuant to which such payments would be made consist of ApolloMed’s employment agreements with each of the named executive officers, ApolloMed’s stock plans and the respective equity and performance awards specifying the terms and conditions of each such award.
The potential payments in the table below are based on the following assumptions:
| · | The “effective time” of the Merger is [●], 2017, which is the assumed date of the Closing solely for purposes of this Merger-related compensation disclosure; |
| · | immediately following the effective time of the Merger, each of ApolloMed’s named executive officers was terminated without “Cause” or resigned for “Good Reason” (as defined in such executive officer’s employment agreement); |
| · | the stock price is $7.07 per share of ApolloMed common stock, which is the average closing price over the first 5 business days following the public announcement of the Merger. |
The amounts shown are estimates based on multiple assumptions and do not reflect certain compensation actions that could occur before the Effective Time of the Merger. As a result, the actual amounts received by a named executive officer may differ materially from the amounts shown in the following table.
The following table sets forth the information regarding compensation that may be paid or become payable to ApolloMed’s named executive officers.
Merger-Related Compensation
for ApolloMed’s Named Executive Officers
| Name | Cash($)(1) | Equity($)(2)(3) | Total($) | |||||||||
| Warren Hosseinion | 919,308 | - | 919,308 | |||||||||
| Gary Augusta | 642,000 | - | 642,000 | |||||||||
| Adrian Vazquez | 919,251 | - | 919,251 | |||||||||
| Mihir Shah | 735,820 | 99,944 | 835,764 | |||||||||
| (1) | Amounts in this column represent the cash payments for severance and benefits continuation to be paid to each executive upon a termination of employment without Cause or a termination for Good Reason. The lump-sum severance amount equals two times the executive’s most recent base salary (but determined prior to any action involving base salary that would constitute Good Reason). The benefits continuation amount equals the cost of coverage for the executive’s group medical, dental and vision programs for a period of 12 months at the time of termination. These amounts are subject to the executive’s execution of a release agreement. |
| (2) | Amounts in this column reflect the aggregate amount attributable to the accelerated vesting of all outstanding unvested stock options upon the change in control held by the executive officers pursuant to the terms of the named executive officers’ option award agreements. The named executive officers hold other vested options, which are set forth on page 184 below. All options held by the named executive officers will be assumed in connection with the change in control. |
| 153 |
| (3) | Amounts in this column do not reflect options to purchase shares of common stock of ApolloMed that were granted to each executive officer on April 6, 2017. Such options grants have since been deemed void and will be cancelled without payment prior to the Effective Time. |
Additional Narrative Description of Arrangements
No named executive officer is entitled to a tax gross-up for golden parachute excise taxes in connection with the Merger. Each employment agreement provides that if the compensation and benefits payable under such agreement would constitute a “parachute payment” under Section 280G of the Code, then the employment agreement or award agreements, as the case may be, (would provide either the full amount or a lesser amount such that no portion is subject to Section 280G, whichever provides the higher after-tax amount, including the potential taxes under Section 4999.) The table above does not reflect any potential cutbacks under this provision.
Please see the section titled “MANAGEMENT OF THE COMBINED COMPANY – ApolloMed Executive Compensation” beginning on page 184 of this joint proxy statement/prospectus for further information about the new employment agreements.
Sale of MMG
The Merger Agreement contemplates that Warren Hosseinion M.D., the sole shareholder of MMG, will sell to APC-LSMA all the issued and outstanding shares of capital stock of MMG for $100 under the Maverick Stock Purchase Agreement. It is anticipated that MMG and AMM will terminate the existing Management Services Agreement between them (the “MMG Management Agreement”) and APC-LSMA will pay AMM $400,000 as a termination payment on or before the Effective Time. APC-LSMA is owned 100% by Dr. Lam and in turn is consolidated by APC, which is deemed to control APC-LSMA.
Indemnification and Liability Insurance
In connection with the Merger, ApolloMed will continue to indemnify its current directors and officers to the maximum extent permitted in accordance with applicable law, the ApolloMed Charter and the ApolloMed Bylaws, and any contractual arrangements. ApolloMed intends to maintain its current directors’ and officers’ insurance policy through the Merger, and obtain runoff coverage for at least an additional [●] years after the Merger. ApolloMed is authorized in its absolute discretion to obtain and maintain insurance as may be necessary, appropriate, or advisable to cover such indemnification obligations.
Interests of NMM’s Directors and Executive Officers in the Merger
In considering the recommendation of the NMM board of directors that NMM stockholders vote to approve all of the presented proposals, NMM stockholders should be aware that some of NMM’s directors and officers have interests in the Merger and have arrangements that are different from, or in addition to, those of NMM stockholders generally. These interests and arrangements may create potential conflicts of interest. NMM’s board of directors was aware of these interests and considered these interests, among other matters, in adopting and approving the Merger Agreement and the transactions contemplated thereby, including the Merger, and in recommending that NMM stockholders approve the NMM Merger Proposal and the NMM Adjournment Proposal.
When NMM’s shareholders consider the recommendation of NMM’s board of directors in favor of approval of the NMM Merger Proposal and the NMM Adjournment Proposal, NMM’s shareholders should keep in mind that NMM’s directors and officers have interests in such proposals that are different from, or in addition to or in conflict with, the interests of its shareholders. These interests include:
| 154 |
| · | certain directors and officers of NMM are expected to continue to serve as directors and officers of the combined company; |
| · | the Merger Agreement contemplates that Warren Hosseinion, M.D., the sole shareholder of MMG, will sell to APC-LSMA (an entity in which Dr. Thomas Lam is the sole shareholder and the sole executive officer, but which is controlled and consolidated by APC) all the issued and outstanding shares of capital stock of MMG for $100 under the Maverick Stock Purchase Agreement; and |
| · | the continued indemnification of current directors and officers of NMM and the continuation of directors’ and officers’ liability insurance after the Merger. |
Regulatory Approvals Required for the Merger
Completion of the Merger is subject to prior receipt of all approvals required to be obtained from applicable governmental and regulatory authorities.
Under the HSR Act, the Merger may not be completed until the expiration of a 30 calendar day waiting period, which began when ApolloMed and NMM each filed a Premerger Notification and Report Form under the HSR Act with the FTC and the Antitrust Division on June 7, 2017. The required waiting period with respect to the Merger expired at 11:59 p.m., New York City time, on or July 7, 2017. The parties to the Merger Agreement are required to use their respective reasonable best efforts to consummate the offer and the Merger, including by taking all reasonable actions necessary to obtain any antitrust or other regulatory approvals. At any time before or after the Effective Time, and notwithstanding that the Merger may have been consummated, the FTC, the Antitrust Division or any state could take such action under the applicable antitrust or competition laws as it deems necessary or desirable. This action could include seeking to enjoin the completion of the Merger or seeking the divestiture of substantial assets of ApolloMed or NMM. Private parties may also institute legal actions under the antitrust laws under some circumstances. Although ApolloMed and NMM believe that the Merger is legal under applicable antitrust laws, a challenge to the Merger on antitrust grounds may be made, and if a challenge is made, it may be successful.
Under the terms of the Merger Agreement, neither ApolloMed nor NMM is required to hold separate (including by trust or otherwise) or divest any of their respective businesses or assets, or enter into any consent decree or other agreement that would restrict either ApolloMed or NMM in the conduct of its business. No additional stockholder approval is expected to be required or sought for any decision by ApolloMed or NMM, after their respective stockholder meetings, to agree to any terms and conditions necessary to resolve any regulatory objections to the Merger, and stockholder approval will not be sought unless additional stockholder approval is required to approve the terms and conditions under applicable law.
ApolloMed must also comply with the applicable federal and state securities laws in connection with the issuance of shares of ApolloMed common stock in the Merger and the filing with the SEC of the registration statement of which this joint proxy statement/prospectus forms a part.
The foregoing is a summary of the material regulatory requirements for the Merger, satisfaction or waiver of certain of which requirements is a condition to the completion of the Merger. There can be no guarantee as to if and when any of the consents or approvals required for the Merger will be obtained or as to the conditions that such consents and approvals may contain.
Under the DGCL, ApolloMed stockholders are not entitled to appraisal rights in connection with the Merger.
NMM shareholders have the right to dissent from the Merger and assert dissenters’ rights, provided the requirements of the California Corporations Code are followed. Any NMM shareholder electing to exercise dissenters’ rights must strictly comply with the provisions of Chapter 13 of the California Corporations Code.
| 155 |
Pursuant to the terms of the Merger Agreement, prior to the closing of the Merger, NMM has agreed to repurchase and cancel all NMM common stock (including any other securities exercisable for or convertible into NMM common stock, or rights to acquire NMM common stock) that are held by dissenting shareholders or by other shareholders who have exercised their dissenters’ rights in accordance with Chapter 13 of the California Corporations Code.
The following is intended to be a summary of the material provisions of the California statutory procedures required to be followed by shareholders in order to demand and perfect dissenters’ rights. This summary, however, is not a complete statement of all applicable requirements and is qualified in its entirety by reference to Chapter 13 of the California Corporations Code. The full text of these dissenters’ provisions is reproduced in its entirety in Annex I to this joint proxy statement/prospectus. If a NMM shareholder wishes to consider exercising dissenters’ rights, they should carefully review the text of Chapter 13 of the California Corporations Code, since failure to timely and properly comply with the requirements of Chapter of the California Corporations Code will result in the loss of dissenters’ rights under California law.
Chapter 13 of the California Corporations Code provides NMM shareholders who do not vote “FOR” approval of the Merger Agreement with the right, subject to compliance with the requirements summarized below, to dissent and demand the payment of, and to be paid in cash for, the fair market value of the shares of NMM common stock owned by such NMM shareholders as of the record date for NMM’s special meeting to consider and vote upon the NMM Merger Proposal. The fair market value of shares of NMM common stock is determined as of December 22, 2016, which was the day of, and immediately prior to, the first public announcement of the terms of the Merger.
Not Vote “FOR” the Merger Agreement
Any NMM shareholder who desires to exercise dissenters’ rights must not have voted his, her or its shares of NMM common stock “FOR” approval of the NMM Merger Proposal. If a NMM shareholder returns a proxy without voting instructions or with instructions to vote “FOR” approval of the NMM Merger Proposal, or votes in person at the NMM special meeting “FOR” approval of the NMM Merger Proposal, his, her or its shares of NMM common stock will be counted as votes in favor of the NMM Merger Proposal and such shareholder will lose any dissenters’ rights. Thus, if a NMM shareholder wishes to dissent and executes and returns a proxy, the proxy must specify that their shares of NMM common stock are to be voted “AGAINST” or “ABSTAIN” with respect to approval of the NMM Merger Proposal.
Notice of Approval
If NMM’s shareholders approve the Merger Agreement, NMM is required within 10 days after the approval to send to those NMM shareholders who did not vote “FOR” approval of the NMM Merger Proposal a written notice of NMM shareholder approval, accompanied by a copy of Sections 1300, 1302, 1303 and 1304 of the California Corporations Code, a statement of the price determined by NMM to represent the fair market value of the dissenting shares immediately prior to the public announcement of the term of the Merger Agreement on December 22, 2016 and a brief description of the procedure to be followed if the NMM shareholder desires to exercise the shareholder’s dissenters’ right under the California Corporations Code. The statement of price determined by NMM to represent the fair market value of dissenting shares, as set forth in the notice of approval, will constitute an offer by NMM to purchase the dissenting shares at the stated price if the Merger is completed and the dissenting shares do not otherwise lose their status as such. Within 30 days after the date of the mailing of the notice of NMM shareholder approval, a dissenting NMM shareholder must submit to NMM, or NMM’s transfer agent, for endorsement as dissenting shares, the stock certificates, if issued, representing their shares of NMM common stock as to which such NMM shareholder is exercising dissenter’s rights. If the dissenting shares are uncertificated, then the NMM shareholder must, within 30 days after the date of the mailing of the notice of NMM shareholder approval, provide written notice of the number of shares of NMM common stock which the shareholder demands that NMM purchase.
Written Demand for Payment
To preserve dissenters’ rights, an NMM shareholder must make a written demand for the purchase of their shares of NMM common stock and payment to them of the fair market value of their shares of NMM common stock within 30 days after the date on which notice of NMM shareholder approval (as described immediately above) of the Merger Agreement is mailed. Simply failing to vote for, or voting against, the NMM Merger Proposal does not constitute a proper written demand under the California Corporations Code. To comply with the requirements under the California Corporations Code, the written demand must:
| 156 |
| · | be received by NMM not later than 30 days after the date on which the notice of approval is mailed; |
| · | specify the shareholder’s name and mailing address and the number of shares of NMM common stock held of record which the shareholder demands that NMM purchase; |
| · | state that the NMM shareholder is demanding purchase of their shares of NMM common stock and payment of the fair market value of such shares; and |
| · | state the price that the NMM shareholder claims to be the fair market value of such shareholder’s shares of NMM common stock as of December 22, 2016, which statement of fair market value constitutes an offer by the NMM shareholder to sell such NMM shareholder’s shares of NMM common stock to NMM at that price. |
Any written demands for payment from NMM shareholders should be sent to NMM at Network Management, Inc., 1668 S. Garfield Avenue, 3rd Floor, Alhambra, California 91801, Attention: Corporate Secretary. Shares of NMM common stock held by shareholders have perfected their dissenters’ rights in accordance with Chapter 13 of the California Corporations Code and have not withdrawn their demands or otherwise lost their dissenters’ rights are referred to in this summary as “dissenting shares.”
Payment of Agreed-Upon Price
If NMM and a dissenting NMM shareholder agree that the shareholder’s shares of NMM common stock are dissenting shares and agree upon the price of the dissenting shares, the dissenting NMM shareholder is entitled to receive the agreed price with interest at the legal rate on judgments from the date of that agreement. Payment for the dissenting shares must be made within 30 days after the later of the date of that agreement or the date on which all statutory and contractual conditions to the Merger are satisfied. Payments are also conditioned on the surrender of the certificates, if issued, representing the dissenting shares within 30 days after the date of the mailing of the notice of NMM shareholder approval.
Determination of Dissenting Shares or Fair Market Value
If NMM denies that the dissenting NMM shareholder’s shares of NMM common stock are dissenting shares, or NMM and the NMM shareholder fail to agree upon the fair market value of the dissenting shares, then, within six months after the notice of NMM shareholder approval of the Merger is sent by NMM, any NMM shareholder demanding purchase of their shares of NMM common stock as dissenting shares or any interested corporation may file a complaint in the superior court in the proper county praying the court to determine whether the shares of NMM common stock are dissenting shares or the fair market value of the dissenting shares, or both, or may intervene in any action pending on such a complaint. If a complaint is not filed or intervention in a pending action is not made within the specified six-month period, the dissenters’ rights are lost. If the fair market value of the dissenting shares is at issue, the court will determine, or will appoint one or more impartial appraisers to determine, such fair market value.
Maintenance of Dissenting Share Status
Except as expressly limited by Chapter 13 of the California Corporations Code, holders of dissenting shares continue to have all the rights and privileges incident to their shares of NMM common stock until the fair market value of their shares of NMM common stock is agreed upon or determined. A holder of dissenting shares may not withdraw a demand for payment unless NMM consents to the withdrawal.
Dissenting shares lose their status as dissenting shares, and dissenting NMM shareholders cease to be entitled to require NMM to purchase their shares of NMM common stock, upon the happening of any of the following:
| · | the Merger is abandoned; |
| · | their shares of NMM common stock are transferred before their submission for the required endorsement; |
| 157 |
| · | the dissenting NMM shareholder and NMM do not agree on the status of the dissenting NMM shareholder’s shares of NMM common stock as dissenting shares or do not agree on the purchase price, but neither NMM nor the shareholder files a complaint or intervenes in a pending action within six months after the date on which NMM mails a notice that NMM’s shareholders have approved the Merger; or |
| · | with the consent of NMM, the dissenting NMM shareholder withdraws its demand for purchase of the dissenting shares. |
NMM shareholders should be aware that the fair value of any shares of NMM common stock as determined under Section 1300 of the California Corporations Code could be more, the same, or less than the Merger consideration. Investment banker opinions as to the fairness from a financial point of view of the consideration payable in a transaction such as the Merger are not an opinion as to, and do not in any way address, fair value under Section 1300 of the California Corporations Code.
The failure of a NMM shareholder to comply strictly with the California Corporations Code requirements will result in a loss of dissenters’ rights. A copy of the relevant statutory provisions is attached as Annex I. NMM shareholders are urged to refer to Annex I for a complete statement concerning dissenters’ rights. The foregoing summary of such rights is qualified in its entirety by reference to Annex I.
Although ApolloMed is the legal acquirer and will issue shares of its common stock to effect the Merger with NMM, if the business combination is completed it will be accounted for as an acquisition of ApolloMed by NMM using the “acquisition” method of accounting. NMM will record net tangible and identifiable intangible assets acquired and liabilities assumed from ApolloMed at their respective fair values at the date of the completion of the Merger. Any excess of the purchase price, which will equal the fair value of the aggregate amount of ApolloMed common stock issued pursuant to the Merger Agreement on the date of the completion of the Merger plus any cash paid in lieu of fractional shares, over the net fair value of such assets and liabilities will be recorded as goodwill.
The financial condition and results of operations of NMM after completion of the Merger will reflect ApolloMed’s results but will not be restated retroactively to reflect the historical financial condition or results of operations of ApolloMed. The earnings of NMM following the completion of the Merger will reflect the effect of acquisition accounting adjustments, including changes in the carrying values of assets and liabilities and on depreciation and amortization expense. Intangible assets with indefinite useful lives and goodwill will not be amortized but will be tested for impairment at least annually, and all assets including goodwill will be tested for impairment when certain indicators are present. If in the future NMM determines that tangible or intangible assets (including goodwill) are impaired, NMM would record an impairment charge at that time.
ApolloMed’s common stock is currently quoted on OTC Pink and traded under the symbol “AMEH.” ApolloMed has applied for listing of its common stock on the NASDAQ Global Market effective as of the closing of the Merger.
| 158 |
The following summary describes material provisions of the Merger Agreement. The provisions of the Merger Agreement are complicated and not easily summarized. This summary may not contain all of the information about the Merger Agreement that is important to you. This summary is qualified in its entirety by reference to the full text of the Merger Agreement, which is attached to this joint proxy statement/prospectus as Annex A and is incorporated by reference into this joint proxy statement/prospectus. You should read the Merger Agreement carefully and in its entirety, as it is the base legal document governing the Merger and the other transactions contemplated thereby.
The Merger Agreement has been included to provide you with information regarding its terms and the transactions described in this joint proxy statement/prospectus. Neither ApolloMed nor NMM intends that the Merger Agreement will be a source of business or operational information about ApolloMed or NMM. The representations, warranties and covenants made in the Merger Agreement by ApolloMed, Merger Sub and NMM were made solely to the parties to, and solely for the purposes of, the Merger Agreement and as of specific dates and were qualified and subject to important limitations agreed to by ApolloMed, Merger Sub and NMM in negotiating the terms of the Merger Agreement. In particular, in your review of the representations and warranties contained in the Merger Agreement and described in this summary, it is important to bear in mind that the representations and warranties were negotiated with the principal purposes of establishing the circumstances in which a party to the Merger Agreement may have the right to not complete the Merger if the representations and warranties of the other party prove to be untrue due to a change in circumstance or otherwise, and allocating risk between the parties to the Merger Agreement, rather than establishing matters as facts. The representations and warranties may also be subject to a contractual standard of materiality different from those generally applicable to stockholders and reports and documents filed with the SEC and in some cases were qualified by disclosures that are not reflected in the Merger Agreement. Moreover, information concerning the subject matter of the representations and warranties may have changed since the date of the Merger Agreement. You should not rely on the representations, warranties and covenants or any description thereof as characterizations of the actual state of facts relating to ApolloMed, Merger Sub and NMM or any of their respective subsidiaries or affiliates.
Form, Effective Time and Closing of Merger
The Merger Agreement provides that, at the Effective Time, Merger Sub, a wholly owned subsidiary of ApolloMed, will merge with and into NMM. Upon completion of the Merger, the separate corporate existence of Merger Sub will cease, and NMM will continue as the surviving entity and as a wholly owned subsidiary of ApolloMed.
If consummated, the Merger will be made effective at the time of filing of the Certificate of Merger with the Secretary of State of the State of California or at such later time as agreed to by the parties in writing and specified in the Certificate of Merger. The Merger Agreement provides that the closing of the Merger shall take place on the second business day after all of the closing conditions set forth in the Merger Agreement have been satisfied or waived or at such other date and time as may be mutually agreed upon by the parties in writing (the “Closing”).
Directors and Officers of Combined Company
Board of Directors
The Merger Agreement provides that the ApolloMed board of directors immediately after the Effective Time will consist of nine directors divided into three classes, designated as follows:
Class I Directors
| · | Michael F. Eng (NMM designee) |
| · | Thomas Lam, M.D. (NMM designee) |
| · | David G. Schmidt (ApolloMed designee) |
| 159 |
Class II Directors
| · | Mitchell W. Kitayama (NMM designee) |
| · | Kenneth Sim, M.D. (NMM designee) |
| · | Mark Fawcett (ApolloMed designee) |
Class III Directors
| · | Li Yu (NMM designee) |
| · | Warren Hosseinion, M.D. (ApolloMed designee) |
| · | Gary Augusta (ApolloMed designee) |
Management
The Merger Agreement further provides that immediately following the Effective Time, the following individuals will be appointed by the ApolloMed board of directors:
| Officer Name: | Position: | |
| Kenneth Sim, M.D. | Executive Chairman | |
| Thomas Lam, M.D. | Co-Chief Executive Officer | |
| Warren Hosseinion, M.D. | Co-Chief Executive Officer | |
| Gary Augusta | President | |
| Hing Ang | Chief Operating Officer | |
| Mihir Shah | Chief Financial Officer | |
| Adrian Vazquez, M.D. | Co-Chief Medical Officer | |
| Albert Young, M.D. | Co-Chief Medical Officer |
Effects of Merger; Merger Consideration
Under the Merger Agreement, at the Effective Time, each issued and outstanding share of NMM common stock will be converted into the right to receive such number of fully paid and nonassessable ApolloMed shares of common stock that results in the NMM shareholders having a right to receive (A) an aggregate number of shares of ApolloMed common stock that represents 82% of the total issued and outstanding shares of ApolloMed common stock immediately following the Effective Time, assuming there are no NMM dissenting shareholder interests as of the Effective Time, calculated in accordance with the Merger Agreement (see “THE MERGER AGREEMENT – Effects of Merger; Merger Consideration” beginning on page 159), plus (B) an aggregate of 2,566,666 shares of ApolloMed common stock, assuming there are no NMM dissenting shareholder interests as of the Effective Time (the “Additional Shares”). In addition, each NMM shareholder shall be entitled to receive such shareholder’s pro rata portion of (i) warrants to purchase an aggregate of 850,000 shares of ApolloMed common stock, exercisable at $11.00 per share and (ii) warrants to purchase an aggregate of 900,000 shares of ApolloMed common stock, exercisable at $10.00 per share (collectively, the “Warrant Consideration”). For purposes of calculating the exchange ratio, (A) the aggregate number of shares of ApolloMed common stock held by the NMM shareholders immediately following the Effective Time will exclude (i) any shares of ApolloMed common stock owned by NMM shareholders immediately prior to the Effective Time, (ii) the Additional Shares and (iii) any shares of ApolloMed common stock issuable to NMM shareholders pursuant to the exercise of the ApolloMed Warrants and/or Warrant Consideration, and (B) the total number of issued and outstanding shares of ApolloMed common stock immediately following the Effective Time shall exclude 499,000 shares of ApolloMed common stock issued or issuable under the Alliance Note pursuant to the Securities Purchase Agreement.
| 160 |
The aggregate consideration to be paid by ApolloMed to the NMM shareholders in the Merger is an amount equal to the total of (i) 90% of the aggregate number of shares of ApolloMed common stock the NMM shareholders are entitled to receive in accordance with the exchange ratio and the Additional Shares (the “Closing Share Payment”), plus (ii) the remainder, if any, from the Holdback Shares, which will comprise 10% of the aggregate number of shares of ApolloMed common stock the NMM shareholders are entitled to receive in accordance with the exchange ratio and the Additional Shares, plus (iii) warrants to purchase a pro-rata portion of an aggregate of (A) 850,000 shares of ApolloMed common stock at an aggregate price of $11.00 per share and (B) 900,000 shares of ApolloMed common stock at an aggregate price of $10.00 per share.
In order for NMM shareholders to receive the applicable merger consideration under the Merger Agreement, NMM shareholders must do the following:
| · | Execute the signature page of a letter of transmittal and provide the shareholder’s wire instructions and address (to be used to distribute cash to the NMM shareholder in lieu of fractional shares of ApolloMed common stock due to the NMM shareholder, if any), and deliver the executed letter of transmittal to the exchange agent. A form of the letter of transmittal is attached as Exhibit E of the Merger Agreement. |
| · | Complete the description of the NMM shareholder’s common stock as attached to the letter of transmittal and deliver the completed description to the exchange agent as set forth therein. |
| · | Execute the Substitute W-9 attached to the letter of transmittal and deliver the executed Substitute W-9 to the exchange agent. |
| · | Execute and deliver the Release and Agreement to Terms of Merger Agreement attached to the letter of transmittal. |
| · | Execute and deliver the Lock-Up Agreements. |
| · | Execute and deliver the Noncompetition and Nonsolicitation Agreement attached to the letter of transmittal. |
| · | Deliver certificate(s) representing shares of NMM common stock to the exchange agent as set forth in the letter of transmittal, unless any of such certificate(s) are held by NMM or any of its representatives, in which case such certificate(s) shall be delivered to the exchange agent on the NMM shareholder’s behalf. |
ApolloMed stockholders will not have any appraisal rights under Delaware law in connection with the matters to be voted on at the ApolloMed special meeting at which approval of the Merger will be considered.
NMM shareholders have the right to dissent from the Merger and assert dissenters’ rights, provided the requirements of the California Corporations Code are followed. Any NMM shareholder electing to exercise dissenters’ rights must strictly comply with the provisions of Chapter 13 of the California Corporations Code.
To preserve dissenters’ rights, an NMM shareholder must make a written demand for the purchase of their shares of NMM common stock and payment to them of the fair market value of their shares of NMM common stock within 30 days after the date on which notice of NMM shareholder approval of the Merger Agreement is mailed. Simply failing to vote for, or voting against, the NMM Merger Proposal does not constitute a proper written demand under the California Corporations Code.
| 161 |
The failure of a NMM shareholder to comply strictly with the California Corporations Code requirements will result in a loss of dissenters’ rights. A copy of the relevant statutory provisions is attached as Annex I. See the section titled “THE MERGER – Dissenters’ Rights” beginning on page 154 of this joint proxy statement/prospectus.
Representations and Warranties
The Merger Agreement contains representations and warranties made by ApolloMed and Merger Sub solely to NMM and by NMM solely to ApolloMed and Merger Sub. The representations and warranties described below and included in the Merger Agreement were made only for purposes of the Merger Agreement and as of specific dates, are solely for the benefit of NMM, Merger Sub and ApolloMed, as applicable, may be subject to limitations, qualifications or exceptions agreed upon by the parties, including those included in confidential disclosures made for the purposes of, among other things, allocating contractual risk between NMM and ApolloMed rather than establishing matters as facts, and may be subject to standards of materiality that differ from those generally applicable to shareholders and reports and documents filed with the SEC. You should not rely on the representations, warranties and covenants or any description thereof as characterizations of the actual state of facts or condition relating to NMM, Merger Sub, ApolloMed or any of their respective subsidiaries or affiliates. Moreover, information concerning the subject matter of the representations, warranties and covenants may change after the date of the Merger Agreement, which subsequent information may or may not be fully reflected in public disclosures by ApolloMed. The representations and warranties and other provisions of the Merger Agreement should not be read alone, but instead should be read only in conjunction with the information provided elsewhere in this joint proxy statement/prospectus.
ApolloMed and Merger Sub have made representation and warranties to NMM, including those related to the following matters:
| · | Authority of ApolloMed; No Conflicts; |
| · | Organization and Power and Authority of ApolloMed; |
| · | Organization and Power and Authority of Merger Sub; |
| · | Financial Statements; Accounts Receivable; |
| · | Absence of Certain Changes; |
| · | Material Contracts; |
| · | Litigation; |
| · | Business Employees and Employee Relations; |
| · | Employee Benefit Plans; |
| · | Taxes; |
| · | Solvency; |
| · | Brokers and Finders; |
| · | Sufficiency of Assets; |
| · | Equity Interests; |
| · | Legal and Regulatory Compliance; |
| 162 |
| · | Permits and Licenses; |
| · | Condition of Assets; |
| · | Financing Statements; Indebtedness; |
| · | Real Property; |
| · | Related Party Transactions; |
| · | Insurance; |
| · | Intangible Personal Property; |
| · | Environmental; |
| · | Books and Records; |
| · | Disclosure; |
| · | No Disqualification Event; and |
| · | SEC Reports; Financial Statements. |
NMM has made representations and warranties to ApolloMed and Merger Sub in the Merger Agreement, including representations and warranties relating to the following matters:
| · | Authority of NMM; No Conflicts; |
| · | Organization; Power and Authority; |
| · | Financial Statements; Accounts Receivable; |
| · | Absence of Certain Changes; |
| · | Material Contracts; |
| · | Litigation; |
| · | Business Employees and Employee Relations; |
| · | Employee Benefit Plans; |
| · | Taxes; |
| · | Solvency; |
| · | Brokers and Finders; |
| · | Sufficiency of Assets; |
| · | Equity Interests; |
| · | Legal and Regulatory Compliance; |
| · | Permits and Licenses; |
| · | Conditions of Assets; |
| 163 |
| · | Financing Statements; Indebtedness; |
| · | Real Property; |
| · | Related-Party Transactions; |
| · | Insurance; |
| · | Intangible Personal Property; Software; |
| · | Environmental; |
| · | Books and Records; |
| · | Disclosure; and |
| · | Accredited Investor. |
Certain representations and warranties in the Merger Agreement are qualified as to “materiality”, “knowledge” or “material adverse effect.” For purposes of the Merger Agreement, a “material adverse effect” means any change, effect, fact, event, occurrence, state of facts or development that, individually or together with any other changes, effects, facts, events, occurrences, states of facts or developments, materially and adversely affects, or could reasonably be expected to materially and adversely affect (a) the consolidated financial condition, results of operations, assets, liabilities, income, business or prospects of NMM or (b) the ability of the applicable party to perform its obligations under this Agreement or (c) ApolloMed’s ability to operate the surviving entity; provided, however, that Material Adverse Effect shall exclude any adverse changes or conditions as and to the extent such changes or conditions relate to or result from (i) general economic conditions or other conditions generally affecting the industry in which NMM’s business competes; or (ii) public or industry knowledge of the transactions contemplated by this Agreement (including, without limitation, any action or inaction by NMM’s business employees and vendors) except if such conditions in either clause (i) or clause (ii) above have a disproportionate impact on NMM’s business.
Conduct of Business Prior the Completion of the Merger
From the date the Merger Agreement was executed (the “Execution Date”) until the Closing, each of ApolloMed, NMM and Merger Sub have agreed to (i) conduct their respective businesses in the ordinary course of their normal, day-to-day operations consistent with their respective past practices and customs, (ii) preserve substantially intact their respective business organizations, and (iii) preserve their present relationships and goodwill with customers, suppliers, and other persons with which they have material business relations. These general obligations include a detailed set of business activities that may not be undertaken during the period between the Execution Date and Closing without the prior written consent of the other party, which consent may not be unreasonably withheld, conditioned or delayed.
No Solicitation
The Merger Agreement contains provisions that restrict each of ApolloMed and NMM from encouraging, soliciting or initiating discussions or negotiations with, or engaging in negotiations or discussions with, or providing non-public information to any person concerning, a merger, consolidation, sale of substantially all assets or other similar transaction involving their respective businesses, assets or equity, in each case that would result in the acquisition in any manner of more than 15% of the voting power or fair market value of the business, assets, or deposits of such party.
| 164 |
Agreement Not to Change Recommendation
NMM’s board of directors will not withdraw their approval of the Merger Agreement or approve or endorse any Acquisition Proposal or take any such actions to further such a proposal, including not entering into any letter of intent or other definitive agreement which is reasonably likely to lead to any such competitor acquisition.
Reasonable Best Efforts
Each party will use its reasonable best efforts to take all actions necessary, proper or advisable in order to consummate the Merger and the other transactions contemplated by the Merger Agreement. Each party will use reasonable best efforts and will cooperate with the other party in the preparation and filing, of all filings required to consummate the transactions contemplated by the Merger Agreement and to obtain regulatory approvals as necessary.
Notice of Certain Events
Each of ApolloMed and NMM have agreed to promptly notify the other party of, and deliver to such other party copies of all documentation relating to (i) obtaining third party consents, (ii) the occurrence of a breach of any representation or warranty in the Merger Agreement, (iii) the commencement of any legal action that relates to either party’s business or the consummation of the Merger, (iv) shareholder communication, (v) material third party contracts, (vi) communications with any governmental authority in connection with the Merger, and (vii) material operating and financial reports prepared for either party’s management.
Confidentiality, Press Releases and Public Announcements
NMM and ApolloMed previously entered into a Nondisclosure Agreement which was incorporated by reference into the Merger Agreement and shall continue in full force and effect until the Closing. Each of the parties agreed that the use of confidential information will be used solely for the purposes of evaluating the party that disclosed such information.
NMM and ApolloMed will consult with each other before issuing, and provide each other the opportunity to review, comment upon and concur with, and use commercially reasonable efforts to agree on, any press release or other public statements with respect to the transactions contemplated by the Merger Agreement.
Third Party Consents and Approvals
Each of NMM, ApolloMed and the Shareholders’ Representative agreed to use its commercially reasonable efforts to take such actions as are necessary or advisable to consummate, as promptly as practicable, the Merger and the other transactions contemplated by this Agreement, including (i) obtaining all necessary consents, authorizations and approvals from any governmental authority, including, without limitation, Notification and Report Forms and related material required to be filed with the FTC and the Antitrust Division under the HSR Act with respect to the transactions contemplated hereby or other third party, and (ii) the execution and delivery of any additional instruments necessary to consummate the Merger.
ApolloMed believes that the Merger does not raise antitrust or other significant regulatory concerns and that both parties will be able to obtain all requisite regulatory approvals prior to the Closing. ApolloMed must comply with the applicable federal and state securities laws in connection with the issuance of shares of ApolloMed common stock in the Merger and the filing with the SEC of the registration statement of which this joint proxy statement/prospectus forms a part.
Proxy/Registration Statement
ApolloMed, NMM and Merger Sub agreed to cooperate with each other in the preparation of, and filing of, this joint proxy statement/prospectus and the registration statement of which this document is a part as soon as practicable after the effectiveness of the Merger Agreement.
| 165 |
NMM Shareholder Approval
As soon as practicable following the date the proxy clearance is obtained and, if applicable, the date the registration statement is effective, NMM shall give notice (the “NMM Shareholder Meeting Notice”) to the NMM shareholders for the purpose of approving the Merger Agreement and the other transactions contemplated by the Merger Agreement, together with any other matters required to be approved or adopted by the NMM shareholders in order to carry out the intentions of the Merger Agreement. In furtherance of that obligation, NMM will take, all action necessary to duly call, give notice of, convene and hold a special meeting of the holders of NMM common stock, to be held no later than 30 calendar days following the date NMM sends the NMM Shareholder Meeting Notice, to consider and vote upon the adoption of the Merger Agreement and approval of the other transactions contemplated by the Merger Agreement as well as any other such matters.
ApolloMed Shareholder Approval
As soon as practicable following the date the proxy clearance is obtained and, if applicable, the date the registration statement is effective, ApolloMed shall give notice (the “ApolloMed Shareholder Meeting Notice”) to the ApolloMed shareholders for the purpose of approving the Merger Agreement and the other transactions contemplated by the Merger Agreement, together with any other matters required to be approved or adopted by the ApolloMed shareholders in order to carry out the intentions of the Merger Agreement. In furtherance of that obligation, ApolloMed will take, all action necessary to duly call, give notice of, convene and hold a special meeting of the holders of ApolloMed common stock, to be held no later than 30 calendar days following the date ApolloMed sends the ApolloMed Shareholder Meeting Notice, to consider and vote upon (i) the Merger, including the issuance of ApolloMed shares that will comprise the merger consideration, and the other transactions contemplated by the Merger Agreement, (ii) the division of the board of directors of ApolloMed into three classes and the amendments to the ApolloMed Charter and ApolloMed Bylaws to effect such board classification, (iii) the election to the board of directors of ApolloMed of the persons designated by NMM and ApolloMed as set forth above, and (iv) any other action required to be approved by the shareholders of ApolloMed in connection with the Merger Agreement, the Merger or any other such matters.
NMM Financial Statements
NMM agreed to provide ApolloMed certain financial statements of NMM and its subsidiaries in accordance with GAAP.
Distribution of NMM Distributable Cash and ApolloMed Warrants
ApolloMed, NMM and Merger Sub agreed that prior to the Closing, (i) NMM may at any time or from time to time in NMM’s sole discretion distribute all or any portion of NMM’s cash and cash equivalents to its shareholders so long as (x) NMM retains sufficient cash and cash equivalents to conduct its business in the ordinary course of business and (y) NMM is able to satisfy the covenant to maintain the minimum level of cash and cash equivalents set forth in the Merger Agreement and (ii) immediately prior to the Closing NMM may make an in-kind distribution to its shareholders of the ApolloMed Warrants such that the ApolloMed Warrants shall not be exercised prior to the Effective Time.
Working Capital Loan
NMM and ApolloMed agreed that NMM would provide a working capital loan to ApolloMed in the principal amount of $9,000,000, which is evidenced by a convertible promissory note. Of the principal amount, (A) $5,000,000 was previously disbursed to ApolloMed pursuant to a $5,000,000 working capital loan evidenced by the Original Note and (B) $4,000,000 is to be used for working capital.
Minimum NMM Cash
NMM covenants and agrees to maintain a minimum amount of cash immediately prior to the Effective Time of not less than $10,000,000.
| 166 |
Indemnification; Holdback Shares
The Merger Agreement provides that the representations and warranties contained therein will survive for a period of two years after the Closing, during which the parties may seek indemnification for any breaches of the Merger Agreement.
The Merger Agreement requires that at the Effective Time, ApolloMed will hold back 10% of the total number of shares of ApolloMed common stock issuable to NMM shareholders in the Merger to secure indemnification obligations of NMM. The Holdback Shares will be held for a period of up to 24 months after the closing of the Merger, during which ApolloMed may seek indemnification for any breach of, or noncompliance with, any provision of the Merger Agreement by NMM. At the end of first year following the closing of the Merger, 50% of the Holdback Shares will be released to the pre-Merger NMM shareholders, subject to any reduction for any indemnification claims and at the end of the second year following the closing of the Merger, the remainder of the Holdback Shares will be released to the pre-Merger NMM shareholders, subject to any reduction for any indemnification claims. Separately, indemnification of pre-Merger NMM shareholders under the Merger Agreement will be made by the issuance by ApolloMed to pre-Merger NMM shareholders of new additional shares of common stock (capped at the same number of shares of ApolloMed common stock as the Holdback Shares).
Conditions to Completion of the Merger
Currently, ApolloMed and NMM expect to complete the Merger during the fourth quarter of 2017. As more fully described in this joint proxy statement/prospectus and in the Merger Agreement, each party’s obligation to complete the Merger depends on a number of conditions being satisfied or, where legally permissible, waived, including the following:
| · | The approval of the Merger Agreement by the NMM shareholders holding at least 95% of the outstanding shares of NMM common stock and representing at least 95% in number of the NMM shareholders; |
| · | The approval of the ApolloMed stockholders of the ApolloMed Merger Proposal, the Board Classification Proposal and each of the directors in the Election of Directors Proposal; |
| · | The effectiveness of the registration statement of which this joint proxy statement/prospectus is a part and the absence of any stop order or related proceeding initiated or threatened by the SEC and not concluded or withdrawn; and |
| · | The absence of any legal restraint or governmental order that would prevent or prohibit the completion of the Merger and the other transactions contemplated by the Merger Agreement. |
The obligation of ApolloMed and Merger Sub to complete the Merger is subject to the satisfaction or waiver of the following additional conditions:
| · | NMM’s representations and warranties being true in all respects to the extent not qualified by material or mutual adverse effect to the extent qualified by materiality or material adverse effect and being true in all material respects (to the extent no qualified by materiality or material adverse effect) as of the date of the date of the Merger Agreement and the Closing except for those otherwise qualified as to a specified date; |
| · | The performance, in all material respects, by NMM and the Shareholders’ Representative, of its covenants and agreements required to be performed or complied with before or on the Closing; |
| 167 |
| · | Delivery to ApolloMed at or before the Closing of all required approvals, consents, authorizations and waivers from NMM and all other closing deliverables from NMM, including, but not limited to, delivery by all NMM shareholders of executed Lock-Up Agreements; |
| · | No action commenced or threatened in writing by a governmental authority, in effect, that would restrain or prevent the Closing or transactions contemplated by the Merger Agreement or seeks damages in connection with such transactions; |
| · | The absence of any material adverse effect on NMM and no event will have occurred or circumstance will exist that, individually or in combination with any other events or circumstances, would reasonably be expected to have a material adverse effect on NMM; and |
| · | NMM’s repurchase and cancellation of all shares of NMM common stock that will not be voted in favor of the Merger or the other transactions contemplated by the Merger Agreement such that there shall be no NMM shareholders who have exercised their dissenters’ rights in respect of the Merger or any other dissenting shareholders; and |
| · | Satisfaction or waiver of all conditions precedent to APC-LSMA’s purchase of all of the issued and outstanding capital stock of MMG. |
The obligation of NMM to complete the Merger is subject to the satisfaction or waiver of the following additional conditions:
| · | The representations and warranties of ApolloMed and Merger Sub being true in all respects, to the extent qualified by materiality or material adverse effect, and others will be true in all material respects as of the date of the Merger Agreement and the Closing, except for those otherwise qualified as to a specified date; |
| · | The performance, in all material respects, by ApolloMed and Merger Sub of their covenants and agreements required to be performed or complied with before or on the Closing; |
| · | Receipt by, and delivery to, NMM at or before the Closing of all required approvals, consents and waivers from ApolloMed and Merger Sub and all closing deliverables and payments from ApolloMed; |
| · | No action commenced or threatened in writing by a governmental authority, in effect, that would restrain or prevent the Closing or transactions contemplated by the Merger Agreement or seeks damages in connection with such transactions; |
| · | The absence of any material adverse effect on ApolloMed and absence of any event that, individually or in combination with any other events or circumstances, would reasonably be expected to have a material adverse effect on ApolloMed; and |
| · | Satisfaction or waiver of all conditions precedent to APC-LSMA’s purchase of all of the issued and outstanding capital stock of MMG. |
Neither ApolloMed nor NMM can be certain when, or if, the conditions to the Merger will be satisfied or waived, or that the Merger will be completed.
Termination of the Merger Agreement
The Merger Agreement may be terminated at any time prior to the Closing by mutual written consent of the parties. The Merger Agreement may also generally be terminated by either party, prior to Closing, in the following circumstances:
| 168 |
| · | If the Merger and other transactions contemplated by the Merger Agreement have not been consummated on or before March 31, 2018 (the “End Date”); |
| · | Any law, order or legal restraint (a) makes the consummation of the Merger and the other transactions contemplated by the Merger Agreement illegal or otherwise prohibited or (b) enjoins a party from consummating the Merger and the other transactions contemplated by the Merger Agreement and such injunction, other legal restraint or order shall have become final and non-appealable; |
| · | If either party (i) withdraws its approval, recommendation or declaration of advisability of the Merger, the Merger Agreement or the consummation of the transactions contemplated thereunder, (ii) adopts, approves or declares advisable the adoption of any offer, proposal for merger, acquisition of assets or other business combination that would result in the acquisition of more than fifteen percent (15%) of the voting power in, or more than fifteen percent (15%) of the fair market value of the business, assets or deposits of such party (an “Acquisition Proposal”); or (iii) agree or propose to take any such actions (each such action, an “Adverse Recommended Change”); |
| · | If ApolloMed fails to obtain the requisite approval of the ApolloMed Merger Proposal, the Board Classification Proposal and each of the directors in the Election of Directors Proposal at its special meeting of stockholders or any adjournment or postponement thereof; |
| · | If NMM fails to obtain the requisite approval of the NMM Merger Proposal at its special meeting of shareholders or any adjournment or postponement thereof; |
| · | If there is a material breach by either party of the non-solicitation provisions or shareholder provisions in the Merger Agreement; |
| · | If there has been a material breach by either party of any representation, warranty, covenant or agreement contained in Merger Agreement that has prevented or would prevent the satisfaction of any condition to the obligations of such party at the closing and such breach has not been waived or cured within 10 business days after written of written notice by the other party; |
| · | If more than five percent (5%) of the outstanding shares of NMM common stock have validly exercised their dissenters’ rights in accordance with the Dissenters’ Rights Rules (and not withdrawn such exercise or otherwise become ineligible to effect such exercise) in respect of the Merger; |
| · | If a material adverse effect with respect to NMM, ApolloMed or Merger Sub has occurred and cannot be cured by the applicable party within 10 business days after receipt of written notice thereof from the applicable party; or |
| · | If ApolloMed or NMM does not accept updated disclosure schedules provided by the other party pursuant to the Merger Agreement. |
In the event that the Merger Agreement is terminated pursuant to the above, the Merger Agreement will become void and of no effect without further obligation or liability of any party (except for certain parties’ obligations of confidentiality and non-use with respect to the other Party’s confidential information pursuant to the Nondisclosure Agreement) and no party will be entitled to any monetary damages, injunctive relief or any indemnification; provided, that no party will be relieved from liability resulting from a knowing and intentional breach prior to such termination of any of its representations, warranties, covenants or agreements set forth in the Merger Agreement or any other transaction contemplated thereunder. Notwithstanding anything to the contrary contained in the Merger Agreement, the obligations in Sections 3.7 (Confidentiality), 9.2 (Effects of Termination) and 9.3 (Fees and Expenses) and Article XII (General Provisions) and Article XIII (Definitions) of the Merger Agreement shall remain in full force and effect.
| 169 |
Termination Fees; Expenses in Connection with the Termination
Notwithstanding the above, ApolloMed and NMM are each subject to a $1,500,000 termination fee in certain circumstances where the Merger Agreement is terminated and it enters into any definitive agreement with respect to, or consummates, any Acquisition Proposal within twelve months of the date of any such termination.
Expenses
Except with respect to costs and expenses of all filing and other fees in connection with any filing under the HSR Act, each of which shall be borne equally by ApolloMed and NMM, all fees and expenses incurred in connection with the Merger Agreement, the Merger and the other transactions contemplated hereby shall be paid by the party incurring such fees or expenses, whether or not the Merger is consummated.
Each party will pay all costs and expenses incurred by it incident to its negotiation and preparation of the Merger Agreement and to its performance and compliance with all agreements and conditions contained in the Merger Agreement on its part to be performed or complied with, including the fees, expenses and disbursements of its counsel, accountants, advisors and consultants. Notwithstanding anything to the contrary contained in the Merger Agreement, all transfer, documentary, sales, use, stamp, registration and other similar taxes, and all conveyance fees, recording charges and other similar charges and fees (including any penalties and interest) incurred in connection with the transactions contemplated by the Merger Agreement shall be paid by the Shareholders’ Representative, acting on behalf of the NMM shareholders.
Amendment, Modification or Waiver
The Merger Agreement may not be amended except by a written amendment signed by all of the parties thereto.
Governing Law; Exclusive Jurisdiction
All disputes, claims or controversies arising out of or relating to the Merger Agreement or the transactions contemplated by the Merger Agreement shall be construed in accordance with and governed by the internal laws of the State of California without giving effect to any choice or conflict of law provision or rule (whether of the State of California or any other jurisdiction) that would cause the application of laws of any jurisdiction other than those of the State of California.
On March 30, 2017, ApolloMed entered into a Securities Purchase Agreement with Alliance pursuant to which Alliance loaned ApolloMed $4,990,000 and ApolloMed issued the Alliance Note to Alliance. In connection with the financing, Alliance requested NMM to guaranty repayment of the Alliance Note if it is not converted into shares of ApolloMed common stock in accordance therewith.
The Alliance Note bears interest at a rate of 6% per annum. The Alliance Note was amended on October 16, 2017 to extend the maturity date such that the entire outstanding principal and all accrued and unpaid interest thereon, is due and payable by ApolloMed to Alliance on the earlier of (i) March 31, 2018 or (ii) the date on which the Merger Agreement is terminated, whichever occurs first (the “Alliance Maturity Date”). If the Merger has not been consummated on or before the Alliance Maturity Date, then the outstanding principal balance and interest will be due 45 days after the Alliance Maturity Date. On the business day following closing of the Merger on or before the Maturity Date, the original principal amount of the Alliance Note, together with all accrued and unpaid interest thereon, will automatically be converted into shares of ApolloMed common stock, at a conversion price of $10.00 per share, subject to adjustment for stock splits, stock dividends, reclassifications and other similar recapitalization transactions that occur after the date of the Alliance Note. The conversion price was determined in negotiations between ApolloMed and Alliance based on a premium to the sales price of the ApolloMed common stock on the OTC. The Alliance Note may not be prepaid, in whole or in part, by ApolloMed nor converted into shares of ApolloMed common stock voluntarily by Alliance.
| 170 |
In connection with the Alliance Note, the parties to the Merger Agreement entered into an Amendment to Agreement and Plan of Merger as of March 30, 2017 (the “Merger Agreement Amendment”). Pursuant to the Merger Agreement Amendment, the shares of ApolloMed common stock issuable upon conversion of the Alliance Note would be excluded from the exchange ratio calculation of the shares of ApolloMed common stock to be issued to NMM shareholders at closing of the Merger. Additionally, as consideration for excluding the shares of ApolloMed common stock issuable upon conversion of the Alliance Note from the calculation of the exchange ratio and NMM’s issuing the guaranty, ApolloMed agreed to issue to NMM shareholders at closing of the Merger, as part of the merger consideration, warrants to purchase an aggregate of 850,000 shares of ApolloMed’s common stock with an exercise price of $11.00 per share.
The Merger Agreement Amendment contains other technical and conforming changes, including provisions for the deposit of the merger consideration at or prior to the Effective Time of the Merger, the preparation and delivery before the closing of the Merger of a spreadsheet regarding calculation of the merger consideration and the addition of certain defined terms.
Effective as of October 17, 2017, the parties to the Merger Agreement executed a second amendment to the Merger Agreement (“Amendment No. 2”). Pursuant to Amendment No. 2, the merger consideration was amended to provide that each outstanding share of NMM common stock will be converted into the right to receive such number of shares of ApolloMed common stock that would result in the NMM shareholders having a right to receive (i) an aggregate number of shares of ApolloMed common stock that represents 82% of the total issued and outstanding shares of ApolloMed common stock immediately following the consummation of the Merger (assuming there are no NMM dissenting shareholder interests as of the effective time of the Merger) and (ii) an aggregate of 2,566,666 shares of ApolloMed common stock. In addition, Amendment No. 2 provides that each NMM shareholder will be entitled to receive such shareholder’s pro rata portion of (i) warrants to purchase an aggregate of 850,000 shares of ApolloMed common stock exercisable at $11.00 per share, and (ii) warrants to purchase an aggregate of 900,000 shares of ApolloMed common stock exercisable at $10.00 per share. Amendment No. 2 contains other conforming changes, including provisions authorizing the issuance of shares of NMM common stock and options (which options must be exercised or cancelled prior to the closing) and extending the End Date to March 31, 2018.
Amendment No. 2 also contemplates NMM to provide a new working capital loan in the amount of nine million dollars evidenced by a promissory note, which is convertible into shares of common stock of ApolloMed at $10 per share (the “Restated NMM Note”). Of the principal amount, (A) $5,000,000 is required to be used to refinance a $5,000,000 working capital loan that was previously loaned by NMM to the Company pursuant to a Promissory Note dated January 3, 2017 (the “Original Note”) and (B) $4,000,000 is to be used for working capital. The Restated NMM Note cancels and replaces the Original Note and with the effect that the entire outstanding principal balance of the Original Note, all accrued and unpaid interest thereon, and any applicable fees, costs and charges rolls into and becomes payable pursuant to the terms of the Restated NMM Note.
| 171 |
AGREEMENTS RELATED TO THE MERGER
Eddie Lam, M.D., Thomas Lam, M.D., Su Kin Lee, M.D., Kenneth Sim, M.D., Theresa Tseng, M.D., Yang Chern Tseng, M.D., and Albert Young, M.D. have each entered into an agreement with ApolloMed pursuant to which each has agreed to vote all of the shares of NMM common stock owned or controlled by them in favor of the Merger, the Merger Agreement and the transactions contemplated by the Merger Agreement. As of the close of business on [●], 2017, the record date for the special meeting, Eddie Lam, M.D., Thomas Lam, M.D., Su Kin Lee, M.D., Kenneth Sim, M.D., Theresa Tseng, M.D., Yang Chern Tseng, M.D., and Albert Young, M.D. collectively owned, directly or indirectly, [●] shares of NMM common stock, which represented approximately [●]% of the outstanding shares of NMM common stock. These stock holders also granted ApolloMed an irrevocable proxy and power of attorney to cause their shares of NMM common stock to be counted as present at the NMM shareholders meeting and to execute consents in respect of such NMM shares in accordance with the Voting Agreements.
Under the Voting Agreements, subject to certain exceptions, the security holders also agreed not to sell or transfer NMM common stock held by them until the earliest of the date of termination of the Merger Agreement or the Effective Time of the Merger. The Voting Agreement exceptions permit the holders to transfer shares of NMM common stock (i) to such holder’s family member or a family trust or a charitable organization so long as such transferee agrees in writing to be bound by the terms and provisions of such Voting Agreement, (ii) in connection with the exercise of stock options for NMM common stock but only to the extent of such holder’s exercise price and income or other tax liability with respect to such exercise and only to the extent permitted under the Merger Agreement and (iii) that were acquired upon the exercise of stock options expiring after the date of the Voting Agreement and prior to the Effective Time.
Concurrently with the execution of the Merger Agreement and as a condition to ApolloMed’s and Merger Sub’s willingness to consummate the transactions contemplated by the Merger Agreement, NMM has agreed to relinquish its redemption rights relating to the Series A preferred stock it owns in ApolloMed pursuant to the terms and conditions of a Consent and Waiver Agreement dated as of December 21, 2016 by and between ApolloMed and NMM (the “Consent and Waiver Agreement”). Under the terms of the Consent and Waiver Agreement, NMM agrees to waive its right to redeem its 1,111,111 shares of ApolloMed’s Series A preferred stock pursuant to Section 6 of ApolloMed’s amended and restated certificate of designation. Additionally, NMM consents to and approves an amendment to ApolloMed’s amended and restated certificate of designation removing the redemption provision of Section 6.
Prior to or concurrently with the completion of the Merger and as a condition to the obligation of ApolloMed and Merger Sub to consummate the transactions contemplated thereby, each shareholder of NMM, other than dissenting shareholders, is required to enter into a Lock-Up Agreement with ApolloMed. Under the terms of the Lock-Up Agreement, each NMM shareholder will agree not to, without the prior written consent of ApolloMed and except in limited circumstances (i) offer, pledge, sell, contract to sell, sell any option or contract purchase, purchase any option or contract to sell, grant any option, right or warrant to purchase or otherwise transfer or dispose of Covered Securities (as defined in the Lock-Up Agreement) or (ii) enter into any swap or other agreement that transfers, in whole or in part, any of the economic consequences of ownership of the Covered Securities (as defined in the Lock-Up Agreement).
The lock-up restrictions terminate with respect to one-third of the shares of ApolloMed common stock issued in connection with the Merger immediately following each of (i) the 18th month anniversary of the Effective Time of the Merger, (ii) the 30th month anniversary of the Effective Time of the Merger and (iii) the 42nd month anniversary of the Effective Time of the Merger.
| 172 |
MARKET PRICE AND DIVIDEND INFORMATION
As of [●], 2017, there were approximately [●] stockholders of record holding [●] shares of ApolloMed’s common stock. This number does not include an indeterminate number of stockholders whose shares are held by brokers in street name. The holders of ApolloMed’s common stock are entitled to one vote for each share held of record on all matters submitted to a vote of stockholders. Holders of ApolloMed’s common stock have no preemptive rights and no right to convert their common stock into any other securities. There are no redemption or sinking fund provisions applicable to ApolloMed’s common stock.
ApolloMed’s common stock is currently quoted on OTC Pink and traded under the symbol “AMEH.” On December 21, 2016, the last full trading day before the announcement of the Merger, the last reported sale price of ApolloMed common stock was $3.99 per share, and, on [·], 2017, the latest practicable date prior to the date of this joint proxy statement/prospectus, the last reported sale price of ApolloMed common stock was $[·] per share. ApolloMed has applied for listing of its common stock on the NASDAQ Global Market effective as of the closing of the Merger. NMM is a privately held company, and there is no established public trading market for its securities.
The following table sets forth the range of the high and low bid prices of ApolloMed’s common stock for the periods indicated. The quotations below reflect inter-dealer prices, without retail markup, markdown or commissions and may not necessarily represent actual transactions.
| High | Low | |||||||
| Fiscal Year ending March 31, 2018 | ||||||||
| First Quarter | $ | 11.00 | $ | 8.25 | ||||
| Second Quarter | 10.00 | 8.00 | ||||||
| Third Quarter (through October 24, 2017) | 9.75 | 8.00 | ||||||
| High | Low | |||||||
| Fiscal Year ended March 31, 2017 | ||||||||
| First Quarter | $ | 7.50 | $ | 3.75 | ||||
| Second Quarter | 6.00 | 3.55 | ||||||
| Third Quarter | 9.00 | 1.41 | ||||||
| Fourth Quarter | 10.25 | 7.50 | ||||||
| High | Low | |||||||
| Fiscal Year ended March 31, 2016 | ||||||||
| First Quarter | $ | 9.75 | $ | 3.75 | ||||
| Second Quarter | 10.00 | 6.00 | ||||||
| Third Quarter | 7.25 | 4.75 | ||||||
| Fourth Quarter | 6.00 | 4.00 | ||||||
Dividends
To date ApolloMed has not paid any cash dividends on its common stock and does not contemplate the payment of cash dividends in the foreseeable future. ApolloMed’s future dividend policy will depend on its earnings, capital requirements, financial condition and other factors considered relevant to ApolloMed’s ability to pay dividends.
| 173 |
UNAUDITED PRO FORMA CONDENSED COMBINED FINANCIAL STATEMENTS
On December 21, 2016, Apollo Medical Holdings, Inc., a Delaware corporation (“ApolloMed”), Network Medical Management, Inc., a California corporation (“NMM”), Apollo Acquisition Corp., a California corporation and a wholly owned subsidiary of ApolloMed (“Merger Sub”), and Kenneth Sim (the “Shareholders’ Representative”) entered into an agreement and plan of merger (as amended on March 30, 2017 and October 17, 2017, the “Merger Agreement”) that provides for, among other things, the merger of Merger Sub with and into NMM, with NMM continuing as the surviving entity and a wholly owned subsidiary of ApolloMed, on the terms and conditions set forth in the Merger Agreement (the “Merger”). The boards of directors of each of ApolloMed and NMM have approved the Merger Agreement and the transactions contemplated by the Merger Agreement, including the Merger. If consummated, the Merger will be made effective at the time of filing a certificate of merger (the “Certificate of Merger”) with the Secretary of State of the State of California or at such later time as agreed to by the parties in writing and specified in the Certificate of Merger (the “Effective Time”).
Pursuant to the Merger Agreement, at the Effective Time, each issued and outstanding share of NMM common stock will be converted into the right to receive (i) such number of fully paid and nonassessable ApolloMed shares of common stock that results in the NMM shareholders having a right to receive an aggregate number of shares of ApolloMed common stock that represents 82% of the total issued and outstanding shares of ApolloMed common stock immediately following the Effective Time, assuming there are no NMM dissenting shareholder interests as of the Effective Time (the “exchange ratio”), plus (ii) an aggregate of 2,566,666 ApolloMed common stock, assuming there are no NMM dissenting shareholder interests as of the Effective Time, and (iii) warrants to purchase a pro-rata portion of an aggregate of 850,000 shares of common stock of ApolloMed, exercisable at $11.00 per share and warrants to purchase an aggregate of 900,000 shares of common stock of ApolloMed at $10.00 per share. At the Effective Time, pre-Merger ApolloMed stockholders will continue to own and hold their existing shares of ApolloMed common stock. At the Effective Time, ApolloMed will hold back 10% of the total number of shares of ApolloMed common stock issuable to pre-Merger NMM shareholders in the Merger to secure indemnification of ApolloMed and its affiliates under the Merger Agreement. Separately, indemnification of pre-Merger NMM shareholders under the Merger Agreement will be made by the issuance by ApolloMed to pre-Merger NMM shareholders of new additional shares of common stock (capped at the same number of shares of ApolloMed common stock as are subject to the holdback for the indemnification of ApolloMed).
For purposes of calculating the exchange ratio, (A) the aggregate number of shares of ApolloMed common stock held by the NMM shareholders immediately following the Effective Time will exclude (i) any shares of ApolloMed common stock owned by NMM shareholders immediately prior to the Effective Time, (ii) the Series A warrant and Series B warrant issued by ApolloMed to NMM to purchase ApolloMed common stock (the “ApolloMed Warrants”) and (iii) any shares of ApolloMed common stock issued or issuable to NMM shareholders pursuant to the exercise of the ApolloMed Warrants, and (B) the total number of issued and outstanding shares of ApolloMed common stock immediately following the Effective Time shall exclude 499,000 shares of ApolloMed common stock issued or issuable under a Convertible Promissory Note to Alliance Apex, LLC (“Alliance”) for $4.99 million pursuant to the Securities Purchase Agreement between ApolloMed and Alliance dated as of March 30, 2017.
The following unaudited pro forma condensed combined balance sheet as of June 30, 2017 and the unaudited pro forma condensed combined statement of operations for the three months ended June 30, 2017 and the fiscal year ended March 31, 2017, which give effect to the proposed Merger of Merger Sub with and into NMM, are presented herein. The proposed Merger will be accounted for as a “reverse merger” business combination under the acquisition method of accounting with NMM treated as the accounting acquirer. NMM was determined to be the accounting acquirer based upon the terms of the Merger and other factors, such as relative voting rights and the composition of the combined company’s board of directors and senior management. The unaudited pro forma condensed combined balance sheet combines the unaudited condensed balance sheets of ApolloMed and NMM as of June 30, 2017 and gives effect to the Merger as if it had been completed on June 30, 2017. In addition, because NMM has a fiscal year end of December 31 and ApolloMed has a fiscal year end of March 31, the unaudited pro forma condensed combined statement of operations for the three months ended June 30, 2017 combine the historical condensed statement of operations of ApolloMed for its three months ended June 30, 2017 and the historical condensed statement of operations of NMM for its three months ended March 31, 2017 giving pro forma effect to the Merger as if it had been completed on April 1, 2017 and January 1, 2017, respectively.; and for the fiscal year ended March 31, 2017 combine the historical condensed statement of operations of ApolloMed for its fiscal year ended March 31, 2017 and the historical condensed statement of operations of NMM for its fiscal year ended December 31, 2016, giving pro forma effect to the Merger as if it had been completed on April 1, 2016 and January 1, 2016, respectively. The historical financial information has been adjusted in the unaudited pro forma condensed combined financial statements to give effect to pro forma events that are (1) directly attributable to the Merger, (2) factually supportable, and (3) with respect to the statements of operations, expected to have a continuing impact on the combined company.
| 174 |
The unaudited pro forma condensed combined financial statements presented are based on the assumptions and adjustments described in the accompanying notes. The unaudited pro forma condensed combined financial statements are presented for illustrative purposes and do not purport to represent what the financial position or results of operations would actually have been if the Merger occurred as of the dates indicated or what such financial position or results will be for any future periods for the combined company. The unaudited pro forma condensed combined financial statements are based upon the respective historical consolidated financial statements of ApolloMed and NMM as outline above, and should be read in conjunction with the:
| · | accompanying notes to the unaudited pro forma condensed combined financial statements; | |
| · | the historical audited consolidated financial statements of ApolloMed as of and for the fiscal years ended March 31, 2017 and 2016 included in this joint proxy statement/prospectus; |
| · | the historical unaudited condensed consolidated financial statements of ApolloMed as of and for the three months ended June 30, 2017 and 2016 included in this joint proxy statement/prospectus; | |
| · | the historical audited consolidated financial statements of NMM as of and for the fiscal years ended December 31, 2016, 2015 and 2014 included in this joint proxy statement/prospectus; | |
| · | the historical unaudited condensed consolidated financial statements of NMM as of and for the three and six months ended June 30, 2017 and 2016 included in this joint proxy statement/prospectus; and | |
| · | management’s discussion and analysis of financial condition and results of operations for both ApolloMed and NMM and “Risk Factors” included in this joint proxy statement/prospectus. |
The application of the acquisition method of accounting is dependent upon certain valuations and other studies that have yet to be completed or have not progressed to a stage where there is sufficient information for a definitive measurement. Accordingly, the pro forma adjustments are preliminary, subject to further revision as additional information becomes available and additional analyses are performed, and have been made solely for the purpose of providing unaudited pro forma condensed combined financial statements. Upon consummation of the Merger, final valuations and studies will be performed. Differences between these preliminary estimates and the final acquisition accounting may occur and these differences could have a material impact on the accompanying unaudited pro forma condensed combined financial statements and the combined company’s future financial position and results of operations. Fair values determined as of the assumed acquisition dates are based on the most recently available information. To the extent there are significant changes to ApolloMed’s or NMM’s business, or as new information becomes available, the assumptions and estimates herein could change significantly.
Because NMM will be treated as the accounting acquirer, NMM’s assets and liabilities will be recorded at their precombination carrying amounts and the historical operations that are reflected in the financial statements will be those of NMM. ApolloMed’s assets and liabilities will be measured and recognized at their fair values as of the date of the Merger, and consolidated with the assets, liabilities and results of operations of NMM after the consummation of the Merger.
The unaudited pro forma condensed combined statements of operations include certain acquisition accounting adjustments. The unaudited pro forma condensed combined statements of operations do not include the impact of any revenue, cost or other operating synergies that may result from the Merger or any related restructuring costs. The unaudited pro forma condensed combined statements of operations do not reflect certain amounts resulting from the Merger that were determined to be of a nonrecurring nature.
| 175 |
UNAUDITED PRO FORMA CONDENSED COMBINED BALANCE SHEET
As of June 30, 2017
| Historical | ||||||||||||||||||||||
| ApolloMed | NMM | Pro forma adjustments for Merger | Pro forma adjustments for Purchase Accounting | Pro Forma Combined | ||||||||||||||||||
| Assets | ||||||||||||||||||||||
| Cash and cash equivalents | $ | 31,206,495 | $ | 65,787,183 | $ | (8,465,197 | ) | 5(i) | $ | 88,528,481 | ||||||||||||
| 4,000,000 | 5(f) | |||||||||||||||||||||
| (4,000,000 | ) | 5(f) | ||||||||||||||||||||
| Restricted cash | - | - | - | - | - | |||||||||||||||||
| Fiduciary cash | - | 1,047,828 | - | - | 1,047,828 | |||||||||||||||||
| Investment in marketable securities | - | 1,053,108 | - | 1,053,108 | ||||||||||||||||||
| Accounts receivable, net | 5,423,618 | 2,814,363 | - | 8,237,981 | ||||||||||||||||||
| Other receivables | 806,148 | 5,624,622 | (438,307 | ) | 5(m) | - | 5,935,067 | |||||||||||||||
| (57,396 | ) | 5(g) | ||||||||||||||||||||
| Loan receivable | - | - | - | - | ||||||||||||||||||
| Prepaid expenses and other current assets | 282,732 | 1,889,268 | - | - | 2,172,000 | |||||||||||||||||
| Total current assets | 37,718,993 | 78,216,372 | (8,960,900 | ) | - | 106,974,465 | ||||||||||||||||
| Property and equipment, net | 1,167,680 | 10,583,715 | - | - | 11,751,395 | |||||||||||||||||
| Loans receivable | - | 10,000,000 | (5,000,000 | ) | 5(f) | - | 5,000,000 | |||||||||||||||
| 9,043,146 | 5(f) | |||||||||||||||||||||
| (9,043,146 | ) | 5(f) | ||||||||||||||||||||
| Investments in other entities - equity method | - | 24,688,225 | - | - | 24,688,225 | |||||||||||||||||
| Investments in other entities - cost method | - | 10,550,002 | (10,550,002 | ) | 5(b) | - | - | |||||||||||||||
| Derivative asset - warrants | - | 5,466,665 | (5,466,665 | ) | 5(k) | - | - | |||||||||||||||
| Restricted cash | 745,117 | - | - | - | 745,117 | |||||||||||||||||
| Intangible assets, net | 1,822,542 | 99,396,732 | - | (1,822,542 | ) | 4(e) | 116,941,732 | |||||||||||||||
| 17,545,000 | 4(a) | |||||||||||||||||||||
| Goodwill | 1,622,483 | 103,407,351 | - | (1,622,483 | ) | 4(f) | 162,399,418 | |||||||||||||||
| 58,992,067 | 3 | |||||||||||||||||||||
| Deferred tax assets | - | - | - | 2,432,950 | 4(b) | 2,432,950 | ||||||||||||||||
| Other assets | 221,979 | 1,472,430 | - | - | 1,694,409 | |||||||||||||||||
| Total Assets | $ | 43,298,794 | $ | 343,781,492 | $ | (29,977,567 | ) | $ | 75,524,992 | $ | 432,627,711 | |||||||||||
| Liabilities, mezzanine equity and stockholders' equity | ||||||||||||||||||||||
| Accounts payable and accrued liabilities | $ | 16,212,983 | $ | 6,274,556 | $ | (57,396 | ) | 5(g) | $ | - | $ | 24,991,836 | ||||||||||
| (438,307 | ) | 5(m) | ||||||||||||||||||||
| 500,000 | 6 | 2,500,000 | 6 | |||||||||||||||||||
| Capitation and incentives payables | - | 11,600,000 | - | - | 11,600,000 | |||||||||||||||||
| Fiduciary accounts payable | - | 1,047,828 | - | - | 1,047,828 | |||||||||||||||||
| Income taxes payable | - | 6,672,106 | - | - | 6,672,106 | |||||||||||||||||
| Medical liabilities | 19,718,135 | 18,519,670 | - | - | 38,237,805 | |||||||||||||||||
| Convertible note payable, net | 4,882,667 | - | (5,142,000 | ) | 5(c) | 259,333 | 4(i) | - | ||||||||||||||
| 9,043,146 | 5(f) | |||||||||||||||||||||
| (9,043,146 | ) | 5(f) | ||||||||||||||||||||
| Capital Lease | - | 47,793 | - | - | 47,793 | |||||||||||||||||
| Line of credit | 25,000 | - | - | - | 25,000 | |||||||||||||||||
| Total current liabilities | 40,838,785 | 44,161,953 | (5,137,703 | ) | 2,759,333 | 82,622,368 | ||||||||||||||||
| Note payable - related party | 5,000,000 | - | (5,000,000 | ) | 5(f) | - | - | |||||||||||||||
| Stock liability for unissued shares | - | 2,422,675 | - | - | 2,422,675 | |||||||||||||||||
| Deferred rent liability | 715,462 | - | - | (715,462 | ) | 4(c) | - | |||||||||||||||
| Deferred tax liability | 83,667 | 42,512,506 | - | (83,667 | ) | 4(c) | 42,512,506 | |||||||||||||||
| Total liabilities | $ | 46,637,914 | $ | 89,097,134 | $ | (10,137,703 | ) | $ | 1,960,204 | $ | 127,557,549 | |||||||||||
| Commitments and Contingencies | ||||||||||||||||||||||
| Mezzanine equity | ||||||||||||||||||||||
| Noncontrolling interest | - | 160,407,386 | - | 10,238,000 | 4(k) | 170,645,386 | ||||||||||||||||
| Network Medical Management, Inc. redeemable common stock | - | 86,894,870 | (86,894,870 | ) | 5(j) | - | - | |||||||||||||||
| Additional paid-in capital | - | 1,322,246 | (1,322,246 | ) | 5(j) | - | - | |||||||||||||||
| Total Network Medical Management, Inc. redeemable common stock | - | 88,217,116 | (88,217,116 | ) | - | - | ||||||||||||||||
| Stockholders' equity | ||||||||||||||||||||||
| Series A Preferred stock | 7,077,778 | - | - | (7,077,778 | ) | 4(j) | - | |||||||||||||||
| Series B Preferred stock | 3,884,745 | - | - | (3,884,745 | ) | 4(j) | - | |||||||||||||||
| Common stock | 6,033 | - | - | - | 3 | 36,586 | ||||||||||||||||
| 500 | 5(c) | - | ||||||||||||||||||||
| 30,053 | 5(a) 5(j) | - | ||||||||||||||||||||
| Additional paid-in capital | 26,555,514 | - | - | (26,555,514 | ) | 4(d) | 119,158,201 | |||||||||||||||
| - | 66,378,635 | 3 | ||||||||||||||||||||
| 4,997,700 | 5(c) | - | ||||||||||||||||||||
| (10,238,000 | ) | 4(k) | ||||||||||||||||||||
| (18,197,000 | ) | 5(b) | ||||||||||||||||||||
| 88,187,063 | 5(j) | |||||||||||||||||||||
| (8,465,197 | ) | 5(i) | ||||||||||||||||||||
| (3,505,000 | ) | 5(l) | ||||||||||||||||||||
| Retained earnings (accumulated deficit) | (41,266,193 | ) | 5,571,093 | - | 41,266,193 | 4(d) | 10,900,226 | |||||||||||||||
| (500,000 | ) | 6 | ||||||||||||||||||||
| 7,646,998 | 5(b) | |||||||||||||||||||||
| (43,146 | ) | 5(f) | ||||||||||||||||||||
| 43,146 | 5(f) | |||||||||||||||||||||
| 143,800 | 5(c) | |||||||||||||||||||||
| 33,335 | 5(k) | |||||||||||||||||||||
| 3,505,000 | 5(l) | |||||||||||||||||||||
| (5,500,000 | ) | 5(k) | ||||||||||||||||||||
| Noncontrolling interest | 403,003 | 488,763 | - | 3,437,997 | 4(g) | 4,329,763 | ||||||||||||||||
| Total stockholders' equity | (3,339,120 | ) | 6,059,856 | 68,377,252 | 63,326,788 | 134,424,776 | ||||||||||||||||
| Total liabilities, mezzanine equity and stockholders' equity | $ | 43,298,794 | $ | 343,781,492 | $ | (29,977,567 | ) | $ | 75,524,992 | $ | 432,627,711 | |||||||||||
| Book value per share | $ | (0.55 | ) | $ | 0.02 | $ | 3.67 | |||||||||||||||
The accompanying notes are an integral part of the unaudited pro forma condensed combined financial statements.
| 176 |
UNAUDITED PRO FORMA CONDENSED COMBINED STATEMENT OF OPERATIONS
For the three months ended June 30, 2017
| Historical | ||||||||||||||||||||||
| Apollo Q1 2018 FS | NMM Q1 2017 FS |
|||||||||||||||||||||
| ApolloMed | NMM | Pro
forma adjustments for Merger |
Pro
forma adjustments for purchase accounting |
Pro
Forma Combined |
||||||||||||||||||
| Net revenues | $ | 41,575,480 | $ | 85,336,062 | $ | (1,162,122 | ) | 5(h) | $ | - | $ | 125,749,420 | ||||||||||
| Cost and expenses: | ||||||||||||||||||||||
| Cost of services | 40,239,642 | 59,542,572 | (1,162,122 | ) | 5(h) | - | 98,620,092 | |||||||||||||||
| General and administrative | 4,889,184 | 5,276,575 | - | - | 10,165,759 | |||||||||||||||||
| - | - | |||||||||||||||||||||
| Depreciation and amortization | 155,267 | 4,836,351 | - | (81,725 | ) | 4(h) | 5,335,005 | |||||||||||||||
| - | 425,112 | 4(a) | ||||||||||||||||||||
| Impairment of goodwill and other | - | - | - | - | - | |||||||||||||||||
| Total costs and expenses | 45,284,093 | 69,655,498 | (1,162,122 | ) | 343,387 | 114,120,856 | ||||||||||||||||
| Income (loss) from operations | (3,708,613 | ) | 15,680,564 | - | (343,387 | ) | 11,628,564 | |||||||||||||||
| Other income (expense): | ||||||||||||||||||||||
| Interest expense | (192,989 | ) | (811 | ) | 63,194 | 5(d) | - | (130,606 | ) | |||||||||||||
| Gain (loss) on change in fair value of warrant and conversion feature liabilities | - | 1,522,222 | - | - | 1,522,222 | |||||||||||||||||
| Gain (loss) on debt extinguishment | - | - | (43,146 | ) | 5(f) | - | - | |||||||||||||||
| 43,146 | 5(f) | |||||||||||||||||||||
| Income from equity method investments | - | 2,227,262 | - | - | 2,227,262 | |||||||||||||||||
| Loss on debt extinguishment | - | - | - | - | - | |||||||||||||||||
| Other income | 38,657 | 183,799 | (63,194 | ) | 5(d) | - | 159,262 | |||||||||||||||
| Total other income (expense), net | (154,332 | ) | 3,932,472 | - | - | 3,778,140 | ||||||||||||||||
| Income (loss) before (benefit from) provision for income taxes | (3,862,945 | ) | 19,613,036 | - | (343,387 | ) | 15,406,704 | |||||||||||||||
| (Benefit from) provision for income taxes | (29,891 | ) | 7,889,245 | - | (139,916 | ) | 5(e) | 7,719,438 | ||||||||||||||
| Net income (loss) | $ | (3,833,054 | ) | $ | 11,723,791 | $ | - | $ | (203,470 | ) | $ | 7,687,267 | ||||||||||
| Net (loss) income attributable to non-controlling interest | (221,242 | ) | 7,374,130 | (946,515 | ) | 5(n) | 6,206,373 | |||||||||||||||
| Net income (loss) attributable to Network Medical Management/Apollo Medical Holdings, Inc. | $ | (3,611,812 | ) | $ | 4,349,661 | $ | 946,515 | $ | (203,470 | ) | $ | 1,480,894 | ||||||||||
| Net loss per share attributable to common shareholders, basic | $ | (0.60 | ) | $ | 0.01 | $ | 0.04 | |||||||||||||||
| Weighted average number of common shares outstanding - basic | 6,033,518 | 366,343,818 | 30,551,775 | 5(o) | 36,585,293 | |||||||||||||||||
| Net loss per share attributable to common shareholders, diluted | $ | 0.01 | $ | 0.04 | ||||||||||||||||||
| Weighted average number of common shares outstanding - diluted | 374,134,971 | 40,616,420 | ||||||||||||||||||||
The accompanying notes are an integral part of the unaudited pro forma condensed combined financial statements.
| 177 |
UNAUDITED PRO FORMA CONDENSED COMBINED STATEMENT OF OPERATIONS
For the fiscal year ended March 31, 2017
| Historical | ||||||||||||||||||||||
| ApolloMed (FYE 3/31/17) |
NMM (FYE 12/31/2016) |
Pro
forma adjustments for Merger |
Pro
forma adjustments for purchase accounting |
Pro
Forma Combined |
||||||||||||||||||
| Net revenues | $ | 57,427,701 | $ | 305,934,915 | $ | (5,182,181 | ) | 5(h) | $ | - | $ | 358,180,435 | ||||||||||
| Cost and expenses: | ||||||||||||||||||||||
| Cost of services | 48,735,537 | 254,468,120 | (4,867,181 | ) | 5(h) | - | 298,336,476 | |||||||||||||||
| General and administrative | 18,583,372 | 21,339,436 | - | - | 39,607,808 | |||||||||||||||||
| (315,000 | ) | 5(h) | - | |||||||||||||||||||
| Depreciation and amortization | 645,742 | 18,114,440 | - | (380,632 | ) | 4(h) | 20,080,001 | |||||||||||||||
| - | 1,700,451 | 4(a) | ||||||||||||||||||||
| Impairment of goodwill and other | - | 324,306 | - | - | 324,306 | |||||||||||||||||
| Total costs and expenses | 67,964,651 | 294,246,302 | (5,182,181 | ) | 1,319,819 | 358,348,591 | ||||||||||||||||
| Income (loss) from operations | (10,536,950 | ) | 11,688,613 | - | (1,319,819 | ) | (168,156 | ) | ||||||||||||||
| Other income (expense): | ||||||||||||||||||||||
| Interest expense | (82,905 | ) | (61,589 | ) | 57,396 | 5(d) | - | (87,098 | ) | |||||||||||||
| Gain (loss) on change in fair value of warrant and conversion feature liabilities | 1,633,333 | 1,722,221 | - | - | 3,355,554 | |||||||||||||||||
| Income from equity method investments | - | 4,748,542 | - | - | 4,748,542 | |||||||||||||||||
| Gain on deconsolidation of variable interest entity | 242,411 | - | - | - | 242,411 | |||||||||||||||||
| Gain (loss) on debt extinguishment | - | - | (43,146 | ) | 5(f) | - | - | |||||||||||||||
| - | - | 43,146 | 5(f) | - | - | |||||||||||||||||
| Other income | 14,701 | 738,422 | - | - | 753,123 | |||||||||||||||||
| Total other income (expense), net | 1,807,540 | 7,147,596 | 57,396 | - | 9,012,532 | |||||||||||||||||
| Income (loss) before (benefit from) provision for income taxes | (8,729,410 | ) | 18,836,209 | (57,396 | ) | (1,319,819 | ) | 8,844,376 | ||||||||||||||
| (Benefit from) provision for income taxes | (47,495 | ) | 8,816,412 | 23,387 | 5(e) | (537,773 | ) | 5(e) | 8,254,530 | |||||||||||||
| Net income (loss) | $ | (8,681,915 | ) | $ | 10,019,797 | $ | 34,009 | $ | (782,046 | ) | $ | 589,846 | ||||||||||
| Net (loss) income attributable to non-controlling interest | 287,901 | (1,433,730 | ) | 709,810 | 5(n) | - | (436,019 | ) | ||||||||||||||
| Net income (loss) attributable to Network Medical Management/Apollo Medical Holdings, Inc. | $ | (8,969,816 | ) | $ | 11,453,527 | $ | (675,801 | ) | $ | (782,046 | ) | $ | 1,025,865 | |||||||||
| Net loss per share attributable to common shareholders, basic | $ | (1.49 | ) | $ | 0.03 | $ | 0.03 | |||||||||||||||
| Weighted average number of common shares outstanding - basic | 6,001,680 | 360,634,339 | 27,942,039 | 5(o) | 33,943,719 | |||||||||||||||||
| Net loss per share attributable to common shareholders, diluted | $ | 0.03 | $ | 0.03 | ||||||||||||||||||
| Weighted average number of common shares outstanding - diluted | 367,945,833 | 36,651,835 | ||||||||||||||||||||
The accompanying notes are an integral part of the unaudited pro forma condensed combined financial statements.
| 178 |
Notes to Unaudited Pro Forma Condensed Combined Financial Statements
1. Description of the Business Combination and Basis of Pro Forma Presentation
The unaudited pro forma condensed combined financial statements were prepared in accordance with accounting principles generally accepted in the United States of America and pursuant to the rules and regulations of SEC Regulation S-X, and present the pro forma financial position and results of operations of the combined companies based upon the historical data of ApolloMed and NMM after giving effect to the Merger.
2. Preliminary Purchase Consideration
The fair value of the purchase consideration expected to be transferred on the closing date includes the value of the estimated equity consideration, the fair value of the pre-existing ApolloMed Series A preferred stock and Series B preferred stock held by NMM on the acquisition date, the fair value of NMM’s 50% share in APA ACO, Inc. (“APAACO”), and the fair value of unvested ApolloMed stock options, less the fair value of the warrants to be issued to the shareholders of NMM by ApolloMed at closing. The fair value per share of ApolloMed common stock was assumed for pro forma purposes to be $8.01 per share. This is the closing price of ApolloMed on October 17, 2017 and may change significantly if the trading price of ApolloMed’s common stock fluctuates materially from the market value as of October 17, 2017. The accompanying unaudited pro forma condensed combined financial statements reflect an estimated preliminary purchase price of approximately $66.4 million.
The calculation of the estimated preliminary purchase consideration is as follows:
Estimated equity consideration
ApolloMed will issue in the aggregate to NMM shareholders (i) a number of shares of ApolloMed common stock, which will represent 82% of the total issued and outstanding shares of ApolloMed common stock immediately following the Effective Time, assuming there are no NMM dissenting shareholder interests as of the Effective Time and (ii) 2,566,666 shares of ApolloMed common stock, assuming there are no NMM dissenting shareholder interests as of the Effective Time. In addition, NMM shareholders will receive their pro rata share of (i) warrants to purchase 850,000 shares of ApolloMed common stock at an exercise price of $11 per share and (ii) warrants to purchase 900,000 shares of ApolloMed common stock, at an exercise price of $10 per share. The estimated preliminary equity consideration, which represents a portion of the consideration deemed transferred to the ApolloMed stockholders in the Merger, is calculated based on the number of shares of the combined company that ApolloMed stockholders will own as of the closing of the Merger.
| Estimated number of shares of the combined company to be owned by ApolloMed stockholders(1) | 6,033,500 | |||
| Multiplied by the assumed price per share of ApolloMed common stock (2) | $ | 8.01 | ||
| Estimated equity consideration | $ | 48,328,335 |
| 179 |
| (1) | Represents the estimated number of shares of the combined company that ApolloMed stockholders would own at closing of the Merger. |
| (2) | Represents the closing price of ApolloMed common stock on October 17, 2017. The fair value of the consideration transferred in the Merger will ultimately be measured using the actual closing price of ApolloMed common stock on the Merger closing date. A 10% increase or decrease in the closing trading price of ApolloMed’s common stock on October 17, 2017 would cause a corresponding increase or decrease in the fair value of consideration transferred of $4,832,833. |
Fair value of ApolloMed’s preferred shares held by NMM
NMM currently owns all the shares of ApolloMed Series A preferred stock and Series B preferred stock. As part of the Merger, the ApolloMed Series A preferred stock and Series B preferred stock is remeasured at fair value and included as part of the consideration transferred to ApolloMed. The fair value of the Series A preferred stock and Series B preferred stock is reflective of the liquidation preferences, claims of priority and conversion option values thereof. In aggregate, the Series A preferred stock and Series B preferred stock were valued to be $18,197,000. The valuation methodology was based on an Option Pricing Method ("OPM") which utilized the observable publicly traded common stock price in valuing the Series A preferred stock and the Series B preferred stock within the context of the capital structure of the Company. OPM assumptions included an expected term of 5 years, volatility rate of 38.9%, and a Rf-rate of 1.5%. The fair value of the liquidation preference for the Series A preferred stock and the Series B preferred stock was determined to be $13,340,000 and the fair value of the conversion option was determined to be $4,857,000 or an aggregate total fair value of $18,197,000.
Fair value of NMM’s 50% share of APA ACO Inc.
APA ACO Inc. (“APAACO”) a Next Generation Accountable Care Organization (“NGACO”) is owned 50% by ApolloMed and 50% NMM. NMM’s noncontrolling interest in APAACO has been remeasured at fair value as of the closing date and is added to the consideration transferred to ApolloMed as a result of NMM relinquishing its equity investment in APAACO in order to obtain control of ApolloMed. The fair value of NMM’s noncontrolling interest in APAACO has been estimated to be $3,505,000.
Fair value of the ApolloMed outstanding stock options
The estimated fair value of the outstanding ApolloMed stock options is included in consideration transferred in accordance with ASC 805. The outstanding ApolloMed stock options are expected to vest in conjunction with the Merger due to a pre-existing change-of-control provision associated with the awards. There is no future service requirement.
Fair value of warrants to be issued by ApolloMed to NMM shareholders
The fair value of the warrants to purchase 850,000 and 900,000 shares of ApolloMed common stock to be issued to the NMM shareholders as part of the merger consideration at the time of the Merger represents a reduction in the estimated purchase consideration for ApolloMed.
The total estimated equity consideration was recorded to common stock at par ($.001 per share) and the remainder to additional paid-in capital.
| 180 |
Total estimated preliminary purchase consideration consists of the following:
| Estimated equity consideration | $ | 48,328,335 | ||
| Estimated fair value of ApolloMed preferred stock held by NMM | $ | 18,197,000 | ||
| Estimated fair value of NMM’s noncontrolling interest in APAACO | $ | 3,505,000 | ||
| Estimated fair value of the outstanding ApolloMed stock options | $ | 298,333 | ||
| Estimated fair value of the warrants to be issued to NMM’s shareholders by ApolloMed | $ | (3,944,000 | ) | |
| Total estimated preliminary purchase consideration | $ | 66,384,668 |
MMG transaction
In conjunction with the Merger, Warren Hosseinion M.D., the sole shareholder of Maverick Medical Group (“MMG”), will sell to APC-LSMA Designated Shareholder Medical Corporation (“APC-LSMA”) all the issued and outstanding shares of capital stock of MMG. MMG has historically been included in the consolidated financial statement filed by ApolloMed. APC-LSMA will pay $100 to Warren Hosseinion M.D. in consideration for all the shares of MMG. As the transaction is between related parties, the purchase consideration of MMG reflected in the preliminary purchase price allocation was determined to be the fair value of MMG. It is anticipated that MMG and Apollo Medical Management (“AMM”) will terminate the existing Management Services Agreement between them (the “MMG Management Agreement”) and APC-LSMA will pay AMM $400,000 as a termination payment on or before the Effective Time. APC-LSMA is owned 100% by Dr. Lam. APC-LSMA has historically been included in the consolidated financial statement of Allied Physicians of California IPA dba Allied Pacific IPA (“APC”) which in turn is included in the consolidated financial statement of NMM. For purposes of the pro forma financial statements, the MMG transaction will be accounted for within the combined group, with the MMG transaction being reflected within non-controlling interest. The preliminary purchase consideration and preliminary purchase price allocation will incorporate both acquisitions.
3. Preliminary Purchase Price Allocation
Under the acquisition method of accounting, the identifiable assets acquired and liabilities assumed of ApolloMed, the accounting acquiree, are recorded at the Merger date fair values and added to those of NMM, the accounting acquiror. The pro forma adjustments are preliminary and based on estimates of the fair value and useful lives of the assets acquired and liabilities assumed and have been prepared to illustrate the estimated effect of the Merger between NMM and ApolloMed and the acquisition of MMG by APC-LSMA. The final purchase price allocation is dependent upon certain valuation and other studies that have not yet been completed. The final determination of the purchase price allocation, upon the consummation of the Merger, will be based on ApolloMed’s net assets acquired as of that date and will depend on a number of factors, which cannot be predicted with any certainty at this time. The purchase price allocation may change materially based on the receipt of more detailed information. Accordingly, the pro forma purchase price allocation is preliminary and is subject to further adjustment as additional information becomes available and as additional analyses and final valuations are completed. There can be no assurance that these additional analyses and final valuations will not result in significant changes to the estimates of fair value set forth below.
The following table sets forth a preliminary allocation of the estimated preliminary purchase price to the identifiable tangible and intangible assets acquired and liabilities assumed of ApolloMed and MMG based on ApolloMed’s consolidated balance sheet as of June 30, 2017, with the excess recorded as goodwill:
| Assets acquired | ||||
| Cash and cash equivalents | $ | 35,206,495 | ||
| Accounts receivable | 5,423,618 | |||
| Other receivables | 806,148 | |||
| Due from affiliates | - | |||
| Prepaid expenses | 282,732 | |||
| PPE | 1,167,680 | |||
| Restricted cash | 745,117 | |||
| Fair value of intangible assets acquired | 17,545,000 | |||
| Deferred tax assets | 2,432,950 | |||
| Other assets | 221,979 | |||
| Total assets acquired | $ | 63,831,719 | ||
| Liabilities assumed | ||||
| Accounts payable and accrued liabilities | $ | 18,712,983 | ||
| Medical liabilities | 19,718,135 | |||
| Line of credit | 25,000 | |||
| Convertible note payable, net | 5,142,000 | |||
| Convertible note payable - related party | 9,000,000 | |||
| Noncontrolling interest | 3,841,000 | |||
| Total liabilities assumed and noncontrolling interest | $ | 56,439,118 | ||
| Net assets acquired | $ | 7,392,601 | ||
| Goodwill | $ | 58,992,067 |
| 181 |
Goodwill represents the excess of the preliminary estimated purchase consideration over the fair value of the underlying net assets acquired. Goodwill is not amortized but instead is reviewed for impairment at least annually, and potentially more frequent if there are any indicators of impairment.
The pro forma historical net book value adjustments and goodwill adjustment as shown above are further described in Note 4 of Notes to Unaudited Pro Forma Condensed Combined Financial Information.
4. Purchase Accounting Adjustments
| (a) | The following table indicates the preliminary estimated fair value of each of the ApolloMed identifiable intangible assets and the related estimated useful life thereof: |
| Preliminary estimated fair value |
Weighted average useful life (years) |
Estimated amortization expense for the three months ended June 30, 2017 |
||||||||||
| Indefinite lived assets: | ||||||||||||
| Medicare license | $ | 3,129,000 | $ | - | ||||||||
| Amortized intangible assets: | ||||||||||||
| Network relationships | 2,948,000 | 10 | 73,700 | |||||||||
| Member relationships | 7,258,000 | 7.8 | 232,628 | |||||||||
| Patient management platform | 2,180,000 | 7 | 77,857 | |||||||||
| Tradename/trademarks | 2,030,000 | 12.4 | 40,927 | |||||||||
| Pro forma adjustment | $ | 17,545,000 | $ | 425,112 | ||||||||
| Preliminary estimated fair value |
Weighted average useful life (years) |
Estimated amortization expense for the year ended March 31, 2017 |
||||||||||
| Indefinite lived assets: | ||||||||||||
| Medicare license | $ | 3,129,000 | $ | - | ||||||||
| Amortized intangible assets: | ||||||||||||
| Network relationships | 2,948,000 | 10 | 294,800 | |||||||||
| Member relationships | 7,258,000 | 7.8 | 930,513 | |||||||||
| Patient management platform | 2,180,000 | 7 | 311,429 | |||||||||
| Tradename/trademarks | 2,030,000 | 12.4 | 163,710 | |||||||||
| Pro forma adjustment | $ | 17,545,000 | $ | 1,700,451 | ||||||||
Preliminary identifiable intangible assets of ApolloMed consist of anticipated intangibles derived from Medicare license, network relationships, member relationships, patient management platform and tradename/trademarks.
| 182 |
The following summarizes the valuation methods used to estimate the fair value of the identifiable intangible assets:
| • | Medicare license - combination of income approach and cost approach – cost to obtain a Medicare license |
| • | Network relationships - income approach — multi-period excess earnings method |
| • | Patient management platform - cost approach – cost to recreate the platform |
| • | Tradename / trademarks - income approach — relief from royalty method |
Medicare license will be accounted for as an indefinite-lived intangible asset as the license is expected to be maintained as long as the business continues its operations.
For purposes of estimating the fair values of the intangible assets, benchmarking information, publicly available information as well as a variety of other assumptions, including market participant assumptions, were used.
The amortization related to the amortizable identifiable intangible assets is reflected on a straight line basis as a pro forma adjustment in the unaudited pro forma condensed combined statements of operations. The identifiable intangible assets and related amortization are preliminary and are based on management’s estimates. As discussed above, the amount that will ultimately be allocated to identifiable intangible assets, and the related amount of amortization, may differ materially from this preliminary allocation. In addition, the periods the amortization impacts will ultimately be based on the periods in which the associated economic benefits or detriments are expected to be derived or, where appropriate, based on the use of a straight-line method. Therefore, the amount of amortization following the closing of the Merger may differ significantly among periods based upon the final value assigned and amortization methodology used for each identifiable intangible asset.
| (b) | Represents the adjustment necessary to conform ApolloMed’s deferred tax assets acquired as of the pro forma assumed closing date to their preliminary estimated fair value. |
| (c) | Represents the elimination of ApolloMed’s deferred rent liability and deferred tax liability as a purchase accounting adjustment. |
| (d) | Reflects the elimination of ApolloMed’s historical additional paid-in capital and accumulated deficit. |
| (e) | Reflects the elimination of ApolloMed’s historical intangible assets. |
| (f) | Reflects the elimination of ApolloMed’s historical goodwill. |
| (g) | Represents the adjustment necessary to increase ApolloMed’s non-controlling interest in Apollo Palliative Services (“APS”) to its estimated fair value as part of the purchase accounting fair value adjustments detailed in Note 3 as summarized in the table below: |
For the three months ended June 30, 2017:
| Elimination of ApolloMed’s historical non-controlling interest | $ | (403,003 | ) | |
| Reflects the estimated fair value of ApolloMed’s non-controlling interest in APS | $ | 3,841,000 | ||
| Pro forma adjustment | $ | 3,437,997 |
For the year ended March 31, 2017:
| Elimination of ApolloMed’s historical non-controlling interest | $ | (624,245 | ) | |
| Reflects the estimated fair value of ApolloMed’s non-controlling interest in APS | $ | 3,841,000 | ||
| Pro forma adjustment | $ | 3,216,755 |
| (h) | Reflects the elimination of ApolloMed’s amortization of historical intangible assets that have been eliminated in purchase accounting for the respective period. |
| 183 |
| (i) | Represents the adjustment necessary to conform ApolloMed’s convertible note payable, net to its preliminary estimated fair value as of the assumed closing date. The convertible note payable was issued to Alliance for $4,990,000 pursuant to the Securities Purchase Agreement dated as of March 30, 2017. |
| (j) | Reflects the elimination of ApolloMed’s historical Series A preferred stock and Series B preferred stock, which are held by NMM. |
| (k) | Reflects the adjustment necessary to reflect the estimated fair value of the MMG purchase price within non-controlling interest. |
5. Accounting Policies and Merger-Related Pro Forma Adjustments
Based on NMM’s review of ApolloMed’s summary of significant accounting policies disclosed in ApolloMed’s financial statements, the nature and amount of any adjustments to the historical financial statements of ApolloMed to conform its accounting policies to those of NMM are not expected to be significant. Upon consummation of the Merger, further review of ApolloMed’s accounting policies and financial statements may result in required revisions to ApolloMed’s policies and classifications to conform to NMM’s accounting policies.
The following pro forma adjustments are based on preliminary estimates, which may change significantly as additional information is obtained:
| (a) | To record the conversion or exchange of NMM common stock into shares of ApolloMed common stock as follows: |
| Estimated number of shares of the combined company on an as-converted basis following the exchange | 33,520,000 | |||
| Multiplied by percentage of shares estimated to be issued to NMM’s shareholders | 82.0 | % | ||
| Multiplied by the par value of common stock | $ | 0.001 | ||
| Pro forma adjustment to common stock per exchange ratio | $ | 27,486 | ||
| Plus: Additional shares issued to NMM’s shareholders | $ | 2,567 | ||
| Total pro forma adjustment to common stock | $ | 30,053 |
| (b) | To eliminate the historical book value of NMM’s investment in ApolloMed’s Series A preferred stock and Series B preferred stock ($10,550,002) and record a non-recurring gain of $7,646,998 on the change in the fair value of the investment with an off-setting ($18,197,000) to additional paid-in-capital representing the fair value of the Series A preferred stock and Series B preferred stock included in the purchase consideration. The gain on the change in fair value is not expected to have a continuing impact on the combined results and is not reflected in the pro forma results of operations. |
| (c) | To record the conversion of the ApolloMed convertible note payable ($5,142,000) and accrued interest held by Alliance into 499,820 shares of ApolloMed common stock with a conversion price of $10.00 per share and a non-recurring gain of $143,800 on the conversion. The gain on conversion is not expected to have a continuing impact on the combined results and is not reflected in the pro forma results of operations. |
| (d) | To eliminate interest expense/income associated with the notes payable and receivable between ApolloMed and NMM that will be eliminated upon the Merger. The note was issued by NMM to ApolloMed in January 2017 to be used as a working capital loan in the principal amount of $5,000,000. |
| (e) | This adjustment reflects the income tax effect of the pro forma adjustments described in notes 4(a), 4(h), 5(d) and 5(h), using an estimated income tax rate of 40.746% for the respective period. |
| 184 |
| (f) | To record the issuance of a convertible promissory note of $9,000,000 from NMM to ApolloMed to replace the $5,000,000 working capital loan and extend an additional $4,000,000. The convertible promissory note was recorded at fair value of $9,043,146 and Apollo recognized a loss on debt extinguishment of $43,146 which eliminates with the gain on extinguishment of $43,146 in NMM. The $9,043,146 convertible loan is eliminated upon consolidation. |
| (g) | To eliminate the accrued interest payable and accrued interest receivable associated with notes 5(d) above. |
| (h) | To eliminate revenues and expenses recorded for transactions between ApolloMed and NMM during the relevant period. |
| (i) | To record the estimated pro-rata cash distributions to the NMM shareholders prior to the Merger related to the $10,000,000 NMM minimum cash balance to be maintained on the assumed closing date pursuant to Section 3.15 of the Merger Agreement. NMM is entitled to distribute any excess cash to its shareholders prior to the Merger. This distribution was recorded as an adjustment to additional paid-in capital instead of retained earnings as NMM is in a deficit position. |
| (j) | To record the conversion of the NMM redeemable common stock and additional paid-in capital into ApolloMed common stock and additional paid-in capital as part of the Merger, based on the assumption that all NMM shareholders will participate in the exchange, as follows: |
| Eliminate historical NMM redeemable common stock | $ | (86,894,870 | ) | |
| Eliminate historical NMM additional paid-in capital | $ | (1,322,246 | ) | |
| Common stock pro forma adjustment described in note 5(a) above | $ | 30,053 | ||
| Pro forma adjustment to additional paid-in capital | $ | 88,187,063 |
| (k) | To eliminate the historical book value of NMM’s derivative asset – warrants ($5,466,665) related to NMM’s holding of Series A and Series B warrants in ApolloMed common stock and to record a one-time gain of $33,335 in retained earnings for the difference between the estimated fair value of these warrants at the Merger date and the balance sheet carrying amount of the derivative asset – warrants with an offsetting adjustment of $5,500,000 to retained earnings to reflect the pro-rata distribution of the warrants to the shareholders of NMM immediately prior to the Merger. The loss based upon the change in fair value of the derivative asset is not expected to have a continuing impact on the results of the combined company and is not reflected in the pro forma results of operations. |
| (l) | To record a non-recurring gain of $3,505,000 related to the fair value of NMM’s 50% equity investment in APAACO and the elimination of the NMM investment in consolidation against additional paid-in capital. The gain related to the change in fair value is not expected to have a continuing impact on the results of the combined company and is not reflected on the pro forma results of operations. The entry to additional paid-in capital represents the elimination of the investment in APAACO on a consolidated basis based upon the Merger. |
| (m) | To eliminate amounts receivable / payable between ApolloMed and NMM. |
| (n) | To reclassify the net income of MMG into non-controlling interest for the respective period. |
| (o) | The pro forma combined basic and diluted earnings per share have been adjusted to reflect the pro forma net income for the three months ended June 30, 2017. In addition, the number of shares used in calculating the pro forma combined basic and diluted net income per share has been adjusted to reflect the estimated total number of common stock of the combined company that would be outstanding as of the closing of the Merger. The estimated total numbers of shares of common stock of the combined company that would be outstanding as of the closing of the Merger is calculated to be 36,585,293 and 40,616,420 on a basic and fully diluted basis, respectively. The following table sets forth the calculation of the pro forma weighted average number of common shares outstanding – basic and diluted: |
| 185 |
| NMM weighted average number of shares outstanding as if the Merger occurred on April 1, 2017 | 398,352,118 | |||
| Divided by the exchange ratio | 14.49 | |||
| Post conversion basis shares | 27,486,026 | |||
| ApolloMed's weighted average number of shares as of June 30, 2017 | 6,033,518 | |||
| Plus: Additional NMM issuance | 2,566,666 | |||
| Plus: Apollo Alliance issuance | 499,083 | |||
| Pro forma weighted average number of shares | 36,585,293 | |||
| Weighted average shares - basic | 36,585,293 | |||
| Preferred stock | 1,666,666 | |||
| Stock options | 1,099,850 | |||
| Warrants | 1,264,611 | |||
| Weighted average shares - diluted | 40,616,420 |
| The pro forma combined basic and diluted earnings per share have been adjusted to reflect the pro forma net income for the year ended March 31, 2017. In addition, the number of shares used in calculating the pro forma combined basic and diluted net income per share has been adjusted to reflect the estimated total number of common stock of the combined company that would be outstanding as of the closing of the Merger. The estimated total numbers of shares of common stock of the combined company that would be outstanding as of the closing of the Merger is calculated to be 33,943,719 and 36,651,835 on a basic and fully diluted basis, respectively. The following table sets forth the calculation of the pro forma weighted average number of common shares outstanding – basic and diluted: |
| NMM weighted average number of shares outstanding as if the Merger occurred on April 1, 2016 | 360,529,486 | |||
| Divided by the exchange ratio | 14.49 | |||
| Post conversion basis shares | 24,876,290 | |||
| ApolloMed's weighted average number of shares as of March 31, 2017 | 6,001,680 | |||
| Plus: Additional NMM issuance | 2,566,666 | |||
| Plus: Apollo Alliance issuance | 499,083 | |||
| Pro forma weighted average number of shares | 33,943,719 | |||
| Weighted average shares - basic | 33,943,719 | |||
| Preferred stock | 1,666,666 | |||
| Stock options | 902,950 | |||
| Warrants | 138,500 | |||
| Weighted average shares - diluted | 36,651,835 |
6. Merger Related Costs
The pro forma adjustment related to merger costs of $3,000,000 reflected in the accounts payable and accrued liabilities consist of the estimated accrual to be incurred by NMM and ApolloMed in connection with the Merger which were not reflected in each of the historical consolidated balance sheets. $500,000 of the estimated merger costs is attributable to NMM which is reflected as an adjustment to retained earnings. $2,500,000 of the estimated merger costs is attributable to ApolloMed and is expected to be paid after the closing of the Merger. The estimated merger costs of ApolloMed have been reflected as an assumed liability as part of the purchase accounting adjustments.
These merger-related costs are not expected to have a continuing impact on the results of the combined company. There was no material Merger related costs included in the historical results of operations of ApolloMed or NMM requiring pro forma adjustment.
| 186 |
MANAGEMENT OF THE COMBINED COMPANY
At the closing of the Merger, the ApolloMed Charter and ApolloMed Bylaws will be amended to divide the board of directors into three classes, Class I, Class II and Class III, with three directors in each class.
Pursuant to the terms of the Merger Agreement, ApolloMed has agreed to use reasonable efforts to cause the board of directors of ApolloMed to consist, on or following the Effective Time of the Merger, of: Thomas Lam M.D., David G. Schmidt and Michael F. Eng as Class I directors, Mitchell W. Kitayama, Kenneth Sim, M.D. and Mark Fawcett as Class II directors and Warren Hosseinion M.D., Gary Augusta and Li Yu as Class III directors.
In addition, ApolloMed and NMM agreed that the officers of ApolloMed, on or following the Effective Time of the Merger, will be the following persons: Kenneth Sim M.D. to serve as Executive Chairman, Thomas Lam M.D. and Warren Hosseinion M.D. to serve as Co-Chief Executive Officers, Gary Augusta to serve as President, Hing Ang to serve as Chief Operating Officer, Mihir Shah to serve as Chief Financial Officer and Adrian Vazquez M.D. and Albert Young M.D. to serve as Co-Chief Medical Officers.
It is contemplated that Suresh Nihalani and Ted Schreck, current directors of ApolloMed, will resign immediately upon the closing of the Merger as constituted above.
The following table lists the names, ages (as of [●], 2017) and positions of the individuals who are expected to serve as executive officers and directors of ApolloMed upon completion of the Merger:
|
Name |
Age |
Position(s) |
||
| Executive Officers | ||||
| Kenneth Sim, M.D. | 64 | Executive Chairman and Class II Director | ||
| Warren Hosseinion, M.D. | 45 | Co-Chief Executive Officer and Class III Director | ||
| Thomas S. Lam, M.D. | 68 | Co-Chief Executive Officer and Class I Director | ||
| Gary Augusta | 50 | President and Class III Director | ||
| Hing Ang | 59 | Chief Operating Officer | ||
| Mihir Shah | 39 | Chief Financial Officer | ||
| Adrian Vazquez, M.D. | 47 | Co-Chief Medical Officer | ||
| Albert Young, M.D. | 70 | Co-Chief Medical Officer | ||
| Non-Employee Directors | ||||
| Michael F. Eng | 70 | Class I Director | ||
| David G. Schmidt | 70 | Class II Director | ||
| Mitchell W. Kitayama | 60 | Class II Director | ||
| Mark Fawcett | 50 | Class II Director | ||
| Li Yu | 75 | Class III Director |
Kenneth Sim, M.D. Dr. Sim has been the Chairman of NMM since 2013 and has been a member of NMM’s board of directors since 2006. Dr. Sim is also the Chairman of the board of APC. Dr. Sim is a Fellow of the American College of Surgeons and was awarded the Independent Physician Leadership Award in 2014 by the Los Angeles County Medical Association. Dr. Sim is also a member of the Governing Board of Directors at Alhambra Hospital Medical Center and a Board Member on the National Council of Asian Pacific Islander Physicians. As an entrepreneur, Dr. Sim founded “Healthcare City” in the City of Industry, California, which helped streamline the healthcare process by providing outpatient health services at one location including surgical center, senior wellness center, laboratory, radiology and urgent care. He received his bachelor's degree from the University of California Los Angeles and received his medical training from the Loma Linda University School of Medicine and the Autonomous University of Guadalajara, Guadalajara, Mexico.
| 187 |
Warren Hosseinion, M.D. Dr. Hosseinion has been ApolloMed’s Chief Executive Officer and a member of ApolloMed’s board of directors since July 2008. In 2001, Dr. Hosseinion co-founded ApolloMed Hospitalists, a California medical corporation (“ApolloMed Hospitalists” or “AMH”), in Los Angeles with Dr. Adrian Vazquez. Dr. Hosseinion received his B.S. in biology from the University of San Francisco, his M.S. in physiology and biophysics from Georgetown University Graduate School, his medical degree from the Georgetown University School of Medicine and his residency in internal medicine from the Los Angeles County-University of Southern California Medical Center.
Thomas S. Lam, M.D. Dr. Lam has been a member of ApolloMed’s board of directors since January 2016. Dr. Lam has served as Chief Executive Officer of NMM since January 2006. Dr. Lam has served as Chief Executive Officer of NMM since January 2006 and has been a member of NMM’s board of directors since 2005. From January 2006 to September 2014, Dr. Lam was the Chairman and CEO of APC. Since October 2014, he has served as the Chief Executive Officer and Chief Financial Officer of APC. Dr. Lam was the recipient of the Corporate Citizens of the Year Award from the Board of Directors of East Los Angeles College Foundation in April 2014. In February 2015, YMCA Board of Directors of West San Gabriel Valley honored Dr. Lam as the recipient of Heart of the Community Award. Dr. Lam received his medical training from New York Medical College and gastroenterology training from Georgetown University. Dr. Lam serves as the nominee of NMM.
Gary Augusta. Mr. Augusta has been a member of ApolloMed’s board of directors since March 2012 and has been Executive Chairman since October 2013. In addition to board responsibilities, Mr. Augusta focuses on strategic planning, corporate development, capital raising and population health technology for the company. Mr. Augusta also serves as President of Flacane Advisors focusing on healthcare and technology advisory and investments. From January 2010 to December 2014, Mr. Augusta was President of SpaGus Ventures and SpaGus Capital Partners focusing on healthcare and technology investments and advisory services. From March 2004 to December 2009, Mr. Augusta was President and CEO of OCTANe, an innovation development company. From March 2001 to January 2004, Mr. Augusta was a Corporate Officer at Fluor, Inc., a Fortune 500 company, focusing on Corporate Development and M&A. From June 1994 to March 2000, Mr. Augusta was a Consultant and Principal with AT Kearney, a leading global consulting firm. He earned a BS in Mechanical Engineering from the University of Rhode Island and a Master of Science and Management (MSM) from Georgia Institute of Technology (Georgia Tech).
Hing Ang, CPA. Mr. Ang has been the Executive Vice President since 2014 and Chief Financial Officer of NMM since 2016. Mr. Ang spent his last 10 years with NMM where he gained extensive health care operation experience through the senior director of operations since 2007 to his current positions. Prior to joining NMM, Mr. Ang held a variety of senior management positions for a variety of companies internationally. Mr. Ang is a Fellow of the Association of Chartered Certified Accountants in England and he is also licensed as a Certified Public Accountant in California.
Mihir Shah. Mr. Shah, CPA, became ApolloMed’s Chief Financial Officer on July 21, 2016, having served as ApolloMed’s accounting consultant from March 2016 through July 20, 2016. From April 2015 to February 2016, Mr. Shah served as Chief Financial Officer of Unitek Information Systems, Inc., a private equity-backed company that offers nursing, allied health and information technology training programs. From April 2013 to March 2015, he was Vice President and Controller of Health Essentials, LLC, a private equity-backed healthcare organization that provides post-acute care and hospice/palliative care services to the frail and elderly population in California. Mr. Shah was employed at Arcadian Health Plan from December 2005 through March 2013, serving as its Vice President Finance and Analytics from January 2010 through March 2013, Senior Director of Finance and Analytics from January 2008 through December 2009, and Senior Financial Analyst from December 2005 through December 2007. He is a Certified Public Accountant and received a Master of Commerce-Cost Accounting from Gujarat University in Ahmedabad, India.
Adrian Vazquez, M.D. Dr. Vazquez, has served as ApolloMed’s Chief Medical Officer since March 2014, having previously served as ApolloMed’s President and Chairman of the ApolloMed board of directors from 2008 to 2011. Dr. Vazquez co-founded ApolloMed Hospitalists in 2001. He received his B.S. in biology from the University of California, Irvine, his medical degree from the UC Irvine School of Medicine and his residency in internal medicine from the Los Angeles County-University of Southern California Medical Center.
| 188 |
Albert Young, M.D. Dr. Young has been the Chief Medical Officer of NMM since 2006 and has been a member of NMM’s board of directors since 2010. Dr. Young is also the Chief Medical Officer of APC. Dr. Young received his medical degree from West Virginia University School of Medicine and completed his internal medicine residency training at Los Angeles County and USC Medical Center. Upon completing his residency training, Dr. Young completed a Fellowship in pulmonary medicine. An advocate of general preventive medicine, Dr. Young also obtained a Master’s in Public Health from UCLA in 1998.
Michael F. Eng. Michael Eng has served as a City Councilman from 2003 to 2006, a State Assemblyman from 2006 to 2012 and a College Trustee since 2013. While in the Legislature, he served on the Assembly Health Committee. Prior to his elected offices, he was appointed to the Board of Acupuncture by the Governor of California. He has practiced federal immigration and nationality law and currently is a college instructor at California State University Los Angeles. His education consists of a Law Degree from UCLA and a Bachelor’s and Master’s Degree from University of Hawaii. He was previously employed by Kaiser Permanente.
David Schmidt. Mr. Schmidt has been a member of ApolloMed’s board of directors since May 2013. He has served since January 2011 as Principal of Schmidt & Associates, a consultancy practice that focuses on strategic planning and implementation in the healthcare industry. Since April 2015 Mr. Schmidt has also served as the CEO of the TPG-International Health Academy, a company that organizes trade missions to expose Senior Health Plan and Health System executives from the United States to other country's health systems. From August 2002 to December 2010, he served as the CEO and Member of the Board of SCAN Health Plan, a provider of Medicare Advantage plans. From 2000 to 2002 he served as CEO of Medicheck, a firm that provided Internet-based financial service management to healthcare organizations, which was sold to Passport Health Communications. He served on Passport’s Board from 2002 to 2006. From 1992 to 1998 he was the Senior Vice President of Sales and Customer Services for Care America/Blue Shield Health Plan and Regional Vice President for FHP Healthcare. He received a BA in Economics from UCLA and a MBA from The Anderson School of Management at UCLA. Prior to his healthcare experience he held senior management roles in manufacturing companies including Avery Dennison. He also serves on the board of Beacon Healthcare Systems and was a founding board member of the SCAN Foundation, a 501(c)(3) corporation focused on long term care in the United States.
Mitchell W. Kitayama. Mr. Kitayama is the Chairman of Winslow Drake, a boutique investment advisory and wealth management practice which he joined in 2016. Mr. Kitayama is also the Managing Director for MMK & Associates, Inc. advising financial institutions, medical groups and private companies in strategic planning, risk management, mergers and acquisitions, cash management, organizational infrastructure and funding and capital strategies. Mr. Kitayama served on the board and is the treasurer for the Los Angeles Ronald McDonald House and serves on the Finance and Investment Committees for the Ronald McDonald House Charities of Southern California. Mr. Kitayama served two terms as chairman for the American Diabetes Association Los Angeles, member of the National Finance Committee in Washington DC, and was National Ambassador for the ADA Research Foundation. Mr. Kitayama also served as Vice President and Treasurer for First American Bank in Bryan, Texas, CorEast Saving Bank in Richmond, Virginia (the fifth largest bank in Virginia), and Goldome Realty Credit Corp. in Buffalo, New York (the fifth largest mortgage bank in the country). Mr. Kitayama served as a cabinet member for United Way of Greater Los Angeles Tocqueville Society and member of the UW Campaign President’s Cabinet. Mr. Kitayama is a certified cash manager/treasury professional and has an MBA and BA Biology with Chemistry minor from Baylor University.
Mark Fawcett. Mr. Fawcett has been a member of ApolloMed’s board of directors since January 2016. Since 2002, Mr. Fawcett has served as Senior Vice President and Treasurer of Fresenius Medical Care Holdings, Inc. (“FMCH”) and its subsidiaries. FMCH is a wholly-owned subsidiary of Fresenius (NYSE: FMS) (collectively with FMCH and their respective subsidiaries, “FMS”). FMS is the world’s leading provider of chronic kidney failure products and services. Prior to his joining FMS, Mr. Fawcett was Director in Corporate Finance at BankBoston beginning in 1997. Mr. Fawcett had various positions of increasing responsibility beginning in 1988 with Merrill Lynch in New York and London then at The Bank of New York. Mr. Fawcett graduated with a B.A. in psychology from Wesleyan University and a M.B.A. from Columbia University Business School. Mr. Fawcett serves on the ApolloMed board as the nominee of NNA, an affiliate of FMCH.
| 189 |
Li Yu. Mr. Yu has been the Chief Executive Officer of Preferred Bank since 1993 and was also the President of Preferred Bank from 1993 to 2012. From December 1991 to the present, Mr. Yu has served as Chairman of the Board of Directors and served on the Loan Committee and Investment Committee of Preferred Bank. Under his leadership, Preferred Bank grew from a de novo bank with $20 million in initial capital in 1991 to one of the largest independent commercial banks in California with $2.1 billion in total assets. Mr. Yu was also the President of the National Association of Chinese American Bankers, and is currently a member of the Board of Visitors of UCLA’s Anderson Graduate School of Management. Mr. Yu received his MBA from the University of California, Los Angeles.
There are no family relationships among any of the current ApolloMed executive officers and directors, and there are no family relationships among any of the proposed combined company executive officers and directors.
The ApolloMed board has made independence determinations in accordance with the NASDAQ listing standards, which state that a director will not be independent if:
(i) the director, or an immediate family member of the director, is, or within the last three years was, employed by the company or any of its subsidiaries;
(ii) the director, or an immediate family member of the director, has received, during any twelve-month period within the last three years, more than $120,000 in direct compensation from the company, other than director and committee fees, and pension or other forms of deferred compensation for prior service (provided such compensation is not contingent on continued service);
(iii) the director, or an immediate family member of the director, is a current partner of a firm that is the company’s (or any of its subsidiaries) internal or external auditor; or is a current employee of such a firm; or who was, within the last three years (but is no longer), a partner or employee of such firm and personally worked on the company’s audit within that time;
(iv) the director, or an immediate family member of the director, is, or has been within the last three years, employed as an executive officer of another company where any of the company’s present executive officers at the same time serve or served on that company’s compensation committee; or
(v) the director is a current employee, or an immediate family member of such director is a current executive officer, of a company that has made payments to, or received payments from, the company for property or services in an amount, which, in any of the last three fiscal years, exceeds the greater of $1 million or two percent (2%) of such other company’s consolidated gross revenues.
With respect to any relationship not covered above, the determination of whether the relationship is material, and therefore whether a director would be independent, will be made by those directors who satisfy the independence criteria set forth above.
In addition to the forgoing, the ApolloMed board also makes such independence determinations with respect to its audit committee and compensation committee members after taking into account the additional independence and financial literacy standards for members of each such committee, as applicable, in accordance with and pursuant to the rules and regulations of the SEC and NASDAQ listing rules as currently in effect.
| 190 |
ApolloMed has determined that [●], [●], and [●] have no material relationship with ApolloMed that would interfere with the exercise of independent judgment and are “independent directors” as that term is defined in the NASDAQ Listing Rules.
The ApolloMed board has a standing Audit Committee, Compensation Committee and Nominating/Corporate Governance Committee. The composition, functions and general responsibilities of each committee are summarized below.
Audit Committee
The Audit Committee currently consists of David Schmidt (Chairman), Suresh Nihalani and Ted Schreck. On or following the Effective Time of the Merger, it is expected that the Audit Committee will be reconstituted to consist of [●], [●] and [●]. The ApolloMed board has determined that Mr. Schmidt is an audit committee financial expert, as that term is defined in Item 401(h) of Regulation S-K of the Exchange Act, and is independent within the meaning of Item 7(d)(3)(iv) of Schedule 14A of the Exchange Act. The ApolloMed board also believes that all members of the Audit Committee meet the independence and knowledge requirements of NASDAQ as currently in effect.
Consistent with ApolloMed’s Audit Committee Charter, no member of the Audit Committee may serve on the audit committees of more than two other public companies (in addition to ApolloMed’s). Currently, no member of the Audit Committee serves on more than two other public company audit committees.
The Audit Committee operates under a written charter, a copy of which is available on ApolloMed’s website. The Audit Committee’s duties include (a) monitoring and ensuring (i) the integrity of ApolloMed’s financial statements, (ii) compliance with legal and regulatory requirements, (iii) the qualifications and independence of ApolloMed’s independent auditors, and (iv) the performance of ApolloMed’s internal audit function and external auditors; (b) preparing the report required to be prepared by the Audit Committee under the rules of the SEC for inclusion in ApolloMed’s proxy statement; and (c) overseeing ApolloMed’s accounting and financial reporting processes the audits of ApolloMed’s financial statements. In addition, the Audit Committee has responsibility for reviewing complaints about, and investigating allegations of, financial impropriety or misconduct.
As part of its responsibility, the Audit Committee is responsible for engaging ApolloMed’s independent registered public accounting firm, as well as pre-approving audit and non-audit services performed by ApolloMed’s independent registered public accounting firm in order to assure that the provision of such services does not impair their independence. The Audit Committee has adopted, and the ApolloMed board has ratified, an Audit Committee Pre-Approval Policy, which is also available on ApolloMed’s website.
It is expected that the Audit Committee of the combined company will retain these duties and responsibilities following completion of the Merger.
Compensation Committee
The Compensation Committee consists of Messrs. Nihalani (Chairman), Schmidt and Schreck. On or following the Effective Time of the Merger, it is expected that the Compensation Committee will be reconstituted to consist of [●], [●] and [●]. The ApolloMed board has determined that all members of the Compensation Committee qualify as “independent” directors as defined under NASDAQ rules, as a “non-employee director” as defined in Rule 16b-3(b)(3) under the Exchange Act and as an “outside director” within the meaning of Section 162(m)(4)(C)(i) of the Code. No member of the Compensation Committee was at any time during fiscal year 2017 an officer or employee of ApolloMed. The Compensation Committee held two meetings and acted by written consent five times during fiscal year 2017. None of ApolloMed’s executive officers served on the compensation committee of another entity or on any other committee of the board of directors of another entity performing similar functions during fiscal year 2017.
| 191 |
The Compensation Committee operates under a written charter, a copy of which is available on ApolloMed’s website. The Compensation Committee establishes the compensation and benefits of ApolloMed’s executive officers. The compensation committee also administers employee benefit plans, including equity incentive plans.
It is expected that the Compensation Committee of the combined company will retain these duties and responsibilities following completion of the Merger.
Nominating/Corporate Governance Committee
The Nominating/Corporate Governance Committee consists of Messrs. Schreck (Chairman), Nihalani and Schmidt. On or following the Effective Time of the Merger, it is expected that the Compensation Committee will be reconstituted to consist of [●], [●] and [●]. All members of the Nominating and Corporate Governance Committee meet the independence requirements of NASDAQ as currently in effect. The Nominating/Corporate Governance Committee met one time during fiscal year 2017.
The Nominating and Corporate Governance Committee operates under a written charter, a copy of which is available on the ApolloMed website. The Nominating and Corporate Governance Committee has the primary responsibility for overseeing ApolloMed’s corporate governance compliance practices, as well as supervising the affairs of ApolloMed as they relate to the nomination of directors. The principal ongoing functions of the Nominating and Corporate Governance Committee include developing criteria for selecting new directors, establishing and monitoring procedures for the receipt and consideration of director nominations by stockholders and others, considering and examining director candidates, recommending director nominations to the board, developing and recommending corporate governance principles for ApolloMed and monitoring ApolloMed’s compliance with those principles and establishing and monitoring procedures for the receipt of stockholder communications directed to the board.
The Nominating and Corporate Governance Committee is also responsible for conducting an annual evaluation of the ApolloMed board to determine whether the board and its committees are functioning effectively.
It is expected that the Nominating and Corporate Governance Committee of the combined company will retain these duties and responsibilities following completion of the Merger.
The board of directors of ApolloMed may from time to time establish other committees.
ApolloMed is currently led by Warren Hosseinion M.D. who has served as ApolloMed’s Chief Executive Officer since July 2008, and Gary Augusta, who has served as ApolloMed’s Executive Chairman since October 2013. ApolloMed has not formally named an independent lead director. Following the Effective Time of the Merger, ApolloMed will be led by Drs. Hosseinion and Lam (as Co-Chief Executive Officers) and Kenneth Sim M.D. will become Executive Chairman replacing Mr. Augusta.
ApolloMed’s board leadership structure is commonly utilized by many other public companies in the United States, and it believes that this leadership structure has been effective for ApolloMed. ApolloMed believes that having a Chief Executive Officer who can focus on the broad executive and operational issues facing the company, and a separate Executive Chairman who can focus on board and oversight functions, independent chairs for each of the board committees and only independent directors serving on these committees allocates responsibility and creates checks and balances for ApolloMed. This structure provides ApolloMed with leadership to ensure continuity of its operational, executive and board functions by individuals playing to their strongest qualities, combined with oversight of the company by experienced independent directors.
| 192 |
Risk Management Oversight Function of the Board
The ApolloMed board has allocated responsibilities for overseeing risk associated with the company’s business among the board as a whole and the committees of the ApolloMed board. The ApolloMed board and the committees of the board have undertaken some risk oversight review in accordance with this policy. In performing its risk oversight function, the ApolloMed board is responsible for overseeing management’s development and execution of appropriate business strategies to mitigate the risk that such strategies will fail to generate long-term value for the company and its stockholders or that such strategies will motivate management to take excessive risks. The ApolloMed board periodically reviews information regarding the company’s financial, operational and strategic risks.
Each of the ApolloMed board’s committees is responsible for overseeing the management of company risks that fall within the committee’s areas of responsibility, including identifying, quantifying and assisting management in mitigating risks. In performing this function, each committee has full access to management, as well as the ability to engage advisors. As set forth in its charter, the Audit Committee is responsible for discussing with management the company’s major financial risk exposures and the steps management has taken to monitor and control those exposures. The Audit Committee provides updates to the ApolloMed board at its regular meetings. The Audit Committee also meets privately with the company’s independent registered public accounting firm and ApolloMed’s Chief Financial Officer at least quarterly. The Compensation Committee is responsible for overseeing the company’s risk management related to employee compensation plans and arrangements.
ApolloMed Director Compensation
For fiscal year 2017, ApolloMed’s independent directors were paid director fees in the amount of $1,000 per month and issued a stock option under ApolloMed’s 2015 Plan to purchase 20,000 shares of ApolloMed common stock at a price of $5.00 per share, such amount vesting pro rata monthly over 12 months from the date of grant. Directors who are employees of ApolloMed receive no additional compensation for serving as directors.
The following table presents the total compensation for each person who served as a non-executive member of ApolloMed’s board of directors during the year ended March 31, 2017 and who is expected to continue to serve on the board of directors of the combined company:
|
Name |
Fees Earned or Paid in Cash ($) |
Stock Awards ($) |
Option Awards ($) (1) |
Non-Equity Incentive Plan Compensation ($) |
Change in Pension Value and Nonqualified Deferred Compensation Earnings ($) |
All
Other Compensation ($) |
Total ($) |
|||||||||||||||||||||
| Mark Fawcett(2) | $ | 12,000 | $ | $ | 89,000 | $ | — | $ | — | $ | 9,000 | $ | 110,000 | |||||||||||||||
| Thomas Lam, M.D.(3) | $ | — | $ | $ | — | $ | — | $ | — | $ | — | $ | — | |||||||||||||||
| David Schmidt | $ | 12,000 | $ | $ | 89,000 | $ | — | $ | — | $ | — | $ | 101,000 | |||||||||||||||
(1) For a discussion of the assumptions used in the valuation of awards (estimated forfeitures are not considered for purposes of these computations and the full fair value is recognized in the year of grant), see the notes to the consolidated financial statements included in this joint proxy statement/prospectus.
(2) Received an additional $9,000 relating to out-of-town traveling time.
(3) Dr. Lam is not considered an independent director and does not receive any compensation for his service as a director.
NMM directors receive a stipend for each board meeting attended. The stipend was $500 per meeting for 2016 and the aggregate stipend payments made to all NMM directors in 2016 was $56,000.
| 193 |
The following table presents the total compensation for each person who served as a board member of NMM’s board of directors during the year ended December 31, 2016, and who is expected to continue to serve on the board of directors of the combined company. Please see “MANAGEMENT OF THE COMBINED COMPANY – NMM Executive Officer Compensation” and related Summary Compensation Table for 2014-2016 beginning on page 192 for further compensation disclosure. There were no stock options granted to any NMM director that were outstanding as of December 31, 2016.
| Name | Fees Earned or Paid in Cash ($) |
Stock Awards ($) |
Option Awards ($) |
Non-Equity Incentive Plan Compensation ($) |
Change in Pension Value and Nonqualified Deferred Compensation Earnings ($) |
All
Other Compensation ($) |
Total ($) |
|||||||||||||||||||||
| Kenneth Sim, M.D. | $ | 2,500 | $ | - | $ | - | $ | - | $ | - | $ | $ | 2,500 | |||||||||||||||
| Thomas Lam, M.D. | $ | 2,500 | $ | - | $ | - | $ | - | $ | - | $ | $ | 2,500 | |||||||||||||||
| Albert Young, M.D. | $ | 2,500 | $ | - | $ | - | $ | - | $ | - | $ | $ | 2,500 | |||||||||||||||
ApolloMed Executive Officer Compensation
2017 Summary Compensation Table
The following table provides summary compensation as of March 31, 2017 and 2016 regarding ApolloMed’s executive officers who are expected to continue as executive officers of the combined company subsequent to the Merger:
Name
and Principal |
Year |
Salary |
Bonus |
Stock |
Option Awards(1) |
Non-equity |
Nonqualified |
All
Other |
Total | |||||||||||||||||||||||||||
| Warren Hosseinion | 2017 | $ | 520,581 | (2) | $ | — | $ | — | $ | — | $ | — | $ | — | $ 84,889 | (4) | $ | 605,470 | ||||||||||||||||||
| Chief Executive Offıcer | 2016 | 394,998 | (2) | 30,000 | (3) | — | 485,000 | (14) | — | — | 117,193 | (4) | 1,027,191 | |||||||||||||||||||||||
| Gary Augusta | 2017 | 306,550 | (5) | — | — | — | — | — | 6,975 | (7) | 313,525 | |||||||||||||||||||||||||
| Executive Chairman | 2016 | 300,000 | (5) | 30,000 | (6) | — | 487,000 | (15) | — | — | — | 817,000 | ||||||||||||||||||||||||
| Adrian Vazquez | 2017 | 498,882 | (8) | — | — | — | — | — | 85,017 | (10) | 583,899 | |||||||||||||||||||||||||
| Chief Medical Offıcer | 2016 | 394,292 | (8) | 15,000 | (9) | — | 121,000 | (16) | — | — | 117,847 | (10) | 648,139 | |||||||||||||||||||||||
| Mihir Shah | 2017 | 328,083 | (11) | 30,000 | (12) | — | 202,200 | (17) | — | — | 12,711 | (13) | 572,994 | |||||||||||||||||||||||
| Chief Financial Offıcer | 2016 | 1,008 | (11) | — | — | — | — | — | — | 1,008 | ||||||||||||||||||||||||||
| (1) | The amount shown in this column reflects the aggregate grant date fair value computed in accordance with Financial Accounting Standards Board Accounting Standards Codification 718 ‘‘Compensation — Stock Compensation’’. Please see the notes below for discussions of the assumptions and methodologies used to calculate the valuations of the stock and option awards. |
| (2) | Dr. Hosseinion’s salary is for both patient care/medical director and non-clinical work in his role as ApolloMed’s Chief Executive Officer. |
| (3) | Dr. Hosseinion earned and received an incentive bonus of $30,000 in 2016. |
| (4) | Reflects personal benefits payments to Dr. Hosseinion for health, life, disability insurance premiums aggregating $31,344 in 2017 and $31,423 in 2016; payment of $44,230 for unused paid time off (PTO) and $9,315 of accrued, but not yet paid unused PTO in 2017; payment of $30,770 for unused PTO in 2016; and allowance for vehicle, cell phone and computer expenses of $55,000 in 2016. |
| 194 |
| (5) | Mr. Augusta received compensation for providing business and strategic services to ApolloMed and for his role as ApolloMed’s Executive Chairman. |
| (6) | Mr. Augusta received a bonus of $30,000 in 2016 for providing business and strategic services, and for his role as Executive Chairman on the ApolloMed board. |
| (7) | Reflects the value of accrued paid-time off that has not been used or paid out in 2017. |
| (8) | Dr. Vazquez’s salary is for both patient care/medical director and non-clinical work in his role as ApolloMed’s Chief Medical Officer. |
| (9) | Dr. Vazquez earned an incentive bonus of $15,000 in 2016 and received the bonus payment in 2017. |
| (10) | Reflects personal benefits payments to Dr. Vazquez for health, life and disability insurance premiums aggregating $31,471 in 2017 and $25,347 in 2016; payment of $44,230 for unused paid time off (PTO) and $9,316 of accrued, but not yet paid unused PTO in 2017; payment of $37,500 for PTO that was earned in 2016 but was paid in 2017; and allowance for vehicle, cell phone and computer expenses of $55,000 in 2016. |
| (11) | Mr. Shah was appointed as ApolloMed’s Chief Financial Officer and Principal Financial and Accounting Officer on July 21, 2016. Amount consists of (i) compensation of $202,367 for the period from July 21, 2016 through March 31, 2017 and (ii) compensation of $125,716 for services as ApolloMed’s accounting consultant for the period from April 1, 2016 through July 20, 2016 and $1,008 in fiscal 2016. |
| (12) | Mr. Shah earned and received an incentive bonus of $30,000 in 2017. |
| (13) | Reflects the value of accrued paid-time off that has not been used or paid out in 2017. |
| (14) | In February 2016, the ApolloMed board authorized the issuance of options for 93,500 shares of common stock with an exercise price of $6.369 per share to Dr. Hosseinion. Two-thirds of the options vested immediately and the remaining one-third vest monthly in equal amounts over a twelve-month period. The options expire on the fifth anniversary of issuance. The fair value of the 93,500 stock options was $485,000, and was determined using the Black-Scholes option pricing model. The calculation was based on ApolloMed’s closing stock price on the date of grant and the following weighted-average inputs: |
| Expected term (in years) | 6.0 | |||
| Volatility | 132.91 | % | ||
| Dividends | 0.0 | % | ||
| Discount rate | 1.31 | % |
| (15) | In February 2016, the ApolloMed board authorized the issuance of options for 93,500 shares of common stock with an exercise price of $5.79 per share to Mr. Augusta. Two-thirds of the options vested immediately and the remaining one-third vest monthly in equal amounts over a twelve-month period. The options expire on the tenth anniversary of issuance. The fair value of the 93,500 stock options was $487,000, and was determined using the Black-Scholes option pricing model. The calculation was based on ApolloMed’s closing stock price on the date of grant and the following weighted-average inputs: |
| Expected term (in years) | 6.0 | |||
| Volatility | 132.91 | % | ||
| Dividends | 0.0 | % | ||
| Discount rate | 1.31 | % |
| 195 |
| (16) | In February 2016, the ApolloMed board authorized the issuance of options for 23,400 shares of common stock with an exercise price of $6.369 per share to Dr. Vazquez. Two-thirds of the options vested immediately and the remaining one-third vest monthly in equal amounts over a twelve-month period. The options expire on the fifth anniversary of issuance. The fair value of the 23,400 stock options was $121,000, and was determined using the Black-Scholes option pricing model. The calculation was based on ApolloMed’s closing stock price on the date of grant and the following weighted-average inputs: |
| Expected term (in years) | 6.0 | |||
| Volatility | 132.91 | % | ||
| Dividends | 0.0 | % | ||
| Discount rate | 1.31 | % |
| (17) | In November 2016, the ApolloMed board authorized the issuance of options for 50,000 shares of common stock with an exercise price of $4.50 per share to Mr. Shah. The options vest monthly in equal amounts over a thirty-six months period and expire on the tenth anniversary of issuance. The fair value of the 50,000 stock options was $202,000, and was determined using the Black-Scholes option pricing model. The calculation was based on ApolloMed’s closing stock price on the date of grant and the following weighted-average inputs: |
| Expected term (in years) | 6.0 | |||
| Volatility | 132.17 | % | ||
| Dividends | 0.0 | % | ||
| Discount rate | 0.83 | % |
ApolloMed has entered into employment agreements with several of ApolloMed’s key personnel, including ApolloMed’s executive officers, which provide for, among other items, annual base salaries, discretionary bonuses and participation in ApolloMed’s equity incentive plans. These agreements also contain termination and severance clauses that require ApolloMed to make payments to certain of these employees if certain events occur as defined in their respective agreements.
On December 20, 2016, AMM entered into substantially similar employment agreements with each of Warren Hosseinion, M.D., ApolloMed’s Chief Executive Officer (the “Hosseinion Employment Agreement”), Gary Augusta, ApolloMed’s Chairman of the ApolloMed board of directors (the “Augusta Employment Agreement”), Mihir Shah, ApolloMed’s Chief Financial Officer (as amended on July 1, 2017, the “Shah Employment Agreement”) and Adrian Vazquez, M.D., ApolloMed’s Chief Medical Officer (individually, the “Vazquez Employment Agreement” and, together with the Hosseinion Employment Agreement, the Augusta Employment Agreement and the Shah Employment Agreement, the “Executive Employment Agreements”). The Executive Employment Agreements replaced employment agreements previously entered into with (i) Dr. Hosseinion and Dr. Vazquez on March 28, 2014, as amended on January 12, 2016 and as amended and restated on June 29, 2016, and (ii) Mr. Shah on July 21, 2016. Mr. Augusta’s consulting agreement through Flacane Advisers, Inc. has been terminated.
Hosseinion Employment Agreement
The Hosseinion Employment Agreement has a term of three years, with automatic renewals for successive one-year periods unless either party gives written notice not to renew at least 60 days prior to the expiration of the current term. Dr. Hosseinion’s annual base salary is $450,000, which is subject to review on an annual basis. Dr. Hosseinion is also eligible to receive an annual cash bonus for each fiscal year on such terms and conditions as the ApolloMed board of directors shall determine in its discretion, which authority the ApolloMed board has delegated to the Compensation Committee. Dr. Hosseinion is entitled to participate in any long-term incentive plan that may be available to similarly positioned executives. Dr. Hosseinion also accrues 20 business days of paid time off per calendar year, and any accrued but unused days are paid in cash at the end of the year.
| 196 |
Dr. Hosseinion is eligible to participate in any employee benefit plan which is or may, in the future, be made available by ApolloMed to ApolloMed’s employees; is entitled to prompt reimbursement of reasonable and usual business expenses; shall have paid by ApolloMed premiums for medical, dental and vision care coverage, as well as premiums for short-term and long-term disability insurance, and term life insurance providing for no less than $2,000,000 of coverage.
AMM may terminate the Hosseinion Employment Agreement in the event of death or disability, without cause upon thirty (30) days prior written notice, or for Cause (as defined in the Hosseinion Employment Agreement). Dr. Hosseinion may terminate the Hosseinion Employment Agreement at any time and for any reason, including, but not limited to, Good Reason (as defined in the Hosseinion Employment Agreement).
Upon termination of Dr. Hosseinion’s employment by AMM for Cause or by Dr. Hosseinion without Good Reason, he shall be entitled to any accrued but unpaid base salary, annual bonus, paid time off and expense reimbursement. Upon termination of Dr. Hosseinion’s employment without Cause or by Dr. Hosseinion for Good Reason, in addition to any accrued but unpaid base salary, paid time off and expense reimbursement, he shall be entitled to receive an amount equal to 24 months of his base salary in effect before the employment terminates. Dr. Hosseinion shall also be entitled to an amount in cash equal to the premiums that AMM pays for Dr. Hosseinion under its group medical, dental and vision programs for 12 months following the date of termination.
The Hosseinion Employment Agreement also contains restrictive covenants for AMM’s benefit and customary provisions regarding confidentiality of information and assignment of inventions.
Augusta Employment Agreement
The Augusta Employment Agreement has a term of three years, with automatic renewals for successive one-year periods unless either party gives written notice not to renew at least 60 days prior to the expiration of the current term. Mr. Augusta’s annual base salary is $300,000, which is subject to review on an annual basis. Mr. Augusta is also eligible to receive an annual cash bonus for each fiscal year on such terms and conditions as the ApolloMed board shall determine in its discretion, which authority the ApolloMed board has delegated to the Compensation Committee. Mr. Augusta is entitled to participate in any long-term incentive plan that may be available to similarly positioned executives. Mr. Augusta also accrues 20 business days of paid time off per calendar year, and any accrued but unused days are paid in cash at the end of the year.
Mr. Augusta is eligible to participate in any employee benefit plan which is or may, in the future, be made available by ApolloMed to ApolloMed’s employees; is entitled to prompt reimbursement of reasonable and usual business expenses; shall have paid by ApolloMed premiums for medical, dental and vision care coverage, as well as premiums for short-term and long-term disability insurance, and term life insurance providing for no less than $2,000,000 of coverage.
AMM may terminate the Augusta Employment Agreement in the event of death or disability, without cause upon thirty (30) days prior written notice, or for Cause (as defined in the Augusta Employment Agreement). Mr. Augusta may terminate the Augusta Employment Agreement at any time and for any reason, including, but not limited to, Good Reason (as defined in the Augusta Employment Agreement).
Upon termination of Mr. Augusta’s employment by AMM for Cause or by Mr. Augusta without Good Reason he shall be entitled to any accrued but unpaid base salary, annual bonus, paid time off and expense reimbursement. Upon termination of Mr. Augusta’s employment without Cause or by Mr. Augusta for Good Reason, in addition to any accrued but unpaid base salary, paid time off and expense reimbursement, he shall be entitled to receive an amount equal to 24 months of his base salary in effect before the employment terminates. Mr. Augusta shall also be entitled to an amount in cash equal to the premiums that AMM pays for Mr. Augusta under its group medical, dental and vision programs for 12 months following the date of termination.
The Augusta Employment Agreement also contains restrictive covenants for AMM’s benefit and customary provisions regarding confidentiality of information and assignment of inventions.
| 197 |
Vazquez Employment Agreement
The Vazquez Employment Agreement has a term of three years, with automatic renewals for successive one-year periods unless either party gives written notice not to renew at least 60 days prior to the expiration of the current term. Dr. Vazquez’s annual base salary is $450,000, which is subject to review on an annual basis. Dr. Vazquez is also eligible to receive an annual cash bonus for each fiscal year on such terms and conditions as the ApolloMed board shall determine in its discretion, which authority the ApolloMed board has delegated to the Compensation Committee. Dr. Vazquez is entitled to participate in any long-term incentive plan that may be available to similarly positioned executives. Dr. Vazquez also accrues 20 business days of paid time off per calendar year, and any accrued but unused days are paid in cash at the end of the year.
Dr. Vazquez is eligible to participate in any employee benefit plan which is or may, in the future, be made available by ApolloMed to ApolloMed’s employees; is entitled to prompt reimbursement of reasonable and usual business expenses; shall have paid by ApolloMed premiums for medical, dental and vision care coverage, as well as premiums for short-term and long-term disability insurance, and term life insurance providing for no less than $2,000,000 of coverage.
AMM may terminate the Vazquez Employment Agreement in the event of death or disability, without cause upon thirty (30) days prior written notice, or for Cause (as defined in the Vazquez Employment Agreement). Dr. Vazquez may terminate the Vazquez Employment Agreement at any time and for any reason, including, but not limited to, Good Reason (as defined in the Vazquez Employment Agreement).
Upon termination of Dr. Vazquez’s employment by AMM for Cause or by Dr. Vazquez without Good Reason he shall be entitled to any accrued but unpaid base salary, annual bonus, paid time off and expense reimbursement. Upon termination of Dr. Vazquez’s employment without Cause or by Dr. Vazquez for Good Reason, in addition to any accrued but unpaid base salary, paid time off and expense reimbursement, he shall be entitled to receive an amount equal to 24 months of his base salary in effect before the employment terminates. Dr. Vazquez shall also be entitled to an amount in cash equal to the premiums that AMM pays for Dr. Vazquez under its group medical, dental and vision programs for 12 months following the date of termination.
The Vazquez Employment Agreement also contains restrictive covenants for AMM’s benefit and customary provisions regarding confidentiality of information and assignment of inventions.
Shah Employment Agreement
The Shah Employment Agreement has a term of three years, with automatic renewals for successive one-year periods unless either party gives written notice not to renew at least 60 days prior to the expiration of the current term. Mr. Shah’s annual base salary was $260,000, which is subject to review on an annual basis. The Compensation Committee reviewed Mr. Shah’s base salary in June 2017 and increased his annual base salary to $350,000 effective July 1, 2017. Mr. Shah is also eligible to receive an annual cash bonus for each fiscal year on such terms and conditions as the ApolloMed board shall determine in its discretion, which authority the ApolloMed board has delegated to the Compensation Committee. Mr. Shah is entitled to participate in any long-term incentive plan that may be available to similarly positioned executives. Mr. Shah also accrues 20 business days of paid time off per calendar year, and any accrued but unused days are paid in cash at the end of the year.
Mr. Shah is eligible to participate in any employee benefit plan which is or may, in the future, be made available by ApolloMed to ApolloMed’s employees; is entitled to prompt reimbursement of reasonable and usual business expenses; shall have paid by ApolloMed premiums for medical, dental and vision care coverage, as well as premiums for short-term and long-term disability insurance, and term life insurance providing for no less than $2,000,000 of coverage.
AMM may terminate the Shah Employment Agreement in the event of death or disability, without cause upon thirty (30) days prior written notice, or for Cause (as defined in the Shah Employment Agreement). Mr. Shah may terminate the Shah Employment Agreement at any time and for any reason, including, but not limited to, Good Reason (as defined in the Shah Employment Agreement).
| 198 |
Upon termination of Mr. Shah’s employment by AMM for Cause or by Mr. Shah without Good Reason he shall be entitled to any accrued but unpaid base salary, annual bonus, paid time off and expense reimbursement. Upon termination of Mr. Shah’s employment without Cause or by Mr. Shah for Good Reason, in addition to any accrued but unpaid base salary, paid time off and expense reimbursement, he shall be entitled to receive an amount equal to 24 months of his base salary in effect before the employment terminates. Mr. Shah shall also be entitled to an amount in cash equal to the premiums that AMM pays for Mr. Shah under its group medical, dental and vision programs for 12 months following the date of termination.
The Shah Employment Agreement also contains restrictive covenants for AMM’s benefit and customary provisions regarding confidentiality of information and assignment of inventions.
Other Agreements with Drs. Hosseinion and Vazquez
Effective June 29, 2016, AMH entered into substantially similar Amended and Restated Hospitalist Participation Service Agreements with each of Dr. Hosseinion (the “Hosseinion Hospitalist Participation Agreement”) and Dr. Vazquez (individually, the ”Vazquez Hospitalist Participation Agreement” and, together with the Hosseinion Hospitalist Participation Agreement, the “Hospitalist Participation Agreements”), replacing agreements between AMH and Drs. Hosseinion and Vazquez that had originally been entered into on March 28, 2014 and amended on January 12, 2016. Pursuant to the Hospitalist Participation Agreements, Drs. Hosseinion and Vazquez provide physician services for AMH. The purpose of the new Hospitalist Participation Agreements is to align payment and benefit provisions, and make other technical changes, to the employment agreements that were previously in effect with each of Drs. Hosseinion and Vazquez. Each of the Hospitalist Participation Agreements provides for (i) hourly compensation rates for covered inpatient intensive medicine services; (ii) ApolloMed’s obligation to secure and pay for medical malpractice insurance, with specified minimum coverage, on behalf of Drs. Hosseinion and Vazquez; and (iii) maintain or purchase a “tail” policy for at least five years following the termination of the respective Hospitalist Participation Agreements. The Hospitalist Participation Agreements contain other provisions typical for an agreement of this type, including non-disclosure, non-solicitation, termination and arbitration of disputes provisions. The Hosseinion Hospitalist Participation Agreement replaced, and thereby terminated, the prior hospitalist participation service agreement between AMH and Dr. Hosseinion, and the Vazquez Hospitalist Participation Agreement replaced, and thereby terminated, the prior hospitalist participation service agreement between AMH and Dr. Vazquez.
As a condition of ApolloMed’s causing ApolloMed’s affiliates to enter into the Hospitalist Participation Agreements, also on March 28, 2014 ApolloMed entered into substantially similar stock option agreements with each of Dr. Hosseinion (the “Hosseinion Stock Option Agreement”) and Dr. Vazquez (individually, the “Vazquez Stock Option Agreement” and, together with the Hosseinion Stock Option Agreement, the “Executive Stock Option Agreements”). Each Executive Stock Option Agreement provides that Dr. Hosseinion or Dr. Vazquez grant ApolloMed the option to purchase (at fair market value) all equity interests in ApolloMed held by Dr. Hosseinion or Dr. Vazquez, as the case may be, in the event that (i) their respective Hospitalist Participation Agreement or Executive Employment Agreement is terminated by ApolloMed for cause due to a willful or intentional breach by Dr. Hosseinion or Dr. Vazquez, as the case may be; (ii) Dr. Hosseinion or Dr. Vazquez commits fraud or any felony against ApolloMed or any of ApolloMed’s affiliates; (iii) Dr. Hosseinion or Dr. Vazquez directly or indirectly solicits any patients, customers, clients, employees, agents or independent contractors of ApolloMed’s or any of ApolloMed’s affiliates for competitive purposes; or (iv) Dr. Hosseinion or Dr. Vazquez directly or indirectly Competes (as such term is defined in the Executive Stock Option Agreements) with ApolloMed or any of ApolloMed’s affiliates.
Outstanding Equity Awards at Fiscal Year-End
During the year ended March 31, 2017, ApolloMed issued options to purchase an aggregate of 149,200 shares of ApolloMed’s common stock to certain employees, directors and consultants. The stock options were awarded under ApolloMed’s 2015 Equity Incentive Plan (the ‘‘2015 Plan’’), and entitle the recipient to purchase the stated numbers of share of ApolloMed’s common stock at the stated exercise price when the applicable vesting requirements are satisfied. The options have exercise prices ranging from $4.50 − $6.00 and vesting terms between six months through three years.
| 199 |
The following table summarizes the outstanding equity option awards as of March 31, 2017 held by each of ApolloMed’s executive officers who are expected to continue as executive officers of the combined company.
| OPTION AWARDS | ||||||||||||||||||
| Number of | Number of | |||||||||||||||||
| Securities | Securities | |||||||||||||||||
| Underlying | Underlying | |||||||||||||||||
| Name and | Unexercised | Unexercised | Option | Option | ||||||||||||||
| Principal | Options- | Options- | Exercise | Expiration | ||||||||||||||
| Position | Grant Date | Exercisable | Unexercisable | Price (1) | Date | |||||||||||||
| Warren Hosseinion, M.D. | 12/9/2010 | 30,000 | - | $ | 1.50 | 12/8/2020 | ||||||||||||
| Chief Executive Officer | 7/10/2014 | 18,333 | 1,667 | $ | 10.00 | 7/9/2024 | ||||||||||||
| 2/15/2016 | 93,500 | - | $ | 6.37 | 2/14/2021 | |||||||||||||
| Gary Augusta | 7/10/2014 | 18,333 | 1,667 | $ | 10.00 | 7/9/2024 | ||||||||||||
| Executive Chairman | 2/15/2016 | 93,500 | - | $ | 5.79 | 2/14/2026 | ||||||||||||
| Mihir Shah | 11/14/2016 | 5,556 | 44,444 | $ | 4.50 | 11/13/2026 | ||||||||||||
| Chief Financial Officer | ||||||||||||||||||
| Adrian Vazquez, M.D. | 12/9/2010 | 30,000 | - | $ | 1.50 | 12/8/2020 | ||||||||||||
| Chief Medical Officer | 7/10/2014 | 9,167 | 833 | $ | 10.00 | 7/9/2024 | ||||||||||||
| 2/15/2016 | 23,400 | - | $ | 6.37 | 2/14/2021 | |||||||||||||
(1) All options have been issued with an exercise price equal to the closing price of ApolloMed’s common stock on the date of grant except 93,500 and 23,400 options granted to Drs. Hosseinion and Vazquez at an exercise price of $6.37 per share, or 110% of the closing price of ApolloMed’s common stock on the date of grant. The weighted average closing stock price for the 93,500 and 23,400 options on the dates of grant was $5.79 per share.
None of ApolloMed’s named executive officers exercised any stock options or had stock awards that were subject to vesting during the fiscal year ended March 31, 2017.
Potential Payments upon Termination or Change-In-Control
During fiscal year 2017, all of ApolloMed’s executive officers had provisions in their then-current employment or consulting agreements providing for payments upon certain types of termination of employment, which are substantially similar to each other. For a description of those provisions, please see “MANAGEMENT OF THE COMBINED COMPANY – Employment Agreements” above. In addition, upon the occurrence of a change of control, the Compensation Committee is authorized to take certain actions with respect to the acceleration of awards outstanding under the 2015 Plan, the 2013 Equity Incentive Plan and the 2010 Equity Incentive Plan.
NMM Compensation Discussion and Analysis
NMM’s compensation philosophy is to attract and retain talented and dedicated executives who will work to achieve NMM’s desired business direction, strategy, and performance. The primary goals of NMM’s compensation program for NMM’s named executive officers, as identified in NMM’s Summary Compensation Table for 2014-2016, are (i) to attract, motivate and retain talented executives with the skill sets and expertise NMM needs to meet its business objectives, (ii) to be competitive in the marketplace, (iii) to tie annual and long-term cash and equity incentives to the achievement of specified performance objectives that will result in increased shareholder value, and (iv) to be cost-effective. To achieve these goals, the NMM board of directors reviews and approves the executive compensation packages for its executive officers, including the named executive officers, with guidance and input from members of NMM’s senior management. These packages are generally based on a mix of salary and discretionary bonus but do not include any equity awards except in the case of Mr. Hing Ang (one of the named executive officers) whose compensation package includes stock options as described below.
| 200 |
Establishment of Cash and Equity Compensation
NMM’s board of directors typically reviews executive compensation levels on an annual basis to ensure they remain competitive in NMM’s industry. Data for this review is prepared and provided to the NMM board of directors by, and with input from, members of NMM’s senior management.
NMM does not retain the services of third-party executive compensation specialists in connection with the establishment of cash and equity compensation and related policies.
NMM evaluates individual executive performance with a goal of setting compensation at levels the NMM board believes are comparable with executives in other companies of similar size and stage of development. NMM’s relative performance and NMM’s own strategic goals are also taken into account in setting compensation levels. The primary elements of NMM’s compensation plan as described in greater detail below are base salary and discretionary annual bonus. NMM does not provide equity compensation except in the case of Mr. Hing Ang (one of the named executive officers) whose compensation package includes stock options as described below.
Base Salary
NMM tries to establish and maintain competitive annual base salaries for its named executive officers. While base salaries are not primarily performance-based, NMM believes it is important to provide adequate, fixed compensation to executives working in a highly volatile and competitive industry such as the health care industry. NMM provides fixed salary compensation to its named executive officers based on their responsibilities and individual experience and NMM’s growth and achievements.
As a result of NMM’s significant growth and expansion into various medical markets and geographical locations since 2014 and NMM’s named executive officers taking on multiple roles within NMM, including those which are typically carried out by other executive officer positions at other companies, the board of directors approved increased annual base salaries for each of 2014, 2015 and 2016 for two of its named executive officers as follows: Dr. Kenneth Sim, Executive Chairman — $440,840 (2014), $442,620 (2015) and $473,818 (2016), and Dr. Thomas Lam, Chief Executive Officer — $440,840 (2014), $442,620 (2015) and $473,818 (2016). The annual base salary for Mr. Hing Ang, NMM’s Chief Financial Officer, was increased as follows: $150,519 (2014), $150,956 (2015) and $167,692 (2016). The annual base salary for Dr. Albert Young, NMM’s Chief Medical Officer, remained unchanged at $337,840 from 2014 to 2015 but was increased to $350,834 for 2016.
Discretionary Annual Cash Bonus
In addition to base salaries, NMM management provides recommendations to the board of directors for approval regarding the amount and allocation of discretionary annual cash bonuses for NMM employees, which amounts are based on NMM net income, prior-year bonuses and corporate and individual performance. As a result of NMM’s significant growth and expansion into various medical markets and geographical locations, the board of directors approved discretionary annual cash bonuses for its named executive officers as follows: Dr. Kenneth Sim, Executive Chairman — $2,800,938 (2014) and $350,000 (2016); Dr. Thomas Lam, Chief Executive Officer — $2,800,938 (2014) and $350,000 (2016); Mr. Hing Ang, Chief Financial Officer — $50,000 (2014), $100,000 (2015) and $230,000 (2016); and Dr. Albert Young, Chief Medical Officer — $728,073 (2014) and $100,000 (2016).
| 201 |
Equity Compensation
In March 2016, based on the recommendations of management, the NMM board of directors granted an option to Mr. Hing Ang, NMM’s Chief Financial Officer, to purchase 1,100,000 shares of common stock at an exercise price of $1.00 per share, based on the following vesting schedule:
| Year 2014 | 150,000 NMM shares |
| Year 2015 | 150,000 NMM shares |
| Year 2016 | 250,000 NMM shares |
| Year 2017 | 250,000 NMM shares |
| Year 2018 | 300,000 NMM shares |
The estimated fair value of the stock option was $9,472 and was computed using the Black-Scholes option pricing model and the following assumptions: (i) estimated market price of $0.41 per share; (ii) exercise price of $1.00 per share; (iii) expected term of 1 year; (iv) volatility of 62.79%; (v) annual dividend yield of 3.53%; (vi) discount rate of 0.85%; and (vii) forfeiture rate of 8%. In recommending the stock option grant to NMM’s CFO, management considered a number of factors, including the critical role played by the CFO in the significant growth, development, and expansion of NMM in recent years. NMM’s CFO subsequently declined to exercise his stock option and, in lieu of such stock option, NMM and ApolloMed intend to replace Mr. Ang’s NMM stock option with an option to purchase 75,914 shares of ApolloMed common stock at an exercise price of $9.25 per share, based on the following vesting schedule:
| Year 2014-2017 | 55,210 ApolloMed shares |
| Year 2018 | 20,704 ApolloMed shares |
In fiscal years 2014 through 2016, there were no grants of equity compensation, stock awards or stock options issued to the named executive officers (except to Mr. Hing Ang as described above).
Employment Agreements
NMM has not entered into an employment agreement with any of its current executive officers.
Severance and Change-in-Control Benefits
None of NMM’s current executive officers are entitled to severance or change of control benefits.
Employee Benefit Plan
NMM has a qualified 401(k) plan which covers substantially all employees who have completed at least six months of service and meet minimum age requirements. Participants may contribute a portion of their compensation to the plan, up to the maximum amount permitted under Section 401(k) of the Internal Revenue Code. Participants become fully vested after six years of service. NMM matches a portion of the participants' contributions. NMM's matching contributions for the years ended December 31, 2016 and 2015 were approximately $170,917 and $137,661, respectively. No contributions were made by NMM under its 401(k) Plan during fiscal years 2014-2016 for any of its named executive officers.
Other Compensation
All of NMM’s named executive officers have standard benefits that are offered to all full-time, exempt employees. These standard benefits include health, dental and life insurance. NMM intends to continue to maintain the current benefits and perquisites for NMM’s named executive officers; however, NMM’s board of directors, in its discretion, may in the future revise, amend, or add to the benefits and perquisites of any named executive officer if it deems it advisable.
NMM Executive Officer Compensation
Summary Compensation Table for 2014-2016
The following table provides summary compensation as of December 31, 2016, 2015 and 2014 regarding NMM’s executive officers who are expected to continue as executive officers of the combined company.
| 202 |
The following table sets forth information regarding compensation earned in or with respect to fiscal years 2014, 2015 and 2016 by:
| · | Thomas Lam, M.D., Chief Executive Officer; |
| · | Kenneth Sim, M.D., Executive Chairman; |
| · | Hing Ang, Chief Financial Officer; and |
| · | Albert Young, M.D., Chief Medical Officer. |
The foregoing NMM executive officers are expected to continue as executive officers of the combined company and are referred to collectively as NMM’s named executive officers.
| Name and Principal Position |
Year | Salary | Bonus | Stock awards ($) |
Option Awards |
Non-equity incentive plan compensation ($) |
Change in pension value and nonqualified deferred compensation earnings ($) |
All other compensation (1)(2) |
Total | |||||||||||||||||||||||||||
| Thomas Lam, M.D. | 2016 | $ | 473,818 | $ | 350,000 | — | $ | — | — | — | $ | 13,275 | $ | 837,093 | ||||||||||||||||||||||
| Chief Executive Officer |
2015 | $ | 442,620 | $ | — | — | $ | — | — | — | $ | 12,512 | $ | 455,132 | ||||||||||||||||||||||
| 2014 | $ | 440,840 | $ | 2,800,938 | — | $ | — | — | — | $ | 11,862 | $ | 3,253,640 | |||||||||||||||||||||||
| Kenneth Sim, M.D. | 2016 | $ | 473,818 | $ | 350,000 | — | $ | — | — | — | $ | 19,127 | $ | 842,945 | ||||||||||||||||||||||
| Executive Chairman | 2015 | $ | 442,620 | $ | — | — | $ | — | — | — | $ | 18,038 | $ | 460,658 | ||||||||||||||||||||||
| 2014 | $ | 440,840 | $ | 2,800,938 | — | $ | — | — | — | $ | 17,123 | $ | 3,258,901 | |||||||||||||||||||||||
| Hing Ang | 2016 | $ | 167,692 | $ | 230,000 | — | $ | 9,472 | (3) | — | — | $ | — | $ | 407,164 | |||||||||||||||||||||
| Chief Financial Officer | 2015 | $ | 150,956 | $ | 100,000 | — | $ | — | — | — | $ | 21,400 | $ | 272,356 | ||||||||||||||||||||||
| 2014 | $ | 150,519 | $ | 50,000 | — | $ | — | — | — | $ | — | $ | 200,519 | |||||||||||||||||||||||
| Albert Young, M.D. | 2016 | $ | 350,834 | $ | 100,000 | — | $ | — | — | — | $ | 6,142 | $ | 456,976 | ||||||||||||||||||||||
| Chief Medical Officer | 2015 | $ | 337,840 | $ | — | — | $ | — | — | — | $ | 5,783 | $ | 343,623 | ||||||||||||||||||||||
| 2014 | $ | 337,840 | $ | 728,073 | — | $ | — | — | — | $ | 5,488 | $ | 1,071,401 | |||||||||||||||||||||||
(1) No contributions were made by NMM under its 401(k) Plan during fiscal years 2014-2016 for any of its named executive officers.
(2) Reflects health, dental and life insurance premiums paid by NMM for the benefit of Dr. Thomas Lam, Dr. Kenneth Sim and Dr. Albert Young aggregating $38,544 (2016), $36,333 (2015) and $34,473 (2014); and payments to Mr. Hing Ang in the amount of $21,400 (2015) for unused paid time off.
(3) In March 2016, based on the recommendations of management, the NMM board of directors granted an option to Mr. Hing Ang, NMM’s Chief Financial Officer, to purchase 1,100,000 shares of common stock at an exercise price of $1.00 per share, based on the following vesting schedule:
| Year 2014 | 150,000 NMM shares |
| Year 2015 | 150,000 NMM shares |
| Year 2016 | 250,000 NMM shares |
| Year 2017 | 250,000 NMM shares |
| Year 2018 | 300,000 NMM shares |
The estimated fair value of the stock option was $9,472 and was computed using the Black-Scholes option pricing model and the following assumptions: (i) estimated market price of $0.41 per share; (ii) exercise price of $1.00 per share; (iii) expected term of 1 year; (iv) volatility of 62.79%; (v) annual dividend yield of 3.53%; (vi) discount rate of 0.85%; and (vii) forfeiture rate of 8%. In recommending the stock option grant to NMM’s CFO, management considered a number of factors, including the critical role played by the CFO in the significant growth, development, and expansion of NMM in recent years. NMM’s CFO subsequently declined to exercise his stock option and, in lieu of such stock option, NMM and ApolloMed intend to replace Mr. Ang’s NMM stock option with an option to purchase 75,914 shares of ApolloMed common stock at an exercise price of $9.25 per share, based on the following vesting schedule:
| Year 2014-2017 | 55,210 ApolloMed shares |
| Year 2018 | 20,704 ApolloMed shares |
| 203 |
None of NMM’s named executive officers is covered by a pension plan or other similar benefit plan that provides for payments or other benefits at, following, or in connection with retirement.
Nonqualified Deferred Contribution and Other Nonqualified Deferred Compensation Plan
None of NMM’s named executive officers is covered by a nonqualified deferred contribution or other nonqualified deferred compensation plan.
Employment Agreements and Change in Control Arrangements
NMM has not entered into employment agreements with any of its executive officers, and none of NMM’s named executive officers are entitled to severance or change of control benefits.
Compensation Policies and Practices as Related to Risk Management
NMM management does not believe that NMM maintains compensation policies or practices that are reasonably likely to have a material adverse effect on NMM. NMM’s employees’ base salaries are fixed in amount and thus NMM does not believe that they encourage excessive risk-taking.
| 204 |
PRINCIPAL STOCKHOLDERS OF APOLLOMED
The following tables set forth information, as of October 30, 2017, concerning, except as indicated by the footnotes below:
| · | each person whom ApolloMed knows beneficially owns more than 5% of any class of shares of ApolloMed’s common stock; |
| · | each of ApolloMed’s directors; |
| · | each named executive officer listed in ApolloMed’s Summary Compensation Table above; and |
| · | all of ApolloMed’s directors and executive officers as a group. |
Unless otherwise noted below, the address of each beneficial owner listed in the table is c/o Apollo Medical Holdings, Inc. at 700 North Brand Boulevard, Suite 1400, Glendale, California 91203.
ApolloMed has determined beneficial ownership in accordance with the rules of the SEC. Except as indicated by the footnotes below, ApolloMed believes, based on the information furnished to it, that the persons and entities named in the table below have sole voting and investment power with respect to all shares of common stock that they beneficially own, subject to applicable community property laws.
Applicable percentage ownership is based on 6,033,495 shares of common stock, 1,111,111 shares of Series A preferred stock and 555,555 shares of Series B preferred stock issued and outstanding, according to the records maintained by ApolloMed’s transfer agent. Each share of Series A preferred stock and Series B preferred stock is entitled to one vote for each share of common stock into which such preferred stock is convertible, which is currently on a one-for-one basis. The holders of Series A preferred stock and Series B preferred stock vote together with the holders of common stock. In computing the number of shares of stock beneficially owned by a person and the percentage ownership of that person, ApolloMed deemed to be outstanding all shares of stock subject to options, warrants, and convertible securities held by that person or entity that are currently exercisable or convertible or that will become exercisable or convertible within 60 days following October 30, 2017. ApolloMed did not deem these shares outstanding, however, for the purpose of computing the percentage ownership of any other person.
The information provided in the following table is based on ApolloMed’s records, information filed with the SEC, and information provided to ApolloMed by the applicable holder of the stock, except where otherwise noted.
Series A and Series B Preferred Stock
| Series A Preferred Stock | Series B Preferred Stock | |||||||||||||||
|
Name and Address of Beneficial Owner |
Shares |
Percent of Class |
Shares |
Percent of Class |
||||||||||||
| Network Medical Management, Inc. 1668 S. Garfield Ave. Alhambra, California 91801 |
1,111,111 | (1) | 100 | % | 555,555 | (1) | 100 | % | ||||||||
| 205 |
Common Stock
| Name of Beneficial Owner | Shares Beneficially Owned |
Percent of Class |
||||||
| 5% Stockholders: | ||||||||
| Network
Medical Management, Inc. 1668 Garfield Avenue, 2nd Floor Alhambra, California 91801 (2) |
3,333,332 | (3) | 35.6 | % | ||||
| NNA of Nevada, Inc. 920 Winter Street Waltham, Massachusetts 02451 (4) |
800,000 | 13.3 | % | |||||
| Directors and Named Executive Officers | ||||||||
| Warren Hosseinion, M.D. | 1,162,088 | (5) | 18.8 | % | ||||
| Adrian Vazquez, M.D. | 977,821 | (6) | 16.0 | % | ||||
| Gary Augusta | 282,570 | (7) | 4.6 | % | ||||
| Mihir Shah | 15,972 | (8) | 0.3 | % | ||||
| Mark Fawcett | 35,000 | (9) | 0.6 | % | ||||
| Thomas Lam, M.D. | 3,333,332 | (10) | 35.6 | % | ||||
| Suresh Nihalani | 119,998 | (11) | 2.0 | % | ||||
| Edward Schreck | 140,000 | (12) | 2.3 | % | ||||
| David Schmidt | 80,000 | (13) | 1.3 | % | ||||
| All Executive Officers and Directors as a Group (9 persons) | 6,146,781 | (14) | 61.4 | % | ||||
| (1) | Excludes 1,666,666 shares of common stock subject to warrants that are exercisable within 60 days following October [__], 2017. | |
| (2) | The board of directors of NMM comprising of Kenneth Sim, M.D., Thomas Lam, M.D., Hung Chuen Yeung, M.D., Yang Chern Tseng, M.D., Dennis Chan, M.D., Wing Chan, M.D., George Lai, M.D., Hong Liang, M.D., Wei Wang, M.D., Paul Liu, M.D., Su Kin Lee, M.D., Nora Tee, M.D., Wan Yao, M.D., Pen Hong Lee, M.D., Theresa Tseng, M.D., Ron Gu, M.D., Mary Wang, M.D., Eddie Lam, M.D., Albert Young, M.D., Lakhi Sakhrani, M.D. and Paul Chu, M.D. have shared voting and dispositive power over the shares held by NMM. Each of the directors disclaim beneficial ownership of these shares except to the extent of his or her pecuniary interest therein. |
| (3) | Includes 1,111,111 shares of common stock issuable on conversion of 1,111,111 shares of Series A Preferred Stock, 555,555 shares of common stock issuable on conversion of 555,555 shares of Series B Preferred Stock, and 1,666,666 shares of common stock subject to warrants that are exercisable within 60 days following October [__], 2017. | |
| (4) | NNA is an indirect, wholly-owned subsidiary of Fresenius Medical Care Holdings, Inc. (“FMCH”). FMCH is an indirect wholly-owned subsidiary of Fresenius Medical Care AG & Co. KGaA (“FMC AG & Co. KGaA”). FMC AG & Co. KGaA is a German partnership limited by shares. FMC AG & Co. KGaA has been informed that as of June 30, 2016, Fresenius SE & Co. KGaA (“Fresenius SE”) owned approximately 30.9%, of FMC AG & Co. KGaA’s ordinary shares. Fresenius SE is also the owner of all of the outstanding share capital of Fresenius Medical Care Management AG (“Management AG”), the general partner of FMC AG & Co. KGaA and, accordingly, has the sole power to elect the Supervisory Board of Management AG. The Supervisory Board of Management AG has the sole power to appoint the Management Board of Management AG, which acts for Management AG as general partner in conducting the business of FMC AG & Co. KGaA. Through its ownership of the general partner of FMC AG & Co. KGaA, Fresenius SE has de facto management control of FMC AG & Co. KGaA. Based on the most recent notification to Fresenius SE, Fresenius SE has been informed that the Else Kröner-Fresenius Stiftung (the “Foundation”) owns approximately 27% of Fresenius SE’s ordinary shares. The Foundation is also the sole shareholder of Fresenius Management SE (“FSE Management”), the general partner of Fresenius SE, and has sole power to elect the Supervisory Board of FSE Management, which appoints the Management Board of FSE Management. The Management Board of FSE Management acts for FSE Management as general partner in the management of Fresenius SE. Pursuant to the terms of Mrs. Else Kröner’s will, under which the Foundation acquired most of its Fresenius SE ordinary shares, Mrs. Kröner’s executors exercise, through the Foundation, voting and dispositive power over the Fresenius SE ordinary shares held by the Foundation. They also exercise voting and dispositive power over the shares of FSE Management held by the Foundation. The persons presently serving as the executors of Mrs. Kröner’s estate are Dr. Dieter Schenk, Dr. Karl Schneider and Mr. Winfried Baranowski. Dr. Schneider and Dr. Schenk are each members (and Dr. Schenk the deputy chairman) of the Supervisory Board of FSE Management. Dr. Schenk is also vice chairman of the Supervisory Board of the FMC AG & Co. KGaA and of the Supervisory Board of Management AG. Mr. Baranowski is a member of the foundation council (Stiftungsrat) of the Foundation. Under the beneficial ownership rules of the Securities and Exchange Commission, because they hold dispositive power over the Fresenius SE ordinary shares and the FSE Management shares held directly by the Foundation, Mrs. Kröner’s executors may be deemed to beneficially own the Fresenius SE ordinary shares and FSE Management shares held by the Foundation. The foregoing information is based on and subject to the qualifications set forth in a Schedule 13/D filed by NNA on November 23, 2016. |
| (5) | Includes 149,750 shares subject to options that are exercisable within 60 days following October [__], 2017. |
| (6) | Includes 65,483 shares subject to options that are exercisable within 60 days following October [__], 2017. |
| (7) | Includes 116,625 shares subject to options that are exercisable within 60 days following October [__], 2017. |
| (8) | Includes 15,972 shares subject to options that are exercisable within 60 days following October [__], 2017. |
| (9) | Includes 35,000 shares subject to options that are exercisable within 60 days following October [__], 2017. Does not include shares held by NNA. Mr. Fawcett is the Senior Vice President and Treasurer of FMCH, the parent corporation of NNA. |
| (10) | Includes 1,111,111 shares of common stock issuable on conversion of 1,111,111 shares of Series A Preferred Stock, 555,555 shares of common stock issuable on conversion of 555,555 shares of Series B Preferred Stock, and 1,666,666 shares of common stock subject to warrants held by NMM that are exercisable within 60 days following October [__], 2017. Dr. Lam is the Chief Executive Officer, a director and a shareholder of NMM. Dr. Lam disclaims beneficial ownership of the shares beneficially owned by NMM. |
| (11) | Includes 40,000 shares held by a trust of which Mr. Nihalani is trustee and beneficiary, and 40,000 shares subject to options that are exercisable within 60 days following October [__], 2017. |
| (12) | Includes 140,000 shares subject to options that are exercisable within 60 days following October [__], 2017. |
| (13) | Includes 80,000 shares subject to options that are exercisable within 60 days following October [__], 2017. |
| (14) | Includes all of the shares identified in Notes 3 through 11. |
| 206 |
The following table and the related notes present certain information with respect to the beneficial ownership of NMM as of October 30, 2017 by:
| · | those persons who are known to NMM to be the beneficial owners of more than 5% of NMM’s common stock; |
| · | each of NMM’s directors and named executive officers; and |
| · | all directors or executive officers of NMM as a group. |
Beneficial ownership is determined in accordance with the rules of the SEC. NMM believes, based on the information furnished to NMM, that the persons and entities named in the table below will have sole voting and investment power with respect to all shares of the common stock that they will beneficially own upon completion of the Merger, subject to applicable community property laws. In computing the number of shares beneficially owned by a person and the percentage ownership of that person, shares of common stock underlying convertible preferred stock, stock options, warrants or other exercisable or convertible securities held by that person that are exercisable or convertible currently or within 60 days of October 30, 2017 are deemed outstanding, but such shares of common stock are not deemed outstanding for purposes of computing the percentage ownership of any other person.
Unless otherwise noted below, the address of each beneficial owner listed in the table is c/o Network Medical Management, Inc. at 1668 S. Garfield Avenue, 3rd Floor, Alhambra, California 91801.
| Name of Beneficial Owner | Shares Beneficially Owned |
Percent of Class |
||||||
| 5% Shareholders: | ||||||||
| Allied Physicians of California, A Professional Medical Corporation(1) | 24,582,400 | 6.2 | % | |||||
| Directors and Named Executive Officers | ||||||||
| Paul Liu, M.D. | 19,858,205 | 5.0 | % | |||||
| Thomas Lam, M.D. | 22,852,883 | 5.7 | % | |||||
| Lakhi Sakhrani, M.D. | 22,615,979 | 5.7 | % | |||||
| Kenneth Sim, M.D. | 22,853,483 | 5.7 | % | |||||
| Dennis Chan, M.D. | 17,517,665 | 4.4 | % | |||||
| Wing Chan, M.D. | 17,386,712 | 4.4 | % | |||||
| Paul Chu, M.D. | 6,789,386 | 1.7 | % | |||||
| Ron Gu, M.D. | 816,667 | * | ||||||
| George Lai, M.D. | 4,830,574 | 1.2 | % | |||||
| Eddie Lam, M.D. | 10,738,578 | 2.7 | % | |||||
| Pen Hong Lee, M.D. | 13,096,893 | 3.3 | % | |||||
| Su Kin Lee, M.D. | 16,471,544 | 4.1 | % | |||||
| Hong Liang | 6,717,911 | 1.7 | % | |||||
| Linda Marsh | - | - | ||||||
| Thuy Pham, M.D. | - | - | ||||||
| Nora Tee, M.D. | 4,997,406 | 1.3 | % | |||||
| Theresa Tseng | 13,445,656 | 3.4 | % | |||||
| Yang Chern Tseng, M.D. | 7,567,838 | 1.9 | % | |||||
| Mary Wang, M.D. | 1,926,697 | * | ||||||
| Wei Wang, M.D. | 6,241,737 | 1.6 | % | |||||
| Wan Yao, M.D. | 2,682,663 | * | ||||||
| Hung Chuen Yeung, M.D. | 1,923,713 | * | ||||||
| Albert Young, M.D. | 12,618,851 | 3.2 | % | |||||
| Hing Ang | - | - | ||||||
| All Executive Officers and Directors as a Group (25 persons) | 233,951,042 | 58.7 | % | |||||
* Represents beneficial ownership of less than 1%.
| (1) | The board of directors of APC comprising of Kenneth Sim, M.D., Thomas Lam, M.D., Dennis Chan, M.D., Wei Wang, M.D., Paul Liu, M.D., Su Kin Lee, M.D., Pen Hong Lee, M.D., Theresa Tseng, M.D., Lei Ding, M.D., Jack Wu, M.D., Raymond Cheung, M.D., Po Long Lew, D.O., Yuan Fei Chang, M.D., Peter Ma, M.D., Zhaoyang Pan, M.D., Jonathan Wu, M.D., Yu Yao, M.D., Jacqueline Wong, M.D., David Gu, D.O., and Paul Chu, M.D. have shared voting and dispositive power over the shares held by APC. Each of the directors disclaim beneficial ownership of these shares except to the extent of his or her pecuniary interest therein. |
| 207 |
ApolloMed Transactions and Relationships with Directors, Executive Officers and Five Percent Stockholders
Other than compensation described in “MANAGEMENT OF THE COMBINED COMPANY” elsewhere in this joint proxy statement/prospectus, ApolloMed believes that the only transaction or series of transactions in ApolloMed’s last three years to which ApolloMed was or is to be a participant in which the amount involved exceeds $120,000 during any 12-month period and in which any director, executive officer or holder of more than five percent of ApolloMed’s capital stock, or members of any such person’s immediate family, had or is expected to have a direct or indirect material interest are as follows:
Warren Hosseinion M.D., the Chief Executive Officer of ApolloMed, is the sole shareholder of BAHA Acquisition, a California Medical Corporation (“BAHA Acquisition”), which acquired 100% of the equity in BAHA pursuant to a Stock Purchase Agreement dated as of November 4, 2016. BAHA previously entered into a Management Services Agreement dated as of February 17, 2015 with AMM whereby AMM provided management services to BAHA.
On January 12, 2016, ApolloMed entered into a consulting agreement with Gary Augusta, the President of Flacane and ApolloMed’s Executive Chairman, whereby Mr. Augusta was paid $25,000 per month and was eligible to receive stock options in exchange for providing business and strategic services to ApolloMed; this consulting agreement has since been terminated and Mr. Augusta entered into a new employment agreement with AMM as of December 2016. In addition, Mr. Augusta is subject to a Directors’ Agreement with ApolloMed dated March 7, 2012.
As of December 31, 2016 and March 31, 2016, accounts payable in the condensed consolidated balance sheets include $0 and $104,500, respectively, for principal and accrued interest owed to a 9% note holder who is also a stockholder of ApolloMed.
In September 2015, ApolloMed was issued a promissory note by Rob Mikitarian, a minority owner in ApolloMed Palliative, in the principal amount of approximately $150,000. The note accrues interest at 3% per annum and is due on or before September 2017. At December 31, 2016 and March 31, 2016, the outstanding balance of the note was approximately $150,000, and is included in other receivables in the accompanying condensed consolidated balance sheets.
In September 2015, ApolloMed was issued a promissory note by Dr. Liviu Chindris, a minority owner in ApolloMed Palliative, in the principal amount of approximately $105,000. The note accrues interest at 3% per annum and is due on or before September 2017. At December 31, 2016 and March 31, 2016, the outstanding balance of the note was approximately $105,000, and is included in other receivables in the accompanying condensed consolidated balance sheets.
In November, 2016 ApolloMed issued the Chindris Note to Dr. Liviu Chindris, a minority owner in ApolloMed Palliative, in the principal amount of $400,000, bearing interest at the rate of 12% annually. The note is due February 17, 2017.
On January 3, 2017, NMM provided the Working Capital Loan in the principal amount of $5,000,000, which is evidenced by a Promissory Note. The Working Capital Loan has a term of two years, with ApolloMed’s payment obligations commencing on February 1, 2017 and continuing on a quarterly basis thereafter until January 2019. Under the terms of the Working Capital Loan, ApolloMed must pay NMM interest on the principal balance outstanding at the Prime Rate plus one percent. As used in the Working Capital Loan, “Prime Rate” means the prime rate of interest for commercial customers as publicly or privately announced from time to time by Bank of America. All outstanding principal and accrued but unpaid interest under the Promissory Note is due and payable in full in January 2019. ApolloMed may voluntarily prepay the outstanding principal and interest in whole or in part without penalty or premium.
| 208 |
Series A Preferred Stock and Warrant
On October 14, 2015, ApolloMed entered into a Securities Purchase Agreement (the “2015 Agreement”) with NMM pursuant to which ApolloMed sold to NMM, and NMM purchased from ApolloMed, in a private offering of securities, 1,111,111 units, each unit consisting of one share of ApolloMed’s Series A preferred stock and a warrant to purchase one share of ApolloMed’s common stock at an exercise price of $9.00 per share. NMM paid ApolloMed an aggregate of $10,000,000 for the units, the proceeds of which were used by ApolloMed primarily to repay certain outstanding indebtedness owed by ApolloMed to NNA and the balance for working capital.
The Series A preferred stock has a liquidation preference in the amount of $9.00 per share plus any declared and unpaid dividends. The Series A preferred stock can be voted for the number of shares of common stock into which the Series A preferred stock could then be converted, which initially is one-for-one.
The Series A preferred stock is convertible into common stock, at the option of the holder thereof, at any time after issuance at an initial conversion rate of one-for-one, subject to adjustment in the event of stock dividends, stock splits and certain other similar transactions. In addition, the Series A preferred stock is mandatorily convertible not sooner than the earlier to occur of (i) the later of (x) January 31, 2017 or (y) 60 days after the date on which ApolloMed files its quarterly report on Form 10-Q for the period ended September 30, 2016 (the “Redemption Expiration Date”); or (ii) the date on which ApolloMed received the written, irrevocable decision of NMM not to require a redemption of the Series A preferred stock (as described in the following paragraph), in the event that ApolloMed receives aggregate gross proceeds of not less than $5,000,000 in one or more transactions for the sale of ApolloMed’s equity securities or securities convertible into, or exchangeable for, ApolloMed’s equity securities (other than any transactions with NMM as the holder of the Series A preferred stock).
At any time prior to conversion and through the Redemption Expiration Date, the Series A preferred stock was redeemable at the option of NMM, on one occasion, in the event that ApolloMed’s net revenues for the four quarters ended September 30, 2016, as reported in its periodic filings under the Securities Exchange Act of 1934, as amended, were less than $60,000,000. In such event, ApolloMed had up to one year from the date of the notice of redemption by NMM to redeem the Series A preferred stock, warrants and any shares of common stock issued in connection with the exercise of any warrants theretofore (collectively the “Redeemed Securities”), for the aggregate price paid therefore by NMM, together with interest at a rate of 10% per annum from the date of the notice of redemption until the closing of the redemption. ApolloMed did not attain the $60,000,000 net revenues milestone by such date. NMM relinquished its redemption rights relating to the Series A preferred stock pursuant to the terms of a Consent and Waiver Agreement dated December 21, 2016 by and between ApolloMed and NMM (the “NMM Waiver”), which was entered into in connection with the entering into of the Merger Agreement.
The warrants may be exercised at any time after issuance and through October 14, 2020, for $9.00 per share, subject to adjustment in the event of stock dividends and stock splits and has a “cashless exercise” feature. The warrants are not separately transferable from the Series A preferred stock for which they relate (one-for-one).
Series B Preferred Stock and Warrant
On March 30, 2016, ApolloMed entered into a Securities Purchase Agreement with NMM (the “2016 Agreement”) pursuant to which ApolloMed sold to NMM, and NMM purchased from ApolloMed, in a private offering of securities, 555,555 units, each unit consisting of one share of ApolloMed’s Series B preferred stock and a warrant to purchase one share of ApolloMed’s common stock at an exercise price of $10.00 per share. NMM paid ApolloMed an aggregate of $4,999,995 for the units, the proceeds of which were used by ApolloMed for working capital.
The Series B preferred stock has a liquidation preference in the amount of $9.00 per share plus any declared and unpaid dividends. The Series B preferred stock can be voted for the number of shares of common stock into which the Series B preferred stock could then be converted, which initially is one-for-one.
| 209 |
The Series B preferred stock is convertible into shares of ApolloMed’s common stock, at the option of the holder thereof at any time after issuance at an initial conversion rate of one-for-one, subject to adjustment in the event of stock dividends, stock splits and certain other similar transactions. The Series B preferred stock was mandatorily convertible at any time prior to and including March 31, 2017 in the event that ApolloMed engaged in one or more transactions for the sale of its equity securities or securities convertible into, or exchangeable for, ApolloMed’s equity securities resulting in gross proceeds of not less than $5,000,000, not including any transactions with NMM as the holder of the Series B preferred stock.
The warrants may be exercised at any time after issuance and through March 30, 2021, for $10.00 per share, subject to adjustment in the event of stock dividends and stock splits, and has a “cashless exercise” feature. The warrants are not separately transferable from the Series B preferred stock for which they relate (one-for-one).
Business Arrangements with NMM Affiliates
ApolloMed derives a significant amount of its revenue from certain business relationships with NMM affiliates, as follows:
AMH signed an agreement with APC on February 1, 2016, pursuant to which ApolloMed provides 24/7 hospitalist services to patients of APC and certain of its affiliates at Garfield Medical Center. APC pays ApolloMed a capitation rate of $137,675 per month under this agreement. The term of the agreement is for one year, with automatic renewals unless terminated for cause (as defined in the agreement) or terminated without cause on 90 days’ notice. The agreement also contains confidentiality and non-solicitation provisions. AMH is an affiliate of ApolloMed and APC is an affiliate of NMM.
AMM signed an MSA with APCN on May 1, 2016, pursuant to which ApolloMed provides management services to APCN. APCN pays ApolloMed $20,000 per month under this agreement. The initial term of the agreement is for three years. AMM is a wholly-owned subsidiary of ApolloMed and APCN is an affiliate of NMM.
AMM signed an MSA with Allied Physicians ACO, LLC (“AP-ACO”) on June 30, 2016, pursuant to which ApolloMed provides management services to AP-ACO. AP-ACO pays ApolloMed $15,000 per month under this agreement. The initial term of the agreement is for three years. AP-ACO is an affiliate of NMM.
ApolloMed Palliative signed an agreement with APC on February 1, 2016, as amended on October 1, 2016, pursuant to which ApolloMed provides hospice, palliative and home health services to APC. APC pays ApolloMed on a case rate basis under this agreement, in accordance with a fee schedule as in effect from time to time. The term of the agreement is for two years, with automatic one-year renewals unless terminated for cause (as defined in the agreement) or terminated without cause on 90 days’ notice. ApolloMed Palliative is a majority-owned subsidiary of ApolloMed.
Brand New Day Care Management Agreement
On July 1, 2017, APAACO and Universal Care, Inc. dba Brand New Day (‘‘UCI’’) entered into a chronic care management agreement (the ‘‘Care Management Agreement’’), pursuant to which UCI will provide care management programs for certain APAACO patients with congestive heart failure, chronic obstructive pulmonary disease and diabetes (‘‘Covered Services’’). Initially, the parties shall run a pilot program in which APAACO will refer up to 50 patients in the Los Angeles area to receive non-emergency Covered Services care from UCI care managers. The patients will also have access to additional services for an additional fee. APAACO will pay UCI $50,000 per month per patient enrolled in the program. APAACO may adjust fees upward or downward upon giving UCI 60 working days’ prior notice.
The term of the Care Management Agreement is one year. Thereafter, the Care Management Agreement shall renew automatically for successive one-year periods unless either party gives the other party notice of termination. The Care Management Agreement shall terminate automatically upon the revocation, suspension or restriction of any license, certificates or other authority required to be maintained by UCI. Additionally, either party may terminate the Care Management Agreement with Cause (as defined in the Care Management Agreement) by giving 45 day’s prior notice or without cause by giving 90 days’ prior notice.
APAACO is owned 50% by ApolloMed and 50% by NMM. UCI is 50% owned by APC, which is a variable interest entity of NMM. Dr. Kenneth Lam, one of ApolloMed’s directors, is the Chief Executive Officer of NMM.
| 210 |
Relationship with NNA
On October 15, 2015, ApolloMed repaid, from the proceeds of the sale of the securities to NMM under the 2015 Agreement, ApolloMed’s then entire outstanding term loan and revolving credit facility with NNA, in the aggregate amount of $7,304,506, consisting of principal plus accrued interest.
On November 17, 2015, ApolloMed entered into a Conversion Agreement (the ‘‘Conversion Agreement’’), pursuant to which ApolloMed issued 275,000 shares of ApolloMed’s common stock and paid accrued and unpaid interest of $47,112, to NNA, in full satisfaction of NNA’s conversion and other rights under a convertible note in the principal amount of $2,000,000 which note NNA held. Pursuant to the Conversion Agreement, ApolloMed issued a total of 325,000 shares of ApolloMed’s common stock to NNA in exchange for all warrants held by NNA, under which NNA originally had the right to purchase 300,000 shares of ApolloMed’s common stock at an exercise price of $10.00 per share and 200,000 shares of ApolloMed’s common stock at an exercise price of $20.00 per share, in each case subject to anti-dilution adjustments. As a result of the foregoing transactions, NNA converted an aggregate $1,402,500 of principal and accrued interest, as well as exercised warrants, into an aggregate 600,000 shares of ApolloMed’s common stock.
The Conversion Agreement also amended certain terms of a Registration Rights Agreement dated March 28, 2014 between us and NNA (the ‘‘Registration Rights Agreement’’), with respect to the timing of the filing deadline for a resale registration statement covering NNA’s registrable securities. As most recently amended, the Registration Rights Agreement provides that ApolloMed is required to prepare and file with the SEC a registration statement covering the sale of NNA’s registrable securities by March 31, 2018. If ApolloMed fails to do so by such date, and for each month thereafter until ApolloMed files the registration statement registering NNA’s registrable securities, ApolloMed must pay NNA liquidated damages of 1.5% of the total purchase price of the registrable securities owned by NNA, payable in shares of ApolloMed’s common stock. ApolloMed is also required to use ApolloMed’s commercially reasonable best efforts to cause the registration statement registering NNA’s registrable securities to be declared effective by the SEC by the earlier of (i) June 30, 2018 or (ii) the 5th trading day after the date ApolloMed is notified by the SEC that such registration statement will not be reviewed or will not be subject to further review to have such registration statement declared effective by the SEC.
The Conversion Agreement also amended the Investment Agreement dated March 28, 2014 between ApolloMed and NNA (i) to delete NNA’s right to subscribe to purchase a pro rata share of certain new equity securities that may be issued by us in the future and (ii) to provide that NNA must hold at least 200,000 shares of ApolloMed’s common stock to have the right (a) to appoint a representative to attend all meetings of ApolloMed’s board and any committee thereof in a nonvoting observer capacity, and (b) to have a representative nominated as a member of the ApolloMed board and each committee thereof, including without limitation the Compensation Committee.
ApolloMed Related Person Transactions
Primarily because of laws prohibiting the corporate practice of medicine, ApolloMed has entered into long-term management service agreements, loan agreements and other similar arrangements with affiliated physician entities. These physician entities must have only physician owners and therefore ApolloMed’s Chief Executive Officer, Warren Hosseinion M.D., serves as ApolloMed’s nominee owner in such entities, as described below.
Each of ApolloMed Hospitalists, ACC, MMG, AKM and SCHC has entered into a management agreement with AMM under which AMM has exclusive authority to manage each of the affiliated entities and is obligated to provide all non-physician personnel. AMM is entitled to management fees as set forth in each management agreement. The term of each management agreement is 20 years from its effective date, and each such management agreement automatically renews for successive five-year periods unless terminated earlier for cause or because of a party’s breach.
| 211 |
In connection with the management agreements, Dr. Hosseinion has entered into Physician Shareholder Agreements in favor of ApolloMed, in his capacity as a shareholder of, and for the account of, each of the affiliated entities that have entered into management agreements with AMM. The purpose of the Physician Shareholder Agreements is to memorialize the agreement of Dr. Hosseinion to act in accordance with the management agreement and to the extent of Dr. Hosseinion’s personal authority, to refrain from any action or inaction that would result in a breach by any affiliated entity of its obligations under its management agreement. To that end, each Physician Shareholder Agreement contains covenants which obligate Dr. Hosseinion to comply with the applicable management agreement and restrict Dr. Hosseinion’s ability to transfer equity held by Dr. Hosseinion in the applicable affiliated entity or to issue new equity in the applicable affiliated entity. Each management agreement also provides ApolloMed with the right to designate a third party to acquire all (or such amount such that the transferee would acquire a 51% interest) of Dr. Hosseinion’s equity in the applicable affiliated entity for $100, subject to a fair market value adjustment, if applicable.
Each of ApolloMed Hospitalists, ACC, MMG, AKM and SCHC has additionally entered into an Intercompany Loan Agreement with AMM under which AMM has agreed to provide a revolving loan commitment to each such affiliated entities in an amount set forth in each Intercompany Loan Agreement. Each Intercompany Loan Agreement provides that AMM’s obligation to make any advances automatically terminates concurrently with the termination of the management agreement with the applicable affiliated entity. In addition, each Intercompany Loan Agreement provides that (i) any material breach by Dr. Hosseinion of the applicable Physician Shareholder Agreement or (ii) the termination of the management agreement with the applicable affiliated entity constitutes an event of default under the Intercompany Loan Agreement. The Intercompany Loan Agreement with ApolloMed Hospitalists provides for a maximum advance of $10 million and terminates on September 30, 2018. The Intercompany Loan Agreement with ACC provides for a maximum advance of $1 million and terminates on July 31, 2018. The Intercompany Loan Agreement, as amended, with MMG provides for a maximum advance of $2 million and terminates on February 1, 2018. The Intercompany Loan Agreement with AKM provides for a maximum advance of $5 million and terminates on May 30, 2019. The Intercompany Loan Agreement with SCHC provides for a maximum advance of $5 million and terminates on July 21, 2019. Outstanding principal under each of the Intercompany Loan Agreements bears interest at the greater of 10% per annum or the LIBOR rate described in each Intercompany Loan Agreement.
Certain Relationships and Related Party Transactions of NMM
Other than compensation described in “MANAGEMENT OF THE COMBINED COMPANY” elsewhere in this joint proxy statement/prospectus, NMM believes that the only transaction or series of transactions during NMM’s last three fiscal years to which NMM was or is to be a participant in which the amount involved exceeds $120,000 and in which any NMM director or executive officer who will serve as a director or an executive officer of ApolloMed following the Merger, or any holder of more than five percent of NMM’s common stock, or members of any such person’s immediate family, had or are expected to have a direct or indirect material interest are as follows:
Allied Physicians of California IPA
On July 1, 1999, APC entered into an amended and restated management and administrative services agreement with NMM for an initial fixed term of 30 years. In accordance with relevant accounting guidance, APC is determined to be a VIE and NMM is the primary beneficiary with the ability to direct the activities (excluding clinical decisions) that most significantly affect APC’s economic performance through its majority representation of the APC Joint Planning Board; therefore APC is consolidated by NMM. As of March 31, 2017, APC owns 6.29% of NMM. Kenneth Sim, M.D. is a shareholder, director and the Chairman of NMM, a shareholder, director and the Chairman of APC, and will serve as the Executive Chairman of the combined company. Thomas Lam, M.D. is a shareholder, director and the Chief Executive Officer of NMM, a shareholder, director and the Chief Executive and Financial Officer of APC, a Director of ApolloMed and will serve as the Co-Chief Executive Officer of the combined company. Albert Young, M.D. is a shareholder, director and the Chief Medical Officer of NMM, a shareholder of APC, and will serve as the Co-Chief Medical Officer of the combined company.
Advanced Diagnostic and Surgical Center
Advanced Diagnostic and Surgical Center, Inc. (“ADSC”) was formed on February 6, 2001, and operates an ambulatory surgery center in Alhambra, California. During the year ended December 31, 2016, APC paid approximately $265,000 to ADSC for services as a provider. Dr. Kenneth Sim is a director and the President of ADSC, and has a 10% ownership interest in ADSC. In addition, Dr. Thomas Lam is a director and the Chief Financial Officer of ADSC, and has a 10% ownership interest in ADSC.
| 212 |
AHMC International Cancer Center
On November 15, 2016, APC-LSMA agreed to purchase and acquire from AHMC International Cancer Center, A Medical Corporation, a California professional corporation dba AHMC International Cancer Center (“ICC”), 40% of the aggregate issued and outstanding shares of capital stock of ICC for $400,000 in cash. ICC has entered into agreements with organizations such as healthcare service plans, independent physician practice associations, medical groups and other purchasers of medical services (“Healthplans”) for the arrangement of the provision of healthcare services to subscribers or enrollees of said Healthplans. In addition, ICC has entered into written agreements with physicians and other healthcare professionals to provide or arrange for the provision of healthcare services to enrollees of participating Healthplans who have contracted or will contract with ICC for healthcare services. Subsequent to the acquisition, it was agreed that ICC’s working capital needs shall be funded as and when needed through capital contributions and/or subordinated debt by the shareholders of ICC on a pro rata basis based on their respective ownership interests in ICC. This transaction has not yet been completed. It is anticipated that Dr. Kenneth Sim and Dr. Thomas Lam will be directors and/or officers of ICC.
Allied Physicians ACO
On December 18, 2016, NMM, ACO Acquisition Corporation #2, and AP-ACO entered into a reorganization agreement whereby ACO Acquisition Corporation #2, a newly organized entity which NMM is its sole shareholder, merged into AP-ACO, effective on December 20, 2016, resulting in NMM becoming the sole shareholder of AP-ACO. AP-ACO operates an ACO, as defined under the MSSP, which is comprised of the ACO’s network of independent medical practices. The primary reason for the business combination was for NMM to acquire the member relationships of AP-ACO. As a result of the merger transaction, all of the membership interests of AP-ACO issued and outstanding immediately prior to the effective date were converted on a pro rata basis into 4,000,000 shares of NMM common stock. Prior to the merger with NMM, AP-ACO had minimal activity. For the year ended December 31, 2015, AP-ACO had approximately $200 (unaudited) of operating expenses and net loss. Each of APC, Dr. Kenneth Sim (who is a manager and the Secretary of AP-ACO) and Dr. Thomas Lam (who is the President of AP-ACO) owned membership interests in AP-ACO which were converted into 1,600,000, 245,238 and 245,238 shares of NMM, respectively, as a result of the Merger.
AMG
AMG, a Professional Medical Corporation (“AMG”) was formed on July 9, 1992, and contracts with APC as a medical group provider. During the years ended December 31, 2016 and 2015, APC paid approximately $2.2 million and $2.0 million, respectively, to AMG for services as a provider. AMG and APC are negotiations for APC (through APC-LSMA) to acquire all of the ownership interests in AMG. Dr. Kenneth Sim is a director and the Chief Financial Officer of AMG, and has a 25% ownership interest in AMG. In addition, Dr. Thomas Lam is a director and the Chairman of AMG, and has a 25% ownership interest in AMG.
APC-LSMA
Due to laws prohibiting a California professional corporation which has more than one shareholder (such as APC) from being a shareholder in another California professional corporation, APC cannot directly own shares in other professional corporations in which APC has invested, specifically: LaSalle Medical Associates (“LMA”), Pacific Medical Imaging and Oncology Center, Inc. (“PMIOC”) and Diagnostic Medical Group (“DMG”). An exception to this prohibition, however, permits a professional corporation that has only one shareholder to own shares in another professional corporation. In reliance on this exception, APC-LSMA was formed on October 15, 2012 as a professional corporation, in which Dr. Thomas Lam is the sole shareholder and the sole executive officer of APC-LSMA. APC-LSMA is controlled and consolidated by APC who is the primary beneficiary of this VIE. The only activity of APC-LSMA is to hold APC’s investments in medical corporations, specifically, LMA, PMIOC and DMG. See descriptions of these entities below.
| 213 |
APCN-ACO
On November 11, 2015, NMM, ACO Acquisition Corporation, and APCN-ACO, A Medical Professional Corp. (“APCN-ACO”) entered into a reorganization agreement whereby ACO Acquisition Corporation, a newly organized entity which NMM is its sole shareholder, merged with APCN-ACO, effective on January 8, 2016, resulting in NMM becoming the sole shareholder of APCN-ACO. APCN-ACO operates an ACO, as defined under the MSSP, which is comprised of the ACO’s network of independent medical practices. The primary reason for the business combination was for NMM to acquire the member relationships of APCN-ACO. As a result of the merger transaction, all of APCN-ACO’s shares were converted into 7,500,000 shares of NMM common stock. Prior to the merger with NMM, APCN-ACO had minimal activity. For the year ended December 31, 2015, APCN-ACO had approximately $171,000 (unaudited) of operating expenses and net loss, which included $160,000 (unaudited) of management fees from an unrelated service provider. Dr. Kenneth Sim owned a nominal number of shares in APCN-ACO which were converted into 600 shares of NMM as a result of the merger. Dr. Thomas Lam is a director and the Chief Executive Officer of APCN-ACO. Mr. Hing Ang is a director and the Chief Financial Officer of APCN-ACO, is the Chief Financial Officer of NMM, and will serve as the Chief Operating Officer of the combined company.
ApolloMed
NMM has engaged in various related party transactions with ApolloMed. See “RELATED PARTY TRANSACTIONS – Series A and Series B Financings” above for more information.
Concourse Diagnostic Surgery Center
Concourse Diagnostic Surgery Center, LLC (“CDSC”) was formed on March 25, 2010, and operates an ambulatory surgery center in City of Industry, California that is Medicare Certified and accredited by the Accreditation Association for Ambulatory Healthcare, Inc. During 2011, APC invested $625,000 for a 41.59% ownership in CDSC. Due to capital stock changes in 2016, APC’s ownership percentage in CDSC’s capital stock changed to 43.8% and 43.43% on May 31, 2016 and July 31, 2016, respectively. CDSC is consolidated as a VIE by APC as it was determined that APC has a controlling financial interest in CDSC and is the primary beneficiary of CDSC. Dr. Kenneth Sim is a manager and the President of CDSC, and has a 11.34% ownership interest in CDSC. In addition, Dr. Thomas Lam is a manager and the Chief Financial Officer of CDSC, and has a 5.05% ownership interest in CDSC.
Diagnostic Medical Group
On May 14, 2016, David C.P. Chen M.D., Inc., a California professional corporation doing business as DMG, David C.P. Chen M.D., individually (collectively “Seller”) and APC-LSMA entered into a share purchase agreement whereby APC-LSMA acquired a 40% ownership interest in DMG for total cash consideration of $1,600,000. In July 2016, APC advanced $200,000 to DMG pursuant to a promissory note agreement. The note accrues interest at 3.5% per annum and matures on June 30, 2018. The balance of $200,000 is as of December 31, 2016. During 2016, APC also contributed its portion of additional capital of $40,000 to DMG for working capital purposes, which represents APC’s 40% investment portion. During the years ended December 31, 2016 and 2015, APC paid approximately $5.3 million and $4.6 million, respectively, to DMG for provider services. APC recorded income from this investment of $43,698 in 2016 and has an investment balance of $1,683,698 at December 31, 2016. Dr. Thomas Lam is a director of DMG.
LaSalle Medical Associates
LMA was founded by Dr. Albert Arteaga in 1996 and currently operates four neighborhood medical centers employing more than 120 healthcare professionals, treating children, adults and seniors in San Bernardino County. LMA is also an IPA of independently contracted doctors, hospitals and clinics, delivering care to more than 245,000 patients in Fresno, Kings, Los Angeles, Madera, Riverside, San Bernardino and Tulare Counties. During 2012, APC-LSMA entered into a share purchase agreement whereby APC-LSMA invested $5,000,000 for a 25% interest in LMA’s IPA line of business. NMM has a management services agreement with LMA. For the years ended December 31, 2016 and 2015, APC recorded income from this investment of $3,857,391 and $985,616, respectively. During the years ended December 31, 2016 and 2015, APC also received dividends of $2,000,000 and $500,000, respectively, from LMA. During the years ended December 31, 2016 and 2015, NMM received approximately $17.2 million and $15.4 million, respectively, in management fees from LMA. As noted above, Dr. Thomas Lam is the sole shareholder and the sole executive officer of APC-LSMA. Dr. Lam is also a director of LMA. Dr. Kenneth Sim is the Chief Financial Officer and a director of LMA.
| 214 |
Medical Property Partners
NMM leases office space from Medical Property Partners, LLC (“MPP”). During the years ended December 31, 2016 and 2015, NMM paid approximately $1.0 million and $0.7 million, respectively, to MPP for office space. Dr. Kenneth Sim is a managing partner of MPP, and has an 11.82% ownership interest in MPP. Dr. Thomas Lam is a managing partner of MPP, and has a 7.26% ownership interest in MPP. Dr. Albert Young is a managing partner of MPP, and has a 9.12% ownership interest in MPP.
Netlytics
NMM entered into a Joint Venture Agreement dated as of January 25, 2017, with MediPortal LLC, a New York limited liability company (“MediPortal”), and Rulemeister Inc., a California corporation (“Rulemeister”), to form a joint venture company to be named Netlytics Enterprise LLC (“Netlytics”) for the purpose of developing and implementing a fully-integrated electronic platform that will enable ACOs, IPAs, health plans and other health care payers and providers to aggregate data and utilize analytic tools to effectively engage in population health management. Netlytics was formed on November 1, 2016. The respective ownership interests of NMM, MediPortal and Rulemeister in Netlytics will be 55%, 30% and 15%. In exchange for its 55% interest, NMM will contribute $275,000 as its capital contribution to Netlytics. It is anticipated that Dr. Kenneth Sim and Dr. Thomas Lam will be managers of Netlytics. Dr. Kenneth Sim, Dr. Thomas Lam and Dr. Albert Young each own 0.5% of MediPortal.
Pacific Ambulatory Surgery Center
Pacific Ambulatory Surgery Center, LLC, a California limited liability company (“PASC”), is a multi-specialty outpatient surgery center that is certified to participate in the Medicare program and is accredited by the Accreditation Association for Ambulatory Health Care. PASC has entered into agreements with organizations such as healthcare service plans, independent physician practice associations, medical groups and other purchasers of healthcare services for the arrangement of the provision of outpatient surgery center services to subscribers or enrollees of such health plans. On November 15, 2016, PASC and APC, entered into a membership interest purchase agreement whereby PASC sold 40% of its aggregate issued and outstanding membership interests to APC for total consideration of $800,000.
In connection with the membership interest purchase agreement, PASC entered into a management services agreement with NMM, which requires the payment of management fees computed as 2% of PASC revenues. The term of the management services agreement commenced on the effective date and extend for a period of 60 months thereafter, and may be extended in writing at the sole option of NMM for an additional period of 60 months following the expiration of the initial term and is automatically renewed for additional consecutive terms of three years unless terminated by either party. PASC shall not be permitted to terminate the management services agreement for any reason during the initial term and, if extended, the extended term.
APC recorded a loss from this investment of $20,296 in 2016 and has an investment balance of $779,704 at December 31, 2016. APC is the sole manager of PASC.
Pacific Medical Imaging and Oncology Center
PMIOC was incorporated in 2004, and provides comprehensive diagnostic imaging services such as MRI/MRA, PET/CT, CT, nuclear medicine, ultrasound, digital x-rays, bone densitometry and digital mammography at its facilities. In July 2015, APC-LSMA entered into a share purchase agreement whereby APC-LSMA invested $1,200,000 for a 40% ownership in PMIOC. APC paid $564,000 cash, and APCN-ACO and AP-ACO paid an aggregate of $36,000 on behalf of APC, for this investment with the remaining $600,000 due on or before December 31, 2016, pursuant to a promissory note dated July 1, 2015. The remaining balance of $600,000 was repaid in full in 2016. APC and PMIOC have an Ancillary Service Contract together whereby PMIOC provides covered services on behalf of APC to managed care enrollees assigned to APC. Under the Ancillary Service Contract, APC paid PMIOC fees of $1,797,064 and $1,889,366 for the years ended December 31, 2016 and 2015, respectively. During the years ended December 31, 2016 and 2015, APC recorded income from this investment of $19,722 and $126,705, respectively. Dr. Thomas Lam is a director of PMIOC.
| 215 |
Preferred Bank
On July 24, 2015, NMM entered into a promissory note agreement with Preferred Bank to borrow up to $15,000,000. The note was guaranteed by two officers of APC. The interest rate is based on the Wall Street Journal “prime rate” plus 1.00% or 4.25% as of December 31, 2015 and required 18 monthly consecutive interest payments, beginning August 24, 2015; 59 monthly consecutive principal and interest payments in the initial amount of $54,896 each, beginning February 24, 2017 and maturing on January 24, 2022. NMM borrowed $10,000,000 in October 2015 and repaid the entire amount in December 2015. The loan was cancelled on July 27, 2016.
In April 2012, NMM entered into a promissory note agreement with Preferred Bank, which was amended on April 9, 2016 (as amended, the “NMM Business Loan Agreement”). The NMM Business Loan Agreement modifies certain terms of the promissory note agreement in order to (i) increase the original loan availability amount of $2,000,000 to $10,000,000, (ii) extend the maturity date under the promissory note agreement to April 22, 2018, and (iii) add six additional guarantees. The interest rate is based on the Wall Street Journal “prime rate” plus 0.125% or 3.625% and 3.375% as of December 31, 2016 and 2015, respectively. As of December 31, 2016, NMM was not in compliance with certain financial debt covenant requirements contained in the loan agreement. Subsequent to year end, NMM obtained a waiver from the bank for noncompliance of the financial debt covenant requirements as of and for the years ended December 31, 2016 and 2015. The loan is personally guaranteed by 13 NMM shareholders who are also members of NMM’s board of directors and is collateralized by substantially all assets of NMM. No amounts were drawn on this line during 2016 and 2015 and no amounts were outstanding as of December 31, 2016 and 2015.
Mr. Li Yu is the Chairman of the Board of Directors and Chief Executive Officer of Preferred Bank, and serves on its Loan Committee and Investment Committee. Pursuant to the Merger Agreement, Mr. Yu has been selected by NMM, and ApolloMed has agreed to use reasonable efforts to elect Mr. Yu, as a Class III director, to the ApolloMed board of directors, subject to the approval of the ApolloMed stockholders.
San Gabriel Valley Management Corporation
San Gabriel Valley Management Corporation (“SGVMC”) was formed on May 21, 1987, and provides property maintenance and management services to CDSC, MPP, and AMG. Dr. Kenneth Sim is a director of SGVMC, and has a 20% ownership interest in SGVMC. In addition, Hing Ang is the Chief Accountant and Administrator of SGVMC.
Tag-2 Medical Investment Group, LLC
During the years ended December 31, 2016 and 2015, APC paid approximately $0.2 million and $0.3 million, respectively, to Tag-2 Medical Investment Group, LLC (“Tag-2”) for office space. APC was also the guarantor for Tag-2’s loan from Preferred Bank, in connection with which APC pledged collateral to the bank consisting of a $1,000,000 certificate of deposit. In November 2016, the collateral and guarantee were no longer required, as Tag-2 was able to renew the loan without APC’s collateral and guarantee. Dr. Kenneth Sim is the President of Tag-2, and has an 8.69% ownership interest in Tag-2. Dr. Thomas Lam is the Chief Financial Officer of Tag-2, and has an 8.69% ownership interest in Tag-2. Dr. Albert Young is a director of Tag-2, and has an 8.69% ownership interest in Tag-2.
Universal Care
UCI is a privately held health plan that has been in operation since 1985 and holds a license under the California Knox-Keene Act to operate as a full-service health plan. UCI contracts with the CMS under the Medicare Advantage Prescription Drug Program. On August 10, 2015, Universal Care Acquisition Partners, LLC (“UCAP”), a 100% owned subsidiary of APC, entered into a Stock Purchase Agreement with UCI to purchase 100,000 shares of UCI class A-2 voting common stock (comprising 48.9% of the total outstanding UCI shares, but 50% of UCI’s voting common stock) for $10,000,000. During the years ended December 31, 2016 and 2015, NMM recorded income from this investment of $848,027 and $94,333, respectively, and has an investment balance of $10,942,360 and 10,094,333 at December 31, 2016 and 2015, respectively. In 2015, NMM also advanced $5,000,000 to UCI for working capital purposes as a subordinated loan which accrues interest at the prime rate plus 1%, or 4.50% and 4.25% as of December 31, 2016 and 2015, respectively, with interest to be paid monthly. Pursuant to the stock purchase agreement, the principal repayment schedule is based on certain contingent criteria. The entire note receivable is as of December 31, 2016 and 2015 in the amount of $5,000,000 (see UCI disclosure above). Dr. Kenneth Sim and Dr. Thomas Lam are each directors of UCI and managers of UCAP.
| 216 |
NMM’s Policies Regarding Related Party Transactions
NMM’s policy with respect to related party transactions is administered by the NMM board. Under NMM’s related party transaction policy, a “Related Party Transaction” is any transaction, arrangement, or relationship (or any series of similar transactions, arrangements, or relationships) in which NMM or any of its subsidiaries is or will be a participant and in which any Related Person has or will have a direct or indirect material interest. A “Related Person” is any of NMM’s executive officers, directors or director nominees, any stockholder beneficially owning in excess of 5% of NMM’s stock, and any immediate family member of any of the foregoing persons, where disclosed to NMM.
NMM’s policy is to enter into or ratify Related Party Transactions only when NMM’s board determines that the Related Party Transaction in question is in, or is not inconsistent with, the best interests of NMM. In making this determination, the NMM board may take into account, among other factors it deems appropriate, whether the Related Party Transaction is on terms no less favorable than terms generally available to an unaffiliated third party under the same or similar circumstances and the extent of the Related Person’s interest in the transaction.
| 217 |
CERTAIN MATERIAL U.S. FEDERAL INCOME TAX CONSEQUENCES OF THE MERGER
The following is a discussion of the material U.S. federal income tax consequences of the Merger applicable to U.S. Holders (as defined below) who exchange their NMM common stock for ApolloMed common stock and warrants in the Merger, but does not purport in any manner to be a complete or otherwise material analysis of all potential tax effects. The effects of other U.S. federal tax laws, such as estate and gift tax laws, and any applicable state, local, or foreign tax laws are not discussed. This discussion is based on the Code, U.S. Treasury Regulations promulgated thereunder, judicial decisions, and published rulings and administrative pronouncements of the IRS in effect as of the date of the Merger. These authorities may change or be subject to differing interpretations. Any such change may be applied retroactively in a manner that could adversely affect a holder of NMM common stock.
This discussion assumes and is limited to U.S. Holders who hold their NMM common stock and will hold their shares of ApolloMed common stock and warrants received in exchange therefor, as “capital assets” within the meaning of Section 1221 of the Code (generally, property held for investment). This discussion is an overview of certain potential tax treatment and does not address all U.S. federal income tax consequences relevant to the particular circumstances of an NMM common shareholder. In addition, it does not address consequences relevant to holders of NMM common stock that are subject to particular U.S. or foreign tax rules, including, without limitation:
| · | persons subject to the alternative minimum tax or Medicare contribution tax on net investment income; |
| · | persons whose functional currency is not the U.S. dollar; |
| · | persons holding NMM common stock as part of a hedge, straddle, or other risk reduction strategy or as part of a conversion transaction or other integrated investment; |
| · | persons who are not U.S. Holders; |
| · | banks, insurance companies, and other financial institutions; |
| · | mutual funds, real estate investment trusts or regulated investment companies; |
| · | brokers, dealers, or traders in securities; |
| · | partnerships, other entities or arrangements treated as partnerships for U.S. federal income tax purposes, and other pass-through entities (and investors therein); |
| · | tax-exempt organizations or governmental organizations; |
| · | persons deemed to sell NMM common stock under the constructive sale provisions of the Code; |
| · | persons who hold or receive NMM common stock pursuant to the exercise of any employee stock options or otherwise as compensation; |
| · | persons who hold NMM common stock as “qualified small business stock” pursuant to Section 1202 of the Code; |
| · | persons holding NMM common stock who exercise dissenters’ rights; and |
| · | tax-qualified retirement plans. |
For purposes of this discussion, a “U.S. Holder” is a beneficial owner of NMM common stock that, for U.S. federal income tax purposes, is or is treated as:
| · | an individual who is a citizen or resident of the United States; |
| 218 |
| · | a corporation (or other entity taxable as a corporation for U.S. federal income tax purposes) created or organized under the laws of the United States, any state thereof, or the District of Columbia; |
| · | an estate, the income of which is subject to U.S. federal income tax regardless of its source; or |
| · | a trust if either a court within the United States is able to exercise primary supervision over the administration of such trust and one or more United States persons (within the meaning of Section 7701(a)(30) of the Code) have the authority to control all substantial decisions of such trust, or the trust has a valid election in effect under applicable Treasury Regulations to be treated as a United States person for U.S. federal income tax purposes. |
Holders of NMM common stock that are not U.S. Holders may have different U.S. federal income tax consequences than those described below and are urged to consult their own tax advisors regarding the tax treatment of the Merger to them under U.S. and non-U.S. tax laws.
If an entity treated as a partnership for U.S. federal income tax purposes holds NMM common stock, the tax treatment of a partner in the partnership will depend on the status of the partner, the activities of the partnership and certain determinations made at the partner level. Accordingly, partnerships holding NMM common stock and the partners in such partnerships should consult their tax advisors regarding the U.S. federal income tax consequences to them.
In addition, the following discussion does not address the tax consequences of the Merger under U.S. federal non-income, state, local and non-U.S. tax laws. Furthermore, the following discussion does not address any tax consequences of transactions effectuated before, after or at the same time as the Merger, whether or not they are in connection with the Merger.
SHAREHOLDERS SHOULD CONSULT THEIR TAX ADVISORS WITH RESPECT TO THE APPLICATION OF THE U.S. FEDERAL INCOME TAX LAWS TO THEIR PARTICULAR SITUATIONS AS WELL AS ANY TAX CONSEQUENCES OF THE MERGER ARISING UNDER THE U.S. FEDERAL ESTATE OR GIFT TAX LAWS OR UNDER THE LAWS OF ANY STATE, LOCAL OR NON-U.S. TAXING JURISDICTION OR UNDER ANY APPLICABLE INCOME TAX TREATY.
Material U.S. Federal Income Tax Considerations of the Merger
The Merger has been structured to qualify as a “reorganization” within the meaning of Section 368(a) of the Code. Completion of the Merger is not conditioned upon the delivery of any opinions from counsel or any other determinations as of such date, that the Merger will qualify as a “reorganization.” However, in connection with the filing of this joint proxy statement/prospectus of which this document is a part, ApolloMed has received an opinion of MWE that, as of the date of such opinion, if certain factual circumstances exist, the Merger will be treated for federal income tax purposes as a reorganization within the meaning of Section 368(a) of the Internal Revenue Code and that ApolloMed and NMM will each be a party to that reorganization. The tax opinion is an exhibit to this joint proxy statement/prospectus and the disclosure in this section is based upon such tax opinion. In addition, no ruling from the IRS has been or will be requested in connection with the Merger with respect to the tax treatment. Subject to the qualifications and assumptions described in this proxy statement/prospectus/information statement, the Merger will be treated for U.S. federal income tax purposes as a reorganization within the meaning of Section 368(a) of the Code. Accordingly, the tax consequences to U.S. Holders of NMM common stock will be as follows:
| · | a U.S. Holder will not recognize gain or loss upon the exchange of NMM common stock for ApolloMed common stock and warrants pursuant to the Merger, except to the extent of cash received in lieu of a fractional share of ApolloMed common stock as described below; |
| · | a U.S. Holder’s aggregate tax basis for the shares of ApolloMed common stock and warrants received in the Merger (including any fractional share interest for which cash is received) will equal the shareholder’s aggregate tax basis in the shares of NMM common stock surrendered upon completion of the Merger (such aggregate tax basis to be allocated to such shares of ApolloMed common stock and warrants based on their relative fair market value); |
| 219 |
| · | the holding period of the shares of ApolloMed common stock and warrants received by a U.S. Holder in the Merger should include the holding period of the shares of NMM common stock surrendered in exchange therefor; and |
| · | a U.S. Holder who receives cash in lieu of a fractional share of ApolloMed common stock in the Merger should generally recognize capital gain or loss in an amount equal to the difference between the amount of cash received instead of a fractional share and the shareholder’s tax basis allocable to such fractional share. |
Capital gains or losses recognized in the Merger as described above generally will constitute long-term capital gain or loss if the U.S. Holder’s holding period in the NMM common stock surrendered in the Merger is more than one year as of the effective date of the Merger. Long-term capital gains recognized by certain non-corporate U.S. Holders, including individuals, are currently subject to taxation at preferential rates. Short-term capital gains are taxed at rates applicable to ordinary income. The deductibility of capital losses is subject to limitations. In addition, for purposes of the above discussion of the bases and holding periods for shares of NMM common stock and ApolloMed common stock and warrants, shareholders who acquired different blocks of NMM common stock at different times for different prices must calculate their gains and losses and holding periods separately for each identifiable block of such stock exchanged in the Merger.
A portion of each Holdback Share issued to an NMM shareholder will be treated as “imputed interest” under Section 483 of the Code, with the amount of such imputed interest being based upon the applicable federal rate at the time of Merger and the period between the closing date of the Merger and the date on which the Holdback Share is issued to the NMM shareholder. The portion of such Holdback Share treated as imputed interest will be ordinary income to the NMM shareholder, rather than capital gain, and will be taxable to the NMM shareholder upon receipt.
An NMM shareholder will be required to retain records pertaining to the Merger. Each U.S. Holder who owned, immediately before the Merger, at least one percent (by vote or value) of the total outstanding stock of NMM is required to attach a statement to their tax returns for the year in which the Merger is consummated that contains the information listed in Treasury Regulation Section 1.368-3(b). Such statement must include the names and employer identification numbers of ApolloMed and NMM, the date of the Merger, the shareholder’s tax basis in, and the fair market value of, such shareholder’s NMM common stock surrendered in the Merger.
If the Merger fails to qualify as a reorganization within the meaning of Section 368(a) of the Code and does not otherwise qualify for tax-free treatment under another provision of the Code, then a U.S. Holder would recognize gain or loss upon the exchange of NMM common stock for ApolloMed common stock and warrants equal to the difference between the fair market value, at the time of the Merger, of the ApolloMed common stock and warrants received in the Merger (including any cash received in lieu of a fractional share) and such U.S. Holder’s tax basis in the NMM common stock surrendered in the Merger. Such gain or loss would be long-term capital gain or loss if the NMM common stock was held for more than one year at the time of the Merger. In such event, the tax basis of ApolloMed common stock and warrants received in the Merger would equal their fair market value at the time of the Merger and the holding period of such ApolloMed common stock and warrants would commence the day after the Merger. NMM shareholders are urged to consult their own tax advisors regarding the possibility of the Merger failing to qualify as a reorganization or for tax-free treatment under another provision of the Code and the tax consequences of such event.
Information Reporting and Backup Withholding
Certain shareholders may be subject to information reporting and backup withholding (currently at a rate of 28%) in connection with the Merger. Certain persons, including corporations, are exempt from backup withholding but may be required to demonstrate such status by providing appropriate documentation. Any amount withheld under the backup withholding rules is not an additional tax and may be refunded or credited against such shareholder’s U.S. federal income tax liability provided that the required information is properly furnished by the NMM shareholder in a timely manner to the IRS.
| 220 |
Pre-Merger Distribution of ApolloMed Warrants to NMM Shareholders
To the extent NMM distributes existing ApolloMed Warrants to NMM shareholders prior to the consummation of the Merger, such distribution will constitute a dividend for U.S. federal income tax purposes to the extent of NMM’s current or accumulated earnings and profits, as determined under U.S. federal income tax principles. The amount of such dividend will equal the fair market value of such ApolloMed Warrants at the time of the distribution. To the extent the amount of such dividend is greater than NMM’s current or accumulated earnings and profits, the excess will first be treated as a tax-free return of capital and will reduce (but not below zero) the NMM shareholder’s adjusted tax basis in the NMM common stock, and any remaining excess will be treated as capital gain from a sale or exchange of the NMM common stock. The tax basis of such ApolloMed Warrants received by an NMM shareholder will equal their fair market value at the time of the distribution and holding period for such ApolloMed Warrants will commence the day following the distribution.
THE PRECEDING DISCUSSION DOES NOT PURPORT TO BE A COMPLETE ANALYSIS OR DISCUSSION OF ALL OF THE MERGER’S POTENTIAL TAX EFFECTS. U.S. HOLDERS OF NMM STOCK SHOULD CONSULT THEIR TAX ADVISORS AS TO THE SPECIFIC TAX CONSEQUENCES TO THEM OF THE MERGER, INCLUDING TAX RETURN REPORTING REQUIREMENTS, AND THE APPLICABILITY AND EFFECT OF U.S. FEDERAL, STATE, LOCAL AND OTHER APPLICABLE TAX LAWS.
| 221 |
ApolloMed is a physician-centric, integrated population health management company working to provide coordinated outcomes-based medical care in a cost-effective manner. Led by a management team with over a decade of experience, ApolloMed has built a company and culture that is focused on physicians providing high-quality medical care, population health management and care coordination for patients, particularly senior patients and patients with multiple chronic conditions. ApolloMed believes it is well-positioned to take advantage of changes in the rapidly evolving U.S. healthcare industry, as there is a growing national movement towards more results-oriented healthcare centered on the triple aim of patient satisfaction, high-quality care and cost efficiency.
ApolloMed implements and operates innovative health care models to create a patient-centered, physician-centric experience. It has the following integrated, synergistic operations:
| · | Hospitalists, which includes ApolloMed’s contracted physicians who focus on the delivery of comprehensive medical care to hospitalized patients; |
| · | An MSSP ACO, which focuses on providing high-quality and cost-efficient care to Medicare FFS patients; |
| · | A NGACO, which started operations on January 1, 2017, and focuses on providing high-quality and cost-efficient care for Medicare FFS patients; |
| · | An IPA, which contracts with physicians and provides care to Medicare, Medicaid, commercial and dual-eligible patients on a risk- and value-based fee basis; |
| · | One clinic which ApolloMed owns, and which provides specialty care in the greater Los Angeles area; |
| · | Hospice care, palliative care, and home health services, which include ApolloMed’s at-home and end-of-life services; and |
| · | A cloud-based population health management IT platform, which was acquired in January 2016, and includes digital care plans, a case management module, connectivity with multiple healthcare tracking devices and also integrates clinical data. |
ApolloMed operates in one reportable segment, the healthcare delivery segment. ApolloMed’s revenue streams, which are described in greater detail below in “ApolloMed’s Revenue Streams and Business Operations”, are diversified among its various operations and contract types, and include:
| · | Traditional FFS reimbursement; and |
| · | Risk and value-based contracts with health plans, third party IPAs, hospitals and the NGACO and MSSP sponsored by CMS, which are the primary revenue sources for ApolloMed’s hospitalists, ACOs, IPAs and hospice/palliative care operations. |
ApolloMed serves Medicare, Medicaid, health maintenance organization (“HMO”) and uninsured patients in California. It provides services to patients, the majority of whom are covered by private or public insurance, with a small portion of its revenue coming from non-insured patients. ApolloMed provides care coordination services to each major constituent of the healthcare delivery system, including patients, families, primary care physicians, specialists, acute care hospitals, alternative sites of inpatient care, physician groups and health plans.
ApolloMed’s mission is to transform the delivery of healthcare services in the communities it serves by implementing innovative population health models and creating a patient-centered, physician-centric experience in a high performance environment of integrated care.
| 222 |
The original business owned by ApolloMed was ApolloMed Hospitalists, a hospitalist company, which was incorporated in California in June 2001, and which began operations at Glendale Memorial Hospital. Through a reverse merger, ApolloMed became a publicly held company in June 2008. ApolloMed was initially organized around the admission and care of patients at inpatient facilities such as hospitals. It has grown its inpatient strategy by providing high-quality care and innovative solutions for its hospital and managed care clients.
In 2012, ApolloMed formed an ACO, ApolloMed ACO, and an IPA, MMG. In 2013, it expanded its service offering to include integrated inpatient and outpatient services through MMG. ApolloMed ACO participates in the MSSP, the goal of which is to improve the quality of patient care and outcomes through more efficient and coordinated approach among providers.
In 2014, ApolloMed added several complementary operations by acquiring, either directly or through affiliated entities that are wholly-owned by its Chief Executive Officer, Warren Hosseinion, M.D., as nominee shareholder on its behalf of, AKM, an IPA, outpatient primary care and specialty clinics and hospice/palliative care and home health entities. During fiscal2016, ApolloMed combined the operations of AKM into those of MMG.
On July 21, 2014, through an affiliate wholly-owned by Dr. Hosseinion, as nominee shareholder on its behalf, ApolloMed acquired SCHC, a specialty clinic that focuses on cardiac care and diagnostic testing. SCHC has a MSA, with AMM, pursuant to which AMM manages all non-medical services for SCHC and has exclusive authority over all non-medical decision making related to the ongoing business operations of SCHC.
On January 12, 2016, through its wholly-owned subsidiary Apollo Care Connect, ApolloMed acquired certain technology and other assets of Healarium, Inc., which provides ApolloMed with a population health management platform that includes digital care plans, a case management module, connectivity with multiple healthcare tracking devices and the ability to integrate with multiple electronic health records to capture clinical data.
On November 4, 2016, through an affiliate wholly-owned by Dr. Hosseinion, as nominee shareholder on its behalf, ApolloMed acquired all the stock of BAHA from Scott Enderby, D.O. (“Enderby”). BAHA is a hospitalist, intensivist and post-acute care practice with a presence at three acute care hospitals, one long-term acute care hospital and several skilled nursing facilities in San Francisco.
On January 18, 2017, CMS announced that APAACO, which is owned 50% by ApolloMed, had been approved to participate in the new NGACO Model program. APAACO had applied to participate in the NGACO Model in 2016 and had received conditional approval from CMS in August 2016. Through the NGACO Model, CMS has partnered with APAACO and other ACOs experienced in coordinating care for populations of patients and whose provider groups are willing to assume higher levels of financial risk and reward under the NGACO Model. The NGACO program began on January 1, 2017.
ApolloMed operates through the following subsidiaries:
| · | AMM |
| · | Pulmonary Critical Care Management, Inc. (“PCCM”) |
| · | Verdugo Medical Management, Inc. (“VMM”); |
| · | ApolloMed ACO; |
| · | ApolloMed Palliative; |
| · | BCHC; |
| · | HCHHA; |
| · | Apollo Care Connect; and |
| · | APAACO. |
ApolloMed has a controlling interest in ApolloMed Palliative, which owns two Los Angeles-based companies, BCHC and HCHHA. ApolloMed’s palliative care services focus on providing relief from the symptoms and stress of a serious illness. The goal is to improve quality of life for both the patient and the patient’s family.
| 223 |
AMM, PCCM and VMM each operates as a physician practice management company and is in the business of providing management services to physician practice corporations under long-term MSAs, pursuant to which AMM, PCCM or VMM, as applicable, manages certain non-medical services for the physician group and has exclusive authority over all non-medical decision making related to ongoing business operations.
Through AMM, ApolloMed manages its other affiliates, including:
| · | AMH; |
| · | MMG; |
| · | BAHA; and |
| · | SCHC |
ApolloMed’s physician network consists of hospitalists, primary care physicians and specialist physicians primarily through its owned and affiliated physician groups.
Through PCCM ApolloMed manages Los Angeles Lung Center (“LALC”), and through VMM it manages Eli Hendel, M.D., Inc. (“Hendel”). On January 1, 2017, PCCM and VMM amended the MSAs entered into with LALC and Hendel, respectively. Based on its evaluation of current accounting guidance, ApolloMed determined that it no longer holds an explicit or implicit variable interest in these entities. ApolloMed has consolidated the results of these entities through December 31, 2016.
The MSAs that AMM, PCCM and VMM enter into with physician groups generally provide for management fees that are recognized as earned based on a percentage of revenues or cash collections generated by the physician practices. During fiscal 2017, ApolloMed entered into two MSAs with various hospitals to provide staffing.
On February 17, 2015, ApolloMed entered into a long-term management services agreement (the “Bay Area MSA”) with a hospitalist group located in the San Francisco Bay Area. Under the Bay Area MSA, ApolloMed provides certain business administrative services, including accounting, human resources management and supervision of all non-medical business operations. ApolloMed has evaluated the impact of the Bay Area MSA and has determined that it triggers VIE accounting, which requires the consolidation of the hospitalist group into ApolloMed’s consolidated financial statements. On November 4, 2016, ApolloMed acquired BAHA, through an affiliate wholly-owned by Dr. Hosseinion, as nominee shareholder on its behalf. As of the date of acquisition, ApolloMed obtained a controlling interest in BAHA.
During fiscal 2016, ApolloMed disposed of substantially all the assets of ACC. ACC was a clinic providing care in the Los Angeles area.
ApolloMed ACO participates in the MSSP, the goal of which is to improve the quality of patient care and outcomes through more efficient and coordinated approach among providers. In January 2017, CMS announced that APAACO was approved to participate in the NGACO Model, which began on January 1, 2017 and the AIPBP track, which began on April 1, 2017. The goal of the NGACO is to improve the quality of patient care and outcomes through more efficient and coordinated approach among providers.
ApolloMed’s principal executive offices are located at 700 North Brand Blvd., Suite 1400, Glendale, California 91203 and its telephone number is (818) 396-8050.
ApolloMed was incorporated in the State of Delaware on November 1, 1985 under the name of McKinnely Investment, Inc. On November 5, 1986 McKinnely Investment, Inc. changed its name to Acculine Industries, Incorporated and Acculine Industries, Incorporated changed its name to Siclone Industries, Incorporated on May 24, 1988. On July 3, 2008, Apollo Medical Holdings, Inc. merged into Siclone Industries, Incorporated and Siclone Industries, Incorporated, as the surviving entity from the merger, simultaneously changed its name to Apollo Medical Holdings Inc. ApolloMed’s website URL is http://apollomed.net. Information contained on, or accessible through, the website is not a part of, and is not incorporated by reference into, this Report.
| 224 |
U.S. healthcare spending has increased steadily over the past 20 years. According to CMS, the estimated total U.S. healthcare expenditures are expected to grow by 5.6% for 2016 through 2025, and 4.7 percent per year on a per capita basis. Health Spending is projected to grow 1.2% faster than the U.S. gross domestic product over the 2016 through 2025 period; as a result the health share of gross domestic product is expected to rise from 17.8% in 2015 to 19.9 percent by 2025.
CMS further reports that health spending growth by federal and state & local governments is projected to outpace growth by private businesses, households, and private payers over the projection period (5.9% compared to 5.4%, respectively) in part due to ongoing strong enrollment growth in Medicare by the baby boomer generation coupled with continued government funding dedicated to subsidizing premiums for lower income Marketplace enrollees.
Hospitalists
“Hospitalist” is the term used for doctors who are specialized in the care of patients in the hospital. This movement was initiated over a decade ago and has evolved due to many factors. These factors include:
| · | convenience; |
| · | efficiency; |
| · | financial strains on primary care doctors; |
| · | patient safety; |
| · | cost-effectiveness for hospitals; and |
| · | need for more specialized and coordinated care for hospitalized patients. |
Hospital care expenditures represent the largest segment of U.S. healthcare industry spending. According to CMS estimates, total hospital spending is anticipated to grow at an average rate of 5.5% per year for 2016 through 2025, compared to 4.9% for 2010 through 2015. The faster growth partly reflects anticipated increases in growth in the use and intensity of hospital services by Medicare’s beneficiaries over the coming decade. Hospital price growth is projected to rise from 0.9% in 2015 to an average rate of 2.4% for 2016 through 2015 related to expected faster growth in the prices of inputs required to provide hospital care.
Hospitalists assume the inpatient care responsibilities that are otherwise provided by the patient’s primary care physician or other attending physician and are reimbursed by third parties using the same visit-based or procedural billing codes as are used by the primary care physician or attending physician.
Hospitalists focus exclusively on inpatient care without the distraction of outpatient care responsibilities. Additionally, by practicing each day in the same facility, hospitalists perform consistent functions, interact regularly with the same specialists and other healthcare professionals and become accustomed to specific and unique hospital processes, which can result in greater efficiency, less process variability and better patient outcomes. Finally, hospitalists manage the treatment of a large number of patients with similar clinical needs and therefore develop practice expertise in both the diagnosis and treatment of common conditions that require hospitalization. For these reasons, ApolloMed believes that hospitalists generate operating and cost efficiencies and produce better patient outcomes. Hospitalists have an increasingly important role in pushing quality through readmission prevention, infection control, electronic health records use, patient experience scores, core measures, and appropriate use of order sets.
According to the Society of Hospital Medicine, the number of hospitalists has grown over the past decade from a few hundred to more than 52,000 at the end of 2016, making it one of the fastest-growing medical specialties in the U.S. The percentage of hospitals using hospitalists has risen from 29% in 2003 to 72% in 2014.
During fiscal 2017, ApolloMed entered into four new hospitalist service agreements, pursuant to which it provides comprehensive hospitalist services to hospitals. As of March 31, 2017, ApolloMed provided hospitalist, intensivist and physician advisor services at over 20 hospitals in Southern, Central and Northern California, and had contracts with over 50 IPAs, medical groups, health plans and hospitals.
| 225 |
IPAs
An IPA is an association of independent physicians, or other organization that contracts with independent physicians, and provides services to managed care organizations on a negotiated per capita rate, flat retainer fee, or negotiated FFS basis.
Medicare
The Medicare program was established in 1965 and became effective in 1967 as a federally-funded U.S. health insurance program for people aged 65 and older, and it was later expanded to include individuals with end-stage renal disease and certain disabled persons, regardless of income or age. Initially, Medicare was offered only on an FFS basis. Under the Medicare FFS payment system, an individual can choose any licensed physician enrolled in Medicare and use the services of any hospital, healthcare provider or facility certified by Medicare. CMS reimburses providers, based on a fee schedule, if Medicare covers the service and CMS considers it medically necessary.
Growth in Medicare spending is expected to continue to increase due to population demographics. By the year 2030, the number of these elderly persons is expected to climb to 72.8 million, or 20.3% of the total U.S. population.
Medicare Advantage is a Medicare health plan program developed and administered by CMS as an alternative to the traditional FFS Medicare program. Medicare Advantage plans contract with CMS to provide benefits to beneficiaries for a fixed premium PMPM. According to the Kaiser Family Foundation (“Kaiser”), in 2016 Medicare Advantage represented only 31% of total Medicare members, creating a significant opportunity for additional Medicare Advantage penetration of newly eligible seniors. The share of Medicare beneficiaries in such plans has risen rapidly in recent years; according to Kaiser, it reached approximately 33% by the end of open enrollment period in 2017 from approximately 13% in 2004. The reasons for this include that plan costs can be significantly lower than the corresponding cost for beneficiaries in the traditional Medicare FFS program, and plans typically provide extra benefits and provide preventive care and wellness programs.
Many health plans subcontract a significant portion of the responsibility for managing patient care to integrated medical systems such as ApolloMed. These integrated healthcare systems, whether medical groups or IPAs, offer a comprehensive medical delivery system and sophisticated care management know-how and infrastructure to more efficiently provide for the healthcare needs of the population enrolled with that health plan. Reimbursement models for these arrangements vary around the country. In California, health plans typically prospectively pay the IPA or medical group a fixed PMPM, or capitation payment, which is often based on a percentage of the amount received by the health plan. Capitation payments to IPAs or medical groups, in the aggregate, represent a prospective budget from which the IPA manages care-related expenses on behalf of the population enrolled with that IPA. Those IPAs or medical groups that manage care-related expenses under the capitated levels will realize an operating profit; if care-related expenses exceed projected levels, the IPA will realize an operating deficit.
Integrated healthcare delivery companies such as ApolloMed can utilize their medical care and quality management strategies and interventions for potential high cost cases and aggressively manage them to improve the health of its population and therefore lower costs for these patients. Additionally, IPAs and medical groups such as MMG have established physician performance metrics that allow them to monitor quality and service outcomes achieved by participating physicians in order to reward efficient, high quality care delivered to members and to initiate improvement efforts for physicians whose results can be enhanced.
ApolloMed provides managed care services through MMG, and it has entered into capitation agreements with health plans, either directly or through a management service organization (“MSO”).
| 226 |
Medicaid
Medicaid is a Federal entitlement program administered by the states that provides healthcare and long-term care services and support to low-income Americans. Medicaid is funded jointly by the states and the Federal government. The Federal government guarantees matching funds to states for qualifying Medicaid expenditures based on each state’s Federal medical assistance percentage, which is calculated annually and varies inversely with the average personal income in the state. Each state establishes its own eligibility standards, benefit packages, payment rates and program administration within Federal guidelines. In an effort to improve quality and provide more uniform and cost-effective care, many states have implemented Medicaid managed care programs to improve access to coordinated care, to improve preventive care and to control healthcare costs. Under Medicaid managed care programs, a health plan receives capitation payments from the state. The health plan then arranges for healthcare services to be provided by contracting either directly with providers or with IPAs and medical groups, such as MMG. MMG has entered into capitation agreements with health plans, either directly or through an MSO.
Commercial
Patients enrolled in health plans offered through their employers are generally referred to as commercial members. According to the United States Census Bureau, in 2014, the last year for which data is available, approximately 55.4% of non-elderly U.S. citizens received their healthcare benefits through their employers, which contracted with health plans to administer these healthcare benefits. Nationally, commercial employer-sponsored health plan enrollment was approximately 150 million in 2015.
Dual Eligibles
A portion of Medicaid beneficiaries are dual eligibles, meaning that they are low-income seniors and people with disabilities who are enrolled in both Medicaid and Medicare. Based on CMS estimates, there are approximately 10.7 million dual eligible enrollees with annual spending of approximately $285 billion. Only a small percentage of the total spending on dual eligibles is administered by managed care organizations. Dual eligibles tend to consume more healthcare services due to their tendency to have more chronic conditions. In some states, dual eligible patients are being voluntarily enrolled and/or auto-assigned into managed care programs. About 1.1 million low-income seniors and people with disabilities in California receive health care services through both the Medicare and Medi-Cal (Medicaid nationally) programs.
Health Reform Acts
In an effort to reduce the number of uninsured and intending to control healthcare expenditures, President Obama signed the ACA in 2010, as amended by the Health Care and Education Reconciliation Act of 2010 (the “Health Reform Acts”). The Health Reform Acts seek a reduction of up to 32 million uninsured individuals by 2019, while potentially increasing Medicaid coverage by up to 16 million individuals and net commercial coverage by 16 million individuals. CMS projects that the total number of uninsured Americans will fall to 23 million by 2023 from 45 million in 2012. The current enrollment numbers (as of February 2016) are roughly 20 million total between the ACA between the Marketplace. The uninsured rate remains at an all-time low with 10.9% of under 65 uninsured as of 4th quarter 2016 according to CDC data. ApolloMed believes that this represents a significant new market opportunity for health plans and integrated healthcare delivery companies. Efforts to amend, or repeal and replace, the ACA and Health Reform Acts could have a material impact on ApolloMed’s business and market opportunities.
As of March 31, 2017, MMG delivered services to nearly 15,000 members through a network of over 140 primary care physicians and over 380 specialist physicians.
ACOs
One provision of the Health Reform Acts required CMS to establish an MSSP that promotes accountability and coordination of care through the creation of ACOs, which, as described below, are eligible to participate in some of the savings generated by such ACOs. The Medicare FFS program was designed for beneficiaries in the Medicare FFS program. CMS established the MSSP to facilitate coordination and cooperation among providers to improve the quality of care and reduce unnecessary costs. Eligible providers, hospitals and suppliers may participate in the MSSP by creating an ACO and then applying to CMS. MSSP ACOs must have at least 5,000 Medicare beneficiaries in order to be eligible to participate in the program.
| 227 |
The MSSP is designed to improve beneficiary outcomes and increase value of care by (1) promoting accountability for the care of Medicare FFS beneficiaries; (2) requiring coordinated care for all services provided under Medicare FFS; and (3) encouraging investment in infrastructure and redesigned care processes. The MSSP rewards ACOs that lower their healthcare costs while meeting performance standards on quality of care and patient satisfaction. Under the final MSSP rules, Medicare will continue to pay individual providers and suppliers for specific items and services as it currently does under the FFS payment system. The MSSP rules require CMS to develop a benchmark for savings to be achieved by each ACO if the ACO is to receive shared savings. An ACO that meets the program’s quality performance standards will be eligible to receive a share of the savings to the extent its assigned beneficiary medical expenditures are below the medical expenditure benchmark provided by CMS. A minimum savings rate (“MSR”) must be achieved before the ACO can receive a share of the savings. Once the MSR is surpassed, all the savings below the benchmark provided by CMS will be shared 50% with the ACO. The MSR varies depending on the number of patients assigned to the ACO, starting at 3.9% for ACOs with patients totaling 5,000 and increasing to 2% for ACOs with more than 60,000 patients. The MSSP program is an all-or-nothing system, that is, an ACO either earns all of its allocable savings or none of it. In performance year 2014 (fiscal 2016), ApolloMed did not receive an MSSP payment from CMS. Although ApolloMed exceeded its total benchmark expenditures, generating $3.9 million in total savings and achieving an ACO Quality Score of 90.4% on its Quality Performance Report, CMS determined that ApolloMed did not meet the minimum savings threshold in performance year 2015 and therefore did not receive the “all or nothing” annual shared savings payment in fiscal 2017. ApolloMed is eligible to be considered for an all-or-nothing payment under this program for performance year 2016 (which, if it is paid, would be paid to ApolloMed in fiscal 2018). However, ApolloMed does not believe that it will be eligible to receive payments for performance years beginning 2017, because of its transition to, and business focus on, the NGACO Model, in which it is participating as of January 1, 2017.
CMS assigns a beneficiary to the preliminary roster of an ACO if the ACO physicians billed for a “plurality” of services during the calendar year preceding the performance period. A plurality means the ACO physicians provided a greater proportion of primary care services, measured in terms of allowed charges, than the physicians in any other ACO or Medicare-enrolled tax identification number. CMS sets the benchmark for each ACO using the historical medical costs of the beneficiaries assigned to the ACO. Under the final MSSP rules, primary care physicians may only join one ACO, unless they have more than one Medicare tax identification number.
In January 2016, CMS announced the first batch of participants in the NGACO Model. CMS is implementing the NGACO Model under section 1115A of the Social Security Act, which authorizes CMS, through its Center for Medicare and Medicaid Innovation, to test innovative payment and service delivery models that have the potential to reduce Medicare, Medicaid or Children’s Health Insurance Program expenditures while maintaining or improving the quality of beneficiaries’ care. The purpose of the NGACO Model is to test an alternative Medicare ACO payment model. Specifically, this model will test whether health outcomes improve and Medicare Parts A and B expenditures for Medicare FFS beneficiaries decrease if Medicare ACOs (1) accept a higher level of financial risk compared to existing Medicare ACO payment models, and (2) are permitted to select certain innovative Medicare payment arrangements and to offer certain additional benefit enhancements to their assigned Medicare FFS beneficiaries. On January 18, 2017, CMS announced that APAACO had been approved to participate in the NGACO Model. Through this new model, CMS will partner with APAACO and other ACOs experienced in coordinating care for populations of patients and whose provider groups are willing to assume higher levels of financial risk and reward under the NGACO Model. APAACO began operations on January 1, 2017.
To position itself to participate in the NGACO Model, ApolloMed has devoted, and intends to continue to devote, significant effort and resources, financial and otherwise, to the NGACO Model, and refocused away from certain other parts of its historic business and revenue streams, which will receive less emphasis in the future and could result in reduced revenue from these activities. No revenues were generated from the NGACO Model in fiscal 2017.
| 228 |
Hospice Care, Palliative Care and Home Health Organizations
Hospice companies serve terminally ill patients and their families. Comprehensive management of the healthcare services and products needed by hospice patients and their families are provided through the use of an interdisciplinary team. Depending upon a patient’s needs, each hospice patient is assigned an interdisciplinary team comprised of a physician, nurse(s), home health aide(s), social worker(s), chaplain, dietary counselor and bereavement coordinator, as well as other care professionals. Hospice services are provided primarily in the patient’s home or other residence, such as an assisted living residence or nursing home, or in a hospital. Medicare’s hospice benefit is designed for patients expected to live six months or less. Hospice services for a patient can continue, however, for more than six months, as long as the patient remains eligible as reflected by a physician’s certification.
Home health care companies provide direct home nursing and therapy services in addition to nutrition and disease management education. These services are provided by licensed and Medicare-certified skilled nurses and other paraprofessional nursing personnel.
Hospitalists
Through its affiliated physician group, AMH, ApolloMed:
| · | Provides admission, daily rounding and discharge of patients at acute care hospitals and long-term acute hospitals for health plans, hospitals and IPAs |
| · | Evaluates patients in the emergency room to determine if they may be safely discharged to home, a skilled nursing facility or other facility |
| · | Provides physician advisor consultative services for hospitals, which entail meeting daily with hospital case managers to review the charts, lab studies and imaging studies of hospitalized patients to determine if they meet criteria for continued stay in the hospital, to determine observation versus inpatient status and to evaluate proper coding |
| · | Provides intensivist/ICU services for hospitals |
| · | Provides out-of-network to in-network transfers of patients for health plans and IPAs |
IPA
ApolloMed’s IPA is a network of independent primary care physicians and specialists who collectively care for HMO patients under either a capitated payment or FFS arrangement. Under the capitated model, an HMO pays ApolloMed’s IPA a PMPM rate, or a “capitation” payment, and then assigns ApolloMed’s IPAs the responsibility for providing the physician services required by the applicable patients. The physicians in ApolloMed’s IPA are exclusively in control of, and responsible for, all aspects of the practice of medicine for ApolloMed’s patients. ApolloMed’s IPA enters into contracts with HMOs, either directly or through a risk-shifting arrangement with MSOs, to provide physician services to enrollees of the HMOs. Most of the HMO agreements have an initial term of two years renewing automatically for successive one-year terms. The HMO agreements generally provide for a termination by the HMOs for cause at any time, although ApolloMed has never experienced a termination. The HMO agreements generally allow either party to terminate the HMO agreements without cause with a four to six month notice.
Through its IPA, ApolloMed provides the following services:
| · | Physician recruiting |
| · | Physician contracting |
| · | Medical management, including utilization management and quality assurance |
| 229 |
| · | Provider relations |
| · | Member services, including annual wellness evaluations |
| · | Education of physicians on proper coding |
| · | Data collection and analysis |
| · | Pre-negotiating contracts with specialists, labs, imaging centers, nursing homes and other vendors |
ApolloMed’s IPA entered into an agreement with an MSO to receive 98% of the gross revenue received for all enrollees attributable to ApolloMed during the term of the provider service agreement (“PSA”) and ApolloMed is responsible for all medical services required by the enrollees.
ACOs
ApolloMed currently owns one MSSP ACO, ApolloMed ACO, and co-owns one NGACO with NMM, APAACO. ACOs are entities that contract with CMS to serve the Medicare FFS population with the goal of better care for individuals, improved health for populations and lower costs. ACOs share savings with CMS to the extent that the actual costs of serving assigned beneficiaries are below certain trended benchmarks of such beneficiaries and certain quality performance measures are achieved.
ApolloMed ACO
In 2012, ApolloMed formed an MSSP ACO, ApolloMed ACO, which focuses on providing high-quality and cost-efficient care to Medicare FFS patients. Through ApolloMed ACO, ApolloMed provides the following services for its physicians and patients:
| · | Population health management, using an analytics platform to analyze monthly claims data from CMS and data collected from each physician’s practice |
| · | Care coordination in the inpatient and outpatient settings using case managers |
| · | High-risk management of patients with multiple chronic conditions |
| · | Educating ApolloMed’s physicians. For example, ApolloMed has a partnership with Boehringer Ingelheim to educate its physicians on patients with chronic obstructive pulmonary disease |
| · | Services for ApolloMed’s patients. For example, ApolloMed provides health education, medication reconciliation and motivational interviewing for its patients |
| · | Promote use of evidence-based medicine by ApolloMed’s physicians |
As of March 31, 2017, ApolloMed ACO had over 30 physicians and nearly 2,200 Medicare FFS beneficiaries in California. The decrease in physicians and Medicare FFS beneficiaries compared to fiscal 2016 is primarily the result of providers enrolling in ApolloMed’s NGACO and their patients becoming beneficiaries under ApolloMed’s NGACO.
APAACO
On January 18, 2017, CMS announced that APAACO had been approved to participate in the NGACO Model. APAACO had applied to participate in the NGACO Model in 2016 and had received conditional approval from CMS in August 2016. The NGACO Model is a new CMS program that builds upon previous ACO programs. Through this new model, CMS will provide an opportunity to APAACO and other ACOs experienced in coordinating care for populations of patients and whose provider groups are willing to assume higher levels of financial risk and reward to participate in this new attribution-based risk sharing model. As discussed in more detail below, there are different levels of financial risk and reward a NGACO may select, and the extent of risk and reward may be limited on a percentage basis.
In October 2017, CMS notified APAACO that it has not been renewed for participation in the AIPBP payment mechanism of the NGACO Model for performance year 2018 due to certain alleged deficiencies in performance by APAACO. APAACO does not believe the allegations by CMS of performance deficiencies are valid or justify the CMS non-renewal determination and is in discussions with CMS regarding possible reversal of such determination. If APAACO is not successful in convincing CMS to reverse its decision then the payment mechanism under the NGACO Model would default to traditional FFS. This would result in the loss in monthly revenues of cash flow currently being generated by APAACO and would thus have a material adverse effect on ApolloMed’s future revenues and potential cash flow.
| 230 |
APAACO began operations on January 1, 2017. Under the NGACO Model, APAACO will be responsible for the medical management and care coordination of over 32,000 Medicare beneficiaries in California. This number may decrease due to beneficiaries who join a managed care (HMO) plan, pass away or move out of the service area. In 2016, in advance of commencing ApolloMed’s participation in the program, APAACO signed agreements with over 700 providers, including more than 590 physicians, 18 hospitals, more than 15 skilled nursing facilities and multiple labs, radiology centers, outpatient surgery centers, dialysis clinics and other service providers. Under the terms of ApolloMed’s agreements with these parties, the NGACO Model providers, including hospitals, agreed to receive 100% of their claims for ACO beneficiaries reimbursed by APAACO. APAACO negotiated discounted Medicare rates with multiple physicians and other service providers, discounted diagnosis-related group rates with multiple hospitals and discounted resource utilization group rates with multiple skilled nursing facilities.
In connection with the approval by CMS for APAACO to participate in the NGACO Model, CMS and APAACO have entered into the Participation Agreement. AMM has a long-term MSA with APAACO. The term of the Participation Agreement is two performance years, through December 31, 2018. CMS may offer to renew the Participation Agreement for an additional two performance years. Additionally, the Participation Agreement may be terminated sooner by CMS as specified therein, and CMS has the authority to alter or change the program over this time period.
Among many requirements to be eligible to participate in the NGACO Model, ACOs must have at least 10,000 assigned Medicare beneficiaries and must maintain that number throughout each performance year. APAACO started its performance year with 32,078 assigned Medicare beneficiaries.
The NGACO Model uses a prospectively-set cost benchmark, which is established prior to the start of each performance year. The benchmark is based on four factors:
Baseline: The 2017 performance year NGACO Model baseline for APAACO is based on calendar year 2014 expenditures. The baseline is updated each year to reflect the NGACO’s participant list for the given year.
Trend: A projected trend that is similar to the national projected trend used in the Medicare Advantage program.
Risk Adjustment: To account for differing medical condition acuity of an ACO’s beneficiaries. The risk adjustment is based on Hierarchical Condition Category (“HCC”) risk scores. The ACO’s full HCC risk score has an annual cap of up to 3%.
Discount: Unlike the MSSP ACO program, the NGACO Model does not utilize a Minimum Savings Rate. Instead, CMS applies a discount to the benchmark once the baseline has been calculated, trended and risk-adjusted. The base discount is 2.25% and can range from 0% to 3% depending on the three factors of (1) regional efficiency, (2) national efficiency and (3) quality score attained by the ACO.
NGACOs must provide a financial guarantee to CMS. The financial guarantee must be in an amount equal to 2% of its total capped Medicare Part A and Part B expenditures for beneficiaries. CMS allows the following forms of financial guarantees: (1) funds placed in an escrow amount; (2) a line of credit as evidenced by a letter of credit upon which only CMS may draw; or (3) a surety bond.
APAACO’s total capped Medicare Part A and Part B expenditures were approximately $335 million for performance year 1, and therefore APAACO submitted a letter of credit for $6.7 million to CMS.
As required by the Participation Agreement, APAACO shall maintain an aligned population of at least 10,000 beneficiaries during each performance year. APAACO and its participants may not participate in any other Medicare shared savings initiatives. APAACO shall require its participants and preferred providers to make medically necessary covered services available to beneficiaries in accordance with applicable laws, regulations and guidance.
| 231 |
APAACO shall implement processes and protocols that relate to specified objectives for patient-centered care consistent with the NGACO model. In connection therewith, APAACO shall require its participants to comply with and implement these designated processes and protocols, and shall institute remedial processes and penalties, as appropriate, for participants that fail to comply with or implement a required process or protocol.
CMS shall use APAACO’s quality scores calculated under the relevant provisions of the Participation Agreement to determine, in part, its “Performance Year Benchmark”. CMS shall assess APAACO’s quality performance using the quality measures set forth in the Participation Agreement and the quality measure data required to be reported by APAACO as set forth in the Participation Agreement. CMS shall use APAACO’s performance on each of the quality measures to calculate its total quality score according to a methodology to be determined by CMS prior to the start of each performance year. For each performance year, CMS shall determine APAACO’s Performance Year Benchmark. No later than 15 days before the beginning of each performance year, CMS shall provide the ACO with a Performance Year Benchmark Report consisting of APAACO’s Performance Year Benchmark. On a quarterly basis during each performance year, CMS shall provide APAACO with a Quarterly Financial Report. The Quarterly Financial Report may comprise adjustments to the Performance Year Benchmark resulting from updated information regarding any factors that affect the Performance Year Benchmark calculation.
For each performance year, APAACO shall submit to CMS its selections for risk arrangement; the amount of a savings/loss cap; alternative payment mechanism; benefits enhancements, if any; and its decision regarding voluntary alignment under the NGACO Model. APAACO must obtain CMS consent before voluntarily discontinuing any benefit enhancement during a performance year.
For each performance year, CMS shall pay APAACO in accordance with the alternative payment mechanism, if any, for which CMS has approved APAACO; the risk arrangement for which APAACO has been approved by CMS; and as otherwise provided in the Participation Agreement. Following the end of each performance year, and at such other times as may be required under the Participation Agreement, CMS will issue a settlement report to APAACO setting forth the amount of any shared savings or shared losses and the amount of other monies owed. If CMS owes APAACO shared savings or other monies owed, CMS shall pay the ACO in full within 30 days after the date on which the relevant settlement report is deemed final, except as provided in the Participation Agreement. If APAACO owes CMS shared losses or other monies owed as a result of a final settlement, APAACO shall pay CMS in full within 30 days after the relevant settlement report is deemed final. If APAACO fails to pay the amounts due to CMS in full within 30 days after the date of a demand letter or settlement report, CMS shall assess simple interest on the unpaid balance at the rate applicable to other Medicare debts under current provisions of law and applicable regulations. In addition, CMS and the U.S. Department of the Treasury may use any applicable debt collection tools available to collect any amounts owed by APAACO.
Unless specifically permitted under the Participation Agreement, APAACO participants, preferred providers and other individuals or entities performing functions and services related to ACO activities are prohibited from providing gifts or other remuneration to beneficiaries to induce them to receive items or services from APAACO, its participants or preferred providers, or to induce them to continue to receive items or services from APAACO, its participants or preferred providers.
APAACO shall maintain the privacy and security of all NGACO-related information that identifies individual beneficiaries in accordance with HIPAA, Privacy and Security Rules and all relevant HIPAA guidance applicable to the use and disclosure of protected health information by covered entities, as well as applicable state laws and regulations.
The Participation Agreement requires APAACO to report specified information on a publicly accessible website maintained by it, which information includes organizational information, shared savings and shares losses information, and performance on quality measures.
The NGACO Model offers two risk arrangement options. In Arrangement A, the ACO takes 80% of Medicare Part A and Part B risk. In Arrangement B, the ACO takes 100% of Medicare Part A and Part B risk. Under each risk arrangement, the ACO can cap aggregate savings and losses anywhere between 5% to 15%. The cap is elected annually by the ACO. APAACO has opted for Risk Arrangement A and a shared savings and losses cap of 5%.
| 232 |
The NGACO Model offers four payment mechanisms:
| · | Payment Mechanism #1: Normal FFS. |
| · | Payment Mechanism #2: Normal FFS plus Infrastructure payments of $6 Per Beneficiary Per Month (“PBPM”). |
| · | Payment Mechanism #3: Population-Based Payments (“PBP”). PBP payments provide ACOs with a monthly payment to support ongoing ACO activities. ACO participants and preferred providers must agree to percentage payment fee reductions, which are then used to estimate a monthly PBP payment to be received by the ACO. |
| · | Payment Mechanism #4: AIPBP. Under this mechanism, CMS will estimate the total annual expenditures of the ACO’s aligned beneficiaries and pay that projected amount in PBPM payments. ACOs in AIPBP may have alternative compensation arrangements with their providers, including 100% FFS, discounted FFS, capitation or case rates. |
APAACO began operations on January 1, 2017. APAACO opted for, and was approved by CMS to participate in, the AIPBP track, which is the most advanced risk-taking payment model, effective April 1, 2017. APAACO is the only ACO in the United States out of 44 approved NGACOs that is participating in the AIPBP track. Under the AIPBP track, CMS will estimate the total annual expenditures for APAACO's patients and then pay that projected amount to ApolloMed in a per-beneficiary, per-month payment. ApolloMed would then be responsible for paying all Part A and Part B costs for in-network participating providers and preferred providers with whom it has contracted.
The NGACO Model provides ACOs with additional tools not found in the ACO programs, but that are used in the Medicare Advantage program to improve quality and lower cost, including preferred provider networks, negotiated discounts and beneficiary incentives.
AMM has entered into a long-term MSA with APAACO (the “APAACO MSA”). Under the APAACO MSA, AMM provides APAACO with care coordination, data analytics and reporting, technology and other administrative capabilities to enable participating providers to deliver better care and lower healthcare costs for their Medicare FFS beneficiaries. APAACO employs local operations and clinical staff to drive physician engagement and care coordination improvements.
Clinic
ApolloMed’s outpatient clinic provides specialty services, such as cardiology and pulmonary services. ApolloMed also owns an imaging center complete with magnetic resonance imaging (“MRI”), compound tomography (“CT”), cardiac echo, ultrasound, and nuclear and exercise stress-test equipment. ApolloMed’s clinic focuses on the efficient delivery of ambulatory treatment and ancillary services, with an increasing emphasis on preventive care and managing chronic conditions. ApolloMed’s clinic also serves as a post-discharge center for patients who have just left the hospital.
ApolloMed’s clinic is located within ApolloMed’s historical core service areas in the greater Los Angeles area. The clinic has served its communities for many years, handles approximately 25,000 patient visits per year and provides specialty services and lab and imaging services.
Hospice Care, Palliative Care and Home Health Care Operations
ApolloMed’s hospice care, palliative care and home health operations provide hospice care, palliative care and home health services for patients using an interdisciplinary team composed of physicians, nurses and other healthcare workers. For hospice services, depending on the needs of the specific patient in each case, the ApolloMed service team may include a physician, nurse, home health aide, medical social worker, chaplain, dietary counselor and bereavement coordinator. ApolloMed’s hospice and palliative care services are provided in the patient's home, assisted living or nursing home or in a hospital. ApolloMed’s home health services are provided directly in each patient’s home and may include skilled nursing and therapy services, as well as specialty programs such as disease management education, nutrition and help with daily living activities.
| 233 |
ApolloMed’s hospice and home health services are currently offered only in Southern California, with an average daily census of about 28 hospice patients and 80 home health patients during fiscal 2017. ApolloMed experienced a decrease in patients compared to fiscal 2016 primarily as a function of restructuring its hospice/palliative care and home health operations.
ApolloMed generates revenue through various contractual agreements which vary in both structure and by type of business operation. These contracts are multi-year renewable contracts that include traditional FFS, capitation, case rates, and professional and institutional risk contracts. ApolloMed’s revenue streams consist of contracted, FFS, capitation and MSSP revenue.
| 234 |
Contracted revenue
Contracted revenue represents revenue generated under management agreements for which ApolloMed provides physician and other healthcare staffing and administrative services in return for a contractually negotiated fee. Contracted revenue consists primarily of billings based on hours of healthcare staffing provided at agreed-upon hourly rates. Additionally, contracted revenue also includes supplemental revenue from hospitals where ApolloMed may have an FFS contract arrangement or provide physician advisory services to the medical staff at a specific facility. Such contract terms generally either provide for a fixed monthly dollar amount or a variable amount based upon measurable monthly activity, such as hours staffed, patient visits or collections per visit, compared to a minimum activity threshold. Such supplemental revenues based on variable arrangements are usually contractually fixed on a monthly, quarterly or annual basis considering the variable factors negotiated in each such agreement. Additionally, ApolloMed derives a portion of its revenue as a contractual bonus from collections received by its partners and such revenue is contingent upon the collection of third-party billings. In certain cases, the revenue is also subject to achieving certain quality metrics.
FFS revenue
FFS revenue represents revenue earned under agreements in which ApolloMed bills and collects the professional component of charges for medical services rendered by its contracted and employed physicians. Under its FFS arrangements, ApolloMed bills patients for services provided and receives payment from patients or their third-party payors. FFS revenue is the reported net of contractual allowances and policy discounts. All services provided are expected to result in cash flows and are therefore reflected as net revenue in ApolloMed’s consolidated financial statements. The recognition of net revenue (gross charges less contractual allowances) from patient visits is dependent on such factors as proper completion of medical charts following a patient visit, the forwarding of such charts to ApolloMed’s billing center for medical coding and entering into the ApolloMed billing system and the verification of each patient’s submission or representation at the time services are rendered as to the payor(s) responsible for payment for such services.
Capitation revenue
Capitation revenue represents revenue that ApolloMed generates based on agreements that generally make it liable for excess medical costs. The use of capitation under PSAs is intended to control the use of health care resources by putting ApolloMed at financial risk for services provided to patients. Capitation is a fixed amount of money per patient per unit of time paid in advance for the delivery of health care services. The actual amount of money paid to ApolloMed is determined by the ranges of services that ApolloMed provides, the number of patients involved, and the period of time during which the services are provided. Capitation rates under ApolloMed’s PSAs are generally based on local costs and average utilization of services. To ensure that contracting physicians provide necessary care to their patients, ApolloMed monitors and measures rates of resource utilization in physician practices and submits reports to appropriate regulators. These reports are made available to the public as a measure of health care quality, and can be linked to financial rewards, such as bonuses. For example, ApolloMed receives incentives under “pay-for-performance” programs for quality medical care, based on various criteria.
Additionally, Medicare pays capitation using a “risk adjustment” model, which compensates managed care organizations and providers based on the health status (acuity) of each individual enrollee. Health plans and providers with higher acuity enrollees receive more and those with lower acuity enrollees receive less. Under risk adjustment, capitation is determined based on health severity, measured using patient encounter data. Capitation is paid on an interim basis based on data submitted for the enrollee for the preceding year and is adjusted in subsequent periods after the final data is compiled.
| 235 |
MSSP Revenue
Through its subsidiary, ApolloMed ACO, ApolloMed participates in the MSSP sponsored by CMS. The MSSP allows ACO participants to share in cost savings it generates in connection with rendering medical services to Medicare patients. Payments to ACO participants, if any, are calculated annually and paid once a year by CMS on cost savings generated by the ACO participant relative to the ACO participants’ CMS benchmark. Under the MSSP program, an ACO either receives the full amount of its allocable cost savings or nothing. The MSSP is a newly formed program with minimal history of payments to ACO participants. Under the final MSSP rules, Medicare will continue to pay individual providers and suppliers for specific items and services as it currently does under the FFS payment methodologies. The MSSP rules require CMS to develop a benchmark for savings to be achieved by each ACO if the ACO is to receive shared savings. An ACO that meets the MSSP’s quality performance standards will be eligible to receive a share of the savings to the extent its assigned beneficiary medical expenditures are below the medical expenditure benchmark provided by CMS. An MSR must be achieved before the ACO can receive a share of the savings. Once the MSR is surpassed, all the savings below the benchmark provided by CMS will be shared 50% with the ACO. The MSR varies depending on the number of patients assigned to the ACO, starting at 3.9% for ACOs with patients totaling 5,000 and increasing to 2% for ACOs with more than 60,000 patients.
ApolloMed considers revenue, if any, under the MSSP, as contingent upon the realization of program savings as determined by CMS, and are not considered earned and therefore are not recognized as revenue until notice from CMS that cash payments are to be imminently received. ApolloMed received an MSSP payment in fiscal 2015 but did not receive an MSSP payment in fiscal 2016 or fiscal 2017. ApolloMed is eligible to be considered for an all-or-nothing payment under this program for performance year 2016 (which, if it is paid, would be paid to ApolloMed in fiscal 2018). However, ApolloMed does not believe that it will be eligible to receive payments for performance years beginning 2017, because of its transition to, and business focus on, the NGACO Model, in which it is participating as of January 1, 2017.
NGACO Model
Through APAACO, ApolloMed participates in the NGACO Model sponsored by CMS. For each performance year, CMS will determine APAACO’s Performance Year Benchmark. No later than 15 days before the beginning of each performance year, CMS will provide APAACO with a Performance Year Benchmark Report consisting of APAACO’s Performance Year Benchmark. On a quarterly basis during each performance year, CMS shall provide APAACO with a Quarterly Financial Report. The Quarterly Financial Report may comprise adjustments to the Performance Year Benchmark resulting from updated information regarding any factors that affect the Performance Year Benchmark calculation. For each performance year, APAACO will submit to CMS its selections for risk arrangement; the amount of a savings/loss cap; alternative payment mechanism; benefits enhancements, if any; and its decision regarding voluntary alignment under the NGACO model. APAACO must obtain CMS consent before voluntarily discontinuing any benefit enhancement during a performance year.
For each performance year, CMS will pay APAACO in accordance with the alternative payment mechanism, if any, for which CMS has approved APAACO; the risk arrangement for which APAACO has been approved by CMS; and as otherwise provided in the Participation Agreement. Following the end of each performance year, and at such other times as may be required under the Participation Agreement, CMS will issue a settlement report to APAACO setting forth the amount of any shared savings or shared losses and the amount of other monies owed. If CMS owes APAACO shared savings or other monies owed, CMS will pay APAACO in full within 30 days after the date on which the relevant settlement report is deemed final, except as provided in the Participation Agreement. If APAACO owes CMS shared losses or other monies owed as a result of a final settlement, APAACO shall pay CMS in full within 30 days after the relevant settlement report is deemed final. If APAACO fails to pay the amounts due to CMS in full within 30 days after the date of a demand letter or settlement report, CMS will assess simple interest on the unpaid balance at the rate applicable to other Medicare debts under current provisions of law and applicable regulations. In addition, CMS and the U.S. Department of the Treasury may use any applicable debt collection tools available to collect any amounts owed by APAACO.
ApolloMed’s NGACO operations began on January 1, 2017. APAACO was approved to participate in the AIPBP track, which is the most advanced risk-taking payment model, effective April 1, 2017. APAACO is the only ACO in the United States out of 44 approved NGACOs that is participating in the AIPBP model. Under the AIPBP track, CMS estimates the total annual expenditures for APAACO's patients and then pays that projected amount to ApolloMed in a per-beneficiary, per-month payment. ApolloMed is then responsible for paying all Part A and Part B costs for in-network participating providers and preferred providers with whom it has contracted.
| 236 |
No revenues were generated from the NGACO Model in fiscal 2017 and management is in the process of evaluating the appropriate revenue recognition.
Hospitalist Agreements
During the year, ApolloMed entered into several new hospitalist agreements with hospitals, whereby it earns a stipend fee plus a fee based on an agreed percentage of FFS collections. The fee is recorded at an amount net of the portion owed to the hospitals (ApolloMed collects all fees on behalf of the hospitals). The fee revenue is further reduced by a portion subject to quality metrics which is only recorded as revenue upon ApolloMed’s meeting these metrics. ApolloMed considered the indicators of gross revenue and net revenue reporting and determined that revenue from this arrangement is recorded at net.
Types of Revenue by Business Operation
Each of ApolloMed’s operations generates revenue in the following manners:
· Hospitalists. AMH contracts with health plans or IPAs to be paid on fee schedules or case rates to see patients and earns revenue primarily on a contracted basis. AMH also contracts directly with hospitals for fixed monthly stipends for continuous staffing coverage.
· IPA. MMG earns revenue based on capitation payments from health plans. In California, health plans prospectively pay the IPA or medical group a fixed PMPM amount, or capitation payment, which is often based on a percentage of the amount received by the health plan. Capitation payments to medical groups or IPAs, in the aggregate, represent a prospective budget from which the IPA manages care-related expenses on behalf of the population enrolled with that IPA. Those IPAs or medical groups that manage care-related expenses under the capitated levels will realize an operating profit; if care-related expenses exceed projected levels, the IPA will realize an operating deficit.
· ACO and APAACO. ApolloMed ACO and APAACO are different versions of a “shared savings” performance model that, in each case, has contracted with CMS and earns revenue from MSSP based on cost-savings achieved. As discussed above, the MSSP rewards ACOs that lower their healthcare costs while meeting performance standards on quality of care and patient satisfaction on an all-or-nothing basis once a year.
· Care Clinics - ApolloMed Care Clinic’s clinics receive the majority of their revenue from traditional FFS models where the physicians are paid based on professional fee schedules from various health plans, and also receive capitated payments from IPAs, including MMG.
· Palliative Care, Home Health and Hospice Service Operations - ApolloMed Palliative, which includes BCHC and Holistic Health, receives both FFS and contracted revenue. Under the home health Prospective Payment System (“PPS”) of reimbursement, for Medicare and Medicare Advantage programs paid at episodic rates, ApolloMed estimates net revenues to be recorded based on a reimbursement rate which is determined using relevant data, relating to each patient’s health status including clinical condition, functional abilities and service needs, as well as applicable wage indices to give effect to geographic differences in wage levels of employees providing services to the patient. Billings under PPS are initially recognized as deferred revenue and are subsequently amortized into revenue over an average patient treatment period. The process for recognizing revenue to be recorded is based on certain assumptions and judgments, including (i) the average length of time of each treatment as compared to a standard 60 day episode; (ii) any differences between the clinical assessment of and the therapy service needs for each patient at the time of certification as compared to actual experience; and (iii) the level of adjustments to the fixed reimbursement rate relating to patients who receive a limited number of visits, are discharged but readmitted to another agency within the same 60-day episodic period or are subject to certain other factors during the episode. Revenues for hospice are recorded on an accrual basis based on the number of days a patient has been on service at amounts equal to an estimated payment rate. The payment rate is dependent on whether a patient is receiving routine home care, general inpatient care, continuous home care or respite care. Adjustments to Medicare revenues are recorded based on an inability to obtain appropriate billing documentation or authorizations acceptable to the payor or other reasons unrelated to credit risk.
| 237 |
Key Payors
ApolloMed has a few key payors that represent a significant portion of its net revenue. For the fiscal year ended March 31, 2017, four payors accounted for 47.2% of ApolloMed's net revenue. For the fiscal year ended March 31, 2016, three payors accounted for 55.4% of ApolloMed’s net revenue.
| Year Ended March 31, 2017 |
Year Ended March 31, 2016 |
|||||||
| Governmental - Medicare/Medi-Cal | 18.8 | % | 29.8 | % | ||||
| L.A. Care | 13.1 | % | 15.7 | % | ||||
| Allied Physicians | 8.5 | % | 0.0 | % | ||||
| HealthNet | 6.8 | % | 9.9 | % | ||||
ApolloMed’s business and operations are located exclusively in California, and all of ApolloMed’s revenue is derived from its operations in California. As of March 31, 2017, through its managed physician practices, ApolloMed provided hospitalist services at more than 20 acute-care hospitals and long-term acute care facilities in California, and operated one specialty medical clinic in the Los Angeles area. MMG provides primary and specialist care through its contracted physicians to over 15,000 patients throughout the greater Los Angeles area. ApolloMed ACO has nearly 2,200 Medicare beneficiaries assigned to it by CMS in California. Additionally, ApolloMed had approximately 32,000 beneficiaries in its NGACO, exclusively in California at the start of its performance year in January 2017.
ApolloMed’s mission is to transform the delivery of health services to the communities it serves by implementing innovative population health and care coordination models and by creating a patient-centered, physician-centric experience in a high-performing environment of integrated care.
ApolloMed’s current intention is to implement its strategy through a combination of organic growth and acquisitions, as well as dispositions when appropriate. While it has taken many concrete steps to achieve its strategy, there is no guarantee that it will be successful in these endeavors and it may not achieve its strategic goals. The principal elements of ApolloMed’s growth strategy are:
Pursue growth opportunities in established markets
ApolloMed identifies growth opportunities in established markets it serves by working with its local network physicians. Opportunities may include continued physician enrolment for MMG and ApolloMed ACO, additional or expanded hospitalist contracts, new risk-based insurance contracts and new clinic acquisitions.
Continue to strengthen ApolloMed’s market presence and reputation
ApolloMed positions itself to thrive in a changing healthcare environment by continuing to build and operate high-performing, patient-centered care networks, fully engaging in health and wellness, and enhancing its reputation in its markets. ApolloMed focuses particularly on patient safety, patient satisfaction, care coordination, population health and implementing clinical quality best practices across all its operations. ApolloMed measures the health status of its patients with the goal of directly improving their health.
| 238 |
Focus on high-quality, patient-centered care
ApolloMed provides high-quality, patient-centered care in its communities. ApolloMed has implemented several initiatives to maintain and enhance the delivery of high-quality care, including clinical best practices, information technology and tools, coordination of care, home visits, annual wellness exams and population health.
Drive physician collaboration and alignment
ApolloMed fosters a collaborative approach among its physicians to provide what it believes to be clinically superior healthcare services. ApolloMed provides medical management, population health management and care coordination resources to its physicians sufficient to support the necessary, high-quality services to its patients. ApolloMed has implemented several initiatives, including active participation of physician leadership in ApolloMed ACO, MMG and hospitalist boards and subcommittees, training programs and information technology resources. In addition, ApolloMed is aligning with its physicians in various forms of risk contracting, including pay-for-performance programs such as clinical documentation improvement to improve RAF scores and certain programs, such as annual wellness visits, to improve Medicare Advantage STAR ratings.
Expand ambulatory services and further its population health strategies
ApolloMed is flexible and competitive in a dynamic healthcare environment. ApolloMed intends to continue to add medical management and population health management resources to its ambulatory care services. ApolloMed intends to pursue further strategies in physician practice management and population health services, such as predictive analytics and telemedicine services. ApolloMed also intends to pursue the expansion of certain strategic services, such as home health care, hospice and palliative care services in an attempt to create a more comprehensive network of healthcare services.
Pursue selective acquisitions
ApolloMed believes that its philosophy, built on patient-centered healthcare and clinical quality and efficiency, gives it a competitive advantage in expanding its services in its existing markets as well as other markets through acquisitions or partnerships. ApolloMed regularly monitors opportunities to acquire hospitalist groups, IPAs, ACOs and clinics that fit its vision and long-term strategies.
Pursue selective dispositions
ApolloMed regularly monitors the performance of its operations and has curtailed, cut back on or disposed of certain operations that either are not performing up to its expectations or are creating a financial strain on it.
Expand its relationships with payors and facilities in selective markets across the United States
ApolloMed intends to explore ways to develop relationships with existing and new health plans and hospitals in selective markets across the United States in order to participate in the growing hospitalist medicine market, under value-based contracts.
Acquisitions and Dispositions
In furtherance of its growth strategy, ApolloMed regularly evaluates opportunities to add to its portfolio of healthcare companies in areas where it does not have a presence, in order to expand its geographic footprint, in areas where it already has a presence to increase its market share, and in areas of practice that are complementary to its existing business model. Similarly, ApolloMed periodically evaluates parts of its business that may not fit within its overall business model or may be underperforming and, when appropriate, ApolloMed may dispose of such companies.
| 239 |
On January 12, 2016, through its wholly-owned subsidiary Apollo Care Connect, ApolloMed acquired certain technology and other assets of Healarium, Inc. This acquisition provides ApolloMed with a population health management platform that includes digital care plans, a case management module, connectivity with multiple healthcare tracking devices and the ability to integrate with multiple electronic health records to capture clinical data. ApolloMed issued 275,000 shares of its common stock in exchange for the acquired assets and the seller paid ApolloMed $200,000.
Also during fiscal 2016, ApolloMed sold substantially all the assets of ACC. ACC was a clinic providing care in Los Angeles area. The purchase price was $61,000 of which ApolloMed received $10,000 in cash and the balance in the form of a non-interest bearing promissory note in the principal amount of $51,000. ApolloMed also combined the operations of one of its IPAs, AKM, into those of its other IPA, MMG.
On November 4, 2016, through an affiliated wholly-owned by Dr. Hosseinion, as nominee shareholder on its behalf, ApolloMed acquired all the stock of BAHA from Enderby. BAHA is a hospitalist, intensivist and post-acute care practice with a presence at three acute care hospitals, one long-term acute care hospital and several skilled nursing facilities in San Francisco.
Corporate Practice of Medicine
ApolloMed’s consolidated financial statements include ApolloMed’s accounts and those of ApolloMed’s subsidiaries and certain affiliated medical practices. Some states have laws that prohibit business entities with non-physician owners, such as ApolloMed, from practicing medicine, which are generally referred to as corporate practice of medicine. States that have corporate practice of medicine laws require only physicians to practice medicine, exercise control over medical decisions or engage in certain arrangements with other physicians, such as fee-splitting. California is a corporate practice of medicine state. Therefore, in California, ApolloMed operates by maintaining long-term management service agreements with its affiliates, each of which are owned and operated by physicians only, and which employ or contract with additional physicians to provide hospitalist services. Under MSAs, ApolloMed provides and performs all non-medical management and administrative services, including financial management, information systems, marketing, risk management and administrative support. The management agreements typically have an initial term of 20 years unless terminated by either party for cause. These MSAs are not terminable by ApolloMed’s affiliates, except in the case of gross negligence, fraud, or other illegal acts by ApolloMed, or ApolloMed’s bankruptcy.
Through the MSAs and the relationship with the physician owners of its medical affiliates, ApolloMed has exclusive authority over all non-medical decisions related to the ongoing business operations of those affiliates. Consequently, ApolloMed consolidates the revenue and expenses of its affiliates from the date of execution of the management agreements, as the primary beneficiary of these VIEs.
When necessary, Dr. Hosseinion, ApolloMed’s Chief Executive Officer, serves as nominee shareholder, on ApolloMed’s behalf, of affiliated medical practices, in order to comply with corporate practice of medicine laws and certain accounting rules applicable to consolidated financial reporting by ApolloMed’s affiliates, as VIEs.
The healthcare industry is highly competitive and fragmented across all of ApolloMed’s services and operations. ApolloMed competes for customers with many other healthcare providers, including local physicians and practice groups as well as local, regional and national networks of physicians, hospitals and other healthcare companies, many of which are substantially larger than ApolloMed and have significantly greater financial and other resources, including personnel, than ApolloMed has.
Hospitalists
AMH faces competition primarily from numerous small inpatient practices as well as large physician groups, many of whom have greater financial, personnel and other resources available to them. Some of ApolloMed’s competitors operate on a national level, such as EmCare, Team Health and Sound Physicians. In addition, because the market for hospitalist services is highly fragmented and the ability of individual physicians to provide services in any hospital where they have certain credentials and privileges, competition for growth in existing and expanding markets is not limited to ApolloMed’s largest competitors.
| 240 |
IPAs
ApolloMed’s affiliated IPA, MMG, competes with other IPAs, medical groups and hospitals, many of whom have greater financial, personnel and other resources available to them. For example, in Los Angeles, examples of ApolloMed’s competitors include Regal Medical Group and Lakeside Medical group, which are part of the Heritage Provider Network (“Heritage”), as well as HealthCare Partners, which is owned by DaVita HealthCare Partners (“DaVita”).
ACOs
ApolloMed ACO and APAACO compete with hospitals, sophisticated provider groups, and MSOs in the creation, administration, and management of ACOs, many of whom have greater financial, personnel and other resources available to them. For example, in Los Angeles, competitors with APAACO include Heritage California ACO and DaVita Medical ACO California.
Hospice Care, Palliative Care and Home Health Care
The palliative care and hospice care providers with which ApolloMed competes include not-for-profit and charity-funded programs that may have strong ties to their local communities and for-profit programs, many of whom have greater financial, personnel and other resources available to them. Home health providers include not-for-profit and for-profit facility-based agencies, such as hospitals or nursing homes, as well as independent companies, some of which are large publicly-traded companies and which have greater financial, personnel and other resources available to them.
ApolloMed Palliative competes with hospice and home health agencies, many of whom have greater financial, personnel and other resources available to them. In Los Angeles, ApolloMed’s competitors include Vitas and Lakeview.
Professional Liability and Other Insurance Coverage
ApolloMed’s business has an inherent and significant risk of claims of medical malpractice against its affiliated physicians and against ApolloMed. ApolloMed’s independent physician contractors and ApolloMed pay premiums for third-party professional liability insurance that indemnifies ApolloMed’s affiliated hospitalists and ApolloMed on a claims-made basis for losses incurred related to medical malpractice litigation. Professional liability coverage is required in order for ApolloMed’s affiliated hospitalists to maintain hospital privileges. ApolloMed’s physicians carry first dollar coverage with limits of liability equal to not less than $1,000,000 for all claims based on occurrence up to an aggregate of $3,000,000 per year.
While ApolloMed believes that its insurance coverage is adequate based upon its claims experience and the nature and risks of its business, ApolloMed cannot be certain that its insurance coverage will be adequate to cover liabilities arising out of claims asserted against it, its affiliated professional organizations or its affiliated hospitalists in the future where the outcomes of such claims are unfavorable. ApolloMed believes that the ultimate resolution of all pending claims, including liabilities in excess of its insurance coverage, will not have a material adverse effect on its financial position, results of operations or cash flows; however, there can be no assurance that future claims will not have such a material adverse effect on ApolloMed’s business.
ApolloMed also maintains worker’s compensation, director and officer, and other third-party insurance coverage subject to deductibles and other restrictions that it believes are in accordance with industry standards. ApolloMed believes that these insurance coverage limits are appropriate based upon its claims experience and the nature and risks of its business. However, it cannot assure that any pending or future claim will not be successful or, if successful, will not exceed the limits of available insurance coverage.
| 241 |
Significant Federal and State Healthcare Laws Governing ApolloMed’s Business
As a healthcare company, ApolloMed’s operations and relationships with healthcare providers such as hospitals, other healthcare facilities, and healthcare professionals are subject to extensive and increasing regulation by numerous federal, state, and local government entities. These laws and regulations often are interpreted broadly and enforced aggressively by multiple government agencies, including the OIG, the U.S. Department of Justice, CMS, and various state authorities. ApolloMed has included brief descriptions of some, but not all, of the laws and regulations that affect ApolloMed’s business below.
Imposition of liabilities associated with a violation of any of these healthcare laws and regulations could have a material adverse effect on ApolloMed’s business, financial condition and results of operations. ApolloMed cannot guarantee that its arrangements or business practices will not be subject to government scrutiny or be found to violate certain healthcare laws. Government investigations and prosecutions, even if ApolloMed is ultimately found to be without fault, can be costly and disruptive to ApolloMed’s business. Moreover, changes in healthcare legislation or government regulation may restrict ApolloMed’s existing operations, limit the expansion of ApolloMed’s business or impose additional compliance requirements and costs, any of which could have a material adverse effect on ApolloMed’s business, financial condition and results of operations.
False Claims Acts
The federal False Claims Act imposes civil liability on individuals or entities that submit false or fraudulent claims for payment to the federal government. The False Claims Act provides, in part, that the federal government may bring a lawsuit against any person whom it believes has knowingly or recklessly presented, or caused to be presented, a false or fraudulent request for payment from the federal government, or who has made a false statement or used a false record to get a claim for payment approved. Private parties may initiate qui tam whistleblower lawsuits against any person or entity under the False Claims Act in the name of the government and may share in the proceeds of a successful suit.
The federal government has used the False Claims Act to prosecute a wide variety of alleged false claims and fraud allegedly perpetrated against Medicare and state healthcare programs. By way of illustration, these prosecutions may be based upon alleged coding errors, billing for services not rendered, billing services at a higher payment rate than appropriate, and billing for care that is not considered medically necessary. The government and a number of courts also have taken the position that claims presented in violation of certain other statutes, including the federal Anti-Kickback Statute or the Stark Law, can be considered a violation of the False Claims Act based on the theory that a provider impliedly certifies compliance with all applicable laws, regulations, and other rules when submitting claims for reimbursement.
Penalties for False Claims Act violations include fines ranging from $5,500 to $11,000 for each false claim, plus up to three times the amount of damages sustained by the government. A False Claims Act violation may provide the basis for the imposition of administrative penalties as well as exclusion from participation in governmental healthcare programs, including Medicare and Medicaid. In addition to the provisions of the False Claims Act, which provide for civil enforcement, the federal government also can use several criminal statutes to prosecute persons who are alleged to have submitted false or fraudulent claims for payment to the federal government.
A number of states have enacted false claims acts that are similar to the False Claims Act. Even more states are expected to do so in the future because Section 6031 of the DRA, amended the federal law to encourage these types of changes, along with a corresponding increase in state initiated false claims enforcement efforts. Under the DRA, if a state enacts a false claims act that is at least as stringent as the federal statute and that also meets certain other requirements, the state will be eligible to receive a greater share of any monetary recovery obtained pursuant to certain actions brought under the state’s false claims act. The OIG, in consultation with the Attorney General of the United States, is responsible for determining if a state’s false claims act complies with the statutory requirements. Currently, many states, including California have some form of state false claims act.
| 242 |
Anti-Kickback Statutes
The federal Anti-Kickback Statute is a provision of the Social Security Act that prohibits as a felony offense the knowing and willful offer, payment, solicitation or receipt of any form of remuneration in return for, or to induce, (1) the referral of a patient for items or services for which payment may be made in whole or part under Medicare, Medicaid or other federal healthcare programs, (2) the furnishing or arranging for the furnishing of items or services reimbursable under Medicare, Medicaid or other federal healthcare programs or (3) the purchase, lease, or order or arranging or recommending the purchasing, leasing or ordering of any item or service reimbursable under Medicare, Medicaid or other federal healthcare programs. The ACA amended section 1128B of the Social Security Act to make it clear that a person need not have actual knowledge of the statute, or specific intent to violate the statute, as a predicate for a violation. The OIG, which has the authority to impose administrative sanctions for violation of the statute, has adopted as its standard for review a judicial interpretation which concludes that the statute prohibits any arrangement where even one purpose of the remuneration is to induce or reward referrals. A violation of the Anti-Kickback Statute is a felony punishable by imprisonment, criminal fines of up to $25,000, civil fines of up to $50,000 per violation and three times the amount of the unlawful remuneration. A violation also can result in exclusion from Medicare, Medicaid or other federal healthcare programs. In addition, pursuant to the changes of the ACA, a claim that includes items or services resulting from a violation of the Anti-Kickback Statute is a false claim for purposes of the False Claims Act.
Due to the breadth of the Anti-Kickback Statute’s broad prohibitions, statutory exceptions exist that protect certain arrangements from prosecution. In addition, the OIG has published safe harbor regulations that specify arrangements that also are deemed protected from prosecution under the Anti-Kickback Statute, provided all applicable criteria are met. The failure of an activity to meet all of the applicable safe harbor criteria does not necessarily mean that the particular arrangement violates the Anti-Kickback Statute, but these arrangements may be subject to scrutiny and prosecution by enforcement agencies. The conduct or business arrangement, however, does increase the risk of scrutiny by government enforcement authorities. ApolloMed may be less willing than some of its competitors to take actions or enter into business arrangements that do not clearly satisfy the safe harbors. As a result, this unwillingness may put ApolloMed at a competitive disadvantage.
Some states have enacted statutes and regulations similar to the Anti-Kickback Statute, but which may be applicable regardless of the payor source for the patient. These state laws may contain exceptions and safe harbors that are different from and/or more limited than those of the federal law and that may vary from state to state. For example, California has adopted the Physician Outpatient Referral Act (“PORA”). PORA makes it unlawful for a healing arts licensee, including physicians and surgeons, and other licensed professionals, to refer a person for certain health care services if the licensee has a financial interest, with the person or entity that receives the referral. While the law also provides certain exemptions from this prohibition, failure to fit within an exemption in violation of PORA can lead to a misdemeanor offense that may subject a physician to civil penalties and disciplinary action by the Medical Board of California.
Although ApolloMed has established policies and procedures to ensure that its arrangements with physicians comply with current laws and applicable regulations, ApolloMed cannot assure you that regulatory authorities that enforce these laws will not determine that some of these arrangements violate the Anti-Kickback Statute or other applicable laws. An adverse determination could subject ApolloMed to liabilities under the Social Security Act, including criminal penalties, civil monetary penalties and exclusion from participation in Medicare, Medicaid or other federal health care programs, any of which could have a material adverse effect on ApolloMed’s business, financial condition or results of operations.
Federal Stark Law
The Federal Stark Law, also known as the physician self-referral law, generally prohibits a physician from referring Medicare and Medicaid patients to an entity (including hospitals) providing ‘‘designated health services,’’ if the physician or a member of the physician’s immediate family has a ‘‘financial relationship’’ with the entity, unless a specific exception applies. Designated health services include, among other services, inpatient and outpatient hospital services, clinical laboratory services, certain imaging services, and other items or services that ApolloMed’s affiliated physicians may order. The prohibition applies regardless of the reasons for the financial relationship and the referral; and therefore, unlike the federal Anti-Kickback Statute, intent to violate the law is not required. Like the Anti-Kickback Statute, the Stark Law contains a number of statutory and regulatory exceptions intended to protect certain types of transactions and business arrangements from penalty. Unlike safe harbors under the Anti-Kickback Statute with which compliance is voluntary, an arrangement must comply with every requirement of a Stark Law exception or the arrangement is in violation of the Stark Law.
| 243 |
The penalties for violating the Stark Law can include the denial of payment for services ordered in violation of the statute, mandatory refunds of any sums paid for such services and civil penalties of up to $15,000 for each violation, double damages, and possible exclusion from future participation in the governmental healthcare programs. A person who engages in a scheme to circumvent the Stark Law’s prohibitions may be fined up to $100,000 for each applicable arrangement or scheme.
Some states have enacted statutes and regulations similar to the Stark Law, but which may be applicable to the referral of patients regardless of their payor source and which may apply to different types of services. These state laws may contain statutory and regulatory exceptions that are different from those of the federal law and that may vary from state to state.
Because the Stark Law and its implementing regulations continue to evolve, ApolloMed does not always have the benefit of significant regulatory or judicial interpretation of this law and its regulations. ApolloMed attempts to structure its relationships to meet an exception to the Stark Law, but the regulations implementing the exceptions are detailed and complex, and ApolloMed cannot be certain that every relationship complies fully with the Stark Law. In addition, in the July 2008 final Stark rule, CMS indicated that it will continue to enact further regulations tightening aspects of the Stark Law that it perceives allow for Medicare program abuse, especially those regulations that still permit physicians to profit from their referrals of ancillary services. There can be no assurance that the arrangements entered into by ApolloMed with physicians and facilities will be found to be in compliance with the Stark Law, as it ultimately may be implemented or interpreted.
Health Information Privacy and Security Standards
Among other directives, the Administrative Simplification Provisions of HIPAA required HHS to adopt standards to protect the privacy and security of certain health-related information. The HIPAA privacy regulations contain detailed requirements concerning the use and disclosure of individually identifiable health information by “HIPAA covered entities,” which include entities like ApolloMed, ApolloMed’s affiliated hospitalists, and practice groups.
In addition to the privacy requirements, HIPAA covered entities must implement certain administrative, physical, and technical security standards to protect the integrity, confidentiality and availability of certain electronic health information received, maintained, or transmitted. HIPAA also implemented the use of standard transaction code sets and standard identifiers that covered entities must use when submitting or receiving certain electronic healthcare transactions, including activities associated with the billing and collection of healthcare claims.
The American Recovery and Reinvestment Act enacted on February 18, 2009, included HITECH which modified the HIPAA legislation significantly. Pursuant to HITECH, certain provisions of the HIPAA privacy and security regulations become directly applicable to “HIPAA business associates”.
Violations of the HIPAA privacy and security standards may result in civil and criminal penalties. Historically, these included: (1) civil money penalties of $100 per incident, to a maximum of $25,000, per person, per year, per standard violated and (2) depending upon the nature of the violation, fines of up to $250,000 and imprisonment for up to ten years. The passage of HITECH significantly modified the enforcement structure, creating a tiered system of civil money penalties that range from $100 to $50,000 per violation, with a cap of $1.5 million per year for identical violations. ApolloMed must also comply with the “breach notification” regulations, which implement certain provisions of HITECH. Under these regulations, in addition to reasonable remediation, covered entities must promptly notify affected individuals in the case of a breach of “unsecured PHI,” which is defined by HHS guidance, as well as the Secretary of HHS and the media in cases where a breach affects more than 500 individuals. Breaches affecting fewer than 500 individuals must be reported to the HHS Secretary on an annual basis. The regulations also require business associates of covered entities to notify the covered entity of breaches at or by the business associate. Formal enforcement of the new breach notification regulations began on February 22, 2010.
| 244 |
ApolloMed expects increased federal and state HIPAA privacy and security enforcement efforts. Under HITECH, state Attorneys General now have the right to prosecute HIPAA violations committed against residents of their states. In addition, HITECH mandates that the Secretary of HHS conduct periodic compliance audits of HIPAA covered entities and business associates. It also tasks HHS with establishing a methodology whereby harmed individuals who were the victims of breaches of unsecured PHI may receive a percentage of the civil monetary penalty fine or monetary settlement paid by the violator. This methodology for compensation to harmed individuals was initially required to be in place by February 17, 2012; however, no rules or regulations implementing this methodology have yet been adopted by HHS. HHS may nonetheless eventually establish such methodology for compensation to harmed individuals.
Many states also have laws that protect the privacy and security of confidential, personal information. These laws may be similar to or even more stringent than the federal provisions. Not only may some of these state laws impose fines and penalties upon violators, but some may afford private rights of action to individuals who believe their personal information has been misused.
Fee-Splitting and Corporate Practice of Medicine
Some states, including California, have laws that prohibit business entities, such as ApolloMed and its subsidiaries, from practicing medicine, employing physicians to practice medicine, exercising control over medical decisions by physicians (also known collectively as the corporate practice of medicine) or engaging in certain arrangements, such as fee-splitting, with physicians. In these states, a violation of the corporate practice of medicine prohibition constitutes the unlawful practice of medicine, which is a public offense punishable by fines and other criminal penalties. In addition, any physician who participates in a scheme that violates the state’s corporate practice of medicine prohibition may be punished for aiding and abetting a lay entity in the unlawful practice of medicine. ApolloMed operates by maintaining long-term management contracts with affiliated professional organizations, which are each owned and operated by physicians and which employ or contract with additional physicians to provide hospitalist services. Under these arrangements, ApolloMed performs only non-medical administrative services, does not represent that ApolloMed offers medical services, and does not exercise influence or control over the practice of medicine by the physicians or the affiliated professional organizations. The California Medical Board, as well as other state’s regulatory bodies, has taken the position that certain physician practice management agreements that confer too much control over a physician practice violate the prohibition against corporate practice of medicine.
ApolloMed operates by maintaining long-term management contracts with affiliated professional organizations, which are each owned and operated by physicians and other individuals, and which employ or contract with additional physicians to provide clinical services. Under these arrangements, ApolloMed performs only non-medical administrative services, does not represent that ApolloMed offers medical services, and does not exercise influence or control over the practice of medicine by the physicians or the affiliated professional organizations.
For financial reporting purposes, however, ApolloMed consolidates the revenues and expenses of all its practice groups that it owns or manages because ApolloMed has a controlling financial interest in these practices based on applicable accounting rules and as described in ApolloMed’s consolidated financial statements. In states where fee-splitting is prohibited between physicians and non-physicians, the fees that ApolloMed receives through its management contracts have been established on a basis that ApolloMed believes complies with the applicable state laws.
| 245 |
Some of the relevant laws, regulations, and agency interpretations in the State of California and other states that have corporate practice prohibitions have been subject to limited judicial and regulatory interpretation. Moreover, state laws are subject to change and regulatory authorities and other parties, including ApolloMed’s affiliated physicians, may assert that, despite these arrangements, ApolloMed is engaged in the prohibited corporate practice of medicine or that ApolloMed’s arrangements constitute unlawful fee-splitting. If this occurred, ApolloMed could be subject to civil or criminal penalties, ApolloMed’s contracts could be found legally invalid and unenforceable (in whole or in part), or ApolloMed could be required to restructure its contractual arrangements. If ApolloMed were required to restructure its operating structures due to determination that a corporate practice of medicine violation existed, such a restructuring might include revisions of ApolloMed’s management services agreements, which might include a modification of the management fee, and/or establishing an alternative structure.
Deficit Reduction Act of 2005
Among other mandates, the DRA created a new Medicaid Integrity Program designed to enhance federal and state efforts to detect Medicaid fraud, waste and abuse. Additionally, section 6032 of the DRA requires entities that make or receive annual Medicaid payments of $5.0 million or more from any one state to provide their employees, contractors and agents with written policies and employee handbook materials on federal and state False Claims Acts and related statues. At this time, ApolloMed is not required to comply with section 6032 because ApolloMed receives less than $5.0 million in Medicaid payments annually from any one state. However, ApolloMed may likely be required to comply in the future as ApolloMed’s Medicaid billings increase.
Other Federal Healthcare Compliance Laws
ApolloMed is also subject to other federal healthcare laws.
In 1995, Congress amended the federal criminal statutes set forth in Title 18 of the United States Code by defining additional federal crimes that could have an impact on ApolloMed’s business, including “Health Care Fraud” and “False Statements Relating to Health Care Matters.” The Health Care Fraud provision prohibits any person from knowingly and willfully executing, or attempting to execute, a scheme to defraud any healthcare benefit program. As defined in this provision of Title 18, a “healthcare benefit program” can be either a government or private payor plan. Violation of this statute may be charged as a felony offense and may result in fines, imprisonment or both. The ACA amended section 1347 of Title 18 to provide that a person may be convicted under the Health Care Fraud provision even in the absence of proof that the person had actual knowledge of, or specific intent to violate, the statute.
The False Statements Relating to Health Care Matters provision prohibits, in any matter involving a federal health care program, anyone from knowingly and willfully falsifying, concealing or covering up, by any trick, scheme or device, a material fact, or making any materially false, fictitious or fraudulent statement or representation, or making or using any materially false writing or document knowing that it contains a materially false or fraudulent statement. A violation of this statute may be charged as a felony offense and may result in fines, imprisonment or both.
Under the Civil Monetary Penalties law of the Social Security Act, a person, including any individual or organization, may be subject to civil monetary penalties, treble damages and exclusion from participation in federal health care programs for certain specified conduct. One provision of the Civil Monetary Penalties law precludes any person (including an organization) from knowingly presenting or causing to be presented to any United States officer, employee, agent, or department, or any state agency, a claim for payment for medical or other items or services that the person knows or should know (a) were not provided as described in the coding of the claim, (b) is a false or fraudulent claim, (c) is for a service furnished by an unlicensed physician, (d) is for medical or other items or service furnished by a person or an entity that is in a period of exclusion from the program or (e) are medically unnecessary items or services. Violations of the law may result in penalties of up to $10,000 per claim, treble damages, and exclusion from federal healthcare programs. In addition, the OIG may impose civil monetary penalties against any physician who knowingly accepts payment from a hospital (as well as against the hospital making the payment) as an inducement to reduce or limit medically necessary services provided to Medicare or Medicaid program beneficiaries. Further, except as specifically permitted under the Civil Monetary Penalties law, a person who offers or transfers to a Medicare or Medicaid beneficiary any remuneration that the person knows or should know is likely to influence the beneficiary’s selection of a particular provider of Medicare or Medicaid payable items or services may be liable for civil money penalties of up to $10,000 for each wrongful act.
| 246 |
Other State Healthcare Compliance Provisions
In addition to the state laws previously described, ApolloMed may also be subject to other state fraud and abuse statutes and regulations if it expands its operations beyond California. Many states have adopted a form of anti-kickback law, self-referral prohibition, and false claims and insurance fraud prohibition. The scope of these laws and the interpretations of them vary from state to state and are enforced by state courts and regulatory authorities, each with broad discretion. Generally, state laws reach to all healthcare services and not just those covered under a governmental healthcare program. A determination of liability under any of these laws could result in fines and penalties and restrictions on ApolloMed’s ability to operate in these states. ApolloMed cannot assure that its arrangements or business practices will not be subject to government scrutiny or be found to violate applicable fraud and abuse laws.
Knox-Keene Act and Other State Insurance Laws
Some of the medical groups and IPAs that have entered into management services agreements with us, have historically contracted with health plans and other payors to receive a PMPM or percentage of premium capitation payment for professional (physician) services and assumed the financial responsibility for professional services. In many of these cases, the health plans or other payors separately enter into contracts with hospitals that directly receive payment (either a capitation or FFS payment) and assume some type of contractual financial responsibility for their institutional (hospital) services. In some instances, ApolloMed’s managed medical groups and IPAs have been paid by their contracting payor for the financial outcome of managing the care dollars associated with both the professional and institutional services received by the medical groups’ and IPAs’ members. In the case of institutional services, the medical groups and IPAs have recognized a percentage of the surplus of institutional revenues less institutional expense as the medical groups’ and IPAs’ net revenues and has also been responsible for some percentage of any short-fall in the event that institutional expenses exceed institutional revenues. Notwithstanding, neither ApolloMed nor any of its managed medical groups or IPAs are contractually obligated to pay claims to any hospitals or other institutions under these arrangements. The DMHC licenses and regulates health care service plans pursuant to the Knox-Keene Act. ApolloMed does not hold a limited Knox-Keene license. If DMHC were to determine that ApolloMed has been inappropriately taking risk for institutional and professional services as a result of ApolloMed’s various hospital and physician arrangements without having a limited Knox-Keene license, ApolloMed may be required to obtain a limited Knox-Keene license to resolve such violations and ApolloMed could be subject to civil and criminal liability, any of which could have a material adverse effect on its business, financial condition or results of operations.
Furthermore, some states require ACOs to be registered or otherwise comply with state insurance laws. ApolloMed’s affiliated ACO does not currently take financial risk, and is therefore not registered with any state insurance agency. If a state insurance agency were to determine that ApolloMed has been inappropriately operating an ACO without state registration or licensure, ApolloMed may be required to obtain such registration or licensure to resolve such violations and ApolloMed could be subject to liability, which could have a material adverse effect on ApolloMed’s business, financial condition or results of operations.
Licensing, Certification, Accreditation and Related Laws and Guidelines
ApolloMed’s clinical personnel are subject to numerous federal, state and local licensing laws and regulations, relating to, among other things, professional credentialing and professional ethics. Since ApolloMed performs services at hospitals and other types of healthcare facilities, it may indirectly be subject to laws applicable to those entities as well as ethical guidelines and operating standards of professional trade associations and private accreditation commissions, such as the American Medical Association and The Joint Commission. There are penalties for non-compliance with these laws and standards, including loss of professional license, civil or criminal fines and penalties, loss of hospital admitting privileges, and exclusion from participation in various governmental and other third-party healthcare programs. ApolloMed’s ability to operate profitably will depend, in part, upon its ability and the ability of ApolloMed’s affiliated physician organizations to obtain and maintain all necessary licenses and other approvals and operate in compliance with applicable health care laws and regulations, including any new laws and regulations or new interpretations of existing laws and regulations.
| 247 |
Professional Licensing Requirements
ApolloMed’s affiliated hospitalists must satisfy and maintain their individual professional licensing in each state where they practice medicine. Activities that qualify as professional misconduct under state law may subject them to sanctions, or to even lose their license and could, possibly, subject us to sanctions as well. Some state boards of medicine impose reciprocal discipline, that is, if a physician is disciplined for having committed professional misconduct in one state where he or she is licensed, another state where he or she is also licensed may impose the same discipline even though the conduct occurred in another state. Professional licensing sanctions may also result in exclusion from participation in governmental healthcare programs, such as Medicare and Medicaid, as well as other third-party programs. ApolloMed’s ability to operate profitably will depend, in part, upon its ability and the ability of its affiliated physician organizations to obtain and maintain all necessary licenses and other approvals and operate in compliance with applicable health care laws and regulations, including any new laws and regulations or new interpretations of existing laws and regulations.
Home Health and Hospice Regulation
ApolloMed has invested in business lines consisting of home health, hospice and palliative care, which require compliance with additional regulatory requirements. For example, ApolloMed must comply with laws relating to hospice care eligibility, the development and maintenance of plans of care, and the coordination of services with nursing homes or assisted living facilities where many of ApolloMed’s patients live. In addition, ApolloMed’s hospice programs are licensed as required under state law as either hospices or home health agencies.
The following is a discussion of the regulations that ApolloMed believes most significantly affect ApolloMed’s home health and hospice business.
Licensure, Certification, Accreditation and Related Laws and Guidelines
ApolloMed’s agencies and facilities are subject to state and local licensing regulations ranging from the adequacy of medical care, to compliance with building codes and environmental protection laws. To assure continued compliance with these various regulations, governmental and other authorities periodically inspect ApolloMed’s agencies and facilities. Additionally, ApolloMed’s clinical professionals are subject to numerous federal, state and local licensing laws and regulations, relating to, among other things, professional credentialing and professional ethics. Clinical professionals are also subject to state and federal regulation regarding prescribing medication and controlled substances. Each state defines the scope of practice of clinical professionals through legislation and through the respective Boards of Medicine and Nursing, and many states require that nurse practitioners and physician assistants work in collaboration with or under the supervision of a physician. There are penalties for noncompliance with these laws and standards, including the loss of professional license, civil or criminal fines and penalties, federal health care program disenrollment, loss of billing privileges, and exclusion from participation in various governmental and other third-party healthcare programs. ApolloMed operates its business to ensure that its employees and agents possess all necessary licenses and certifications.
Reimbursement for palliative care and house call services is generally conditioned on ApolloMed’s clinical professionals providing the correct procedure and diagnosis codes and properly documenting both the service itself and the medical necessity for the service. Incorrect or incomplete documentation and billing information, or the incorrect selection of codes for the level and type of service provided, could result in non-payment for services rendered or lead to allegations of billing fraud.
Medicare Participation
To participate in the Medicare program and receive Medicare payments, ApolloMed’s agencies and facilities must comply with regulations promulgated by CMS. Among other things, these requirements, known as the “Conditions of Participation” relate to the type of facility, its personnel, and its standards of medical care, as well as its compliance with state and local laws and regulations. The Conditions of Participation for hospice programs include, but may not be limited to regulation of the: Governing Body, Medical Director, Direct Provision of Core Services, Professional Management of Non-Core Services, Plan of Care, Continuation of Care, Informed Consent, Training, Quality Assurance, Interdisciplinary Team, Volunteers, Licensure, Central Clinical Records, Surveys and Audits, Billing Audits/ Claims Reviews, Certificate of Need Laws and Other Restrictions, Limitations on For-Profit Ownership, Limits on the Acquisition or Conversion of Non-Profit Health Care Organizations, and Professional Licensure.
| 248 |
To be eligible for Medicare payments for home health services, a patient must be “homebound” (cannot leave home without considerable or taxing effort), require periodic skilled nursing or physical or speech therapy services, and receive treatment under a plan of care established and periodically reviewed by a physician based upon a face-to-face encounter between the patient and the physician.
From time to time ApolloMed receives survey reports containing statements of deficiencies. ApolloMed reviews such reports and takes appropriate corrective action. If a hospice or home health agency were found to be out of compliance and actions were taken against that hospice or home health agency, this could materially adversely affect the entity’s ability to continue to operate, to provide certain services and to participate in the Medicare and Medicaid programs, which could materially adversely affect ApolloMed’s business operations.
Billing Audits/Claims Reviews. The Medicare program and its fiscal intermediaries and other payors periodically conduct pre-payment or post-payment reviews and other reviews and audits of health care claims, including hospice claims. There is pressure from state and federal governments and other payors to scrutinize health care claims to determine their validity and appropriateness. In order to conduct these reviews, the payor requests documentation from us and then reviews that documentation to determine compliance with applicable rules and regulations, including the eligibility of patients to receive hospice benefits, the appropriateness of the care provided to those patients and the documentation of that care. ApolloMed’s claims have been subject to review and audit. ApolloMed makes appropriate provisions in ApolloMed’s accounting records to reduce its revenue for anticipated denial of payment related to these audits and reviews. ApolloMed believes its hospice programs comply with all payor requirements at the time of billing. However, ApolloMed cannot predict whether future billing reviews or similar audits by payors will result in material denials or reductions in revenue.
Professional Licensure and Participation Agreements. Many hospice employees are subject to federal and state laws and regulations governing the ethics and practice of their profession, including physicians, physical, speech and occupational therapists, social workers, home health aides, pharmacists and nurses. In addition, those professionals who are eligible to participate in the Medicare, Medicaid or other federal health care programs as individuals must not have been excluded from participation in those programs at any time.
Environmental and Occupational Health
ApolloMed is subject to federal, state and local regulations governing the storage, use and disposal of materials and waste products. Although ApolloMed believes that its safety procedures for storing, handling and disposing of these hazardous materials comply with the standards prescribed by law and regulation, ApolloMed cannot completely eliminate the risk of accidental contamination or injury from those hazardous materials. In the event of an accident, ApolloMed could be held liable for any damages that result and any liability could exceed the limits or fall outside the coverage of ApolloMed’s insurance. ApolloMed may not be able to maintain insurance on acceptable terms, or at all. ApolloMed could incur significant costs and the diversion of ApolloMed’s management’s attention to comply with current or future environmental laws and regulations.
Federal regulations promulgated by the Occupational Safety and Health Administration impose additional requirements on us including those protecting employees from exposure to elements such as blood-borne pathogens. ApolloMed cannot predict the frequency of compliance, monitoring, or enforcement actions to which it may be subject as those regulations are implemented, and regulations might adversely affect ApolloMed’s operations.
As of June 30, 2017, ApolloMed and its affiliated clinics had 149 employees, of whom 115 were full-time and 34 were part-time, and approximately 80 were employed or independent contractor physicians. ApolloMed also had a broader physician network which, as of June 30, 2017, consisted of approximately 1,000 additional contracted physicians who provided services to ApolloMed. None of ApolloMed’s employees is a member of a labor union, and ApolloMed has never experienced a work stoppage. ApolloMed believes that it enjoys a good working relationship with its employees.
| 249 |
ApolloMed’s corporate headquarters are located at 700 North Brand Boulevard, Suite 1400, Glendale, California 91203. Under the original lease of the premises, ApolloMed occupied space in Suite 220. On October 14, 2014, ApolloMed’s lease was amended by a Second Amendment (the “Second Lease Amendment”), pursuant to which it relocated its corporate headquarters to a larger suite in the same office building in October 2015. The Second Lease Amendment relocates the leased premises from Suite No. 220 to Suite Nos. 1400, 1425 and 1450, which collectively include 16,484 rentable square feet (the “New Premises”). The New Premises were improved with an allowance of $659,360, provided by the landlord, for construction and installation of equipment for the New Premises. The Second Lease Amendment also extends the term of the lease to for approximately six years after ApolloMed occupies the New Premises and increases its security deposit. The Second Lease Amendment sets the New Premises base rent at $37,913 per month for the first year and schedules annual increases in base rent each year until the final rental year, which is capped at $43,957 per month. However, the base rent will be abated by up to $228,049 subject to other terms of the lease.
AMM leases the SCHC premises located in Los Angeles, California, consisting of 8,766 rentable square feet, for a term of 10 years. The base rent for the SCHC lease is approximately $33,000 per month.
In the ordinary course of its business, ApolloMed becomes involved in pending and threatened legal actions and proceedings, most of which involve claims of medical malpractice related to medical services that are provided by ApolloMed’s affiliated hospitalists. ApolloMed may also become subject to other lawsuits which could involve significant claims and/or significant defense costs.
As of September 30, 2017, ApolloMed is not involved in any pending or threatened legal actions or proceedings.
Management’s Discussion and Analysis of Financial Condition and Results of Operations.
You should read the following discussion and analysis of ApolloMed’s financial condition and results of operations together with “Selected historical consolidated financial information” and ApolloMed’s consolidated financial statements and related notes appearing elsewhere in this joint proxy statement/prospectus and in the documents incorporated by reference in this joint proxy statement/prospectus. This discussion and analysis contains forward-looking statements that involve risks, uncertainties and assumptions. The actual results may differ materially from those anticipated in these forward-looking statements as a result of certain factors, including, but not limited to, those set forth under “Risk Factors” and elsewhere in this joint proxy statement/prospectus.
Overview
ApolloMed is a physician-centric, integrated population health management company working to provide coordinated outcomes-based medical care in a cost-effective manner. Led by a management team with over a decade of experience, ApolloMed has built a company and culture that is focused on physicians providing high-quality medical care, population health management and care coordination for patients, particularly senior patients and patients with multiple chronic conditions. ApolloMed believes it is well-positioned to take advantage of changes in the rapidly evolving U.S. healthcare industry, as there is a growing national movement towards more results-oriented healthcare centered on the triple aim of patient satisfaction, high-quality care and cost efficiency.
ApolloMed implements and operates innovative health care models to create a patient-centered, physician-centric experience. ApolloMed has the following integrated, synergistic operations:
| · | Hospitalists, which includes ApolloMed’s contracted physicians who focus on the delivery of comprehensive medical care to hospitalized patients; |
| 250 |
| · | An MSSP ACO, which focuses on providing high-quality and cost-efficient care to Medicare FFS patients; |
| · | A NGACO, which started operations on January 1, 2017, and focuses on providing high-quality and cost-efficient care for Medicare FFS patients; |
| · | An IPA, which contracts with physicians and provides care to Medicare, Medicaid, commercial and dual-eligible patients on a risk- and value-based fee basis; |
| · | One clinic which ApolloMed owns, and which provides specialty care in the greater Los Angeles area; |
| · | Hospice care, palliative care, and home health services, which include ApolloMed’s at-home and end-of-life services; and |
| · | A cloud-based population health management IT platform, which was acquired in January 2016, and includes digital care plans, a case management module, connectivity with multiple healthcare tracking devices and also integrates clinical data. |
ApolloMed operates in one reportable segment, the healthcare delivery segment. ApolloMed’s revenue streams, which are described in greater detail below in “ApolloMed’s Revenue Streams and ApolloMed’s Business Operations”, are diversified among ApolloMed’s various operations and contract types, and include:
| · | Traditional FFS reimbursement; and |
| · | Risk and value-based contracts with health plans, third party IPAs, hospitals and the NGACO and MSSP sponsored by CMS, which are the primary revenue sources for ApolloMed’s hospitalists, ACOs, IPAs and hospice/palliative care operations. |
ApolloMed serves Medicare, Medicaid, HMO and uninsured patients in California. ApolloMed provides services to patients, the majority of whom are covered by private or public insurance, with a small portion of ApolloMed’s revenue coming from non-insured patients. ApolloMed provides care coordination services to each major constituent of the healthcare delivery system, including patients, families, primary care physicians, specialists, acute care hospitals, alternative sites of inpatient care, physician groups and health plans.
ApolloMed’s mission is to transform the delivery of healthcare services in the communities it serves by implementing innovative population health models and creating a patient-centered, physician-centric experience in a high performance environment of integrated care.
The initial business owned by ApolloMed is AMH, a hospitalist company, incorporated in California in June, 2001 and began operations at Glendale Memorial Hospital. Through a reverse merger, ApolloMed became a publicly held company in June 2008. ApolloMed was initially organized around the admission and care of patients at inpatient facilities such as hospitals. ApolloMed has grown its inpatient strategy in a competitive market by providing high-quality care and innovative solutions for ApolloMed’s hospital and managed care clients. In 2012, it formed an ACO, ApolloMed ACO, and an IPA, MMG, and in 2013 it expanded ApolloMed’s service offering to include integrated inpatient and outpatient. In 2014, ApolloMed added several complementary operations by acquiring an IPA, outpatient primary care and specialty clinics, as well as hospice/palliative care and home health entities. In 2016, ApolloMed formed APAACO, to participate in the NGACO Model, for which it was approved by CMS in January 2017.
| 251 |
ApolloMed’s physician network consists of hospitalists, primary care physicians and specialist physicians primarily through ApolloMed’s owned and affiliated physician groups. It operates through the following subsidiaries: AMM, PCCM, VMM and ApolloMed ACO. Through ApolloMed’s wholly-owned subsidiary, AMM, it manages affiliated medical groups, which consist of AMH, MMG, SCHC, and BAHA. Through ApolloMed’s wholly-owned subsidiary, PCCM, it manages LALC, and through ApolloMed’s wholly-owned subsidiary VMM, it manages Hendel. ApolloMed also has a controlling interest in APS, which owns two Los Angeles-based companies, Best Choice Hospice Care LLC and Holistic Health Home Health Care Inc. AMM, PCCM and VMM each operate as a physician practice management company and are in the business of providing management services to physician practice corporations under long-term management service agreements. ApolloMed’s ACO participates in the MSSP, the goal of which is to improve the quality of patient care and outcomes through more efficient and coordinated approach among providers. Revenues earned by ApolloMed ACO are uncertain, and, if such amounts are payable, they will be paid on an annual basis significantly after the time earned, and will be contingent on various factors, including achievement of the minimum savings rate as determined by MSSP for the relevant period.
Highlights
The following describes certain developments in fiscal 2017 to date that are important to understanding ApolloMed’s overall results of operations and financial condition.
Operations and Financings
ApolloMed achieved approximately 30% growth in net revenues from fiscal 2016, almost entirely from ApolloMed’s hospitalist operations. ApolloMed employed locum tenens to full-fill the contracts in the initial phase which increased ApolloMed’s cost of sale substantially. Notwithstanding that growth, ApolloMed’s net loss increased by approximately 6% during the same period.
On November 4, 2016, ApolloMed acquired BAHA, through an affiliate wholly-owned by Dr. Hosseinion, as nominee shareholder on ApolloMed’s behalf. BAHA was managed by ApolloMed under long-term MSA since February 17, 2015 and the results were consolidated in ApolloMed’s financial statements as under VIE accounting. As of the date of acquisition, it obtained a controlling interest in BAHA.
On January 18, 2017, CMS announced that APAACO has been approved to participate in the new NGACO Model. Through the NGACO Model, CMS has partnered with APAACO and other ACOs experienced in coordinating care for populations of patients and whose provider groups are willing to assume higher levels of financial risk and reward under the NGACO Model. The NGACO program began on January 1, 2017. To position ApolloMed to participate in the NGACO Model, ApolloMed has devoted, and intends to continue to devote, significant effort and resources, financial and otherwise, to the NGACO Model, and refocused away from certain other parts of ApolloMed’s historic business and revenue streams, which will receive less emphasis in the future and could result in reduced revenue from these activities. ApolloMed currently anticipates that revenue from the NGACO Model will be a significant source of revenue for it in fiscal 2018 and future periods, although no assurance of that can be given at this time.
During fiscal 2017, ApolloMed raised an aggregate $10.39 million, which consists of a $5.0 million loan received from NMM, a $4.99 million loan received from Alliance and a $0.4 million loan received from an individual, the last mentioned of which was repaid in accordance with its terms.
| 252 |
Results of Operations
Year Ended March 31, 2017 Compared to Year Ended March 31, 2016
The following sets forth selected data from of ApolloMed’s results of operations for the years presented:
| For the Year Ended | ||||||||||||||||
| March 31, | ||||||||||||||||
| $ | % | |||||||||||||||
| 2017 | 2016 | Change | Change | |||||||||||||
| Net revenues | 57,427,701 | 44,048,740 | 13,378,961 | 30 | % | |||||||||||
| Costs and expenses | ||||||||||||||||
| Cost of services | 48,735,537 | 34,000,786 | 14,734,751 | 43 | % | |||||||||||
| General and administrative | 18,583,372 | 16,962,687 | 1,620,685 | 10 | % | |||||||||||
| Depreciation and amortization | 645,742 | 351,396 | 294,346 | 84 | % | |||||||||||
| Total costs and expenses | 67,964,651 | 51,314,869 | 16,649,782 | 32 | % | |||||||||||
| Loss from operations | (10,536,950 | ) | (7,266,129 | ) | (3,270,821 | ) | 45 | % | ||||||||
| Other (expense) income: | ||||||||||||||||
| Interest expense | (82,905 | ) | (542,296 | ) | 451391 | -85 | % | |||||||||
| Gain (loss) on change in fair value of warrant and conversion feature liabilities | 1,633,333 | (408,692 | ) | 2,042,025 | -500 | % | ||||||||||
| Gain on deconsolidation of variable interest entity | 242,411 | - | 242,411 | 100 | % | |||||||||||
| Loss on debt extinguishment | - | (266,366 | ) | 266,366 | -100 | % | ||||||||||
| Other income | 14,701 | 239,057 | (224,356 | ) | -94 | % | ||||||||||
| Total other income (expense), net | 1,807,540 | (978,297 | ) | 2,785,837 | -285 | % | ||||||||||
| Loss before benefit from income taxes | (8,729,410 | ) | (8,244,426 | ) | (484,984 | ) | 6 | % | ||||||||
| Benefit from income taxes | (47,495 | ) | (71,037 | ) | 23,542 | -33 | % | |||||||||
| Net loss | (8,681,915 | ) | (8,173,389 | ) | (508,526 | ) | 6 | % | ||||||||
| Net income attributable to noncontrolling interest | 287,901 | 1,170,655 | (882,754 | ) | -75 | % | ||||||||||
| Net loss attributable to Apollo Medical Holdings, Inc. | $ | (8,969,816 | ) | $ | (9,344,044 | ) | $ | 374,228 | -4 | % | ||||||
Net revenues
Net revenues for the year ended March 31, 2017 increased by approximately $13.4 million, from $44.0 million to $57.4 million, or 30%, as compared to the same period of 2016. The increase in net revenues was primarily due to an increase of $12.2 million from AMH and BAHA as a result of new hospitalist contracts, an increase of $4.3 million in MMG revenues due to the growth in capitated membership and increase in full risk surplus in 2017 from a deficit in 2016 that was driven by a decrease in hospital admits and utilization, and increase in memberships and an increase in $0.1 million in Apollo Care Connect revenue. The increases were partially offset by the decrease of $2.1 million from BCHC and HCHHA due to lower patient census, a decrease of $1.1 million from LALC and Hendel due to deconsolidation during the fourth quarter of fiscal 2017 and lower patient visits.
| 253 |
Cost of services
Cost of services for the year ended March 31, 2017 increased by approximately $14.7 million, from $34.0 million to $48.7 million, or 43%, as compared to the same period of 2016. The increase was primarily due to a $14.4 million increase in AMH and BAHA cost of services that was primarily related to the new hospitalist contracts that started in 2016 and use of contract labor, a $2.8 million increase in MMG due to increases in the PCP capitation and SPC capitation due to increase in membership, increase in claims offset by increases in claims recovery due to high claims eligible for stop loss. Such increases were partially offset by the decrease of $1.0 million from BCHC and HCHHA due to lower patient census, a $0.6 million decrease in SCHC as a result of favorable margins in the current year as compared to the same period of the prior year, decrease of $0.6 million in ACC due to the sale of substantially all its assets during the 2016 fiscal year and related cessation in operations, decrease of $0.3 million in LALC and Hendel due to deconsolidation during the fourth quarter of fiscal 2017.
General and administrative
General and administrative costs for the year ended March 31, 2017 increased by approximately $1.6 million, from $17.0 million to $18.6 million, or 10%, as compared to the same period of 2016. There was an approximate $2.7 million increase relating to AMM from the increase in overheads to manage 30% increase in revenue and merger related cost incurred in fiscal 2017, a $1.1 million increase from SCHC due to increase in operating costs, a $0.9 million increase from AMH and BAHA from the increase in overheads to manage $12.2 million increase in revenue compared to same period in fiscal 2016, $0.4 million increase from Apollo Care Connect due to new operations, which is attributable to the increase in revenues in the current year. The increases were partially offset by a decrease of $1.9 million from MMG as a result of a decrease in payroll and related expenses and management fees, $0.5 million from ACC as a result of a cessation in operations, a decrease of $0.4 million from BCHC and HCHHA due to operational restructure and decreases in revenue, a decrease of $0.3 million from ACO expenses, and a decrease of $0.3 million from LALC and Hendel as a result of the deconsolidation in the fourth quarter of fiscal 2017.
Depreciation and amortization
Depreciation and amortization expense for the year ended March 31, 2017, increased by approximately $0.3 million, from $0.3 million to $0.6 million, or 84%, as compared to the same period of 2016. This increase was primarily due to an increase in depreciation and amortization expense related to the amortization of intangible assets of Apollo Care Connect.
Interest expense
Interest expense for the year ended March 31, 2017, decreased by approximately $0.4 million, from $0.5 million to $0.1 million, or 85%, as compared to the same period of 2016. This decrease was primarily due to the prior year amortization expense of the debt discount as a result of the out of period correction adjustment to properly state ApolloMed’s warrant liability, unamortized debt discount and deferred financing costs that did not occur in the current year.
Gain (loss) on change in fair value of warrant and conversion feature liabilities
The net change in fair value of warrant and conversion feature liabilities for the year ended March 31, 2017, changed by approximately $2.0 million, from a loss of $0.4 million to a gain of $1.6 million, or 500%, as compared to the same period of 2016. This gain resulted from the change in the fair value measurement of ApolloMed’s warrant, which considers, among other things, expected term, the volatility of ApolloMed’s share price, interest rates, associated with the conversion feature of the Series A warrant issued to NMM.
Gain on deconsolidation of VIE
For the year ended March 31, 2017, ApolloMed recorded a gain on deconsolidation of VIE of $0.2 million due to the deconsolidation of LALC and Hendel during the fourth quarter of fiscal 2017.
Loss on Extinguishment of Debt, Net
For the year ended March 31, 2016, ApolloMed incurred a loss on debt extinguishment of $0.3 million in connection with the repayment of NNA debt and conversion of ApolloMed’s then outstanding debt to NNA into shares of ApolloMed’s common stock.
| 254 |
Other income
For the year ended March 31, 2017, the net other income decreased by $0.2 million to $14,701 as a result of the reduction in provider incentives from the health plan.
Benefit from income taxes
For the year ended March 31, 2017, income tax benefit of approximately $0.1 million remained consistent with the prior year.
Net income attributable to noncontrolling interests
For the year ended March 31, 2017, net income attributable to noncontrolling interest decreased by $0.9 million from $1.2 million to $0.3 million, primarily due to the deconsolidation of LALC and Hendel during the fourth quarter of fiscal 2017 and acquisition of the noncontrolling interest in BAHA in November 2016, the results of BAHA are since considered as controlling interest.
Net loss
As a result of the foregoing factors, ApolloMed incurred a net loss for the year ended March 31, 2017 of approximately $8.7 million compared to a net loss of approximately $8.2 million for the year ended March 31, 2016, an increase in net loss of approximately $0.5 million or 6%. Net loss per share was $1.49 for the year ended March 31, 2017 compared to a net loss per share of $1.79 for the year ended March 31, 2016, a decrease in net loss per share of $0.30.
Results of Operations
The results of operations for the three months ended June 30, 2017 reflected a significant financial impact from our investments in population health management infrastructure and value-based care processes for our patients.
The following sets forth selected data from our unaudited results of operations for the periods presented:
| For the Three Months Ended | ||||||||||||||||
| June 30, | ||||||||||||||||
| $ | % | |||||||||||||||
| 2017 | 2016 | Change | Change | |||||||||||||
| Net revenues | $ | 41,575,480 | $ | 12,371,673 | $ | 29,203,807 | 236 | % | ||||||||
| Costs and expenses | ||||||||||||||||
| Cost of services | 40,239,642 | 10,133,005 | 30,106,637 | 297 | % | |||||||||||
| General and administrative | 4,889,184 | 3,836,475 | 1,052,709 | 27 | % | |||||||||||
| Depreciation and amortization | 155,267 | 164,658 | (9,391 | ) | -6 | % | ||||||||||
| Total costs and expenses | 45,284,093 | 14,134,138 | 31,149,955 | 220 | % | |||||||||||
| Loss from operations | (3,708,613 | ) | (1,762,465 | ) | (1,946,148 | ) | 110 | % | ||||||||
| Other (expense) income: | ||||||||||||||||
| Interest expense | (192,989 | ) | (2,659 | ) | (195,557 | ) | 7,158 | % | ||||||||
| Gain on change in fair value of warrant liability | - | 822,222 | (822,222 | ) | -100 | % | ||||||||||
| Other income | 38,657 | 1,971 | 36,686 | 1,861 | % | |||||||||||
| Total other income (expense), net | (154,332 | ) | 821,534 | (975,866 | ) | -119 | % | |||||||||
| Loss before benefit from income taxes | (3,862,945 | ) | (940,931 | ) | (2,922,014 | ) | 311 | % | ||||||||
| Benefit from income taxes | (29,891 | ) | (41,553 | ) | 11,662 | -28 | % | |||||||||
| Net loss | $ | (3,833,054 | ) | $ | (899,378 | ) | $ | (2,933,676 | ) | 326 | % | |||||
| Net loss (income) attributable to non-controlling interest | 221,242 | (415,879 | ) | 637,121 | -153 | % | ||||||||||
| Net loss attributable to Apollo Medical Holdings, Inc. | $ | (3,611,812 | ) | $ | (1,315,257 | ) | $ | (2,296,555 | ) | 175 | % | |||||
Three Months Ended June 30, 2017 Compared to Three Months Ended June 30, 2016
Net revenues
Net revenues for the three months ended June 30, 2017 increased by approximately $29.2 million, or 236%, as compared to the same period of 2016. The increase in net revenues was primarily due to an increase of approximately $27.9 million in APAACO’s revenues resulting from the new NGACO contract with CMS, pursuant to which we started to receive capitation from CMS in this quarter, an increase of approximately $2.5 million in AMH’s revenues and an increase of $0.3 million in BAHA’s revenues, both of which resulted from the new hospitalist contracts that started in the second quarter of fiscal year 2017, and an increase of $0.1 million in SCHC’s revenues related to increased patient visits. These increases were offset by a decrease of $0.2 million in MMG’s revenues, which resulted from deficit in the full risk contracts related to high patient care cost, a decrease of $0.6 million in BCHC’s revenues due to decreased patient census, a decrease of $0.2 million in HCHHA’s revenues due to decreased patient census, as well as a decrease of $0.6 million in revenues of LALC and Hendel due to deconsolidation of the two variable interest entities (“VIEs”) from ApolloMed in the fourth quarter of fiscal year 2017. If ApolloMed is not successful, it expects to have a decrease in net revenues.
Cost of services
Cost of services for the three months ended June 30, 2017 increased by approximately $30.1 million, or 297%, as compared to the same period of 2016. The increase in cost of services was primarily related to an increase of approximately $27.3 million in APAACO expenses related to the patient care, an increase of approximately $2.4 million in AMH’s expenses related to the new hospitalist contracts that increased AMH’s revenues, an increase of approximately $1.2 million in BAHA’s expenses related to its new hospitalist contract and the use of locum providers, and an increase of approximately $0.2 million in MMG’s expenses due to increased costs in patient care. These increases in expenses were offset by a decrease of approximately $0.3 million and a decrease of $0.2 million in BCHC’s expenses and HCHHA’s expenses, respectively, both of which were due to reduction in patient census, as well as a decrease of approximately $0.1 million in each of LALC’s expenses and Hendel’s expenses, respectively, both of which were due to deconsolidation of the two VIEs from us in the fourth quarter of fiscal year 2017 and a decrease of $0.3 million in SCHC’s expenses. If ApolloMed is not successful, it expects to have a decrease in cost of services.
General and administrative
General and administrative (G&A) costs for the three months ended June 30, 2017 increased by approximately $1.1 million, or 27%, as compared to the same period of 2016. Approximately $0.9 million of the increase was due to APAACO’s new NGACO operations, approximately $0.7 million of the increase was related to costs associated with the proposed Merger with NMM, and approximately $0.1 million of the increase correlated to an increase in BAHA’s G&A costs. The increases in our G&A costs were offset by a decrease of approximately $0.4 million in ACO’s G&A costs as the MMSP ACO operations have been gradually merged into the NGACO program, a decrease of approximately $0.1 million in MMG’s G&A costs, and a decrease of approximately $0.1 million in Hendel’s G&A costs due to its deconsolidation from us in the fourth quarter of fiscal year 2017.
Depreciation and amortization
Depreciation and amortization were comparable to the same period of 2016.
Interest expense
Interest expense increased by approximately $0.2 million, or 7,258%, as compared to the same period of 2016. The increase in interest expense is due to the addition of the $5,000,000 NMM Note and $4,990,000 Alliance Note. See Note 7 to the accompanying condensed consolidated financial statements for additional information.
Gain on change in fair value of warrant liability
There was a gain on the change in fair value of the warrant liability of approximately $0.8 million for the three months ended June 30, 2016. This gain resulted from the change in the fair value measurement of ApolloMed’s warrants issued to NMM in October 2015, which consider among other things, expected term, the volatility of ApolloMed’s share price, interest rates, and the probability of additional financing. As there was no warrant liability at either March 31, 2017 or June 30, 2017, there is no change in the fair value of warrant liability for the three months ended June 30, 2017.
Other income
Other income increased by approximately $37,000, or 1,861%, as compared to the same period of 2016. The increase in other income is due to interest from the cash held by APAACO.
Income tax provision (benefit)
Benefit from income taxes was consistent with the same period of the prior year.
Net (loss) income attributable to non-controlling interests
Net (loss) income attributable to non-controlling interests decreased by approximately $0.6 million, or 153%, as compared to the same period of 2016, which resulted from the deconsolidation of LALC and Hendel from ApolloMed in the fourth quarter of fiscal year 2017.
Liquidity and Capital Resources
The accompanying condensed consolidated financial statements have been prepared assuming that ApolloMed will continue as a going concern, which contemplates the realization of assets and settlement of liabilities in the normal course of business.
ApolloMed has a history of operating losses. For the three months ended June 30, 2017 and 2016, ApolloMed had a net loss of approximately $3.8 million and $0.9 million, respectively. ApolloMed generated positive cash flow from operations of approximately $22.6 million for the three months ended June 30, 2017 and used cash in operating activities of approximately $2.3 million for the three months ended June 30, 2016. The positive cash flow for the three months ended June 30, 2017 and the increase in the cash as of June 30, 2017 was primarily derived from APAACO’s new NGACO contract with CMS. All or most of these amounts will be used to pay the corresponding fee for service claims liability in future months. ApolloMed does not expect to have positive cash flow from operations for the remainder of fiscal year 2018. Cash flows used in investing activities for the three months ended June 30, 2017 and 2016, were approximately $36,000 and $163,000, respectively. Cash flows used in financing activities for the three months ended June 30, 2017 and 2016 were approximately $38,000 and $330,000, respectively.
As of June 30, 2017, ApolloMed has a net working capital deficit of approximately $3.1 million and an accumulated deficit of approximately $41.3 million, net borrowings from notes and lines of credit totaling approximately $9.9 million and availability under lines of credit of approximately $0.2 million.
| 255 |
These factors among others raise substantial doubt about ApolloMed’s ability to continue as a going concern. ApolloMed’s long-term ability to continue as a going concern is dependent upon ApolloMed’s ability to increase revenue, reduce costs, achieve a satisfactory level of profitable operations, and obtain additional sources of suitable and adequate financing.
ApolloMed’s ability to continue as a going concern is also dependent our ability to further develop its business. ApolloMed may also have to reduce certain overhead costs through the reduction of salaries and other means, and settle liabilities through negotiation. There can be no assurance that management’s plan and attempts at any or all of these endeavors will be successful.
In addition, ApolloMed’s ability to continue as a going concern depends, in significant part, on its ability to obtain the necessary financing to meet ApolloMed’s obligations and pay its obligations arising from normal business operations as they come due. To date, ApolloMed has funded its operations from a combination of internally generated cash flow and external sources, including the proceeds from the issuance of equity and/or debt securities. ApolloMed expects to continue to fund ApolloMed’s working capital requirements, capital expenditures and payments of principal and interest on outstanding indebtedness, with cash on hand, cash flows from operations, available borrowings under ApolloMed’s lines of credit and, if available, additional financings of equity and/or debt by our current investors and/or others. Management does not believe that ApolloMed has sufficient liquidity to meet its obligations for at least the next twelve months without some additional funds, such as funds available from raising capital. However, no assurance can be given that any such funds will be available at all or available on favorable terms.
ApolloMed therefore, is substantially dependent upon the consummation of the Merger to meet ApolloMed’s liquidity requirements. Until ApolloMed can generate sufficient positive cash flow to fund operations, ApolloMed will remain dependent on raising additional capital through debt and/or equity transactions. Without limiting ApolloMed’s available options, future equity financings will most likely be through the sale of debt and/or equity securities. It is possible that ApolloMed would also offer warrants, options and/or rights in conjunction with any future sales of its securities. Management believes that ApolloMed will be able to raise additional working capital through the issuance of stock and/or debt. Currently, however, ApolloMed does not have any commitments for the proposed Merger or additional capital, nor can ApolloMed provide assurance that any financing will be available to it on favorable terms, or at all. If, after utilizing the existing sources of capital available to ApolloMed, further capital needs are identified and ApolloMed is not successful in obtaining financing, ApolloMed may be forced to curtail its existing or planned future operations.
For the three months ended June 30, 2017, cash provided by operating activities was approximately $22.6 million. This was the result of a change in working capital of $26.0 million due to increases in accounts payable, accrued expenses, medical liabilities and add-backs of non-cash items of $0.4 million, offset by a net loss of $3.8 million. For the three months ended June 30, 2017, ApolloMed’s non-cash expenses primarily included provision for doubtful accounts, net of recoveries, depreciation and amortization expense, stock-based compensation expense, and amortization of debt issuance costs.
For the three months ended June 30, 2017, cash used in investing activities was approximately $36,000 related to purchases of fixed assets.
For the three months ended June 30, 2017, net cash used in financing activities was $38,000, which relates to principal payments of approximately $38,000 on the line of credit.
The unaudited condensed consolidated financial statements do not include any adjustments relating to the recoverability and classification of recorded assets, or the amounts and classification of liabilities that might be necessary in the event that ApolloMed cannot continue as a going concern.
Deconsolidation of VIE
On January 1, 2017, PCCM and VMM amended the MSAs entered into with LALC and Hendel respectively. Based on ApolloMed’s evaluation of current accounting guidance, it was determined that ApolloMed no longer holds an explicit or implicit variable interest in these entities. ApolloMed has consolidated the results of these entities through December 31, 2016. In connection with the amendments, ApolloMed recorded a gain on deconsolidation of $242,411, in the consolidated statement of operations, the deconsolidation of the net assets of the LALC and Hendel entities and related noncontrolling interest of $1,023,183 in the consolidated balance sheet, and a decrease in cash and cash equivalents and in the consolidated statements of cash flows in the amount of $858,670.
| 256 |
NNA Financing
On March 28, 2014, ApolloMed entered into the Credit Agreement pursuant to which NNA, an affiliate of Fresenius, extended to ApolloMed (i) a $1,000,000 revolving line of credit (the “Revolving Loan”) and (ii) a $7,000,000 term loan (the “Term Loan”). ApolloMed drew down the full amount of the Revolving Loan on October 23, 2014. The Term Loan and Revolving Loan were to mature on March 28, 2019, subject to NNA’s right to accelerate payment on the occurrence of certain events. The Term Loan could have been prepaid at any time without penalty or premium. The loans extended under the Credit Agreement were secured by substantially all of ApolloMed’s assets, and were guaranteed by ApolloMed’s subsidiaries and consolidated entities. The guarantees of these subsidiaries and consolidated entities were in turn secured by substantially all of the assets of the subsidiaries and consolidated entities providing the guaranty. Any entity that subsequently became a subsidiary or consolidated entity would have been required to provide a similar guaranty secured by substantially all of its assets and to comply with all of the other applicable requirements in the Credit Agreement and NNA Convertible Note (as defined below).
Concurrently with the Credit Agreement, ApolloMed entered into an Investment Agreement with NNA (the “Investment Agreement”), pursuant to which it issued to NNA a Convertible Note in the original principal amount of $2,000,000 (the “NNA Convertible Note”). ApolloMed drew down the full principal amount of the NNA Convertible Note on July 30, 2014. The NNA Convertible Note was to mature on March 28, 2019, subject to NNA’s right to accelerate payment on the occurrence of certain events. ApolloMed was able to redeem amounts outstanding under the NNA Convertible Note on 60 days’ prior notice to NNA. Amounts outstanding under the NNA Convertible Note were convertible at NNA’s sole election into shares of ApolloMed’s common stock at an initial conversion price of $10.00 per share. ApolloMed’s obligations under the NNA Convertible Note were guaranteed by ApolloMed’s subsidiaries and consolidated entities (including any subsidiaries or consolidated entities that are acquired or formed in the future).
On February 6, 2015, ApolloMed entered into a First Amendment and Acknowledgement (the “Acknowledgement”) with NNA, Warren Hosseinion, M.D., and Adrian Vazquez, M.D. The Acknowledgement amended some provisions of, and/or provided waivers in connection with, each of (i) the Registration Rights Agreement between ApolloMed and NNA, dated March 28, 2014 (the “Registration Rights Agreement”), (ii) the Investment Agreement, (iii) the NNA Convertible Note, and (iv) the NNA Warrants. The amendments to the Registration Rights Agreement included amendments with respect to the timing of the filing deadline for a resale registration statement for the benefit of NNA.
On May 13, 2015, ApolloMed entered into an Amendment to First Amendment and Acknowledgement (the “Amendment”) with NNA. The Amendment amended the Acknowledgement among ApolloMed, NNA, Warren Hosseinion, M.D., and Adrian Vazquez, M.D. and included an extension until June 12, 2015 of a deadline previously contemplated by the Acknowledgement for ApolloMed to file a registration statement covering the sale of NNA’s registrable securities.
On July 7, 2015, ApolloMed entered into an Amendment to First Amendment and Acknowledgement (the “New Amendment”) with NNA. The New Amendment amended the Acknowledgement, as amended by the Amendment, among ApolloMed, NNA, Warren Hosseinion, M.D., and Adrian Vazquez, M.D. and included an extension until October 15, 2015 of a deadline previously contemplated by the Acknowledgement for ApolloMed to file a registration statement covering the sale of NNA’s registrable securities. If the registration statement is not filed with the SEC on or prior to the filing deadline, ApolloMed must pay to NNA an amount in common stock based upon its then fair market value, as liquidated damages equal to 1.50% of the aggregate purchase price paid by NNA.
On August 18, 2015, ApolloMed entered into a Waiver and Consent (the “Waiver”) with NNA, whereby NNA waived and consented to certain provisions of the Credit Agreement and the Convertible Note. Under the terms of the Waiver, NNA (i) agreed to treat BAHA as an “Immaterial Subsidiary” until October 15, 2015 such that until such date BAHA is not subject to most of the requirements of the Credit Agreement and Convertible Note, including the financial covenants contained therein; (ii) waived events of default which have occurred under the Credit Agreement and Convertible Note as a result of payments made by ApolloMed to Adrian Vazquez, M.D. and Warren Hosseinion, M.D. in fiscal years 2014 and 2015, which were not permitted under the Credit Agreement or the Convertible Note; (iii) waived an event of default which occurred under the Credit Agreement and Convertible Note as a result of ApolloMed’s failure to satisfy a consolidated net worth covenant for the fiscal quarter ended June 2015; and (iv) waived an event of default which occurred under the Credit Agreement and Convertible Note as a result of an outstanding principal balance under an Intercompany Loan Agreement which exceeded the permitted amount by $213,276, with such waiver granted by NNA until October 15, 2015 and subject to a maximum excess loan balance of $250,000 during such time.
| 257 |
Under the Investment Agreement, ApolloMed issued to NNA the NNA Warrants.
The Credit Agreement, Investment Agreement and NNA Convertible Note contained various representations, warranties and covenants that ApolloMed made, including the following:
· ApolloMed and its subsidiaries and consolidated entities were prohibited from acquiring another entity or business with a purchase price greater than $500,000 without NNA’s prior consent;
· ApolloMed and its subsidiaries and consolidated entities were prohibited from creating or acquiring new subsidiaries without NNA’s prior approval. It was further prohibited from creating or acquiring any subsidiary that is not wholly-owned by ApolloMed or one of ApolloMed’s subsidiaries;
· ApolloMed was required to meet certain financial covenants as to consolidated EBITDA, leverage ratio, fixed charge coverage ratio and consolidated tangible net worth (in the case of consolidated tangible net worth, adding back certain goodwill and intangible assets of some of ApolloMed’s acquisitions). In particular, it was required (i) to maintain a consolidated tangible net worth of no less than $(3,700,000) as of March 31, 2015, June 30, 2015 and September 30, 2015, respectively, and a consolidated tangible net worth of no less than $0 as of December 31, 2015, and (ii) to have consolidated EBITDA of not less than $1,000,000 and a fixed charge coverage ratio of not less than 1.25 to 1.0, in each case as of September 30, 2015;
· ApolloMed was prohibited from being acquired by merger or consolidation without NNA’s prior consent. With certain exceptions, neither it nor any of ApolloMed’s subsidiaries or consolidated entities was permitted to sell or dispose of any assets;
· With certain exceptions, neither it nor any of ApolloMed’s subsidiaries or consolidated entities were permitted to incur any indebtedness or permit any liens to be placed on their properties without NNA’s prior consent;
· With certain exceptions, neither it nor any of ApolloMed’s subsidiaries or consolidated entities were permitted to make any dividends or distributions or repurchase shares of its capital stock without NNA’s prior consent.
Both the NNA Convertible Note and the NNA Warrants included the following terms:
· The exercise price under the NNA Warrants and the conversion price under the NNA Convertible Note and the number of shares underlying such securities would be adjusted under certain circumstances, resulting in the issuance of additional shares of ApolloMed’s securities. This adjustment would be triggered by ApolloMed’s issuance of shares of ApolloMed’s common stock (or securities issuable into its common stock) at a price per share less than $9.00 per share. The adjustments described in this paragraph did not apply to certain exempt issuances, including the sale of shares of ApolloMed’s common stock in a bona fide, firmly underwritten public offering pursuant to a registration statement under the 1933 Act and with a purchase price per share of at least $20.00 (a “Qualified IPO”). In addition, these adjustments would terminate on the earlier of (i) March 28, 2016 or (ii) ApolloMed’s closing of an equity financing yielding gross cash proceeds of at least $2,000,000 (the “Next Financing”). Any future issuances of ApolloMed’s securities that are not exempt would result in the adjustments described in this paragraph until the adjustments are terminated.
· ApolloMed was required to make cash payments to NNA on a ratable basis if it made any payments to holders of restricted stock units, phantom equity rights, equity appreciation rights or any other payments calculated in reference to the valuation or changes in valuation of ApolloMed’s common stock or equity.
| 258 |
Under the Investment Agreement, ApolloMed also granted the following rights to NNA for so long as NNA holds a specified number shares of ApolloMed’s common stock or NNA Warrants or the NNA Convertible Note convertible into such specified number of shares of ApolloMed’s common stock:
· NNA has the right to have one director nominated to ApolloMed’s board and each board of directors committee, and to appoint one representative to attend meetings of ApolloMed’s board of directors and each ApolloMed board’s committee as an observer.
· With certain specified exceptions, NNA has the right to subscribe for its pro rata share of any of ApolloMed’s issuances of securities on the same terms as such securities are being offered to others. This subscription right does not apply to certain exempt issuances, including the sale of ApolloMed’s shares of common stock in a Qualified IPO.
ApolloMed has also entered into a Registration Rights Agreement with NNA, which, as amended, provides NNA with the following rights, among others:
· NNA has the right to include all of its registrable securities (except for those eligible for resale under Rule 144) in any public offering by ApolloMed of ApolloMed’s securities under a registration statement filed with the SEC.
· ApolloMed is prohibited for an extended period of time from preparing or filing with the SEC a registration statement without the prior consent of NNA.
· ApolloMed is required to prepare and file with the SEC a registration statement covering the sale of NNA’s registrable securities by March 31, 2018. If it fails to do so, on such date, and in each following month until ApolloMed files the registration statement registering NNA’s registrable securities, ApolloMed must pay NNA liquidated damages of 1.5% of the total purchase price of the registrable securities owned by NNA, payable in shares of common stock. ApolloMed is also required to use ApolloMed’s commercially reasonable best efforts to cause the registration statement registering NNA’s registrable securities to be declared effective by the SEC by the earlier of (i) June 30, 2018 or (ii) the 5th trading day after the date ApolloMed is notified by the SEC that such registration statement will not be reviewed or will not be subject to further review to have such registration statement declared effective by the SEC.
On October 14, 2015, NNA converted $1,402,500 of convertible notes and accrued interest, as well as exercised warrants, into an aggregate 600,000 shares of ApolloMed’s common stock. On October 15, 2015, ApolloMed repaid all outstanding principal and accrued and unpaid interested owed to NNA under the Credit Agreement, as described below under “NMM Investments – October 2015 Investment by NMM, Repayment of NNA Debt and Conversion of NNA Warrants”.
NMM Investments
October 2015 Investment by NMM, Repayment of NNA Debt and Conversion of NNA Warrants
On October 14, 2015, ApolloMed entered into the 2015 Agreement with NMM, pursuant to which ApolloMed sold to NMM, and NMM purchased from ApolloMed, in a private offering of securities, 1,111,111 Series A units, each Series A unit consisting of one share of ApolloMed’s Series A convertible preferred stock and a warrant to purchase one share of ApolloMed’s common stock at an exercise price of $9.00 per share. NMM paid ApolloMed an aggregate of $10,000,000 for the Series A units, the proceeds of which ApolloMed used primarily to repay certain outstanding indebtedness owed by ApolloMed to NNA and the balance for working capital.
The Series A preferred stock has a liquidation preference in the amount of $9.00 per share plus any declared and unpaid dividends. The Series A preferred stock can be voted for the number of shares of ApolloMed’s common stock into which the Series A preferred stock could then be converted, which initially is one-for-one.
| 259 |
The Series A preferred stock is convertible into shares of ApolloMed’s common stock, at the option of the holder thereof, at any time after issuance at an initial conversion rate of one-for-one, subject to adjustment in the event of stock dividends, stock splits and certain other similar transactions. The Series A preferred stock is mandatorily convertible not sooner than the earlier to occur of the Redemption Expiration Date or the date on which ApolloMed receives the written, irrevocable decision of NMM not to require a redemption of the Series A preferred stock (as described in the following paragraph), in the event that ApolloMed receives aggregate gross proceeds of not less than $5,000,000 in one or more transactions for the sale of ApolloMed’s equity securities or securities convertible into, or exchangeable for, ApolloMed’s equity securities (other than any transactions with NMM as the holder of the Series A preferred stock).
At any time prior to conversion and through the Redemption Expiration Date, the Series A preferred stock was redeemable at the option of NMM, on one occasion, in the event that ApolloMed’s net revenue for the four quarters ending September 30, 2016, as reported in ApolloMed’s periodic filings under the Exchange Act, were less than $60,000, 000. In such event, ApolloMed had up to one year from the date of the notice of redemption by NMM to redeem the Redeemed Securities for the aggregate price paid therefor by NMM, together with interest at a rate of 10% per annum from the date of the notice of redemption until the closing of the redemption. ApolloMed did not attain the $60,000,000 net revenues milestone by such date. NMM relinquished its redemption rights relating to the Series A preferred stock pursuant to the terms of a Consent and Waiver Agreement dated as of December 21, 2016 by and between ApolloMed and NMM, which was entered into in connection with the entering into of the Merger Agreement.
Any mandatory conversion described above shall not take place until such time as it is determined that conditions for the redemption of the Redeemed Securities have not been satisfied or, if such conditions exist, NMM has decided not to have such securities redeemed.
The warrants may be exercised at any time after issuance and through October 14, 2020, for $9.00 per share, subject to adjustment in the event of stock dividends and stock splits. Alternatively, the warrants may be exercised pursuant to a “cashless exercise” feature, for that number of shares of common stock determined by dividing (x) the aggregate Fair Market Value (as defined in the warrant) of the shares in respect of which the warrant is being converted minus the aggregate Warrant Exercise Price (as defined in the warrant) of such shares by (y) the Fair Market Value of one share of ApolloMed’s common stock. The warrants are not separately transferable from the Series A preferred stock for which they relate (one-for-one).
Pursuant to the 2015 Agreement, NMM has the right to designate to the Nominating/Corporate Governance Committee of the Board of Directors one person to be nominated as a director of ApolloMed. NMM has designated Thomas S. Lam, M.D., and he was first elected as a director on January 19, 2016.
Without the written consent of NMM, between the closing of the 2015 Agreement and the six month anniversary of the closing of the 2015 Agreement, ApolloMed shall not acquire, sell all or substantially all of its assets to, effect a change of control, or merge, combine or consolidate with, any other person engaged in the business of being an MSO, ACO or IPA, or enter into any agreement with respect to any of the foregoing.
The 2015 Agreement contains other provisions typical of a transaction of this nature, including without limitation, representation and warranties, mutual indemnification by the parties, governing law and venue for resolution of disputes.
The securities sold to NMM have not been registered under the Securities Act and there are no registration rights with respect thereto.
On October 15, 2015, ApolloMed repaid, from the proceeds of the sale of the securities to NMM under the 2015 Agreement, ApolloMed’s outstanding term loan and revolving credit facility with NNA pursuant to the Credit Agreement, in the aggregate amount of $7,304,506, consisting of principal plus accrued interest. As of March 31, 2016, no amount remained outstanding to NNA.
| 260 |
On November 17, 2015, ApolloMed entered into the Conversion Agreement, pursuant to which it issued 275,000 shares of ApolloMed’s common stock and paid accrued and unpaid interest of $47,112, to NNA, in full satisfaction of NNA’s conversion and other rights under their Convertible Note in the principal amount of $2,000,000. Pursuant to the Conversion Agreement, ApolloMed issued a total of 325,000 shares of ApolloMed’s common stock to NNA in exchange for all NNA Warrants, under which NNA originally had the right to purchase 300,000 shares of ApolloMed’s common stock at an exercise price of $10 per share and 200,000 shares of ApolloMed’s common stock at an exercise price of $20 per share, in each case subject to anti-dilution adjustments. ApolloMed received no proceeds from NNA in connection with the exercise of the NNA Warrants.
The Conversion Agreement also amended certain terms of the Registration Rights Agreement dated March 28, 2014 between ApolloMed and NNA, with respect to the timing of the filing deadline for a resale registration statement covering NNA’s registrable securities. The Conversion Agreement also amended the Investment Agreement dated March 28, 2014 between ApolloMed and NNA, (i) to delete NNA’s right to subscribe to purchase a pro rata share of certain new equity securities that may be issued by ApolloMed in the future and (ii) to provide that NNA must hold at least 200,000 shares of ApolloMed’s common stock to have the right (y) to appoint a representative to attend all meetings of ApolloMed’s board and any committee thereof in a nonvoting observer capacity, and (z) to have a representative nominated as a member of ApolloMed’s board and each committee thereof, including without limitation, ApolloMed’s compensation committee. NNA nominated Mark Fawcett as its representative on the ApolloMed board and Mr. Fawcett was first elected as a director on January 12, 2016.
March 2016 Investment
On March 30, 2016, ApolloMed entered into the 2016 Agreement with NMM, pursuant to which ApolloMed sold to NMM, and NMM purchased from ApolloMed, in a private offering of securities, 555,555 Series B units, each Series B unit consisting of one share of ApolloMed’s Series B preferred stock and a warrant to purchase one share of ApolloMed’s common stock at an exercise price of $10.00 per share. NMM paid ApolloMed an aggregate of $4,999,995 for the Series B units, the proceeds of which will be used by ApolloMed for working capital.
The Series B preferred stock has a liquidation preference in the amount of $9.00 per share plus any declared and unpaid dividends. The Series B preferred stock can be voted for the number of shares of common stock into which the Series B preferred stock could then be converted, which initially is one-for-one.
The Series B preferred stock is convertible into shares of ApolloMed’s common stock, at the option of the holder thereof, at any time after issuance at an initial conversion rate of one-for-one, subject to adjustment in the event of stock dividends, stock splits and certain other similar transactions. The Series B preferred stock was mandatorily convertible at any time prior to and including March 31, 2017 in the event that ApolloMed engaged in one or more transactions for the sale of its equity securities or securities convertible into, or exchangeable for, ApolloMed’s equity securities resulting in gross proceeds of not less than $5,000,000, not including any transactions with NMM as the holder of the Series B preferred stock.
The warrants may be exercised at any time after issuance and through March 30, 2021, for $10.00 per share, subject to adjustment in the event of stock dividends and stock splits. Alternatively, the warrants may be exercised pursuant to a “cashless exercise” feature, for that number of shares of ApolloMed’s common stock determined by dividing (x) the aggregate Fair Market Value (as defined in the warrant) of the shares in respect of which the warrant is being converted minus the aggregate Warrant Exercise Price (as defined in the warrant) of such shares by (y) the Fair Market Value of one share of ApolloMed’s common stock. The warrants are not separately transferable from the Series B preferred stock for which they relate (one-for-one).
The 2016 Agreement contains other provisions typical of a transaction of this nature, including without limitation, representation and warranties, mutual indemnification by the parties, governing law and venue for resolution of disputes.
The securities sold to NMM have not been registered under the Securities Act and there are no registration rights with respect thereto.
| 261 |
The 2017 Loans
As required by the terms of the Merger Agreement, on January 3, 2017 NMM provided a working capital loan to ApolloMed in the principal amount of $5,000,000, which was evidenced by a promissory note (the “Original Note”). [Effective October 17, 2017 and in connection with Amendment No. 2, the parties entered into a new working capital loan in the amount of $9,000,000 evidenced by a promissory note, which is convertible in to shares of common stock of ApolloMed at $10 per share. Of the principal amount, (A) $5,000,000 is required to be used to refinance a $5,000,000 working capital loan that was previously loaned by NMM to the ApolloMed pursuant to the Original Note and (B) $4,000,000 is to be used for working capital. The Restated NMM Note cancels and replaces the Original Note and with the effect that the entire outstanding principal balance of the Original Note, all accrued and unpaid interest thereon, and any applicable fees, costs and charges rolls into and becomes payable pursuant to the terms of the Restated NMM Note.
Under the terms of the Restated NMM Note, in the event that ApolloMed fails to repay the Alliance Note in full when due, NMM agrees and undertakes to pay Alliance all amounts owed by ApolloMed to Alliance or enter into another agreement with Alliance. The Restated NMM Note has also been amended and restated to include (i) an extension of the maturity date to the earlier of (A) March 31, 2019 or (B) 12 months after the date the Merger Agreement is terminated, (ii) the increase in the principal amount of the Restated NMM Note to $13,990,000 if ApolloMed fails to pay the Alliance Note and NMM either pays all amounts owed under the Alliance Note or enters into another agreement with Alliance (such that in either case the Alliance Note is cancelled) and (iii) a conversion feature allowing the Restated NMM Note to be converted into shares of ApolloMed common stock at $10.00 per share, subject to adjustment for stock splits, dividends, recapitalizations and the like, with such conversion, if exercised in accordance with the terms of the Restated NMM Note, becoming effective on the maturity date.
However, if the Merger Agreement is terminated and the Merger is not consummated, ApolloMed might have an immediate need to raise additional capital to fund ApolloMed’s business and meet ApolloMed’s expenses, including both transactional and operational expenses.
Other Financings
On November 17, 2016, Liviu Chindris, M.D. loaned ApolloMed $400,000 and it issued ApolloMed’s promissory note to Dr. Chindris in such principal amount (the “Chindris Note”), bearing interest at a rate of 12% per annum. The Chindris Note required repayment of the outstanding principal and accrued interest, in full, on or before February 18, 2017. ApolloMed repaid the Chindris Note in full on February 17, 2017. In connection with the Chindris Note, Holdings issued a stock purchase warrant to Dr. Chindris (the “Chindris Warrant”) for the purchase of up to 5,000 shares of ApolloMed’s common stock at an exercise price of $9.00 per share. The relative fair value of the Chindris warrant was $6,880 and was recorded as debt discount to be amortized over the term of the Chindris Note using the straight-line method, which approximates the effective interest method. ApolloMed amortized $6,880 of debt discount to interest expense for the year ended March 31, 2017.
On March 30, 2017, Alliance loaned ApolloMed $4,990,000 and ApolloMed issued the Alliance Note to Alliance, bearing interest at a rate of 6% per annum. As amended on October 16, 2017, upon the earlier of March 31, 2018 or the termination of the Merger, the original principal amount of the Alliance Note, together with all accrued and unpaid interest thereon, shall automatically be converted into 499,000 shares of ApolloMed’s common stock, at a conversion price of $10.00 per share (the “Mandatory Conversion”), subject to adjustment for stock splits, stock dividends, reclassifications and other similar recapitalization transactions that occur after the date of the Alliance Note.
If the closing of the Merger has not occurred on or before the Alliance Maturity Date, then the entire then-outstanding principal balance under the Alliance Note and all accrued, unpaid interest thereon, shall be due and payable on the Maturity Date; provided, however, if the Mandatory Conversion has not occurred on or before the Alliance Maturity Date, then ApolloMed shall have 45 days following the Alliance Maturity Date to repay the outstanding principal, together with accrued and unpaid interest, on the Alliance Note.
In the case of an Event of Default (as defined in the Alliance Note), the entire outstanding principal and all accrued and unpaid interest under the Alliance Note shall automatically become immediately due and payable, without presentment, demand, protest or notice of any kind. If any other event of default occurs and is continuing, Alliance, by written notice to ApolloMed, may declare the outstanding principal and interest under the Alliance Note to be immediately due and payable. After maturity (by acceleration or otherwise), the unpaid balance (both as to principal and unpaid pre-maturity interest) shall bear interest at a default rate equal to the lesser of (a) three percent (3%) over the rate of interest in effect immediately prior to maturity or (ii) the then maximum legal rate allowed under the laws of the State of California. Additionally, ApolloMed shall pay all costs of collection incurred by Alliance, including reasonable attorney’s fees incurred in connection with the Alliance’s reasonable collection efforts.
| 262 |
ApolloMed has granted Alliance both “demand” and “piggyback” registration rights to register the shares of ApolloMed’s common stock issuable upon conversion of the Alliance Note, subject to a good faith, pro rata clawback provision.
Contractual Obligations and Commercial Commitments
Debt Agreements
As of March 31, 2017, ApolloMed has a line of credit with an outstanding principal amount of $62,500.
ApolloMed also has the NMM Note in the principal amount of $5,000,000. Interest is due quarterly at the rate of the Prime Rate plus 1%, with the entire principal balance being due on January 3, 2019.
In addition, ApolloMed has the Alliance Note in the principal amount of $4.99 million. As amended, the note is due and payable to Alliance on (i) March 31, 2018, or (ii) the date on which the Change of Control Transaction (see Note 10 – NMM transaction) is terminated, whichever occurs first (“Maturity Date”). Upon the closing, on or before the Maturity Date, of the Change of Control Transaction, the Note and accrued interest, shall automatically be converted into shares of ApolloMed’s common stock, at a conversion price of $10.00 per share, subject to adjustment for stock splits, stock dividends, reclassifications and other similar recapitalization transactions that occur after the date of the Note. NMM has guaranteed the note in exchange for warrants to purchase 850,000 shares of common stock, to be issued as merger consideration, at an exercise price of $11 per share, that will only be granted in the case that the proposed merger between ApolloMed and NMM occurs (such warrant will not vest and will expire if the contemplated merger transaction does not occur).
ApolloMed has contingent payment arrangements associated with its acquisitions of AKM, SCHC, BCHC, HCHHA and BAHA. The aggregate maximum of contingent payments under these arrangements was $1,650,000, of which $ 954,904 was paid in fiscal 2015 and fiscal 2016 and $154,415 was paid in fiscal 2017, respectively.
Employment Agreements
ApolloMed has entered into employment agreements with several of ApolloMed’s key personnel, including ApolloMed’s executive officers, which provide for, among other items, annual base salaries, discretionary bonuses and participation in ApolloMed’s equity incentive plans. These agreements also contain change of control, termination and severance clauses that require ApolloMed to make payments to certain of these employees if certain events occur as defined in their respective agreements. See “MANAGEMENT OF THE COMBINED COMPANY” on page 177 for more information.
Lease Agreements
ApolloMed’s corporate headquarters are located at 700 North Brand Boulevard, Suite 1400, Glendale, California 91203. Under the lease of the premises, it occupies spaces in Suite Nos. 1400, 1425 and 1450, which collectively include 16,484 rentable square feet (the “Premises”). The Premises were improved with an allowance of $659,360, provided by the landlord, for construction and installation of equipment for the Premises. The lease requires base rent of $37,913 per month for the first year and schedules annual increases in base rent each year until the final rental year, which is capped at $43,957 per month and schedules annual increases in base rent each year until the final rental year, which is capped at $43,957 per month. However, the base rent will be abated by up to $228,049 subject to other terms of the lease.
AMM leases the SCHC premises located in Los Angeles, California, consisting of 8,766 rentable square feet, for a term of ten years. The base rent for the SCHC lease is approximately $33,000 per month.
Future minimum rental payments required under the operating leases are as follows:
| 263 |
Year ending March 31,
| 2018 | $ | 982,000 | ||
| 2019 | 977,000 | |||
| 2020 | 994,000 | |||
| 2021 | 1,012,000 | |||
| 2022 | 716,000 | |||
| Thereafter | 910,000 | |||
| $ | 5,591,000 |
MMG
The DMHC oversees the performance of RBOs in California. An RBO is measured for TNE, working capital, cash to claims ratio and claims timeliness. MMG is an RBO in California and is required to maintain positive TNE. In the fourth quarter of the fiscal year ended March 31, 2016, MMG reported negative TNE. MMG submitted a CAP to the DMHC, which the DMHC approved. MMG has up to one year to cure the deficiency. As a result of actions ApolloMed took, including amending ApolloMed’s existing loan agreement with MMG and entering into a subordination agreement with respect to that loan, as discussed below, MMG had positive TNE as of the third quarter of fiscal 2017 and has maintained positive TNE to date. Since DMHC requirements are that an RBO should have positive TNE for one full quarter to be taken off a CAP, ApolloMed believes that MMG is currently in compliance with DMHC requirements. The DMHC is currently reviewing filings ApolloMed has made to confirm this compliance.
In connection with DMHC’s approval of ApolloMed’s CAP for MMG, on November 22, 2016, AMM entered into an Intercompany Revolving Loan Agreement (the “MMG Loan Agreement”) with MMG, pursuant to which AMM has agreed to lend MMG up to $2,000,000 (the “Commitment Amount”) in one or more advances (collectively, “Advances”) that MMG may request from time to time during the term of the MMG Loan Agreement. Interest on outstanding Advances shall accrue interest at a rate equal to the greater of 10% per annum or the LIBOR rate then in effect, and is payable monthly on the first business day of each month. In an Event of Default (as defined in the MMG Loan Agreement), interest on Advances shall accrue interest at a default rate equal to 3% per annum above the interest rate then in effect. Additionally, in an Event of Default, MMG may, among other things, accelerate all payments due under the MMG Loan Agreement.
The MMG Loan Agreement replaces substantially similar loan agreements between the parties (other than with respect to the Commitment Amount), including without limitation that certain Intercompany Revolving Loan Agreement dated as of February 1, 2013, that certain Amendment No. l to Intercompany Revolving Loan Agreement dated as of March 28, 2014, that certain Intercompany Revolving Loan Agreement dated as of June 27, 2014, and that certain Amendment No. 2 to Intercompany Revolving Loan Agreement dated as of March 30, 2016, all of which were terminated. See “Intercompany Loans” below.
Also on November 22, 2016, and also at the request of the DMHC in connection with its review and approval of the corrective action plan for MMG, AMM and MMG entered into a Subordination Agreement (the “Subordination Agreement”), pursuant to which AMM has agreed to irrevocably and fully subordinate its right to repayment of Advances, together with interest thereon, under the Loan Agreement, to all other present and future creditors of MMG. AMM also agreed that the payment by MMG of principal and interest of Advances under the MMG Loan Agreement will be suspended and will not mature when, excluding the liability of MMG to pay AMM principal and interest under the MMG Loan Agreement, if after giving effect to the payment, MMG would not be in compliance with the financial solvency requirements, as defined in and calculated under Knox-Keene and the rules promulgated thereunder. AMM further agreed that, in the event of the liquidation or dissolution of MMG, the payment by MMG of principal and interest to AMM under the MMG Loan Agreement shall be fully subordinated and subject to the prior payment or provision for payment in full of all claims of all other present and future creditors of MMG.
| 264 |
Upon the written consent of the director of the DMHC, all previous subordination agreements between AMM and MMG, including without limitation that certain Subordination Agreement dated June 27, 2014 between AMM and MMG and that certain Amended and Restated Subordination Agreement between AMM and MMG dated as of March, 30, 2016, were terminated. The Subordination Agreement may not be cancelled, terminated, rescinded or amended by mutual consent or otherwise, without the prior written consent of the director of the DMHC.
In December 2016, in response to a request by Humana Insurance Company and Humana Health Plan, Inc. (collectively “Humana”), MMG arranged for City National Bank (“CNB”) to provide an irrevocable standby letter of credit in an amount up to $235,000 through December 31, 2017, and entered into a security agreement in favor of CNB, as required by the Independent Practice Association Participation Agreement effective January 1, 2015, including the addenda and attachments thereto, and as amended.
Lines of credit
Hendel had a $100,000 revolving line of credit with MUFG Union Bank, N.A., of which $0 and $88,764 was outstanding at March 31, 2017 and 2016, respectively. Borrowings under the line of credit bore interest at the prime rate (as defined) plus 4.50% (8.50% and 8.00% per annum at March 31, 2017 and 2016, respectively), interest only is payable monthly, and the line of credit matured on March 31, 2017. The line of credit was unsecured. Hendel is no longer consolidated effective January 1, 2017 and its operations are not included in ApolloMed’s March 31, 2017 consolidated financial statements subsequent to January 1, 2017.
LALC had a line of credit of $230,000 with JPMorgan Chase Bank, N.A. Borrowing under the line of credit bears interest at a rate of 5.25% and is auto-renewed on an annual basis. ApolloMed has not borrowed any amount under this line of credit as of March 31, 2017 and 2016. The line of credit is unsecured. LALC is no longer consolidated effective January 1, 2017 and its operations are not included in ApolloMed’s March 31, 2017 consolidated financial statements subsequent to January 1, 2017.
BAHA has a line of credit of $150,000 with First Republic Bank. Borrowings under the line of credit bear interest at the prime rate (as defined) plus 3.0% (7.25% and 7.0% per annum at June 30, 2017 and March 31, 2017, respectively). ApolloMed has an outstanding balance of $25,000 and $62,500 as of June 30, 2017 and March 31, 2017, respectively. The line of credit is unsecured.
Intercompany Loans
Each of AMH, ACC, MMG, AKM and SCHC has entered into an Intercompany Loan Agreement with AMM under which AMM has agreed to provide a revolving loan commitment to each of the affiliated entities in an amount set forth in each Intercompany Loan Agreement. Each Intercompany Loan Agreement provides that AMM’s obligation to make any advances automatically terminates concurrently with the termination of the Management Agreement with the applicable affiliated entity. In addition, each Intercompany Loan Agreement provides that (i) any material breach by Dr. Hosseinion of the applicable Physician Shareholder Agreement or (ii) the termination of the Management Agreement with the applicable affiliated entity constitutes an event of default under the Intercompany Loan Agreement. The following tables summarize the various intercompany loan agreements as of June 30, 2017 and March 31, 2017:
| 265 |
| Three Months Ended June 30, 2017 | ||||||||||||||||||||||||||
| Entity | Facility | Expiration | Interest rate per Annum |
Maximum Balance During Period |
Ending Balance |
Principal Paid During Period |
Interest Paid During Period |
|||||||||||||||||||
| AMH | $ | 10,000,000 | 9/30/2018 | 10 | % | $ | 5,204,342 | $ | 4,988,503 | $ | - | $ | - | |||||||||||||
| ACC | 1,000,000 | 7/31/2018 | 10 | % | 1,287,843 | 1,287,843 | - | - | ||||||||||||||||||
| MMG | 2,000,000 | 2/1/2018 | 10 | % | 1,588,769 | 1,587,968 | - | - | ||||||||||||||||||
| AKM | 5,000,000 | 5/30/2019 | 10 | % | - | - | - | - | ||||||||||||||||||
| SCHC | 5,000,000 | 7/21/2019 | 10 | % | 3,128,539 | 3,024,360 | - | - | ||||||||||||||||||
| BAHA | 250,000 | 7/22/2021 | 10 | % | 1,642,076 | 1,642,076 | - | - | ||||||||||||||||||
| $ | 23,250,000 | $ | 12,851,570 | $ | 12,530,750 | $ | - | $ | - | |||||||||||||||||
| Year Ended March 31, 2017 | ||||||||||||||||||||||||||
| Entity | Facility | Expiration | Interest rate per Annum |
Maximum Balance During Period |
Ending Balance |
Principal Paid During Period |
Interest Paid During Period |
|||||||||||||||||||
| AMH | $ | 10,000,000 | 9/30/2018 | 10 | % | $ | 4,904,147 | $ | 4,904,147 | $ | - | $ | - | |||||||||||||
| ACC | 1,000,000 | 7/31/2018 | 10 | % | 1,287,843 | 1,287,843 | 5,000 | - | ||||||||||||||||||
| MMG | 2,000,000 | 2/1/2018 | 10 | % | 1,918,724 | 1,255,111 | 725,107 | - | ||||||||||||||||||
| AKM | 5,000,000 | 5/30/2019 | 10 | % | - | - | - | - | ||||||||||||||||||
| SCHC | 5,000,000 | 7/21/2019 | 10 | % | 3,079,916 | 3,079,916 | 50,000 | - | ||||||||||||||||||
| BAHA | 250,000 | 7/22/2021 | 10 | % | 1,171,526 | 1,171,526 | - | |||||||||||||||||||
| $ | 23,250,000 | |||||||||||||||||||||||||
Critical Accounting Policies
Some of ApolloMed’s accounting policies require the application of judgment by management in selecting appropriate assumptions for calculating financial estimates, which inherently contain some degree of uncertainty. Management bases its estimates on historical experience and various other assumptions that are believed to be reasonable under the circumstances. The historical experience and assumptions form the basis for making judgments about the reported carrying values of assets and liabilities and the reported amounts of revenue and expenses that may not be readily apparent from other sources. Actual results may differ from these estimates under different assumptions or conditions. ApolloMed believes the following are critical accounting policies and related judgments and estimates used in the preparation of ApolloMed’s consolidated financial statements.
Principles of Consolidation
ApolloMed’s consolidated financial statements include the accounts of (1) Apollo Medical Holdings, Inc. and its wholly owned subsidiaries AMM, PCCM, and VMM, (2) ApolloMed’s controlling interest in ApolloMed ACO, and APS, (3) physician practice corporations (“PPCs”) managed under long-term management service agreements including AMH, MMG, ACC, LALC (through December 31, 2016), Hendel (through December 31, 2016), AKM, SCHC and BAHA. Some states have laws that prohibit business entities, such as ApolloMed, from practicing medicine, employing physicians to practice medicine, exercising control over medical decisions by physicians (collectively known as the corporate practice of medicine), or engaging in certain arrangements with physicians, such as fee-splitting. In California, ApolloMed operates by maintaining long-term management service agreements with the PPCs, which are each owned and operated by physicians, and which employ or contract with additional physicians to provide hospitalist services. Under the management agreements, ApolloMed provides and performs all non-medical management and administrative services, including financial management, information systems, marketing, risk management and administrative support. Each management agreement typically has a term from 10 to 20 years unless terminated by either party for cause. The management agreements are not terminable by the PPCs, except in the case of material breach or bankruptcy of the respective PPM. Because, effective on January 1, 2017, ApolloMed no longer holds an explicit or implicit variable interest in LALC and Hendel, the two PPCs are not consolidated as of such date. All intercompany balances and transactions have been eliminated.
| 266 |
Through the management agreements and ApolloMed’s relationship with the stockholders of the PPCs, ApolloMed has exclusive authority over all non-medical decision making related to the ongoing business operations of the PPCs. Consequently, ApolloMed consolidates the revenue and expenses of each PPC from the date of execution of the applicable management agreement.
On January 1, 2017, PCCM amended the management services agreements entered into with LALC and Hendel. Based on ApolloMed’s evaluation of current accounting guidance, it was determined that ApolloMed no longer holds an explicit or implicit variable interest in these entities, and accordingly LALC and Hendel are no longer consolidated and their operations are not included in the March 31, 2017 consolidated financial statements of ApolloMed as of such date. In connection with the amendments, ApolloMed recorded a gain on disposition of $242,411 in the consolidated statement of operations, the reversal of the net assets of the LALC and Hendel entities and related noncontrolling interest of $1,023,183 in the consolidated balance sheet, and a decrease in cash and cash equivalents and in the consolidated statements of cash flows in the amount of $858,670.
All intercompany balances and transactions have been eliminated in consolidation.
Business Combinations
ApolloMed uses the acquisition method of accounting for all business combinations, which requires assets and liabilities of the acquiree to be recorded at fair value (with limited exceptions), to measure the fair value of the consideration transferred, including contingent consideration, to be determined on the acquisition date, and to account for acquisition related costs separately from the business combination.
Reportable Segments
ApolloMed operates as one reportable segment, the healthcare delivery segment, and implements and operates innovative health care models to create a patient-centered, physician-centric experience. It reports ApolloMed’s consolidated financial statements in the aggregate, including all activities in one reportable segment. ApolloMed has determined it has six reporting units, which are comprised of (1) Hospitalist and AMM, (2) IPA, (3) Clinics, (4) Care Connect, (5) ACO, and (6) Palliative Services. While the chief operating decision maker uses financial information related to these reporting units to analyze business performance and allocate resources, the reporting units, as noted above, do not meet the quantitative threshold under U.S. GAAP to be considered a reportable segment. As such, these reporting units are aggregated into a single reportable segment in the consolidated financial statements.
Concentrations
ApolloMed’s business and operations are concentrated in one state, California. Any material changes by California with respect to strategy, taxation and economics of healthcare delivery, reimbursements, financial requirements or other aspects of regulation of the healthcare industry could have an adverse effect on ApolloMed’s operations and cost of doing business.
Revenue Recognition
Revenue consists of primarily contracted, FFS and capitation revenue. Revenue is recorded in the period in which services are rendered. Revenue is derived from the provision of healthcare services to patients within healthcare facilities, medical management and care coordination of network physicians and patients. The form of billing and related risk of collection for such services may vary by customer. The following is a summary of the principal forms of ApolloMed’s billing arrangements and how net revenue is recognized for each.
| 267 |
Contracted revenue
Contracted revenue represents revenue generated under contracts for which ApolloMed provides physician and other healthcare staffing and administrative services in return for a contractually negotiated fee. Contract revenue consists primarily of billings based on hours of healthcare staffing, provided at agreed-to hourly rates. Revenue in such cases is recognized as the hours are worked by ApolloMed’s staff and contractors. Additionally, contract revenue also includes supplemental revenue from hospitals where ApolloMed may have a FFS contract arrangement or provide physician advisory services to the medical staff at a specific facility. Contract revenue for the supplemental billing in such cases is recognized based on the terms of each individual contract. Such contract terms generally either provides for a fixed monthly dollar amount or a variable amount based upon measurable monthly activity, such as hours staffed, patient visits or collections per visit compared to a minimum activity threshold. Such supplemental revenues based on variable arrangements are usually contractually fixed on a monthly, quarterly or annual calculation basis considering the variable factors negotiated in each such arrangement. Such supplemental revenues are recognized as revenue in the period when such amounts are determined to be fixed and therefore contractually obligated as payable by the customer under the terms of the respective agreement. Additionally, ApolloMed derives a portion of its revenue as a contractual bonus from collections received by ApolloMed’s partners and such revenue is contingent upon the collection of third-party billings. These revenues are not considered earned and therefore not recognized as revenue until actual cash collections are achieved in accordance with the contractual arrangements for such services.
Fee-for-Service revenue
FFS revenue represents revenue earned under contracts in which ApolloMed bills and collects the professional component of charges for medical services rendered by ApolloMed’s contracted physicians. Under the FFS arrangements, it bills patients for services provided and receives payment from patients or their third-party payors. FFS revenue is reported net of contractual allowances and policy discounts. All services provided are expected to result in cash flows and are therefore reflected as net revenue in the financial statements. FFS revenue is recognized in the period in which the services are rendered to specific patients and reduced immediately for the estimated impact of contractual allowances in the case of those patients having third-party payor coverage. The recognition of net revenue (gross charges less contractual allowances) from such visits is dependent on such factors as proper completion of medical charts following a patient visit, the forwarding of such charts to ApolloMed’s billing center for medical coding and entering into ApolloMed’s billing system and the verification of each patient’s submission or representation at the time services are rendered as to the payor(s) responsible for payment of such services. Revenue is recorded based on the information known at the time of entering of such information into ApolloMed’s billing systems as well as an estimate of the revenue associated with medical services.
Capitation revenue
Capitation revenue (net of capitation withheld to fund risk share deficits) is recognized in the month in which ApolloMed is obligated to provide services. Minor ongoing adjustments to prior months’ capitation, primarily arising from contracted HMOs finalizing of monthly patient eligibility data for additions or subtractions of enrollees, are recognized in the month they are communicated to ApolloMed. Managed care revenues consist primarily of capitated fees for medical services provided by ApolloMed under a PSA or capitated arrangements directly made with various managed care providers including HMO’s and MSOs. Capitation revenue under the PSA and HMO contracts is prepaid monthly to ApolloMed based on the number of enrollees electing ApolloMed as their healthcare provider. Additionally, Medicare pays capitation using a “Risk Adjustment model,” which compensates managed care organizations and providers based on the health status (acuity) of each individual enrollee. Health plans and providers with higher acuity enrollees will receive more and those with lower acuity enrollees will receive less. Under Risk Adjustment, capitation is determined based on health severity, measured using patient encounter data. Capitation is paid on an interim basis based on data submitted for the enrollee for the preceding year and is adjusted in subsequent periods after the final data is compiled. Positive or negative capitation adjustments are made for Medicare enrollees with conditions requiring more or less healthcare services than assumed in the interim payments. Since ApolloMed cannot reliably predict these adjustments, periodic changes in capitation amounts earned as a result of Risk Adjustment are recognized when those changes are communicated by the health plans to it
HMO contracts also include provisions to share in the risk for enrollee hospitalization, whereby ApolloMed can earn additional incentive revenue or incur penalties based upon the utilization of hospital services. Typically, any shared risk deficits are not payable until and unless ApolloMed generates future risk sharing surpluses, or if the HMO withholds a portion of the capitation revenue to fund any risk share deficits. At the termination of the HMO contract, any accumulated risk share deficit is typically extinguished. Due to the lack of access to information necessary to estimate the related costs, shared-risk amounts receivable from the HMOs are only recorded when such amounts are known. Risk pools for the prior contract years are generally settled in the third or fourth quarter of the following fiscal year.
| 268 |
In addition to risk-sharing revenues, ApolloMed also receives incentives under “pay-for-performance” programs for quality medical care, based on various criteria. These incentives, which are included in other revenues, are generally recorded in the third and fourth quarters of the fiscal year and are recorded when such amounts are known.
Under full risk capitation contracts, an affiliated hospital enters into agreements with several HMOs, pursuant to which, the affiliated hospital provides hospital, medical, and other healthcare services to enrollees under a fixed capitation arrangement (“Capitation Arrangement”). Under the risk pool sharing agreement, the affiliated hospital and medical group agree to establish a Hospital Control Program to serve the enrollees, pursuant to which, the medical group is allocated a percentage of the profit or loss, after deductions for costs to affiliated hospitals. ApolloMed participates in full risk programs under the terms of the PSA, with health plans whereby ApolloMed is wholly liable for the deficits allocated to the medical group under the arrangement.
Medicare Shared Savings Program Revenue
ApolloMed, through its subsidiary ApolloMed ACO, participates in the MSSP, which is sponsored by CMS. The goal of the MSSP is to improve the quality of patient care and outcomes through more efficient and coordinated approach among providers. The MSSP allows ACO participants to share in cost savings it generates in connection with rendering medical services to Medicare patients. Payments to ACO participants, if any, will be calculated annually by CMS on cost savings generated by the ACO participant relative to the ACO participants’ cost savings benchmark. The MSSP is a relatively new program managed by CMS that has an evolving payment methodology. Revenues earned by ApolloMed ACO are uncertain, and, if such amounts are payable by the CMS, they will be paid on an annual basis significantly after the time earned, and will be contingent on various factors, including achievement of the minimum savings rate as determined by MSSP for the relevant period. Such payments are earned and made on an “all or nothing” basis. ApolloMed considers revenue, if any, under the MSSP, as contingent upon the realization of program savings as determined by CMS, and are not considered earned and therefore are not recognized as revenue until notice from CMS that cash payments are to be imminently received.
Hospitalist Agreements
During the year, ApolloMed entered into several new hospitalist agreements with hospitals, whereby it earns a stipend fee plus a fee based on an agreed percentage of FFS collections. The fee is recorded at an amount net of the portion owed to the hospitals (ApolloMed collects all fees on behalf of the hospitals). The fee revenue is further reduced by a portion subject to quality metrics which is only recorded as revenue upon ApolloMed meeting these metrics. ApolloMed considered the indicators of gross revenue and net revenue reporting and determined that revenue from this arrangement is recorded at net.
Goodwill and Indefinite-Lived Intangible Assets
Under FASB ASC 350, Intangibles – Goodwill and Other (“ASC 350”), goodwill and indefinite-lived intangible assets are reviewed at least annually for impairment. Acquired intangible assets with definite lives are amortized over their individual useful lives.
At least annually, at ApolloMed’s fiscal year end, management assesses whether there has been any impairment in the value of goodwill by first comparing the fair value to the net carrying value of the reporting unit. If the carrying value exceeds its estimated fair value, a second step is performed to compute the amount of the impairment. ApolloMed has determined it has six reporting units, which are comprised of (1) Hospitalist and AMM, (2) IPA, (3) Clinics, (4) Care Connect, (5) ACO, and (6) Palliative Services.
| 269 |
An impairment loss is recognized if the implied fair value of the asset being tested is less than its carrying value. In this event, the asset is written down accordingly. The fair values of goodwill are determined using valuation techniques based on estimates, judgments and assumptions management believes are appropriate in the circumstances.
At least annually, indefinite-lived intangible assets are tested for impairment. Impairment for intangible assets with indefinite lives exists if the carrying value of the intangible asset exceeds its fair value. The fair values of indefinite-lived intangible assets are determined using valuation techniques based on estimates, judgments and assumptions management believes are appropriate in the circumstances.
Accounts Receivable and Allowance for Doubtful Accounts
Accounts receivable primarily consists of amounts due from third-party payors, including government sponsored Medicare and Medicaid programs, insurance companies, and amounts due from hospitals and patients. Accounts receivable are recorded and stated at the amount expected to be collected.
ApolloMed maintains reserves for potential credit losses on accounts receivable. Management reviews the composition of accounts receivable and analyzes historical bad debts, customer concentrations, customer credit worthiness, current economic trends and changes in customer payment patterns to evaluate the adequacy of these reserves. ApolloMed also regularly analyses the ultimate collectability of accounts receivable after certain stages of the collection cycle using a look-back analysis to determine the amount of receivables subsequently collected and adjustments are recorded when necessary. Reserves are recorded primarily on a specific identification basis.
Medical Liabilities
ApolloMed is responsible for integrated care that the associated physicians and contracted hospitals provide to ApolloMed’s enrollees under risk-pool arrangements. ApolloMed provides integrated care to health plan enrollees through a network of contracted providers under sub-capitation and direct patient service arrangements, company-operated clinics and staff physicians. Medical costs for professional and institutional services rendered by contracted providers are recorded as cost of services in the accompanying consolidated statements of operations. Costs for operating medical clinics, including the salaries of medical personnel, are also recorded in cost of services, while non-medical personnel and support costs are included in general and administrative expense.
An estimate of amounts due to contracted physicians, hospitals, and other professional providers is included in medical liabilities in the accompanying consolidated balance sheets. Medical liabilities include claims reported as of the balance sheet date and estimates of incurred but not reported claims (“IBNR”). Such estimates are developed using actuarial methods and are based on many variables, including the utilization of health care services, historical payment patterns, cost trends, product mix, seasonality, changes in membership, and other factors. The estimation methods and the resulting reserves are periodically reviewed and updated. Many of the medical contracts are complex in nature and may be subject to differing interpretations regarding amounts due for the provision of various services. Such differing interpretations may not come to light until a substantial period of time has passed following the contract implementation. ApolloMed has a $20,000 per member professional stop-loss and $200,000 per member stop-loss for Medi-Cal patients in institutional risk pools. Any adjustments to reserves are reflected in current operations.
ApolloMed’s medical liabilities were as follows:
| Three Months Ended June 30, 2017 |
Year Ended March 31, 2017 |
|||||||
| Balance, beginning of period | $ | 1,768,231 | $ | 2,670,709 | ||||
| Incurred health care costs: | ||||||||
| Current year | 30,109,821 | 10,365,502 | ||||||
| Claims paid: | ||||||||
| Current year | (11,017,283 | ) | (8,524,215 | ) | ||||
| Prior years | (1,575,049 | ) | (1,881,869 | ) | ||||
| Total claims paid | (12,592,332 | ) | (10,406,084 | ) | ||||
| Risk pool settlement | - | 814,733 | ||||||
| Accrual for net surplus (deficit) from full risk capitation contracts | 432,415 | (1,676,629 | ) | |||||
| Balance, end of period | $ | 19,718,135 | $ | 1,768,231 | ||||
Noncontrolling Interests
The noncontrolling interests recorded in ApolloMed’s consolidated financial statements includes the pre-acquisition equity of those PPC’s in which it has determined that it has a controlling financial interest and for which consolidation is required as a result of management contracts entered into with these entities owned by third-party physicians. The nature of these contracts provide ApolloMed with a monthly management fee to provide the services described above, and as such, the adjustments to noncontrolling interests in any period subsequent to initial consolidation would relate to either capital contributions or distributions by the noncontrolling parties as well as income or losses attributable to certain noncontrolling interests. Noncontrolling interests also represent third-party minority equity ownership interests which are majority owned by ApolloMed.
During the year ended March 31, 2016, ApolloMed entered into an agreement with a shareholder of APS which is one of ApolloMed’s majority owned subsidiaries. In connection with the agreement, the former shareholder received approximately $400,000, of which approximately $252,000 was paid by ApolloMed and the remaining amount of approximately $148,000 was paid by another shareholder of APS, in exchange for his interest in such subsidiary, resulting in an increase in ApolloMed’s ownership interest in APS from 51% to 56%.
| 270 |
New Accounting Pronouncements
In February 2016, the FASB issued ASU 2016-02, Leases (“ASU 2016-02”). This new standard establishes a right-of-use (ROU) model that requires a lessee to record a ROU asset and a lease liability on the balance sheet for all leases with terms longer than 12 months. Leases will be classified as either finance or operating, with classification affecting the pattern of expense recognition in the income statement. ASU 2016-02 is effective for fiscal years beginning after December 15, 2018, including interim periods within those fiscal years. Early adoption is permitted. A modified retrospective transition approach is required for lessees for capital and operating leases existing at, or entered into after, the beginning of the earliest comparative period presented in the financial statements, with certain practical expedients available. ApolloMed is currently evaluating the impact of the adoption of ASU 2016-02 on the consolidated financial statements.
In March 2016, the FASB issued ASU 2016-09, Compensation - Stock Compensation (Topic 718): Improvements to Employee Share-Based Payment Accounting (“ASU 2016-09”). This ASU makes several modifications to Topic 718 related to the accounting for forfeitures, employer tax withholding on share-based compensation, and the financial statement presentation of excess tax benefits or deficiencies. ASU 2016-09 also clarifies the statement of cash flows presentation for certain components of share-based awards. The standard is effective for interim and annual reporting periods beginning after December 15, 2016, with early adoption permitted. ApolloMed adopted this guidance on April 1, 2017 and does not expect such adoption to have a material impact on its consolidated financial statements and related disclosures for fiscal 2018.
In January 2016, the FASB issued ASU No. 2016-01, Financial Instruments - Overall (Topic 825-10): Recognition and Measurement of Financial Assets and Financial Liabilities ("ASU 2016-01"). ASU 2016-01 addresses certain aspects of recognition, measurement, presentation and disclosures of financial instruments including the requirement to measure certain equity investments at fair value with changes in fair value recognized in net income. ASU 2016-01 will become effective for ApolloMed beginning interim period April 1, 2018. ApolloMed is currently evaluating the guidance to determine the potential impact on its financial condition, results of operations, cash flows and financial statement disclosures.
The FASB issued the following accounting standard updates related to Topic 606, Revenue Contracts with Customers:
| · | ASU No. 2014-09, Revenue from Contracts with Customers (Topic 606) (“ASU 2014-09”) in May 2014. ASU 2014-09 requires entities to recognize revenue through the application of a five-step model, which includes identification of the contract, identification of the performance obligations, determination of the transaction price, allocation of the transaction price to the performance obligations and recognition of revenue as the entity satisfies the performance obligations. |
| · | ASU No. 2016-08, Revenue from Contracts with Customers (Topic 606): Principal versus Agent Considerations (Reporting Revenue Gross versus Net) ("ASU 2016-08") in March 2016. ASU 2016-08 does not change the core principle of revenue recognition in Topic 606 but clarifies the implementation guidance on principal versus agent considerations. |
| · | ASU No. 2016-10, Revenue from Contracts with Customers (Topic 606): Identifying Performance Obligations and Licensing ("ASU 2016-10") in April 2016. ASU 2016-10 does not change the core principle of revenue recognition in Topic 606 but clarifies the implementation guidance on identifying performance obligations and the licensing implementation guidance, while retaining the related principles for those areas. |
| 271 |
| · | ASU No. 2016-11, Revenue Recognition (Topic 605) and Derivatives and Hedging (Topic 815): Rescission of SEC Guidance Because of Accounting Standards Updates 2014-09 and 2014-16 Pursuant to Staff Announcements at the March 3, 2016 EITF Meeting (SEC Update) ("ASU 2016-11") in May 2016. ASU 2016-11 rescinds SEC paragraphs pursuant to two SEC Staff Announcements at the March 3, 2016 EITF meeting. The SEC Staff is rescinding SEC Staff Observer comments that are codified in Topic 605 and Topic 932, effective upon adoption of Topic 606. |
| · | ASU No. 2016-12, Revenue from Contracts with Customers (Topic 606): Narrow-Scope Improvements and Practical Expedients in May 2016. ASU 2016-12 does not change the core principle of revenue recognition in Topic 606 but clarifies the implementation guidance on a few narrow areas and adds some practical expedients to the guidance. |
| · | ASU No. 2016-20, Revenue from Contracts with Customers (Topic 606): Technical Corrections and Improvements ("ASU 2 016-20") in December 2016. ASU 2016-20 does not change the core principle of revenue recognition in Topic 606 but summarizes the technical corrections and improvements to ASU 2014-09 and is effective upon adoption of Topic 606. |
These ASUs will become effective for ApolloMed beginning interim period April 1, 2018. ApolloMed currently anticipates adopting the standard using the modified retrospective method. ApolloMed has begun the process of implementing this standard, including performing a review of its revenue streams to identify any differences in the timing, measurement, or presentation of revenue recognition. ApolloMed currently believes that the primary impact will be changes to the timing of recognition of revenues related to FFS and Capitation Revenue and enhanced financial statement disclosures. ApolloMed will continue to assess the impact on all areas of its revenue recognition, disclosure requirements and changes that may be necessary to its internal controls over financial reporting.
In August 2016, the FASB issued ASU No. 2016-15, Statement of Cash Flows (Topic 230) – Classification of Certain Cash Receipts and Cash Payments (“ASU 2016-15”). This ASU provides clarification regarding how certain cash receipts and cash payments are presented and classified in the statement of cash flows. This ASU addresses eight specific cash flow issues with the objective of reducing the existing diversity in practice. The issues addressed in this ASU that will affect ApolloMed are classifying debt prepayments or debt extinguishment costs and contingent consideration payments made after a business combination. This update is effective for annual and interim periods beginning after December 15, 2017, and interim periods within that reporting period. Early adoption is permitted. ApolloMed is currently assessing the impact the adoption of ASU 2016-15 will have on its consolidated financial statements.
In December 2016, the FASB issued ASU No. 2016-18, Statement of Cash Flows (Topic 230) ("ASU 2016-18”). The amendments in ASU 2016-18 require that a statement of cash flows explain the change during the period in the total of cash, cash equivalents, and amounts generally described as restricted cash or restricted cash equivalents. ASU 2016-17 will become effective for ApolloMed beginning interim period April 1, 2018. Early adoption is permitted, including adoption in an interim period. ApolloMed is currently assessing the impact the adoption of ASU 2016-18 will have on ApolloMed’s consolidated financial statements.
In January 2017, the FASB issued ASU No. 2017-01, Business Combinations (Topic 805): Clarifying the Definition of a Business (“ASU 2017-01”). This ASU provides a screen to determine when a set is not a business, which requires that when substantially all of the fair value of the gross assets acquired (or disposed of) is concentrated in a single identifiable asset or a group of similar identifiable assets, the set is not a business, which reduces the number of transactions that need to be further evaluated. If the screen is not met, this ASU requires that to be considered a business, a set must include, at a minimum, an input and a substantive process that together significantly contribute to the ability to create output and also remove the evaluation of whether a market participant could replace missing elements. This update is effective for annual and interim periods beginning after December 15, 2017, including interim periods within those periods. ApolloMed is currently assessing the impact the adoption of ASU 2017-01 will have on ApolloMed’s consolidated financial statements.
| 272 |
In January 2017, the FASB issued ASU No. 2017-04, Intangibles – Goodwill and Other (Topic 350): Simplifying the Test for Goodwill Impairment (“ASU 2017-04”). This ASU eliminates Step 2 from the goodwill impairment test if the carrying amount exceeds the fair value of a reporting unit and also eliminated the requirements for any reporting unit with a zero or negative carrying amount to perform a qualitative assessment and, if it fails that qualitative test, to perform Step 2 of the goodwill impairment test. Therefore, the same impairment assessment applies to all reporting units. An entity is required to disclose the amount of goodwill allocated to each reporting unit with a zero or negative carrying amount of net assets. This update is effective for annual and interim periods beginning after December 15, 2019. Early adoption is permitted for interim or annual goodwill impairment tests performed on testing dates after January 1, 2017. ApolloMed is currently assessing the impact the adoption of ASU 2017-04 will have on ApolloMed’s consolidated financial statements.
Off-Balance Sheet Arrangements
As of March 31, 2017, ApolloMed had no off-balance sheet arrangements.
Quantitative and Qualitative Disclosures About Market Risk
As a smaller reporting company, ApolloMed has elected not to provide the disclosure required by this item.
| 273 |
NMM is a California corporation formed in 1994. NMM, together with its subsidiaries and affiliated physician groups, constitutes a patient- and physician-centric, integrated health care delivery and management services company focused on providing coordinated, outcomes-based medical care in a cost-effective manner. Through capitation agreements between NMM’s affiliated physician groups and various health plans, NMM is responsible for coordinating the care for over 600,000 covered patients in southern and central California through a network of over 10 IPAs with approximately 4,000 contracted physicians. These covered patients are comprised of managed care members whose health coverage is provided through their employer or who have individually acquired health coverage directly from a health plan or as a result of their eligibility for Medicaid or Medicare benefits.
The patients of NMM’s affiliated physician groups and IPAs benefit from an integrated approach to medical care that places the physician at the center of patient care. NMM manages the delivery of healthcare services to patients via a network of affiliated physician groups and other network primary care physicians, network hospitals, and affiliated group and network specialists. Together with case managers, registered nurses and other care coordinators, these medical professionals utilize a comprehensive data analysis engine, sophisticated risk management techniques and clinical protocols to provide high-quality, cost effective care to NMM’s managed members. NMM monitors certain control metrics, such as the number of inpatient acute bed days per 1,000 patients and hospital readmission rates, as they are contributors to quality clinical outcomes and financial performance. Additionally, in an effort to identify changes or trends with respect to its commercial, senior and Medicaid payer classifications, NMM closely monitors the number of managed care members who have enrolled with a NMM affiliated physician group as such member’s primary care physician.
NMM’s mission is to transform the delivery of healthcare services in the communities it serves by implementing innovative population health models and creating a patient-centered, physician-centric experience in a high performance environment of integrated care.
NMM serves Medicare, Medicaid, and HMO patients in California who are covered by private or public insurance. NMM provides care coordination services to each major constituent of the healthcare delivery system, including patients, families, primary care physicians, specialists, acute care hospitals, alternative sites of inpatient care, physician groups and health plans.
NMM operates through the following wholly-owned subsidiaries:
| · | AP-ACO; | |
| · | APCN-ACO, Inc.; and | |
| · | 99 Medical Equipment, Healthcare Supplies & Wheelchair Center. |
AP-ACO and APCN-ACO each participates in the MSSP, the goal of which is to improve the quality of patient care and outcomes through more efficient and coordinated approach among providers. ACOs are entities that contract with CMS to serve the Medicare FFS population with the goal of better care for individuals, improved health for populations and lower costs. ACOs share savings with CMS to the extent that the actual costs of serving assigned beneficiaries are below certain trended benchmarks of such beneficiaries and certain quality performance measures are achieved.
On November 11, 2015, NMM, ACO Acquisition Corporation, and APCN-ACO entered into a reorganization agreement whereby ACO Acquisition Corporation, a newly organized entity which NMM is its sole shareholder, merged with APCN-ACO, effective on January 8, 2016, resulting in APCN-ACO becoming a wholly owned subsidiary of NMM.
| 274 |
On December 18, 2016, NMM, ACO Acquisition Corporation #2, and AP-ACO entered into a reorganization agreement whereby ACO Acquisition Corporation #2, a newly organized entity which NMM is its sole shareholder, merged into AP-ACO, effective on December 20, 2016, resulting in AP-ACO becoming a wholly owned subsidiary of NMM.
On January 18, 2017, CMS announced that APAACO, which is owned 50% by NMM, had been approved to participate in the new NGACO Model program. APAACO had applied to participate in the NGACO Model in 2016 and had received conditional approval from CMS in August 2016. Through the NGACO Model, CMS has partnered with APAACO and other ACOs experienced in coordinating care for populations of patients and whose provider groups are willing to assume higher levels of financial risk and reward under the NGACO Model. The NGACO program began on January 1, 2017.
NMM also has a VIE in APC.
APC was incorporated on August 17, 1992 for the purpose of arranging health care services as an IPA. APC has contracts with various HMOs or licensed health care service plans as defined in the Knox-Keene Act. Each HMO negotiates a fixed amount PMPM that is to be paid to APC. In return, APC arranges for the delivery of health care services by contracting with physicians or professional medical corporations for primary care and specialty care services. APC assumes the financial risk of the cost of delivering health care services in excess of the fixed amounts received. Some of the risk is transferred to the contracted physicians or professional corporations. The risk is also minimized by stop-loss provisions in contracts with HMOs.
On July 1, 1999, APC entered into an amended and restated management and administrative services agreement with NMM (initial management services agreement was entered into in 1997) for an initial fixed term of 30 years. In accordance with relevant accounting guidance, APC is determined to be a VIE and NMM is the primary beneficiary with the ability to direct the activities (excluding clinical decisions) that most significantly affect APC’s economic performance through its majority representation of the APC Joint Planning Board; therefore APC is consolidated by NMM. As of December 31, 2016 and 2015, APC owns 6.29% and 6.16%, respectively, of NMM.
CDSC was formed on March 25, 2010 in the state of California. CDSC is an ambulatory surgery center in City of Industry, California that is Medicare Certified and accredited by the Accreditation Association for Ambulatory Healthcare, Inc. During 2011, APC invested $625,000 for an approximately 41% ownership in CDSC. Due to capital stock changes in 2016, APC’s ownership percentage in CDSC’s capital stock changed to 44% and 43% on May 31, 2016 and July 31, 2016, respectively. CDSC is consolidated as a VIE by APC as it was determined that APC has a controlling financial interest in CDSC and is the primary beneficiary of CDSC.
APC-LSMA was formed on October 15, 2012 as a designated shareholder professional corporation and is solely owned by Dr. Thomas Lam, a shareholder and Chief Executive and Financial Officer of APC. APC-LSMA is controlled and consolidated by APC who is the primary beneficiary of this VIE. The only activity of APC-LSMA is to hold the investments in medical corporations, which includes: LMA, PMIOC and DMG.
UCAP, a 100% owned subsidiary of APC, was formed on June 4, 2014, for the purpose of holding the investment in UCI, a privately held health plan that has been in operation since 1985 in order to help its members through the complexities of the healthcare system. UCI holds a license under the Knox-Keene Act to operate as a full-service health plan. UCI contracts with the CMS under the Medicare Advantage Prescription Drug Program. UCAP purchased from UCI 100,000 shares of UCI class A-2 voting common stock (comprising 50% of UCI’s voting common stock) for $10,000,000.
NMM’s principal executive offices are located at 1668 S. Garfield Ave., 2nd Floor, Alhambra, CA 91801, and its telephone number is (626) 282-0288.
| 275 |
U.S. healthcare spending has increased steadily over the past 20 years. According to CMS, the estimated total U.S. healthcare expenditures are expected to grow by 5.6% for 2016 through 2025, and 4.7 percent per year on a per capita basis. Health spending is projected to grow 1.2% faster than the U.S. gross domestic product over the 2016 through 2025 period; as a result the health share of gross domestic product is expected to rise from 17.8% in 2015 to 19.9 percent by 2025.
CMS further reports that health spending growth by federal and state & local governments is projected to outpace growth by private businesses, households, and private payers over the projection period (5.9% compared to 5.4%, respectively) in part due to ongoing strong enrollment growth in Medicare by the baby boomer generation coupled with continued government funding dedicated to subsidizing premiums for lower income marketplace enrollees.
Managed care health plans were developed, primarily during the 1980s, in an attempt to mitigate the rising cost of providing healthcare benefits to populations covered by traditional health insurance. These managed care health plans enroll members through their employers, under federal Medicare benefits or through state Medicaid programs. As a result of the prevalence of these health plans, many seniors now becoming eligible for Medicare have been interacting with managed care companies through their employers for the last 30 years. Individuals turning 65 now are likely to be far more familiar with the managed care setting than previous Medicare populations.
Many health plans recognize both the opportunity for growth from senior members as well as the potential risks and costs associated with managing additional senior members. In California, many health plans subcontract a significant portion of the responsibility for managing patient care to integrated medical systems such as NMM and its affiliated physician groups. These integrated health care systems, or IPAs, offer a comprehensive medical delivery system and sophisticated care management know-how and infrastructure to more efficiently provide for the health care needs of the population enrolled with that health plan. While reimbursement models for these arrangements vary around the country, health plans often prospectively pay the integrated health care system a fixed PMPM amount, or capitation payment, which is often based on a percentage of the amount received by the health plan. The capitation payment is for much—and sometimes virtually all—of the care needs of the applicable membership. Capitation payments to integrated health care systems, in the aggregate, represent a prospective budget from which the system manages care-related expenses on behalf of the population enrolled with that system. To the extent that these systems manage care-related expenses under the capitated levels, the system realizes an operating profit. On the other hand, if care-related expenses exceed projected levels, the system will realize an operating deficit. Since premiums paid represent a significant amount per person, there is a significant revenue opportunity for an integrated medical system, like NMM, that is able to effectively manage health care costs under the capitated arrangements entered into by its affiliated physician groups.
Integrated medical systems, such as NMM and its affiliated physician groups that have scale are positioned to spread an individual member’s cost experience across a wider population and realize the benefits of pooling medical risk among large numbers. In addition, integrated medical systems with years of managed care experience can utilize their sizeable medical claims data to identify specific medical care and quality management strategies and interventions for potential high cost cases and aggressively manage them to improve the health of its population base and, thus, lower cost. Many integrated medical systems, like NMM and its affiliated physician groups, have also established physician performance metrics that allow them to monitor quality and service outcomes achieved by participating physicians in order to reward efficient, high quality care delivered to members and initiate improvement efforts for physicians whose results can be enhanced.
IPAs
An IPA is an association of independent physicians, or other organization that contracts with independent physicians, and provides services to managed care organizations on a negotiated per capita rate, flat retainer fee, or negotiated FFS basis.
| 276 |
Medicare
The Medicare program was established in 1965 and became effective in 1967 as a federally-funded U.S. health insurance program for people aged 65 and older, and it was later expanded to include individuals with end-stage renal disease and certain disabled persons, regardless of income or age. Initially, Medicare was offered only on an FFS basis. Under the Medicare FFS payment system, an individual can choose any licensed physician enrolled in Medicare and use the services of any hospital, healthcare provider or facility certified by Medicare. CMS reimburses providers, based on a fee schedule, if Medicare covers the service and CMS considers it medically necessary.
Growth in Medicare spending is expected to continue to increase due to population demographics. By the year 2030, the number of these elderly persons is expected to climb to 72.8 million, or 20.3% of the total U.S. population.
Medicare Advantage is a Medicare health plan program developed and administered by CMS as an alternative to the traditional FFS Medicare program. Medicare Advantage plans contract with CMS to provide benefits to beneficiaries for a fixed premium PMPM. According to the Kaiser Family Foundation (“Kaiser”), in 2016 Medicare Advantage represented only 31% of total Medicare members, creating a significant opportunity for additional Medicare Advantage penetration of newly eligible seniors. The share of Medicare beneficiaries in such plans has risen rapidly in recent years; according to Kaiser, it reached approximately 33% by the end of open enrollment period in 2017 from approximately 13% in 2004. The reasons for this include that plan costs can be significantly lower than the corresponding cost for beneficiaries in the traditional Medicare FFS program, and plans typically provide extra benefits and provide preventive care and wellness programs.
Many health plans subcontract a significant portion of the responsibility for managing patient care to integrated medical systems such as NMM and its affiliated physician groups. These integrated healthcare systems, whether medical groups or IPAs, offer a comprehensive medical delivery system and sophisticated care management know-how and infrastructure to more efficiently provide for the healthcare needs of the population enrolled with that health plan. Reimbursement models for these arrangements vary around the country. In California, health plans typically prospectively pay the IPA or medical group a fixed PMPM, or capitation payment, which is often based on a percentage of the amount received by the health plan. Capitation payments to IPAs or medical groups, in the aggregate, represent a prospective budget from which the IPA manages care-related expenses on behalf of the population enrolled with that IPA. Those IPAs or medical groups that manage care-related expenses under the capitated levels will realize an operating profit; if care-related expenses exceed projected levels, the IPA will realize an operating deficit.
Integrated healthcare delivery companies such as NMM and its affiliated physician groups can utilize their medical care and quality management strategies and interventions for potential high cost cases and aggressively manage them to improve the health of its population and therefore lower costs for these patients. Additionally, IPAs and medical groups such as APC have established physician performance metrics that allow them to monitor quality and service outcomes achieved by participating physicians in order to reward efficient, high quality care delivered to members and to initiate improvement efforts for physicians whose results can be enhanced.
Medicaid
Medicaid is a federal entitlement program administered by the states that provides healthcare and long-term care services and support to low-income Americans. Medicaid is funded jointly by the states and the Federal government. The federal government guarantees matching funds to states for qualifying Medicaid expenditures based on each state’s federal medical assistance percentage, which is calculated annually and varies inversely with the average personal income in the state. Each state establishes its own eligibility standards, benefit packages, payment rates and program administration within federal guidelines. In an effort to improve quality and provide more uniform and cost-effective care, many states have implemented Medicaid managed care programs to improve access to coordinated care, to improve preventive care and to control healthcare costs. Under Medicaid managed care programs, a health plan receives capitation payments from the state. The health plan then arranges for healthcare services to be provided by contracting either directly with providers or with IPAs and medical groups, such as MMG. MMG has entered into capitation agreements with health plans, either directly or through an MSO.
| 277 |
NMM believes recognition of the value of managed care as a means of delivering improved health outcomes for Medicaid beneficiaries and effectively controlling costs will continue to strengthen. A growing number of states have mandated that their Medicaid recipients enroll in managed care plans. Other states are considering moving to a mandated managed care approach. As a result, NMM believes a significant market opportunity exists for managed care organizations with operations and programs focused on the distinct socio-economic, cultural and healthcare needs of the uninsured population and the Medicaid populations.
Commercial
Patients enrolled in health plans offered through their employers are generally referred to as commercial members. According to the United States Census Bureau, in 2014, the last year for which data is available, approximately 55.4% of non-elderly U.S. citizens received their healthcare benefits through their employers, which contracted with health plans to administer these healthcare benefits. Nationally, commercial employer-sponsored health plan enrollment was approximately 150 million in 2015.
Dual Eligibles
A portion of Medicaid beneficiaries are dual eligibles, meaning that they are low-income seniors and people with disabilities who are enrolled in both Medicaid and Medicare. Based on CMS estimates, there are approximately 10.7 million dual eligible enrollees with annual spending of approximately $285 billion. Only a small percentage of the total spending on dual eligibles is administered by managed care organizations. Dual eligibles tend to consume more healthcare services due to their tendency to have more chronic conditions. In some states, dual eligible patients are being voluntarily enrolled and/or auto-assigned into managed care programs. About 1.1 million low-income seniors and people with disabilities in California receive health care services through both the Medicare and Medi-Cal (Medicaid nationally) programs.
Health Reform Acts
In an effort to reduce the number of uninsured and intending to control healthcare expenditures, President Obama signed the Health Reform Acts. The Health Reform Acts seek a reduction of up to 32 million uninsured individuals by 2019, while potentially increasing Medicaid coverage by up to 16 million individuals and net commercial coverage by 16 million individuals. CMS projects that the total number of uninsured Americans will fall to 23 million by 2023 from 45 million in 2012. The current enrollment numbers (as of February 2016) are roughly 20 million total between the ACA between the marketplace. The uninsured rate remains at an all-time low with 10.9% of under 65 uninsured as of 4th quarter 2016 according to CDC data. NMM believes that this represents a significant new market opportunity for health plans and integrated healthcare delivery companies. Efforts to amend, or repeal and replace, the ACA and Health Reform Acts could have a material impact on NMM’s business and market opportunities.
The ACA made broad-based changes to the U.S. health care system. As a result of the election of President Trump and the GOP control of both houses of Congress, there is currently a great deal of discussion and debate about the repeal and replacement of the ACA. As a result, the future of the ACA and its underlying programs are subject to substantial uncertainty, making long-term business planning exceedingly difficult. NMM is unable to predict with any degree of certainty whether the ACA will be modified or repealed in its entirety, and if it is repealed, what it will be replaced with; nor is NMM able to predict when any such changes, if enacted, would become effective.
On January 20, 2017, the President signed an executive order that gives the regulatory agencies that enforce the ACA the authority to interpret regulations issued under the ACA in a way that limits fiscal burdens on states and financial or regulatory burdens on individuals, providers, health insurers and others. The practical implications of that order are unclear, and the future of the ACA is uncertain. Currently, there are a number of different legislative proposals being considered, some of which would involve significantly reduced federal spending on the Medicaid program, and constitute a fundamental change in the federal role in health care. These proposals include elements such as the following: ending the entitlement nature of Medicaid (and perhaps Medicare as well) by capping future increases in federal health spending for these programs, and shifting much more of the risk for health costs in the future to states and consumers; reversing the ACA’s expansion of Medicaid that enables states to cover low-income childless adults; changing Medicaid to a state block grant program, including potentially capping spending on a per-enrollee basis; prohibiting the federal government from operating health exchanges; and eliminating the advanced premium tax credits.
| 278 |
Furthermore, in the states that have elected to participate, the ACA provided for the expansion of the Medicaid program to offer eligibility to nearly all low-income people under age 65 with incomes at or below 138% of the federal poverty line. NMM’s affiliated medical groups have benefited from the Medicaid expansion program under the ACA. If the Medicaid expansion is reversed by repeal of the ACA, it could result in loss of Medicaid expansion membership to NMM’s affiliated medical groups, which could have a material adverse effect on its business, financial condition, cash flows, or results of operations. For additional information on federal and state health care reform, refer to “RISK FACTORS - Risks Related to NMM.”
ACOs
One provision of the Health Reform Acts required CMS to establish an MSSP that promotes accountability and coordination of care through the creation of ACOs, which, as described below, are eligible to participate in some of the savings generated by such ACOs. The Medicare FFS program was designed for beneficiaries in the Medicare FFS program. CMS established the MSSP to facilitate coordination and cooperation among providers to improve the quality of care and reduce unnecessary costs. Eligible providers, hospitals and suppliers may participate in the MSSP by creating an ACO and then applying to CMS. MSSP ACOs must have at least 5,000 Medicare beneficiaries in order to be eligible to participate in the program.
The MSSP is designed to improve beneficiary outcomes and increase value of care by (1) promoting accountability for the care of Medicare FFS beneficiaries; (2) requiring coordinated care for all services provided under Medicare FFS; and (3) encouraging investment in infrastructure and redesigned care processes. The MSSP rewards ACOs that lower their healthcare costs while meeting performance standards on quality of care and patient satisfaction. Under the final MSSP rules, Medicare will continue to pay individual providers and suppliers for specific items and services as it currently does under the FFS payment system. The MSSP rules require CMS to develop a benchmark for savings to be achieved by each ACO if the ACO is to receive shared savings. An ACO that meets the program’s quality performance standards will be eligible to receive a share of the savings to the extent its assigned beneficiary medical expenditures are below the medical expenditure benchmark provided by CMS. A minimum savings rate (“MSR”) must be achieved before the ACO can receive a share of the savings. Once the MSR is surpassed, all the savings below the benchmark provided by CMS will be shared 50% with the ACO. The MSR varies depending on the number of patients assigned to the ACO, starting at 3.9% for ACOs with patients totaling 5,000 and increasing to 2% for ACOs with more than 60,000 patients. The MSSP program is an all-or-nothing system, that is, an ACO either earns all of its allocable savings or none of it. In performance year 2014 (fiscal 2016), NMM did not receive an MSSP payment from CMS. Although NMM exceeded its total benchmark expenditures, generating $3.9 million in total savings and achieving an ACO Quality Score of 90.4% on its Quality Performance Report, CMS determined that NMM did not meet the minimum savings threshold in performance year 2015 and therefore did not receive the “all or nothing” annual shared savings payment in fiscal 2017. NMM is eligible to be considered for an all-or-nothing payment under this program for performance year 2016 (which, if it is paid, would be paid to NMM in fiscal 2018). However, NMM does not believe that it will be eligible to receive payments for performance years beginning 2017, because of its transition to, and business focus on, the NGACO Model, in which it is participating as of January 1, 2017.
CMS assigns a beneficiary to the preliminary roster of an ACO if the ACO physicians billed for a “plurality” of services during the calendar year preceding the performance period. A plurality means the ACO physicians provided a greater proportion of primary care services, measured in terms of allowed charges, than the physicians in any other ACO or Medicare-enrolled tax identification number. CMS sets the benchmark for each ACO using the historical medical costs of the beneficiaries assigned to the ACO. Under the final MSSP rules, primary care physicians may only join one ACO, unless they have more than one Medicare tax identification number.
| 279 |
In January 2016, CMS announced the first batch of participants in the NGACO Model. CMS is implementing the NGACO Model under section 1115A of the Social Security Act, which authorizes CMS, through its Center for Medicare and Medicaid Innovation, to test innovative payment and service delivery models that have the potential to reduce Medicare, Medicaid or Children’s Health Insurance Program expenditures while maintaining or improving the quality of beneficiaries’ care. The purpose of the NGACO Model is to test an alternative Medicare ACO payment model. Specifically, this model will test whether health outcomes improve and Medicare Parts A and B expenditures for Medicare FFS beneficiaries decrease if Medicare ACOs (1) accept a higher level of financial risk compared to existing Medicare ACO payment models, and (2) are permitted to select certain innovative Medicare payment arrangements and to offer certain additional benefit enhancements to their assigned Medicare FFS beneficiaries. On January 18, 2017, CMS announced that APAACO had been approved to participate in the NGACO Model. Through this new model, CMS will partner with APAACO and other ACOs experienced in coordinating care for populations of patients and whose provider groups are willing to assume higher levels of financial risk and reward under the NGACO Model. APAACO began operations on January 1, 2017.
To position itself to participate in the NGACO Model, NMM has devoted, and intends to continue to devote, significant effort and resources, financial and otherwise, to the NGACO Model.
MSO
NMM provides management services to medical companies and IPAs, including the following services:
| • | Medical management, including utilization management and quality assurance |
| • | Care coordination in the inpatient and outpatient settings using case managers |
| • | High-risk management of patients with multiple chronic conditions |
| • | Physician and health plan contracting |
| • | Pre-negotiating contracts with specialists, labs, imaging centers, nursing homes and other vendors |
| • | Physician recruiting |
| • | Provider relations |
| • | Member services, including annual wellness evaluations |
| • | Education of physicians on proper coding |
| • | Data collection and analysis |
| • | Population health management, a population health management and analytics platform to analyze monthly claims data from CMS and data collected from each physician’s practice |
| • | Educating NMM’s physicians |
| • | Promote use of evidence-based medicine by NMM’s affiliated physicians |
| 280 |
IPAs
NMM’s affiliated IPAs are comprised of a network of independent primary care physicians and specialists who collectively care for HMO patients typically under either a capitated payment arrangement. Under the capitated model, an HMO pays an IPA a PMPM rate, or a “capitation” payment, and then assigns the IPA the responsibility for providing the physician services required by the applicable patients. The physicians in the IPA are exclusively in control of, and responsible for, all aspects of the practice of medicine for enrolled patients. An IPA enters into contracts with HMOs to provide physician services to enrollees of the HMOs. Most of the HMO agreements have an initial term of two years renewing automatically for successive one-year terms. The HMO agreements generally provide for a termination by the HMOs for cause at any time. The HMO agreements generally allow either party to terminate the HMO agreements without cause typically with a four to six month notice.
ACOs
NMM currently owns two MSSP ACOs, AP-ACO and APCN-ACO and co-owns one NGACO with ApolloMed, APAACO. ACOs are entities that contract with CMS to serve the Medicare FFS population with the goal of better care for individuals, improved health for populations and lower costs. ACOs share savings with CMS to the extent that the actual costs of serving assigned beneficiaries are below certain trended benchmarks of such beneficiaries and certain quality performance measures are achieved.
AP-ACO and APCN-ACO
On November 11, 2015, NMM, ACO Acquisition Corporation, and APCN-ACO entered into a reorganization agreement whereby ACO Acquisition Corporation, a newly organized entity which NMM is its sole shareholder, merged with APCN-ACO, effective on January 8, 2016, resulting in APCN-ACO becoming a wholly owned subsidiary of NMM.
On December 18, 2016, NMM, ACO Acquisition Corporation #2, and AP-ACO entered into a reorganization agreement whereby ACO Acquisition Corporation #2, a newly organized entity which NMM is its sole shareholder, merged into AP-ACO, effective on December 20, 2016, resulting in AP-ACO becoming a wholly owned subsidiary of NMM.
The member relationship assets acquired from both APCN-ACO and AP-ACO represent member lives that are to be utilized by APAACO, an entity owned 50% by NMM and 50% by ApolloMed. These member relationships acquired in 2016 were reenrolled under APA-ACO on January 1, 2017. Members of APCN-ACO and AP-ACO may opt out of the automatic enrollment into APAACO.
APAACO
On January 18, 2017, CMS announced that APAACO had been approved to participate in the NGACO Model. APAACO had applied to participate in the NGACO Model in 2016 and had received conditional approval from CMS in August 2016. The NGACO Model is a new CMS program that builds upon previous ACO programs. Through this new model, CMS will provide an opportunity to APAACO and other ACOs experienced in coordinating care for populations of patients and whose provider groups are willing to assume higher levels of financial risk and reward to participate in this new attribution-based risk sharing model. As discussed in more detail below, there are different levels of financial risk and reward a NGACO may select, and the extent of risk and reward may be limited on a percentage basis.
APAACO began operations on January 1, 2017. Under the NGACO Model, APAACO will be responsible for the medical management and care coordination of over 32,000 Medicare beneficiaries in California. This number may decrease due to beneficiaries who join a managed care (HMO) plan, pass away or move out of the service area. In 2016, APAACO signed agreements with over 700 providers, including more than 590 physicians, 18 hospitals, more than 15 skilled nursing facilities and multiple labs, radiology centers, outpatient surgery centers, dialysis clinics and other service providers. Under the terms of APAACO’s agreements with these parties, the NGACO Model providers, including hospitals, agreed to receive 100% of their claims for ACO beneficiaries reimbursed by APAACO. APAACO negotiated discounted Medicare rates with multiple physicians and other service providers, discounted diagnosis-related group rates with multiple hospitals and discounted resource utilization group rates with multiple skilled nursing facilities.
| 281 |
In connection with the approval by CMS for APAACO to participate in the NGACO Model, CMS and APAACO have entered into the Participation Agreement. AMM has a long-term MSA with APAACO. The term of the Participation Agreement is two performance years, through December 31, 2018. CMS may offer to renew the Participation Agreement for an additional two performance years. Additionally, the Participation Agreement may be terminated sooner by CMS as specified therein, and CMS has the authority to alter or change the program over this time period.
Among many requirements to be eligible to participate in the NGACO Model, ACOs must have at least 10,000 assigned Medicare beneficiaries and must maintain that number throughout each performance year. APAACO started its performance year with 32,078 assigned Medicare beneficiaries.
The NGACO Model uses a prospectively-set cost benchmark, which is established prior to the start of each performance year. The benchmark is based on four factors:
Baseline: The 2017 performance year NGACO Model baseline for APAACO is based on calendar year 2014 expenditures. The baseline is updated each year to reflect the NGACO’s participant list for the given year.
Trend: A projected trend that is similar to the national projected trend used in the Medicare Advantage program.
Risk Adjustment: To account for differing medical condition acuity of an ACO’s beneficiaries. The risk adjustment is based on Hierarchical Condition Category (“HCC”) risk scores. The ACO’s full HCC risk score has an annual cap of up to 3%.
Discount: Unlike the MSSP ACO program, the NGACO Model does not utilize a Minimum Savings Rate. Instead, CMS applies a discount to the benchmark once the baseline has been calculated, trended and risk-adjusted. The base discount is 2.25% and can range from 0% to 3% depending on the three factors of (1) regional efficiency, (2) national efficiency and (3) quality score attained by the ACO.
NGACOs must provide a financial guarantee to CMS. The financial guarantee must be in an amount equal to 2% of its total capped Medicare Part A and Part B expenditures for beneficiaries. CMS allows the following forms of financial guarantees: (1) funds placed in an escrow amount; (2) a line of credit as evidenced by a letter of credit upon which only CMS may draw; or (3) a surety bond.
APAACO’s total capped Medicare Part A and Part B expenditures were approximately $335 million for performance year 1, and therefore APAACO submitted a letter of credit for $6.7 million to CMS.
As required by the Participation Agreement, APAACO shall maintain an aligned population of at least 10,000 beneficiaries during each performance year. APAACO and its participants may not participate in any other Medicare shared savings initiatives. APAACO shall require its participants and preferred providers to make medically necessary covered services available to beneficiaries in accordance with applicable laws, regulations and guidance.
APAACO shall implement processes and protocols that relate to specified objectives for patient-centered care consistent with the NGACO model. In connection therewith, APAACO shall require its participants to comply with and implement these designated processes and protocols, and shall institute remedial processes and penalties, as appropriate, for participants that fail to comply with or implement a required process or protocol.
| 282 |
CMS shall use APAACO’s quality scores calculated under the relevant provisions of the Participation Agreement to determine, in part, its “Performance Year Benchmark”. CMS shall assess APAACO’s quality performance using the quality measures set forth in the Participation Agreement and the quality measure data required to be reported by APAACO as set forth in the Participation Agreement. CMS shall use APAACO’s performance on each of the quality measures to calculate its total quality score according to a methodology to be determined by CMS prior to the start of each performance year. For each performance year, CMS shall determine APAACO’s Performance Year Benchmark. No later than 15 days before the beginning of each performance year, CMS shall provide the ACO with a Performance Year Benchmark Report consisting of APAACO’s Performance Year Benchmark. On a quarterly basis during each performance year, CMS shall provide APAACO with a Quarterly Financial Report. The Quarterly Financial Report may comprise adjustments to the Performance Year Benchmark resulting from updated information regarding any factors that affect the Performance Year Benchmark calculation.
For each performance year, APAACO shall submit to CMS its selections for risk arrangement; the amount of a savings/loss cap; alternative payment mechanism; benefits enhancements, if any; and its decision regarding voluntary alignment under the NGACO Model. APAACO must obtain CMS consent before voluntarily discontinuing any benefit enhancement during a performance year.
For each performance year, CMS shall pay APAACO in accordance with the alternative payment mechanism, if any, for which CMS has approved APAACO; the risk arrangement for which APAACO has been approved by CMS; and as otherwise provided in the Participation Agreement. Following the end of each performance year, and at such other times as may be required under the Participation Agreement, CMS will issue a settlement report to APAACO setting forth the amount of any shared savings or shared losses and the amount of other monies owed. If CMS owes APAACO shared savings or other monies owed, CMS shall pay the ACO in full within 30 days after the date on which the relevant settlement report is deemed final, except as provided in the Participation Agreement. If APAACO owes CMS shared losses or other monies owed as a result of a final settlement, APAACO shall pay CMS in full within 30 days after the relevant settlement report is deemed final. If APAACO fails to pay the amounts due to CMS in full within 30 days after the date of a demand letter or settlement report, CMS shall assess simple interest on the unpaid balance at the rate applicable to other Medicare debts under current provisions of law and applicable regulations. In addition, CMS and the U.S. Department of the Treasury may use any applicable debt collection tools available to collect any amounts owed by APAACO.
Unless specifically permitted under the Participation Agreement, APAACO participants, preferred providers and other individuals or entities performing functions and services related to ACO activities are prohibited from providing gifts or other remuneration to beneficiaries to induce them to receive items or services from APAACO, its participants or preferred providers, or to induce them to continue to receive items or services from APAACO, its participants or preferred providers.
APAACO shall maintain the privacy and security of all NGACO-related information that identifies individual beneficiaries in accordance with HIPAA, Privacy and Security Rules and all relevant HIPAA guidance applicable to the use and disclosure of protected health information by covered entities, as well as applicable state laws and regulations.
The Participation Agreement requires APAACO to report specified information on a publicly accessible website maintained by it, which information includes organizational information, shared savings and shares losses information, and performance on quality measures.
The NGACO Model offers two risk arrangement options. In Arrangement A, the ACO takes 80% of Medicare Part A and Part B risk. In Arrangement B, the ACO takes 100% of Medicare Part A and Part B risk. Under each risk arrangement, the ACO can cap aggregate savings and losses anywhere between 5% to 15%. The cap is elected annually by the ACO. APAACO has opted for Risk Arrangement A and a shared savings and losses cap of 5%.
The NGACO Model offers four payment mechanisms:
| · | Payment Mechanism #1: Normal FFS. |
| · | Payment Mechanism #2: Normal FFS plus Infrastructure payments of $6 PBPM. |
| 283 |
| · | Payment Mechanism #3: PBP. PBP payments provide ACOs with a monthly payment to support ongoing ACO activities. ACO participants and preferred providers must agree to percentage payment fee reductions, which are then used to estimate a monthly PBP payment to be received by the ACO. |
| · | Payment Mechanism #4: AIPBP. Under this mechanism, CMS will estimate the total annual expenditures of the ACO’s aligned beneficiaries and pay that projected amount in PBPM payments. ACOs in AIPBP may have alternative compensation arrangements with their providers, including 100% FFS, discounted FFS, capitation or case rates. |
APAACO began operations on January 1, 2017. APAACO opted for, and was approved by CMS to participate in, the AIPBP track, which is the most advanced risk-taking payment model, effective April 1, 2017. APAACO is the only ACO in the United States out of 44 approved NGACOs that is participating in the AIPBP track. Under the AIPBP track, CMS will estimate the total annual expenditures for APAACO's patients and then pay that projected amount to NMM in a PBPM payment. NMM would then be responsible for paying all Part A and Part B costs for in-network participating providers and preferred providers with whom it has contracted.
The NGACO Model provides ACOs with additional tools not found in the ACO programs, but that are used in the Medicare Advantage program to improve quality and lower cost, including preferred provider networks, negotiated discounts and beneficiary incentives.
AMM has entered into the APAACO MSA. Under the APAACO MSA, AMM provides APAACO with care coordination, data analytics and reporting, technology and other administrative capabilities to enable participating providers to deliver better care and lower healthcare costs for their Medicare FFS beneficiaries. APAACO employs local operations and clinical staff to drive physician engagement and care coordination improvements.
| 284 |
NMM generates revenue through various contractual agreements which vary in both structure and by type of business operation. These contracts are multi-year renewable contracts that include traditional FFS, capitation, case rates, and professional and institutional risk contracts. NMM’s revenue streams consist primarily of capitation revenue, risk pool settlements and incentives, management fee income, surgery center income and FFS.
Capitation revenue
Capitation revenue represents revenue that APC generates based on agreements that generally make it liable for excess medical costs. Managed care revenues of APC consist primarily of capitated fees for medical services provided by APC under a PSA or capitated arrangements directly made with various managed care providers including HMO’s and MSOs. Capitation revenue under the PSA and HMO contracts is prepaid monthly to APC based on the number of enrollees electing APC as their healthcare provider. Health plans and providers with higher acuity enrollees will receive more and those with lower acuity enrollees will receive less.
The use of capitation under PSAs is intended to control the use of health care resources by putting APC at financial risk for services provided to patients. Capitation is a fixed amount of money per patient per unit of time paid in advance for the delivery of health care services. The actual amount of money paid to APC is determined by the ranges of services that APC provides, the number of patients involved, and the period of time during which the services are provided. Capitation rates under APC’s PSAs are generally based on local costs and average utilization of services. To ensure that contracting physicians provide necessary care to their patients, NMM monitors and measures rates of resource utilization in physician practices and submits reports to contracted health plans, which can be linked to financial rewards, such as bonuses. For example, APC receives incentives under “pay-for-performance” programs for quality medical care, based on various criteria.
Additionally, Medicare pays capitation using a “risk adjustment” model, which compensates managed care organizations and providers based on the health status (acuity) of each individual enrollee. Health plans and providers with higher acuity enrollees receive more and those with lower acuity enrollees receive less. Under risk adjustment, capitation is determined based on health severity, measured using patient encounter data. Capitation is paid on an interim basis based on data submitted for the enrollee for the preceding year and is adjusted in subsequent periods after the final data is compiled.
Risk Pool Settlements and Incentives
Contracts with HMO’s also include provisions for APC to participate in the risk (shared risk capitation arrangements) relating to the provision of institutional services (institutional risk) to enrollees, such that APC can earn additional incentive revenue or incur losses based upon the enrollee utilization of hospital services. Typically, any shared risk deficits are not payable until and unless APC generates future risk sharing surpluses, or if the HMO withholds a portion of the capitation revenue to fund any risk share deficits. At the termination of the HMO contract, any accumulated risk share deficit is typically extinguished. In addition to risk sharing revenues, APC is also eligible to participate in an incentive program. As an incentive to control enrollee utilization and to promote quality care, the HMOs have designed the quality incentive programs and commercial generic pharmacy incentive programs to compensate APC for efforts it takes to improve the quality of services and for efficient and effective use of pharmacy supplemental benefits provided to the HMO’s members. The incentive programs track specific performance measures and calculate payments to the IPA based on the performance measures.
| 285 |
APC also has entered into risk sharing arrangements with affiliated hospitals (full risk capitation arrangements) who in turn have entered into capitation arrangements with various HMOs, pursuant to which the affiliated hospital provides, arranges and pays for institutional risk. Under a risk pool sharing agreement, APC is allocated a percentage of the affiliated hospitals surplus or deficit from the risk pool, after deductions for the affiliated hospitals costs.
Management Fee Income
NMM provides claims processing and other administrative services for other IPAs. NMM receives management fee income for the services rendered. Management fees are calculated as a percentage of revenue under capitation contracts with various insurance companies.
Surgery Center Income
CDSC’s surgery center income consists primarily of net patient service revenues that are based upon established billing rates. Third-party payor contractual payment terms are generally based upon predetermined rates per procedure or FFS rates.
FFS revenue
FFS revenue represents revenue earned under agreements for certain reimbursable services in which NMM bills and collects the professional component of charges for medical services rendered by its contracted and employed physicians. Under its FFS arrangements, NMM bills for services provided and receives payment from health plans. All services provided are expected to result in cash flows and are therefore reflected as net revenue in NMM’s consolidated financial statements.
NGACO Model
Through APAACO, NMM participates in the NGACO Model sponsored by CMS. For each performance year, CMS will determine APAACO’s Performance Year Benchmark. No later than 15 days before the beginning of each performance year, CMS will provide APAACO with a Performance Year Benchmark Report consisting of APAACO’s Performance Year Benchmark. On a quarterly basis during each performance year, CMS shall provide APAACO with a Quarterly Financial Report. The Quarterly Financial Report may comprise adjustments to the Performance Year Benchmark resulting from updated information regarding any factors that affect the Performance Year Benchmark calculation. For each performance year, APAACO will submit to CMS its selections for risk arrangement; the amount of a savings/loss cap; alternative payment mechanism; benefits enhancements, if any; and its decision regarding voluntary alignment under the NGACO model. APAACO must obtain CMS consent before voluntarily discontinuing any benefit enhancement during a performance year.
For each performance year, CMS will pay APAACO in accordance with the alternative payment mechanism, if any, for which CMS has approved APAACO; the risk arrangement for which APAACO has been approved by CMS; and as otherwise provided in the Participation Agreement. Following the end of each performance year, and at such other times as may be required under the Participation Agreement, CMS will issue a settlement report to APAACO setting forth the amount of any shared savings or shared losses and the amount of other monies owed. If CMS owes APAACO shared savings or other monies owed, CMS will pay APAACO in full within 30 days after the date on which the relevant settlement report is deemed final, except as provided in the Participation Agreement. If APAACO owes CMS shared losses or other monies owed as a result of a final settlement, APAACO shall pay CMS in full within 30 days after the relevant settlement report is deemed final. If APAACO fails to pay the amounts due to CMS in full within 30 days after the date of a demand letter or settlement report, CMS will assess simple interest on the unpaid balance at the rate applicable to other Medicare debts under current provisions of law and applicable regulations. In addition, CMS and the U.S. Department of the Treasury may use any applicable debt collection tools available to collect any amounts owed by APAACO.
| 286 |
NMM’s NGACO operations began on January 1, 2017. APAACO was approved to participate in the AIPBP track, which is the most advanced risk-taking payment model, effective April 1, 2017. APAACO is the only ACO in the United States out of 44 approved NGACOs that is participating in the AIPBP model. Under the AIPBP track, CMS will estimate the total annual expenditures for APAACO's patients and then pay that projected amount to NMM in a per-beneficiary, per-month payment. NMM would then be responsible for paying all Part A and Part B costs for in-network participating providers and preferred providers with whom it has contracted.
NMM’s business and operations are located exclusively in California, and all of NMM’s revenue is derived from its operations in California. As of March 31, 2017, through capitation agreements with some of the nation’s leading health plans, NMM is responsible for coordinating the care for over 600,000 covered patients in southern and central California through a network of approximately 10 IPAs with approximately 4,000 contracted physicians. These covered patients are comprised of managed care members whose health coverage is provided through their employer or who have individually acquired health coverage directly from a health plan or as a result of their eligibility for Medicaid or Medicare benefits. Additionally, NMM had approximately 32,000 beneficiaries in its NGACO, exclusively in California at the start of its performance year in January 2017.
NMM’s mission is to transform the delivery of health services to the communities it serves by implementing innovative population health and care coordination models and by creating a patient-centered, physician-centric experience in a high-performing environment of integrated care.
NMM’s current intention is to implement its strategy through a combination of organic growth and acquisitions, as well as dispositions when appropriate. While it has taken many concrete steps to achieve its strategy, there is no guarantee that it will be successful in these endeavors and it may not achieve its strategic goals. The principal elements of NMM’s growth strategy are:
Pursue growth opportunities in established markets
NMM identifies growth opportunities in established markets it serves by working with its local network physicians. Opportunities may include continued physician enrolment for APC and APAACO, new risk-based insurance contracts and new acquisitions.
Continue to strengthen NMM’s market presence and reputation
NMM positions itself to thrive in a changing healthcare environment by continuing to build and operate high-performing, patient-centered care networks, fully engaging in health and wellness, and enhancing its reputation in its markets. NMM focuses particularly on patient safety, patient satisfaction, care coordination, population health and implementing clinical quality best practices across all its operations. NMM measures the health status of its patients with the goal of directly improving their health.
Focus on high-quality, patient-centered care
NMM provides high-quality, patient-centered care in its communities. NMM has implemented several initiatives to maintain and enhance the delivery of high-quality care, including clinical best practices, information technology and tools, coordination of care, annual wellness exams and population health.
| 287 |
Drive physician collaboration and alignment
NMM fosters a collaborative approach among its physicians to provide what it believes to be clinically superior healthcare services. NMM provides medical management, population health management and care coordination resources to its physicians sufficient to support the necessary, high-quality services to its patients. NMM has implemented several initiatives, including active participation of physician leadership in APC, APAACO, and hospital boards and subcommittees, training programs and information technology resources. In addition, NMM is aligning with its physicians in various forms of risk contracting, including pay-for-performance programs such as clinical documentation improvement to improve RAF scores and certain programs, such as annual wellness visits, to improve Medicare Advantage STAR ratings.
Expand population health strategies
NMM is flexible and competitive in a dynamic healthcare environment. NMM intends to continue to add medical management and population health management resources to pursue further strategies in physician practice management and population health services, such as predictive analytics and telemedicine services.
Pursue selective acquisitions
NMM believes that its philosophy, built on patient-centered healthcare and clinical quality and efficiency, gives it a competitive advantage in expanding its services in its existing markets as well as other markets through acquisitions or partnerships. NMM regularly monitors opportunities to acquire IPAs, ACOs and other synergistic health care providers that fit its vision and long-term strategies.
Expand its relationships with payors and facilities in selective markets across the United States
NMM intends to explore ways to develop relationships with existing and new health plans and hospitals in selective markets across the United States.
Acquisitions and Dispositions
In furtherance of its growth strategy, NMM regularly evaluates opportunities to add to its portfolio of healthcare companies in areas where it does not have a presence, in order to expand its geographic footprint, in areas where it already has a presence to increase its market share, and in areas of practice that are complementary to its existing business model. Similarly, NMM periodically evaluates parts of its business that may not fit within its overall business model or may be underperforming and, when appropriate, NMM may dispose of such companies.
On July 1, 2015, NMM merged with PIPA MSO with NMM being the surviving entity. PIPA MSO was organized for the purpose of providing management services to medical groups and IPAs. The management service covers billing, collection, accounting, administrative, non-physician personnel staffing, and marketing. NMM acquired the operational and management processes associated with providing management services to medical groups and IPAs.
On April 1, 2015, APC merged with PHW, with APC being the surviving entity.
On November 11, 2015, NMM, ACO Acquisition Corporation, and APCN-ACO entered into a reorganization agreement whereby ACO Acquisition Corporation, a newly organized entity in which NMM is its sole shareholder, merged with APCN-ACO, effective on January 8, 2016. APCN-ACO operates an ACO, as defined under the MSSP, which is comprised of the ACO’s network of independent medical practices. The primary reason for the business combination was for NMM to acquire the member relationships of APCN-ACO. Immediately following the effective date, NMM became the sole shareholder of APCN-ACO.
| 288 |
On December 18, 2016, NMM, ACO Acquisition Corporation #2, and AP-ACO entered into a reorganization agreement whereby ACO Acquisition Corporation #2, a newly organized entity which NMM is its sole shareholder, merged into AP-ACO, effective on December 20, 2016. AP-ACO operates an ACO, as defined under the MSSP, which is comprised of the ACO’s network of independent medical practices. The primary reason for the business combination was for NMM to acquire the member relationships of AP-ACO. Immediately following the effective date, NMM became the sole member of AP-ACO.
The member relationship assets acquired from both APCN-ACO and AP-ACO represent member lives that are to be utilized by APAACO, an entity owned 50% by NMM and 50% by ApolloMed, and is also a NGACO, which was approved in January 2017. These member relationships acquired in 2016 were reenrolled under APA-ACO on January 1, 2017. Members of APCN-ACO and AP-ACO may opt out of the automatic enrollment into APA-ACO.
Corporate Practice of Medicine
NMM’s consolidated financial statements include NMM’s subsidiaries and its VIE, APC. Some states have laws that prohibit business entities with non-physician owners, such as NMM, from practicing medicine, which are generally referred to as corporate practice of medicine. States that have corporate practice of medicine laws require only physicians to practice medicine, exercise control over medical decisions or engage in certain arrangements with other physicians, such as fee-splitting. California is a corporate practice of medicine state. Therefore, in California, NMM operates by maintaining long-term management service agreements with its affiliates, each of which are owned and operated by physicians only, and which employ or contract with additional physicians to provide medical services. Under MSAs, NMM provides and performs all non-medical management and administrative services, including financial management, information systems, marketing, risk management and administrative support.
Through the MSAs and the relationship with the physician owners of its medical affiliates, NMM has exclusive authority over all non-medical decisions related to the ongoing business operations of those affiliates.
When necessary, Dr. Thomas Lam, NMM’s Chief Executive Officer, through APC-LSMA (in which Dr. Lam is the sole shareholder), serves as nominee shareholder, on NMM’s behalf, of affiliated medical practices, in order to comply with corporate practice of medicine laws.
The healthcare industry is highly competitive and fragmented across all of NMM’s services and operations. NMM competes for customers with many other health care management companies and healthcare providers, including local physicians and practice groups as well as local, regional and national networks of physicians, hospitals and other healthcare companies, many of which are substantially larger than NMM and have significantly greater financial and other resources, including personnel, than NMM has.
IPAs
NMM’s affiliated IPA, APC, competes with other IPAs, medical groups and hospitals, many of whom have greater financial, personnel and other resources available to them. For example, in Los Angeles, examples of NMM’s competitors include Regal Medical Group and Lakeside Medical group, which are part of Heritage, as well as HealthCare Partners, which is owned by DaVita.
ACOs
NMM ACO and APAACO compete with hospitals, sophisticated provider groups, and MSOs in the creation, administration, and management of ACOs, many of whom have greater financial, personnel and other resources available to them. For example, in Los Angeles, competitors with APAACO include Heritage California ACO and DaVita Medical ACO California.
| 289 |
Professional Liability and Other Insurance Coverage
NMM’s business has an inherent and significant risk of claims of medical malpractice against its affiliated physicians and against NMM. NMM and its affiliated physician groups pay premiums for third-party professional liability insurance that provides indemnification on a claims-made basis for losses incurred related to medical malpractice litigation.
While NMM believes that its insurance coverage is adequate based upon its claims experience and the nature and risks of its business, NMM cannot be certain that its insurance coverage will be adequate to cover liabilities arising out of claims asserted against it or its affiliated professional organizations in the future where the outcomes of such claims are unfavorable. NMM believes that the ultimate resolution of all pending claims, including liabilities in excess of its insurance coverage, will not have a material adverse effect on its financial position, results of operations or cash flows; however, there can be no assurance that future claims will not have such a material adverse effect on NMM’s business.
NMM also maintains worker’s compensation, director and officer, and other third-party insurance coverage subject to deductibles and other restrictions that it believes are in accordance with industry standards. NMM believes that these insurance coverage limits are appropriate based upon its claims experience and the nature and risks of its business. However, it cannot assure that any pending or future claim will not be successful or, if successful, will not exceed the limits of available insurance coverage.
APC has purchased stop-loss insurance, which will reimburse APC for claims from service providers on a per enrollee basis. The specific retention amount per enrollee per policy period is $55,000 to $60,000 for professional coverage. NMM believes that these insurance coverage limits are appropriate based upon its claims experience and the nature and risks of its business. However, it cannot assure that any pending or future claim will not be successful or, if successful, will not exceed the limits of available insurance coverage.
Significant Federal and State Healthcare Laws Governing NMM’s Business
As a healthcare company, NMM’s operations and relationships with healthcare providers such as hospitals, other healthcare facilities, and healthcare professionals are subject to extensive and increasing regulation by numerous federal, state, and local government entities. These laws and regulations often are interpreted broadly and enforced aggressively by multiple government agencies, including the OIG, the U.S. Department of Justice, CMS, and various state authorities. NMM has included brief descriptions of some, but not all, of the laws and regulations that affect NMM’s business below.
Imposition of liabilities associated with a violation of any of these healthcare laws and regulations could have a material adverse effect on NMM’s business, financial condition and results of operations. NMM cannot guarantee that its arrangements or business practices will not be subject to government scrutiny or be found to violate certain healthcare laws. Government investigations and prosecutions, even if NMM is ultimately found to be without fault, can be costly and disruptive to NMM’s business. Moreover, changes in healthcare legislation or government regulation may restrict NMM’s existing operations, limit the expansion of NMM’s business or impose additional compliance requirements and costs, any of which could have a material adverse effect on NMM’s business, financial condition and results of operations.
False Claims Acts
The federal False Claims Act imposes civil liability on individuals or entities that submit false or fraudulent claims for payment to the federal government. The False Claims Act provides, in part, that the federal government may bring a lawsuit against any person whom it believes has knowingly or recklessly presented, or caused to be presented, a false or fraudulent request for payment from the federal government, or who has made a false statement or used a false record to get a claim for payment approved. Private parties may initiate qui tam whistleblower lawsuits against any person or entity under the False Claims Act in the name of the government and may share in the proceeds of a successful suit.
| 290 |
The federal government has used the False Claims Act to prosecute a wide variety of alleged false claims and fraud allegedly perpetrated against Medicare and state healthcare programs. By way of illustration, these prosecutions may be based upon alleged coding errors, billing for services not rendered, billing services at a higher payment rate than appropriate, and billing for care that is not considered medically necessary. The government and a number of courts also have taken the position that claims presented in violation of certain other statutes, including the federal Anti-Kickback Statute or the Stark Law, can be considered a violation of the False Claims Act based on the theory that a provider impliedly certifies compliance with all applicable laws, regulations, and other rules when submitting claims for reimbursement.
Penalties for False Claims Act violations include fines ranging from $5,500 to $11,000 for each false claim, plus up to three times the amount of damages sustained by the government. A False Claims Act violation may provide the basis for the imposition of administrative penalties as well as exclusion from participation in governmental healthcare programs, including Medicare and Medicaid. In addition to the provisions of the False Claims Act, which provide for civil enforcement, the federal government also can use several criminal statutes to prosecute persons who are alleged to have submitted false or fraudulent claims for payment to the federal government.
A number of states have enacted false claims acts that are similar to the False Claims Act. Even more states are expected to do so in the future because Section 6031 of the DRA, amended the federal law to encourage these types of changes, along with a corresponding increase in state initiated false claims enforcement efforts. Under the DRA, if a state enacts a false claims act that is at least as stringent as the federal statute and that also meets certain other requirements, the state will be eligible to receive a greater share of any monetary recovery obtained pursuant to certain actions brought under the state’s false claims act. The OIG, in consultation with the Attorney General of the United States, is responsible for determining if a state’s false claims act complies with the statutory requirements. Currently, many states, including California have some form of state false claims act.
Anti-Kickback Statutes
The federal Anti-Kickback Statute is a provision of the Social Security Act that prohibits as a felony offense the knowing and willful offer, payment, solicitation or receipt of any form of remuneration in return for, or to induce, (1) the referral of a patient for items or services for which payment may be made in whole or part under Medicare, Medicaid or other federal healthcare programs, (2) the furnishing or arranging for the furnishing of items or services reimbursable under Medicare, Medicaid or other federal healthcare programs or (3) the purchase, lease, or order or arranging or recommending the purchasing, leasing or ordering of any item or service reimbursable under Medicare, Medicaid or other federal healthcare programs. The ACA amended section 1128B of the Social Security Act to make it clear that a person need not have actual knowledge of the statute, or specific intent to violate the statute, as a predicate for a violation. The OIG, which has the authority to impose administrative sanctions for violation of the statute, has adopted as its standard for review a judicial interpretation which concludes that the statute prohibits any arrangement where even one purpose of the remuneration is to induce or reward referrals. A violation of the Anti-Kickback Statute is a felony punishable by imprisonment, criminal fines of up to $25,000, civil fines of up to $50,000 per violation and three times the amount of the unlawful remuneration. A violation also can result in exclusion from Medicare, Medicaid or other federal healthcare programs. In addition, pursuant to the changes of the ACA, a claim that includes items or services resulting from a violation of the Anti-Kickback Statute is a false claim for purposes of the False Claims Act.
Due to the breadth of the Anti-Kickback Statute’s broad prohibitions, statutory exceptions exist that protect certain arrangements from prosecution. In addition, the OIG has published safe harbor regulations that specify arrangements that also are deemed protected from prosecution under the Anti-Kickback Statute, provided all applicable criteria are met. The failure of an activity to meet all of the applicable safe harbor criteria does not necessarily mean that the particular arrangement violates the Anti-Kickback Statute, but these arrangements may be subject to scrutiny and prosecution by enforcement agencies. The conduct or business arrangement, however, does increase the risk of scrutiny by government enforcement authorities. NMM may be less willing than some of its competitors to take actions or enter into business arrangements that do not clearly satisfy the safe harbors. As a result, this unwillingness may put NMM at a competitive disadvantage.
| 291 |
Some states have enacted statutes and regulations similar to the Anti-Kickback Statute, but which may be applicable regardless of the payor source for the patient. These state laws may contain exceptions and safe harbors that are different from and/or more limited than those of the federal law and that may vary from state to state. For example, California has adopted PORA. PORA makes it unlawful for a healing arts licensee, including physicians and surgeons, and other licensed professionals, to refer a person for certain health care services if the licensee has a financial interest, with the person or entity that receives the referral. While the law also provides certain exemptions from this prohibition, failure to fit within an exemption in violation of PORA can lead to a misdemeanor offense that may subject a physician to civil penalties and disciplinary action by the Medical Board of California.
NMM cannot assure shareholders that regulatory authorities that enforce these laws will not determine that some of its arrangements with physicians violate the Anti-Kickback Statute or other applicable laws. An adverse determination could subject NMM to liabilities under the Social Security Act, including criminal penalties, civil monetary penalties and exclusion from participation in Medicare, Medicaid or other federal health care programs, any of which could have a material adverse effect on NMM’s business, financial condition or results of operations.
Federal Stark Law
The Federal Stark Law, also known as the physician self-referral law, generally prohibits a physician from referring Medicare and Medicaid patients to an entity (including hospitals) providing ‘‘designated health services,’’ if the physician or a member of the physician’s immediate family has a ‘‘financial relationship’’ with the entity, unless a specific exception applies. Designated health services include, among other services, inpatient and outpatient hospital services, clinical laboratory services, certain imaging services, and other items or services that NMM’s affiliated physicians may order. The prohibition applies regardless of the reasons for the financial relationship and the referral; and therefore, unlike the federal Anti-Kickback Statute, intent to violate the law is not required. Like the Anti-Kickback Statute, the Stark Law contains a number of statutory and regulatory exceptions intended to protect certain types of transactions and business arrangements from penalty. Unlike safe harbors under the Anti-Kickback Statute with which compliance is voluntary, an arrangement must comply with every requirement of a Stark Law exception or the arrangement is in violation of the Stark Law.
The penalties for violating the Stark Law can include the denial of payment for services ordered in violation of the statute, mandatory refunds of any sums paid for such services and civil penalties of up to $15,000 for each violation, double damages, and possible exclusion from future participation in the governmental healthcare programs. A person who engages in a scheme to circumvent the Stark Law’s prohibitions may be fined up to $100,000 for each applicable arrangement or scheme.
Some states have enacted statutes and regulations similar to the Stark Law, but which may be applicable to the referral of patients regardless of their payor source and which may apply to different types of services. These state laws may contain statutory and regulatory exceptions that are different from those of the federal law and that may vary from state to state.
Because the Stark Law and its implementing regulations continue to evolve, NMM does not always have the benefit of significant regulatory or judicial interpretation of this law and its regulations. NMM attempts to structure its relationships to meet an exception to the Stark Law, but the regulations implementing the exceptions are detailed and complex, and NMM cannot be certain that every relationship complies fully with the Stark Law. In addition, in the July 2008 final Stark rule, CMS indicated that it will continue to enact further regulations tightening aspects of the Stark Law that it perceives allow for Medicare program abuse, especially those regulations that still permit physicians to profit from their referrals of ancillary services. There can be no assurance that the arrangements entered into by NMM with physicians and facilities will be found to be in compliance with the Stark Law, as it ultimately may be implemented or interpreted.
| 292 |
Health Information Privacy and Security Standards
Among other directives, the Administrative Simplification Provisions of HIPAA required HHS to adopt standards to protect the privacy and security of certain health-related information. The HIPAA privacy regulations contain detailed requirements concerning the use and disclosure of individually identifiable health information by “HIPAA covered entities,” which include entities like NMM and its affiliated practice groups.
In addition to the privacy requirements, HIPAA covered entities must implement certain administrative, physical, and technical security standards to protect the integrity, confidentiality and availability of certain electronic health information received, maintained, or transmitted. HIPAA also implemented the use of standard transaction code sets and standard identifiers that covered entities must use when submitting or receiving certain electronic healthcare transactions, including activities associated with the billing and collection of healthcare claims.
The American Recovery and Reinvestment Act enacted on February 18, 2009, included HITECH which modified the HIPAA legislation significantly. Pursuant to HITECH, certain provisions of the HIPAA privacy and security regulations become directly applicable to “HIPAA business associates”.
Violations of the HIPAA privacy and security standards may result in civil and criminal penalties. Historically, these included: (1) civil money penalties of $100 per incident, to a maximum of $25,000, per person, per year, per standard violated and (2) depending upon the nature of the violation, fines of up to $250,000 and imprisonment for up to ten years. The passage of HITECH significantly modified the enforcement structure, creating a tiered system of civil money penalties that range from $100 to $50,000 per violation, with a cap of $1.5 million per year for identical violations. NMM must also comply with the “breach notification” regulations, which implement certain provisions of HITECH. Under these regulations, in addition to reasonable remediation, covered entities must promptly notify affected individuals in the case of a breach of “unsecured PHI,” which is defined by HHS guidance, as well as the Secretary of HHS and the media in cases where a breach affects more than 500 individuals. Breaches affecting fewer than 500 individuals must be reported to the HHS Secretary on an annual basis. The regulations also require business associates of covered entities to notify the covered entity of breaches at or by the business associate. Formal enforcement of the new breach notification regulations began on February 22, 2010.
NMM expects increased federal and state HIPAA privacy and security enforcement efforts. Under HITECH, state Attorneys General now have the right to prosecute HIPAA violations committed against residents of their states. In addition, HITECH mandates that the Secretary of HHS conduct periodic compliance audits of HIPAA covered entities and business associates. It also tasks HHS with establishing a methodology whereby harmed individuals who were the victims of breaches of unsecured PHI may receive a percentage of the civil monetary penalty fine or monetary settlement paid by the violator. This methodology for compensation to harmed individuals was initially required to be in place by February 17, 2012; however, no rules or regulations implementing this methodology have yet been adopted by HHS. HHS may nonetheless eventually establish such methodology for compensation to harmed individuals.
Many states also have laws that protect the privacy and security of confidential, personal information. These laws may be similar to or even more stringent than the federal provisions. Not only may some of these state laws impose fines and penalties upon violators, but some may afford private rights of action to individuals who believe their personal information has been misused.
| 293 |
Fee-Splitting and Corporate Practice of Medicine
Some states, including California, have laws that prohibit business entities, such as NMM and its subsidiaries, from practicing medicine, employing physicians to practice medicine, exercising control over medical decisions by physicians (also known collectively as the corporate practice of medicine) or engaging in certain arrangements, such as fee-splitting, with physicians. In these states, a violation of the corporate practice of medicine prohibition constitutes the unlawful practice of medicine, which is a public offense punishable by fines and other criminal penalties. In addition, any physician who participates in a scheme that violates the state’s corporate practice of medicine prohibition may be punished for aiding and abetting a lay entity in the unlawful practice of medicine. NMM operates by maintaining long-term management contracts with affiliated professional organizations, which are each owned and operated by physicians and which employ or contract with additional physicians to provide medical services. Under these arrangements, NMM performs only non-medical administrative services, does not represent that NMM offers medical services, and does not exercise influence or control over the practice of medicine by the physicians or the affiliated professional organizations. The California Medical Board, as well as other state’s regulatory bodies, has taken the position that certain physician practice management agreements that confer too much control over a physician practice violate the prohibition against corporate practice of medicine.
For financial reporting purposes, however, NMM consolidates the revenues and expenses of its VIE, Allied Physicians of California, because NMM has a controlling financial interest in these practices based on applicable accounting rules and as described in NMM’s consolidated financial statements. In states where fee-splitting is prohibited between physicians and non-physicians, the fees that NMM receives through its management contracts have been established on a basis that NMM believes complies with the applicable state laws.
Some of the relevant laws, regulations, and agency interpretations in the State of California and other states that have corporate practice prohibitions have been subject to limited judicial and regulatory interpretation. Moreover, state laws are subject to change and regulatory authorities and other parties, including NMM’s affiliated physicians, may assert that, despite these arrangements, NMM is engaged in the prohibited corporate practice of medicine or that NMM’s arrangements constitute unlawful fee-splitting. If this occurred, NMM could be subject to civil or criminal penalties, NMM’s contracts could be found legally invalid and unenforceable (in whole or in part), or NMM could be required to restructure its contractual arrangements. If NMM were required to restructure its operating structures due to determination that a corporate practice of medicine violation existed, such a restructuring might include revisions of NMM’s management services agreements, which might include a modification of the management fee, and/or establishing an alternative structure.
Other Federal Healthcare Compliance Laws
NMM is also subject to other federal healthcare laws.
In 1995, Congress amended the federal criminal statutes set forth in Title 18 of the United States Code by defining additional federal crimes that could have an impact on NMM’s business, including “Health Care Fraud” and “False Statements Relating to Health Care Matters.” The Health Care Fraud provision prohibits any person from knowingly and willfully executing, or attempting to execute, a scheme to defraud any healthcare benefit program. As defined in this provision of Title 18, a “healthcare benefit program” can be either a government or private payor plan. Violation of this statute may be charged as a felony offense and may result in fines, imprisonment or both. The ACA amended section 1347 of Title 18 to provide that a person may be convicted under the Health Care Fraud provision even in the absence of proof that the person had actual knowledge of, or specific intent to violate, the statute.
The False Statements Relating to Health Care Matters provision prohibits, in any matter involving a federal health care program, anyone from knowingly and willfully falsifying, concealing or covering up, by any trick, scheme or device, a material fact, or making any materially false, fictitious or fraudulent statement or representation, or making or using any materially false writing or document knowing that it contains a materially false or fraudulent statement. A violation of this statute may be charged as a felony offense and may result in fines, imprisonment or both.
| 294 |
Under the Civil Monetary Penalties law of the Social Security Act, a person, including any individual or organization, may be subject to civil monetary penalties, treble damages and exclusion from participation in federal health care programs for certain specified conduct. One provision of the Civil Monetary Penalties law precludes any person (including an organization) from knowingly presenting or causing to be presented to any United States officer, employee, agent, or department, or any state agency, a claim for payment for medical or other items or services that the person knows or should know (a) were not provided as described in the coding of the claim, (b) is a false or fraudulent claim, (c) is for a service furnished by an unlicensed physician, (d) is for medical or other items or service furnished by a person or an entity that is in a period of exclusion from the program or (e) are medically unnecessary items or services. Violations of the law may result in penalties of up to $10,000 per claim, treble damages, and exclusion from federal healthcare programs. In addition, the OIG may impose civil monetary penalties against any physician who knowingly accepts payment from a hospital (as well as against the hospital making the payment) as an inducement to reduce or limit medically necessary services provided to Medicare or Medicaid program beneficiaries. Further, except as specifically permitted under the Civil Monetary Penalties law, a person who offers or transfers to a Medicare or Medicaid beneficiary any remuneration that the person knows or should know is likely to influence the beneficiary’s selection of a particular provider of Medicare or Medicaid payable items or services may be liable for civil money penalties of up to $10,000 for each wrongful act.
Other State Healthcare Compliance Provisions
In addition to the state laws previously described, NMM may also be subject to other state fraud and abuse statutes and regulations if it expands its operations beyond California. Many states have adopted a form of anti-kickback law, self-referral prohibition, and false claims and insurance fraud prohibition. The scope of these laws and the interpretations of them vary from state to state and are enforced by state courts and regulatory authorities, each with broad discretion. Generally, state laws reach to all healthcare services and not just those covered under a governmental healthcare program. A determination of liability under any of these laws could result in fines and penalties and restrictions on NMM’s ability to operate in these states. NMM cannot assure that its arrangements or business practices will not be subject to government scrutiny or be found to violate applicable fraud and abuse laws.
Knox-Keene Act and Other State Insurance Laws
Some of the medical groups and IPAs that have entered into management services agreements with NMM, have historically contracted with health plans and other payors to receive a PMPM or percentage of premium capitation payment for professional (physician) services and assumed the financial responsibility for professional services. In many of these cases, the health plans or other payors separately enter into contracts with hospitals that directly receive payment (either a capitation or FFS payment) and assume some type of contractual financial responsibility for their institutional (hospital) services. In some instances, NMM’s managed medical groups and IPAs have been paid by their contracting payor for the financial outcome of managing the care dollars associated with both the professional and institutional services received by the medical groups’ and IPAs’ members. In the case of institutional services, the medical groups and IPAs have recognized a percentage of the surplus of institutional revenues less institutional expense as the medical groups’ and IPAs’ net revenues and has also been responsible for some percentage of any short-fall in the event that institutional expenses exceed institutional revenues. Notwithstanding, neither NMM nor any of its managed medical groups or IPAs are contractually obligated to pay claims to any hospitals or other institutions under these arrangements. The DMHC licenses and regulates health care service plans pursuant to the Knox-Keene Act. Neither NMM nor any of its managed medical groups or IPAs hold a limited Knox-Keene license. If DMHC were to determine that NMM or its managed medical groups or IPAs has been inappropriately taking risk for institutional and professional services as a result of their respective various hospital and physician arrangements without having a limited Knox-Keene license, NMM may be required to obtain a limited Knox-Keene license to resolve such violations and NMM could be subject to civil and criminal liability, any of which could have a material adverse effect on its business, financial condition or results of operations.
Furthermore, some states require ACOs to be registered or otherwise comply with state insurance laws. NMM’s affiliated ACOs do not currently take financial risk, and are therefore not registered with any state insurance agency. If a state insurance agency were to determine that NMM has been inappropriately operating an ACO without state registration or licensure, NMM may be required to obtain such registration or licensure to resolve such violations and NMM could be subject to liability, which could have a material adverse effect on NMM’s business, financial condition or results of operations.
As of June 30, 2017, NMM had 309 employees, of whom 308 were full-time and 1 was part-time. None of NMM’s employees is a member of a labor union, and NMM has never experienced a work stoppage. NMM believes that it enjoys a good working relationship with its employees.
| 295 |
NMM’s corporate headquarters is located in Alhambra, California, where it leases and occupies approximately 35,000 square feet of executive office space. The term of the current lease for NMM’s headquarters expired on August 31, 2017 and is now month-to-month, which requires monthly rental payments of approximately $84,000. NMM also maintains other offices located in Monterey Park, Alhambra, City of Industry, Arcadia and El Monte, California. The terms of these leases expire through July 31, 2025 and requires monthly rent payments ranging from approximately $2,300 to approximately $30,000.
NMM is involved from time to time in routine legal matters incidental to its business. As of June 30, 2017, NMM is not involved in any pending or threatened legal actions or proceedings, the adverse outcome of which, in its management’s opinion, would have a material adverse effect on NMM’s financial position, results of operations or cash flows. However, there can be no assurance that future claims will not have such a material adverse effect on NMM’s business.
Management’s Discussion and Analysis of Financial Condition and Results of Operations
You should read the following discussion and analysis of NMM’s financial condition and results of operations together with “Selected historical consolidated financial information” and NMM’s consolidated financial statements and related notes appearing elsewhere in this joint proxy statement/prospectus and in the documents incorporated by reference in this joint proxy statement/prospectus. This discussion and analysis contains forward-looking statements that involve risks, uncertainties and assumptions. The actual results may differ materially from those anticipated in these forward-looking statements as a result of certain factors, including, but not limited to, those set forth under “Risk Factors” and elsewhere in this joint proxy statement/prospectus.
Overview and Recent Developments
NMM is a patient- and physician-focused, integrated health care management company with over 20 years of providing coordinated, outcomes-based medical care in a cost-effective manner. Through capitation agreements between NMM’s affiliated physician groups and various health plans, NMM is responsible for coordinating the care for over 600,000 covered patients in southern and central California through a network of over 10 IPAs with approximately 4,000 contracted physicians. These covered patients are comprised of managed care members whose health coverage is provided through their employer or who have individually acquired health coverage directly from a health plan or as a result of their eligibility for Medicaid or Medicare benefits.
Founded in 1994 and headquartered in Alhambra, California, NMM is an integrated healthcare organization that provides medical management and administrative services to its affiliated medical groups and operates three ACOs, two of which are MSSP ACOs, and the other of which is a NGACO.
The patients of NMM’s affiliated physicians, physician groups and IPAs benefit from an integrated approach to medical care that places the physician at the center of patient care. Together with numerous case managers, registered nurses and other care coordinators, these medical professionals utilize sophisticated risk management techniques and clinical protocols to provide high-quality, cost effective care to NMM’s managed members. NMM monitors certain control metrics, such as the number of inpatient acute bed days per 1,000 patients and hospital readmission rates, as they are contributors to quality clinical outcomes and financial performance. NMM endeavors to stay informed of any changes to the Medicaid and Medicare Advantage programs as such changes may affect its financial performance. Additionally, in an effort to identify changes or trends with respect to its commercial, senior and Medicaid payer classifications, NMM closely monitors the number of managed care members who have enrolled with an NMM affiliated physician group as their primary care physician.
As used in this section, “MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITIONS AND RESULTS OF OPERATIONS,” unless stated otherwise, “NMM” shall collectively refer to each of the following entities: NMM, APC, APC-LSMA, ACO Acquisition Corporation, APCN-ACO, ACO Acquisition Corporation #2, AP-ACO, CDSC, and UCAP (each of which entities is defined and described as follows):
| 296 |
APC was incorporated on August 17, 1992 for the purpose of arranging health care services as an IPA. APC has contracts with various HMOs or licensed health care service plans as defined in the Knox-Keene Act. Each HMO negotiates a fixed amount PMPM that is to be paid to APC. In return, APC arranges for the delivery of health care services by contracting with physicians or professional medical corporations for primary care and specialty care services. APC assumes the financial risk of the cost of delivering health care services in excess of the fixed amounts received. Some of the risk is transferred to the contracted physicians or professional corporations. The risk is also minimized by stop-loss provisions in contracts with HMOs.
On July 1, 1999, APC entered into an amended and restated management and administrative services agreement with NMM (initial management services agreement was entered into in 1997) for an initial fixed term of 30 years. In accordance with relevant accounting guidance, APC is determined to be a VIE and NMM is the primary beneficiary with the ability to direct the activities (excluding clinical decisions) that most significantly affect APC’s economic performance through its majority representation of the APC Joint Planning Board; therefore APC is consolidated by NMM. As of June 30, 2017 and December 31, 2016, APC owns 6.29% of NMM.
APC-LSMA was formed on October 15, 2012 as a designated shareholder professional corporation and is solely owned by Dr. Thomas Lam, a shareholder and Chief Executive and Financial Officer of APC. APC-LSMA is controlled and consolidated by APC who is the primary beneficiary of this VIE. The only activity of APC-LSMA is to hold the investments in medical corporations, which includes: LMA, PMIOC and DMG.
On November 11, 2015, NMM, ACO Acquisition Corporation, and APCN-ACO entered into a reorganization agreement whereby ACO Acquisition Corporation, a newly organized entity in which NMM is its sole shareholder, merged with APCN-ACO, effective on January 8, 2016, resulting in APCN-ACO becoming a wholly-owned subsidiary of NMM.
On December 18, 2016, NMM, ACO Acquisition Corporation #2, and AP-ACO entered into a reorganization agreement whereby ACO Acquisition Corporation #2, a newly organized entity in which NMM is its sole shareholder, merged into AP-ACO, effective on December 20, 2016, resulting in AP-ACO becoming a wholly-owned subsidiary of NMM.
CDSC was formed on March 25, 2010, and operates an ambulatory surgery center in City of Industry, California that is Medicare Certified and accredited by the Accreditation Association for Ambulatory Healthcare, Inc. During 2011, APC invested $625,000 for a 41.59% ownership in CDSC. Due to capital stock changes, APC’s ownership percentage in CDSC’s capital stock changed to 43.8%, 43.43% and 47.05% on May 31, 2016, July 31, 2016 and March 31, 2017, respectively. CDSC is consolidated as a VIE by APC as it was determined that APC has a controlling financial interest in CDSC and is the primary beneficiary of CDSC.
UCAP, a 100% owned subsidiary of APC, was formed on June 4, 2014, for the purpose of holding the investment in UCI.
Recent Developments
Loans Receivable – Related Parties
On January 3, 2017, pursuant to a promissory note agreement, NMM provided a loan to ApolloMed in the principal amount of $5,000,000. The entire outstanding principal amount is due and payable in full on the maturity date of January 3, 2019. Interest accrues at 1% point above the Prime Rate commencing on the first date of the first month immediately following the execution of the note agreement and is to be paid by ApolloMed to NMM in successive quarterly installments.
| 297 |
Amendment to Merger Agreement
As part of an amendment to the Merger Agreement on March 30, 2017, the merger consideration to be paid by ApolloMed to NMM was amended to include warrants to purchase 850,000 shares of common stock at an exercise price of $11 per share, that will only be granted in the case that the proposed Merger between the NMM and ApolloMed occurs, in exchange for NMM providing both a guarantee for ApolloMed’s Alliance Note and as compensation to NMM for relinquishing their right to additional shares in ApolloMed based on the agreed upon exchange ratio with NMM in the event that the Alliance Note is converted to ApolloMed common stock.
Effective as of October 17, 2017, the parties to the Merger Agreement executed a second amendment to the Merger Agreement (“Amendment No. 2”). Pursuant to Amendment No. 2, the merger consideration was amended to provide that each outstanding share of NMM common stock will be converted into the right to receive such number of shares of ApolloMed common stock that would result in the NMM shareholders having a right to receive (i) an aggregate number of shares of ApolloMed common stock that represents 82% of the total issued and outstanding shares of ApolloMed common stock immediately following the consummation of the Merger (assuming there are no NMM dissenting shareholder interests as of the effective time of the Merger) and (ii) an aggregate of 2,566,666 shares of ApolloMed common stock. In addition, Amendment No. 2 provides that each NMM shareholder will be entitled to receive such shareholder’s pro rata portion of (i) warrants to purchase an aggregate of 850,000 shares of ApolloMed common stock exercisable at $11.00 per share, and (ii) warrants to purchase an aggregate of 900,000 shares of ApolloMed common stock exercisable at $10.00 per share. Amendment No. 2 contains other conforming changes, including provisions authorizing the issuance of shares of NMM common stock and options (which options must be exercised or cancelled prior to the closing) and extending the End Date to March 31, 2018.
Amendment No. 2 also contemplates NMM to provide a new working capital loan in the amount of nine million dollars evidenced by a promissory note, which is convertible into shares of common stock of ApolloMed at $10 per share (the “Restated NMM Note”). Of the principal amount, (A) $5,000,000 is required to be used to refinance a $5,000,000 working capital loan that was previously loaned by NMM to the Company pursuant to a Promissory Note dated January 3, 2017 (the “Original Note”) and (B) $4,000,000 is to be used for working capital. The Restated NMM Note cancels and replaces the Original Note and with the effect that the entire outstanding principal balance of the Original Note, all accrued and unpaid interest thereon, and any applicable fees, costs and charges rolls into and becomes payable pursuant to the terms of the Restated NMM Note.
Under the terms of the Restated NMM Note, in the event that ApolloMed fails to repay the Alliance Note in full when due, NMM agrees and undertakes to pay Alliance all amounts owed by ApolloMed to Alliance or enter into another agreement with Alliance. The Restated NMM Note has also been amended and restated to include (i) an extension of the maturity date to the earlier of (A) March 31, 2019 or (B) 12 months after the date the Merger Agreement is terminated, (ii) the increase in the principal amount of the Restated NMM Note to $13,990,000 if ApolloMed fails to pay the Alliance Note and NMM either pays all amounts owed under the Alliance Note or enters into another agreement with Alliance (such that in either case the Alliance Note is cancelled) and (iii) a conversion feature allowing the Restated NMM Note to be converted into shares of ApolloMed common stock at $10.00 per share, subject to adjustment for stock splits, dividends, recapitalizations and the like, with such conversion, if exercised in accordance with the terms of the Restated NMM Note, becoming effective on the maturity date.
Investments
ICC
On November 15, 2016, APC-LSMA, a VIE of APC, agreed to purchase and acquire from ICC 40% of the aggregate issued and outstanding shares of capital stock of ICC for $400,000 in cash. The closing date of the investment was subject to entering into a shareholder agreement and a management services agreement, both of which occurred on August 1, 2017 and was therefore not accounted for as of June 30, 2017. ICC is a professional medical California corporation and has entered into agreements with Healthplans for the arrangement of the provision of healthcare services to subscribers or enrollees of said Healthplans. In addition, ICC has entered into written agreements with physicians and other healthcare professionals to provide or arrange for the provision of healthcare services to enrollees of participating Healthplans who have contracted or will contract with ICC for healthcare services. Subsequent to the acquisition, it was agreed that ICC’s working capital needs shall be funded as and when needed through capital contributions and/or subordinated debt by the shareholders of ICC on a pro rata basis based on their respective ownership interests in ICC.
| 298 |
In connection with the share purchase agreement, ICC entered into a management services agreement with NMM, which requires the payment of management fees computed as 2% of ICC revenues, subject to adjustment to a higher tier based on 12-month gross revenues or a maximum of 8% of ICC revenues. The term of the management services agreement commenced on the August 1, 2017 and extend for a period of 60 months thereafter, and may be extended in writing at the sole option of NMM for an additional period of 60 months following the expiration of the initial term and is automatically renewed for additional consecutive terms of three years unless terminated by either party. The management services agreement may be terminated by either party if certain metrics specified under Section 5.3 of the agreement are not met.
APC accounts for its investment in ICC under the equity method of accounting as APC has the ability to exercise significant influence, but not control over ICC’s operations. The investment of $400,000 was made on September 8, 2017; therefore, no amounts have been recognized for this investment as of June 30, 2017.
Netlytics
NMM entered into a Joint Venture Agreement dated as of January 25, 2017, with MediPortal and Rulemeister to form a joint venture company to be named Netlytics for the purpose of developing and implementing a fully-integrated electronic platform that will enable ACOs, IPAs, health plans and other health care payers and providers to aggregate data and utilize analytic tools to effectively engage in population health management. Netlytics was formed on November 1, 2016. The respective ownership interests of NMM, MediPortal and Rulemeister in Netlytics will be 55%, 30% and 15%. In exchange for its 55% interest, NMM will contribute $275,000 as its capital contribution to Netlytics. In June 2017, APC and Mediportal entered into a subscription agreement. Pursuant to the subscription agreement, APC is to pay Mediportal $405,000 to purchase 270,000 membership interests of Mediportal at a price of $1.50 per membership interest. The effective date of the subscription agreement between APC and Mediportal is subject to completion of due diligence by APC. The effective date of the Joint Venture Agreement is also subject to completion of due diligence by NMM. In addition, there has been no activity in Netlytics and no amounts have been contributed to Netlytics through the date of this filing.
Management Services Agreement
On September 27, 2017, with an effective date of January 1, 2018, NMM entered into a Management Services Agreement (“MSA”) with Joseph M. Molina, M.D., Professional Corporation – Southern California dba Golden Shore Medical Group, a California Professional Corporation (“GSMG”). The MSA requires the payment of management fees in accordance with the management fee schedule therein. The term of the MSA will commence on the effective date through December 31, 2020, and may be extended in writing at the sole option of GSMG for an additional two year term following the expiration of the initial term. GSMG will have the right to terminate the MSA if certain conditions, as defined in the MSA, are met.
Loan Receivable and Management Services Agreement
On October 9, 2017 (“Effective Date”), NMM and APC-LSMA entered into an agreement with Accountable Health Care IPA (“Accountable”), a California professional medical corporation, Signal Health Solutions, Inc. (“Signal”), a California corporation and George M. Jayatilaka, M.D. (“Dr. Jay”), individually, whereby concurrent with the execution of the agreement, APC-LSMA will extend a line of credit to Dr. Jay in the principal amount of up to $10,000,000 (“Dr. Jay Loan”) to fund the working capital needs of Accountable. The line of credit may be funded in installments, as needed by Accountable and as determined from time to time by APC-LSMA. Interest on the Dr. Jay Loan accrues at a rate that is equal to the prime rate plus 1% and payable in monthly installments of interest only on the first day of each month until the date that is 3 years following the initial date of funding, at which time, all outstanding principal and accrued interest thereon shall be due and payable in full. The Dr. Jay Loan will not be subordinated. The Dr. Jay Loan shall at all times be secured by a first-lien security interest in shares of Accountable owned by Dr. Jay.
| 299 |
Concurrently with the funding of the Dr. Jay Loan, Dr. Jay will loan to Accountable the entire proceeds of the Dr. Jay Loan at the same interest rate and maturity date as the Dr. Jay Loan (Dr. Jay-Accountable Subordinated Loan”). Repayment of the Dr. Jay-Accountable Subordinated Loan will be subordinated to Accountable’s creditors in a manner acceptable to the DMHC.
At any time on or before the date that is one year following the initial funding date of the Dr. Jay Loan, APC-LSMA or its designee shall have the right, but not the obligation, to convert up to $5,000,000 of the principal amount into shares of Accountable’s capital stock. At any time after the date that is one year following the funding date, the Dr. Jay Loan may be prepaid at any time. Within three years following the initial funding of the Dr. Jay Loan, APC-LSMA or its designee shall have the right, but not the obligation, to convert the then outstanding principal amount into Accountable shares based on Accountable’s then-current valuation.
Subsequent to the funding of the Dr. Jay Loan, to the extent needed by Accountable for working capital needs at determined by APC-LSMA, APC-LSMA will extend an additional line of credit in the principal amount up to $8,000,000. The funding mechanism, interest rate and maturity date of such additional line of credit shall be the same as the Dr. Jay Loan and additional collateral security in Accountable’s issued and outstanding shares will be required.
As a condition of funding the Dr. Jay Loan, Accountable entered into a management service agreement with NMM to commence on the termination of the Accountable's existing management agreement with MedPoint Management (currently anticipated to be on or about November 1, 2017) and have a term of ten (10) years from its Effective Date. NMM will be responsible for managing 100% of all health plan membership assigned and delegated to Accountable, and all hospital risk pools. The management service agreement requires the payment of IPA management fees as set forth therein.
Concurrent with the initial funding of the Dr. Jay Loan, the Accountable Board of Directors shall be automatically reconstituted to be comprised of two directors, which will comprise of Dr. Jay and a director appointed by APC-LSMA. Dr. Jay and APC-LSMA will have two and one votes as a director, respectively.
Key Financial Measures and Indicators
Operating Revenues
Revenue primarily consists of capitation revenue, risk pool settlements and incentives, management fee income, surgery center income and FFS. Revenue is recorded in the period in which services are rendered. The form of billing and related risk of collection for such services may vary by customer.
Operating Expenses
General
NMM’s largest expense is the cost of hiring staff to provide management and administrative support services to its affiliated physician groups, as further described below. These services include payroll, benefits, human resource services, physician practice billing, revenue cycle services, physician practice management, administrative oversight, coding services, and other consulting services.
| 300 |
NMM’s consolidated operating results for the year ended December 31, 2016, as compared to the year ended December 31, 2015 were as follows:
Network Medical Management, Inc.
Consolidated Statements of Income
| For the years ended | ||||||||||||||||
| December 31, | December 31, | |||||||||||||||
| 2016 | 2015 | $ Change | % Change | |||||||||||||
| REVENUES: | ||||||||||||||||
| Capitation, net | $ | 247,639,181 | $ | 247,244,135 | 395,046 | 0.2 | % | |||||||||
| Risk pool settlements and incentives | 22,641,884 | 37,656,242 | (15,014,358 | ) | -39.9 | % | ||||||||||
| Management fee income | 24,774,941 | 20,834,222 | 3,940,719 | 18.9 | % | |||||||||||
| Surgery center income, net | 6,132,729 | 5,366,490 | 766,239 | 14.3 | % | |||||||||||
| Fee-for-services, net | 3,031,241 | 1,070,864 | 1,960,377 | 183.1 | % | |||||||||||
| Other income | 1,714,939 | 952,752 | 762,187 | 80.0 | % | |||||||||||
| Total revenues | 305,934,915 | 313,124,705 | (7,189,790 | ) | -2.3 | % | ||||||||||
| EXPENSES: | ||||||||||||||||
| Contracted physicians and other services | 254,468,120 | 233,581,805 | 20,886,315 | 8.9 | % | |||||||||||
| General and administrative expenses | 20,759,436 | 22,277,282 | (1,517,846 | ) | -6.8 | % | ||||||||||
| Management fees | 580,000 | 4,507,180 | (3,927,180 | ) | -87.1 | % | ||||||||||
| Depreciation and amortization | 18,114,440 | 9,085,312 | 9,029,128 | 99.4 | % | |||||||||||
| Impairment of goodwill and other | 324,306 | - | 324,306 | 100.0 | % | |||||||||||
| Total expenses | 294,246,302 | 269,451,579 | 24,794,723 | 9.2 | % | |||||||||||
| INCOME FROM OPERATIONS | 11,688,613 | 43,673,126 | (31,984,513 | ) | -73.2 | % | ||||||||||
| OTHER INCOME (EXPENSES): | ||||||||||||||||
| Income from equity method investments | 4,748,542 | 1,206,654 | 3,541,888 | 293.5 | % | |||||||||||
| Interest expense | (61,589 | ) | (209,929 | ) | 148,340 | -70.7 | % | |||||||||
| Interest income | 504,696 | 208,917 | 295,779 | 141.6 | % | |||||||||||
| Change in fair value of derivative instrument | 1,722,221 | (833,333 | ) | 2,555,554 | -306.7 | % | ||||||||||
| Other income | 233,726 | 1,931,635 | (1,697,909 | ) | -87.9 | % | ||||||||||
| Total other income, net | 7,147,596 | 2,303,944 | 4,843,652 | 210.2 | % | |||||||||||
| INCOME BEFORE PROVISION FOR INCOME TAXES | 18,836,209 | 45,977,070 | (27,140,861 | ) | -59.0 | % | ||||||||||
| Provision for income taxes | 8,816,412 | 19,297,447 | (10,481,035 | ) | -54.3 | % | ||||||||||
| NET INCOME | $ | 10,019,797 | $ | 26,679,623 | (16,659,826 | ) | -62.4 | % | ||||||||
| Less: net (loss) income attributable
to noncontrolling interests |
(1,433,730 | ) | 13,862,522 | (15,296,252 | ) | -110.3 | % | |||||||||
| NET INCOME ATTRIBUTABLE TO NETWORK MEDICAL MANAGEMENT, INC. | $ | 11,453,527 | $ | 12,817,101 | (1,363,574 | ) | -10.6 | % | ||||||||
Overview
Net income in 2016 was $10.0 million, as compared to $26.7 million in 2015, a decrease of $16.7 million or 62%.
Membership Information
As of December 31, 2016 and 2015, the total number of affiliated physician groups managed by NMM was 10 groups and 12 groups, respectively, and the total number of affiliated physician group members for whom NMM managed the delivery of healthcare services was 617,791 and 606,078, respectively.
Revenues
NMM’s revenues in 2016 were $305.9 million, as compared to $313.1 million in 2015, a decrease of $7.2 million or 2%. The decrease in revenue was attributable to a decrease of $15 million of risk pool revenue that was accrued in 2015, with no amounts in 2016 as collection was not assured. Such decrease was offset by (i) increases in management fee income of $3.9 million, which was mainly driven by the increase of $1.8 million from LMA and $1.5 million from Health Net Covered California (“HNCC”) as a result of membership increase and receiving maternity kick, (ii) increases in fees-for-service revenue of $2.0 million is mainly due to fees received from Blue Cross, Blue Shield, LA Care, ICC and HNCC, (iii) increases in other income of $0.8 million, and (iv) increases in surgery center income due to increase in patients.
| 301 |
Contracted Physicians and other Services
Expenses related to contracted physicians and other services in 2016 were $254.5 million, as compared to $233.6 million in 2015, an increase of $20.9 million, or 9%. Of this increase, $8.1 million was attributable to increased payments for capitations, $13.9 million in medical claims, and $3.9 million increase in salaries and personnel related expenses due to new hires and transfers from PHW. Such increases were offset by a decrease of $5 million in provider bonuses which are discretionary.
General and Administrative Expenses
General and administrative expenses in 2016 were $20.8 million, as compared to $22.3 million in 2015, a decrease of $1.5 million, or 7%, as compared to 2015. The decrease was attributable to decrease in bonuses of $4.3 million, offset by increases of $1.7 million in consulting expenses, $0.6 million in marketing expenses and increase of $0.2 million in salary and wages and $0.3 million in other operating expenses.
Management Fees
Management fees in 2016 decreased by $3.9 million, or 87%, as compared to 2015. The decrease was attributable to a decrease in bonuses paid to directors in connection with the 2015 acquisitions.
Depreciation and Amortization
Depreciation and amortization expense in 2016 was $18.1 million, as compared to $9.1 million in 2015, an increase of $9.0 million, or 99%, as compared to 2015. The increase was attributable to acquisitions of PIPA MSO and PHW in 2015, which resulted in significant increase in amortization expense associated with such intangible assets, as well increases in depreciation expense from purchases of property and equipment in 2016.
Impairment of goodwill and other
During 2016, NMM impaired the remaining goodwill and investment balance associated with Apple Physicians Organization that was acquired in 2008, as the amount was not determined to be recoverable.
Income from Equity Method Investments
Income from equity method investments in 2016 were $4.7 million, as compared to $1.2 million in 2015, an increase of $3.5 million or 294%, mainly due to the income allocation from LMA of $2.9 million, UCI of $0.7 million, offset by loss from investment of $0.1 million from PMIOC.
Interest Expense
Interest expense in 2016 was $0.1 million, as compared to $0.2 million in 2015, a decrease of $0.1 million or 71%, mainly due to the payoff of the APC’s mortgage loan in February 2016 and line of credit fee and interest expense from capital lease obligations.
Interest Income
Interest income in 2016 was $0.5 million for 2016, as compared to $0.2 million in 2015, an increase of $0.3 million or 142%, mainly due to more cash held in money market account which resulted in more interest earned in 2016.
| 302 |
Change in Fair Value of Derivative Instrument
Change in fair value of derivative instrument was $1.7 million, as compared to $(0.8) million, a change of $2.6 million or 307%, mainly due to an increase in the stock price of ApolloMed common stock.
Other Income
Other income in 2016 was $0.2 million for 2016, as compared to $1.9 million in 2015, a decrease of $1.7 million or 88%, mainly due to performance incentive received from LMA in 2015 that was non-recurring for 2016.
Provision for Income Taxes
Provision for income taxes was $8.8 million for 2016, as compared to $19.3 million in 2015, a decrease of $10.5 million or 54%. This decrease is primarily attributable to a reduction in the amount of pre-tax income in 2016 as compared to 2015.
Net (loss) income attributable to noncontrolling interest
Net loss attributable to noncontrolling interests was $1.4 million for the year ended December 31, 2016 compared to net income attributable to noncontrolling interest of $13.9 million for the year ended December 31, 2015 for a decrease of $15.3 million or 110% primarily due to net loss generated from APC mainly attributable to the decrease in revenues, increases in contracted physicians and other services expense and decrease in tax provision.
Results of Operations - Comparison of December 31, 2015 and December 31, 2014
NMM’s consolidated operating results for the year ended December 31, 2015, as compared to the year ended December 31, 2014 were as follows:
Network Medical Management, Inc.
Consolidated Statements of Operations
| December 31, | December 31, | |||||||||||||||
| 2015 | 2014 | $ Change | % Change | |||||||||||||
| REVENUES: | ||||||||||||||||
| Capitation, net | $ | 247,244,135 | $ | 103,501,636 | 143,742,499 | 138.9 | % | |||||||||
| Risk pool settlements and incentives | 37,656,242 | 12,991,159 | 24,665,083 | 189.9 | % | |||||||||||
| Management fee income | 20,834,222 | 11,954,649 | 8,879,573 | 74.3 | % | |||||||||||
| Surgery center income, net | 5,366,490 | 4,601,143 | 765,347 | 16.6 | % | |||||||||||
| Fee-for-services, net | 1,070,864 | 614,605 | 456,259 | 74.2 | % | |||||||||||
| Other income | 952,752 | 676,897 | 275,855 | 40.8 | % | |||||||||||
| Total revenues | 313,124,705 | 134,340,089 | 178,784,616 | 133.1 | % | |||||||||||
| EXPENSES: | ||||||||||||||||
| Contracted physicians and other services | 233,581,805 | 110,497,210 | 123,084,595 | 111.4 | % | |||||||||||
| General and administrative expenses | 22,277,282 | 27,262,885 | (4,985,603 | ) | -18.3 | % | ||||||||||
| Management fees | 4,507,180 | 8,299,833 | (3,792,653 | ) | -45.7 | % | ||||||||||
| Depreciation and amortization | 9,085,312 | 1,367,434 | 7,717,878 | 564.4 | % | |||||||||||
| Total expenses | 269,451,579 | 147,427,362 | 122,024,217 | 82.8 | % | |||||||||||
| INCOME (LOSS) FROM OPERATIONS | 43,673,126 | (13,087,273 | ) | 56,760,399 | -433.7 | % | ||||||||||
| OTHER INCOME (EXPENSES): | ||||||||||||||||
| Income from equity method investments | 1,206,654 | 2,072,470 | (865,816 | ) | -41.8 | % | ||||||||||
| Interest expense | (209,929 | ) | - | (209,929 | ) | -100.0 | % | |||||||||
| Interest income | 208,917 | 118,650 | 90,267 | 76.1 | % | |||||||||||
| Change in fair value of derivative instrument | (833,333 | ) | - | (833,333 | ) | -100.0 | % | |||||||||
| Other income | 1,931,635 | 126,754 | 1,804,881 | 1423.9 | % | |||||||||||
| Total other income, net | 2,303,944 | 2,317,874 | (13,930 | ) | -0.6 | % | ||||||||||
| INCOME (LOSS) BEFORE PROVISION FOR INCOME TAXES | 45,977,070 | (10,769,399 | ) | 56,746,469 | -526.9 | % | ||||||||||
| Provision for income taxes | 19,297,447 | 2,933,311 | 16,364,136 | 557.9 | % | |||||||||||
| NET INCOME (LOSS) | $ | 26,679,623 | $ | (13,702,710 | ) | 40,382,333 | -294.7 | % | ||||||||
| Less: net (loss) income attributable
to noncontrolling interests |
13,862,522 | (13,073,974 | ) | 26,936,496 | -206.0 | % | ||||||||||
| NET INCOME (LOSS) ATTRIBUTABLE TO NETWORK MEDICAL MANAGEMENT, INC. | $ | 12,817,101 | $ | (628,736 | ) | 13,445,837 | -2138.6 | % | ||||||||
| 303 |
Overview
Net income in 2015 was $26.7 million, as compared to net loss of $13.7 million in 2014, an increase of $40.4 million or 295%.
Membership Information
As of December 31, 2015 and 2014, the total number of affiliated physician groups managed by NMM was 12 groups and 12 groups, respectively, and the total number of affiliated physician group members for whom NMM managed the delivery of healthcare services was 606,078 and 400,873, respectively.
Revenues
NMM’s revenues in 2015 were $313.1 million, as compared to $134.3 million in 2014, an increase of $178.8 million or 133%. The increase in revenue was attributable to (i) increases in revenues generated from capitation and claims that were related to the merger of PIPA MSO in October 2014 and PHW in April 2015, (ii) increases in risk pool settlements and incentives of $24.7 million, which was mainly due to $9.7 million increase in risk pool IBNR accrual, $3.2 million in HNCC shared risk, $4.0 million from LA Care, $3.5 million increase in risk pool quarterly distribution as a result of the merger with PIPA MSO and PHW; (iii) increase in management fee income of $8.9 million, which was mainly driven by the increase of $6.0 million from LMA, (iv) increases in fees-for-service revenue of $0.5 million mainly due to fees received from Blue Cross, Blue Shield, LA Care, ICC and HNCC, (v) increases in other income of $0.3 million, and (vi) increases in surgery center income of $0.8 million due to increase in patients.
Contracted Physicians and other Services
Expenses related to contracted physicians and other services were $233.6 million in 2015, as compared to $110.5 million in 2014, an increase of $123.1 million, or 111%. Of this increase, $46.3 million was attributable to increased payments for capitations, which is consistent with the related capitation revenue increase, $49.7 million in medical claims, $36 million increase in discretionary provider bonus and $8.7 million increase in salaries and personnel related expenses due to new hires and transfers from the PIPA MSO merger. Such increases were offset by a decrease of $17.6 million in stock compensation expense.
General and Administrative Expenses
General and administrative expenses were $22.3 million in 2015, as compared to $27.3 million in 2014, a decrease of $5.0 million, or 18%. The decrease was attributable to a decrease in provider related administrative expenses of $6.9 million, offset by increases of $0.6 million in rent expenses from the PIPA MSO merger, $1.2 million in computer license expense.
| 304 |
Management Fees
Management fees in 2015 were $4.5 million, as compared to $8.3 million in 2014, a decrease of $3.8 million, or 46%. The decrease was attributable to a decrease in bonuses paid to directors in connection with the 2014 acquisitions.
Depreciation and Amortization
Depreciation and amortization expense in 2015 was $9.1 million, as compared to $1.4 million in 2014, an increase of $7.7 million, or 564%. The increase was attributable to acquisitions of PIPA in July 2014, and PIPA MSO and PHW in 2015, which resulted in significant increase in amortization expense associated with such intangible assets, as well increases in depreciation expense from purchases of property and equipment in 2015.
Income from Equity Method Investments
Income from equity method investments in 2015 was $1.2 million, as compared to $2.1 million in 2014, a decrease of $0.9 million or 42%, mainly due to the reduction in income allocation from LMA of $1.1 million, offset by income from investment of $0.2 million from PMIOC, Inc. and UCI.
Interest Expense
Interest expense in 2015 was $0.2 million, as compared to $0 in 2014, an increase of $0.2 million or 100%, mainly due to the amount of interest incurred on APC’s mortgage loan and NMM’s line of credit fees.
Interest Income
Interest income was $0.2 million, as compared to $0.1 million in 2014, an increase of $0.1 million or 76%, mainly due to more cash held in money market account which resulted in more interest earned in 2015.
Change in Fair Value of Derivative Instrument
Change in fair value of derivative instrument in 2015 was $0.8 million, as compared to $0 in 2014, an increase of $0.8 million or 100%, due to fair value adjustment of the warrant derivative instrument.
Other Income
Other income was $1.9 million for 2015, as compared to $0.1 million in 2014, an increase of $1.8 million or 1424%, mainly due to performance incentives received from LMA in 2015 with none in 2014.
Income Taxes
Provision for income taxes was $19.3 million in 2015, as compared to $2.9 million in 2014, an increase of $16.4 million or 558%. This increase is primarily attributable to increase in pre-tax income in 2015 in comparison to 2014. The 2014 income tax provision is as a result of a significant add back of stock based compensation to the 2014 pre-tax loss.
Net income attributable to noncontrolling interest
Net income attributable to noncontrolling interests was $13.9 million for the year ended December 31, 2015 compared to net loss attributable to noncontrolling interest of $13.1 million for the year ended December 31, 2014 for an increase of $26.9 million or 206% primarily due to net income generated from APC and CDSC.
| 305 |
Network Medical Management, Inc.
Condensed Consolidated Statements of Income (Unaudited)
Results of Operations - Comparison of the Six Months Ended June 30, 2017 and 2016
NMM’s unaudited consolidated operating results for the six months ended June 30, 2017, as compared to the six months ended June 30, 2016 were as follows:
| For the six months ended | ||||||||||||||||
| June 30, | June 30, | $ | % | |||||||||||||
| 2017 | 2016 | Variance | Variance | |||||||||||||
| REVENUES: | ||||||||||||||||
| Capitation, net | $ | 127,595,720 | $ | 122,749,816 | $ | 4,845,904 | 4 | % | ||||||||
| Risk pool settlements and incentives | 19,495,798 | 8,798,721 | 10,697,077 | 122 | % | |||||||||||
| Management fee income | 12,824,812 | 12,368,081 | 456,731 | 4 | % | |||||||||||
| Surgery center income, net | 3,433,189 | 3,132,574 | 300,615 | 10 | % | |||||||||||
| Fee-for-services, net | 2,275,272 | 965,515 | 1,309,757 | 136 | % | |||||||||||
| Other income | 1,022,971 | 1,106,677 | (83,706 | ) | -8 | % | ||||||||||
| Total revenues | 166,647,762 | 149,121,384 | 17,526,378 | 12 | % | |||||||||||
| EXPENSES: | ||||||||||||||||
| Contracted physicians and other services | 126,214,808 | 123,072,714 | 3,142,094 | 3 | % | |||||||||||
| General and administrative expenses | 10,858,762 | 8,730,524 | 2,128,238 | 24 | % | |||||||||||
| Management fees | 195,000 | 245,000 | (50,000 | ) | -20 | % | ||||||||||
| Depreciation and amortization | 9,642,330 | 8,648,783 | 993,547 | 11 | % | |||||||||||
| Total expenses | 146,910,900 | 140,697,021 | 6,213,879 | 4 | % | |||||||||||
| INCOME FROM OPERATIONS | 19,736,862 | 8,424,363 | 11,312,499 | 134 | % | |||||||||||
| OTHER INCOME AND (EXPENSES): | ||||||||||||||||
| Income from equity method investments | 1,432,160 | 5,782,047 | (4,349,887 | ) | -75 | % | ||||||||||
| Interest expense | (1,386 | ) | (58,766 | ) | 57,380 | -98 | % | |||||||||
| Interest income | 391,777 | 236,623 | 155,154 | 66 | % | |||||||||||
| Change in fair value of derivative instrument | 127,779 | (594,444 | ) | 722,223 | -121 | % | ||||||||||
| Other income | 28,138 | 43,284 | (15,146 | ) | -35 | % | ||||||||||
| Total other income, net | 1,978,468 | 5,408,744 | (3,430,276 | ) | -63 | % | ||||||||||
| INCOME BEFORE PROVISION FOR INCOME TAXES | 21,715,330 | 13,833,107 | 7,882,223 | 57 | % | |||||||||||
| Provision for income taxes | 8,626,080 | 5,730,590 | 2,895,490 | 51 | % | |||||||||||
| NET INCOME | $ | 13,089,250 | $ | 8,102,517 | $ | 4,986,733 | 62 | % | ||||||||
| Less: net income attributable
to noncontrolling interest |
6,744,846 | 1,801,530 | 4,943,316 | 274 | % | |||||||||||
| NET LOSS ATTRIBUTABLE TO
NETWORK MEDICAL MANAGEMENT, INC.’S SHAREHOLDERS |
$ | 6,344,404 | $ | 6,300,987 | $ | 43,417 | 1 | % | ||||||||
Overview
Net income for the six months ended June 30, 2017 of $6.3 million is consistent and comparable with the same period of the prior year.
Membership Information
As of June 30, 2017 and June 30, 2016, the total number of affiliated physician groups managed by NMM was 10 groups and 11 groups, respectively, and the total number of affiliated physician group members for whom NMM managed the delivery of healthcare services was 615,270 and 615,376, respectively.
Revenues
NMM’s revenues for the six months ended June 30, 2017 were $166.6 million, as compared to $149.1 million for the same period of the prior year, an increase of $17.5 million or 12%. The increase in revenue was attributable to an (i) increase of $4.8 million in capitation and claims revenue related to a net increase in members in the total pool of HMOs and adjustments to capitation rates; (ii) increase of $10.7 million in risk pool settlements and incentives revenue due to $5.8 million from Health Net Covered California (“HNCC”) 2015 shared risk payment , increase of $4.3 million in pre PIPA merger risk pool settlement received, increase of $0.4 million in from 2016 Healthcare Effectiveness Data and Information Set (“HEDIS”) incentive and increase of $0.2 million in AHMC Healthcare 2015 incentives; (iii) increase of $1.3 million in fees for service revenue mainly due to fees received from Blue Cross, Blue Shield, LA Care and HNCC; (iv) increase in management fee income of $0.5 million and (v) an increase of $0.3 million in surgery center income due to increase in number of cases performed, offset by a decrease in other income of $0.1 million.
| 306 |
Contracted Physicians and Other Services
Contracted physicians and other services for the six months ended June 30, 2017 were $126.2 million, as compared to $123.1 million for the same period of the prior year, an increase of $3.1 million or 3%. The increase in contracted physicians and other services was attributable to (i) increase in salary and personnel expenses of $1.3 million, (ii) increase in claims expense of $5.8 million and (iii) increase in provider bonus of $3.9 million, offset by a decrease in capitation expense of $7.9 million, which is related to decreases in senior capitation rates.
General and Administrative Expenses
General and administrative expenses were $10.8 million for the six months ended June 30, 2017, as compared to $8.7 million for the same period of the prior year, an increase of $2.1 million, or 24%. The increase was attributable to (i) increase in accounting fees of $0.9 million, (ii) increase in legal fees of $0.3 million, (iii) increase in computer expense of $0.3 million, (iv) increase in rent expense of $0.2 million, (v) increase in consulting expense of $0.1 million, (vi) increase in marketing expense of $0.6 million, (vii) increase in provider relation expense of $0.1 million, offset by decrease in 401(K) expense of $0.1 million, decrease in transportation expense of $0.1 million and decrease in other general and administrative expenses of $0.2 million
Management Fees
Management fees of $0.2 million for the six months ended June 30, 2017 were comparable and consistent with the same period of prior year.
Depreciation and Amortization
Depreciation and amortization expense was $9.6 million for the six months ended June 30, 2017, as compared to $8.6 million for the same period of the prior year, an increase of $1.0 million, or 11%. The increase was attributable to increase in amortization expense associated with intangible assets, as well increases in depreciation expense from purchases of property and equipment in 2017.
Income from Equity Method Investments
Income from equity method investments was $1.4 million for the six months ended June 30, 2017, as compared to $5.8 million for the same period of the prior year, a decrease of $4.3 million or 75%, mainly due to the reduction in income allocation from LMA of $2.4 million and UCI of $2.5 million, offset by income from investment of $0.6 million from DMG.
Interest Income
Interest income for the six months ended June 30, 2017 was $0.4 million, as compared to $0.2 million for the same period of prior year, which was mainly attributable to the interest income from the related party loan receivable due from ApolloMed and interest income earned from money market accounts.
Change in Fair Value of Derivative Instrument
Change in fair value of derivative instrument was a gain of $0.1 million for the six months ended June 30, 2017, as compared to a loss of $(0.6) million for the same period of the prior year, a decrease of $0.7 million or 121%, mainly due to increase in the stock price of ApolloMed common stock.
Income Taxes
Provision for income taxes was $8.6 million for the six months ended June 30, 2017, as compared to $5.7 million for the same period of the prior year, a decrease of $2.9 million or 51%, primarily attributable to an increase in pre-tax income in the six months ended June 30, 2017 in comparison to June 30, 2016.
Net income attributable to noncontrolling interest
Net income attributable to noncontrolling interests was $6.7 million for the six months ended June 30, 2017, as compared to $1.8 million for the same period of the prior year or an increase of $4.9 million or 274% primarily due to net income generated from APC and CDSC.
| 307 |
Liquidity and Capital Resources
Cash, cash equivalents and investment in marketable securities at June 30, 2017 totaled $66.8 million. Working capital totaled $34.1 million at June 30, 2017, compared to $30.5 million at December 31, 2016, an increase of $3.6 million, or 12%.
NMM has historically financed its operations primarily through internally generated funds. NMM generates cash primarily from fees for medical management services provided to its affiliated physician groups. NMM generally invests cash in money market accounts, which are classified as cash and cash equivalents.
| 308 |
At June 30, 2017, NMM’s cash and cash equivalents increased by $11.0 million from $54.8 million at December 31, 2016 to $65.8 million at June 30, 2017. Cash provided by operating activities during the six months ended June 30, 2017 was $24.8 million, as compared to $1.2 million during the six months ended June 30, 2016. The following non-cash expenses also contributed to the cash provided by operating activities during the six months ended June 30, 2017: depreciation and amortization of $9.6 million, share-based compensation of $0.6 million, gain from change in fair value of derivative instrument of $0.1 million, income from equity method investments of $1.4 million and change in deferred tax liability of $4.4 million. NMM’s cash provided by operating activities includes a net increase in operating assets and liabilities of $7.4 million.
Cash used in investing activities during the six months ended June 30, 2017 was $4.7 million, as compared to $6.2 million during the six months ended June 30, 2016, for which the increase is primarily attributable to advances to affiliate of $5.0 million, purchases of property of equipment of $0.9 million, offset by dividends received from equity method investee of $1.0 million and proceeds from loans receivable of $0.2 million during the six months ended June 30, 2017.
Cash used in financing activities during the six months ended June 30, 2017 was $9.1 million, as compared to $1.4 million during the six months ended June 30, 2016, for which the increase is primarily attributable to dividend payments of $9.5 million, offset by proceeds from exercise of stock options of $0.4 million during the six months ended June 30, 2017.
Credit Facility
In April 2012, NMM entered into the NMM Business Loan Agreement, which was amended on April 9, 2016 and April 7, 2017. The NMM Business Loan Agreement modifies certain terms of the promissory note agreement in order to increase the loan availability amount of $10,000,000 to $20,000,000. The interest rate is based on the Wall Street Journal “prime rate” plus 0.125% or 4.375% and 3.875% as of June 30, 2017 and December 31, 2016, respectively. As of June 30, 2017, NMM was in compliance with the financial debt covenant requirements contained in the loan agreement. As of December 31, 2016, NMM was not in compliance with certain financial debt covenant requirements contained in the loan agreement. Subsequent to year end, NMM obtained a waiver from the bank for noncompliance of the financial debt covenant requirements as of and for the years ended December 31, 2016 and 2015. The loan is personally guaranteed by 14 shareholders and a Trust held by NMM’s Chief Executive Officer, 13 of which are also members of NMM’s board of directors and is collateralized by substantially all assets of NMM. No amounts were drawn on this line during 2016 and 2015 and through June 30, 2017. In addition, no amounts were outstanding as of June 30, 2017 and December 31, 2016.
In April 2012, APC entered into a promissory note agreement with a bank, which was amended on April 22, 2016 and April 7, 2017 (as amended, the “APC Business Loan Agreement”). The APC Business Loan Agreement modifies certain terms of the promissory note agreement in order to (i) increase the original loan availability amount of $3,000,000 to $10,000,000, (ii) extend the maturity date under the promissory note agreement to April 22, 2018, and (iii) add six additional guarantees. The interest rate is based on the Wall Street Journal “prime rate” plus 0.125% or 4.375% and 3.875% as of June 30, 2017 and December 31, 2016, respectively. As of June 30, 2017 and December 31, 2016, APC was not in compliance with certain financial debt covenant requirements contained in the loan agreement. Subsequent to year end, APC obtained a waiver from the bank for noncompliance of the financial debt covenant requirements as of June 30, 2017 and December 31, 2016. The loan is personally guaranteed by 13 shareholders who are also members of NMM’s board of directors and two-non board members and is collateralized by substantially all assets of APC. No amounts were drawn on this line during 2016 and 2015 and through June 30, 2017. In addition, no amounts were outstanding as of June 30, 2017 and December 31, 2016.
Critical Accounting Policies and Estimates
The preparation of the condensed consolidated financial statements of NMM in accordance with U.S. generally accepted accounting principles requires its management to make a number of estimates and assumptions relating to the reported amount of assets and liabilities and the disclosure of contingent assets and liabilities at the date of the consolidated financial statements and to the reported amounts of revenues and expenses during the period. NMM bases its estimates on historical experience and on various other assumptions that NMM believes are reasonable under the circumstances. Changes in estimates are recorded if and when better information becomes available. Actual results could significantly differ from those estimates under different assumptions and conditions. NMM believes that the accounting policies discussed below are those that are most important to the presentation of its financial condition and results of operations and that require its management’s most difficult, subjective and complex judgments.
| 309 |
Principles of Consolidation
NMM’s condensed consolidated financial statements have been prepared by management in accordance with GAAP and include the accounts of NMM and its consolidated VIE, APC and its subsidiary UCAP and APC’s consolidated VIEs, CDSC and APC-LSMA. As of the effective dates of the reorganizations, as described above, the accounts of APCN-ACO and AP-ACO were also included in the consolidation of NMM.
All material intercompany balances and transactions have been eliminated in consolidation.
Use of Estimates
The preparation of condensed consolidated financial statements and related disclosures in conformity with GAAP requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the condensed consolidated financial statements and the reported amounts of revenues and expenses during the reporting period. Significant items subject to such estimates and assumptions include collectability of receivables, recoverability of long-lived and intangible assets, business combination and goodwill valuation and impairment, derivative assets, accrual of medical liabilities (including incurred but not reported claims), determination of shared-risk revenues and receivables, income taxes and valuation of share-based compensation. Management evaluates its estimates and assumptions on an ongoing basis using historical experience and other factors, including the current economic environment, and makes adjustments when facts and circumstances dictate. As future events and their effects cannot be determined with precision, actual results could differ materially from those estimates and assumptions.
Receivables
NMM’s receivables are comprised of accounts receivable, capitation and claims receivable, risk pool and incentive receivables. Accounts receivable primarily consists of NMM management fee receivables and CDSC FFS receivables.
Risk pool and incentive receivables mainly consist of APC full risk pool receivable which is recorded based on a modified cash basis, whereby a receivable is only recorded when expected cash receipts are known or when actual cash is received from Health Source MSO’s who serves as the management company for the hospitals in the risk pools. Capitation and claims receivable relate to the health plan’s capitation which is received by APC in the following month of service. For APC, other receivables are accrued based on invoices sent to the subcontracted IPA for stop loss insurance premium reimbursement and FFS reimbursement for Alhambra Hospital Medical Center’s self–insured program. For NMM, other receivables are accrued based on invoices for certain expense reimbursements from UCI and invoice for transportation reimbursement from the hospital.
Amounts are recorded as a receivable when NMM is able to determine amounts receivable under these contracts and/or agreements based on information provided and collection is reasonably likely to occur. NMM continuously monitors its collections of receivables and its policy is to write off receivables when they are determined to be uncollectible. NMM has not incurred credit losses related to receivables. No allowance for doubtful accounts is recorded at June 30, 2017 and December 31, 2016.
| 310 |
Fair Value Measurements
NMM’s financial instruments consist of cash and cash equivalents, restricted cash, fiduciary cash, investment in marketable securities, accounts receivable, loans receivable – related parties, derivative asset warrants, accounts payable, certain accrued expenses, bank loan, loan payable – related party and the line of credit. The carrying values of the financial instruments classified as current in the accompanying condensed consolidated balance sheets are considered to be at their fair values, due to the short maturity of these instruments. The carrying amount of the long-term bank loan and line of credit approximates fair value as they bear interest at rates that approximate current market rates for debt with similar maturities and credit quality. FASB ASC 820, Fair Value Measurement (“ASC 820”), applies to all financial assets and financial liabilities that are measured and reported on a fair value basis and requires disclosure that establishes a framework for measuring fair value and expands disclosure about fair value measurements. ASC 820 establishes a fair value hierarchy for disclosures of the inputs to valuations used to measure fair value.
This hierarchy prioritizes the inputs into three broad levels as follows:
Level 1—Inputs are unadjusted quoted prices in active markets for identical assets or liabilities that can be accessed at the measurement date.
Level 2—Inputs include quoted prices for similar assets and liabilities in active markets, quoted prices for identical or similar assets or liabilities in markets that are not active, inputs other than quoted prices that are observable for the asset or liability (i.e., interest rates and yield curves), and inputs that are derived principally from or corroborated by observable market data by correlation or other means (market corroborated inputs).
Level 3—Unobservable inputs that reflect assumptions about what market participants would use in pricing the asset or liability. These inputs would be based on the best information available, including NMM’s own data.
Business Combinations
NMM uses the acquisition method of accounting for all business combinations, which requires assets and liabilities of the acquiree to be recorded at fair value, to measure the fair value of the consideration transferred, including contingent consideration, to be determined on the acquisition date, and to account for acquisition related costs separately from the business combination.
Investments in Other Entities (see “RELATED PARTY TRANSACTIONS - Certain Relationships and Related Party Transactions of NMM” for a description of such other entities)
Equity Method
NMM accounts for certain investments using the equity method of accounting when it is determined that the investment provides NMM the ability to exercise significant influence, but not control, over the investee. Significant influence is generally deemed to exist if NMM has an ownership interest in the voting stock of the investee of between 20% and 50%, although other factors, such as representation on the investee’s board of directors, are considered in determining whether the equity method of accounting is appropriate. Under the equity method of accounting, the investment, originally recorded at cost, is adjusted to recognize NMM’s share of net earnings or losses of the investee and is recognized in the consolidated statements of income under “Income from equity method investments” and also is adjusted by contributions to and distributions from the investee. Equity method investments are subject to impairment evaluation. No impairment loss was recorded on equity method investments for the three and six months ended June 30, 2017 and 2016.
Cost Method
NMM uses the cost method to account for investments in companies for which it does not exercise significant influence or control.
NMM reviews its investments in other entities accounted under cost method to determine whether events or changes in circumstances indicate that the investment carrying amount may not be recoverable. The primary factors NMM considers in its determination are the financial condition, operating performance and near term prospects of the investee. If the decline in value is deemed to be other than temporary, NMM would recognize an impairment loss. No impairment loss was recorded on equity method investments for the three and six months ended June 30, 2017 and 2016.
| 311 |
Share-Based Compensation
NMM accounts for share-based compensation arrangements in accordance with ASC 718, Compensation—Stock Compensation, which requires the measurement and recognition of compensation expense for all share-based payment awards to employees and nonemployees based on estimated fair values. ASC 718 further requires a reduction in share-based compensation expense by an estimated forfeiture rate.
NMM uses the Black-Scholes option pricing model to estimate the fair value of stock option awards at the grant date. The model requires the input of highly subjective assumptions, including NMM’s estimated share price, expected stock price volatility, which is based on taking the average historical price volatility for industry peers based on daily price observations over a period equivalent to the expected term of the awards, the expected dividend yield, the expected term of an option, and the risk-free interest rate, which is based on the US Treasury yield curve in effect at the time of grant. NMM uses historical employee exercise behavior, forfeitures, cancellations, and other factors to estimate the expected term.
Changes in subjective input assumptions can materially affect the fair value estimates of an option. Furthermore, the estimated fair value of an option does not necessarily represent the value that will ultimately be realized.
NMM accounts for equity instruments issued to nonemployees and consultants in exchange for goods and services under ASC 505-50, Equity-Based Payments to Non-Employees. As such, the value of the applicable share-based compensation is periodically remeasured using an appropriate valuation model and income or expense is recognized during the vesting terms of the equity instruments. The measurement date for the estimated fair value of the equity instruments issued is the earlier of (i) the date at which a commitment for performance by the nonemployee or consultant is reached or (ii) the date at which the nonemployee or consultant’s performance is complete. In the case of equity instruments issued to consultants, the estimated fair value of the equity instrument is primarily recognized over the term of the consulting agreement.
Noncontrolling Interests
NMM consolidates entities in which NMM has a controlling financial interest. NMM consolidates subsidiaries in which it holds, directly or indirectly, more than 50% of the voting rights, and VIEs in which the NMM is the primary beneficiary. Noncontrolling interests represent third-party equity ownership interests in NMM’s consolidated entities.
Based on the Shareholder Agreement for both NMM and APC, in the event of a disqualifying event, as defined in the agreement, NMM and APC could be required to repurchase the shares from the shareholder based on the triggers outlined in Section 4.1 of the Shareholder Agreement. The triggers that could cause NMM to redeem the shares (redemption feature) is not solely within the control of NMM or APC. As the redemption feature of the shares is not solely within the control of NMM, the common stock and additional paid-in capital of NMM has been classified as mezzanine or temporary equity as redeemable common stock. In addition, as the redemption feature of the shares is not solely within the control of APC, the equity transactions of APC do not qualify as permanent equity and has been classified as mezzanine or temporary equity, accordingly, NMM recognizes noncontrolling interests as mezzanine equity in the consolidated financial statements separate from NMM’s equity. Noncontrolling interests’ partners have less than 50% share of voting rights at any one of the subsidiary or VIE companies. The amount of net income attributable to noncontrolling interests is included in consolidated net income on the face of the consolidated statements of income.
Revenue Recognition
Revenue primarily consists of capitation revenue, risk pool settlements and incentives, management fee income, surgery center income and FFS. Revenue is recorded in the period in which services are rendered. The form of billing and related risk of collection for such services may vary by customer. The following is a summary of the principal forms of APC’s billing arrangements and how revenue is recognized for each.
| 312 |
Capitation, Net
Capitation revenue (net of capitation withheld to fund risk share deficits) is recognized in the month in which the services are provided. Minor ongoing adjustments to prior months’ capitation, primarily arising from HMOs finalizing of monthly eligibility data for additions or subtractions of enrollees, are recognized in the month they are communicated to APC.
Managed care revenues of APC consist primarily of capitated fees for medical services provided by APC under a provider service agreement (“PSA”) or capitated arrangements directly made with various managed care providers including HMO’s and management service organizations (“MSOs”). Capitation revenue under the PSA and HMO contracts is prepaid monthly to APC based on the number of enrollees electing APC as their healthcare provider. Health plans and providers with higher acuity enrollees will receive more and those with lower acuity enrollees will receive less.
Risk Pool Settlements and Incentives
Contracts with HMO’s also include provisions for APC to participate in the risk (shared risk capitation arrangements) relating to the provision of institutional services (institutional risk) to enrollees, such that APC can earn additional incentive revenue or incur losses based upon the enrollee utilization of hospital services. Typically, any shared risk deficits are not payable until and unless APC generates future risk sharing surpluses, or if the HMO withholds a portion of the capitation revenue to fund any risk share deficits. At the termination of the HMO contract, any accumulated risk share deficit is typically extinguished. Due to the lack of access to information necessary to estimate the related healthcare costs (IBNR), revenue from shared risk amounts are recorded when such amounts are known. In addition to risk sharing revenues, APC is also eligible to participate in an incentive program. As an incentive to control enrollee utilization and to promote quality care, the HMOs have designed the quality incentive programs and commercial generic pharmacy incentive programs to compensate APC for efforts it takes to improve the quality of services and for efficient and effective use of pharmacy supplemental benefits provided to the HMO’s members. The incentive programs track specific performance measures and calculate payments to the IPA based on the performance measures.
APC also enter into risk sharing arrangements with affiliated hospitals (full risk capitation arrangements) who in turn have entered into capitation arrangements with various HMOs, pursuant to which the affiliated hospital provides, arranges and pays for institutional risk. Under a risk pool sharing agreement, APC is allocated a percentage of the affiliated hospitals surplus or deficit from the risk pool, after deductions for the affiliated hospitals costs. Advance settlement payments are typically made quarterly in arrears if there is a surplus. However, due to the uncertainty around the settlement of the related IBNR reserve, APC recognizes any excess IBNR reserve on settlement as risk pool settlement revenue when amounts are known. Any excess IBNR is normally settled and paid after a period of approximately one year from the related service period.
Management Fee Income
NMM provides claims processing and other administrative services for other IPAs. NMM receives management fee income for the services rendered. Management fees are calculated as a percentage of revenue under capitation contracts with various insurance companies.
Surgery Center Income
CDSC’s surgery center income consists primarily of net patient service revenues that are recorded based upon established billing rates less allowance for contractual adjustments. Revenues are recorded in the period in which the healthcare services are provided, based upon the estimated amounts due from patients and third-party payors, including commercial health plans, employers, workers’ compensation plans and federal and state agencies (under the Medicare and Medicaid programs). CDSC utilizes the payment history specific to each payor and services to record estimated net revenues to ensure the appropriateness of these estimates. Third-party payor contractual payment terms are generally based upon predetermined rates per procedure or FFS rates.
| 313 |
FFS
FFS revenue primarily represents professional component of charges for medical services rendered by NMM’s contracted physicians and paid to NMM for certain reimbursable services which is recognized at the time reimbursements are received from the health plans.
Goodwill and Intangible Assets
Under FASB ASC 350, Intangibles – Goodwill and Other (“ASC 350”), goodwill and indefinite-lived intangible assets are reviewed at least annually for impairment. Acquired intangible assets with definite lives are amortized over their individual useful lives.
Goodwill represents the excess cost of a business acquisition over the fair value of the net assets acquired.
Identifiable intangible assets with definite useful lives consist primarily of network/payor relationships, management contracts and member relationships, and are amortized between 5 – 15 years on an accelerated method using the discounted cash flow rate. Intangible assets are measured for impairment when events or changes in business conditions suggest that the carrying value of an asset may not be recovered. No intangible assets were deemed to be impaired at June 30, 2017 and December 31, 2016.
Recent Accounting Pronouncements
In May 2014, the FASB issued a new revenue recognition standard, Accounting Standards Update (“ASU”) No. 2014-09, Revenue From Contracts with Customers (Topic 606) (“ASC 2014-09”), that will supersede nearly all existing revenue recognition guidance under GAAP. The revenue recognition standard will allow for the recognition of revenue when a company transfers promised goods or services to customers in an amount that reflects the consideration to which NMM expects to be entitled in exchange for those goods or services. The standard permits the use of either a full retrospective or retrospective with cumulative effect transition method. On August 8, 2015, the FASB issued ASU No. 2015-14, which defers the effective date of ASU No. 2014-09 by one year. The standard is effective for nonpublic entities for annual periods beginning after December 15, 2018, and interim reporting periods within annual reporting periods beginning after December 15, 2019, with the earliest option of adoption being the fiscal year beginning after December 15, 2016. In addition, the FASB issued the following accounting standard updates related to Topic 606, Revenue From Contracts with Customers:
| · | ASU No. 2016-08, Revenue From Contracts with Customers (Topic 606): Principal versus Agent Considerations (Reporting Revenue Gross versus Net) ("ASU 2016-08") in March 2016. ASU 2016-08 does not change the core principle of revenue recognition in Topic 606 but clarifies the implementation guidance on principal versus agent considerations. |
| · | ASU No. 2016-10, Revenue From Contracts with Customers (Topic 606): Identifying Performance Obligations and Licensing ("ASU 2016-10") in April 2016. ASU 2016-10 does not change the core principle of revenue recognition in Topic 606 but clarifies the implementation guidance on identifying performance obligations and the licensing implementation guidance, while retaining the related principles for those areas. |
| · | ASU No. 2016-12, Revenue From Contracts with Customers (Topic 606): Narrow-Scope Improvements and Practical Expedients ("ASU 2016-12") in May 2016. ASU 2016-12 does not change the core principle of revenue recognition in Topic 606 but clarifies the implementation guidance on a few narrow areas and adds some practical expedients to the guidance. |
| 314 |
| · | ASU No. 2016-20, Technical Corrections and Improvements to Topic 606, Revenue From Contracts with Customers (“ASU 2016-20”) in December 2016. ASU 2016-20 does not change the core principle of revenue recognition in Topic 606 but affects narrow aspects of the guidance issued in ASU 2014-09. |
NMM is currently evaluating the impact of ASC 606 on its consolidated financial statements. However, at the current time NMM does not know what impact the new standard will have on revenue recognized and other accounting decisions in future periods, if any, nor what method of adoption will be selected if the impact is material.
In August 2014, the FASB issued ASU No. 2014-15, Presentation of Financial Statements—Going Concern, which will require an entity’s management to assess, for each annual and interim period, whether there is substantial doubt about the entity’s ability to continue as a going concern within one year of the consolidated financial statement issuance date. The definition of substantial doubt within the new standard incorporates a likelihood threshold of “probable” similar to the use of that term under current GAAP for loss contingencies. Certain disclosures will be required if conditions give rise to substantial doubt. ASU 2014-15 is effective for annual periods ending after December 15, 2016, and interim periods within annual periods beginning after December 15, 2016. ASU 2014-15 became effective for NMM as of December 31, 2016. The adoption of this standard did not have any impact on NMM’s current disclosures in the consolidated financial statements.
In February 2015, the FASB issued ASU No. 2015-02, Consolidation (Topic 810): Amendments to the Consolidation Analysis (“ASU 2015-02”). This update changes the guidance with respect to the analyses that a reporting entity must perform to determine whether it should consolidate certain types of legal entities. All legal entities are subject to reevaluation under the revised consolidation model. The new guidance affects the following areas: (1) limited partnerships and similar legal entities, (2) evaluating fees paid to a decision maker or a service provider as a variable interest, (3) the effect of fee arrangements on the primary beneficiary determination, (4) the effect of related parties on the primary beneficiary determination, and (5) certain investment funds. ASU 2015-02 is effective for fiscal years beginning after December 15, 2016, and interim periods within fiscal years beginning after December 15, 2017. Early adoption is permitted, including adoption in an interim period. NMM early adopted ASU 2015-02 effective for the year ended December 31, 2015. The adoption did not have a significant impact on NMM’s consolidated financial statements.
In November 2015, the FASB issued ASU No. 2015-17, Income Taxes (Topic 740): Balance Sheet Classification of Deferred Taxes (“ASU 2015-17”). This amendment simplifies the presentation of deferred tax assets and liabilities on the balance sheet and requires all deferred tax assets and liabilities, along with any related valuation allowance, to be treated as non-current. ASU 2015-17 is effective for financial statements issued for annual periods beginning after December 15, 2017 and interim periods within annual periods beginning after December 15, 2018, with early adoption permitted as of the beginning of an interim or annual reporting period. NMM early adopted ASU 2015-17 with retrospective effect to all periods presented and the adoption did not have any impact on fiscal year 2015.
In January 2016, the FASB issued ASU No. 2016-01, Financial Instruments - Overall (Subtopic 825-10): Recognition and Measurement of Financial Assets and Financial Liabilities ("ASU 2016-01"). ASU 2016-01 addresses certain aspects of recognition, measurement, presentation and disclosures of financial instruments including the requirement to measure certain equity investments at fair value with changes in fair value recognized in net income. ASU 2016-01 will become effective for NMM for fiscal year beginning after December 15, 2018, and interim periods within fiscal years beginning after December 15, 2019. NMM is currently evaluating the guidance to determine the potential impact on its financial position, results of operations, cash flows and related disclosures.
In March 2016, the FASB issued ASU No. 2016-07, Investments – Equity Method and Joint Ventures (Topic 323): Simplifying the Transition to the Equity Method of Accounting ("ASU 2016-07"), which eliminates the requirement that when an investment qualifies for use of the equity method as a result of an increase in the level of ownership interest or degree of influence, an investor must adjust the investment, results of operations, and retained earnings retroactively on a step-by-step basis as if the equity method had been in effect during all previous periods that the investment had been held. The amendments in this ASU are effective for financial statements issued for fiscal years, and interim periods within those fiscal years, beginning after December 15, 2016. The amendments should be applied prospectively upon their effective date to increases in the level of ownership interest or degree of influence that result in the adoption of the equity method. Early adoption of the amendments is permitted. Accordingly, NMM will adopt ASU 2016-07 in 2017 and such adoption is not expected to have an impact on NMM’s consolidated financial statements and footnote disclosures.
| 315 |
In February 2016, the FASB issued ASU No. 2016-02, Leases (Topic 842) (“ASU 2016-02”), which will require organizations to recognize lease assets and lease liabilities on the balance sheet, including leases that were previously classified as operating leases. The ASU will also require additional disclosures about leasing arrangements related to the amount, timing, and uncertainty of cash flows arising from leases. The amendments in this ASU are effective for financial statements issued for fiscal years beginning after December 15, 2019, and interim periods within fiscal years beginning after December 15, 2020. Early adoption of the amendments is permitted and the new guidance shall be applied using a modified retrospective approach. NMM is currently evaluating the impact of the adoption of this standard on its consolidated financial statements and footnote disclosures.
In March 2016, the FASB issued ASU No. 2016-09, Compensation - Stock Compensation (Topic 718): Improvements to Employee Share-Based Payment Accounting (“ASU 2016-09”). This ASU makes several modifications to Topic 718 related to the accounting for forfeitures, employer tax withholding on share-based compensation, and the financial statement presentation of excess tax benefits or deficiencies. ASU 2016-09 also clarifies the statement of cash flows presentation for certain components of share-based awards. The standard is effective for annual reporting periods beginning after December 15, 2017 and interim periods within annual periods beginning after December 15, 2018, with early adoption permitted. NMM expects to adopt this guidance when effective and is currently evaluating the effect that the updated standard will have on its consolidated financial statements and related disclosures.
In August 2016, the FASB issued ASU No. 2016-15, Statement of Cash Flows (Topic 230) – Classification of Certain Cash Receipts and Cash Payments (“ASU 2016-15”). This ASU provides clarification regarding how certain cash receipts and cash payments are presented and classified in the statement of cash flows. This ASU addresses eight specific cash flow issues with the objective of reducing the existing diversity in practice. The issues addressed in this ASU that will affect NMM are classifying debt prepayments or debt extinguishment costs, distributions received from equity method investees, and contingent consideration payments made after a business combination. This update is effective for fiscal years beginning after December 15, 2018, and interim periods within fiscal years beginning after December 15, 2019. Early adoption is permitted, including adoption in an interim period. NMM is currently assessing the impact the adoption of ASU 2016-15 will have on NMM’s consolidated financial statements.
In October 2016, the FASB issued ASU No. 2016-17, Consolidation (Topic 810): Interests Held through Related Parties that are under Common Control ("ASU 2016-17"). ASU 2016-17 amends the consolidation guidance on how a reporting entity that is the single decision maker of a VIE should treat indirect interest in the entity held through related parties that are under common control with the reporting entity when determining whether it is the primary beneficiary of that VIE. Entities that already have adopted ASU 2015-02 are required to apply ASU 2016-17 retrospectively to all relevant prior periods beginning with the fiscal year in which ASU 2015-02 was initially applied. Accordingly, NMM retrospectively adopted ASU 2016-17 effective December 31, 2015 and such adoption did not have an impact on NMM’s consolidated financial statements.
In November 2016, the FASB issued ASU No. 2016-18, Statement of Cash Flows (Topic 230): Restricted Cash ("ASU 2016-18”). The amendments in ASU 2016-18 require that a statement of cash flows explain the change during the period in the total of cash, cash equivalents, and amounts generally described as restricted cash or restricted cash equivalents. ASU 2016-17 is effective for fiscal years beginning after December 15, 2018, and interim periods within fiscal years beginning after December 15, 2019. Early adoption is permitted, including adoption in an interim period. NMM is currently assessing the impact the adoption of ASU 2016-18 will have on NMM’s consolidated financial statements.
| 316 |
In January 2017, the FASB issued ASU No. 2017-01, Business Combinations (Topic 805): Clarifying the Definition of a Business (“ASU 2017-01”). This ASU provides a screen to determine when a set is not a business, which requires that when substantially all of the fair value of the gross assets acquired (or disposed of) is concentrated in a single identifiable asset or a group of similar identifiable assets, the set is not a business, which reduces the number of transactions that need to be further evaluated. If the screen is not met, this ASU require that to be considered a business, a set must include, at a minimum, an input and a substantive process that together significantly contribute to the ability to create output and also remove the evaluation of whether a market participant could replace missing elements. This update is effective for annual periods beginning after December 15, 2018, and interim periods within annual periods beginning after December 15, 2019. NMM is currently assessing the impact the adoption of ASU 2017-01 will have on NMM’s consolidated financial statements.
In January 2017, the FASB issued ASU No. 2017-04, Intangibles – Goodwill and Other (Topic 350): Simplifying the Test for Goodwill Impairment (“ASU 2017-04”). This ASU eliminates Step 2 from the goodwill impairment test if the carrying amount exceeds the fair value of a reporting unit and also eliminates the requirements for any reporting unit with a zero or negative carrying amount to perform a qualitative assessment and, if it fails that qualitative test, to perform Step 2 of the goodwill impairment test. Therefore, the same impairment assessment applies to all reporting units. An entity is required to disclose the amount of goodwill allocated to each reporting unit with a zero or negative carrying amount of net assets. This update is effective on a prospective basis for annual and interim goodwill impairment tests performed for periods beginning after December 15, 2021. Early adoption is permitted for interim and annual goodwill impairment tests performed on testing dates after January 1, 2017. NMM is currently assessing the impact the adoption of ASU 2017-04 will have on NMM’s consolidated financial statements.
Contractual Obligations and Reserves
The below table summarizes by maturity NMM’s significant approximate contractual obligations and reserves as of June 30, 2017:
| Payments due by Period | ||||||||||||||||||||
| Total | 2017 (remaining) | 2018-2019 | 2020-2021 | 2022 and beyond |
||||||||||||||||
| Operating leases (1) | $ | 5,105,000 | $ | 975,000 | $ | 2,600,000 | $ | 1,530,000 | $ | - | ||||||||||
| Capital leases (2) | $ | 48,000 | $ | 48,000 | $ | - | $ | - | $ | - | ||||||||||
| Total contractual obligations | $ | 5,153,000 | $ | 1,023,000 | $ | 2,600,000 | $ | 1,530,000 | $ | - | ||||||||||
(1) Represents lease payments for NMM’s office and equipment rentals.
(2) Represents payments related to computer equipment.
Off-Balance Sheet Arrangements
NMM has no off-balance sheet arrangements that have or are reasonably likely to have a current or future effect on its financial condition, changes in financial condition, revenues or expenses, results of operations, liquidity, capital expenditures or capital resources that are material to investors.
| 317 |
DESCRIPTION OF APOLLOMED CAPITAL STOCK
As a result of the Merger, NMM shareholders who receive shares of ApolloMed common stock in the Merger will become stockholders of ApolloMed. The rights of stockholders of ApolloMed will be governed by Delaware law, the ApolloMed Charter and the ApolloMed Bylaws, as amended. The following briefly summarizes the material terms of ApolloMed’s common stock and Series A and Series B preferred stock. ApolloMed urges you to read the applicable provisions of the DGCL, the ApolloMed Charter and the ApolloMed Bylaws, as well as the proposed amendments to the ApolloMed Charter and the ApolloMed Bylaws carefully in their entirety. Marked copies of the proposed amendments to the ApolloMed Charter and the ApolloMed Bylaws are included in this joint proxy statement/prospectus as Annexes E and F, respectively.
ApolloMed’s authorized capital stock consists of 100,000,000 shares of common stock, par value $0.001 per share, and 5,000,000 shares of preferred stock, $0.001 par value per share of which 1,111,111 shares are designated for Series A preferred stock and 555,555 shares are designated for Series B preferred stock.
As of October 30, 2017, ApolloMed had the following issued and outstanding on a fully diluted basis:
| · | 6,033,495 shares of ApolloMed’s common stock; |
| · | 1,111,111 shares of Series A preferred stock; |
| · | 555,555 shares of Series B preferred stock; |
| · | warrants to purchase an aggregate of 1,970,166 shares of ApolloMed’s common stock; and |
| · | stock options to purchase an aggregate of 1,165,850 shares of ApolloMed commons stock. |
ApolloMed is authorized to issue up to a total of 100,000,000 shares of common stock, par value $0.001 per share. Holders of ApolloMed common stock are entitled to one vote for each share held on all matters submitted to a vote of ApolloMed stockholders. Holders of ApolloMed common stock have no cumulative voting rights or preemptive or conversion rights or other subscription rights. Upon ApolloMed’s liquidation, dissolution or winding-up, holders of ApolloMed common stock are entitled to share in all assets remaining after payment of all liabilities and the liquidation preferences of any of ApolloMed’s outstanding shares of Series A preferred stock and Series B preferred stock. The Series A preferred stock and the Series B preferred stock each have a liquidation preference in the amount of $9.00 per share plus any declared and unpaid dividends. The Series A preferred stock and Series B preferred stock can be voted for the number of shares of common stock into which such preferred could then be converted, which initially is one-for-one. Subject to preferences that may be applicable to any outstanding shares of Series A preferred stock and Series B preferred stock, holders of ApolloMed common stock are entitled to receive dividends, if any, as may be declared from time to time by ApolloMed’s board of directors out of ApolloMed’s assets which are legally available. Such dividends, if any, are payable in cash, in property or in shares of capital stock.
Pursuant to the ApolloMed Bylaws, the presence of holders of a majority of all the shares of ApolloMed stock entitled to vote at the meeting is necessary to constitute a quorum, unless or except to the extent that the presence of a larger number may be required by law. Stockholders present in person or by proxy will be counted for purposes of determining whether a quorum is present. If a quorum is present, an action by stockholders entitled to vote on a matter is approved if the number of votes cast in favor of the action exceeds the number of votes cast in opposition to the action, with the exception of the election of directors, which requires a plurality of the votes cast, represented in person or by proxy, are necessary to constitute a quorum for the transaction of business at any meeting.
| 318 |
Warrants to be Issued as Merger Consideration
As part of the merger consideration, NMM shareholders will be issued warrants to purchase a pro-rata portion of an aggregate of 850,000 shares of common stock of ApolloMed exercisable at $11.00 per share and warrants to purchase a pro-rata portion of an aggregate of 900,000 shares of common stock of ApolloMed, exercisable at $10.00 per share (collectively, the “Warrants”). The following summary of certain terms and provisions of the Warrants offered hereby is not complete and is subject to, and qualified in its entirety by the provisions of the form of Warrant set forth in Annex C. You should carefully review the terms and provisions set forth in the form of Warrant.
Exercisability
The Warrants are exercisable immediately upon issuance and at any time up to the date that is five years from the date of issuance. The Warrants will be exercisable, at the option of each holder, in whole or in part by delivering to ApolloMed a duly executed exercise notice accompanied by payment in full for the number of shares of ApolloMed common stock purchased upon such.
Exercise Price
The initial exercise price per share of ApolloMed common stock purchasable upon exercise (i) of the 850,000 Warrants is equal to $11.00 and (ii) of the 900,000 Warrants is equal to $10.00 is subject to adjustments for distributions, stock splits or subdivisions.
Transferability
Subject to applicable laws, the Warrants may be transferred at the option of the holders upon surrender of the Warrants to ApolloMed, together with the appropriate instruments of transfer.
Listing
The Warrants will be issued in physical form. ApolloMed does not plan on applying to list the Warrants on any national securities exchange or any other nationally recognized trading system.
Rights as a Shareholder
Except as otherwise provided in the Warrant or by virtue of such holder’s ownership of shares of common stock, the holder of Warrants does not have rights or privileges of a holder of shares of common stock of ApolloMed, including any voting rights, until the holder exercises the Warrants.
The provisions of Delaware law, the ApolloMed Charter and the ApolloMed Bylaws could discourage or make it more difficult to accomplish a proxy contest or other change in ApolloMed’s management or the acquisition of control by a holder of a substantial amount of ApolloMed’s voting stock. It is possible that these provisions could make it more difficult to accomplish, or could deter, transactions that stockholders may otherwise consider to be in their best interests or in ApolloMed’s best interests. These provisions are intended to enhance the likelihood of continuity and stability in the composition of ApolloMed’s board of directors and in the policies formulated by the board of directors and to discourage certain types of transactions that may involve an actual or threatened change of ApolloMed’s control. These provisions are designed to reduce ApolloMed’s vulnerability to an unsolicited acquisition proposal and to discourage certain tactics that may be used in proxy fights. Such provisions also may have the effect of preventing changes in ApolloMed’s management.
| 319 |
Authorized but Unissued Shares
The authorized but unissued shares of ApolloMed’s common stock and preferred stock are available for future issuance without any further vote or action by ApolloMed stockholders. These additional shares may be utilized for a variety of corporate purposes, including future public offerings to raise additional capital, corporate acquisitions and employee benefit plans. The existence of authorized but unissued shares of ApolloMed’s common stock and preferred stock could render more difficult or discourage an attempt to obtain control over ApolloMed by means of a proxy contest, tender offer, merger or otherwise.
Delaware Statutory Business Combinations Provision
ApolloMed is subject to the anti-takeover provisions of Section 203 of the DGCL. Section 203 prohibits certain publicly-held Delaware corporation from engaging in a “business combination” with an “interested stockholder” for a period of three years after the date of the transaction in which the person became an interested stockholder, unless the business combination is, or the transaction in which the person became an interested stockholder was, approved in a prescribed manner or another prescribed exception applies. For purposes of Section 203, a “business combination” is defined broadly to include a merger, asset sale or other transaction resulting in a financial benefit to the interested stockholder, and, subject to certain exceptions, an “interested stockholder” is a person who, together with his or her affiliates and associates, owns, or within three years prior did own 15% or more of the corporation’s voting stock.
Classification of the Board
In connection with the Merger, ApolloMed proposes to amend the ApolloMed Charter and ApolloMed Bylaws to classify ApolloMed’s board of directors into three classes of directors. As a result, approximately one-third of ApolloMed’s board of directors will be elected each year. The classification of directors will have the effect of making it more difficult for stockholders to change the composition of ApolloMed’s board. See “apollomed proposal 2 – approval of the board classification PROPOSAL” on page 108 of this joint proxy statement/prospectus.
Special Meetings of Stockholders
ApolloMed’s Bylaws provide that special meetings of the stockholders may be called only by the board of directors, the president, the chief executive officer or the holders of not less than 10% of all shares entitled to vote at the special meeting.
Stockholder Action by Written Consent
Each of the ApolloMed Charter and the ApolloMed Bylaws permit ApolloMed’s stockholders to act by written consent.
The transfer agent and registrar for ApolloMed’s common stock is [●].
ApolloMed’s common stock is currently quoted on OTC Pink and traded under the symbol “AMEH.” ApolloMed has applied for listing of its common stock on the NASDAQ Global Market effective as of the closing of the Merger.
| 320 |
APOLLOMED STOCKHOLDERS AND NMM SHAREHOLDERS
ApolloMed is incorporated under the laws of the State of Delaware and NMM is formed under the laws of the State of California. If the Merger is completed, NMM shareholders will become stockholders of ApolloMed, and their rights will be governed by the DGCL, as well as the ApolloMed Charter and the ApolloMed Bylaws, each as further amended to reflect the proposals being voted on at the ApolloMed special meeting. The rights of ApolloMed stockholders contained in the ApolloMed Charter, the ApolloMed Bylaws and the DGCL differ from the rights of NMM shareholders under the NMM Articles, the NMM Bylaws and the California Corporations Code.
The following discussion summarizes the material differences as of the date of this joint proxy statement/prospectus between the rights of ApolloMed stockholders and the rights of NMM shareholders. The following discussion is only a summary and does not purport to be a complete description of all differences nor is it intended to provide a comprehensive discussion of each company’s governing documents or law. This summary is qualified in its entirety by reference to the full text of each of the ApolloMed Charter, the ApolloMed Bylaws, the DGCL and the California Corporations Code. See “WHERE YOU CAN FIND MORE INFORMATION” beginning on page 314 for information on how to obtain a copy of these documents. A marked copy of the proposed amendments to the ApolloMed Charter and ApolloMed Bylaws are included in this joint proxy statement/prospectus as Annexes E and F, respectively.
| 321 |
Certain Differences Between the Rights of Stockholders of ApolloMed and Shareholders of NMM
| NMM | ApolloMed | |||
| Authorized Capital Stock | NMM is authorized to issue a total of 900,000,000 shares of capital stock, consisting of all common stock with no par value. |
ApolloMed is authorized to issue a total of 105,000,000 shares of capital stock, consisting of the following: · 100,000,000 shares of common stock, par value $0.001 per share; and · 5,000,000 shares of preferred stock, par value $0.001 per share. |
||
| Number of Directors | Under the NMM Bylaws, the number of directors of NMM is set at a minimum of 18 and a maximum of 26, initially fixed at 19. There are currently 23 NMM directors on the board of NMM. | The DGCL permits the charter or bylaws of a corporation to govern the number and term of directors. Per the ApolloMed Bylaws, the number of directors is fixed by the board provided the authorized number of directors cannot be less than one. The ApolloMed Charter further limits the number of directors between three and nine as determined by the board. At the closing of the Merger, the board will be divided into three classes with three directors in each class. | ||
| Classification of Board of Directors | The board of directors of NMM is a declassified board with between 18 and 26 directors, each elected annually at the annual shareholder meeting. | The board of directors of ApolloMed is currently a declassified board. Following the closing of the Merger, the board of directors will be classified into three classes, with one class eligible for re-election at each annual meeting of the stockholders. | ||
| Election of Directors | Directors are elected annually at the annual shareholders meeting. | Directors are elected annually at the annual stockholders meeting by a plurality of the votes cast by the holders of shares entitled to vote, assuming a quorum is present. | ||
| Removal of Directors | According to the NMM Bylaws, the entire board or any director may be removed without cause by a majority of the outstanding shares entitled to vote at an election of directors, subject to certain exceptions. Directors may also be removed for unsound mind or conviction of a felony. | The DGCL provides that any director or the entire board may be removed, with or without case, by the holders of a majority of the shares then entitled to vote at an election of directors. The ApolloMed Charter provides that directors may be removed for cause at any annual or special meeting of stockholders by the same vote as required to elect such director, provided such director receives a copy of the charges against such director delivered at least 30 days prior to the meeting at which such removal is to be considered and such director has an opportunity to be heard. |
| 322 |
| NMM | ApolloMed | |||
| Vacancies on the Board of Directors | Vacancies of directors may be filled at the same meeting of shareholders in which such director was removed. Vacancies may be filled by a majority of the remaining directors, or if the number of directors is less than a quorum, (i) by unanimous written consent, (ii) affirmative vote of majority of directors at a meeting or (iii) a sole remaining director, subject to certain exceptions. | Vacancies may be filled by a majority vote of the remaining directors, though less than a quorum, by a sole remaining director, or by the stockholders. A vacancy is deemed to exist in the case of death, resignation or removal of any director, if the authorized number of directors is increased or if the stockholders fail to elect the full authorized number of directors. The stockholders may elect a director at any time to fill any vacancy not filled by the directors. If a director resigns, the board or the stockholders have the power to elect a successor to take office when the resignation is effective. | ||
| Stockholder Action by Written Consent | Shareholder action by written consent is permitted with execution by the holders of outstanding shares having not less than the minimum number of votes that would be necessary to authorize or take such action at a meeting at which all shares entitled to vote thereon were present and voted. | Under the ApolloMed Bylaws, any action which may be taken at a stockholders meeting may be taken by written consent without a meeting if such action is taken in conformance with the DGCL. | ||
| Amendments to Charter | Under the California Corporation Code, the NMM Articles may be amended if approved by the NMM board and a majority of outstanding shares entitled to vote. |
Under the DGCL, a proposed amendment to the certificate of incorporation requires a resolution adopted by the board and, unless otherwise provided in the charter, the affirmative vote of the holders of a majority of the outstanding stock entitled to vote thereon and a majority of the outstanding stock of each class entitled to vote thereon as a class.
The DGCL also provides that if any such amendment would adversely alter or change the rights of any holders of shares of a class of stock, the vote of the holders of a majority of all outstanding shares of the class, voting as a separate class, is nevertheless required to authorize such amendment. |
||
| Amendment of By-Laws | Amendment to the Bylaws may be adopted by the vote or written consent of holders of a majority of the outstanding shares entitled to vote or by the board of directors, other than an amendment changing the authorized number of directors (except to fix the authorized number of directors pursuant to a Bylaw providing for a variable number of directors). | Under the DGCL, the power to adopt, alter and repeal the bylaws is vested in the stockholders, unless the corporation’s charter vests such power in the board of directors. The fact that such power has been conferred upon the directors shall not divest the stockholders of the power, nor limit their power to adopt, amend or repeal bylaws. The ApolloMed Charter vests the power to amend the ApolloMed Bylaws in the board of directors. The ApolloMed Bylaws vests the power to amend the ApolloMed Bylaws in the board of directors and in the stockholders, with the ability to amend at any such director or stockholder meeting. |
| 323 |
| NMM | ApolloMed | |||
| Voting Rights | Each outstanding share, regardless of class, is entitled to one vote on any matter submitted to a vote of the shareholders, except that shareholders are entitled to cumulative votes at a shareholders’ meeting at which directors are to be elected, subject to notice requirements. The NMM shareholders are also subject to a Shareholders Agreement, which includes transfer restrictions, rights of first refusal, disqualification and mandatory repurchase by NMM, non-compete provisions, non-solicitation provision and shareholder consent to terminate such Shareholders’ Agreement. | Each stockholder has one vote for every share of stock entitled to vote which is registered in such stockholder’s name on the record date for the meeting. Shares of ApolloMed common stock have no cumulative voting rights. Shares of ApolloMed Series A and Series B preferred stock have the right to one vote for each share of common stock into which such preferred stock could then be converted. | ||
| Special Meeting of Stockholders | Special meetings of the shareholders may be called at any time by the board of directors, the chairman of the board, the president or the holders of shares entitled to cast not less than 10% of the votes at the meeting. | The DGCL provides that the board of directors or such person or persons authorized by the corporation’s charter or bylaws may call a special meeting of stockholders. ApolloMed’s Bylaws provide that special meetings may be called by the board of directors, the president, the chief executive officer or the holders of not less than 10% of all shares entitled to vote at the meeting. | ||
| Delivery of Notice Requirements of Stockholder Nominations and Proposals | All notices of meetings must be sent not less than 10 nor more than 60 days before the date of the meeting. Such notice must state the place, date and hour of the meeting and in the case of a special meeting, the general nature of the business to be transacted and no business other than that specified business may be transacted. |
Written notice of the place, date and time of all meetings of the stockholder must be given no less than 10 or more than 50 days before the date on which the meeting is to be held to each stockholder entitled to vote at such meeting, except as otherwise required by law.
|
||
| Dividends | The NMM Articles and NMM Bylaws do not discuss dividend payouts but NMM is otherwise subject to the dividend limitations set forth in the California Corporations Code. The California Corporations Code provides that a corporation may make a distribution to its shareholders if retained earning immediately prior to the dividend payout is at least equal to the amount of the proposed distribution. In the event that sufficient retained earnings are not available for the proposed distribution, a corporation may, nevertheless, make a distribution if it meets both the “quantitative solvency” and the “liquidity” tests. In general, the quantitative solvency test requires that the sum of the assets of the corporation equals at least 1.25 times its liabilities. The liquidity test generally requires that a corporation have current assets at least equal to current liabilities or, if the average of the earnings of the corporation before taxes on income and before interest expenses for the two preceding fiscal years was less than the average of the interest expense of the corporation for such fiscal years, then current assets must equal at least 1.25 times current liabilities. |
Under the DGCL, unless further restricted in the certificate of incorporation, a corporation may declare and pay dividends, out of surplus, or if no surplus exists, out of net profits for the fiscal year in which the dividend is declared and/or the preceding fiscal year (provided that the amount of capital of the corporation is not less than the aggregate amount of the capital represented by the issued and outstanding stock of all classes having a preference upon the distribution of assets).
The ApolloMed Bylaws allow the board to declare dividends in accordance with law. Under the ApolloMed Charter, the holders of the shares of Series A and Series B preferred stock and common stock are entitled to receive dividends, out of any assets legally available, on parity with the holders of the other classes, and must share ratably on an as-converted-to-common-stock basis with the holders of other classes in any declaration or payment of any dividend, payable when, as, and if declared by the board. The Series A and Series B preferred stock has no dividend preference over common stock. |
| 324 |
| NMM | ApolloMed | |||
|
Indemnification of Officers and Directors; Insurance; Advancement of Expenses |
The liability of directors of NMM for monetary damages is eliminated to the fullest extent permissible under California law. Additionally, NMM indemnifies its directors to the maximum extent and in the manner permitted by the California Corporations Code and has the power to indemnify its officers, agents and employees to the maximum extent and in the manner permitted by the California Corporations Code arising by reason of the fact that such person is or was a director, officer, agent or employee of NMM, and includes advance fee payment for directors, or if otherwise authorized by the NMM board. | ApolloMed indemnifies any officer, director, committee member or representative who is a party to any threatened, pending or completed action, suit or proceeding against such person in an official capacity or in any other capacity while serving as a director, officer or agent of ApolloMed and includes advance fee payment; provided ApolloMed is not obligated to pay advance fees for any action against an officer brought directly by ApolloMed for fraud or other willful misconduct in connection with such officer’s duties. ApolloMed has the power to purchase and maintain D&O insurance. |
Certain holders of NMM’s securities are parties to a shareholders’ agreement and a voting agreement that will not apply to the combined company if the Merger is completed.
The validity of the securities offered hereby in connection with the Merger will be passed upon by McDermott Will & Emery LLP.
The consolidated financial statements of Apollo Medical Holdings, Inc. (“ApolloMed”) as of March 31, 2017 and 2016 and for the years then ended included in this joint proxy statement/prospectus and in the Registration Statement have been so included in reliance on the report of BDO USA, LLP, an independent registered public accounting firm (the report on the consolidated financial statements contains an explanatory paragraph regarding ApolloMed’s ability to continue as a going concern) appearing elsewhere herein and in the Registration Statement, given on the authority of said firm as experts in auditing and accounting.
| 325 |
The consolidated financial statements of Network Medical Management, Inc. as of December 31, 2016 and 2015 and for the years then ended included in this joint proxy statement/prospectus and in the Registration Statement have been so included in reliance on the report of BDO USA, LLP, an independent registered public accounting firm appearing elsewhere herein and in the Registration Statement, given on the authority of said firm as experts in auditing and accounting.
The consolidated financial statements of Network Medical Management, Inc. as of December 31, 2014 and for the year then ended included in this joint proxy statement/prospectus and in the Registration Statement have been so included in reliance on the report of DNW & Associates, Inc., an independent auditor appearing elsewhere herein and in the Registration Statement, given on the authority of said firm as experts in auditing and accounting.
WHERE YOU CAN FIND MORE INFORMATION
ApolloMed is subject to the informational requirements of the Exchange Act and in accordance therewith, files annual, quarterly and current reports, proxy statements and other information with the SEC. You may read and copy these reports, statements or other information filed by ApolloMed at the SEC’s Public Reference Room at 100 F Street, N.E., Washington, D.C. 20549, at prescribed rates. Call the SEC at 1-800-SEC-0330 for further information on the operation of the Public Reference Room. In addition, ApolloMed files reports, proxy statements and other information with the SEC electronically, and the SEC maintains a website that contains ApolloMed’s filings as well as reports, proxy statements and information statements, and other information issuers file electronically with the SEC at www.sec.gov.
ApolloMed also makes available free of charge on or through its website at www.ApolloMed.com, its Annual Reports on Form 10-K, Quarterly Reports on Form 10-Q, Current Reports on Form 8-K and amendments to those reports filed or furnished pursuant to Section 13(a) or 15(d) of the Exchange Act. The website addresses for the SEC and ApolloMed are inactive textual references only and not active hyperlinks. The information contained on, or that can be accessed through, those websites is not part of this joint proxy statement/prospectus.
You should rely only on the information contained in this joint proxy statement/prospectus. Neither ApolloMed nor NMM has authorized anyone to provide you with different information. Therefore, if anyone gives you different or additional information, you should not rely on it. The information contained in this joint proxy statement/prospectus is correct as of its date. It might not continue to be correct after this date. ApolloMed has supplied all of the information about ApolloMed and its subsidiaries contained in this joint proxy statement/prospectus and NMM has supplied all of the information contained in this joint proxy statement/prospectus about NMM. ApolloMed is relying on the correctness of the information supplied by NMM and NMM is relying on the correctness of the information supplied by ApolloMed.
| 326 |
NETWORK MEDICAL MANAGEMENT, INC.
INDEX TO FINANCIAL STATEMENTS
Network Medical Management, Inc.
Consolidated Financial Statements
Years Ended December 31, 2016 and 2015
F-1
Network Medical Management, Inc.
Contents
F-2
Report of Independent Registered Public Accounting Firm
Board of Directors
Network Medical Management, Inc.
Alhambra, California
We have audited the accompanying consolidated balance sheets of Network Medical Management, Inc. (“Company”) as of December 31, 2016 and 2015 and the related consolidated statements of income, mezzanine equity, stockholders’ equity (deficit), and cash flows for the years then ended. These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States) and in accordance with auditing standards generally accepted in the United States of America. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. Our audits included consideration of internal control over financial reporting as a basis for designing audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion. An audit also includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of Network Medical Management, Inc. at December 31, 2016 and 2015, and the results of their operations and their cash flows for the years then ended, in conformity with accounting principles generally accepted in the United States of America.
/s/ BDO USA, LLP
Los Angeles, California
July 14, 2017
F-3
Consolidated Financial Statements
F-4
Network Medical Management, Inc.
Consolidated Balance Sheets
| December 31, | 2016 | 2015 | ||||||
| Assets | ||||||||
| Current assets | ||||||||
| Cash and cash equivalents | $ | 54,824,580 | $ | 59,014,715 | ||||
| Restricted cash | 101,132 | 100,376 | ||||||
| Fiduciary cash | 1,050,739 | 2,364,134 | ||||||
| Investment in marketable securities | 1,051,807 | 1,041,360 | ||||||
| Accounts receivable | 3,136,388 | 3,035,021 | ||||||
| Capitation and claims receivable | 445,181 | 1,263,526 | ||||||
| Risk pool and incentive receivable | 19,633,117 | 27,619,301 | ||||||
| Subscription receivable | - | 1,825,000 | ||||||
| Sign-on bonus, current portion | 424,000 | 424,000 | ||||||
| Prepaid expenses and other current assets | 489,354 | 317,043 | ||||||
| Total current assets | 81,156,298 | 97,004,476 | ||||||
| Noncurrent assets | ||||||||
| Land, property and equipment, net | 10,373,333 | 8,326,824 | ||||||
| Intangible assets, net | 108,094,049 | 121,103,612 | ||||||
| Goodwill | 103,407,351 | 100,851,144 | ||||||
| Loans receivable - related parties | 5,200,000 | 5,000,000 | ||||||
| Sign-on bonus, net of current portion | 783,625 | 1,207,625 | ||||||
| Investments in other entities – equity method | 24,256,065 | 19,075,219 | ||||||
| Investments in other entities – cost method | 10,575,002 | 7,077,778 | ||||||
| Derivative asset - warrants | 5,338,886 | 2,088,889 | ||||||
| Other assets | 814,353 | 751,000 | ||||||
| Total noncurrent assets | 268,842,664 | 265,482,091 | ||||||
| Total assets | $ | 349,998,962 | $ | 362,486,567 | ||||
F-5
Network Medical Management, Inc.
Consolidated Balance Sheets (Continued)
| December 31, | 2016 | 2015 | ||||||
| Liabilities, Mezzanine Equity and Shareholders’ Equity (Deficit) | ||||||||
| Current liabilities | ||||||||
| Accounts payable and accrued expenses | $ | 8,083,277 | $ | 10,656,156 | ||||
| Capitation incentives payable | 19,621,645 | 14,438,980 | ||||||
| Fiduciary accounts payable | 1,050,739 | 2,364,134 | ||||||
| Medical liabilities | 18,957,465 | 16,011,519 | ||||||
| Income taxes payable | 2,810,357 | 20,351,296 | ||||||
| Bank loan, current portion | - | 45,183 | ||||||
| Loan payable to related party | - | 600,000 | ||||||
| Capital lease obligations | 102,348 | 97,264 | ||||||
| Total current liabilities | 50,625,831 | 64,564,532 | ||||||
| Noncurrent liabilities | ||||||||
| Deferred tax liability | 46,932,207 | 48,964,169 | ||||||
| Liability for unissued equity shares | 1,997,650 | 1,997,650 | ||||||
| Bank loan, net of current portion | - | 1,432,378 | ||||||
| Total noncurrent liabilities | 48,929,857 | 52,394,197 | ||||||
| Total liabilities | 99,555,688 | 116,958,729 | ||||||
| Commitments, Contingencies and Subsequent Events (Notes 13 and 17) | ||||||||
| Mezzanine equity | ||||||||
| Noncontrolling interest in Allied Pacific of California IPA | 162,855,554 | 161,028,806 | ||||||
| Redeemable common stock, stated value; shares authorized 900,000,000; 396,858,568 and 379,282,368 shares issued respectively; and 366,343,818 and 350,367,618 shares outstanding, respectively | 86,894,870 | 75,830,520 | ||||||
| Additional paid-in capital | 1,084,544 | 488,353 | ||||||
| Total Network Medical Management, Inc. redeemable common stock | 87,979,414 | 76,318,873 | ||||||
| Shareholders’ equity (deficit) | ||||||||
| Network Medical Management, Inc. shareholders’ equity (deficit): | ||||||||
| Retained earnings (accumulated deficit) | (773,311 | ) | 7,773,162 | |||||
| Total Network Medical Management, Inc. shareholders’ equity (deficit) | (773,311 | ) | 7,773,162 | |||||
| Noncontrolling interest in Concourse Diagnostic Surgery Center | 381,617 | 406,997 | ||||||
| Total shareholders’ equity (deficit) | (391,694 | ) | 8,180,159 | |||||
| Total liabilities, mezzanine equity and shareholders’ equity (deficit) | $ | 349,998,962 | $ | 362,486,567 | ||||
See accompanying notes to consolidated financial statements.
F-6
Network Medical Management, Inc.
Consolidated Statements of Income
| Year ended December 31, | 2016 | 2015 | ||||||
| Revenue | ||||||||
| Capitation, net | $ | 247,639,181 | $ | 247,244,135 | ||||
| Risk pool settlements and incentives | 22,641,884 | 37,656,242 | ||||||
| Management fee income | 24,774,941 | 20,834,222 | ||||||
| Surgery center income, net | 6,132,729 | 5,366,490 | ||||||
| Fee-for-service, net | 3,031,241 | 1,070,864 | ||||||
| Other income | 1,714,939 | 952,752 | ||||||
| Total revenue | 305,934,915 | 313,124,705 | ||||||
| Expenses | ||||||||
| Contracted physicians and other services | 254,468,120 | 233,581,805 | ||||||
| General and administrative expenses | 20,759,436 | 22,277,282 | ||||||
| Management fees | 580,000 | 4,507,180 | ||||||
| Depreciation and amortization | 18,114,440 | 9,085,312 | ||||||
| Impairment of goodwill and other | 324,306 | - | ||||||
| Total expenses | 294,246,302 | 269,451,579 | ||||||
| Income from operations | 11,688,613 | 43,673,126 | ||||||
| Other income (expense) | ||||||||
| Income from equity method investments | 4,748,542 | 1,206,654 | ||||||
| Interest expense | (61,589 | ) | (209,929 | ) | ||||
| Interest income | 504,696 | 208,917 | ||||||
| Change in fair value of derivative instrument | 1,722,221 | (833,333 | ) | |||||
| Other income | 233,726 | 1,931,635 | ||||||
| Total other income, net | 7,147,596 | 2,303,944 | ||||||
| Income before provision for income taxes | 18,836,209 | 45,977,070 | ||||||
| Provision for income taxes | 8,816,412 | 19,297,447 | ||||||
| Net income | 10,019,797 | 26,679,623 | ||||||
| Less: Net (loss) income attributable to noncontrolling interests | (1,433,730 | ) | 13,862,522 | |||||
| Net income attributable to Network Medical Management, Inc. | $ | 11,453,527 | $ | 12,817,101 | ||||
| Earnings per share – basic | $ | 0.03 | $ | 0.05 | ||||
| Earnings per share – diluted | $ | 0.03 | $ | 0.05 | ||||
| Weighted average shares of common stock outstanding – basic | 360,634,339 | 256,619,159 | ||||||
| Weighted average shares of common stock outstanding –diluted | 367,945,833 | 263,734,916 | ||||||
See accompanying notes to consolidated financial statements.
F-7
Network Medical Management, Inc.
Consolidated Statements of Mezzanine Equity
| Mezzanine Equity – Noncontrolling |
Mezzanine Equity - NMM Redeemable Common Stock | |||||||||||||||||||||||||||
| Interest in APC | Common Stock | Treasury Stock | Additional | Total NMM | ||||||||||||||||||||||||
| Noncontrolling Interest |
Shares | Amount | Shares | Amount | Paid-in Capital |
Redeemable Common Stock |
||||||||||||||||||||||
| Balance, January 1, 2015 | $ | 105,067,503 | 175,703,886 | $ | 1,882,559 | 22,982,400 | $ | - | $ | 89,099 | $ | 1,971,658 | ||||||||||||||||
| - | ||||||||||||||||||||||||||||
| Net income | 13,187,054 | - | - | - | - | - | - | |||||||||||||||||||||
| Shares issued in connection with acquisitions | 37,238,000 | 157,876,218 | 57,887,947 | - | - | - | 57,887,947 | |||||||||||||||||||||
| Shares issued for cash | 10,503,114 | 16,787,514 | 15,987,514 | - | - | - | 15,987,514 | |||||||||||||||||||||
| Share-based compensation | 1,531,883 | - | 72,500 | - | - | 399,254 | 471,754 | |||||||||||||||||||||
| Noncontrolling interest capital change | 1,200 | - | - | - | - | - | - | |||||||||||||||||||||
| Dividends | (6,499,948 | ) | - | - | - | - | - | - | ||||||||||||||||||||
| Balance, December 31, 2015 | 161,028,806 | 350,367,618 | 75,830,520 | 22,982,400 | - | 488,353 | 76,318,873 | |||||||||||||||||||||
| Net income (loss) | (2,427,779 | ) | - | - | - | - | - | - | ||||||||||||||||||||
| Shares repurchased | (410,000 | ) | (107,500 | ) | (107,500 | ) | - | - | - | (107,500 | ) | |||||||||||||||||
| Shares issued in connection with acquisitions | - | 9,900,000 | 5,155,000 | 1,600,000 | - | - | 5,155,000 | |||||||||||||||||||||
| Shares issued for cash and exercise of options | 3,321,850 | 6,183,700 | 6,016,850 | - | - | - | 6,016,850 | |||||||||||||||||||||
| Share-based compensation | 1,358,047 | - | - | - | - | 596,191 | 596,191 | |||||||||||||||||||||
| Noncontrolling interest capital change | 1,234,630 | - | - | - | - | - | - | |||||||||||||||||||||
| Dividends | (1,250,000 | ) | - | - | - | - | - | - | ||||||||||||||||||||
| Balance, December 31, 2016 | $ | 162,855,554 | 366,343,818 | $ | 86,894,870 | 24,582,400 | $ | - | $ | 1,084,544 | $ | 87,979,414 | ||||||||||||||||
F-8
Network Medical Management, Inc.
Consolidated Statements of Shareholders’ Equity (Deficit)
| Total NMM | ||||||||||||||||
| Retained earnings/ Accumulated |
Total NMM Shareholders’ |
Noncontrolling Interest in |
Total Shareholders’ |
|||||||||||||
| Deficit | Equity | CDSC | Equity (Deficit) | |||||||||||||
| Balance, January 1, 2015 | $ | (4,108,304 | ) | $ | (4,108,304 | ) | $ | 594,100 | $ | (3,514,204 | ) | |||||
| - | - | |||||||||||||||
| Net income | 12,817,101 | 12,817,101 | 675,468 | 13,492,569 | ||||||||||||
| Dividends | (935,635 | ) | (935,635 | ) | (862,571 | ) | (1,798,206 | ) | ||||||||
| Balance, December 31, 2015 | 7,773,162 | 7,773,162 | 406,997 | 8,180,159 | ||||||||||||
| Net income (loss) | 11,453,527 | 11,453,527 | 994,049 | 12,447,576 | ||||||||||||
| Noncontrolling interest capital change | - | - | (110,000 | ) | (110,000 | ) | ||||||||||
| Dividends | (20,000,000 | ) | (20,000,000 | ) | (909,429 | ) | (20,909,429 | ) | ||||||||
| Balance, December 31, 2016 | $ | (773,311 | ) | $ | (773,311 | ) | $ | 381,617 | $ | (391,694 | ) | |||||
See accompanying notes to consolidated financial statements.
F-9
Network Medical Management, Inc.
Consolidated Statements of Cash Flows
| Years ended December 31, | 2016 | 2015 | ||||||
| Cash flows from operating activities | ||||||||
| Net income | $ | 10,019,797 | $ | 26,679,623 | ||||
| Adjustments to reconcile net income to net cash provided by operating activities: | ||||||||
| Depreciation and amortization | 18,114,440 | 9,085,312 | ||||||
| Impairment of goodwill and other | 324,306 | - | ||||||
| Share-based compensation | 1,954,238 | 2,003,637 | ||||||
| Change in fair value of derivative instrument | (1,722,221 | ) | 833,333 | |||||
| Income from equity method investments | (4,748,542 | ) | (1,206,654 | ) | ||||
| Deferred tax | (3,009,779 | ) | (4,768,523 | ) | ||||
| Changes in operating assets and liabilities, net of acquisition amounts: | ||||||||
| Accounts receivable | (101,367 | ) | (1,608,439 | ) | ||||
| Capitation and claims receivable | 818,345 | 440,453 | ||||||
| Risk pool and incentive receivable | 7,986,184 | (16,505,347 | ) | |||||
| Prepaid expenses and other current assets | (172,311 | ) | 782,218 | |||||
| Sign-on bonus | - | (125,000 | ) | |||||
| Refundable income taxes | - | 129,592 | ||||||
| Other assets | (63,353 | ) | (662,128 | ) | ||||
| Accounts payable and accrued expenses | 1,927,121 | (11,727,762 | ) | |||||
| Capitation incentives payable | 5,182,665 | 6,531,846 | ||||||
| Medical liabilities | 2,945,946 | 4,118,774 | ||||||
| Income taxes payable | (17,540,939 | ) | 18,378,069 | |||||
| Net cash provided by operating activities | 21,914,530 | 32,379,004 | ||||||
| Cash flows from investing activities | ||||||||
| Purchases of marketable securities | (10,447 | ) | (6,740 | ) | ||||
| Change in restricted cash | (756 | ) | 199,624 | |||||
| Advances to related parties – loans receivable | (200,000 | ) | (5,000,000 | ) | ||||
| Dividends received from equity method investments | 2,000,000 | 500,000 | ||||||
| Purchases of investments – cost method | (5,000,000 | ) | (10,000,000 | ) | ||||
| Purchases of investments – equity method | (2,440,000 | ) | (10,571,697 | ) | ||||
| Purchases of property and equipment | (3,306,294 | ) | (1,524,881 | ) | ||||
| Net cash used in investing activities | (8,957,497 | ) | (26,403,694 | ) | ||||
F-10
Network Medical Management, Inc.
Consolidated Statements of Cash Flows (Continued)
| Years ended December 31, | 2016 | 2015 | ||||||
| Cash flows from financing activities | ||||||||
| Repayment of loan payable – related party | (600,000 | ) | - | |||||
| Dividends paid | (26,659,119 | ) | (3,798,154 | ) | ||||
| Change in noncontrolling interest capital | 1,124,320 | 1,200 | ||||||
| Borrowings on bank loan | - | 10,000,000 | ||||||
| Principal payments on bank loan | (1,477,561 | ) | (10,050,917 | ) | ||||
| Payment of capital lease obligations | (181,008 | ) | (79,372 | ) | ||||
| Proceeds from exercise of stock options included in liabilities | - | 1,997,650 | ||||||
| Proceeds from exercise of stock options | 260,000 | - | ||||||
| Proceeds from common stock offering | 10,903,700 | 24,665,628 | ||||||
| Repurchase of common shares | (517,500 | ) | - | |||||
| Net cash (used in) provided by financing activities | (17,147,168 | ) | 22,736,035 | |||||
| Net (decrease) increase in cash and cash equivalents | (4,190,135 | ) | 28,711,345 | |||||
| Cash and cash equivalents, beginning of year | 59,014,715 | 30,303,370 | ||||||
| Cash and cash equivalents, end of year | $ | 54,824,580 | $ | 59,014,715 | ||||
| Supplemental disclosures of cash flow information | ||||||||
| Cash paid for income taxes | $ | 29,366,184 | $ | 5,352,866 | ||||
| Cash paid for interest | 61,589 | 209,929 | ||||||
| Supplemental disclosures of non-cash investing and financing activities | ||||||||
| Stock issued in connection with acquisitions | $ | 5,155,000 | $ | 95,125,947 | ||||
| Deferred tax liability adjusted to goodwill | 977,817 | 22,588,761 | ||||||
| Equipment purchased with capital lease | 186,092 | 176,636 | ||||||
| Subscriptions receivable related to shares issued | - | 1,825,000 | ||||||
| Dividends declared included in accounts payable and accrued expenses | - | 4,500,000 | ||||||
| Reclassification of stock options exercised to liability for unissued common shares | - | 1,997,650 | ||||||
| Reclassification of fiduciary cash to payable | 1,313,395 | 1,562,876 | ||||||
| Loan payable – related party related to investment in PMIOC | - | 636,000 | ||||||
See accompanying notes to consolidated financial statements.
F-11
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
| 1. | Description of Business |
Network Medical Management, Inc. (““NMM”) was incorporated in the State of California in March 1994 for the purpose of providing management services to medical companies and independent practice associations (“IPAs”). The management services cover primarily billing, collection, accounting, administrative, and marketing.
Allied Physicians of California IPA, a Professional Medical Corporation d.b.a. Allied Pacific of California IPA, a Professional Medical Corporation DBA Allied Pacific of California (“APC”) was incorporated on August 17, 1992 for the purpose of arranging health care services as an IPA. APC has contracts with various health maintenance organizations (“HMOs”) or licensed health care service plans as defined in the Knox-Keene Health Care Service Plan Act of 1975. Each HMO negotiates a fixed amount per member per month (“PMPM”) that is to be paid to APC. In return, APC arranges for the delivery of health care services by contracting with physicians or professional medical corporations for primary care and specialty care services. APC assumes the financial risk of the cost of delivering health care services in excess of the fixed amounts received. Some of the risk is transferred to the contracted physicians or professional corporations. The risk is also minimized by stop-loss provisions in contracts with HMOs.
On July 1, 1999, APC entered into an amended and restated management and administrative services agreement with NMM (initial management services agreement was entered into in 1997) for an initial fixed term of 30 years. In accordance with relevant accounting guidance, APC is determined to be a Variable Interest Entity (“VIE”) and NMM is the primary beneficiary with the ability to direct the activities (excluding clinical decisions) that most significantly affect APC’s economic performance through its majority representation of the APC Joint Planning Board; therefore APC is consolidated by NMM. As of December 31, 2016 and 2015, APC owns 6.29% and 6.16%, respectively, of NMM.
Concourse Diagnostic Surgery Center, LLC (“CDSC”) was formed on March 25, 2010 in the state of California. CDSC is an ambulatory surgery center in City of Industry, California, is organized by a group of highly qualified physicians, and the surgical center utilizes some of the most advanced equipment in Eastern Los Angeles County and San Gabriel Valley. The facility is Medicare Certified and accredited by the Accreditation Association for Ambulatory Healthcare, Inc. During 2011, APC invested $625,000 for a 41.59% ownership in CDSC. Due to capital stock changes in 2016, APC’s ownership percentage in CDSC’s capital stock changed to 43.8% and 43.43% on May 31, 2016 and July 31, 2016, respectively. CDSC is consolidated as a VIE by APC as it was determined that APC has a controlling financial interest in CDSC and is the primary beneficiary of CDSC.
APC-LSMA was formed on October 15, 2012 as a designated shareholder professional corporation and is solely owned by Dr. Thomas Lam, a shareholder and Chief Executive and Financial Officer of APC. APC-LSMA is controlled and consolidated by APC who is the primary beneficiary of this VIE. The only activity of APC-LSMA is to hold the investments in medical corporations, which includes: LaSalle Medical Associates, Pacific Medical Imaging and Oncology Center, Inc. (“PMIOC”) and Diagnostic Medical Group (“DMG”).
Universal Care Acquisition Partners, LLC (“UCAP”), a 100% owned subsidiary of APC, was formed on June 4, 2014, for the purpose of holding the investment in Universal Care, Inc. (“UCI”).
F-12
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
On November 11, 2015, NMM, ACO Acquisition Corporation, and APCN-ACO, A Medical Professional Corp. (“APCN-ACO”) entered into a reorganization agreement whereby ACO Acquisition Corporation, a newly organized entity in which NMM is its sole shareholder, merged with APCN-ACO, effective on January 8, 2016, resulting in APCN-ACO becoming a wholly owned subsidiary of NMM (see Note 3).
On December 18, 2016, NMM, ACO Acquisition Corporation #2, and Allied Physicians ACO, LLC (“AP-ACO”) entered into a reorganization agreement whereby ACO Acquisition Corporation #2, a newly organized entity in which NMM is its sole shareholder, merged into AP-ACO, effective on December 20, 2016, resulting in AP-ACO becoming a wholly owned subsidiary of NMM (see Note 3).
Unless stated otherwise, NMM, ACO Acquisition Corp., APCN ACO, ACO Acquisition Corporation #2, AP ACO, APC, CDSC, APC-LSMA and UCAP are collectively referred to herein as the “the Company.”
| 2. | Basis of Presentation and Summary of Significant Accounting Policies |
Principles of Consolidation
The Company’s consolidated financial statements have been prepared by management in accordance with accounting principles generally accepted in the United States of America (“GAAP”) and include the accounts of NMM and its consolidated VIE, APC and its subsidiary UCAP and APC’s consolidated VIEs, CDSC and APC-LSMA. As of the effective dates of the reorganizations, as described above, the accounts of APCN-ACO and AP-ACO were also included in the consolidation of NMM.
All material intercompany balances and transactions have been eliminated in consolidation.
Business Combinations
The Company uses the acquisition method of accounting for all business combinations, which requires assets and liabilities of the acquiree to be recorded at fair value, to measure the fair value of the consideration transferred, including contingent consideration, to be determined on the acquisition date, and to account for acquisition related costs separately from the business combination.
Use of Estimates
The preparation of consolidated financial statements and related disclosures in conformity with GAAP requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the consolidated financial statements and the reported amounts of revenues and expenses during the reporting period. Significant items subject to such estimates and assumptions include collectability of receivables, recoverability of long-lived and intangible assets, business combination and goodwill valuation and impairment, derivative assets, accrual of medical liabilities (including incurred, but not reported claims), determination of shared-risk revenues and receivables, income taxes and valuation of share-based compensation. Management evaluates its estimates and assumptions on an ongoing basis using historical experience and other factors, including the current economic environment, and makes adjustments when facts and circumstances dictate. As future events and their effects cannot be determined with precision, actual results could differ materially from those estimates and assumptions.
F-13
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
Cash and Cash Equivalents
Cash and cash equivalents primarily consist of money market funds and certificates of deposit. The Company considers all highly liquid investments that are both readily convertible into known amounts of cash and mature within ninety days from their date of purchase to be cash equivalents.
The Company maintains its cash in deposit accounts with several banks, which at times may exceed Federal Deposit Insurance Corporation (“FDIC”) insured limits. The Company has not experienced any losses in such accounts. The Company believes they are not exposed to any significant credit risk on its cash and cash equivalents. As of December 31, 2016, the Company’s deposit accounts with banks exceeded the FDIC’s insured limit by approximately $74.2 million. The Company has not experienced any losses to date and performs ongoing evaluations of these financial institutions to limit the Company’s concentration of risk exposure.
Restricted Cash
APC is required to maintain a reserve fund by a certain health plan. The required reserve at December 31, 2016 and 2015 was $101,132 and $100,376, respectively, and is held in a certificate of deposit account with initial maturities of six months at the date of purchase.
Fiduciary Cash
As of December 31, 2016 and 2015, APC recorded fiduciary cash of $1,050,739 and $2,364,134, respectively, which represents cash received from the health plans on behalf of subcontractor IPAs. APC remits the amounts to the subcontractor IPAs the following month and such remittances are included in fiduciary accounts payable in the accompanying consolidated balance sheets.
Investments in Marketable Securities
The appropriate classification of investments is determined at the time of purchase and such designation is reevaluated at each balance sheet date. Investments in marketable securities have been classified and accounted for as held-to-maturity based on management’s investment intentions relating to these securities. Held-to-maturity marketable securities are stated at amortized cost, which approximates fair value. As of December 31, 2016 and 2015, short-term marketable securities in the amount of $1,051,807 and $1,041,360, respectively, consist of certificates of deposit with various financial institutions, reported at par value plus accrued interest, with maturity dates from four months to twelve months (see Note 14). Investments in certificates of deposits are classified as Level 1 investments in the fair value hierarchy.
The remainder of this page intentionally left blank.
F-14
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
Receivables
The Company’s receivables are comprised of accounts receivable, capitation and claims receivable, risk pool and incentive receivables. Accounts receivable primarily consists of NMM management fee receivables and CDSC fee-for-service (“FFS”) receivables. Risk pool and incentive receivables mainly consist of APC full risk pool receivable that is only recorded when expected cash receipts are known or when actual cash is received from Health Source MSO’s who serves as the management company for the hospitals in the risk pools. Capitation and claims receivable relate to the health plan’s capitation, which is received by APC in the following month of service. For APC, other receivables are accrued based on invoices sent to the subcontracted IPA for stop loss insurance premium reimbursement and FFS reimbursement for Alhambra Hospital Medical Center’s self–insured program. For NMM, other receivables are accrued based on invoices for certain expense reimbursements from UCI and invoice for transportation reimbursement from the hospital.
Amounts are recorded as a receivable when the Company is able to determine amounts receivable under these contracts and/or agreements based on information provided and collection is reasonably likely to occur. The Company continuously monitors its collections of receivables and its policy is to write off receivables when they are determined to be uncollectible. The Company has not incurred credit losses related to receivables. No allowance for doubtful accounts is recorded at December 31, 2016 or 2015.
Concentrations of Risks
Four HMO’s accounted for 69% and 71% of the total capitation revenue for the years ended December 31, 2016 and 2015, respectively. The loss of these HMO contracts would have an adverse impact on the operations of APC.
Three and four HMO’s accounted for 96% and 99% of the total risk pool settlement revenue for the years ended December 31, 2016 and 2015, respectively. The loss of these HMO contracts would have an adverse impact on the operations of APC.
Three HMO’s accounted for 83% and 85% of the total fee for services revenue for the years ended December 31, 2016 and 2015, respectively.
No provider accounted for 10% or more of the total surgery center income for the years ended December 31, 2016 and 2015, respectively.
One provider accounted for approximately 70% and 74% of total management fee income for the years ended December 31, 2016 and 2015, respectively. The loss of provider would have an adverse impact on the operations of NMM.
As of December 31, 2016 and 2015, two and one providers accounted for approximately 29% and 49%, respectively, of total accounts receivable balance.
As of December 31, 2016 and 2015, two providers accounted for 97% and 100%, respectively, of the total risk pool and incentive receivable balance.
As of December 31, 2016 and 2015, one and two providers accounted for 100% and 95%, respectively, of the total capitation and claims receivable balance.
F-15
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
Land, Property and Equipment, Net
Land is carried at cost and is not depreciated as it is considered to have an infinite useful life.
Property and equipment, including leasehold improvements, are carried at cost less accumulated depreciation and amortization. Depreciation is provided principally on the straight-line method over the estimated useful lives of the assets ranging from three to ten years. Leasehold improvements are amortized on a straight-line basis over the shorter of the terms of the respective leases or the expected useful lives of those improvements.
Maintenance and repairs are charged to expense as incurred. Upon sale or retirement, the asset cost and related accumulated depreciation and amortization is removed from the accounts, and any related gain or loss is included in the determination of consolidated net income.
Sign-On Bonus
Pursuant to the Exclusivity Amendment Agreement entered into between APC and certain primary care physicians in October 2014 (see Note 12), APC is required to pay the provider a $25,000 sign-on bonus in three increments, the first by October 31, 2014, the second at the end of the sixth month of agreement term, and the third at the end of the 12th month of agreement term. APC capitalized an aggregate of $2,120,000 related to the sign-on bonus to be amortized over the contractual term of 5 years. If the agreement is terminated by the provider prior to the completion of the contract term, with or without cause, the sign-on bonus shall be fully repaid to APC by the terminating medical provider. During the years ended December 31, 2016 and 2015, APC recorded amortization expense related to the sign-on bonus of $424,000 and $405,250, respectively, which is included in the depreciation and amortization expense of the consolidated statements of income for the years ended December 31, 2016 and 2015. As of December 31, 2016 and 2015, the net sign-on bonus balance was $1,207,625 and $1,631,625, respectively. The remaining balance of the sign-on bonus as of December 31, 2016 is expected to be amortized as follows:
| Years ending December 31, | Amount | |||
| 2017 | $ | 424,000 | ||
| 2018 | 424,000 | |||
| 2019 | 340,875 | |||
| 2020 | 18,750 | |||
| Total future minimum amortization | $ | 1,207,625 | ||
Fair Value Measurements
The Company’s financial instruments consist of cash and cash equivalents, fiduciary cash, restricted cash, investment in marketable securities, accounts receivable, loans receivable – related parties, derivative asset (warrants), accounts payable, certain accrued expenses, bank loan, loan payable – related party and the line of credit. The carrying values of the financial instruments classified as current in the accompanying consolidated balance sheets are considered to be at their fair values, due to the short maturity of these instruments. The carrying amount of the long-term bank loan and line of credit approximates fair value as they bear interest at rates that approximate current market rates for debt with similar maturities and credit quality.
F-16
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
Financial Accounting Standards Board (“FASB”) Accounting Standards Codification (“ASC”) 820, Fair Value Measurement (“ASC 820”), applies to all financial assets and financial liabilities that are measured and reported on a fair value basis and requires disclosure that establishes a framework for measuring fair value and expands disclosure about fair value measurements. ASC 820 establishes a fair value hierarchy for disclosures of the inputs to valuations used to measure fair value.
This hierarchy prioritizes the inputs into three broad levels as follows:
Level 1—Inputs are unadjusted quoted prices in active markets for identical assets or liabilities that can be accessed at the measurement date.
Level 2—Inputs include quoted prices for similar assets and liabilities in active markets, quoted prices for identical or similar assets or liabilities in markets that are not active, inputs other than quoted prices that are observable for the asset or liability (i.e., interest rates and yield curves), and inputs that are derived principally from or corroborated by observable market data by correlation or other means (market corroborated inputs).
Level 3—Unobservable inputs that reflect assumptions about what market participants would use in pricing the asset or liability. These inputs would be based on the best information available, including the Company’s own data.
The carrying amounts and fair values of the Company’s financial instruments as of December 31, 2016 are presented below:
| Fair Value Measurements | ||||||||||||||||
| Level 1 | Level 2 | Level 3 | Total | |||||||||||||
| Assets | ||||||||||||||||
| Money market accounts | $ | 42,553,887 | $ | - | $ | - | $ | 42,553,887 | ||||||||
| Marketable securities – certificates of deposit | 1,051,807 | - | - | 1,051,807 | ||||||||||||
| Derivative asset (warrants) | - | - | 5,338,886 | 5,338,886 | ||||||||||||
| Total | $ | 43,605,694 | $ | - | $ | 5,338,886 | $ | 48,944,580 | ||||||||
The level 3 assets represent warrants in the common stock of Apollo Medical Holdings, Inc. (“AMEH”) and are included in derivative asset – warrants in the consolidated balance sheets.
The remainder of this page intentionally left blank.
F-17
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
The following is a reconciliation of the opening and closing balances for financial instruments measured at fair value on a recurring basis using significant unobservable inputs (Level 3) for the year ended December 31, 2016:
| Derivative Asset (Warrants) |
||||
| Balance, December 31, 2015 | $ | 2,088,889 | ||
| Fair value of warrants acquired in AMEH | 1,527,776 | |||
| Change in fair value of warrants | 1,722,221 | |||
| Balance, December 31, 2016 | $ | 5,338,886 | ||
The carrying amounts and fair values of the Company’s financial instruments as of December 31, 2015 are presented below:
| Fair Value Measurements | ||||||||||||||||
| Level 1 | Level 2 | Level 3 | Total | |||||||||||||
| Assets | ||||||||||||||||
| Money market accounts | $ | 22,207,123 | $ | - | $ | - | $ | 22,207,123 | ||||||||
| Marketable securities – certificates of deposit | 1,041,360 | - | - | 1,041,360 | ||||||||||||
| Derivative asset (warrants) | - | - | 2,088,889 | 2,088,889 | ||||||||||||
| Total | $ | 23,248,483 | $ | - | $ | 2,088,889 | $ | 25,337,372 | ||||||||
The following is a reconciliation of the opening and closing balances for financial instruments measured at fair value on a recurring basis using significant unobservable inputs (Level 3) for the year ended December 31, 2015:
| Derivative Asset (Warrants) |
||||
| Balance, January 1, 2015 | $ | - | ||
| Fair value of warrants acquired in AMEH | 2,922,222 | |||
| Change in fair value of warrants | (833,333 | ) | ||
| Balance, December 31, 2015 | $ | 2,088,889 | ||
F-18
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
The fair value of the warrant derivative asset of approximately $5.3 million at December 31, 2016 was estimated using the Monte Carlo valuation model, using the following inputs: term of 3.79 – 4.24 years, risk free rate of 1.67% - 1.76%, no dividends, volatility of 63.0% - 62.5%, share price of $7.50 per share based on the trading price of the AMEH common stock adjusted for a marketability discount, and a 0% probability of redemption of the warrant shares issued along with the shares of AMEH’s convertible preferred stock issued in the financing (see Note 7). The fair value of the warrant derivative asset purchased on March 30, 2016 of approximately $1.5 million was estimated at issuance date using the Monte Carlo valuation model, using the following inputs: term of 5 years, risk free rate of 1.2%, no dividends, volatility of 69.9%, share price of $5.93 per share based on the trading price of AMEH’s common stock adjusted for a marketability discount, and a 0% probability of redemption of the warrant shares issued along with the shares of AMEH’s convertible preferred stock issued in the financing.
The fair value of the warrant derivative asset of approximately $2.1 million at December 31, 2015 was estimated using the Monte Carlo valuation model, using the following inputs: term of 4.8 years, risk free rate of 1.71%, no dividends, volatility of 65.7%, share price of $4.75 per share based on the trading price of AMEH’s common stock adjusted for a marketability discount, and a 0% probability of redemption of the warrant shares issued along with the shares of AMEH’s convertible preferred stock issued in the financing (see Note 7). The fair value of the warrant derivative asset purchased on October 14, 2015 of approximately $2.9 million was estimated at issuance using the Monte Carlo valuation model, using the following inputs: term of 5 years, risk free rate of 1.3%, no dividends, volatility of 63.3%, share price of $6.00 per share based on the trading price of AMEH’s common stock adjusted for a marketability discount, and a 0% probability of redemption of the warrant shares issued along with the shares of AMEH’s convertible preferred stock issued in the financing.
There have been no changes in Level 1, Level 2, or Level 3 classification and no changes in valuation techniques for these assets for the years ended December 31, 2016 and 2015.
Intangibles and Long-Lived Assets
Intangible assets with finite lives include network/payor relationships, management contracts and member relationships and are stated at cost, less accumulated amortization and impairment losses. These intangible assets are amortized on accelerated method using the discounted cash flow rate.
Finite-lived intangibles and long-lived assets are reviewed for impairment whenever events or changes in circumstances indicate that the carrying amount of an asset may not be recoverable. If the expected future cash flows from the use of such assets (undiscounted and without interest charges) are less than the carrying value, a write-down would be recorded to reduce the carrying value of the asset to its estimated fair value. Fair value is determined based on appropriate valuation techniques. The Company determined that there was no impairment of its finite-lived intangible or long-lived assets during the years ended December 31, 2016 and 2015.
Goodwill
Goodwill represents the difference between the purchase consideration of an acquired business and the fair value of the identifiable tangible and intangible net assets acquired. Goodwill is tested for impairment on an annual basis and whenever events or circumstances indicate that the carrying amount of such asset may not be recoverable. The Company’s impairment review process compares the fair value of the reporting unit in which the goodwill resides to its carrying value.
F-19
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
Testing for impairment of goodwill is a two-step process. The first step requires the Company to compare the estimated fair value of its reporting unit with its respective carrying value. The Company has determined it has three reporting units, a management services unit, an accountable care organization unit and a health care services unit.
If the fair value is less than the carrying value, goodwill is potentially impaired and the Company then completes the second step to measure the impairment loss, if any. The second step requires the calculation of the implied fair value of goodwill by deducting the fair value of all tangible and intangible net assets from the fair value of the reporting unit. If the implied fair value of goodwill is less than the carrying amount of enterprise goodwill, an impairment loss is recognized equal to the difference.
During the year ended December 31, 2016, the Company recorded an impairment charge of $316,610 related to the acquisition of Apple Physicians Organization in 2008, as the amount was not determined to be recoverable. No impairment loss was recorded by the Company during the year ended December 31, 2015.
Reportable Segments
The Company operates as one reportable segment, the healthcare delivery segment, and implements and operates innovative health care models to create a patient-centered, physician-centric experience. The Company reports its consolidated financial statements in the aggregate, including all activities in one reportable segment.
Investments in Other Entities
Equity Method
The Company accounts for certain investments using the equity method of accounting when it is determined that the investment provides the Company the ability to exercise significant influence, but not control, over the investee. Significant influence is generally deemed to exist if the Company has an ownership interest in the voting stock of the investee of between 20% and 50%, although other factors, such as representation on the investee’s board of directors, are considered in determining whether the equity method of accounting is appropriate. Under the equity method of accounting, the investment, originally recorded at cost, is adjusted to recognize the Company’s share of net earnings or losses of the investee and is recognized in the consolidated statements of income under “Income from equity method investments” and also is adjusted by contributions to and distributions from the investee. Equity method investments are subject to impairment evaluation. No impairment loss was recorded on equity method investments for the years ended December 31, 2016 and 2015.
Cost Method
The Company uses the cost method to account for investments in companies for which it does not exercise significant influence or control.
The Company reviews its investments in other entities accounted under cost method to determine whether events or changes in circumstances indicate that the investment carrying amount may not be recoverable. The primary factors the Company considers in its determination are the financial condition, operating performance and near term prospects of the investee.
F-20
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
If the decline in value is deemed to be other than temporary, the Company would recognize an impairment loss. No impairment loss was recorded on investments accounted under the cost method for the years ended December 31, 2016 and 2015.
Medical Liabilities
APC is responsible for integrated care that the associated physicians and contracted hospitals provide to its enrollees. APC provides integrated care to health plan enrollees through a network of contracted providers under sub-capitation and direct patient service arrangements. Medical costs for professional and institutional services rendered by contracted providers are recorded as contracted physicians and other services expenses in the accompanying consolidated statements of income.
Costs incurred by CDSC for operating its ambulatory surgical center, are included in general and administrative expenses in the consolidated statements of income.
An estimate of amounts due to contracted physicians, hospitals, and other professional providers is included in medical liabilities in the accompanying consolidated balance sheets. Medical liabilities include claims reported as of the balance sheet date and estimates of incurred, but not reported claims (“IBNR”). Such estimates are developed using actuarial methods and are based on numerous variables, including the utilization of health care services, historical payment patterns, cost trends, product mix, seasonality, changes in membership, and other factors. The estimation methods and the resulting reserves are periodically reviewed and updated. Many of the medical contracts are complex in nature and may be subject to differing interpretations regarding amounts due for the provision of various services. Such differing interpretations may not come to light until a substantial period of time has passed following the contract implementation. APC has a $60,000 retention per member professional stop loss and $55,000 per member stop loss for Medi-Cal patients for professional claims. Any adjustments to reserves are reflected in current operations.
Revenue Recognition
Revenue primarily consists of capitation revenue, risk pool settlements and incentives, management fee income, surgery center income and fee-for-services. Revenue is recorded in the period in which services are rendered. The form of billing and related risk of collection for such services may vary by customer. The following is a summary of the principal forms of the Company’s billing arrangements and how revenue is recognized for each.
Capitation, Net
Capitation revenue (net of capitation withheld to fund risk share deficits) is recognized in the month in which the services are provided. Minor ongoing adjustments to prior months’ capitation, primarily arising from HMOs finalizing of monthly eligibility data for additions or subtractions of enrollees, are recognized in the month they are communicated to APC. Managed care revenues of APC consist primarily of capitated fees for medical services provided by APC under a provider service agreement (“PSA”) or capitated arrangements directly made with various managed care providers including HMO’s and management service organizations (“MSOs”). Capitation revenue under the PSA and HMO contracts is prepaid monthly to APC based on the number of enrollees electing APC as their healthcare provider. Health plans and providers with higher acuity enrollees will receive more and those with lower acuity enrollees will receive less.
F-21
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
Risk Pool Settlements and Incentives
Contracts with HMO’s also include provisions for APC to participate in the risk (shared risk capitation arrangements) relating to the provision of institutional services (institutional risk) to enrollees, such that APC can earn additional incentive revenue or incur losses based upon the enrollee utilization of hospital services. Typically, any shared risk deficits are not payable until and unless APC generates future risk sharing surpluses, or if the HMO withholds a portion of the capitation revenue to fund any risk share deficits. At the termination of the HMO contract, any accumulated risk share deficit is typically extinguished. Due to the lack of access to information necessary to estimate the related healthcare costs (“IBNR”), revenue from shared risk amounts are recorded when such amounts are known. In addition to risk sharing revenues, APC is also eligible to participate in an incentive program. As an incentive to control enrollee utilization and to promote quality care, the HMOs have designed the quality incentive programs and commercial generic pharmacy incentive programs to compensate APC for efforts it takes to improve the quality of services and for efficient and effective use of pharmacy supplemental benefits provided to the HMO’s members. The incentive programs track specific performance measures and calculate payments to the IPA based on the performance measures.
APC also enter into risk sharing arrangements with affiliated hospitals (full risk capitation arrangements) who in turn have entered into capitation arrangements with various HMOs, pursuant to which the affiliated hospital provides, arranges and pays for institutional risk. Under a risk pool sharing agreement, APC is allocated a percentage of the affiliated hospitals surplus or deficit from the risk pool, after deductions for the affiliated hospitals costs. Advance settlement payments are typically made quarterly in arrears if there is a surplus. However, due to the uncertainty around the settlement of the related IBNR reserve, APC recognizes any excess IBNR reserve on settlement as risk pool settlement revenue on a modified cash basis. Any excess IBNR is normally settled and paid after a period of approximately one year from the related service period.
Management Fee Income
NMM provides claims processing and other administrative services for other IPAs. NMM receives management fee income for the services rendered. Management fees are calculated as a percentage of revenue under capitation contracts with various insurance companies.
Surgery Center Income
CDSC’s surgery center income consists primarily of net patient service revenues that are recorded based upon established billing rates less allowance for contractual adjustments. Revenues are recorded in the period in which the healthcare services are provided, based upon the estimated amounts due from patients and third-party payors, including commercial health plans, employers, workers’ compensation plans and federal and state agencies (under the Medicare and Medicaid programs).
CDSC utilizes the payment history specific to each payor and services to record estimated net revenues to ensure the appropriateness of these estimates. Third-party payor contractual payment terms are generally based upon predetermined rates per procedure or fee-for-service rates.
F-22
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
Fee-for-Service
Fee-for-service revenue primarily represents professional component of charges for medical services rendered by the Company’s contracted physicians and paid to the Company for certain reimbursable services, which is recognized at the time reimbursements are received from the health plans.
Stop-Loss Provisions
Stop-loss insurance limits the cost of medical services for enrollees whose professional care costs exceed a specified level. Stop-loss insurance premiums are reported as medical expenses and insurance recoveries are reported as a reduction of related medical expenses. The Company is contingently liable to the extent that any insurer becomes unable to meet its contractual obligation. As of December 31, 2016 and 2015, the liability balance for stop-loss provision was $0.
The Company has purchased stop-loss insurance, which will reimburse the Company for claims from service providers on a per enrollee basis. The specific retention amount per enrollee per policy period is $55,000 to $60,000 for professional coverage.
Income Taxes
Deferred income taxes are provided for temporary differences between financial and tax reporting in accordance with the liability method.
The Company utilizes ASC 740, which requires the recognition of deferred tax assets and liabilities for the expected future tax consequences of events that have been included in the consolidated financial statements or tax returns. Under this method, deferred income taxes are recognized for the tax consequences in future years of differences between the tax basis of asset and liabilities and their financial reporting amounts at each period end based on enacted tax laws and statutory tax rates applicable to the periods in which the differences are expected to affect taxable income. Valuation allowances are established, when necessary, to reduce deferred tax assets to the amount expected to be realized.
The Company uses a recognition threshold of more-likely-than-not and a measurement attribute on all tax positions taken or expected to be taken in a tax return in order to be recognized in the financial statements. Once the recognition threshold is met, the tax position is then measured to determine the actual amount of benefit to recognize in the consolidated financial statements. The Company recognizes interest and penalties on taxes, if any, within operations as income tax expense. No interest or penalties on taxes were recognized in 2016 and 2015. The Company is subject to U.S federal income tax examination from 2013 onward and state income tax examination from 2012 onward.
Share-Based Compensation
The Company accounts for share-based compensation arrangements in accordance with ASC 718, Compensation—Stock Compensation, which requires the measurement and recognition of compensation expense for all share-based payment awards to employees and nonemployees based on estimated fair values. ASC 718 further requires a reduction in share-based compensation expense by an estimated forfeiture rate.
F-23
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
The Company uses the Black-Scholes option pricing model to estimate the fair value of stock option awards at the grant date. The model requires the input of highly subjective assumptions, including the Company’s estimated share price, expected stock price volatility, which is based on taking the average historical price volatility for industry peers based on daily price observations over a period equivalent to the expected term of the awards, the expected dividend yield, the expected term of an option, and the risk-free interest rate, which is based on the US Treasury yield curve in effect at the time of grant. The Company uses historical employee exercise behavior, forfeitures, cancellations, and other factors to estimate the expected term.
Changes in subjective input assumptions can materially affect the fair value estimates of an option. Furthermore, the estimated fair value of an option does not necessarily represent the value that will ultimately be realized.
The Company accounts for equity instruments issued to nonemployees and consultants in exchange for goods and services under ASC 505-50, Equity-Based Payments to Non-Employees. As such, the value of the applicable share-based compensation is periodically remeasured using an appropriate valuation model and income or expense is recognized during the vesting terms of the equity instruments. The measurement date for the estimated fair value of the equity instruments issued is the earlier of (i) the date at which a commitment for performance by the nonemployee or consultant is reached or (ii) the date at which the nonemployee or consultant’s performance is complete. In the case of equity instruments issued to consultants, the estimated fair value of the equity instrument is primarily recognized over the term of the consulting agreement.
Basic and Diluted Earnings Per Share
Basic earnings (loss) per share is computed by dividing net income (loss) attributable to NMM’s shareholders by the weighted average number of common shares outstanding during the periods presented. Diluted earnings per share is computed using the weighted average number of common shares outstanding plus the effect of dilutive securities outstanding during the periods presented, using treasury method. See Note 16 for more details.
Noncontrolling Interests
The Company consolidates entities in which the Company has a controlling financial interest. The Company consolidates subsidiaries in which the Company hold, directly or indirectly, more than 50% of the voting rights, and variable interest entities (VIEs) in which the Company is the primary beneficiary. Noncontrolling interests represent third-party equity ownership interests in the Company’s consolidated entities. The amount of net income attributable to noncontrolling interests is disclosed in the consolidated statements of income.
Mezzanine Equity
Based on the shareholder agreements for both NMM and APC, in the event of a disqualifying event, as defined in the agreements, NMM and APC could be required to repurchase the shares from their respective shareholders based on certain triggers outlined in the shareholder agreements. The triggers that could cause NMM to redeem the shares are not solely within the control of NMM. As the redemption feature of the shares is not solely within the control of NMM, the common stock and additional paid-in capital of NMM has been classified in mezzanine or temporary equity as redeemable common stock.
F-24
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
In addition, as the redemption feature of the shares is not solely within the control of APC, the equity of APC does not qualify as permanent equity and has been classified as mezzanine or temporary equity. Accordingly, the Company recognizes noncontrolling interests in APC as mezzanine equity in the consolidated financial statements.
Recent Accounting Pronouncements
In May 2014, the FASB issued a new revenue recognition standard, Accounting Standards Update (“ASU”) No. 2014-09, Revenue From Contracts with Customers (Topic 606) (“ASC 2014-09”), that will supersede nearly all existing revenue recognition guidance under GAAP. The revenue recognition standard will allow for the recognition of revenue when a company transfers promised goods or services to customers in an amount that reflects the consideration to which the Company expects to be entitled in exchange for those goods or services. The standard permits the use of either a full retrospective or retrospective with cumulative effect transition method. On August 8, 2015, the FASB issued ASU No. 2015-14, which defers the effective date of ASU No. 2014-09 by one year. The standard is effective for nonpublic entities for annual periods beginning after December 15, 2018, and interim reporting periods within annual reporting periods beginning after December 15, 2019, with the earliest option of adoption being the fiscal year beginning after December 15, 2016. In addition, the FASB issued the following accounting standard updates related to Topic 606, Revenue from Contracts with Customers:
| · | ASU No. 2016-08, Revenue From Contracts with Customers (Topic 606): Principal versus Agent Considerations (Reporting Revenue Gross versus Net) (“ASU 2016-08”) in March 2016. ASU 2016-08 does not change the core principle of revenue recognition in Topic 606, but clarifies the implementation guidance on principal versus agent considerations. |
| · | ASU No. 2016-10, Revenue from Contracts with Customers (Topic 606): Identifying Performance Obligations and Licensing (“ASU 2016-10”) in April 2016. ASU 2016-10 does not change the core principle of revenue recognition in Topic 606, but clarifies the implementation guidance on identifying performance obligations and the licensing implementation guidance, while retaining the related principles for those areas. |
| · | ASU No. 2016-12, Revenue from Contracts with Customers (Topic 606): Narrow-Scope Improvements and Practical Expedients (“ASU 2016-12”) in May 2016. ASU 2016-12 does not change the core principle of revenue recognition in Topic 606, but clarifies the implementation guidance on a few narrow areas and adds some practical expedients to the guidance. |
| · | ASU No. 2016-20, Technical Corrections and Improvements to Topic 606, Revenue from Contracts with Customers (“ASU 2016-20”) in December 2016. ASU 2016-20 does not change the core principle of revenue recognition in Topic 606, but affects narrow aspects of the guidance issued in ASU 2014-09. |
The Company is currently evaluating the impact of ASC 606 on its consolidated financial statements. However, at the current time the Company does not know what impact the new standard will have on revenue recognized and other accounting decisions in future periods, if any, nor what method of adoption will be selected if the impact is material.
In February 2015, the FASB issued ASU No. 2015-02, Consolidation (Topic 810): Amendments to the Consolidation Analysis (“ASU 2015-02”). This update changes the guidance with respect to the analyses that a reporting entity must perform to determine whether it should consolidate certain types of legal entities.
F-25
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
All legal entities are subject to reevaluation under the revised consolidation model. The new guidance affects the following areas: (1) limited partnerships and similar legal entities, (2) evaluating fees paid to a decision maker or a service provider as a variable interest, (3) the effect of fee arrangements on the primary beneficiary determination, (4) the effect of related parties on the primary beneficiary determination, and (5) certain investment funds. ASU 2015-02 is effective for fiscal years beginning after December 15, 2016, and interim periods within fiscal years beginning after December 15, 2017. Early adoption is permitted, including adoption in an interim period. The Company early adopted ASU 2015-02 effective for the year ended December 31, 2015. The adoption did not have a significant impact on the Company’s consolidated financial statements.
In November 2015, the FASB issued ASU No. 2015-17, Income Taxes (Topic 740): Balance Sheet Classification of Deferred Taxes (“ASU 2015-17”). This amendment simplifies the presentation of deferred tax assets and liabilities on the balance sheet and requires all deferred tax assets and liabilities, along with any related valuation allowance, to be treated as non-current. ASU 2015-17 is effective for financial statements issued for annual periods beginning after December 15, 2017 and interim periods within annual periods beginning after December 15, 2018, with early adoption permitted as of the beginning of an interim or annual reporting period. The Company early adopted ASU 2015-17 with retrospective effect to all periods presented and the adoption did not have any impact on fiscal year 2015.
In January 2016, the FASB issued ASU No. 2016-01, Financial Instruments - Overall (Subtopic 825-10): Recognition and Measurement of Financial Assets and Financial Liabilities (“ASU 2016-01”). ASU 2016-01 addresses certain aspects of recognition, measurement, presentation and disclosures of financial instruments including the requirement to measure certain equity investments at fair value with changes in fair value recognized in net income. ASU 2016-01 will become effective for the Company for fiscal year beginning after December 15, 2018, and interim periods within fiscal years beginning after December 15, 2019. The Company is currently evaluating the guidance to determine the potential impact on its financial position, results of operations, cash flows and related disclosures.
In March 2016, the FASB issued ASU No. 2016-07, Investments – Equity Method and Joint Ventures (Topic 323): Simplifying the Transition to the Equity Method of Accounting (“ASU 2016-07”), which eliminates the requirement that when an investment qualifies for use of the equity method as a result of an increase in the level of ownership interest or degree of influence, an investor must adjust the investment, results of operations, and retained earnings retroactively on a step-by-step basis as if the equity method had been in effect during all previous periods that the investment had been held. The amendments in this ASU are effective for financial statements issued for fiscal years, and interim periods within those fiscal years, beginning after December 15, 2016. The amendments should be applied prospectively upon their effective date to increases in the level of ownership interest or degree of influence that result in the adoption of the equity method.
Early adoption of the amendments is permitted. Accordingly, the Company will adopt ASU 2016-07 in 2017 and such adoption is not expected to have an impact on the Company’s consolidated financial statements and footnote disclosures.
In February 2016, the FASB issued ASU No. 2016-02, Leases (Topic 842) (“ASU 2016-02”), which will require organizations to recognize lease assets and lease liabilities on the balance sheet, including leases that were previously classified as operating leases. The ASU will also require additional disclosures about leasing arrangements related to the amount, timing, and uncertainty of cash flows arising from leases.
F-26
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
The amendments in this ASU are effective for financial statements issued for fiscal years beginning after December 15, 2019, and interim periods within fiscal years beginning after December 15, 2020. Early adoption of the amendments is permitted and the new guidance shall be applied using a modified retrospective approach. The Company is currently evaluating the impact of the adoption of this standard on its consolidated financial statements and footnote disclosures.
In March 2016, the FASB issued ASU No. 2016-09, Compensation - Stock Compensation (Topic 718): Improvements to Employee Share-Based Payment Accounting (“ASU 2016-09”). This ASU makes several modifications to Topic 718 related to the accounting for forfeitures, employer tax withholding on share-based compensation, and the financial statement presentation of excess tax benefits or deficiencies. ASU 2016-09 also clarifies the statement of cash flows presentation for certain components of share-based awards. The standard is effective for annual reporting periods beginning after December 15, 2017 and interim periods within annual periods beginning after December 15, 2018, with early adoption permitted. The Company expects to adopt this guidance when effective and is currently evaluating the effect that the updated standard will have on its consolidated financial statements and related disclosures.
In August 2016, the FASB issued ASU No. 2016-15, Statement of Cash Flows (Topic 230) – Classification of Certain Cash Receipts and Cash Payments (“ASU 2016-15”). This ASU provides clarification regarding how certain cash receipts and cash payments are presented and classified in the statement of cash flows. This ASU addresses eight specific cash flow issues with the objective of reducing the existing diversity in practice. The issues addressed in this ASU that will affect the Company are classifying debt prepayments or debt extinguishment costs, distributions received from equity method investees, and contingent consideration payments made after a business combination. This update is effective for fiscal years beginning after December 15, 2018, and interim periods within fiscal years beginning after December 15, 2019. Early adoption is permitted, including adoption in an interim period. The Company is currently assessing the impact the adoption of ASU 2016-15 will have on the Company’s consolidated financial statements.
In October 2016, the FASB issued ASU No. 2016-17, Consolidation (Topic 810): Interests Held through Related Parties that are under Common Control (“ASU 2016-17”). ASU 2016-17 amends the consolidation guidance on how a reporting entity that is the single decision maker of a VIE should treat indirect interest in the entity held through related parties that are under common control with the reporting entity when determining whether it is the primary beneficiary of that VIE. Entities that already have adopted ASU 2015-02 are required to apply ASU 2016-17 retrospectively to all relevant prior periods beginning with the fiscal year in which ASU 2015-02 was initially applied. Accordingly, the Company retrospectively adopted ASU 2016-17 effective December 31, 2015 and such adoption did not have an impact on the Company’s consolidated financial statements.
In November 2016, the FASB issued ASU No. 2016-18, Statement of Cash Flows (Topic 230): Restricted Cash (“ASU 2016-18”). The amendments in ASU 2016-18 require that a statement of cash flows explain the change during the period in the total of cash, cash equivalents, and amounts generally described as restricted cash or restricted cash equivalents. ASU 2016-17 is effective for fiscal years beginning after December 15, 2018, and interim periods within fiscal years beginning after December 15, 2019. Early adoption is permitted, including adoption in an interim period. The Company is currently assessing the impact the adoption of ASU 2016-18 will have on the Company’s consolidated financial statements.
F-27
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
In January 2017, the FASB issued ASU No. 2017-01, Business Combinations (Topic 805): Clarifying the Definition of a Business (“ASU 2017-01”). This ASU provides a screen to determine when a set is not a business, which requires that when substantially all of the fair value of the gross assets acquired (or disposed of) is concentrated in a single identifiable asset or a group of similar identifiable assets, the set is not a business, which reduces the number of transactions that need to be further evaluated. If the screen is not met, this ASU require that to be considered a business, a set must include, at a minimum, an input and a substantive process that together significantly contribute to the ability to create output and also remove the evaluation of whether a market participant could replace missing elements. This update is effective for annual periods beginning after December 15, 2018, and interim periods within annual periods beginning after December 15, 2019. The Company is currently assessing the impact the adoption of ASU 2017-01 will have on the Company’s consolidated financial statements.
In January 2017, the FASB issued ASU No. 2017-04, Intangibles – Goodwill and Other (Topic 350): Simplifying the Test for Goodwill Impairment (“ASU 2017-04”). This ASU eliminates Step 2 from the goodwill impairment test if the carrying amount exceeds the fair value of a reporting unit and also eliminates the requirements for any reporting unit with a zero or negative carrying amount to perform a qualitative assessment and, if it fails that qualitative test, to perform Step 2 of the goodwill impairment test. Therefore, the same impairment assessment applies to all reporting units. An entity is required to disclose the amount of goodwill allocated to each reporting unit with a zero or negative carrying amount of net assets. This update is effective on a prospective basis for annual and interim goodwill impairment tests performed for periods beginning after December 15, 2021. Early adoption is permitted for interim and annual goodwill impairment tests performed on testing dates after January 1, 2017. The Company is currently assessing the impact the adoption of ASU 2017-04 will have on the Company’s consolidated financial statements.
| 3. | Mergers and Acquisitions |
PIPA MSO, Inc.
On July 1, 2015, NMM merged with PIPA MSO, Inc. (“PIPA MSO”), a California corporation with NMM being the surviving entity. PIPA MSO was organized for the purpose of providing management services to medical groups and IPAs. The management service covers billing, collection, accounting, administrative, non-physician personnel staffing, and marketing. NMM acquired the operational and management processes associated with providing management services to medical groups and IPA’s.
NMM issued 157,876,218 shares of its common stock to the PIPA MSO shareholders with a fair value of $57,887,947 ($0.37 per share, which is based on management’s evaluation of the share price), representing approximately 44% of the issued and outstanding shares of NMM in exchange for shares held by former shareholders of PIPA MSO.
The fair value of the NMM share price was determined based on the use of the income and market approaches to derive the business enterprise value and applying a rate of 50% to the discounted cash flow method and 25% each to the guideline public company method and guideline mergers & acquisitions method. A discount of 28.5% for lack of marketability was then applied to determine the per share value. There was no cash consideration in this transaction. Transaction costs are not included as a component of consideration transferred and were expensed as incurred, which were minimal and are included in general and administrative expenses in the accompanying consolidated statements of income.
F-28
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
The Company accounted for the acquisition as a business combination using the acquisition method of accounting which requires, among other things, that assets acquired and liabilities assumed be recognized at their fair values as of the acquisition date and be recorded on the balance sheet. Under the acquisition method of accounting, the total purchase consideration was allocated to the underlying tangible and intangible assets acquired and liabilities assumed based on their respective fair values, with the remainder allocated to goodwill. Goodwill is not deductible for tax purposes.
The final allocation of the total purchase price to the net assets acquired and liabilities assumed is as follows:
| Cash and cash equivalents | $ | 576,480 | ||
| Other current assets | 7,392 | |||
| Identifiable intangible asset – management contract | 22,832,000 | |||
| Goodwill | 44,321,086 | |||
| Total assets acquired | 67,736,958 | |||
| Accounts payable and accrued expenses | (545,884 | ) | ||
| Deferred tax liabilities | (9,303,127 | ) | ||
| Total liabilities assumed | (9,849,011 | ) | ||
| Net assets acquired | $ | 57,887,947 |
In the view of management, the goodwill recorded in the transaction reflects the Company’s future cash flow expectations and its market position in the healthcare industry. The intangible asset represents $22,832,000 recognized for the fair value of the management contracts that have an approximate useful life of 15 years. The valuation of the management contract acquired was based on management’s evaluation and estimates, available information, and reasonable and supportable assumptions, and are considered Level 3 measurements. The fair value of the management contract was estimated utilizing the income – discounted cash flow and market valuation approaches.
The following unaudited supplemental pro forma information for the year ended December 31, 2015, assumes the acquisition of PIPA MSO had occurred as of January 1, 2015. The pro forma data is for informational purposes only and may not necessarily reflect the actual results of operations had PIPA MSO been operated as part of NMM since January 1, 2015.
| As reported | Pro-forma (unaudited) |
|||||||
| Total revenues | $ | 313,124,795 | $ | 314,282,760 | ||||
| Consolidated net income | $ | 12,817,101 | $ | 12,915,885 | ||||
| Earnings per share – basic | $ | 0.05 | $ | 0.05 | ||||
| Earnings per share – diluted | $ | 0.05 | $ | 0.05 | ||||
| Weighted average shares of common stock outstanding – basic | 256,619,159 | 256,619,159 | ||||||
| Weighted average shares of common stock outstanding – diluted | 263,734,916 | 263,734,916 | ||||||
F-29
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
Physicians Healthways Medical Corporation
On April 1, 2015, APC merged with Physicians Healthways Medical Corporation (“PHW”), a California professional corporation, with APC being the surviving entity.
APC issued 60,714,750 shares of common stock with a fair value of $37,238,000 to the PHW shareholders. Per management’s evaluation, which utilized the income – discounted cash flow and market approaches, the estimated fair value of the APC common stock issued as consideration for the transaction was $37,238,000.
APC acquired intangible assets related to the network/payor relationships (approximately 58,000 health plan members of the PHW IPA and its physician members). Transaction costs are not included as a component of consideration transferred and were expensed as incurred, which were minimal and are included in general and administrative expenses in the accompanying consolidated statements of income.
The Company accounted for the acquisition as a business combination using the acquisition method of accounting which requires, among other things, that assets acquired and liabilities assumed be recognized at their fair values as of the acquisition date and be recorded on the balance sheet. Under the acquisition method of accounting, the total purchase consideration was allocated to the intangible assets acquired with the remainder allocated to goodwill. Goodwill is not deductible for tax purposes.
The final allocation of the total purchase consideration to the net assets acquired is summarized as follows:
| Identifiable intangible asset - network/payor relationships | $ | 32,606,000 | ||
| Goodwill | 17,917,634 | |||
| Total assets acquired | 50,523,634 | |||
| Deferred tax liability | (13,285,634 | ) | ||
| Total liabilities assumed | (13,285,634 | ) | ||
| Net assets acquired | $ | 37,238,000 |
In the view of management, the goodwill recorded in the transaction reflects the Company’s future cash flow expectations and its market position in the healthcare industry. The intangible asset represents $32,606,000 recognized for the fair value of the network/payor relationships that has an approximate useful life of 15 years. The valuation of the network/payor relationships acquired was based on management’s evaluation, management’s estimates, available information, and reasonable and supportable assumptions, and are considered Level 3 measurements. The fair value of the network/payor relationships was estimated utilizing the income – discounted cash flow and market valuation approaches.
F-30
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
The following unaudited supplemental pro forma information for the year ended December 31, 2015, assumes the acquisition of PHW had occurred as of January 1, 2015. The pro forma data is for informational purposes only and may not necessarily reflect the actual results of operations had PHW been operated as part of APC since January 1, 2015.
| As reported | Pro-forma (unaudited) |
|||||||
| Total revenues | $ | 313,124,705 | $ | 325,280,119 | ||||
| Consolidated net income | $ | 12,817,101 | $ | 12,794,310 | ||||
| Earnings per share – basic | $ | 0.05 | $ | 0.05 | ||||
| Earnings per share – diluted | $ | 0.05 | $ | 0.05 | ||||
| Weighted average shares of common stock outstanding – basic | 256,619,159 | 256,619,159 | ||||||
| Weighted average shares of common stock outstanding – diluted | 263,734,916 | 263,734,916 | ||||||
APCN-ACO and ACO Acquisition Corporation
On November 11, 2015, NMM, ACO Acquisition Corporation, and APCN-ACO, A Medical Professional Corp. (“APCN-ACO”) entered into a reorganization agreement whereby ACO Acquisition Corporation, a newly organized entity in which NMM is its sole shareholder, merged with APCN-ACO, effective on January 8, 2016, the date of filing the merger agreement with the California Secretary of State. APCN-ACO operates an accountable care organization (“ACO”), as defined under the Medicare Shares Savings Program (“MSSP”), which is comprised of the ACO’s network of independent medical practices. The primary reason for the business combination was for NMM to acquire the member relationships of APCN-ACO.
Immediately following the effective date, NMM became the sole shareholder of APCN-ACO. On the effective date, each share of APCN-ACO’s common stock issued and outstanding immediately prior to the effective date, was converted at 0.6 of one fully paid and nonassessable share(s) of common stock of NMM, immediately following which, each one share of common stock of ACO Acquisition Corporation was converted into and became one fully paid and nonassessable share of APCN-ACO’s common stock. As a result of the merger transaction, all of APCN-ACO’s shares were converted into 7,500,000 shares of NMM common stock.
All of APCN-ACO’s right, title and interest in and to all of its assets as of the effective date were included as part of the merger, including, without limitation, all of the following assets: (i) 75% of the issued and outstanding equity interests of 99 Medical Equipment Healthcare Supplies & Wheelchair Center (“99 DME”); (ii) 25% of the issued and outstanding equity interests of Allegiance Home Health, Inc.; and (iii) 5% economic interest in Pacific Medical Imaging & Oncology Center, Inc. (“PMIOC”). 99 DME is a medical equipment store that specializes in the retail sale of medical supplies and mobility equipment. On January 8, 2016, APCN-ACO purchased the remaining 25% interest in 99 DME for $12,500, resulting in APCN-ACO having 100% ownership of the issued and outstanding equity interests of 99 DME. Allegiance Home Health, Inc. is a California Corporation that engages in providing skilling nursing, physical therapy, speech pathology, medical social worker and home health aide. See Note 7 for further information regarding PMIOC.
F-31
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
NMM issued 7,500,000 shares of common stock to the APCN-ACO shareholders, with a fair value of $3,075,000. Based on the Company’s valuation, which utilized the income – discounted cash flow and market approaches, the estimated fair value of the NMM common stock issued as consideration for the transaction was $0.41 per share. Transaction costs are not included as a component of consideration transferred and were expensed as incurred, which were minimal and are included in general and administrative expenses in the accompanying consolidated statements of income.
The Company accounted for the acquisition as a business combination using the acquisition method of accounting which requires, among other things, that assets acquired and liabilities assumed be recognized at their fair values as of the acquisition date and be recorded on the consolidated balance sheets. Under the acquisition method of accounting, the total purchase consideration was allocated to the intangible assets acquired with the remainder allocated to goodwill. Goodwill is not deductible for tax purposes.
The final allocation of the total purchase price to the net assets acquired is summarized as follows:
| Investments in other entities – cost method | $ | 25,000 | ||
| Identifiable intangible asset - member relationships | 1,738,000 | |||
| Goodwill | 1,679,849 | |||
| Total assets acquired | 3,442,849 | |||
| Deferred tax liability | (367,849 | ) | ||
| Total liabilities assumed | (367,849 | ) | ||
| Net assets acquired | $ | 3,075,000 |
In the view of management, the goodwill recorded in the transaction reflects the Company’s future cash flow expectations and its market position in the healthcare industry. The intangible asset represents $1,738,000 recognized for the fair value of the member relationships that has an approximate useful life of 7 years. The valuation of the member relationships acquired was based on management’s estimates, available information, and reasonable and supportable assumptions, and are considered Level 3 measurements. The fair value of the member relationships was estimated utilizing the income – discounted cash flow and market valuation approaches.
Prior to the merger with NMM, APCN-ACO had minimal activity. For the year ended December 31, 2015, APCN-ACO had approximately $171,000 (unaudited) of operating expenses and net loss, which included $160,000 (unaudited) of management fees from an unrelated service provider. Due to insignificant operations, the Company did not determine it is necessary to present supplemental pro forma information for the year ended December 31, 2015.
F-32
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
ACO Acquisition Corporation #2, and Allied Physicians ACO, LLC
On December 18, 2016, NMM, ACO Acquisition
Corporation #2, and Allied Physicians ACO, LLC
(“AP-ACO”) entered into a reorganization agreement whereby ACO Acquisition Corporation #2, a newly organized entity
which NMM is its sole shareholder, merged into AP-ACO, effective on December 20, 2016, the date of filing the merger agreement
with the California Secretary of State. AP-ACO operates an ACO, as defined under the MSSP, which is comprised of the ACO’s
network of independent medical practices. The primary reason for the business combination was for NMM to acquire the member relationships
of AP-ACO.
Immediately following the effective date, NMM became the sole member of AP-ACO. On the effective date, all of the membership interests of AP-ACO issued and outstanding immediately prior to the effective date were converted on a pro rata basis into 4,000,000 shares of NMM common stock. All of AP-ACO’s right, title and interest in and to all of its assets as of the effective date were included as part of the merger, including, without limitation, all of AP-ACO’s economic interest in PMIOC. See note 7 for further information regarding PMIOC.
NMM issued 4,000,000 shares of common stock (which includes 1,600,000 shares issued to APC) with a fair value of $2,080,000 to the members of AP-ACO. Per management’s evaluation, which utilized the income – discounted cash flow and market approaches, the estimated fair value of the NMM common stock issued as consideration for the transaction was $0.52 per share. Transaction costs are not included as a component of consideration transferred and were expensed as incurred, which were minimal and are included in general and administrative expenses in the accompanying consolidated statements of income.
NMM did not acquire any identifiable tangible assets and did no assume any liabilities as a result of the acquisition.
The Company accounted for the acquisition as a business combination using the acquisition method of accounting which requires, among other things, that assets acquired and liabilities assumed be recognized at their fair values as of the acquisition date and be recorded on the consolidated balance sheets. Under the acquisition method of accounting, the total purchase consideration was allocated to the intangible assets acquired with the remainder allocated to goodwill. Goodwill is not deductible for tax purposes.
The final allocation of the total purchase price to the net assets acquired is summarized as follows:
| Identifiable intangible asset - member relationships | $ | 1,497,000 | ||
| Goodwill | 1,192,968 | |||
| Total assets acquired | 2,689,968 | |||
| Deferred tax liability | (609,968 | ) | ||
| Total liabilities assumed | (609,968 | ) | ||
| Net assets acquired | $ | 2,080,000 |
F-33
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
In the view of management, the goodwill recorded in the transaction reflects the Company’s future cash flow expectations and its market position in the healthcare industry. The intangible asset represents $1,497,000 recognized for the fair value of the member relationships that has an approximate useful life of 5 years. The valuation of the member relationships acquired was based on a management’s evaluation, management’s estimates, available information, and reasonable and supportable assumptions, and are considered Level 3 measurements. The fair value of the member relationships was estimated utilizing the income – discounted cash flow and market valuation approaches.
Prior to the merger with NMM, AP-ACO had minimal activity. For the year ended December 31, 2015, AP-ACO had approximately $200 (unaudited) of operating expenses and net loss. Due to insignificant operations, the Company did not determine it is necessary to present supplemental pro forma information for the year ended December 31, 2015.
| 4. | Land, Property and Equipment, Net |
Land, property and equipment, net consists of:
| 2016 | 2015 | |||||||
| Land | $ | 3,300,000 | $ | 3,300,000 | ||||
| Buildings | 2,510,161 | 2,499,469 | ||||||
| Computer software | 2,263,805 | 1,441,521 | ||||||
| Furniture and equipment | 7,928,054 | 6,381,381 | ||||||
| Construction in progress | 954,470 | 100,000 | ||||||
| Leasehold improvements | 1,621,605 | 1,363,337 | ||||||
| 18,578,095 | 15,085,708 | |||||||
| Less accumulated depreciation and amortization | (8,204,762 | ) | (6,758,884 | ) | ||||
| Land, property and equipment, net | $ | 10,373,333 | $ | 8,326,824 | ||||
Depreciation and amortization expense was $1,445,877 and $952,110 for the years ended December 31, 2016 and 2015, respectively.
| 5. | Intangible Assets, Net |
At December 31, 2016, intangible assets, net consists of the following:
| Useful Life (Years) |
Gross December 31, 2015 |
Additions | Gross December 31, 2016 |
Accumulated Amortization |
Net December 31, 2016 |
|||||||||||||||||
| Network/payor relationships | 15 | $ | 106,660,000 | $ | - | $ | 106,660,000 | $ | (22,186,665 | ) | $ | 84,473,335 | ||||||||||
| Management contracts | 15 | 22,832,000 | - | 22,832,000 | (2,446,286 | ) | 20,385,714 | |||||||||||||||
| Member relationships | 5-7 | - | 3,235,000 | 3,235,000 | - | 3,235,000 | ||||||||||||||||
| $ | 129,492,000 | $ | 3,235,000 | $ | 132,727,000 | $ | (24,632,951 | ) | $ | 108,094,049 | ||||||||||||
F-34
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
At December 31, 2015, intangible assets, net consists of the following:
| Useful Life (Years) |
Gross December 31, 2014 |
Additions | Gross December 31, 2015 |
Accumulated Amortization |
Net December 31, 2015 |
|||||||||||||||||
| Network/payor relationships | 15 | $ | 74,054,000 | $ | 32,606,000 | $ | 106,660,000 | $ | (7,817,588 | ) | $ | 98,842,412 | ||||||||||
| Management contracts | 15 | - | 22,832,000 | 22,832,000 | (570,800 | ) | 22,261,200 | |||||||||||||||
| $ | 74,054,000 | $ | 55,438,000 | $ | 129,492,000 | $ | (8,388,388 | ) | $ | 121,103,612 | ||||||||||||
Included in depreciation and amortization on the consolidated statements of income is amortization expense of $16,244,563 and $7,727,952 for the years ended December 31, 2016 and 2015, respectively.
Future amortization expense is estimated to be approximately as follows for the years ending December 31:
| Amount | ||||
| 2017 | $ | 17,000,000 | ||
| 2018 | 15,300,000 | |||
| 2019 | 13,000,000 | |||
| 2020 | 11,300,000 | |||
| 2021 | 9,700,000 | |||
| Thereafter | 41,794,049 | |||
| $ | 108,094,049 | |||
The member relationship assets acquired from both APCN-ACO and AP-ACO represent member lives that are to be utilized by APA-ACO, and are considered part of the ACO operating segment. APA-ACO, an entity owned 50% by NMM and 50% by Apollo Medical Holdings, Inc. (“AMEH”) (see Note 7) and is also a Next Gen ACO (“NGACO”), which was approved in January 2017. The Center for Medicare and Medicaid services (“CMS”) is implementing the NGACO Model under section 1115A of the Social Security Act, which authorizes CMS, through its Center for Medicare and Medicaid Innovation, to test innovative payment and service delivery models that have the potential to reduce Medicare, Medicaid or Children’s Health Insurance Program expenditures while maintaining or improving the quality of beneficiaries’ care. The purpose of the NGACO Model is to test an alternative Medicare ACO payment model. Specifically, this model will test whether health outcomes improve and Medicare Parts A and B expenditures for Medicare FFS beneficiaries decrease if Medicare ACOs (1) accept a higher level of financial risk compared to existing Medicare ACO payment models, and (2) are permitted to select certain innovative Medicare payment arrangements and to offer certain additional benefit enhancements to their assigned Medicare FFS beneficiaries. These member relationships acquired in 2016 were reenrolled under APA-ACO on January 1, 2017. Members of APCN-ACO and AP-ACO may opt out of the automatic enrollment into APA-ACO.
F-35
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
| 6. | Goodwill |
The following is a summary of goodwill activity for the years ended December 31, 2016 and 2015:
Management Services Reporting Unit
| Balance at January 1, 2015 | $ | - | ||
| Acquisition of PIPA MSO | 44,321,086 | |||
| Balance at December 31, 2015 and 2016 | $ | 44,321,086 |
Health Care Services Reporting Unit
| Balance at January 1, 2015 | $ | 38,612,424 | ||
| Acquisition of PHW | 17,917,634 | |||
| Balance at December 31, 2015 | 56,530,058 | |||
| Impairment loss in Apple Physicians Organization | (316,610 | ) | ||
| Balance at December 31, 2016 | $ | 56,213,448 |
ACO Reporting Unit
| Balance at January 1, 2016 | $ | - | ||
| Acquisition of APCN-ACO | 1,679,849 | |||
| Acquisition of AP-ACO | 1,192,968 | |||
| Balance at December 31, 2016 | $ | 2,872,817 |
Total
| Balance at January 1, 2015 | $ | 38,612,424 | ||
| Acquisitions | 62,238,720 | |||
| Balance at December 31, 2015 | 100,851,144 | |||
| Acquisitions | 2,872,817 | |||
| Impairment loss in Apple Physicians Organization | (316,610 | ) | ||
| Balance at December 31, 2016 | $ | 103,407,351 |
F-36
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
| 7. | Investments in Other Entities |
Equity Method
LaSalle Medical Associates
LaSalle Medical Associates, Inc., (“LMA”) was founded by Dr. Albert Arteaga in 1996 and currently operates four neighborhood medical centers employing more than 120 dedicated healthcare professionals, treating children, adults and seniors in San Bernardino County. LMA’s patients are primarily served by Medi-Cal and they also accept Blue Cross, Blue Shield, Molina, Care 1st, Health Net and Inland Empire Health Plan. LMA is also an IPA of independently contracted doctors, hospitals and clinics, delivering high quality care to more than 245,000 patients in Fresno, Kings, Los Angeles, Madera, Riverside, San Bernardino and Tulare Counties. During 2012, APC-LSMA entered into a share purchase agreement whereby APC-LSMA invested $5,000,000 for a 25% interest in LMA’s IPA line of business. NMM has a management services agreement with LMA. APC accounts for its investment in LMA under the equity method as APC has the ability to exercise significant influence, but not control over LMA’s operations. For the years ended December 31, 2016 and 2015, APC recorded income from this investment of $3,857,391 and $985,616, respectively, in the accompanying consolidated statements of income. During the years ended December 31, 2016 and 2015, APC also received dividends of $2,000,000 and $500,000, respectively, from LMA. The investment balance was $9,503,875 and $7,646,484 at December 31, 2016 and 2015, respectively.
LMA’s IPA line of business summarized balance sheets at December 31, 2016 and 2015 and summarized statements of income for the years ended December 31, 2016 and 2015 are as follows (unaudited):
Balance Sheets
| December 31, |
2016 (unaudited) |
2015 (unaudited) |
||||||
| Assets | ||||||||
| Cash and cash equivalents | $ | 18,441,306 | $ | 22,746,976 | ||||
| Restricted cash | - | 1,800,000 | ||||||
| Receivables, net | 3,142,173 | 2,807,126 | ||||||
| Investments | - | 8,117,474 | ||||||
| Other current assets | 1,589,606 | 166,537 | ||||||
| Loan receivable | 1,250,000 | - | ||||||
| Other assets | 657,171 | 1,267,356 | ||||||
| Total assets | $ | 25,080,256 | $ | 36,905,469 | ||||
F-37
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
Liabilities and Stockholders’ Equity
| December 31, |
2016 (unaudited) |
2015 (unaudited) |
||||||
| Current liabilities | $ | 18,253,224 | $ | 22,506,477 | ||||
| Stockholders’ equity | 6,827,032 | 14,398,992 | ||||||
| Total liabilities and stockholders’ equity | $ | 25,080,256 | $ | 36,905,469 | ||||
Statements of Income
| Years ended December 31, |
2016 (unaudited) |
2015 (unaudited) |
||||||
| Revenues | $ | 191,530,251 | $ | 169,488,210 | ||||
| Expenses | 164,694,297 | 162,815,750 | ||||||
| Income before provision for income taxes | 26,835,954 | 6,672,460 | ||||||
| Provision for income taxes | (11,406,393 | ) | (2,730,200 | ) | ||||
| Net income | $ | 15,429,561 | $ | 3,942,460 | ||||
PMIOC
PMIOC was incorporated in 2004 in the state of California. PMIOC provides comprehensive diagnostic imaging services using state-of-the-art technology. PMIOC offers high quality diagnostic services such as MRI/MRA, PET/CT, CT, nuclear medicine, ultrasound, digital x-rays, bone densitometry and digital mammography at their facilities.
In July 2015, APC-LSMA entered into a share purchase agreement whereby APC-LSMA invested $1,200,000 for a 40% ownership in PMIOC. APC paid $564,000 cash, and APCN-ACO and AP-ACO paid an aggregate of $36,000 on behalf of APC, for this investment with the remaining $600,000 due on or before December 31, 2016, pursuant to a promissory note dated July 1, 2015. The remaining balance of $600,000 was included in notes payable – related party as of December 31, 2015 and was repaid in full in 2016.
APC and PMIOC have an Ancillary Service Contract together whereby PMIOC provides covered services on behalf of APC to enrollees of the plans of APC. Under the Ancillary Service Contract APC paid PMIOC fees of $1,797,064 and $1,889,366 for the years ended December 31, 2016 and 2015, respectively. APC accounts for its investment in PMIOC under the equity method of accounting as APC has the ability to exercise significant influence, but not control over PMIOC’s operations. During the years ended December 31, 2016 and 2015, APC recorded income from this investment of $19,722 and $126,705, respectively, in the accompanying consolidated statements of income and has an investment balance of $1,346,428 and $1,326,705 at December 31, 2016 and 2015, respectively.
F-38
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
Universal Care, Inc.
Universal Care, Inc. (“UCI”) is a privately held health plan that has been in operation since 1985 in order to help its members through the complexities of the healthcare system. UCI holds a license under the California Knox-Keene Health Care Services Plan Act (Knox-Keene Act) to operate as a full-service health plan. UCI contracts with the CMS under the Medicare Advantage Prescription Drug Program.
On August 10, 2015, UCAP, an entity solely owned 100% by APC with APC’s executives, Dr. Thomas Lam, Dr. Pen Lee and Dr. Kenneth Sim, as designated managers of UCAP, purchased from UCI 100,000 shares of UCI class A-2 voting common stock (comprising 48.9% of the total outstanding UCI shares, but 50% of UCI’s voting common stock) for $10,000,000. APC accounts for its investment in UCI under the equity method of accounting as APC has the ability to exercise significant influence, but not control over UCI’s operations. During the years ended December 31, 2016 and 2015, the Company recorded income from this investment of $848,027 and $94,333 (represents allocation of net income of UCI from November 18, 2015 through December 31, 2015), respectively, in the accompanying consolidated statements of income and has an investment balance of $10,942,360 and $10,094,333 at December 31, 2016 and 2015, respectively.
In 2015, the Company also advanced $5,000,000 to UCI for working capital purposes. The subordinated loan accrues interest at the prime rate plus 1%, or 4.75% and 4.50% as of December 31, 2016 and 2015, respectively, with interest to be paid monthly. Pursuant to the stock purchase agreement, the principal repayment schedule is based on certain contingent criteria. The entire note receivable has been classified as non-current loans receivable - related parties on the consolidated balance sheets as of December 31, 2016 and 2015 in the amount of $5,000,000.
UCI’s balance sheets at December 31, 2016 and 2015 and statements of income for the years ended December 31, 2016 and 2015 are as follows:
Balance Sheets
| December 31, |
2016 (unaudited) |
2015 (unaudited) |
||||||
| Assets | ||||||||
| Cash | $ | 23,155,207 | $ | 13,654,114 | ||||
| Receivables, net | 17,928,792 | 14,104,690 | ||||||
| Other current assets | 11,319,582 | 11,700,474 | ||||||
| Other assets | 2,432,338 | 1,313,720 | ||||||
| Property and equipment, net | 1,099,766 | 1,091,361 | ||||||
| Total assets | $ | 55,935,685 | $ | 41,864,359 | ||||
F-39
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
Liabilities and Stockholders’ Equity
| December 31, |
2016 (unaudited) |
2015 (unaudited) |
||||||
| Current liabilities | $ | 46,718,155 | $ | 34,558,426 | ||||
| Other liabilities | 8,075,977 | 10,093,585 | ||||||
| Stockholders’ equity (deficit) | 1,141,553 | (2,787,652 | ) | |||||
| Total liabilities and stockholders’ equity (deficit) | $ | 55,935,685 | $ | 41,864,359 | ||||
Statements of Income
| Years ended December 31, |
2016 (unaudited) |
2015 (unaudited) |
||||||
| Revenues | $ | 161,289,612 | $ | 118,875,432 | ||||
| Expenses | 161,277,959 | 121,548,237 | ||||||
| Income (loss) before benefit for income taxes | 11,653 | (2,672,805 | ) | |||||
| Benefit for income taxes | (1,615,678 | ) | (1,957,947 | ) | ||||
| Income (loss) before other income and discontinued operations | 1,627,331 | (714,858 | ) | |||||
| Other income | 106,875 | - | ||||||
| Loss from discontinued operations | - | (1,122,518 | ) | |||||
| Total other income (loss) from discontinued operations | 106,875 | (1,122,518 | ) | |||||
| Net income (loss) | $ | 1,734,206 | $ | (1,837,376 | ) | |||
DMG
On May 14, 2016, David C.P. Chen M.D., Inc., a California professional corporation doing business as Diagnostic Medical Group (“DMG”), David C.P. Chen M.D., individually (collectively “Seller”) and APC-LSMA, a designated shareholder professional corporation formed on October 15, 2012, which is 100% owned by Dr. Thomas Lam (CEO of APC) and is controlled and consolidated by APC who is the primary beneficiary of this VIE, entered into a share purchase agreement whereby APC-LSMA acquired a 40% ownership interest in DMG for total cash consideration of $1,600,000.
Seller may in Seller’s sole discretion (but shall not be obligated to) use all or a portion of the purchase price proceeds to purchase shares of common stock of APC and/or NMM. The purchase price for any shares of APC and/or NMM common stock shall be at the then applicable price per share established by APC and/or NMM Board of Directors, respectively (which, as of the closing date is $1.00 per share of APC common stock and $1.00 per share of NMM common stock).
F-40
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
Notwithstanding the foregoing, in the event Seller (in Seller’s sole discretion) uses a portion of the purchase price proceeds to purchase shares of APC common stock, Seller shall have the right to purchase 60,000 shares of APC common stock for the aggregate purchase price of $10,000 (the “AP Share Option”), provided that, (i) the AP Share Option shall automatically expire on the date that is three (3) months after the closing date unless exercised by written notice given by Seller to APC prior to the expiration thereof; and (ii) any shares of APC common stock purchased by Seller that are not covered by the AP Share Option shall be purchased by Seller at the then applicable price per share established by the APC Board of Directors. See note 12 for details of the accounting for the stock option.
In July 2016, APC advanced $200,000 to DMG pursuant to a promissory note agreement. The note accrues interest at 3.5% per annum and matures on June 30, 2018. The balance of $200,000 is included in loans receivable – related parties in the accompanying consolidated balance sheet as of December 31, 2016.
During 2016, APC also contributed its portion of additional capital of $40,000 to DMG for working capital purposes, which represents APC’s 40% investment portion.
APC accounts for its investment in DMG under the equity method of accounting as APC has the ability to exercise significant influence, but not control over DMG’s operations. APC recorded income from this investment of $43,698 in 2016 in the accompanying consolidated statement of operations and has an investment balance of $1,683,698 at December 31, 2016.
PASC
Pacific Ambulatory Surgery Center, LLC (“PASC”), a California limited liability company, is a multi-specialty outpatient surgery center that is certified to participate in the Medicare program and is accredited by the Accreditation Association for Ambulatory Health Care. PASC has entered into agreements with organizations such as healthcare service plans, independent physician practice associations, medical groups and other purchasers of healthcare services for the arrangement of the provision of outpatient surgery center services to subscribers or enrollees of such health plans. On November 15, 2016, PASC and APC, entered into a membership interest purchase agreement whereby PASC sold 40% of its aggregate issued and outstanding membership interests to APC for total consideration of $800,000.
In connection with the membership interest purchase agreement, PASC entered into a management services agreement with NMM, which requires the payment of management fees computed as 2% of PASC revenues. The term of the management services agreement commenced on the effective date and extend for a period of 60 months thereafter, and may be extended in writing at the sole option of NMM for an additional period of 60 months following the expiration of the initial term and is automatically renewed for additional consecutive terms of three years unless terminated by either party. PASC shall not be permitted to terminate the management services agreement for any reason during the initial term and, if extended, the extended term.
APC accounts for its investment in PASC under the equity method of accounting as APC has the ability to exercise significant influence, but not control over PASC’s operations. APC recorded a loss from this investment of $20,296 in 2016 in the accompanying consolidated statement of income and has an investment balance of $779,704 at December 31, 2016.
F-41
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
APA-ACO
On May 25, 2016, NMM and AMEH established APA-ACO as a joint venture entity to facilitate the member lives acquired by NMM through its acquisitions of AP-ACO and APCN-ACO to NGACO (see Note 5). There has been no activity for this joint venture as of December 31, 2016.
ICC
On November 15, 2016, APC-LSMA, a holding company of APC, agreed to purchase and acquire from AHMC International Cancer Center (“ICC”) 40% of the aggregate issued and outstanding shares of capital stock of ICC for $400,000 in cash. ICC is a professional medical California corporation and has entered into agreements with organizations such as healthcare service plans, independent physician practice associations, medical groups and other purchasers of medical services (“Healthplans”) for the arrangement of the provision of healthcare services to subscribers or enrollees of said Healthplans. In addition, ICC has entered into written agreements with physicians and other healthcare professionals to provide or arrange for the provision of healthcare services to enrollees of participating Healthplans who have contracted or will contract with ICC for healthcare services. Subsequent to the acquisition, it was agreed that ICC’s working capital needs shall be funded as and when needed through capital contributions and/or subordinated debt by the shareholders of ICC on a pro rata basis based on their respective ownership interests in ICC. This transaction has not been completed yet, as certain requirements were not met.
Investments in other entities – equity method consists of the following:
| Years ended December 31, | 2016 | 2015 | ||||||
| Universal Care, Inc. | $ | 10,942,360 | $ | 10,094,333 | ||||
| LaSalle Medical Associates – IPA Line of Business | 9,503,875 | 7,646,484 | ||||||
| Diagnostic Medical Group | 1,683,698 | - | ||||||
| Pacific Medical Imaging & Oncology Center, Inc. | 1,346,428 | 1,326,705 | ||||||
| Pacific Ambulatory Surgery Center, LLC | 779,704 | - | ||||||
| Apple Physicians Organization | - | 7,697 | ||||||
| $ | 24,256,065 | $ | 19,075,219 | |||||
During the year ended December 31, 2016, the Company recorded an impairment charge of $7,697 related to the investment from the acquisition of Apple Physicians Organization in 2008, as the amount was not determined to be recoverable.
Cost Method
Apollo Medical Holdings, Inc.
On October 14, 2015, the Company invested $10 million in connection with the purchase of shares of Series A preferred stock (“Series A Preferred Stock”) and warrants (“Series A Warrants”) of AMEH, a publicly traded company, in which Dr. Thomas Lam, the CEO of NMM, is also a director. At the time, the investment represented a 16.9% equity ownership interest of AMEH, and it was determined that NMM does not have the ability to exercise significant influence over the operating and financial policies of AMEH, and as such, is accounted for under the cost method as of December 31, 2016 and 2015.
F-42
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
The Series A Preferred Stock has a liquidation preference in the amount of $9.00 per share plus any declared and unpaid dividends. The Series A Preferred Stock can be voted for the number of shares of AMEH Common Stock into which the Series A Preferred Stock could then be converted, which initially is one-for-one. The Series A Preferred Stock is convertible into shares of AMEH Common Stock, at the option of NMM, at any time after issuance at an initial conversion rate of one-for-one, subject to adjustment in the event of stock dividends, stock splits and certain other similar transactions. The Series A Preferred Stock is mandatorily convertible not sooner than the earlier to occur of (i) the later of (x) January 31, 2017 or (y) 60 days after the date on which AMEH file their quarterly report on Form 10-Q for the period ended September 30, 2016 (the “Redemption Expiration Date”); or (ii) the date on which AMEH receive the written, irrevocable decision of NMM not to require a redemption of the Series A Preferred Stock (as described in the following paragraph), in the event that AMEH engage in one or more transactions resulting in gross proceeds of not less than $5,000,000, not including any transaction with NMM.
At any time prior to conversion and through the Redemption Expiration Date, the Series A Preferred Stock may be redeemed at the option of NMM, on one occasion, in the event that AMEH’s net revenue for the four quarters ended September 30, 2016, as reported in its periodic filings under the Exchange Act, are less than $60,000,000. In such event, AMEH shall have up to one year from the date of the notice of redemption by NMM to redeem the Series A Preferred Stock, the Series A Warrants and any shares of Common Stock issued in connection with the exercise of any Series A Warrants theretofore (collectively the “Redeemed Securities”), for the aggregate price paid therefore by NMM, together with interest at a rate of 10% per annum from the date of the notice of redemption until the closing of the redemption. Any mandatory conversion described in the previous paragraph shall not take place until such time as it is determined that that conditions for the redemption of the Redeemed Securities have not been satisfied or, if such conditions exist, NMM has decided not to have such securities redeemed. NMM has agreed to relinquish its redemption rights relating to the Series A Preferred Stock it owns in AMEH pursuant to the terms of a Consent and Waiver Agreement dated as of December 21, 2016 by and between AMEH and NMM. The Series A Warrants may be exercised at any time after issuance and through October 14, 2020, for $9.00 per share, subject to adjustment in the event of stock dividends and stock splits.
Alternatively, the Series A Warrants may be exercised pursuant to a “cashless exercise” feature, for that number of shares of Common Stock determined by dividing (x) the aggregate Fair Market Value (as defined in the Series A Warrant) of the shares in respect of which the Series A Warrant is being converted minus the aggregate Warrant Exercise Price (as defined in the Series A Warrant) of such shares by (y) the Fair Market Value of one share of AMEH Common Stock. The Series A Warrants are not separately transferable from the Series A Preferred Stock. The Series A Warrants are subject to redemption in the event that the Series A Preferred Stock is redeemed by NMM, as described above.
NMM has the right to designate to the Nominating/Corporate Governance Committee of the Board of Directors one person to be nominated as a director of AMEH. NMM has designated Thomas S. Lam, M.D., and he was elected as a director of AMEH on January 19, 2016.
On March 30, 2016, NMM purchased 555,555 units of AMEH’s securities for $4,999,995, each unit consisting of one share of Series B convertible preferred stock (“Series B Preferred Stock”) and a stock purchase warrant (a “Series B Warrants”) to purchase one share of AMEH’s common stock at $10.00 per share, none of which securities have yet been converted or exercised for AMEH common stock, but which could result in the issuance by AMEH of up to 1,111,111 shares of AMEH common stock to NMM if they converted all of the Series B Preferred Stock and exercised all of the Series B Warrants that are currently held.
F-43
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
The Series B Preferred Stock has a liquidation preference in the amount of $9.00 per share plus any declared and unpaid dividends. The Series B Preferred Stock can be voted for the number of shares of Common Stock into which the Series B Preferred Stock could then be converted, which initially is one-for-one.
Based on the relative fair values of the investment in the Series A and B preferred stock and the related warrants, the carrying balance of the investment in AMEH as of December 31, 2016 and 2015 was $10,550,002 and $7,077,778, respectively, and is included in Investments in other entities – cost method in the accompanying consolidated balance sheets.
The Series B Warrants may be exercised at any time after issuance and through March 31, 2021, for $10.00 per share, subject to adjustment in the event of stock dividends and stock splits. Alternatively, the Series B Warrants may be exercised pursuant to a “cashless exercise” feature, for that number of shares of AMEH Common Stock determined by dividing (x) the aggregate Fair Market Value (as defined in the Series B Warrants) of the shares in respect of which the Series B Warrants is being converted minus the aggregate Warrant Exercise Price (as defined in the Series B Warrants) of such shares by (y) the Fair Market Value of one share of AMEH Common Stock. The Series B Warrants are not separately transferable from the Series B Preferred Stock.
The Series A and Series B warrants are accounted for as derivative instruments and recorded at their fair values of $5,338,886 and $2,088,889 (see Note 2) as of December 31, 2016 and 2015, respectively, and are included in Derivative asset - warrants in the accompanying consolidated balance sheets.
On December 21, 2016, AMEH, entered into an Agreement and Plan of Merger (the “Merger Agreement”) among AMEH, Apollo Acquisition Corp., a California corporation and wholly-owned subsidiary of AMEH (“Merger Subsidiary”), NMM, and Kenneth Sim, M.D., not individually, but in his capacity as the representative of the shareholders of NMM (the “Shareholders’ Representative”).
Thomas Lam, M.D. and Kenneth Sim, M.D. entered into Voting Agreements with AMEH. Under the Voting Agreements, Dr. Sim and Dr. Lam have agreed, among other things, to vote in favor of the approval and adoption of the Merger (as such term is defined below) and the Merger Agreement.
Under the terms of the Merger Agreement, Merger Subsidiary will merge with and into NMM, with NMM becoming a wholly-owned subsidiary of AMEH (the “Merger”). The Merger is intended to qualify for federal income tax purposes as a tax deferred reorganization under the provisions of Section 368(a) of the Internal Revenue Code of 1986. In the transaction, NMM will receive such number of shares of AMEH common stock such that NMM shareholders will own 82% and AMEH shareholders will own 18% of issued and outstanding shares of AMEH at closing. Additionally, NMM agreed to relinquish its redemption rights relating to the preferred stock it owns in AMEH pursuant to the terms of a Consent and Waiver Agreement dated as of December 21, 2016 by and between AMEH and NMM.
The transaction was approved unanimously by the Board of Directors of both companies. Consummation of the Merger is subject to various closing conditions, including, among other things, approval by the stockholders of AMEH and the stockholders of NMM. As part of the Merger Agreement, AMEH and NMM have made various mutual representations and warranties. Within five business days following the execution of the Merger Agreement, NMM was required provide a working capital loan to AMEH in the principal amount of $5,000,000, which occurred on January 3, 2017 and is evidenced by a promissory note (see above).
F-44
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
The Merger Agreement grants each party the ability to update disclosure schedules through January 20, 2017. If any updated disclosure schedules are found to be unacceptable to the receiving party, as determined in such receiving party’s sole discretion, then such receiving party may terminate the Merger Agreement no later than February 3, 2017 (see Note 17 for amendment to the Merger Agreement). The Merger Agreement provides that Thomas Lam, M.D., current Chief Executive Officer of NMM, and Warren Hosseinion, M.D., current Chief Executive Officer of AMEH will be Co-Chief Executive Officers of the combined company upon closing of the transaction. Kenneth Sim, M.D., who currently serves as Chairman of NMM, will be Executive Chairman of AMEH. Gary Augusta, current Executive Chairman of AMEH, will be President, Mihir Shah will continue as Chief Financial Officer, and Hing Ang, current Chief Financial Officer of NMM will be the Chief Operating Officer. Adrian Vazquez, M.D. and Albert Young, M.D. current Medical Officers of AMEH will be Co-Chief Medical Officers. The Board of Directors will consist of nine directors, five appointees (including three independent directors) from NMM and four appointees (including two independent directors) from AMEH.
| 8. | Accounts Payable and Accrued Expenses |
Accounts payable and accrued expenses consists of the following:
| December 31, | 2016 | 2015 | ||||||
| Accounts payable | $ | 420,351 | $ | 762,503 | ||||
| Specialty capitation payable | 678,335 | - | ||||||
| Subcontractor IPA risk pool payable | 1,709,112 | 687,357 | ||||||
| ACA payable | 718,808 | 1,562,680 | ||||||
| Dividends payable | - | 4,500,000 | ||||||
| Deferred revenue | 603,041 | 656,906 | ||||||
| Accrued compensation | 2,537,703 | 743,597 | ||||||
| Accrued other | 1,415,927 | 1,743,113 | ||||||
| $ | 8,083,277 | $ | 10,656,156 | |||||
| 9. | Medical Liabilities |
Medical liabilities consists of the following:
| Years ended December 31, | 2016 | 2015 | ||||||
| Balance, beginning of year | $ | 16,011,519 | $ | 11,892,747 | ||||
| Claims paid for previous year | (14,501,482 | ) | (11,686,430 | ) | ||||
| Incurred health care costs | 98,906,764 | 82,201,352 | ||||||
| Claims paid for current year | (84,520,493 | ) | (69,995,093 | ) | ||||
| Adjustments | 3,061,157 | 3,598,943 | ||||||
| Balance, end of year | $ | 18,957,465 | $ | 16,011,519 | ||||
F-45
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
| 10. | Bank Loan, Lines of Credit and Loan Payable – Related Party |
Bank Loan
Bank loan consists of the following:
| December 31, | 2016 | 2015 | ||||||
| Bank loan bearing interest at 4.88%, matures on January 13, 2034 | $ | - | $ | 1,477,561 | ||||
| Less: current portion | - | (45,183 | ) | |||||
| Bank loan, net of current portion | $ | - | $ | 1,432,378 | ||||
On January 13, 2014, APC entered into a mortgage loan agreement with a bank in the amount of $1,575,000. This note was guaranteed by one of APC’s board members, Theresa C. Tseng. Interest on the Note was 4.63% per annum. The note required APC to make 239 monthly payments of $10,132 commencing February 13, 2014 and maturing on January 13, 2034. The loan was collateralized by both the building and the rents due APC on the same building. On February 4, 2016, this loan was repaid in full. In connection with this repayment, APC incurred a prepayment penalty of $44,200 and the amount is included in interest expense in the accompanying consolidated statement of operations for the year ended December 31, 2016.
The loan agreement contained certain affirmative covenants and as of December 31, 2015, APC was in compliance with all covenants.
Interest expense on the note payable totaled $26,465 for the year ended December 31, 2015.
On July 24, 2015, NMM entered into a promissory note agreement with a bank to borrow up to $15,000,000. The note was guaranteed by two officers of APC. The interest rate is based on the Wall Street Journal “prime rate” plus 1.00% or 4.50% as of December 31, 2015 and required 18 monthly consecutive interest payments, beginning August 24, 2015; 59 monthly consecutive principal and interest payments in the initial amount of $54,896 each, beginning February 24, 2017 and maturing on January 24, 2022. NMM borrowed $10,000,000 in October 2015 and repaid the entire amount in December 2015. The loan was cancelled on July 27, 2016.
Lines of Credit
In April 2012, NMM entered into a promissory note agreement with a bank, which was amended on April 9, 2016 (as amended, the “NMM Business Loan Agreement”). The NMM Business Loan Agreement modifies certain terms of the promissory note agreement in order to (i) increase the original loan availability amount of $2,000,000 to $10,000,000, (ii) extend the maturity date under the promissory note agreement to April 22, 2018, and (iii) add six additional guarantees. The interest rate is based on the Wall Street Journal “prime rate” plus 0.125% or 3.875% and 3.625% as of December 31, 2016 and 2015, respectively. As of December 31, 2016, the Company was not in compliance with certain financial debt covenant requirements contained in the loan agreement. Subsequent to year end, NMM obtained a waiver from the bank for noncompliance of the financial debt covenant requirements as of and for the years ended December 31, 2016 and 2015. The loan is personally guaranteed by 13 shareholders who are also members of the Company’s board of directors and is collateralized by substantially all assets of NMM. No amounts were drawn on this line during 2016 and 2015 and no amounts were outstanding as of December 31, 2016 and 2015.
F-46
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
In April 2012, APC entered into a promissory note agreement with a bank, which was amended on April 22, 2016 (as amended, the “APC Business Loan Agreement”). The APC Business Loan Agreement modifies certain terms of the promissory note agreement in order to (i) increase the original loan availability amount of $3,000,000 to $10,000,000, (ii) extend the maturity date under the promissory note agreement to April 22, 2018, and (iii) add six additional guarantees. The interest rate is based on the Wall Street Journal “prime rate” plus 0.125% or 3.875% and 3.625% as of December 31, 2016 and 2015, respectively. As of December 31, 2016 and 2015, the Company was not in compliance with certain financial debt covenant requirements contained in the loan agreement. Subsequent to year end, APC obtained a waiver from the bank for noncompliance of the financial debt covenant requirements as of and for the years ended December 31, 2016 and 2015. The loan is personally guaranteed by 13 shareholders who are also members of the Company’s board of directors and two-non board members and is collateralized by substantially all assets of APC. No amounts were drawn on this line during 2016 and 2015 and no amounts were outstanding as of December 31, 2016 and 2015.
Loan Payable to Related Party
In connection with the investment in PMIOC (see Note 7), APC entered into a promissory note agreement on July 1, 2015 for $600,000, which represents the remaining unpaid balance of the investment consideration. The remaining balance of $600,000 was included in loan payable – related party as of December 31, 2015 and was repaid in full in 2016.
The remainder of this page intentionally left blank.
F-47
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
| 11. | Income Taxes |
Provision for (benefit from) Income tax consists of the following for the years ended December 31:
| 2016 | 2015 | |||||||
| Current | ||||||||
| Federal | $ | 9,161,855 | $ | 19,193,646 | ||||
| State | 2,664,336 | 4,872,324 | ||||||
| 11,826,191 | 24,065,970 | |||||||
| Deferred | ||||||||
| Federal | (2,199,180 | ) | (3,897,730 | ) | ||||
| State | (810,599 | ) | (870,793 | ) | ||||
| (3,009,779 | ) | (4,768,523 | ) | |||||
| Total income tax expense | $ | 8,816,412 | $ | 19,297,447 | ||||
The Company uses the liability method of accounting for income taxes as set forth in ASC 740. Under the liability method, deferred taxes are determined based on differences between the financial statement and tax bases of assets and liabilities using enacted tax rates. As of December 31, 2016, the Company does not have any Federal or California tax net operating loss carryforwards.
The provision for income taxes differs from the amount computed by applying the federal income tax rate as follows for the year ended December 31:
| 2016 | 2015 | |||||||
| Tax provision at U.S. Federal statutory rates | 35.0 | % | 35.0 | % | ||||
| State income taxes net of federal benefit | 6.0 | 5.7 | ||||||
| Federal rate adjustment | - | 1.6 | ||||||
| Non-deductible permanent items | 6.5 | 0.1 | ||||||
| Non-taxable entities | (3.2 | ) | (0.9 | ) | ||||
| Others | 2.5 | 0.5 | ||||||
| Effective income tax rate | 46.8 | % | 42.0 | % | ||||
F-48
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
Significant components of the Company’s deferred tax assets (liabilities) include the following as of December 31:
| 2016 | 2015 | |||||||
| Deferred tax assets (liabilities) | ||||||||
| State taxes | $ | 888,867 | $ | 1,700,906 | ||||
| Stock options | 1,685,965 | 889,692 | ||||||
| Accrued payroll and related cost | 208,576 | 162,799 | ||||||
| Property and equipment | (2,009,313 | ) | (1,339,315 | ) | ||||
| Acquired intangible assets | (44,036,361 | ) | (49,344,878 | ) | ||||
| Other | (3,669,941 | ) | (1,033,373 | ) | ||||
| Net deferred tax liabilities | $ | (46,932,207 | ) | $ | (48,964,169 | ) | ||
As of December 31, 2016 and 2015, the Company does not have any unrecognized tax benefits related to various federal and state income tax matters. The Company will recognize accrued interest and penalties related to unrecognized tax benefits in income tax expense.
The Company is subject to U.S. federal income tax as well as income tax of multiple state tax jurisdictions. The Company is subject to U.S federal income tax examination from 2013 onward and state income tax examination from 2012 onward. APC’s 2015 U.S. Federal tax return is currently being audited by the Internal Revenue Service. APC currently does not expect any material adjustments to arise from this audit. The Company does not anticipate material unrecognized tax benefits within the next 12 months.
| 12. | Mezzanine and Shareholders’ Equity |
All common stock has no par value and is non-transferable and is governed by the stockholders’ agreement. As the redemption feature (see Note 2) of the shares of common stock of NMM was not within the control of the NMM, all common stock and additional paid-in capital did not qualify as permanent equity and was classified as mezzanine or temporary equity as redeemable common stock.
The 24,582,400 and 22,982,400 shares of common stock classified as treasury stock as of December 31, 2016 and 2015, respectively, represents shares of NMM stock issued to APC. As NMM consolidates APC, such shares are not considered to be outstanding.
NMM
Stock Split
On June 30, 2015, NMM filed an amendment to its Articles of Incorporation to effectuate a 3.192-for-1 stock split.
On July 28, 2015, NMM filed an amendment to its Articles of Incorporation to effectuate a 3-for-1 stock split.
F-49
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
All share and per share amounts relating to the common stock and stock options to purchase common stock, including the respective exercise prices of each such option, included in the consolidated financial statements and footnotes have been retroactively adjusted to reflect the increased number of shares resulting from this action. The number of authorized, but unissued, shares were not adjusted as a result of the stock split. No fractional shares were issued following the stock split and NMM has paid cash in lieu of any fractional shares resulting from the stock split of an insignificant amount.
Authorized Share Capital
On July 28, 2015, subsequent to the 3:1 stock split stated above, NMM filed an amendment to its Articles of Incorporation to increase its authorized number of common shares from 300,000,000 to 900,000,000 shares.
NMM is required to reserve and keep available out of the authorized, but unissued shares of common stock such number of shares sufficient to effect the exercise of all outstanding options granted and available for grant under APC’s Exclusivity Amendment Agreement and shares offered to providers or members to purchase from time to time. The number of shares of common stock issued and outstanding and shares reserved for issuance as of December 31, 2016 is as follows:
| 2016 | ||||
| Shares of common stock issued and outstanding | 366,343,818 | |||
| Unissued October 1, 2014 stock options granted | 2,031,600 | |||
| Total | 368,375,418 | |||
2015 Share Issuances
During 2015, NMM issued an aggregate of 157,876,218 shares of common stock as consideration for the acquisition of PIPA MSO. The fair value of the stock was determined to be $0.37 per share for total valuation of the consideration of $57,887,947 (see Note 3).
During 2015, NMM issued an aggregate of 750,000 shares of common stock at a price of $0.33 per share to a group of doctors. The share price was determined to be below the estimated fair market value of NMM’s stock on the measurement date; and therefore resulted in additional share-based compensation expense of $72,500 in 2015. NMM received aggregate proceeds of $250,000 from the sale of these shares of common stock.
During 2015, NMM issued an aggregate of 15,437,514 shares of common stock at $1.00 per share for aggregate proceeds of $15,437,514, of which $1,300,000 was included in subscription receivable on the consolidated balance sheet as of December 31, 2015, which was paid in full in January 2016.
During 2015, NMM issued 600,000 shares of common stock at $0.50 per share for aggregate proceeds of $300,000.
F-50
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
During 2015, an aggregate of 5,932,350 stock options from the Exclusivity Amendment Agreement (see stock options section below) were exercised at $0.167 per share and the aggregate amount received by NMM of $988,725 was recorded as a long-term liability for unissued equity shares until the termination date of October 1, 2019. Despite being legally issued shares, these shares are not considered outstanding and are excluded from the earnings (loss) per share calculation due to the forfeiture feature contained in the agreement.
2016 Share Issuances and Repurchases
During 2016, 107,500 shares of NMM common stock were repurchased at $1.00 per share for $107,500. Such share repurchase reduced the number of shares issued and outstanding as they were subsequently retired.
During 2016, NMM issued 7,500,000 shares of common stock as consideration for the acquisition of APCN-ACO. The fair value of the stock was determined to be $0.41 per share for total valuation of the consideration of $3,075,000 (see Note 3).
During 2016, NMM issued 4,000,000 shares of common stock (which includes 1,600,000 issued to APC) as consideration for the acquisition of AP-ACO. The fair value of the stock was determined to be $0.52 per share for total valuation of the consideration of $2,080,000 (see Note 3).
During 2016, NMM sold 5,850,000 shares of common stock at $1.00 per share for aggregate proceeds of $5,850,000.
During 2016, NMM sold 83,700 shares of common stock at $0.50 per share for aggregate proceeds of $41,850.
During 2016, an option was exercised for the purchase of 250,000 shares of NMM common stock at $0.50 per share for gross proceeds of $125,000.
APC
As the redemption feature (see Note 2) of the shares is not solely within the control of APC, the equity of APC does not qualify as permanent equity and has been classified as noncontrolling interests in mezzanine or temporary equity.
2015 Share Issuances
During 2015, APC issued an aggregate of 60,714,750 shares of common stock as consideration for the acquisition of PHW. The fair value of the stock was determined to be $0.62 per share for total valuation of the consideration of $37,238,000 (see Note 3).
During 2015, APC sold an aggregate of 1,500,000 shares of common stock at a price of $0.17 per share to a group of doctors. The share price was determined to be below the estimated fair market value of APC’s stock on the measurement date; therefore, resulted in additional share-based compensation expense of $680,000 in 2015. APC received aggregate proceeds of $250,000 from the sale of shares of common stock.
F-51
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
During 2015, an aggregate of 6,053,550 stock options from the Exclusivity Amendment Agreement, were exercised at $0.167 per share and the aggregate amount received of $1,008,925 was recorded as a long-term liability for unissued equity shares until the termination date of October 1, 2019. These shares are not considered outstanding due to the forfeiture feature contained in the agreement.
During 2015, APC sold an aggregate of 10,253,114 shares of common stock at $1.00 per share for aggregate proceeds of $10,253,114, of which $525,000 was included in subscription receivable on the consolidated balance sheet as of December 31, 2015, which was collected in full in January 2016.
2016 Share Issuances and Repurchases
During 2016, APC sold an aggregate of 3,145,000 shares of common stock at $1.00 per share for aggregate proceeds of $3,145,000.
During 2016, APC sold 83,700 shares of common stock at a price of $0.50 per share to a board member for cash proceeds of $41,850. The share price was determined to be below the estimated fair market value of APC’s common stock on the measurement date; therefore, resulted in additional share-based compensation expense of $21,762 recorded in 2016.
During 2016, an option was exercised for the purchase of 250,000 shares of APC common stock at $0.50 per share for gross proceeds of $125,000.
During 2016, an option was exercised for the purchase of 60,000 shares of APC common stock at $0.17 per share for gross proceeds of $10,000.
During 2016, APC issued an aggregate of 1,500,000 shares of common stock to former shareholders of Pacific Independent Physician Association, a Medical Group, Inc. (“PIPA”) for no consideration; therefore, resulted in additional share-based compensation expense of $380,000 recorded in 2016.
During 2016, an aggregate of 410,000 shares of APC common stock were repurchased at $1.00 per share for $410,000. Such share repurchases reduced the number of shares issued and outstanding as they were subsequently retired.
During 2016, $525,000 of cash was received related to an APC stock subscription receivable at December 31, 2015.
The remainder of this page intentionally left blank.
F-52
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
Stock Options
Stock Options Issued Under Primary Care Physician Agreements
On October 1, 2014, NMM and APC entered into an Exclusivity Amendment Agreement as part of the Primary Care Physician Agreement to issue stock options to purchase shares of NMM and APC common stock. The medical providers agreed to exclusivity to APC for health enrollees in consideration per provider of a sign-on bonus in the amount of $25,000 (or $15,000 if already a preferred provider). The stock options were granted from the date of agreement through May 1, 2015 and are treated as issuances to non-employees. The exercise price of the stock options is $0.167 per share and providers can exercise anytime between August 1, 2015 and October 1, 2019, as long as the providers continue to provide services pursuant to the terms of the agreement through October 1, 2019. If the agreement is terminated by the provider with or without cause, the sign-on bonus and any capitation payment above standard rates made in accordance with the terms of the agreement shall be fully repaid to APC by the terminating medical provider. In addition, any unexercised share options held by the terminating medical provider will be forfeited on effective date of termination, and any share options that have been exercised will be bought back by NMM and APC at the original purchase price.
On May 1, 2015, in connection with the formula contained in the Exclusivity Amendment Agreement, it was determined that effective on August 1, 2015, stock options for the purchase of a total of 7,963,950 eligible shares were granted to the medical providers. The stock options have a term of 5 years, which is through the term of the Exclusivity Amendment Agreement. These options are accounted for as options granted to non-employees. In accordance with relevant accounting guidance, the value of the applicable share-based compensation is periodically remeasured using an appropriate valuation model and income or expense is recognized during the vesting terms of the equity instruments at each reporting period end date.
During the year ended December 31, 2015, a total of 5,932,350 NMM stock options were exercised for the purchase of shares of common stock that resulted in aggregate proceeds received by NMM of $988,725, which in accordance with relevant accounting guidance are reflected as long-term liability for unissued equity shares as of December 31, 2016 and 2015 based on the features noted above.
During the year ended December 31, 2015, a total of 6,053,550 APC stock options were exercised for the purchase of shares of common stock that resulted in aggregate proceeds received by APC of $1,008,925, which in accordance with relevant accounting guidance are reflected as long-term liability for unissued equity shares as of December 31, 2016 and 2015 based on the features noted above.
F-53
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
The stock options under the Exclusivity Amendment Agreement were accounted for at fair value, as determined using the Black-Scholes option pricing model and the following assumptions:
| Year ended December 31, | 2016 | 2015 | ||||||
| Expected term | 2.75 years | 3.75 years | ||||||
| Expected volatility | 53.01 | % | 66.62 | % | ||||
| Risk-free interest rate | 1.47 | % | 1.31 | % | ||||
| Market value of common stock | $0.52 - $0.76 | $0.37 - $0.62 | ||||||
| Annual dividend yield | 2.51% - 3.53 | % | 0.28% - 0.75 | % | ||||
| Forfeiture rate | 8 | % | 0% - 4 | % | ||||
The Company’s stock option activity for options grants under the Exclusivity Amendment Agreement for NMM is summarized below:
| Shares | Weighted Average Exercise Price |
Weighted Average Remaining Contractual Term (Years) |
Aggregate Intrinsic Value |
|||||||||||||
| Options outstanding at January 1, 2015 | 7,963,950 | $ | 0.167 | 4.75 | $ | 167,003 | ||||||||||
| Options granted | - | - | - | - | ||||||||||||
| Options exercised | (5,932,350 | ) | 0.167 | - | 753,319 | |||||||||||
| Options forfeited | - | - | - | - | ||||||||||||
| Options outstanding at December 31, 2015 | 2,031,600 | $ | 0.167 | 3.75 | $ | 473,363 | ||||||||||
| Options exercisable at December 31, 2015 | 2,031,600 | $ | 0.167 | 3.75 | $ | 473,363 | ||||||||||
| Options outstanding at January 1, 2016 | 2,031,600 | $ | 0.167 | 3.75 | $ | 473,363 | ||||||||||
| Options granted | - | - | - | - | ||||||||||||
| Options exercised | - | - | - | - | ||||||||||||
| Options forfeited | - | - | - | - | ||||||||||||
| Options outstanding at December 31, 2016 | 2,031,600 | $ | 0.167 | 2.75 | $ | 717,155 | ||||||||||
| Options exercisable at December 31, 2016 | 2,031,600 | $ | 0.167 | 2.75 | $ | 717,155 | ||||||||||
The remainder of this page intentionally left blank.
F-54
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
The Company’s stock option activity for options grants under the Exclusivity Amendment Agreement for APC is summarized below:
| Shares | Weighted Average Exercise Price |
Weighted Average Remaining Contractual Term (Years) |
Aggregate Intrinsic Value |
|||||||||||||
| Options outstanding at January 1, 2015 | 7,963,950 | $ | 0.167 | 4.75 | $ | 3,395,297 | ||||||||||
| Options granted | - | - | - | - | ||||||||||||
| Options exercised | (6,053,550 | ) | 0.167 | - | 2,812,883 | |||||||||||
| Options forfeited | - | - | - | - | ||||||||||||
| - | - | |||||||||||||||
| Options outstanding at December 31, 2015 | 1,910,400 | $ | 0.167 | 3.75 | $ | 960,931 | ||||||||||
| Options exercisable at December 31, 2015 | 1,910,400 | $ | 0.167 | 3.75 | $ | 960,931 | ||||||||||
| Options outstanding at January 1, 2016 | 1,910,400 | $ | 0.167 | 3.75 | $ | 960,931 | ||||||||||
| Options granted | - | - | - | - | ||||||||||||
| Options exercised | - | - | - | - | ||||||||||||
| Options forfeited | - | - | - | - | ||||||||||||
| Options outstanding at December 31, 2016 | 1,910,400 | $ | 0.167 | 2.75 | $ | 1,138,598 | ||||||||||
| Options exercisable at December 31, 2016 | 1,910,400 | $ | 0.167 | 2.75 | $ | 1,138,598 | ||||||||||
The aggregate intrinsic value is calculated as the difference between the exercise price and the estimated fair value of NMM and APC’s common stock as of December 31, 2016 and 2015.
Share-based compensation expense related to common stock option awards granted in connection with the Exclusivity Amendment Agreement recognized over their respective vesting periods is as follows:
| Year ended December 31, | 2016 | 2015 | ||||||
| Contracted physicians and other services | $ | 1,512,740 | $ | 1,193,637 | ||||
The remaining unrecognized share based compensation expense of stock option awards granted in connection with the Exclusivity Amendment Agreement as of December 31, 2016 was $1,508,471 and $2,580,359 for NMM and APC, respectively, which is expected to be recognized over the remaining term of 2.75 years.
Other Options
In August 2015, NMM granted an option to a medical provider to purchase 250,000 shares of common stock at an exercise price of $0.50 per share. The stock option has a term of one year. The estimated fair value of the stock option was $15,000 and was computed using the Black-Scholes option pricing model and the following assumptions: (i) estimated market price of $0.43 per share; (ii) exercise price of $0.50 per share; (iii) expected term of 1 year; (iv) volatility of 50%; (v) annual dividend yield of 0.28%; and (vi) discount rate of 1.00%. The Company expensed $15,000 as share-based compensation during the year ended December 31, 2015.
F-55
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
In August 2015, APC granted an option to a medical provider to purchase 250,000 shares of common stock at an exercise price of $0.50 per share. The stock option has a term of one year. The estimated fair value of the stock option was $42,500 and was computed using the Black-Scholes option pricing model and the following assumptions: (i) estimated market price of $0.67 per share; (ii) exercise price of $0.50 per share; (iii) expected term of 1 year; (iv) volatility of 50%; (v) annual dividend yield of 0.75%; and (vi) discount rate of 1.00%. The Company expensed $42,500 as share-based compensation during the year ended December 31, 2015.
In May 2016, APC granted an option to a medical provider to purchase 60,000 shares of common stock at an exercise price of $0.17 per share. The stock option has a term of one year. The estimated fair value of the stock option was $35,000 and was computed using the Black-Scholes option pricing model and the following assumptions: (i) estimated market price of $0.76 per share; (ii) exercise price of $0.17 per share; (iii) expected term of 1 year; (iv) volatility of 50%; (v) annual dividend yield of 0.75%; and (vi) discount rate of 1.00%. The Company expensed $35,000 as share-based compensation during the year ended December 31, 2016.
In March 2016, NMM granted an option to the CFO of NMM to purchase 1,100,000 shares of common stock at an exercise price of $1.00 per share. The stock option had a term of five years, with the following vesting schedule (i) 150,000 (2014), 150,000 (2015), 250,000 (2016), 250,000 (2017) and 300,000 (2018). The estimated fair value of the stock option was $9,472 and was computed using the Black-Scholes option pricing model and the following assumptions: (i) estimated market price of $0.41 per share; (ii) exercise price of $1.00 per share; (iii) expected term of 1 year; (iv) volatility of 62.79%; (v) annual dividend yield of 3.53%; (vi) discount rate of 0.85%; and (vii) forfeiture rate of 8%. The Company expensed $4,736 as share-based compensation during the year ended December 31, 2016.
Dividends, Reduction of Capital and Distributions
During the years ended December 31, 2016 and 2015, NMM paid dividends of $20,000,000 and $935,635, respectively.
During the year ended December 31, 2016, APC paid dividends of $5,750,000, of which $4,500,000 was accrued at December 31, 2015. The $1,250,000 dividends that were declared in 2016 were recorded as a reduction of capital as a result of having an accumulated deficit at the time of the issuance.
During the years ended December 31, 2016 and 2015, CDSC paid distributions of $909,429 and $862,571, respectively. In addition, CDSC had net capital change of $110,000 during the year ended December 31, 2016, which resulted in an increase in APC’s ownership in CDSC from 41.6% to 43.43% as of December 31, 2016.
F-56
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
| 13. | Commitments and Contingencies |
Operating Leases
The Company leases office space and equipment under certain non-cancelable operating lease agreements. Rental expense for the years ended December 31, 2016 and 2015 was approximately $2,400,000 and $2,200,000, respectively. As of December 31, 2016 and 2015, the future minimum rental payments under non-cancelable operating leases were as follows:
| Years ending December 31, | Amount | |||
| 2017 | $ | 2,000,000 | ||
| 2018 | 1,100,000 | |||
| 2019 | 1,000,000 | |||
| 2020 | 700,000 | |||
| 2021 | 500,000 | |||
| Total | $ | 5,300,000 | ||
Equipment Subject to Capital Lease
In January 2016, NMM entered into a lease for certain computer equipment. Under the terms of the lease agreement NMM have the option to purchase the equipment at the end of the original two year lease term for $1 (bargain purchase option). In accordance with relevant accounting guidance the lease is classified as a capital lease. The lease requires monthly payments of $8,050 through December 30, 2017 and bears interest at the rate of 3.625% per annum.
In January 2015, NMM entered into a lease for certain phone equipment. Under the terms of the lease agreement NMM are obligated to purchase the equipment at the end of the original two year lease term for $1 (bargain purchase option). In accordance with relevant accounting guidance the lease is classified as a capital lease. The lease requires monthly payments of $7,641 through January 1, 2017 and bears interest at the rate of 3.625% per annum. The remaining obligation of this capital lease was $97,264 as of December 31, 2015 and was fully paid off in 2016.
The remainder of this page intentionally left blank.
F-57
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
The following is a schedule of future minimum lease payments on the non-cancelable capital lease as of December 31, 2016:
| Year ending December 31, | Amount | |||
| 2016 | $ | 104,218 | ||
| Total minimum payments required | 104,218 | |||
| Less amount representing interest | (1,870 | ) | ||
| Present value of net minimum lease payments | 102,348 | |||
| Less current portion | (102,348 | ) | ||
| Long-term portion | $ | - | ||
| Equipment under capital lease | $ | 186,092 | ||
| Less: accumulated amortization | (37,218 | ) | ||
| $ | 148,874 | |||
Regulatory Matters
Laws and regulations governing the Medicare program and healthcare generally are complex and subject to interpretation. The Company believes that it is in compliance with all applicable laws and regulations and is not aware of any pending or threatened investigations involving allegations of potential wrongdoing. While no regulatory inquiries have been made, compliance with such laws and regulations can be subject to future government review and interpretation as well as significant regulatory action including fines, penalties, and exclusion from the Medicare and Medi-Cal programs.
As a risk-bearing organization, the Company is required to follow regulations of the California Department of Managed Health Care (“DMHC”). The Company must comply with a minimum working capital requirement, Tangible Net Equity (“TNE”) requirement, cash-to-claims ratio and claims payment requirements prescribed by the DMHC. TNE is defined as net assets less intangibles, less non-allowable assets (which include amounts due from affiliates), plus subordinated obligations. At December 31, 2016 and 2015, the Company was in compliance with these regulations.
Many of the Company’s payor and provider contracts are complex in nature and may be subject to differing interpretations regarding amounts due for the provision of medical services. Such differing interpretations may not come to light until a substantial period of time has passed following contract implementation. Liabilities for claims disputes are recorded when the loss is probable and can be estimated. Any adjustments to reserves are reflected in current operations.
F-58
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
Legislation and HIPAA
The healthcare industry is subject to numerous laws and regulations of federal, state and local governments. These laws and regulations include, but are not necessarily limited to, matters such as licensure, accreditation, government healthcare program participation requirements, reimbursement for patient services, and Medicare and Medicaid fraud and abuse. Government activity has continued with respect to investigations and allegations concerning possible violations of fraud and abuse statutes and regulations by healthcare providers. Violations of these laws and regulations could result in expulsion from government healthcare programs together with the imposition of significant fines and penalties, as well as significant repayments for patient services previously billed.
The Company believes that it is in compliance with fraud and abuse regulations as well as other applicable government laws and regulations. Compliance with such laws and regulations can be subject to future government review and interpretation as well as regulatory actions unknown or unasserted at this time.
The Health Insurance Portability and Accountability Act (“HIPAA”) assures health insurance portability, reduces healthcare fraud and abuse, guarantees security and privacy of health information, and enforces standards for health information. The Health Information Technology for Economic and Clinical Health Act (“HITECH Act”) expanded upon HIPAA in a number of ways, including establishing notification requirements for certain breaches of protected health information. In addition to these federal rules, California has also developed strict standards for the privacy and security of health information as well as for reporting certain violations and breaches. The Company may be subject to significant fines and penalties if found not to be compliant with these state or federal provisions.
Affordable Care Act
The Patient Protection and Affordable Care Act (“PPACA”) is resulting in substantial reform in the United States health care system. The legislation impacts multiple aspects of the health care system, including many provisions that change payments from Medicare, Medicaid and insurance companies. Starting in 2014, the legislation required the establishment of health insurance exchanges, which will provide individuals without employer-provided health care coverage the opportunity to purchase insurance. It is anticipated that some employers currently offering insurance to employees will opt to have employees seek insurance coverage through the insurance exchanges. It is possible that the reimbursement rates paid by insurers participating in the insurance exchanges may be substantially different than rates paid under current health insurance products. Another significant component of the PPACA is the expansion of the Medicaid program to a wide range of newly eligible individuals. In anticipation of this expansion, payments under certain existing programs, such as Medicare disproportionate share, will be substantially decreased. Each state’s participation in an expanded Medicaid program is optional. However, the PPACA may be repealed and replaced under the current administration. The potential outcome of the repeal and replacement is unknown at this time and could have a material impact on the Company.
Litigation
The Company is involved from time to time in routine legal matters incidental to its business. In the opinion of the management, resolution of such matters is not expected to have a material effect on its financial position or results of operations.
F-59
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
Liability Insurance
The Company believes that its insurance coverage is appropriate based upon the Company’s claims experience and the nature and risks of the Company’s business. In addition to the known incidents that have resulted in the assertion of claims, the Company cannot be certain that its insurance coverage will be adequate to cover liabilities arising out of claims asserted against the Company, the Company’s affiliated professional organizations or the Company’s affiliated hospitalists in the future where the outcomes of such claims are unfavorable. The Company believes that the ultimate resolution of all pending claims, including liabilities in excess of the Company’s insurance coverage, will not have a material adverse effect on the Company’s financial position, results of operations or cash flows; however, there can be no assurance that future claims will not have such a material adverse effect on the Company’s business. Contracted physicians are required to obtain their own insurance coverage.
Although the Company currently maintains liability insurance policies on a claims-made basis, which are intended to cover malpractice liability and certain other claims, the coverage must be renewed annually, and may not continue to be available to the Company in future years at acceptable costs, and on favorable terms.
| 14. | Related Party Transactions |
In October 2015, NMM invested $10 million in connection with the purchase of shares of Series A Preferred Stock and Series A Warrants of AMEH in which Dr. Thomas Lam, the CEO of NMM became a director of AMEH. In March 2016, NMM invested an additional $5,000,000 in connection with the purchase of shares of Series B Preferred Stock and Series B Warrants of AMEH (see Note 7). In addition, as of December 31, 2016, NMM has a receivable balance of $200,000 due from AMEH for reimbursement of expenses included in accounts receivable in the accompanying consolidated balance sheet.
On November 16, 2015, APC entered into a subordinated note receivable agreement with UCI, a 48.9% owned equity method investee, in the amount of $5,000,000 (see Note 7). The note accrues interest at prime plus 1% per annum, or 4.75% at December 31, 2016 and is due on or before September 2017. At December 31, 2016 and 2015, the balance of the note was $5,000,000, and is reflected in the accompanying consolidated balance sheets.
During the year ended December 31, 2016, APC paid approximately $265,000 to Advance Diagnostic Surgery Center for services as a provider. Advance Diagnostic Surgery Center shares common ownership with certain board members of APC.
During the years ended December 31, 2016 and 2015, NMM received approximately $17.2 million and $15.4 million, respectively, in management fees from LMA, which is accounted for under the equity method based on 25% equity ownership interest held by APC (see Note 7).
During the years ended December 31, 2016 and 2015, APC paid approximately $1.8 million and $1.9 million, respectively, to PMIOC for provider services, which is accounted for under the equity method based on 40% equity ownership interest held by APC (see Note 7).
During the years ended December 31, 2016 and 2015, APC paid approximately $2.2 million and $2.0 million, respectively, to AMG, Inc. for services as a provider. AMG, Inc. shares common ownership with certain board members of APC.
F-60
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
During the years ended December 31, 2016 and 2015, APC paid approximately $5.3 million and $4.6 million, respectively, to DMG for provider services, which is accounted for under the equity method based on 40% equity ownership interest held by APC (see Note 7).
During the years ended December 31, 2016 and 2015, NMM paid approximately $1.0 million and $0.7 million, respectively, to Medical Property Partners (“MPP”) for office lease. MPP shares common ownership with certain board members of NMM.
During the years ended December 31, 2016 and 2015, APC paid approximately $0.2 million and $0.3 million, respectively, to Tag-2 Medical Investment Group, LLC (“Tag-2”) for office lease. Tag-2 shares common ownership with certain board members of APC. APC was also the guarantor for Tag-2’s loan with a bank. In connection with the loan agreement, APC provided collateral to the bank, which represents the $1,000,000 certificate of deposit accounted for as investment in marketable securities (see Note 2). In November 2016, the collateral and guarantee were no longer required, as Tag-2 was able to renew the loan without such collateral and guarantee requirement.
During the years ended December 31, 2016 and 2015, APC paid an aggregate of approximately $26.7 and $26.5 million, respectively to shareholders for provider services.
During the year ended December 31, 2016 and 2015, APC paid an aggregate of approximately $14.0 million and $11.7 million, respectively, to shareholders who are also officers of APC for provider services.
For related party loan payable, see Note 10.
For loans receivable from related parties, see Note 7.
| 15. | Employee Benefit Plan |
NMM has a qualified 401(k) plan that covers substantially all employees who have completed at least six months of service and meet minimum age requirements. Participants may contribute a portion of their compensation to the plan, up to the maximum amount permitted under Section 401(k) of the Internal Revenue Code. Participants become fully vested after six years of service. NMM matches a portion of the participants’ contributions. NMM’s matching contributions for the years ended December 31, 2016 and 2015 was approximately $320,000 and $58,000, respectively.
| 16. | Earnings Per Share |
As of December 31, 2016 and 2015, 5,932,350 shares had been issued as a result of the exercise of stock options. Despite being legally issued shares, these shares are not considered outstanding due to the forfeiture feature of the stock options (see Note 12), and accordingly these shares are excluded from the basic earnings per share computations and included in the diluted earnings per share computations. In addition, for the years ended December 31, 2016 and 2015, dilutive shares from stock options outstanding of 1,379,144 and 1,183,407, respectively, are excluded from the basic earnings per share computations as their inclusion would be anti-dilutive and included in the diluted earnings per share computations.
F-61
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
Below is a summary of the earnings per share computations:
| Years ended December 31, | 2016 | 2015 | ||||||
| Earnings per share – basic | $ | 0.03 | $ | 0.05 | ||||
| Earnings per share – diluted | $ | 0.03 | $ | 0.05 | ||||
| Weighted average shares of common stock outstanding – basic | 360,634,339 | 256,619,159 | ||||||
| Weighted average shares of common stock outstanding – diluted | 367,945,833 | 263,734,916 | ||||||
| 17. | Subsequent Events |
The Company has evaluated subsequent events through July 13, 2017, the date the accompanying consolidated financial statements were available to be issued, and determined that no subsequent events have occurred that would require recognition in the consolidated financial statements or disclosure in the notes thereto, other than as disclosed in the accompanying notes to the consolidated financial statements.
Loans Receivable – Related Parties
On January 3, 2017, pursuant to a promissory note agreement, NMM provided a loan to AMEH in the principal amount of $5,000,000. The entire outstanding principal amount is due and payable in full on the maturity date of January 3, 2019. Interest accrues at 1% point above the Prime Rate commencing on the first date of the first month immediately following the execution of the note agreement and is to be paid by AMEH to NMM in successive quarterly installments.
Amendment to Merger Agreement
As part of an amendment to the Merger Agreement on March 30, 2017, the merger consideration to be paid by AMEH to NMM was amended to include warrants to purchase 850,000 shares of common stock at an exercise price of $11 per share, that will only be granted in the case that the proposed merger between the NMM and AMEH occurs (such warrant will not vest and will expire if the contemplated merger transaction does not occur), in exchange for NMM providing both a guarantee for AMEH’s $5,000,000 convertible note payable to Alliance Apex (“Alliance Note”) and as compensation to NMM for relinquishing their right to additional shares in AMEH based on the agreed upon exchange ratio with NMM in the event that the Alliance Note is converted to AMEH common stock.
Equity
From January 1, 2017 through April 30, 2017, NMM received cash in the aggregate amount of $248,925 from the exercise of stock options to purchase 1,493,550 shares of NMM common stock at $0.17 per share.
From January 1, 2017 through April 30, 2017, APC received cash in the aggregate amount of $176,100 from the exercise of stock options to purchase 1,056,600 shares of APC common stock at $0.17 per share.
In March 2017, NMM paid bonuses in the aggregate of $2,020,000 to board members based on a 3 tier payment system for 2016 performance that was accrued as of December 31, 2016.
F-62
Network Medical Management, Inc.
Notes to Consolidated Financial Statements
On March 17, 2017, APC paid dividends of $8,750,000 to its shareholders.
Investments - Netlytics
NMM entered into a Joint Venture Agreement dated as of January 25, 2017, with Mediportal LLC, a New York limited liability company, and Rulemeister Inc., a California corporation, to form a joint venture company to be named Netlytics Enterprise LLC (“Netlytics”) for the purpose of developing and implementing a fully-integrated electronic platform that will enable ACOs, IPAs, health plans and other health care payers and providers to aggregate data and utilize analytic tools to effectively engage in population health management. Netlytics was formed on November 1, 2016. The respective ownership interests of NMM, Mediportal and Rulemeister in Netlytics will be 55%, 30% and 15%. In exchange for its 55% interest, NMM will contribute $275,000 as its capital contribution to Netlytics. As of the date these consolidated financial statements are available to be issued, there has been no activity and no amounts have been contributed to Netlytics.
F-63
NETWORK MEDICAL MANAGEMENT, INC.
INDEX TO 2014 AUDITED FINANCIAL STATEMENTS
F-64
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
CONSOLIDATED FINANCIAL STATEMENTS
AS OF AND FOR THE YEAR ENDED DECEMBER 31, 2014
F-65
CERTIFIED PUBLIC ACCOUNTANTS
430 S GARFIELD AVE SUITE 428
ALHAMBRA, CA 91801
| Eric Wu, CPA | Tel: 626-452-1149 | |
| Fax: 626-452-1156 |
Independent Auditors' Report
To the Board of Directors and Stockholders of
Network Medical Management Inc. and Affiliates:
Report on the Financial Statements
We have audited the accompanying consolidated balance sheet of Network Medical Management Inc. and Affiliates as of December 31, 2014, and the related consolidated statements of operation, shareholders’ deficit and redeemable common stock, and cash flows for the year ended December 31, 2014.
Management’s Responsibility for the Financial Statements
Management is responsible for the preparation and fair presentation of these consolidated financial statements in accordance with accounting principles generally accepted in the United States of America; this includes the design, implementation, and maintenance of internal control relevant to the preparation and fair presentation of consolidated financial statements that are free from material misstatement, whether due to fraud or error.
Auditor’s Responsibility
Our responsibility is to express an opinion on these consolidated financial statements based on our audit. We conducted our audit in accordance with auditing standards generally accepted in the United States of America. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the consolidated financial statements are free from material misstatement.
An audit involves performing procedures to obtain audit evidence about the amounts and disclosures in the consolidated financial statements. The procedures selected depend on the auditor’s judgment, including the assessment of the risks of material misstatement of the financial statements, whether due to fraud or error. In making those risk assessments, the auditor considers internal control relevant to the entity’s preparation and fair presentation of the financial statements in order to design audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the entity’s internal control. Accordingly, we express no such opinion. An audit also includes evaluating the appropriateness of accounting policies used and the reasonableness of significant accounting estimates made by management, as well as evaluating the overall presentation of the financial statements.
We believe that the audit evidence we have obtained is sufficient and appropriate to provide a basis for our audit opinion.
F-66
Opinion
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of Network Medical Management Inc. and Affiliates as of December 31, 2014 and the results of its operations and its cash flows for the year then ended in accordance with accounting principles generally accepted in the United States of America.
Our previous report dated March 31, 2015 has been withdrawn and the consolidated financial statements have been restated as discussed in note 17.
/s/ DNW & ASSOCIATES, INC.
El Monte, California
April 30, 2017
F-67
NETWORK MEDICAL MANAGEMENT, INC. AND AFFILIATES
CONSOLIDATED BALANCE SHEET
| December 31, 2014 | ||||
| ASSETS | ||||
| CURRENT ASSETS: | ||||
| Cash and cash equivalents | $ | 30,303,370 | ||
| Restricted cash | 300,000 | |||
| Fiduciary cash | 801,258 | |||
| Investment in marketable securities | 1,034,620 | |||
| Accounts receivable | 1,426,582 | |||
| Capitation and claims receivable | 1,703,979 | |||
| Risk pool receivable | 11,113,954 | |||
| Other receivables | 1,040,915 | |||
| Refundable income tax | 129,592 | |||
| Prepaid expenses | 50,954 | |||
| Total current assets | 47,905,224 | |||
| NONCURRENT ASSETS: | ||||
| Land, property and equipment, net | 7,577,417 | |||
| Intangible assets, net | 73,393,564 | |||
| Goodwill | 38,612,424 | |||
| Investments in other entities | 7,160,868 | |||
| Sign-on bonus | 1,911,875 | |||
| Other assets | 88,872 | |||
| Total noncurrent assets | 128,745,020 | |||
| Total assets | $ | 176,650,244 | ||
See accompanying notes to the financial statements
F-68
NETWORK MEDICAL MANAGEMENT, INC. AND AFFILIATES
CONSOLIDATED BALANCE SHEET
| LIABILITIES AND SHAREHOLDER'S DEFICIT | ||||
| CURRENT LIABILITIES: | ||||
| Accounts payable and accrued liabilities | $ | 17,878,520 | ||
| Capitation and incentives payables | 7,907,134 | |||
| Fiduciary accounts payable | 801,258 | |||
| Medical liabilities | 11,892,745 | |||
| Income taxes payable | 1,973,227 | |||
| Notes payable, current portion | 45,183 | |||
| Total current liabilities | 40,498,067 | |||
| NONCURRENT LIABILITIES: | ||||
| Deferred tax liability | 31,143,925 | |||
| Notes payable, long-term portion | 1,483,295 | |||
| Total noncurrent liabilities | 32,627,220 | |||
| Total liabilities | 73,125,287 | |||
| MEZZANINE EQUITY: | ||||
| Noncontrolling interest | 105,067,500 | |||
| Network Medical Management, Inc. shareholders’ equity: Common stock, stated value; shares authorized 300,000,000; shares outstanding 175,703,886 at 12/31/14. | 1,882,559 | |||
| Additional paid-in capital | 89,099 | |||
| Total Network Medical Management Inc. redeemable common stock | 1,971,658 | |||
| SHAREHOLDERS’ DEFICIT: | ||||
| Accumulated deficit | (4,108,304 | ) | ||
| Total Network Medical Management, Inc. shareholders' equity | (4,108,304 | ) | ||
| Noncontrolling interest | 594,103 | |||
| Total shareholders' deficit | (3,514,201 | ) | ||
| Total liabilities and shareholder's equity | $ | 176,650,244 |
See accompanying notes to the financial statements
F-69
Network Medical Management, Inc. and Affiliates
Consolidated Statements of Shareholders’ Deficit and Redeemable Common Stock December 31, 2014
| Mezzanine Equity For NMM Redeemable Common Stock | Total NMM | |||||||||||||||||||||||||||||||||||||||||||
|
Mezzanine Equity For Noncontrolling Interest in APC |
Common Stock | Treasury Stock | Additional Paid-in |
Total NMM Redeemable |
Accumulated | Total NMM Stockholders' |
APC's Noncontrolling |
Total Shareholders' |
||||||||||||||||||||||||||||||||||||
| Interest | Noncontrolling | Shares | Amount | Shares | Amount | Capital | Common Stock | Deficit | Deficit | Interest in CDSC | Deficit | |||||||||||||||||||||||||||||||||
| Balance, December 31, 2013 | $ | 13,189,609 | 175,933,710 | $ | 4,475,331 | - | $ | - | $ | - | 4,475,331 | $ | (3,479,568 | ) | $ | (3,479,568 | ) | $ | 662,744 | $ | (2,816,824 | ) | ||||||||||||||||||||||
| Net income | (13,720,378 | ) | (628,736 | ) | (628,736 | ) | 646,403 | 17,667 | ||||||||||||||||||||||||||||||||||||
| Shares repurchased | (328,400 | ) | (229,824 | ) | (24,000 | ) | (24,000 | ) | - | |||||||||||||||||||||||||||||||||||
| Shares issued in connection with acquisition Shares issued to consolidated VIE | 86,832,000 | 22,982,400 | - | |||||||||||||||||||||||||||||||||||||||||
| Shares issued for cash | 22,951,350 | - | ||||||||||||||||||||||||||||||||||||||||||
| Stock based compensation | 90,771 | 89,099 | 89,099 | - | ||||||||||||||||||||||||||||||||||||||||
| Noncontrolling interest capital change | (548,981 | ) | (548,981 | ) | ||||||||||||||||||||||||||||||||||||||||
| Dividends Repayment of capital | (3,947,452 | ) | (2,568,772 | ) | (2,568,772 | ) | (166,063 | ) | (166,063 | ) | ||||||||||||||||||||||||||||||||||
| Balance, December 31, 2014 | $ | 105,067,500 | 175,703,886 | $ | 1,882,559 | 22,982,400 | $ | - | $ | 89,099 | $ | 1,971,658 | $ | (4,108,304 | ) | $ | (4,108,304 | ) | $ | 594,103 | $ | (3,514,201 | ) | |||||||||||||||||||||
See accompanying notes to the financial statements
F-70
NETWORK MEDICAL MANAGEMENT, INC. AND AFFILIATES
CONSOLIDATED STATEMENT OF OPERATIONS
FOR THE YEAR-ENDED DECEMBER 31, 2014
|
For the Year Ended December 31, 2014 |
||||
| REVENUE: | ||||
| Management income | $ | 11,954,649 | ||
| Capitation and claims | 103,501,636 | |||
| Surgery center income | 4,601,143 | |||
| Risk pool settlements and bonuses | 12,991,159 | |||
| Fee for services | 614,605 | |||
| Miscellaneous income | 676,897 | |||
| Total revenue | 134,340,089 | |||
| EXPENSES: | ||||
| Contracted physicians and other services | 110,497,210 | |||
| General and administrative expenses | 27,262,885 | |||
| Management fees | 8,299,833 | |||
| Depreciation and amortization | 1,367,434 | |||
| Total expenses | 147,427,362 | |||
| LOSS FROM OPERATIONS | (13,087,273 | ) | ||
| OTHER INCOME: | ||||
| Income from equity method investments | 2,072,470 | |||
| Interest income, net | 118,650 | |||
| Other | 126,754 | |||
| Total other, net | 2,317,874 | |||
| LOSS BEFORE INCOME TAXES | (10,769,399 | ) | ||
| INCOME TAXES: | ||||
| Current tax expense | 2,541,384 | |||
| Deferred tax expense | 391,927 | |||
| Total income taxes, net | 2,933,311 | |||
| NET LOSS | $ | (13,702,710 | ) | |
| Less: Net loss attributable to noncontrolling interests | ||||
| (13,073,974 | ) | |||
| NET LOSS ATTRIBUTABLE TO NETWORK MEDICAL MANAGEMENT, INC.’S SHAREHOLDERS | ||||
| $ | (628,736 | ) | ||
See accompanying notes to the financial statements
F-71
NETWORK MEDICAL MANAGEMENT, INC. AND AFFILIATES
CONSOLIDATED STATEMENT OF CASH FLOWS
FOR THE YEAR-ENDED DECEMBER 31, 2014
| Year Ended December 31, 2014 |
||||
| CASH FLOWS FROM OPERATING ACTIVITIES: | ||||
| Net income (loss) | $ | (13,702,710 | ) | |
| Adjustments to reconcile net income to net cash provided by operating activities: | ||||
| Depreciation and amortization | 1,367,434 | |||
| Stock-based compensation expense | 19,471,869 | |||
| Gain on equity method investment | (2,072,470 | ) | ||
| Deferred tax | 267,750 | |||
| Changes in assets and liabilities: | ||||
| Accounts receivable | (6,705,986 | ) | ||
| Other receivable | (2,001,075 | ) | ||
| Prepaid expenses and other current assets | 65,890 | |||
| Accounts payable and accrued liabilities | 4,418,323 | |||
| Income taxes payable | 1,666,408 | |||
| Medical liabilities | 13,399,657 | |||
| Net cash provided by operating activities | 16,175,090 | |||
| CASH FLOWS FROM INVESTING ACTIVITIES: | ||||
| Cash received from the merger | 5,560,662 | |||
| Purchases of marketable securities | (1,034,620 | ) | ||
| Proceeds from note receivable | 5,000,000 | |||
| Increase in restricted cash | (300,000 | ) | ||
| Purchases of property and equipment | (660,288 | ) | ||
| Net cash used in investing activities | 8,565,754 | |||
| CASH FLOWS FROM FINANCING ACTIVITIES: | ||||
| Dividends/repayment of capital paid | (6,682,287 | ) | ||
| Principal payments on notes payable | (4,561,332 | ) | ||
| Purchase of treasury stock | (328,400 | ) | ||
| Proceeds from common stock offering | 3,659,351 | |||
| Repurchase of shares | (24,000 | ) | ||
| Net cash provided by financing activities | (7,936,668 | ) | ||
| Net increase (decrease) in cash and cash equivalents | 16,804,176 | |||
| Cash and cash equivalents, beginning of year | 13,499,194 | |||
| Cash and cash equivalents, end of year | $ | 30,303,370 | ||
| SUPPLEMENTARY DISCLOSURES OF CASH FLOW INFORMATION | ||||
| Interest paid | $ | 150,486 | ||
| Income taxes paid | $ | 11,129 | ||
| Non-Cash Financing and Investing Activities: Stock issued for acquisition | $ | 86,832,000 | ||
| Deferred tax liability adjusted to goodwill | $ | 29,621,600 | ||
| Reclass of fiduciary cash to payable | $ | 801,258 | ||
See accompanying notes to the financial statements
F-72
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
Note 1 – Description of Business
Network Medical Management, Inc. and Affiliate is comprised of three entities: Network Medical Management, Inc. (“NMM”) and Allied Pacific of California IPA, a Professional Medical Corporation d.b.a. Allied Pacific of California IPA, a Professional Medical Corporation DBA Allied Pacific of California (“APC”) and Concourse Diagnostic Surgery Center, LLC. (“CDSC”). NMM was organized for the purpose of providing management services to medical companies and independent practice associations (“IPAs”). The management service covers billing, collection, accounting, administrative, and marketing. APC was incorporated on August 17, 1992 for the purpose of arranging health care services as an IPA. APC has contracts with various health maintenance organizations (“HMOs”) or licensed health care service plans as defined in the Knox-Keene Health Care Service Plan Act of 1975. Each HMO negotiates a fixed amount per member per month ("PMPM") that is to be paid to APC. In return, APC arranges for the delivery of health care services by contracting with physicians or professional medical corporations for primary care and specialty care services. APC assumes the financial risk of the cost of delivering health care services in excess of the fixed amounts received. Some of the risk is transferred to the contracted physicians or professional corporations. The risk is also minimized by stop-loss provisions in contracts with HMOs.
On July 1, 1999, APC entered into an amended and restated management and administrative services agreement with NMM (initial management services agreement was entered into in 1997) for an initial fixed term of 30 years. In accordance with relevant accounting guidance, APC is determined to be a Variable Interest Entity (“VIE”) and NMM is the primary beneficiary with the ability to direct the activities (excluding clinical decisions) that most significantly affect APC’s economic performance through its majority representation of the APC Joint Planning Board; therefore APC is consolidated with NMM. As of December 31, 2014, APC owns 11.57% of NMM.
CDSC was formed on March 25, 2010 in the state of California. CDSC is an ambulatory surgery center in City of Industry, California, is organized by a group of highly qualified physicians, and the surgical center utilizes the most advanced equipment in Eastern Los Angeles County and San Gabriel Valley. The facility is Medicare Certified and accredited by the Accreditation Association for Ambulatory Healthcare, Inc. During 2011, APC invested $625,000 for a 41.6% ownership in CDSC. CDSC has five members on its board of directors. Four of CDSC’s five board members are on the board of directors of NMM and two of the five directors are also on the board of APC. APC and CDSC have an Ancillary Services Contract together whereby CDSC provides covered services on behalf of APC to enrollees of the plans of APC. Under the Ancillary Services Agreement, CDSC is paid for authorized service related to 1) Commercial, Point of Service and Medicare, 2) Medi-Cal Healthy Families and Healthy Kids, and 3) Implant devices. Under the Ancillary Services Agreement APC paid CDSC fees of approximately $57,391 for the years ended December 31, 2014. CDSC is consolidated as a VIE by APC as it was determined that APC has a controlling financial interest in CDSC and is the primary beneficiary of CDSC.
APC-LSMA was formed on October 15, 2012 as a designated shareholder professional corporation and is solely owned by Dr. Thomas Lam, a shareholder and Chief Executive and Financial Officer of APC. APC-LSMA is controlled and consolidated by APC who is the primary beneficiary of this VIE. The only activity of APC-LSMA is to hold the investments in medical corporations, which include LaSalle Medical Associates.
F-73
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
Unless stated otherwise, NMM, APC, CDSC, APC-LSMA and UCAP are collectively referred to herein as the “Company.”
Note 2 – Basis of Presentation and Summary of Significant Accounting Policies
Principles of Consolidation
The Company’s consolidated financial statements have been prepared by management in accordance with accounting principles generally accepted in the United States of America (“GAAP”) and include the accounts of NMM, its consolidated VIE, APC, and its subsidiary UCAP and APC’s consolidated VIEs, CDSC and APC-LSMA. All material intercompany balances and transactions have been eliminated in consolidation.
Business Combinations
The Company uses the acquisition method of accounting for all business combinations, which requires assets and liabilities of the acquiree to be recorded at fair value, to measure the fair value of the consideration transferred, including contingent consideration, to be determined on the acquisition date, and to account for acquisition related costs separately from the business combination.
Use of Estimates
The preparation of consolidated financial statements and related disclosures in conformity with GAAP requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the consolidated financial statements and the reported amounts of revenues and expenses during the reporting period. Significant items subject to such estimates and assumptions include collectability of receivables, recoverability of long-lived and intangible assets, business combination and goodwill impairment, accrual of medical liabilities, determination of shared-risk revenues, income taxes, and stock-based compensation. Management evaluates its estimates and assumptions on an ongoing basis using historical experience and other factors, including the current economic environment, and makes adjustments when facts and circumstances dictate. As future events and their effects cannot be determined with precision, actual results could differ significantly from those estimates and assumptions.
Cash and Cash Equivalents
The Company considers all highly liquid investments that are both readily convertible into known amounts of cash and mature within ninety days from their date of purchase to be cash equivalents.
The Company maintains its cash in deposit accounts with several banks, which at times may exceed federally insured limits. The Company has not experienced any losses in such accounts. The Company believes they are not exposed to any significant credit risk on its cash and cash equivalents. As of December 31, 2014, the Company’s deposit accounts with banks exceeded the Federal Deposit Insurance Corporation’s insured limit by $35,116,379.
F-74
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
Restricted Cash
The Company is required to maintain a reserve fund by certain Health Plans. The required reserve at December 31, 2014 was $300,000.
Fiduciary Cash
As of December 31, 2014, the Company recorded fiduciary cash of $801,258 which represents cash received from the health plans on behalf of subcontractor IPAs. The Company remits the amounts to the subcontractor IPAs the following month and such remittances are included in fiduciary accounts payable in the accompanying consolidated balance sheet.
Investments in Marketable Securities
The appropriate classification of investments is determined at the time of purchase and such designation is reevaluated at each balance sheet date. Investments in marketable securities have been classified and accounted for as held-to-maturity based on management’s investment intentions relating to these securities. Held-to-maturity marketable securities are stated at amortized cost, which approximates fair value. As of December 31, 2014, short-term marketable securities in the amount of $1,034,620 consist of certificates of deposit with various financial institutions, reported at par value plus accrued interest, with maturity dates from four months to twelve months. Investments in certificates of deposits are classified as Level 1 investments in the fair value hierarchy.
Accounts Receivable
The Company’s receivables are comprised of accounts receivable, capitation and claims receivable, risk pool and incentive receivables. Accounts receivable primarily consists of NMM management fee receivables and CDSC fee-for-service (“FFS”) receivables. Risk pool and incentive receivables mainly consist of APC full risk pool receivable which is recorded based on a modified cash basis, whereby a receivable is only recorded when expected cash receipts are known or when actual cash is received from Health Source MSO’s who serves as the management company for the hospitals in the risk pools. Capitation and claims receivable relate to the health plan’s capitation which is received by APC in the following month of service. For APC, other receivables is accrued based on invoices sent to the subcontracted IPA for stop loss insurance premium reimbursement and FFS reimbursement for Alhambra Hospital Medical Center’s self–insured program. For NMM, other receivable is accrued based on invoices for certain expense reimbursements from UCI and invoice for transportation reimbursement from the hospital. Amounts are recorded as a receivable when the Company is able to determine amounts receivable under these contracts and/or agreements based on information provided and collection is reasonably likely to occur. The Company continuously monitors its collections of receivables and its policy is to write off receivables when they are determined to be uncollectible. The Company has not incurred credit losses related to receivables. No allowance for doubtful accounts is recorded at December 31, 2014.
Concentrations of Risks
Seven health maintenance organizations (“HMOs”) accounted for 88% of the total capitation fee received for the year ended December 31, 2014. The loss of these HMO contracts would have an adverse impact on the operation of APC. However, management does not foresee the loss of these contracts in the near future.
F-75
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
Land, Property and Equipment, Net
Land is carried at cost and is not depreciated as it is considered to have an infinite useful life.
Property and equipment, including leasehold improvements, are carried at cost less accumulated depreciation and amortization. Depreciation is provided principally on the straight-line method over the estimated useful lives of the assets ranging from three to ten years. Leasehold improvements are amortized on a straight-line basis over the shorter of the lives of the respective leases or the expected useful lives of those improvements. Maintenance and repairs are charged to expense as incurred. Upon sale or retirement, the asset cost and related accumulated depreciation and amortization is removed from the accounts, and any related gain or loss is included in the determination of consolidated net income.
Fair Value Measurements
The Company’s consolidated financial instruments consist of cash and cash equivalents, fiduciary cash, restricted cash, investment in marketable securities, accounts receivable, accounts payable, certain accrued liabilities, and long-term debt. The carrying values of the current consolidated financial instruments are considered to be representative of their fair market value, due to the short maturity of these instruments. The carrying amount of the long-term debt approximates fair value as it bears interest at rates which approximates current market rates for debt with similar maturities and credit quality.
Financial Accounting Standards Board Accounting Standards Codification (“ASC”) 820, Fair Value Measurements and Disclosures, applies to all financial assets and financial liabilities that are measured and reported on a fair value basis and requires disclosure that establishes a framework for measuring fair value and expands disclosure about fair value measurements. ASC 820 establishes a valuation hierarchy for disclosures of the inputs to valuations used to measure fair value.
This hierarchy prioritizes the inputs into three broad levels as follows:
Level 1—Inputs are unadjusted quoted prices in active markets for identical assets or liabilities that can be accessed at the measurement date.
Level 2—Inputs include quoted prices for similar assets and liabilities in active markets, quoted prices for identical or similar assets or liabilities in markets that are not active, inputs other than quoted prices that are observable for the asset or liability (i.e., interest rates and yield curves), and inputs that are derived principally from or corroborated by observable market data by correlation or other means (market corroborated inputs).
Level 3—Unobservable inputs that reflect assumptions about what market participants would use in pricing the asset or liability. These inputs would be based on the best information available, including the Company’s own data.
Finite-Lived Intangibles and Long-Lived Assets
Intangible assets with finite lives include network/payor relationships and are stated at cost, less accumulated amortization and impairment losses. These intangible assets are amortized on a straight-line basis over their expected period of benefit.
F-76
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
Finite-lived and long-lived assets are reviewed for impairment whenever events or changes in circumstances indicate that the carrying amount of an asset may not be recoverable. If the expected future cash flows from the use of such assets (undiscounted and without interest charges) are less than the carrying value, a write-down would be recorded to reduce the carrying value of the asset to its estimated fair value. Fair value is determined based on appropriate valuation techniques. The Company determined that there were no impairments of its finite-lived intangible or long-lived assets during the periods presented.
Goodwill
Goodwill represents the difference between the purchase price of an acquired business and the fair value of the identifiable tangible and intangible net assets acquired. Goodwill is tested for impairment on an annual basis and whenever events or circumstances indicate that the carrying amount of such asset may not be recoverable.
Testing for impairment of goodwill is a two-step process. The first step requires the Company to compare the estimated fair value of its reporting unit with its respective carrying value. The Company has determined it has a single reporting unit. The Company established, and continues to evaluate, its reporting unit based on its internal reporting structure and defines such reporting unit at its operating segment level using a combination of valuation techniques.
If the fair value is less than the carrying value, goodwill is potentially impaired and the Company then completes the second step to measure the impairment loss, if any. The second step requires the calculation of the implied fair value of goodwill by deducting the fair value of all tangible and intangible net assets from the fair value of the reporting unit. If the implied fair value of goodwill is less than the carrying amount of enterprise goodwill, an impairment loss is recognized equal to the difference.
No impairment indicators were noted by the Company during the periods presented.
Medical Liabilities
The Company is responsible for integrated care that the associated physicians and contracted hospitals provide to its enrollees under risk-pool arrangements. The Company provides integrated care to health plan enrollees through a network of contracted providers under sub-capitation and direct patient service arrangements, company-operated clinics and staff physicians. Medical costs for professional and institutional services rendered by contracted providers are recorded as cost of services in the accompanying consolidated statements of operations. Costs for operating medical its ambulatory surgical center are included in general and administrative expense.
An estimate of amounts due to contracted physicians, hospitals, and other professional providers is included in medical liabilities in the accompanying consolidated balance sheets. Medical liabilities include claims reported as of the balance sheet date and estimates of incurred but not reported claims (“IBNR”). Such estimates are developed using actuarial methods and are based on many variables, including the utilization of health care services, historical payment patterns, cost trends, product mix, seasonality, changes in membership, and other factors. The estimation methods and the resulting reserves are periodically reviewed and updated. Many of the medical contracts are complex in nature and may be subject to differing interpretations regarding amounts due for the provision of various services. Such differing interpretations may not come to light until a substantial period of time has passed following the contract implementation.
F-77
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
Sign-On Bonus
Pursuant to the Exclusivity Amendment Agreement entered into between APC and certain primary care physicians in October 2014 (see Note 12), APC shall pay to the provider $25,000 sign-on bonus in three increments, the first by October 31, 2014, the second at the end of the sixth month of agreement term, and the third at the end of the 12th month of agreement term. APC capitalized an aggregate of $1,995,000 related to the sign-on bonus to be amortized over the contractual term of 5 years. During the year ended December 31, 2014, APC recorded amortization expense related to the sign-on bonus of $83,125. As of December 31, 2014, the net sign-on bonus balance was $1,911,875. The remaining balance is expected to be amortized as follows: $399,000 in 2015, $399,000 in 2017; $399,000 in 2018; $315,875 in 2019.
Revenue Recognition
Revenue consists of capitation revenue, risk pool settlements and incentives, and management fee income. Revenue is recorded in the period in which services are rendered. Revenue is principally derived from the provision of healthcare staffing services to patients within healthcare facilities. The form of billing and related risk of collection for such services may vary by customer. The following is a summary of the principal forms of the Company’s billing arrangements and how net revenue is recognized for each.
-Capitation revenue
Capitation revenue (net of capitation withheld to fund risk share deficits) is recognized in the month in which the Company is obligated to provide services. Minor ongoing adjustments to prior months’ capitation, primarily arising from contracted HMOs finalizing of monthly patient eligibility data for additions or subtractions of enrollees, are recognized in the month they are communicated to the Company. Managed care revenues of the Company consist primarily of capitated fees for medical services provided by the Company under a provider service agreement (“PSA”) or capitated arrangements directly made with various managed care providers including HMO’s and management service organizations (“MSOs”). Capitation revenue under the PSA and HMO contracts is prepaid monthly to the Company based on the number of enrollees electing the Company as their healthcare provider. Health plans and providers with higher acuity enrollees will receive more and those with lower acuity enrollees will receive less.
-Risk Pool Settlements and Bonuses
HMO contracts also include provisions to share in the risk for enrollee hospitalization, whereby the Company can earn additional incentive revenue or incur penalties based upon the utilization of hospital services. Typically, any shared risk deficits are not payable until and unless the Company generates future risk sharing surpluses, or if the HMO withholds a portion of the capitation revenue to fund any risk share deficits. At the termination of the HMO contract, any accumulated risk share deficit is typically extinguished. Due to the lack of access to information necessary to estimate the related costs, shared-risk amounts receivable from the HMOs are only recorded when such amounts are known. Risk pools for the prior contract years are generally final settled in the third or fourth quarter of the following fiscal year. The Company recorded a risk pool receivable in the amount of $11,113,954 as of December 31, 2014.
F-78
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
In addition to risk-sharing revenues, the Company also receives incentives to control member utilization and to promote quality care. These incentive programs track specific performance measures and calculate payments to the IPA based on these performance measures.
-Management Income
The Company provides claims processing and other administrative services for other IPAs. The Company receives management income for the services rendered. Management fees are calculated as a percentage of revenue under capitation contracts with various insurance companies.
Surgery Center Income
CDSC’s surgery center income is recorded in the period in which the services are rendered to the patients.
Fee-for-Service
Fee-for-service revenue represents revenue earned under contracts in which the Company bills and collects the professional component of charges for medical services rendered by our contracted physicians. Under the fee-for-service arrangements, the Company bills patients for services provided and receives payment from patients or their third-party payors. Fee-for-service revenue is reported net of contractual allowances and policy discounts. All services provided are expected to result in cash flows and are therefore reflected as net revenue in the consolidated statements of income. Fee-for-service revenue is recognized in the period in which the services are rendered to specific patients and reduced immediately for the estimated impact of contractual allowances in the case of those patients having third-party payor coverage. The recognition of net revenue (gross charges less contractual allowances) from such visits is dependent on such factors as proper completion of medical charts following a patient visit, the forwarding of such charts to the Company’s billing center for medical coding and entering into the Company’s billing system and the verification of each patient’s submission or representation at the time services are rendered as to the payor(s) responsible for payment of such services. Revenue is recorded based on the information known at the time of entering of such information into the Company’s billing systems as well as an estimate of the revenue associated with medical services.
Stop-Loss Provisions
Stop-loss insurance limits the cost of medical services for enrollees whose professional care costs exceed a specified level. Stop-loss insurance premiums are reported as medical expenses and insurance recoveries are reported as a reduction of related medical expenses. The Company is contingently liable to the extent that any insurer becomes unable to meet its contractual obligation. As of December 31, 2014, the liability balance for stop-loss provision was $0.
The Company has purchased stop-loss insurance, which will reimburse the Company for claims from service providers on a per enrollee basis. The specific retention amount per enrollee per policy period is $55,000 for professional coverage.
F-79
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
Income Taxes
Deferred income taxes are provided for temporary differences between financial and tax reporting in accordance with the liability method.
The Company utilizes ASC Topic 740, which requires the recognition of deferred tax assets and liabilities for the expected future tax consequences of events that have been included in the consolidated financial statements or tax returns. Under this method, deferred income taxes are recognized for the tax consequences in future years of differences between the tax basis of asset and liabilities and their financial reporting amounts at each period end based on enacted tax laws and statutory tax rates applicable to the periods in which the differences are expected to affect taxable income.
Valuation allowances are established, when necessary, to reduce deferred tax assets to the amount expected to be realized.
The Company adopted the provisions of ASC 740, which addresses the determination of whether tax benefits claimed or expected to be claimed on a tax return should be recorded in the consolidated financial statements. Under ASC 740, the Company may recognize the tax benefit from an uncertain tax position only if it is more likely than not that the tax benefit will be sustained on examination by the taxing authorities, based on the technical merits of the position. The tax benefits recognized in the consolidated financial statements from such a position should be measured based on the largest benefit that has a greater than fifty percent likelihood of being realized upon ultimate settlement. ASC 740 also provides guidance on derecognition, classification, interest and penalties on income taxes, accounting in interim periods and requires increased disclosures. At December 31, 2014, the Company did not have any uncertain tax position.
Investments in Other Entities
The Company accounts for certain investments using the equity method of accounting when it is determined that the investment provides the Company the ability to exercise significant influence, but not control, over the investee. Significant influence is generally deemed to exist if the Company has an ownership interest in the voting stock of the investee of between 20% and 50%, although other factors, such as representation on the investee’s Board of Directors, are considered in determining whether the equity method of accounting is appropriate. Under the equity method of accounting, the investment, originally recorded at cost, is adjusted to recognize our share of net earnings or losses of the investee and is recognized in the consolidated statements of operations in the caption “Income from equity method investments” and also is adjusted by contributions to and distributions from the investee.
Stock-based Compensation
Stock-based compensation is measured at the grant date based on the fair value of the award and is recognized as expense, net of estimated forfeitures, straight line over the requisite service period, which is generally the vesting period of the respective award.
Determining the fair value of stock-based awards at the grant date requires judgment. The company uses the Black-Scholes option pricing model to determine the fair value of stock-based awards. The determination of the grant-date fair value of options using an option pricing model is affected by a number of complex and subjective variables. These variables include the fair value of our common stock, the expected term of the awards, our expected stock price volatility, risk-free interest rates, and expected dividends, which are estimated as follows:
F-80
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
• Fair Value of Our Common Stock. Since we do not have the market closing price of our common stock as reported on the Stock Exchange market, the fair value of the common stock underlying the stock-based awards was determined by our board of directors.
• Expected Term. The expected term represents the period that our stock-based awards are expected to be outstanding. As we do not have sufficient historical experience for determining the expected term of the awards granted, we have based our estimate expected term on actual options granted on October 1, 2014. The company has not used the simplified method calculates the expected term as the average of the time-to-vesting and the contractual life, as this award contractually are not granted limited time to exercise their stock options (typically 30–90 days). Instead, it has adopted the time approach using remaining vesting period for the grant.
• Expected Volatility. As the company does not have a significant trading history for our common stock, the expected stock price volatility for our common stock was estimated by taking the average historic price volatility for industry peers based on daily price observations over a period equivalent to the expected term of the awards. It has not relied on implied volatilities of traded options in our industry peers’ common stock because the volume of activity was relatively low. The company intends to continue to consistently apply this process using the same or similar public companies.
• Risk-free Rate. The risk-free interest rate is based on the yields of U.S. Treasury securities with maturities similar to the expected term of the stock-based awards.
• Dividend Yield. The company has not declared or paid any cash dividend and a dividend yield of 0% is used in 2014.
In addition to the assumptions used in the Black-Scholes option-pricing model, the company must also estimate a forfeiture rate to calculate the stock-based compensation expense for our awards. The forfeiture rate is based on an analysis of our actual forfeitures. The company will continue to evaluate the appropriateness of the forfeiture rate based on actual forfeiture experience, analysis of members’ turnover, and other factors.
The company has also used the criteria which are complex (outlined in ASC 718-10-25-6 through 25-19) for determining whether an award should be classified as a liability or as equity. In order for an award to be classified as equity, it should possess a vesting condition and fulfill certain other requirements. The vesting conditions included in an equity classified award will affect the way companies recognize compensation cost. On the other hand, ASC 718 describes certain types of awards that should be classified as a liability, although certain exceptions exist; including an award with conditions or other features that are indexed to something other than a market, performance, or service condition; and share award with a repurchase feature that permits an employee to avoid, for a reasonable period (at least six months) after the stock issuance, the risks and rewards that are normally associated with stock ownership.
Non-Controlling Interests
The Company consolidates entities in which the Company has a controlling financial interest. The Company consolidates subsidiaries in which the Company hold, directly or indirectly, more than 50% of the voting rights, and variable interest entities (VIEs) in which the Company is the primary beneficiary. Non-controlling interests represent third-party equity ownership interests in the Company’s consolidated entities.
F-81
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
Based on the Shareholder Agreement for both NMM and APC, in the event of election disqualifying event, as defined in the agreement, NMM and APC could be required to repurchase the shares from the shareholder based on the triggers outlined in Section 4.1 of the Shareholder Agreement. The triggers that could cause NMM to redeem the shares (redemption feature) is not solely within the control of NMM or APC. As the redemption feature of the shares is not solely within the control of NMM, the common stock and additional paid-in capital of NMM has been classified as mezzanine or temporary equity as redeemable common stock. In addition, as the redemption feature of the shares is not solely within the control of APC, the equity transactions of APC do not qualify as permanent equity and has been classified as mezzanine or temporary equity, accordingly, NMM recognizes noncontrolling interests as mezzanine equity in the consolidated financial statements separate from NMM’s equity. Noncontrolling interests’ partners have less than 50% share of voting rights at any one of the subsidiary or VIE companies. The amount of net income attributable to noncontrolling interests is included in consolidated net income on the face of the consolidated statements of income.
Recent Accounting Pronouncements
In May 2014, the FASB and the International Accounting Standards Board (“IASB”) jointly issued a new revenue recognition standard, Accounting Standards Update (“ASU”) No. 2014-09, Revenue From Contracts with Customers, that will supersede nearly all existing revenue recognition guidance under GAAP. The revenue recognition standard will allow for the recognition of revenue when a company transfers promised goods or services to customers in an amount that reflects the consideration to which the company expects to be entitled in exchange for those goods or services. The standard permits the use of either a full retrospective or retrospective with cumulative effect transition method.
In August 2014, the FASB issued ASU No. 2014-15, Presentation of Financial Statements—Going Concern, which will require an entity’s management to assess, for each annual and interim period, whether there is substantial doubt about the entity’s ability to continue as a going concern within one year of the consolidated financial statement issuance date. The definition of substantial doubt within the new standard incorporates a likelihood threshold of “probable” similar to the use of that term under current GAAP for loss contingencies. Certain disclosures will be required if conditions give rise to substantial doubt. The guidance will be effective for the Company beginning with fiscal 2017. Early adoption is permitted. The Company does not anticipate that this guidance will materially impact its consolidated financial statements and related disclosures.
In March 2016, the FASB issued Accounting Standard Update 2016-09 (ASU 2016-09) Compensation - Stock Compensation, in order to simplify certain aspects of the accounting for share-based payment award transactions, including income tax consequences, classification of awards as either equity or liability, classification of excess tax benefits, and taxes withheld and paid on employee stock award vesting on the statement of cash flows. ASU 2016-09 requires that companies elect to account for forfeitures based on an estimate of the number of awards for which the requisite service period will not be rendered or to account for forfeitures as they occur. ASU 2016-09 is effective for the interim and annual periods ending after December 15, 2016. Early adoption is permitted. The Company is beginning to evaluate the impact this standard will have on our consolidated financial statements and related disclosures.
F-82
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
Note 3 - Acquisitions
Pacific Independent Physician Association, a Medical Group, Inc.
On October 1, 2014, APC merged with Pacific Independent Physician Association, A Medical Group Inc., a California corporation (“PIPA”) pursuant to the Agreement and Plan of Reorganization dated July 18, 2014 (“Merger Agreement”) with APC being the surviving entity.
APC issued 52,625,406 shares of common stock valued at $86,832,000 or $1.65 per share to the PIPA shareholders to acquire all of the assets, liabilities, and operations of PIPA. Transaction costs are not included as a component of consideration transferred and were expensed as incurred. The related transaction costs expensed for the year ended December 31, 2014 was minimal and are included in general and administrative expenses in the consolidated statements of operations.
The Company accounted for the acquisition as a business combination using the acquisition method of accounting which requires, among other things, that assets acquired and liabilities assumed be recognized at their fair values as of the purchase date and be recorded on the balance sheet. Under the acquisition method of accounting, the total purchase price was allocated to the underlying tangible and intangible assets acquired and liabilities assumed based on their respective fair values, with the remainder allocated to goodwill. Goodwill is not deductible for tax purposes. The final allocation of the total purchase price to the net assets acquired and liabilities assumed and included in the Company’s consolidated balance sheet at December 31, 2014 is as follows:
| Cash and cash equivalents | $ | 5,560,662 | ||
| Accounts receivable | 5,871,172 | |||
| Other current assets | 43,084 | |||
| Property, plant and equipment | 5,657,420 | |||
| Intangible asset | 74,054,000 | |||
| Other asset | 589,810 | |||
| Goodwill | 38,295,814 | |||
| Total asset acquired | 130,071,962 | |||
| Accounts payable | (253,932 | ) | ||
| Accrued liabilities | (11,214,990 | ) | ||
| Deferred tax liabilities | (30,230,153 | ) | ||
| Loan payable | (1,540,887 | ) | ||
| Total liabilities assumed | (43,239,962 | ) | ||
| Total purchase price | $ | 86,832,000 |
F-83
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
In the view of management, the goodwill recorded in the transaction reflects the Company’s future cash flow expectations and its market position in the healthcare industry. The intangible asset includes $74,054,000 recognized for the fair value of the network/payor relationships that has an approximate useful life of 15 years. The valuation of the intangible asset acquired was based on third-party valuations, management’s estimates, available information, and reasonable and supportable assumptions, are considered Level 3 measurements. The fair value of the network/payor relationship was estimated utilizing the income and market valuation approaches.
Note 4 – Land, Property and Equipment, Net
Land, property and equipment, net consisted of:
| 2014 | ||||
| Land | $ | 3,300,000 | ||
| Building | 2,339,799 | |||
| Computer software | 1,111,164 | |||
| Furniture and equipment | 5,584,825 | |||
| Leasehold improvements | 1,076,971 | |||
| 13,412,759 | ||||
| Less accumulated depreciation and amortization | (5,835,342 | ) | ||
| Land Property and Equipment, Net | $ | 7,577,417 | ||
Depreciation and amortization expense of property and equipment was $623,873 for year ended December 31, 2014.
Note 5 - Intangible Assets, Net
At December 31, 2014, intangible assets, net consisted of the following:
| Amortization Period |
Gross Amounts |
Accumulated Amortization |
Net Amount | |||||||||||
| Network/payor relationships | 15 Years | $ | 74,054,000 | $ | 660,436 | $ | 73,393,564 | |||||||
Amortization expense related to the intangible assets totaled $660,436 for year ended December 31, 2014.
F-84
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
Future amortization expense is as follows for each of the five following year ending December 31:
| 2015 | $ | 4,516,527 | ||
| 2016 | 9,949,142 | |||
| 2017 | 9,075,663 | |||
| 2018 | 7,903,922 | |||
| 2019 | 6,881,312 | |||
| Thereafter | 35,066,998 | |||
| Total | $ | 73,393,564 |
Note 6 – Goodwill
The following is a summary of goodwill activity:
| Balance at January 1, 2014 | $ | 316,610 | ||
| Acquisition of PIPA | 38,295,814 | |||
| Balance at December 31, 2014 | $ | 38,612,424 |
Note 7 - Investment in Other Entities
LaSalle Medical Associates
During 2012, the Company invested $5,000,000 for a 25% interest in LaSalle Medical Associates’ IPA line of business (“LMA”). The Company accounted for its investment in LMA under the equity method of accounting as the Company had the ability to exercise significant influence over LMA’s operations, but not control over LMA’s operations. The Company recorded income from this investment of $2,072,470 and has an investment balance of $7,160,868 at December 31, 2014.
Note 8 - Accounts Payable and Accrued Expenses
Accounts payable and accrued expenses consisted of the following:
| December 31, 2014 | ||||
| Accounts payable | $ | 14,422,767 | ||
| Accrued compensation | 730,360 | |||
| Accrued other | 2,725,393 | |||
| $ | 17,878,520 | |||
F-85
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
Note 9 - Medical Liabilities
Medical liabilities consisted of the following:
| December 31, 2014 | ||||
| Balance, beginning of period | $ | 5,057,724 | ||
| Incurred health care costs: | 38,681,583 | |||
| Claims paid | (36,167,170 | ) | ||
| Adjustments | 4,320,608 | |||
| Balance, end of period | $ | 11,892,745 | ||
Note 10 - Notes and Lines of Credit Payable
Notes payable consisted of the following:
| December 31, 2014 | ||||
| Note payable bearing interest at 4.88%, final maturity January 13, 2034 | $ | 1,528,478 | ||
| Less current maturities | 45,183 | |||
| Long-term debt, net of current maturities | $ | 1,483,295 | ||
On January 13, 2014, the Company entered into a mortgage loan agreement with a bank in the amount of $1,575,000. This Note is guaranteed by one of the Company’s members, Theresa C. Tseng. Interest on the Note is 4.63%. The note requires the Company to make 239 monthly payments of $10,132 commencing February 13, 2014 and maturing on January 13, 2034.
Current and future maturities of the debt are:
| 2015 | $ | 45,183 | ||
| 2016 | 121,584 | |||
| 2017 | 121,584 | |||
| 2018 | 121,584 | |||
| 2019 | 121,584 | |||
| Thereafter | 996,959 | |||
| Total | $ | 1,528,478 |
The loan was collateralized by both the building and the rents due the Company on the same building.
The loan agreement contains certain affirmative covenants and as of December 31, 2014, the Company was in compliance with all covenants.
Interest expense on the note payable totaled $63,790 for the year ended December 31, 2014
On February 4, 2016, this loan was repaid in full. In connection with this repayment, the Company incurred a prepayment penalty of $44,200.
F-86
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
Lines of Credit
NMM has a $2,000,000 revolving line of credit with a bank which matured on April 9, 2016. The line of credit was guaranteed by eight shareholders who are also members of the Company’s board of directors. The line of credit bore interest at variable rates based on the WSJ prime rate which was 3.375% at December 31, 2014.
APC has a $3,000,000 revolving line of credit with a bank which matured on April 22, 2016.
The line of credit was guaranteed by eight shareholders who are also members of the Company’s board of directors. The line of credit bore interest at variable rates based on the WSJ prime rate which was 3.375% at December 31, 2014. A standby letter of credit in the amount of $105,016 is issued as a contingency for potential unpaid claims by beneficiaries, Aetna and Cigna, as required by the HMO.
There were no borrowings outstanding against the lines of credit at December 31, 2014.
Note 11 – Income Taxes
Income tax expense from continuing operations consists of the following for the year ended December 31:
| 2014 | ||||
| Current | ||||
| Federal | $ | 1,997,031 | ||
| State | 544,353 | |||
| 2,541,384 | ||||
| Deferred | ||||
| Federal | 278,429 | |||
| State | 113,498 | |||
| 391,927 | ||||
| Total income tax expense | $ | 2,933,311 | ||
F-87
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
The Company uses the liability method of accounting income taxes as set forth in ASC 740. Under the liability method, deferred taxes are determined based on differences between the financial statement and tax bases of assets and liabilities using enacted tax rates. As of December 31, 2014, the Company does not have any federal or California tax net operating loss carryforwards.
Significant components of the Company’s deferred assets as of December 31, 2014 are shown below. The Company’s effective tax rate is different from the federal statutory rate of 34% due primarily to state income taxes.
Deferred tax assets (liabilities) consist of the following at December 31, 2014:
| 2014 | ||||
| Deferred tax assets (liabilities): | ||||
| State taxes | $ | 182,768 | ||
| Accrued payroll and related costs | 94,220 | |||
| Property and equipment | (1,108,583 | ) | ||
| Acquired intangible assets | (29,235,886 | ) | ||
| Others | (1,076,444 | ) | ||
| Net deferred tax assets (liabilities) before valuation allowance | (31,143,925 | ) | ||
| Valuation Allowance | - | |||
| Net deferred tax liabilities | $ | (31,143,925 | ) | |
The provision for income taxes differs from the amount computed by applying the federal income tax rate as follow for the year ended December 31, 2014:
| 2014 | ||||
| Tax provision at U.S. Federal statutory rates | 34.0 | % | ||
| State income taxes net of federal benefit | -4.1 | % | ||
| Non-deductible permanent items | -61.1 | % | ||
| Non-taxable entities | 3.5 | % | ||
| Other | 0.50 | % | ||
| Effective income tax rate | -27.2 | % | ||
F-88
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
As of December 31, 2014, the Company does not have any unrecognized tax benefit related to various federal and state income tax matters. The Company will recognize accrued interest and penalties related to unrecognized tax benefit in income tax expense.
The Company is subjected to US federal income tax as well as income tax of California. The Company and its subsidiaries’ state income tax returns are open to audit under the statute of limitations for the year ended December 31, 2012 thru 2014. The Company does not anticipate material unrecognized tax benefits within the next 12 months.
Note 12 - Mezzanine and Shareholders’ Equity
NMM:
Stock Split
On June 30, 2015, NMM filed an amendment to its Articles of Incorporation to effectuate a 3.192-for-1 stock split.
On July 28, 2015, NMM filed an amendment to its Articles of Incorporation to effectuate a 3-for-1 stock split.
All share and per share amounts relating to the common stock and stock options to purchase common stock, including the respective exercise prices of each such option, included in the consolidated financial statements and footnotes have been retroactively adjusted to reflect the increased number of shares resulting from this action. The par value and the number of authorized, but unissued, shares were not adjusted as a result of the stock split. No fractional shares were issued following the stock split and APC has paid cash in lieu of any fractional shares resulting from the stock split.
Authorized Stock
All common stock is non-transferable and is governed by the stockholders’ agreement.
At December 31, 2014, the Company was authorized to issue up to 300,000,000 shares of common stock. The Company is required to reserve and keep available out of the authorized but unissued shares of common stock such number of shares sufficient to effect the exercise of all outstanding options granted and available for grant under the Company’s Exclusivity Amendment Agreement and shares offered to providers or members to purchase from time to time. The number of shares of common stock reserved for these purposes is as follows:
| December 31, 2014 | ||||
| Shares of common stock issued and outstanding | 175,703,886 | |||
| Unvested October 1, 2014 stock options granted (unadjusted) | 4,025,250 | |||
| Total | 179,729,136 | |||
Shares Issuance
In 2014, the Company repurchased 229,824 shares at approximately $0.10 (post-split) per share from one shareholder.
F-89
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
The Company issued a repayment of capital to shareholders amounting to $2,568,772.
APC:
Stock Split
During 2014, APC filed an amendment to its Articles of Incorporation to effectuate a 2-for 1 stock split.
On July 28, 2015, APC filed an amendment to its Articles of Incorporation to effectuate a 3-for-1 stock split.
All share and per share amounts relating to the common stock and stock options to purchase common stock, including the respective exercise prices of each such option, included in the consolidated financial statements and footnotes have been retroactively adjusted to reflect the increased number of shares resulting from this action. The par value and the number of authorized, but unissued, shares were not adjusted as a result of the stock split. No fractional shares were issued following the stock split and APC has paid cash in lieu of any fractional shares resulting from the stock split.
Authorized Stock
All common stock is non-transferable and is governed by the stockholders’ agreement.
At December 31, 2014, the Company was authorized to issue up to 500,000,000 shares of common stock. The Company is required to reserve and keep available out of the authorized but unissued shares of common stock such number of shares sufficient to effect the exercise of all outstanding options granted and available for grant under the Company’s Exclusivity Amendment Agreement and shares offered to providers or members to purchase from time to time. The number of shares of common stock reserved for these purposes is as follows:
| December 31, 2014 | ||||
| Shares of common stock issued and outstanding | 315,752,436 | |||
| Unvested October 1, 2014 stock options granted (unadjusted) | 4,025,250 | |||
| Total | 319,777,686 | |||
Shares Issuance
During 2014, APC repurchased 1,970,400 at approximately $0.17 per share (post split) from several shareholders for a total consideration of $328,400.
During 2014, APC issued 7,698,00 shares (15,396,000 post-split shares) at $1 (approximately $0.17 post-split) in exchange for consideration of $2,566,000 from several shareholders. However, these issuances of shares are deemed issued below market value, which is at approximately, $3.32 per share (approximately $0.55 post-split). Had these issuances been issued at fair market value, total consideration should have been $8,519,120. Accordingly, the difference between actual share issuances at cost and fair market value of $5,953,120 is treated as share-based compensation and included in general and administrative expenses in the accompanying statement of operations.
F-90
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
During 2014, several shareholders were awarded shares related to the PIPA merger of 13,120,209 shares (26,240,418 post-split) at $0.25 per share (approximately $0.04 post-split) for a total consideration of $1,093,351. However, these issuances of shares are deemed issued below market value, which is at approximately, $3.30 per share (approximately $0.55 post-split). Had these issuances been issued at fair market value, total consideration should have been $14,432,230. Accordingly, the difference between actual share issuances at cost and fair market value of $13,338,879 is treated as share-based compensation and included in general and administrative expenses in the accompanying statement of operations.
On Oct 1, 2014, APC issued 157,876,218 shares of common stock valued at approximately $86,832,000 to the PIPA shareholders to acquire all of the assets, liabilities and operation of PIPA (See Note 3).
During 2014, APC issued repayment of capital to the shareholders amounting to $3,947,452.
Stock Options Issued Under NMM Primary Care Physician Agreements
On October 1, 2014, APC, entered into an Exclusivity Amendment as part of the Primary Care Physician Agreement to issue one lot of Network Medical Management Inc.’s and another lot of APC’s shares as stock options to medical providers where they agree to give exclusivity for health enrollees to the Company for $25,000 sign-on bonus (or $15,000 if he or she is already a preferred provider). In addition, provider is incentivized by issuance of share options for increasing enrollees in Commercial, Medicare and Medi-Cal members between the date of agreement to May 1, 2015. Share options will be priced at fifty cents ($0.50) per share ($0.167 post split) and providers can exercise anytime between August 1, 2015 and October 1, 2019. If agreement is terminated with or without cause, the sign-on bonus and any capitation payment made under this term of agreements shall be fully repaid. Any share options that has been exercised will be bought back at the original purchased price. On December 31, 2014, based on the terms of this agreement, the Company estimated that the medical providers were eligible for 1,341,750 options in NMM and APC respectively.
The stock options were accounted for at their fair value, as determined by the Black-Scholes valuation model, using the following assumptions:
| NMM | APC | |||||||
| Expected volatility | 62.9 | % | 62.9 | % | ||||
| Expected life | 4.75 years | 4.75 years | ||||||
| Risk-free interest rate | 1.65 | % | 1.65 | % | ||||
| Dividend yield | 0 | % | 0 | % | ||||
| Market value of common stock | $ | 1.75 | $ | 1.78 | * |
F-91
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
NMM’s stock option activity in relation to shares issued to APC providers is summarized below:
| Weighted- Average |
||||||||||||||||
| Weighted-Average Per Share |
Remaining Life |
Aggregate | ||||||||||||||
| Shares | Exercise Price | (Years) | Intrinsic Value | |||||||||||||
| Balance, January 1, 2014 | - | $ | - | - | $ | - | ||||||||||
| Granted | 7,963,950 | 0.167 | 4.75 | 167,003 | ||||||||||||
| Cancelled/expired | - | - | - | - | ||||||||||||
| Exercised | - | - | - | - | ||||||||||||
| Balance, December 31, 2014 | 7,963,950 | $ | 0.167 | 4.75 | $ | 167,003 | ||||||||||
APC’s stock option activity in relation to shares issued to APC providers is summarized below:
| Weighted- Average |
||||||||||||||||
| Weighted-Average Per Share |
Remaining Life |
Aggregate | ||||||||||||||
| Shares | Exercise Price | (Years) | Intrinsic Value | |||||||||||||
| Balance, January 1, 2014 | - | $ | - | - | $ | - | ||||||||||
| Granted | 7,963,950 | 0.167 | 4.75 | 3,395,297 | ||||||||||||
| Cancelled/expired | - | - | - | - | ||||||||||||
| Exercised | - | - | - | - | ||||||||||||
| Balance, December 31, 2014 | 7,963,950 | $ | 0.167 | 4.75 | $ | 3,395,297 | ||||||||||
As of December 31, 2014, NMM and APC’s total unrecognized compensation costs related to non-vested stock-based compensation arrangements granted to those under the Company’s Exclusivity Amendment Agreement for common stock options grant on October 1, 2014 amounted to $1.76 million and $1.80 million, respectively.
The weighted-average period of years expected to recognize these compensation costs in NMM and APC as at December 2014 was 4.75 years.
Stock-based compensation expenses of NMM and APC related to common stock option awards recognized over their respective vesting periods charged to APC totaled $179,870 were as follows:
F-92
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
| Year Ended December 31. 2014 | ||||||||
| NMM | APC | |||||||
| Stock-based compensation expense: | ||||||||
| Cost of services | $ | 89,099 | $ | 90,771 | ||||
| General and administrative | - | - | ||||||
| Total | $ | 89,099 | $ | 90,771 | ||||
Note 13 - Commitments and Contingencies
Operating Leases
The Company leases office space under certain non-cancelable operating lease agreements. Rental expense for the year ended December 31, 2014 was $896,376. As of December 31, 2014, the future minimum rental payments under non-cancelable operating lease were as follows:
| 2015 | $ | 896,376 | ||
| 2016 | 1,879,513 | |||
| 2017 | 2,146,763 | |||
| 2018 | 2,116,922 | |||
| 2019 | 2,136,182 | |||
| Thereafter | 2,871,513 | |||
| Total | $ | 12,047,269 |
Regulatory Matters
Laws and regulations governing the Medicare program and healthcare generally are complex and subject to interpretation. The Company believes that it is in compliance with all applicable laws and regulations and is not aware of any pending or threatened investigations involving allegations of potential wrongdoing. While no such regulatory inquiries have been made, compliance with such laws and regulations can be subject to future government review and interpretation as well as significant regulatory action including fines, penalties, and exclusion from the Medicare and Medi-Cal programs.
As a risk-bearing organization, the Company is required to follow regulations of the California Department of Managed Health Care (“DMHC”). The Company must comply with a minimum working capital requirement, Tangible Net Equity (“TNE”) requirement, cash-to-claims ratio and claims payment requirements prescribed by the DMHC. TNE is defined as net assets less intangibles, less non-allowable assets (which include amounts due from affiliates), plus subordinated obligations. At December 31, 2014, the Company was in compliance with these regulations.
Many of the Company's payer and provider contracts are complex in nature and may be subject to differing interpretations regarding amounts due for the provision of medical services. Such differing interpretations may not come to light until a substantial period of time has passed following contract implementation. Liabilities for claims disputes are recorded when the loss is probable and can be estimated. Any adjustments to reserves are reflected in current operations.
F-93
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
Legislation and HIPAA
The healthcare industry is subject to numerous laws and regulations of federal, state and local governments. These laws and regulations include, but are not necessarily limited to, matters such as licensure, accreditation, government healthcare program participation requirements, reimbursement for patient services, and Medicare and Medicaid fraud and abuse. Government activity has continued with respect to investigations and allegations concerning possible violations of fraud and abuse statutes and regulations by healthcare providers. Violations of these laws and regulations could result in expulsion from government healthcare programs together with the imposition of significant fines and penalties, as well as significant repayments for patient services previously billed.
The Company believes that it is in compliance with fraud and abuse regulations as well as other applicable government laws and regulations. Compliance with such laws and regulations can be subject to future government review and interpretation as well as regulatory actions unknown or unasserted at this time.
The Health Insurance Portability and Accountability Act (“HIPAA”) assures health insurance portability, reduces healthcare fraud and abuse, guarantees security and privacy of health information, and enforces standards for health information. The Health Information Technology for Economic and Clinical Health Act (“HITECH Act”) expanded upon HIPAA in a number of ways, including establishing notification requirements for certain breaches of protected health information. In addition to these federal rules, California has also developed strict standards for the privacy and security of health information as well as for reporting certain violations and breaches. The Company may be subject to significant fines and penalties if found not to be compliant with these state or federal provisions.
Affordable Care Act
The Patient Protection and Affordable Care Act (“PPACA”) will substantially reform the United States health care system. The legislation impacts multiple aspects of the health care system, including many provisions that change payments from Medicare, Medicaid and insurance companies. Starting in 2014, the legislation required the establishment of health insurance exchanges, which will provide individuals without employer-provided health care coverage the opportunity to purchase insurance. It is anticipated that some employers currently offering insurance to employees will opt to have employees seek insurance coverage through the insurance exchanges. It is possible that the reimbursement rates paid by insurers participating in the insurance exchanges may be substantially different than rates paid under current health insurance products. Another significant component of the PPACA is the expansion of the Medicaid program to a wide range of newly eligible individuals. In anticipation of this expansion, payments under certain existing programs, such as Medicare disproportionate share, will be substantially decreased. Each state’s participation in an expanded Medicaid program is optional.
Litigation
The Company is involved from time to time in routine legal matters incidental to its business. In the opinion of the Management, resolution of such matters is not expected to have a material effect on its financial position or results of operations.
F-94
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
Liability Insurance
The Company believes that the Company’s insurance coverage is appropriate based upon the Company’s claims experience and the nature and risks of the Company’s business. In addition to the known incidents that have resulted in the assertion of claims, the Company cannot be certain that the Company’s insurance coverage will be adequate to cover liabilities arising out of claims asserted against the Company, the Company’s affiliated professional organizations or the Company’s affiliated hospitalists in the future where the outcomes of such claims are unfavorable. The Company believes that the ultimate resolution of all pending claims, including liabilities in excess of the Company’s insurance coverage, will not have a material adverse effect on the Company’s financial position, results of operations or cash flows; however, there can be no assurance that future claims will not have such a material adverse effect on the Company’s business. Although the Company currently maintains liability insurance policies on a claims-made basis, which are intended to cover malpractice liability and certain other claims, the coverage must be renewed annually, and may not continue to be available to the Company in future years at acceptable costs, and on favorable terms.
Note 14 – Employee Benefit Plan
NMM has a qualified 401(k) plan which covers substantially all employees who have completed at least six months of service and meet minimum age requirements. Participants may contribute a portion of their compensation to the plan, up to the maximum amount permitted under Section 401(k) of the Internal Revenue Code. Participants become fully vested after six years of service. The Company matched a portion of the participants' contributions. The Company's matching contribution for the year ended December 31, 2014 was $38,920.
Note 15 - Related Party Transactions
During the year, APC paid approximately $3.8 million to 13 medical service providers which are owned by board members or shareholders with greater than 5% ownership. These payments are related to the medical service provided in the ordinary course of business.
During the years, APC paid approximately $1.8 million to AMG, Inc. for services as a provider. AMG Inc. shares common ownership with certain board members of APC.
During the year, NMM paid approximately $710,000 to Medical Property Partners (“MPP”) for office lease. MPP shares common ownership with certain board members of NMM.
During the year ended December 31, 2014, NMM received $9,386,883 in management fees from LaSalle Medical Associates, which is accounted for under the equity method based on 25% equity ownership interest held by APC (see Note 7)
F-95
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
Note 16 - Subsequent Events
The Company has evaluated subsequent events through April 30, 2017, the date the accompanying consolidated financial statements were available to be issued, and determined that no subsequent events have occurred that would require recognition in the consolidated financial statements or disclosure in the notes thereto, other than as disclosed in the accompanying notes to the consolidated financial statements.
Merger Transaction
PIPA MSO, Inc.
On July 1, 2015, NMM merged with PIPA (“PIPA”) MSO, Inc. (“PIPA MSO”), a California corporation with NMM being the surviving entity. PIPA MSO was organized for the purpose of providing management services to medical groups and IPAs. The management service covers billing, collection, accounting, administrative, non-physician personnel staffing, and marketing. NMM acquired the operational and management processes associated with providing management services to medical groups and IPA's.
NMM issued 157,876,218 shares of common stock valued at approximately $57,887,947 ($0.37 per share, which is based on management’s evaluation of the share price) to the PIPA MSO shareholders (representing approximately 44% of the issued and outstanding shares of NMM) to acquire all of the assets, liabilities, and operations of PIPA MSO. There was no cash consideration in this transaction. Transaction costs are not included as a component of consideration transferred and were expensed as incurred, which were minimal.
The Company accounted for the acquisition as a business combination using the acquisition method of accounting which requires, among other things, that assets acquired and liabilities assumed be recognized at their fair values as of the acquisition date and be recorded on the balance sheet. Under the acquisition method of accounting, the total purchase price was allocated to the underlying tangible and intangible assets acquired and liabilities assumed based on their respective fair values, with the remainder allocated to goodwill. Goodwill is not deductible for tax purposes.
The final allocation of the total purchase price to the net assets acquired and liabilities assumed is as follows:
| Cash and cash equivalents | $ | 576,480 | ||
| Other current assets | 7,392 | |||
| Identifiable intangible asset – management contract | 22,832,000 | |||
| Goodwill | 44,321,086 | |||
| Total assets acquired | 67,736,958 | |||
| Accounts payable and accrued liabilities | (545,831 | ) | ||
| Deferred tax liabilities | (9,303,127 | ) | ||
| Total liabilities assumed | (9,849,011 | |||
| Net assets acquired | $ | 57,887,947 |
F-96
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
In the view of management, the goodwill recorded in the transaction reflects the Company’s future cash flow expectations and its market position in the healthcare industry. The intangible asset includes $22,832,000 recognized for the fair value of the management contracts that have an approximate useful life of 15 years. The valuation of the management contract acquired was based on management’s evaluation, management’s estimates, available information, and reasonable and supportable assumptions, and are considered Level 3 measurements. The fair value of the management contract was estimated utilizing the income and market valuation approaches.
Physicians Healthways Medical Corporation
On April 1, 2015, APC merged with Physicians Healthways Medical Corporation (“PHW”), a California professional corporation, with APC being the surviving entity.
APC issued 60,714,750 shares of common stock valued at approximately $37,238,000 to the PHW shareholders. Per management’s evaluation, which utilized the income and market approaches, the estimated fair value of the APC common stock issued as consideration for the transaction was $37,238,000.
APC acquired intangible assets related to the network/payor relationships (approximately 58,000 health plan members of the PHW Independent Physicians Association and its Physician Members). Transaction costs are not included as a component of consideration transferred and were expensed as incurred, which were minimal and are included in general and administrative expenses in the accompanying consolidated statements of operations.
The Company accounted for the acquisition as a business combination using the acquisition method of accounting which requires, among other things, that assets acquired and liabilities assumed be recognized at their fair values as of the acquisition date and be recorded on the balance sheet. Under the acquisition method of accounting, the total purchase price was allocated to the intangible assets acquired with the remainder allocated to goodwill. Goodwill is not deductible for tax purposes. The final allocation of the total purchase price to the net assets acquired is summarized as follows:
| Identifiable intangible asset - network/payor relationships | $ | 32,606,000 | ||
| Goodwill | 17,917,634 | |||
| Total assets acquired | 50,523,634 | |||
| Deferred tax liability | (13,285,634 | ) | ||
| Total liabilities assumed | (13,285,634 | ) | ||
| Net assets acquired | $ | 37,238,000 |
F-97
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
In the view of management, the goodwill recorded in the transaction reflects the Company’s future cash flow expectations and its market position in the healthcare industry. The intangible asset includes $32,606,000 recognized for the fair value of the network/payor relationships that has an approximate useful life of 15 years. The valuation of the network/payor relationships acquired was based on management’s evaluation, management’s estimates, available information, and reasonable and supportable assumptions, and are considered Level 3 measurements. The fair value of the network/payor relationships was estimated utilizing the income and market valuation approaches.
APCN-ACO and ACO Acquisition Corporation
On November 11, 2015, NMM, ACO Acquisition Corporation, and APCN-ACO entered into a reorganization agreement whereby ACO Acquisition Corporation, a newly organized entity which NMM is its sole shareholder, will merge with APCN-ACO, effective on January 8, 2016 (date of filing of merger agreement with the California Secretary of State). APCN-ACO operates an accountable care organization (“ACO”), as defined under the Medicare Shares Savings Program (“MSSP”), which is comprised of the ACO’s network of independent medical practices. The primary reason for the business combination was for NMM to acquire the member relationships of APCN-ACO.
Immediately following the effective date, NMM became the sole shareholder of APCN-ACO. On the effective date, each share of APCN-ACO’s common stock issued and outstanding immediately prior to the effective date, was converted at 0.6 of one fully paid and nonassessable share(s) of common stock of NMM, immediately following which, each one share of common stock of ACO Acquisition Corporation was converted into and became one fully paid and nonassessable share of APCN-ACO’s common stock. As a result of the merger transaction, all of APCN-ACO’s shares were converted into 7,500,000 shares of NMM common stock.
All of APCN-ACO’s right, title and interest in and to all of its assets as of the effective date were included as part of the merger, including, without limitation, all of the following assets: (i) 75% of the issued and outstanding equity interests of 99 Medical Equipment Healthcare Supplies & Wheelchair Center (“99 DME”); (ii) 25% of the issued and outstanding equity interests of Allegiance Home Health, Inc.; and (iii) 5% economic interest in Pacific Medical Imaging & Oncology Center, Inc. (“PMIOC”). 99 DME is a medical equipment store that specializes in the retail sale of medical supplies and mobility equipment. On January 8, 2016, APCN-ACO purchased the remaining 25% interest in 99 DME for $12,500, resulting in APCN-ACO having 100% ownership of the issued and outstanding equity interests of 99 DME. Allegiance Home Health, Inc. is a California Corporation that engages in providing skilling nursing, physical therapy, speech pathology, medical social worker and home health aide. See Note 7 for further information regarding PMIOC.
NMM issued 7,500,000 shares of common stock to the APCN-ACO shareholders, with a fair value of $3,075,000. Based on the Company’s valuation, which utilized the income – discounted cash flow and market approaches, the estimated fair value of the NMM common stock issued as consideration for the transaction was $0.41 per share. Transaction costs are not included as a component of consideration transferred and were expensed as incurred, which were minimal.
The Company accounted for the acquisition as a business combination using the acquisition method of accounting which requires, among other things, that assets acquired and liabilities assumed be recognized at their fair values as of the acquisition date and be recorded on the consolidated balance sheet. Under the acquisition method of accounting, the total purchase consideration was allocated to the intangible assets acquired with the remainder allocated to goodwill. Goodwill is not deductible for tax purposes.
F-98
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
The final allocation of the total purchase price to the net assets acquired is summarized as follows:
| Investment in other entities – cost method | $ | 25,000 | ||
| Identifiable intangible asset – member relationships | $ | 1,738,000 | ||
| Goodwill | 1,679,849 | |||
| Total assets acquired | 3,442,849 | |||
| Deferred tax liability | (367,849 | ) | ||
| Total liabilities assumed | (367,849 | ) | ||
| Net assets acquired | $ | 3,075,000 |
ACO Acquisition Corporation #2, and Allied Physicians ACO, LLC
On December 18, 2016, NMM, ACO Acquisition Corporation #2, and Allied Physicians ACO, LLC (“AP-ACO”) entered into a reorganization agreement whereby ACO Acquisition Corporation #2, a newly organized entity which NMM is its sole shareholder, will merge into AP-ACO, effective on December 20, 2016 (date of filing of merger agreement with the California Secretary of State). AP-ACO operates an accountable care organization (“ACO”), as defined under the Medicare Shares Savings Program (“MSSP”), which is comprised of the ACO’s network of independent medical practices. The primary reason for the business combination to for NMM to acquire the member relationships of AP-ACO.
Immediately following the effective date, NMM became the sole member of Allied Physicians ACO, LLC. On the effective date, all of the membership interests of Allied Physicians ACO, LLC issued and outstanding immediately prior to the effective date were converted on a pro rata basis into four million (4,000,000) shares of NMM common stock. All of Allied Physicians ACO, LLC’s right, title and interest in and to all of its assets as of the effective date were included as part of the merger, including, without limitation, all of Allied Physicians ACO, LLC’s economic interest in PMIOC. See note 7 for details of the type of business that PMIOC is in and activities that it conducts.
NMM issued 4,000,000 shares of common stock valued at $2,080,000 to the members of Allied Physicians ACO, LLC. Per management’s evaluation, which utilized the income and market approaches, the estimated fair value of the NMM common stock issued as consideration for the transaction was $0.52 per share. Transaction costs are not included as a component of consideration transferred and were expensed as incurred, which were minimal.
NMM did not acquire any identifiable tangible assets and did no assume any liabilities as a result of the acquisition. NMM acquired intangible assets related to the member relationships.
F-99
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
The Company accounted for the acquisition as a business combination using the acquisition method of accounting which requires, among other things, that assets acquired and liabilities assumed be recognized at their fair values as of the acquisition date and be recorded on the balance sheet. Under the acquisition method of accounting, the total purchase price was allocated to the intangible assets acquired with the remainder allocated to goodwill. Goodwill is not deductible for tax purposes.
The final allocation of the total purchase price to the net assets acquired is summarized as follows:
| Identifiable intangible asset – member relationships | $ | 1,497,000 | ||
| Goodwill | 1,192,968 | |||
| Total assets acquired | 2,689,968 | |||
| Deferred tax liability | (609,968 | ) | ||
| Total liabilities assumed | (609,968 | ) | ||
| Net assets acquired | $ | 2,080,000 |
Investment in Other Entities:
Equity Method
Pacific Medical Imaging & Oncology Center, Inc.:
Pacific Medical Imaging & Oncology Center, Inc. (“PMIOC”) was incorporated in 2004 in the state of California. PMIOC provides comprehensive diagnostic imaging services using state-of-the-art technology. PMIOC offers high quality diagnostic services such as MRI/MRA, PET/CT, CT, nuclear medicine, ultrasound, digital x-rays, bone densitometry and digital mammography at their facilities.
In July 2015, APC invested $1,200,000 for a 40% ownership in PMIOC. APC paid $564,000 cash for this investment with the remaining $636,000 due on or before December 31, 2016, pursuant to a promissory note dated July 1, 2015. The remaining balance of $600,000 was included in notes payable as of December 31, 2015 and was repaid in full in 2016.
APC accounted for its investment in PMIOC under the equity method of accounting as APC has the ability to exercise significant influence, but not control over PMIOC’s operations.
Universal Care, Inc.
Universal Care, Inc. (“UCI”) is a family run, privately held health plan that has been in operation since 1985 in order to help its members through the complex healthcare system. UCI is owned by Howard E. Davis and various family members. UCI holds a license under the California Knox-Keene Health Care Services Plan Act (Knox-Keene Act) to operate as a full-service health plan. UCI contracts with the Center for Medicare and Medicaid services (CMS) under the Medicare Advantage Prescription Drug Program.
F-100
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
On November 18, 2015, UCAP, an entity solely owned 100% by APC with APC’s executives, purchased from UCI 100,000 shares of UCI class A-2 voting common stock (comprising 48.9% of the total outstanding UCI shares, but 50% UCI’s voting common stock) for $10,000,000. APC accounted for its investment in UCI under the equity method of accounting as APC has the ability to exercise significant influence, but not control over UCI’s operations.
In 2015, the Company also advanced $5,000,000 to UCI for working capital purposes. The subordinated loan accrues interest at the prime rate plus 1% or 4.75% as of December 31, 2016 with interest to be paid monthly. Pursuant to the stock purchase agreement, the principal repayment schedule is based on certain contingent criteria.
DMG:
On May 14, 2016, David C.P. Chen M.D., Inc., a California professional corporation doing business as Diagnostic Medical Group (“DMG”), David C.P. Chen M.D., individually (collectively “Seller”) and APC-LSMA, a designated shareholder professional corporation formed on October 15, 2012, which is 100% owned by Dr. Thomas Lam (CEO of APC) and is controlled and consolidated by APC who is the primary beneficiary of this VIE, entered into a share purchase agreement whereby APC-LSMA acquired a 40% ownership interest in DMG for total cash consideration of $1,600,000.
Seller may in Seller’s sole discretion (but shall not be obligated to) use all or a portion of the purchase price proceeds to purchase shares of common stock of APC and/or NMM. The purchase price for any shares of APC and/or NMM common stock shall be at the then applicable price per share established by APC and/or NMM Board of Directors, respectively (which, as of the closing date is $1.00 per share of APC common stock and $1.00 per share of NMM common stock). Notwithstanding the foregoing, in the event Seller (in Seller’s sole discretion) uses a portion of the purchase price proceeds to purchase shares of APC common stock, Seller shall have the right to purchase sixty thousand (60,000) shares of APC common stock for the aggregate purchase price of Ten Thousand Dollars ($10,000) (the “AP Share Option”), provided that, (i) the AP Share Option shall automatically expire on the date that is three (3) months after the closing date unless exercised by written notice given by Seller to APC prior to the expiration thereof; and (ii) any shares of APC common stock purchased by Seller that are not covered by the AP Share Option shall be purchased by Seller at the then applicable price per share established by the APC Board of Directors. See note 12 for details of the accounting for the stock option.
APC accounted for its investment in DMG under the equity method of accounting as APC has the ability to exercise significant influence, but not control over DMG’s operation
F-101
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
Pacific Ambulatory Surgery Center
Pacific Ambulatory Surgery Center, LLC, a California limited liability company (“PASC”), is a multi-specialty outpatient surgery center that is certified to participate in the Medicare program and is accredited by the Accreditation Association for Ambulatory Health Care. PASC has entered into agreements with organizations such as healthcare service plans, independent physician practice associations, medical groups and other purchasers of healthcare services for the arrangement of the provision of outpatient surgery center services to subscribers or enrollees of such health plans. On November 15, 2016, PASC and APC, entered into a membership interest purchase agreement whereby PASC sold 40% of its aggregate issued and outstanding membership interests to APC for total consideration of $800,000.
In connection with the membership interest purchase agreement, PASC entered into a management services agreement with NMM, which requires the payment of management fees computed as 2% of PASC revenues. The term of the management services agreement commenced on the effective date and extend for a period of 60 months thereafter, and may be extended in writing at the sole option of NMM for an additional period of 60 months following the expiration of the initial term and is automatically renewed for additional consecutive terms of three years unless terminated by either party. PASC shall not be permitted to terminate the management services agreement for any reason during the initial term and, if extended, the extended term.
APC accounted for its investment in PASC under the equity method of accounting as APC has the ability to exercise significant influence, but not control over PASC’s operations.
APA-ACO
On May 25, 2016, NMM and AMEH established APA-ACO as a joint venture entity to facilitate the member lives acquired by NMM through its acquisitions of AP-ACO and APCN-ACO to NGACO (see Note 5). There has been no activity for this joint venture as of December 31, 2016.
Cost Method
Apollo Medical Holdings, Inc.
On October 14, 2015, the Company invested $10 million in connection with the purchase of shares of Series A preferred stock (“Series A Preferred Stock”) and warrants (“Series A Warrants”) of Apollo Medical Holdings, Inc. (“AMEH”), a publicly traded company, in which Dr. Thomas Lam, the CEO of NMM, is also a director of AMEH. At the time, the investment represented a 16.9% equity ownership interest of AMEH, and it was determined that NMM does not have the ability to exercise significant influence over the operating and financial policies of AMEH.
The Series A Preferred Stock has a liquidation preference in the amount of $9.00 per share plus any declared and unpaid dividends. The Series A Preferred Stock can be voted for the number of shares of AMEH Common Stock into which the Series A Preferred Stock could then be converted, which initially is one-for-one.
The Series A Preferred Stock is convertible into shares of AMEH Common Stock, at the option of NMM, at any time after issuance at an initial conversion rate of one-for-one, subject to adjustment in the event of stock dividends, stock splits and certain other similar transactions. The Series A Preferred Stock is mandatorily convertible not sooner than the earlier to occur of (i) the later of (x) January 31, 2017 or (y) 60 days after the date on which AMEH file their quarterly report on Form 10-Q for the period ended September 30, 2016 (the “Redemption Expiration Date”); or (ii) the date on which AMEH receive the written, irrevocable decision of NMM not to require a redemption of the Series A Preferred Stock (as described in the following paragraph), in the event that AMEH engage in one or more transactions resulting in gross proceeds of not less than $5,000,000, not including any transaction with NMM.
F-102
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
At any time prior to conversion and through the Redemption Expiration Date, the Series A Preferred Stock may be redeemed at the option of NMM, on one occasion, in the event that AMEH’s net revenue for the four quarters ended September 30, 2016, as reported in its periodic filings under the Exchange Act, are less than $60,000,000. In such event, AMEH shall have up to one year from the date of the notice of redemption by NMM to redeem the Series A Preferred Stock, the Series A Warrants and any shares of Common Stock issued in connection with the exercise of any Series A Warrants theretofore (collectively the “Redeemed Securities”), for the aggregate price paid therefore by NMM, together with interest at a rate of 10% per annum from the date of the notice of redemption until the closing of the redemption. Any mandatory conversion described in the previous paragraph shall not take place until such time as it is determined that that conditions for the redemption of the Redeemed Securities have not been satisfied or, if such conditions exist, NMM has decided not to have such securities redeemed. NMM has agreed to relinquish its redemption rights relating to the Series A Preferred Stock it owns in AMEH pursuant to the terms of a Consent and Waiver Agreement dated as of December 21, 2016 by and between AMEH and NMM.
The Series A Warrants may be exercised at any time after issuance and through October 14, 2020, for $9.00 per share, subject to adjustment in the event of stock dividends and stock splits. Alternatively, the Series A Warrants may be exercised pursuant to a “cashless exercise” feature, for that number of shares of Common Stock determined by dividing (x) the aggregate Fair Market Value (as defined in the Series A Warrant) of the shares in respect of which the Series A Warrant is being converted minus the aggregate Warrant Exercise Price (as defined in the Series A Warrant) of such shares by (y) the Fair Market Value of one share of AMEH Common Stock. The Series A Warrants are not separately transferable from the Series A Preferred Stock. The Series A Warrants are subject to redemption in the event that the Series A Preferred Stock is redeemed by NMM, as described above.
NMM has the right to designate to the Nominating/Corporate Governance Committee of the Board of Directors one person to be nominated as a director of AMEH. NMM has designated Thomas S. Lam, M.D., and he was elected as a director of AMEH on January 19, 2016.
On March 30, 2016, NMM purchased 555,555 units of AMEH’s securities for $4,999,995, each unit consisting of one share of Series B convertible preferred stock (“Series B Preferred Stock”) and a stock purchase warrant (a “Series B Warrant”) to purchase one share of AMEH’s common stock at $10.00 per share, none of which securities have yet been converted or exercised for AMEH common stock but which could result in the issuance by AMEH of up to 1,111,110 shares of AMEH common stock to NMM if they converted all of the Series B Preferred Stock and exercised all of the Series B Warrants that are currently held.
The Series B Preferred Stock has a liquidation preference in the amount of $9.00 per share plus any declared and unpaid dividends. The Series B Preferred Stock can be voted for the number of shares of Common Stock into which the Series B Preferred Stock could then be converted, which initially is one-for-one.
F-103
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
The Series B Warrants may be exercised at any time after issuance and through March 31, 2021, for $10.00 per share, subject to adjustment in the event of stock dividends and stock splits. Alternatively, the Series B Warrants may be exercised pursuant to a “cashless exercise” feature, for that number of shares of AMEH Common Stock determined by dividing (x) the aggregate Fair Market Value (as defined in the Series B Warrant) of the shares in respect of which the Series B Warrant is being converted minus the aggregate Warrant Exercise Price (as defined in the Series B Warrant) of such shares by (y) the Fair Market Value of one share of AMEH Common Stock. The Series B Warrants are not separately transferable from the Series B Preferred Stock.
On December 21, 2016, Apollo Medical Holdings, Inc. (“AMEH”), entered into an Agreement and Plan of Merger (the “Merger Agreement”) among AMEH, Apollo Acquisition Corp., a California corporation and wholly-owned subsidiary of AMEH (“Merger Subsidiary”), NMM, and Kenneth Sim, M.D., not individually but in his capacity as the representative of the shareholders of NMM (the “Shareholders’ Representative”).
Thomas Lam, M.D. and Kenneth Sim, M.D. entered into Voting Agreements with AMEH. Under the Voting Agreements, Dr. Sim and Dr. Lam have agreed, among other things, to vote in favor of the approval and adoption of the Merger (as such term is defined below) and the Merger Agreement.
Under the terms of the Merger Agreement, Merger Subsidiary will merge with and into NMM, with NMM becoming a wholly-owned subsidiary of AMEH (the “Merger”). The Merger is intended to qualify for federal income tax purposes as a tax deferred reorganization under the provisions of Section 368(a) of the Internal Revenue Code of 1986. In the transaction, NMM will receive such number of shares of AMEH common stock such that NMM shareholders will own 82% and AMEH shareholders will own 18% of issued and outstanding shares of AMEH at closing. Additionally, NMM has agreed to relinquish its redemption rights relating to preferred stock it owns in AMEH pursuant to the terms of a Consent and Waiver Agreement dated as of December 21, 2016 by and between the AMEH and NMM. The transaction was approved unanimously by the Board of Directors of both companies. Consummation of the Merger is subject to various closing conditions, including, among other things, approval by the stockholders of AMEH and the stockholders of NMM. As part of the Merger Agreement, AMEH and NMM have made various mutual representations and warranties.
Within five business days following the execution of the Merger Agreement, NMM was required provide a working capital loan to AMEH in the principal amount of $5,000,000, which occurred on January 3, 2017 and is evidenced by a promissory note (see above).
The Merger Agreement grants each party the ability to update disclosure schedules through January 20, 2017. If any updated disclosure schedules are found to be unacceptable to the receiving party, as determined in such receiving party’s sole discretion, then such receiving party may terminate the Merger Agreement no later than February 3, 2017.
F-104
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
The Merger Agreement provides that Thomas Lam, M.D., current Chief Executive Officer of NMM, and Warren Hosseinion, M.D., current Chief Executive Officer of AMEH will be Co-Chief Executive Officers of the combined company upon closing of the transaction. Kenneth Sim, M.D., who currently serves as Chairman of NMM, will be Executive Chairman of AMEH. Gary Augusta, current Executive Chairman of AMEH, will be President, Mihir Shah will continue as Chief Financial Officer, and Hing Ang, current Chief Financial Officer of NMM will be the Chief Operating Officer. Adrian Vazquez, M.D. and Albert Young, M.D. current Medical Officers of AMEH will be Co-Chief Medical Officers. The Board of Directors will consist of nine directors, five appointees (including three independent directors) from NMM and four appointees (including two independent directors) from AMEH.
As part of an amendment to the Merger Agreement on March 30, 2017, the merger consideration to be paid by AMEH to NMM was amended to include warrants to purchase 850,000 shares of common stock at an exercise price of $11 per share, that will only be granted in the case that the proposed merger between the NMM and AMEH occurs (such warrant will not vest and will expire if the contemplated merger transaction does not occur), in exchange for NMM providing both a guarantee for AMEH’s convertible note payable to Alliance Apex (Alliance Note) and as compensation to NMM for relinquishing their right to additional shares in AMEH based on the agreed upon exchange ratio with NMM in the event that the Alliance Note is converted to AMEH common stock.
Loan Receivable
On January 3, 2017, pursuant to a promissory note agreement, NMM provided a loan to AMEH in the principal amount of $5,000,000. The entire outstanding principal amount is due and payable in full on the maturity date of January 3, 2019. Interest accrues at 1% point above the Prime Rate commencing on the first date of the first month immediately following the execution of the note agreement and is to be paid by AMEH to NMM in successive quarterly installments.
Bank Loan and Lines of Credit
On July 24, 2015, NMM entered into a promissory note agreement with a bank to borrow up to $15,000,000. The note was guaranteed by two officers of APC. The interest rate is based on the Wall Street Journal “prime rate” plus 1.00% or 4.25% as of December 31, 2015 and required 18 monthly consecutive interest payments, beginning August 24, 2015; 59 monthly consecutive principal and interest payments in the initial amount of $54,896 each, beginning February 24, 2017 and maturing on January 24, 2022. NMM borrowed $10,000,000 in October 2015 and repaid the entire amount in December 2015. The loan was cancelled on July 27, 2016.
In April 2012, APC entered into a promissory note agreement with a bank, which was amended on April 22, 2016 (as amended, the “APC Business Loan Agreement”). The APC Business Loan Agreement modifies certain terms of the promissory note agreement in order to (i) increase the original loan availability amount of $3,000,000 to $10,000,000, (ii) extend the maturity date under the promissory note agreement to April 22, 2018, and (iii) add six additional guarantees. The interest rate is based on the Wall Street Journal “prime rate” plus 0.125% or 3.625% and 3.375% as of December 31, 2016 and 2015, respectively. As of December 31, 2016, the Company was not in compliance with certain financial debt covenant requirements contained in the loan agreement. Subsequent to year end, APC obtained a waiver from the bank for noncompliance of the financial debt covenant requirements as of December 31, 2016. The loan is personally guaranteed by 13 shareholders who are also members of the Company’s board of directors and two-non board members and is collateralized by substantially all assets of APC. No amounts were drawn on this line during 2016 and 2015 and no amounts were outstanding as of December 31, 2016 and 2015.
F-105
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
Equity Issuances
NMM:
On June 30, 2015, NMM filed an amendment to its Articles of Incorporation to effectuate a 3.192-for-1 stock split.
On July 28, 2015, NMM filed an amendment to its Articles of Incorporation to effectuate a 3-for-1 stock split.
On July 28, 2015, consequential to the 3:1 stock split stated above, NMM filed an amendment to its Articles of Incorporation to increase its authorized number of common stock from 300,000,000 to 900,000,000 shares.
During 2015, NMM sold an aggregate of 750,000 shares of common stock at a price of $0.33 per share to a group of doctors. The sales price was determined to be below the estimated fair market value of NMM’s stock on the measurement date; therefore, resulted in additional share-based compensation expense of $72,500. NMM received aggregate proceeds of $250,000 from the sale of shares of common stock.
During 2015, NMM issued an aggregate of 157,876,218 shares of common stock as consideration for the acquisition of PIPA MSO. The fair value of the stock was determined to be $0.37 per share for total valuation of the consideration of $57,887,947.
During 2015, an aggregate of 5,932,350 stock options from the Exclusivity Amendment Agreement were exercised at $0.167 per share and the aggregate amount received by NMM of $988,725 was recorded as a long-term liability for unissued equity shares until the termination date of October 1, 2019.
During 2015, NMM sold an aggregate of 15,437,514 shares of common stock at $1.00 per share for aggregate proceeds of $15,437,514.
During 2015, NMM sold 600,000 shares of common stock at $0.50 per share for aggregate proceeds of $300,000.
During 2016, NMM issued 7,500,000 shares of common stock as consideration for the acquisition of APCN-ACO. The fair value of the stock was determined to be $0.41 per share for total valuation of the consideration of $3,075,000.
During 2016, NMM issued 4,000,000 shares of common stock as consideration for the acquisition of AP-ACO. The fair value of the stock was determined to be $0.52 per share for total valuation of the consideration of $2,080,000.
F-106
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
During 2016, NMM sold 5,850,000 shares of common stock at $1.00 per share for aggregate proceeds of $5,850,000.
During 2016, NMM sold 83,700 shares of common stock at $0.50 per share for aggregate proceeds of $41,850.
During 2016, an option was exercised for the purchase of 250,000 shares of NMM common stock at $0.50 per share for gross proceeds of $125,000.
During 2016, 107,500 shares of NMM common stock were repurchased at $1.00 per share. Such share repurchase reduced the number of shares issued and outstanding.
From January 1, 2017 through April 30, 2017, the Company received cash in the aggregate amount of $248,925 from the exercise of stock options to purchase 1,493,550 shares of NMM common stock at $0.17 per share.
In March 2017, NMM paid bonuses in the aggregate of $2,020,000 to board members based on a 3 tier payment system for 2016 performance that was accrued as of December 31, 2016
APC:
On July 28, 2015, APC filed an amendment to its Articles of Incorporation to effectuate a 3-for-1 stock split.
On July 28, 2015, consequential to the 3:1 stock split stated above, APC filed an amendment to its Articles of Incorporation to increase its authorized number of common stock from 500,000,000 to 1,500,000,000 shares.
During 2015, APC sold an aggregate of 1,500,000 shares of common stock at a price of $0.17 per share to a group of doctors. The sales price was determined to be below the estimated fair market value of APC’s stock on the measurement date; therefore, resulted in additional share-based compensation expense of $680,000. APC received aggregate proceeds of $250,000 from the sale of shares of common stock.
During 2015, APC issued an aggregate of 60,714,750 shares of common stock as consideration for the acquisition of PHW. The fair value of the stock was determined to be $0.62 per share for total valuation of the consideration of $37,238,000.
During 2015, an aggregate of 6,053,550 stock options from the Exclusivity Amendment Agreement, were exercised at $0.167 per share and the aggregate amount received of $1,008,925 was recorded as a long-term liability for unissued equity shares until the termination date of October 1, 2019. These shares are not considered outstanding and are excluded from the earnings per share calculation due to the forfeiture feature contained in the agreement.
During 2015, APC sold an aggregate of 10,253,114 shares of common stock at $1.00 per share for aggregate proceeds of $10,253,114.
F-107
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
During 2016, APC sold an aggregate of 3,145,000 shares of common stock at $1.00 per share for aggregate proceeds of $3,145,000.
During 2016, an option was exercised for the purchase of 250,000 shares of APC common stock at $0.50 per share for gross proceeds of $125,000.
During 2016, an aggregate of 410,000 shares of APC common stock were repurchased at $1.00 per share. Such share repurchase reduced the number of shares issued and outstanding.
During 2016, APC sold 83,700 shares of common stock at a price of $0.50 per share to a board member for cash proceeds of $41,850. The sales price was determined to be below the estimated fair market value of APC’s common stock on the measurement date; therefore, resulted in additional share-based compensation expense of $21,762.
During 2016, an option was exercised for the purchase of 60,000 shares of APC common stock at $0.17 per share for gross proceeds of $10,000.
During 2016, APC issued an aggregate of 1,500,000 shares of common stock at a price of $0.22 per share to former shareholders of PIPA MSO for no consideration; therefore, resulted in additional share-based compensation expense of $380,000.
From January 1, 2017 through April 30, 2017, APC received cash in the aggregate amount of $176,100 from the exercise of stock options to purchase 1,056,600 shares of APC common stock at $0.17 per share.
On March 17, 2017, APC paid dividends of $8,750,000 to its shareholders.
Investment
On November 15, 2016, APC-LSMA, a holding company of APC, agreed to purchase and acquire from AHMC International Cancer Center (“ICC”) 40% of the aggregate issued and outstanding shares of capital stock of ICC for $400,000 in cash. ICC is a professional medical California corporation and has entered into agreements with organizations such as healthcare service plans, independent physician practice associations, medical groups and other purchasers of medical services (“Healthplans”) for the arrangement of the provision of healthcare services to subscribers or enrollees of said Healthplans. In addition, ICC has entered into written agreements with physicians and other healthcare professionals to provide or arrange for the provision of healthcare services to enrollees of participating Healthplans who have contracted or will contract with ICC for healthcare services. Subsequent to the acquisition, it was agreed that ICC’s working capital needs shall be funded as and when needed through capital contributions and/or subordinated debt by the shareholders of ICC on a pro rata basis based on their respective ownership interests in ICC. This transaction has not been completed yet, as certain requirements were not met.
F-108
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
Note 17 – Restatement of Financial Statements
The Company has restated its previously issued consolidated financial statements for the year-ended December 31, 2014 and all related disclosures. The primary changes are:
| · | Changes of accounting treatment of Concourse Diagnostic Surgery Center, LLC. See Note 1. CDSC was previous treated as investment under equity method. This restatement consolidates CDSC as a VIE of APC as it was determined that APC has a controlling financial interest in CDSC and is the primary beneficiary of CDSC. |
| · | As described in Note 3, APC acquired PIPA in a business combination using the acquisition method of accounting in an all-stock transaction. The Company previously has used price per share based on its most recent sales as the basis for its purchase price allocation, which was later deemed below fair market value. The Company hired an outside valuation firm to assist management to revalue the price per share of its common stock at the acquisition date. In addition, the Company reevaluated its purchase price allocation and made proper adjustments to the value of the identifiable intangible assets, goodwill and related deferred tax liability. |
| · | As described in Note 12, the Company discovered that some of the shares issuances and exercise of stock options had been issued below fair market value. The Company hired an outside valuation firm to assist management to revalue the price per share at the date of the stock issuance. Adjustments are reflected in this restatement. |
| · | The Company discovered that sign-on bonus for its medical service providers should have been capitalized and amortized over 5 years. |
| · | The Company accrued full risk pool income in this restatement under the modified cash basis. The Company previously recorded full risk income at the time cash is received.” Income tax provision changed accordingly with the above changes. |
| · | The above changes resulting in Company net income decreased from $1,343,235 to a restated loss of $628,732. Total assets increased from $72,399,240 to a restated amount of $176,650,247. Total liabilities increased from $34,053,759 to a restated amount of $73,125,287. Total shareholders’ equity increased from $38,345,481 to a restated $103,524,960. |
The previously reported, restatement adjustments and restated amounts for those accounts affected by this restatements in the consolidated statement of operations for the year-ended December 31, 2014 and on the consolidated balance sheet as of December 31, 2014 are as follows:
F-109
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
Consolidated Balance Sheet Data
December 31, 2014
| Previously | Restatement | |||||||||||
| Assets | Reported | Adjustment | Restated | |||||||||
| Cash and cash equivalents | 28,153,371 | 2,149,999 | a | 30,303,370 | ||||||||
| Restricted cash | 300,000 | - | 300,000 | |||||||||
| Fiduciary cash | - | 801,258 | a | 801,258 | ||||||||
| Investment in marketable securities | - | 1,034,620 | a | 1,034,620 | ||||||||
| Accounts receivable | 1,201,908 | 224,674 | b | 1,426,582 | ||||||||
| Capitation and claims receivable | 1,839,597 | (135,618) | c | 1,703,979 | ||||||||
| Risk pool receivable | 2,893,807 | 8,220,147 | d | 11,113,954 | ||||||||
| Other receivables | 349,347 | 691,568 | e | 1,040,915 | ||||||||
| Refundable income tax | 582,147 | (452,555) | f | 129,592 | ||||||||
| Prepaid expenses | 35,105 | 15,849 | g | 50,954 | ||||||||
| Land, property and equipment, net | 4,963,107 | 2,614,310 | h | 7,577,417 | ||||||||
| Intangible assets, net | - | 73,393,564 | i | 73,393,564 | ||||||||
| Goodwill | 23,942,283 | 14,670,141 | j | 38,612,424 | ||||||||
| Investments in other entities - CDSC | 977,700 | 6,183,168 | k | 7,160,868 | ||||||||
| Investments in other entities - LaSalle | 7,160,868 | (7,160,868) | k | - | ||||||||
| Sign-on bonus | - | 1,911,875 | l | 1,911,875 | ||||||||
| Other assets | - | 88,872 | m | 88,872 | ||||||||
| Total assets | 72,399,240 | 104,251,004 | 176,650,244 | |||||||||
| Liabilities | ||||||||||||
| Accounts payable and accrued liabilities | 12,510,132 | 5,368,388 | n | 17,878,520 | ||||||||
| Capitation and incentives payables | 7,616,402 | 290,732 | o | 7,907,134 | ||||||||
| Fiduciary accounts payable | - | 801,258 | p | 801,258 | ||||||||
| Medical liabilities | 11,892,747 | (2 | ) | 11,892,745 | ||||||||
| Income taxes payable | - | 1,973,227 | f | 1,973,227 | ||||||||
| Notes payable, current portion | 45,183 | - | 45,183 | |||||||||
| Deferred tax liability | 506,000 | 30,637,925 | q | 31,143,925 | ||||||||
| Notes payable, long-term portion | 1,483,295 | - | 1,483,295 | |||||||||
| Total liabilities | 34,053,759 | 39,071,528 | 73,125,287 | |||||||||
| Mezzanine equity | ||||||||||||
| Noncontrolling interest | - | 105,067,500 | r | 105,067,500 | ||||||||
| Network Medical Management, Inc. shareholders’ equity: | ||||||||||||
| Common Stock | 40,252,406 | (38,369,847) | r | 1,882,559 | ||||||||
| Additional paid-in capital | - | 89,099 | r | 89,099 | ||||||||
| Total Network Medical Management Inc. redeemable common stock | 40,252,406 | (38,280,748 | ) | 1,971,658 | ||||||||
| Shareholders' equity | ||||||||||||
| Accumulated deficit | (1,906,925 | ) | (2,201,379) | r | (4,108,304 | ) | ||||||
| Total Network Medical Management, Inc. shareholder's equity | (1,906,925 | ) | (2,201,379 | ) | (4,108,304 | ) | ||||||
| Noncontrolling Interest | - | 594,103 | 594,103 | |||||||||
| Total shareholders' equity | (1,906,925 | ) | (1,607,276 | ) | (3,514,201 | ) | ||||||
| Total liabilities and shareholder's equity | 72,399,240 | 104,251,004 | 176,650,244 | |||||||||
F-110
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
| a. | Reclassification of $4,245,891 to accounts payable and reclassification of ($998,651) to accounts receivable due to a cut-off error, reclassification ($801,258) to fiduciary cash, added $738,637 from CDSC due to consolidation, reclassification of $1,034,620 for a net of $2,149,999. |
| b. | Added CDSC accounts receivable of $788,005, reduced net intercompany management fee of ($563,331), for a net adjustment of $224,674. |
| c. | Reclassification to other receivables (see e. below) for a net adjustment of ($135,618). |
| d. | Added full risk pool income receivables based on a modified cash basis of $8,220,147; full risk pool income was previously recorded at the time cash is received. |
| e. | Added reclassification of $135,618 (see c. above), added reclassification of $998,651 (see a. above), added $200,000 from PIPA purchase price allocation, added $127,500 in other receivable, reclassification of ($17,401) to other asset (see i and m below), eliminated intercompany receivable of ($752,800) for a net adjustment of $691,568. |
| f. | Income tax payable and refundable changed due to changes in taxable income and tax provision. |
| g. | Added prepaid expense from CDSC of $15,849. |
| h. | Added fixed assets of $1,855,086 and related accumulated depreciation of ($1,139,732) from CDSC, added $1,219,718 in FMV step-up to buildings purchased related to the merger with PIPA and $679,238 in related accumulated depreciation, for a net adjustment of $2,614,310. |
| i. | Added gross intangible asset of $74,054,000 related to the PIPA merger and -$660,436 in accumulated amortization for a net adjustment of $73,393,564. |
| j. | Goodwill increased by $14,670,141 due to revaluing the stock related to the PIPA merger. |
| k. | To eliminate income recorded under equity method relating to CDSC income. CDSC is now consolidated in this restatement. |
| l. | Added capitalized sign-on bonus of $1,995,000 and related accumulated amortization of -$83,125 for a net adjustment of $1,911,875. |
| m. | Added reclassification of $21,000 (see e above) and added other assets of $67,872 from CDSC for a net adjustment of $88,872. |
| n. | Reclassification of $4,245,891 from cash (see a above), added $$3,012,032 from revised purchase price allocation related to PIPA merger, added $641,890 in management fee related to risk pool income, reclassification of $3,600 from other payable to other assets, added CDSC accounts payable of $242,585, reclassification of ($801,258) to fiduciary payable, eliminating intercompany AP of ($1,958,023), reclassification of ($18,329) to incentive payable for a net adjustment of $5,368,388. |
| o. | Increase of $272,403 in star incentive payable, reclassification of $18,329 (see m above) for a net adjustment of $290,732 |
| p. | Reclassification from n. above for a net adjustment of $801,258. |
| q. | Increase of deferred tax liability of $30,637,925 related to revised purchase price allocation. |
| r. | Restatement resulting in common stock revalued at FMV relating to the PIPA merger and revised shareholder equity due to the addition of non-controlling interest (NCI) calculation. |
F-111
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
Consolidated Income Statement Data
For the year-ended December 31, 2014
| Previously | Restatement | |||||||||||
| Revenue | Reported | Adjustment | Restated | |||||||||
| Management income | 11,954,649 | - | 11,954,649 | |||||||||
| Capitation and claims | 104,116,239 | (614,603 | )a | 103,501,636 | ||||||||
| Surgery center income | - | 4,601,143 | b | 4,601,143 | ||||||||
| Risk pool settlements and bonuses | 7,642,081 | 5,349,078 | c | 12,991,159 | ||||||||
| Fee for services | - | 614,605 | a | 614,605 | ||||||||
| Miscellaneous income | - | 676,897 | a | 676,897 | ||||||||
| 123,712,969 | 10,627,120 | 134,340,089 | ||||||||||
| Expenses | ||||||||||||
| Contracted physicians and other services | 82,394,600 | 28,102,610 | d | 110,497,210 | ||||||||
| General and administrative expenses | 18,059,054 | 9,203,831 | e | 27,262,885 | ||||||||
| Management fees | 3,757,858 | 4,541,975 | f | 8,299,833 | ||||||||
| Directors' fee | 21,280,660 | (21,280,660 | )g | - | ||||||||
| Depreciation and amortization | 255,873 | 1,111,561 | h | 1,367,434 | ||||||||
| 125,748,045 | 21,679,317 | 147,427,362 | ||||||||||
| Income (loss) from operations | (2,035,076 | ) | (11,052,197 | ) | (13,087,273 | ) | ||||||
| Other income (expense): | ||||||||||||
| Gain from equity method investments | 2,373,707 | (301,237 | )i | 2,072,470 | ||||||||
| Interest income | 329,557 | (210,907 | )j | 118,650 | ||||||||
| Interest expense | (63,790 | ) | 63,790 | k | - | |||||||
| Other | 896,437 | (769,683 | )l | 126,754 | ||||||||
| 3,535,911 | (1,218,037 | ) | 2,317,874 | |||||||||
| Income (loss) before income taxes | 1,500,835 | (12,270,234 | ) | (10,769,399 | ) | |||||||
| Income taxes | ||||||||||||
| Current tax expense | 1,600 | 2,539,784 | m | 2,541,384 | ||||||||
| Deferred tax expense | 156,000 | 235,927 | m | 391,927 | ||||||||
| 157,600 | 2,775,711 | 2,933,311 | ||||||||||
| Net Income (loss) | 1,343,235 | (15,045,945 | ) | (13,702,710 | ) | |||||||
| Less: Net loss attributable to noncontrolling interests | - | (13,073,974 | )n | (13,073,974 | ) | |||||||
| Net Income (loss)attributable to NMM's shareholders | 1,343,235 | (1,971,971 | ) | (628,736 | ) | |||||||
F-112
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
| a. | Reclassification between income accounts. |
| b. | Added $4,601,143 in surgical center income due to CDSC consolidation. |
| c. | Record additional risk pool income of $5,349,078. |
| d. | Added $272,400 star incentive expense, added $179,870 in stock compensation related to sign-on bonus, reduced ($2,122,500) in sign-on bonus reclass to amortizable asset over 5 years, add $19,291,999 share-based comp for shares issued below fair market value, eliminate intercompany expense of ($56,707), reclassification of payroll expense from e. below of $10,537,548 for a net adjustment of $28,102,610. |
| e. | Added G&A expense of $3,157,082 from CDSC, reclassification of ($56,542) to other expense, reclassification of $2,655,686 in management fees, reclassification of $14,082,999 in directors’ fee, reclassification of payroll expense of ($10,537,548) to d. above, reclassification of ($97,846) to j. below for a net adjustment of $9,203,831. |
| f. | Reclassification of ($2,655,686) to e., reclassification of $7,197,661 from g. for a net adjustment of $4,541,975. |
| g. | Reclassification to e. and f. above. |
| h. | Added $371,017 of depreciation expense from CDSC, added sign-on bonus amortization of $83,125, added intangible asset amortization of $660,436 and misc. depreciation adjustment of ($3,017) for a net adjustment of $1,111,561. |
| i. | Eliminate CDSC equity income of ($301,327), now consolidated. |
| j. | Added ($34,057) in additional interest expense, added bank loan interest from CDSC of ($17,014), reclassification of ($63,790) from k. below and other adjustment of $1,800, reclassification of ($97,846) from e above for a net adjustment of ($210,907) |
| k. | Reclassification to j above. |
| l. | Reclassification between income accounts. |
| m. | Income tax provision increased by $2,775,711 as a result of increased in taxable income. |
| n. | This restatement includes revised non-controlling interest calculation. |
F-113
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
Consolidated Statement of Cash Flow
For the year-ended December 31, 2014
| Previously | Restatement | |||||||||||
| Reported | Adjustment | Restated | ||||||||||
| CASH FLOWS FROM OPERATING ACTIVITIES: | ||||||||||||
| Net income (loss) | 1,343,235 | (15,045,945 | ) | (13,702,710 | ) | |||||||
| Adjustments to reconcile net income to net cash provided by operating activities: | ||||||||||||
| Depreciation and amortization | 255,873 | 1,111,561 | 1,367,434 | |||||||||
| Stock-based compensation expense | - | 19,471,869 | 19,471,869 | |||||||||
| Gain on equity method investment | (2,373,707 | ) | 301,237 | (2,072,470 | ) | |||||||
| Deferred tax | 156,000 | 111,750 | 267,750 | |||||||||
| Dividend income | 33,100 | (33,100 | ) | - | ||||||||
| Changes in assets and liabilities: | - | |||||||||||
| Accounts receivable | (4,112,014 | ) | (2,593,972 | ) | (6,705,986 | ) | ||||||
| Other receivable | - | (2,001,075 | ) | (2,001,075 | ) | |||||||
| Prepaid expenses and other current assets | (24,710 | ) | 90,600 | 65,890 | ||||||||
| Accounts payable and accrued liabilities | 10,449,890 | (6,031,567 | ) | 4,418,323 | ||||||||
| Income taxes payable (refundable) | (847,198 | ) | 2,513,606 | 1,666,408 | ||||||||
| Due from affiliate | 8,031 | (8,031 | ) | |||||||||
| Medical liabilities | 13,127,256 | 272,401 | 13,399,657 | |||||||||
| 18,015,756 | (1,840,666 | ) | 16,175,090 | |||||||||
| CASH FLOWS FROM INVESTING ACTIVITIES: | ||||||||||||
| Cash received from the merger | - | 5,560,662 | 5,560,662 | |||||||||
| Purchase of marketable securities | - | (1,034,620 | ) | (1,034,620 | ) | |||||||
| Proceeds from note receivable | - | 5,000,000 | 5,000,000 | |||||||||
| Increase in restricted cash | - | (300,000 | ) | (300,000 | ) | |||||||
| Purchases of property and equipment | (639,287 | ) | (21,001 | ) | (660,288 | ) | ||||||
| Net cash used in investing activities | (639,287 | ) | 9,205,041 | 8,565,754 | ||||||||
| CASH FLOWS FROM FINANCING ACTIVITIES: | ||||||||||||
| Proceeds from note receivable | 5,000,000 | (5,000,000 | ) | - | ||||||||
| Return of capital from CDSC | 50,000 | (50,000 | ) | - | ||||||||
| Dividends/repayment of capital paid | (6,852,224 | ) | 169,937 | (6,682,287 | ) | |||||||
| Principal payments on notes payable | (3,815,538 | ) | (745,794 | ) | (4,561,332 | ) | ||||||
| Purchase of treasury stock | (328,400 | ) | - | (328,400 | ) | |||||||
| Proceeds from common stock offering | 3,995,351 | (336,000 | ) | 3,659,351 | ||||||||
| Repurchase of shares | (24,000 | ) | - | (24,000 | ) | |||||||
| Net cash provided by financing activities | (1,974,811 | ) | (5,961,857 | ) | (7,936,668 | ) | ||||||
| Net increase (decrease) in cash and cash equivalents | 15,401,658 | 1,402,518 | 16,804,176 | |||||||||
| Cash and cash equivalents, beginning of year | 13,051,713 | 447,481 | 13,499,194 | |||||||||
| Cash and cash equivalents, end of year | 28,453,371 | 1,849,999 | 30,303,370 | |||||||||
F-114
NETWORK MEDICAL MANAGEMENT INC. AND AFFILIATES
NOTES TO FINANCIAL STATEMENTS
DECEMBER 31, 2014
The changes in cash used or provided in operating, investing and financing activities are primarily due to reclassifications and the addition of CDSC cash activities as discussed in the restated balance sheet and income statement.
The cash and cash equivalents increased $2,884,618 from original audited of $28,453,371 to restated $30,303,370. The changes are related to: increase in cash of $738,637 from CDSC consolidation, increase of $3,247,240 in cash as a result of reclassifications from accounts receivable and accounts payable due to a cut-off error, reclassification to restricted cash ($300,000), reclassification of ($1,034,620) to investment in marketable securities and reclassification to fiduciary cash of ($801,258) for a net change of $1,849,999.
F-115
Network Medical Management, Inc.
Condensed Consolidated
Financial Statements (Unaudited)
As
of June 30, 2017 and December 31, 2016
and for the Three and Six Months Ended June 30, 2017 and 2016
F-116
Network Medical Management, Inc.
Contents
F-117
Condensed Consolidated Financial Statements (Unaudited)
F-118
Network Medical Management, Inc.
Condensed Consolidated Balance Sheets (Unaudited)
|
June 30, 2017 |
December 31, 2016 |
|||||||
| Assets | ||||||||
| Current assets | ||||||||
| Cash and cash equivalents | $ | 65,787,183 | $ | 54,824,580 | ||||
| Restricted cash | - | 101,132 | ||||||
| Fiduciary cash | 1,047,828 | 1,050,739 | ||||||
| Investment in marketable securities | 1,053,108 | 1,051,807 | ||||||
| Accounts receivable | 2,814,363 | 3,136,388 | ||||||
| Capitation and claims receivable | 688,890 | 445,181 | ||||||
| Risk pool and incentive receivable | 4,935,732 | 19,633,117 | ||||||
| Prepaid expenses and other current assets | 1,889,268 | 913,354 | ||||||
| Total current assets | 78,216,372 | 81,156,298 | ||||||
| Noncurrent assets | ||||||||
| Land, property and equipment, net | 10,583,715 | 10,373,333 | ||||||
| Intangible assets, net | 99,396,732 | 108,094,049 | ||||||
| Goodwill | 103,407,351 | 103,407,351 | ||||||
| Loans receivable - related parties | 10,000,000 | 5,200,000 | ||||||
| Investments in other entities - equity method | 24,688,225 | 24,256,065 | ||||||
| Investments in other entities - cost method | 10,550,002 | 10,575,002 | ||||||
| Derivative asset - warrants | 5,466,665 | 5,338,886 | ||||||
| Other assets | 1,472,430 | 1,597,978 | ||||||
| Total noncurrent assets | 265,565,120 | 268,842,664 | ||||||
| Total assets | $ | 343,781,492 | $ | 349,998,962 | ||||
F-119
Network Medical Management, Inc.
Condensed Consolidated Balance Sheets (Unaudited)
(Continued)
| June 30, 2017 |
December 31, 2016 |
|||||||
| Liabilities, Mezzanine Equity and Shareholders’ Equity (Deficit) | ||||||||
| Current liabilities | ||||||||
| Accounts payable and accrued expenses | $ | 6,274,556 | $ | 8,083,277 | ||||
| Capitation incentives payable | 11,600,000 | 19,621,645 | ||||||
| Fiduciary accounts payable | 1,047,828 | 1,050,739 | ||||||
| Medical liabilities | 18,519,670 | 18,957,465 | ||||||
| Income taxes payable | 6,672,106 | 2,810,357 | ||||||
| Capital lease obligations | 47,793 | 102,348 | ||||||
| Total current liabilities | 44,161,953 | 50,625,831 | ||||||
| Noncurrent liabilities | ||||||||
| Deferred tax liability | 42,512,506 | 46,932,207 | ||||||
| Liability for unissued equity shares | 2,422,675 | 1,997,650 | ||||||
| Total noncurrent liabilities | 44,935,181 | 48,929,857 | ||||||
| Total liabilities | 89,097,134 | 99,555,688 | ||||||
| Commitments and Contingencies (Note 10) | ||||||||
| Mezzanine equity | ||||||||
| Noncontrolling interest in Allied Pacific of California IPA | 160,407,386 | 162,855,554 | ||||||
| Redeemable common stock, stated value; shares authorized 900,000,000; 398,352,118 and 396,858,568 shares issued, respectively; and 366,343,818 shares outstanding | 86,894,870 | 86,894,870 | ||||||
| Additional paid-in capital | 1,322,246 | 1,084,544 | ||||||
| Total Network Medical Management, Inc. redeemable common stock | 88,217,116 | 87,979,414 | ||||||
| Shareholders’ equity (deficit) | ||||||||
| Network Medical Management, Inc. shareholders’ equity (deficit): | ||||||||
| Retained earnings (accumulated deficit) | 5,571,093 | (773,311 | ) | |||||
| Total Network Medical Management, Inc. shareholders’ equity (deficit) | 5,571,093 | (773,311 | ) | |||||
| Noncontrolling interest in Concourse Diagnostic Surgery Center | 488,763 | 381,617 | ||||||
| Total shareholders’ equity (deficit) | 6,059,856 | (391,694 | ) | |||||
| Total liabilities, mezzanine equity and shareholders’ equity (deficit) | $ | 343,781,492 | $ | 349,998,962 | ||||
See accompanying notes to unaudited condensed consolidated financial statements.
F-120
Network Medical Management, Inc.
Condensed Consolidated Statements of Income (Unaudited)
| Three Months Ended June 30, | Six Months Ended June 30, | |||||||||||||||
| 2017 | 2016 | 2017 | 2016 | |||||||||||||
| Revenue | ||||||||||||||||
| Capitation, net | $ | 62,879,587 | $ | 61,434,728 | $ | 127,595,720 | $ | 122,749,816 | ||||||||
| Risk pool settlements and incentives | 8,358,598 | 4,246,773 | 19,495,798 | 8,798,721 | ||||||||||||
| Management fee income | 6,287,702 | 6,229,768 | 12,824,812 | 12,368,081 | ||||||||||||
| Surgery center income, net | 1,979,486 | 1,529,009 | 3,433,189 | 3,132,574 | ||||||||||||
| Fee-for-service, net | 1,065,062 | 662,219 | 2,275,272 | 965,515 | ||||||||||||
| Other income | 741,265 | 601,257 | 1,022,971 | 1,106,677 | ||||||||||||
| Total revenue | 81,311,700 | 74,703,754 | 166,647,762 | 149,121,384 | ||||||||||||
| Expenses | ||||||||||||||||
| Contracted physicians and other services | 66,672,236 | 63,563,441 | 126,214,808 | 123,072,714 | ||||||||||||
| General and administrative expenses | 5,714,687 | 4,700,307 | 10,858,762 | 8,730,524 | ||||||||||||
| Management fees | 62,500 | 122,500 | 195,000 | 245,000 | ||||||||||||
| Depreciation and amortization | 4,805,979 | 4,481,787 | 9,642,330 | 8,648,783 | ||||||||||||
| Total expenses | 77,255,402 | 72,868,035 | 146,910,900 | 140,697,021 | ||||||||||||
| Income from operations | 4,056,298 | 1,835,719 | 19,736,862 | 8,424,363 | ||||||||||||
| Other income (expense) | ||||||||||||||||
| Income (loss) from equity method investments | (795,102 | ) | 2,783,550 | 1,432,160 | 5,782,047 | |||||||||||
| Interest expense | (575 | ) | (2,028 | ) | (1,386 | ) | (58,766 | ) | ||||||||
| Interest income | 209,492 | 90,681 | 391,777 | 236,623 | ||||||||||||
| Change in fair value of derivative instrument | (1,394,443 | ) | (1,316,666 | ) | 127,779 | (594,444 | ) | |||||||||
| Other income | 26,624 | 14,016 | 28,138 | 43,284 | ||||||||||||
| Total other income (expense), net | (1,954,004 | ) | 1,569,553 | 1,978,468 | 5,408,744 | |||||||||||
| Income before provision for income taxes | 2,102,294 | 3,405,272 | 21,715,330 | 13,833,107 | ||||||||||||
| Provision for income taxes | 736,835 | 1,420,456 | 8,626,080 | 5,730,590 | ||||||||||||
| Net income | 1,365,459 | 1,984,816 | 13,089,250 | 8,102,517 | ||||||||||||
| Less: Net income (loss) attributable to noncontrolling interests | (629,284 | ) | (497,121 | ) | 6,744,846 | 1,801,530 | ||||||||||
| Net income attributable to Network Medical Management, Inc. | $ | 1,994,743 | $ | 2,481,937 | $ | 6,344,404 | $ | 6,300,987 | ||||||||
| Earnings per share - basic | $ | 0.01 | $ | 0.01 | $ | 0.02 | $ | 0.02 | ||||||||
| Earnings per share - diluted | $ | 0.01 | $ | 0.01 | $ | 0.02 | $ | 0.02 | ||||||||
| Weighted average shares of common stock outstanding - basic | 366,343,818 | 360,537,618 | 366,343,818 | 359,724,706 | ||||||||||||
| Weighted average shares of common stock outstanding -diluted | 373,769,718 | 367,674,063 | 373,769,718 | 366,861,151 | ||||||||||||
See accompanying notes to unaudited condensed consolidated financial statements.
F-121
Network Medical Management, Inc.
Condensed Consolidated Statements of Mezzanine Equity (Unaudited)
| Mezzanine Equity - Noncontrolling |
Mezzanine Equity - NMM Redeemable Common Stock | |||||||||||||||||||||||||||
| Interest in APC |
Common Stock | Treasury Stock | Additional | Total NMM Redeemable |
||||||||||||||||||||||||
| Noncontrolling Interest |
Shares | Amount | Shares | Amount | Paid-in Capital |
Common Stock |
||||||||||||||||||||||
| Balance, December 31, 2016 | $ | 162,855,554 | 366,343,818 | $ | 86,894,870 | 24,582,400 | $ | - | $ | 1,084,544 | $ | 87,979,414 | ||||||||||||||||
| Net income | 5,897,068 | - | - | - | - | - | - | |||||||||||||||||||||
| Share-based compensation | 404,764 | - | - | - | - | 237,702 | 237,702 | |||||||||||||||||||||
| Dividends paid | (8,750,000 | ) | - | - | - | - | - | - | ||||||||||||||||||||
| Balance, June 30, 2017 | $ | 160,407,386 | 366,343,818 | $ | 86,894,870 | 24,582,400 | $ | - | $ | 1,322,246 | $ | 88,217,116 | ||||||||||||||||
See accompanying notes to unaudited condensed consolidated financial statements.
F-122
Network Medical Management, Inc.
Condensed Consolidated Statements of Shareholders’ Equity (Deficit) (Unaudited)
| Total NMM | ||||||||||||||||
| Retained Earnings (Accumulated Deficit) |
Total NMM Shareholders’ (Deficit) Equity |
Noncontrolling Interest in CDSC |
Total Shareholders’ Equity (Deficit) |
|||||||||||||
| Balance, December 31, 2016 | $ | (773,311 | ) | $ | (773,311 | ) | $ | 381,617 | $ | (391,694 | ) | |||||
| Net income | 6,344,404 | 6,344,404 | 847,778 | 7,192,182 | ||||||||||||
| Dividends paid | - | - | (740,632 | ) | (740,632 | ) | ||||||||||
| Balance, June 30, 2017 | $ | 5,571,093 | $ | 5,571,093 | $ | 488,763 | $ | 6,059,856 | ||||||||
See accompanying notes to unaudited condensed consolidated financial statements.
F-123
Network Medical Management, Inc.
Condensed Consolidated Statements of Cash Flows (Unaudited)
| Six Months Ended June 30, 2017 |
Six Months Ended June 30, 2016 |
|||||||
| Cash flows from operating activities | ||||||||
| Net income | $ | 13,089,250 | $ | 8,102,517 | ||||
| Adjustments to reconcile net income to net cash provided by operating activities: | ||||||||
| Depreciation and amortization | 9,642,330 | 8,648,783 | ||||||
| Share-based compensation | 642,466 | 756,369 | ||||||
| Change in fair value of derivative instrument | (127,779 | ) | 594,444 | |||||
| Income from equity method investments | (1,432,160 | ) | (5,782,047 | ) | ||||
| Deferred tax | (4,419,701 | ) | 1,355,635 | |||||
| Changes in operating assets and liabilities | ||||||||
| Restricted cash | 101,132 | (377 | ) | |||||
| Accounts receivable | 322,025 | 642,010 | ||||||
| Capitation and claims receivable | (243,709 | ) | 808,797 | |||||
| Risk pool and incentive receivable | 14,697,385 | 3,179,028 | ||||||
| Prepaid expenses and other current assets | (975,914 | ) | (210,259 | ) | ||||
| Other assets | (86,452 | ) | (47,217 | ) | ||||
| Accounts payable and accrued expenses | (1,808,721 | ) | (1,982,101 | ) | ||||
| Capitation incentives payable | (8,021,645 | ) | (4,435,880 | ) | ||||
| Medical liabilities | (437,795 | ) | 895,436 | |||||
| Income taxes payable | 3,861,749 | (11,330,145 | ) | |||||
| Net cash provided by operating activities | 24,802,461 | 1,194,993 | ||||||
| Cash flows from investing activities | ||||||||
| Purchases of marketable securities | (1,301 | ) | (3,894 | ) | ||||
| Repayments from related parties - loans receivable | 200,000 | - | ||||||
| Advances to related parties - loans receivable | (5,000,000 | ) | (104,836 | ) | ||||
| Dividends received from investments in other entities - equity method | 1,000,000 | - | ||||||
| Purchases of investments in other entities - cost method | - | (5,000,000 | ) | |||||
| Proceeds from sale of investments in other entities - cost method | 25,000 | - | ||||||
| Purchases of property and equipment | (943,395 | ) | (1,121,502 | ) | ||||
| Net cash used in investing activities | (4,719,696 | ) | (6,230,232 | ) | ||||
F-124
Network Medical Management, Inc.
Condensed Consolidated Statements of Cash Flows (Unaudited)
(Continued)
| Six Months Ended June 30, 2017 |
Six Months Ended June 30, 2016 |
|||||||
| Cash flows from financing activities | ||||||||
| Dividends paid | (9,490,632 | ) | (6,056,528 | ) | ||||
| Change in noncontrolling interest capital | - | (135,000 | ) | |||||
| Principal payments on bank loan | - | (1,477,561 | ) | |||||
| Repurchase of common shares | - | (300,000 | ) | |||||
| Payment of capital lease obligations | (54,555 | ) | (89,684 | ) | ||||
| Proceeds from exercise of stock options included in liabilities | 425,025 | - | ||||||
| Proceeds from common stock offering | - | 6,640,000 | ||||||
| Net cash used in financing activities | (9,120,162 | ) | (1,418,773 | ) | ||||
| Net increase (decrease) in cash and cash equivalents | 10,962,603 | (6,454,012 | ) | |||||
| Cash and cash equivalents, beginning of period | 54,824,580 | 59,014,715 | ||||||
| Cash and cash equivalents, end of period | $ | 65,787,183 | $ | 52,560,703 | ||||
| Supplemental disclosures of cash flow information | ||||||||
| Cash paid for income taxes | $ | 9,195,024 | $ | 15,722,680 | ||||
| Cash paid for interest | 1,386 | 58,766 | ||||||
| Supplemental disclosures of non-cash investing and financing activities | ||||||||
| Stock issued in connection with acquisitions | $ | - | $ | 3,075,000 | ||||
| Deferred tax liability adjusted to goodwill | - | 367,851 | ||||||
| Equipment purchased with capital lease | - | 186,091 | ||||||
| Increase in accounts payable and accrued expenses for purchase of property and equipment | - | 383,180 | ||||||
| Reclassification of stock options exercised to liability for unissued common shares | 425,025 | - | ||||||
| Reclassification of fiduciary cash to payable | 2,911 | 1,313,279 | ||||||
See accompanying notes to unaudited condensed consolidated financial statements.
F-125
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
| 1. | Description of Business |
Network Medical Management, Inc. (“NMM”) was incorporated in the State of California in March 1994 for the purpose of providing management services to medical companies and independent practice associations (“IPAs”). The management services cover primarily billing, collection, accounting, administrative, and marketing.
Allied Physicians of California IPA, a Professional Medical Corporation d.b.a. Allied Pacific of California IPA, a Professional Medical Corporation DBA Allied Pacific of California (“APC”) was incorporated on August 17, 1992 for the purpose of arranging health care services as an IPA. APC has contracts with various health maintenance organizations (“HMOs”) or licensed health care service plans as defined in the Knox-Keene Health Care Service Plan Act of 1975. Each HMO negotiates a fixed amount per member per month (“PMPM”) that is to be paid to APC. In return, APC arranges for the delivery of health care services by contracting with physicians or professional medical corporations for primary care and specialty care services. APC assumes the financial risk of the cost of delivering health care services in excess of the fixed amounts received. Some of the risk is transferred to the contracted physicians or professional corporations. The risk is also minimized by stop-loss provisions in contracts with HMOs.
On July 1, 1999, APC entered into an amended and restated management and administrative services agreement with NMM (initial management services agreement was entered into in 1997) for an initial fixed term of 30 years. In accordance with relevant accounting guidance, APC is determined to be a Variable Interest Entity (“VIE”) and NMM is the primary beneficiary with the ability to direct the activities (excluding clinical decisions) that most significantly affect APC’s economic performance through its majority representation of the APC Joint Planning Board; therefore APC is consolidated by NMM. As of both June 30, 2017 and December 31, 2016, APC owns 6.29% of NMM.
Concourse Diagnostic Surgery Center, LLC (“CDSC”) was formed on March 25, 2010 in the state of California. CDSC is an ambulatory surgery center in City of Industry, California, is organized by a group of highly qualified physicians, and the surgical center utilizes some of the most advanced equipment in Eastern Los Angeles County and San Gabriel Valley. The facility is Medicare Certified and accredited by the Accreditation Association for Ambulatory Healthcare. During 2011, APC invested $625,000 for a 41.59% ownership in CDSC. Due to capital stock changes, APC’s ownership percentage in CDSC’s capital stock changed to 43.8%, 43.43% and 47.05% on May 31, 2016, July 31, 2016 and March 31, 2017, respectively. APC’s allocation of the profit and loss of CDSC is based on the profit and loss ratio of 43.92% and 41.59% for the three and six months ended June 30, 2017 and 2016, respectively. CDSC is consolidated as a VIE by APC as it was determined that APC has a controlling financial interest in CDSC and is the primary beneficiary of CDSC.
APC-LSMA was formed on October 15, 2012 as a designated shareholder professional corporation and is solely owned by Dr. Thomas Lam, a shareholder and Chief Executive and Financial Officer of APC. APC-LSMA is controlled and consolidated by APC who is the primary beneficiary of this VIE. The only activity of APC-LSMA is to hold the investments in medical corporations, which includes: LaSalle Medical Associates, Pacific Medical Imaging and Oncology Center, Inc. (“PMIOC”) and Diagnostic Medical Group (“DMG”).
Universal Care Acquisition Partners, LLC (“UCAP”), a 100% owned subsidiary of APC, was formed on June 4, 2014, for the purpose of holding the investment in Universal Care, Inc. (“UCI”).
F-126
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
On November 11, 2015, NMM, ACO Acquisition Corporation, and APCN-ACO, A Medical Professional Corp. (“APCN-ACO”) entered into a reorganization agreement whereby ACO Acquisition Corporation, a newly organized entity in which NMM is its sole shareholder, merged with APCN-ACO, effective on January 8, 2016, resulting in APCN-ACO becoming a wholly owned subsidiary of NMM.
On December 18, 2016, NMM, ACO Acquisition Corporation #2, and Allied Physicians ACO, LLC (“AP-ACO”) entered into a reorganization agreement whereby ACO Acquisition Corporation #2, a newly organized entity in which NMM is its sole shareholder, merged into AP-ACO, effective on December 20, 2016, resulting in AP-ACO becoming a wholly owned subsidiary of NMM.
Unless stated otherwise, NMM, ACO Acquisition Corp., APCN ACO, ACO Acquisition Corporation #2, AP ACO, APC, CDSC, APC-LSMA and UCAP are collectively referred to herein as the “the Company.”
| 2. | Basis of Presentation and Summary of Significant Accounting Policies |
Principles of Consolidation
The Company’s condensed consolidated financial statements include the accounts of NMM and its consolidated VIE, APC and its subsidiary UCAP and APC’s consolidated VIEs, CDSC and APC-LSMA. As of the effective dates of the reorganizations, as described above, the accounts of APCN-ACO and AP-ACO were also included in the consolidation of NMM.
All material intercompany balances and transactions have been eliminated in consolidation.
The condensed consolidated financial statements of the Company have been prepared in accordance with generally accepted accounting principles in the United States of America (“GAAP”), for interim financial information. Accordingly, they do not include certain notes and financial presentations normally required under GAAP for complete financial reporting. The interim financial information is unaudited, but reflects all normal adjustments and accruals that are, in the opinion of management, considered necessary to provide a fair presentation for the interim periods presented. The accompanying condensed consolidated financial statements should be read in conjunction with the audited consolidated financial statements for the fiscal year ended December 31, 2016.
The results of operations for the three and six months ended June 30, 2017 are not necessarily indicative of the results to be expected for the entire fiscal year ending December 31, 2017.
Use of Estimates
The preparation of condensed consolidated financial statements and related disclosures in conformity with GAAP requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the condensed consolidated financial statements and the reported amounts of revenues and expenses during the reporting period. Significant items subject to such estimates and assumptions include collectability of receivables, recoverability of long-lived and intangible assets, business combination and goodwill valuation and impairment, derivative assets, accrual of medical liabilities (including incurred, but not reported claims), determination of shared-risk revenues and receivables, income taxes and valuation of share-based compensation. Management evaluates its estimates and assumptions on an ongoing basis using historical experience and other factors, including the current economic environment, and makes adjustments when facts and circumstances dictate. As future events and their effects cannot be determined with precision, actual results could differ materially from those estimates and assumptions.
F-127
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
Receivables
The Company’s receivables are comprised of accounts receivable, capitation and claims receivable, risk pool and incentive receivable. Accounts receivable primarily consists of NMM management fee receivables and CDSC fee-for-service (“FFS”) receivables.
Risk pool and incentive receivable mainly consists of APC full risk pool receivable that is only recorded when expected cash receipts are known or when actual cash is received from Health Source MSO who serves as the management company for the hospitals in the risk pools. Capitation and claims receivable relate to the health plan’s capitation that is received by APC in the following month of service. For APC, other receivables are accrued based on invoices sent to the subcontracted IPA for stop loss insurance premium reimbursement and FFS reimbursement for Alhambra Hospital Medical Center’s self-insured program. For NMM, other receivables are accrued based on invoices for certain expense reimbursements from UCI and invoice for transportation reimbursement from the hospital.
Amounts are recorded as a receivable when the Company is able to determine amounts receivable under these contracts and/or agreements based on information provided and collection is reasonably likely to occur. The Company continuously monitors its collections of receivables and its policy is to write off receivables when they are determined to be uncollectible. The Company has not incurred credit losses related to receivables. No allowance for doubtful accounts is recorded at June 30, 2017 and December 31, 2016.
Concentrations of Risks
Four HMOs accounted for 69% and 70% of the total capitation revenue for the six months ended June 30, 2017 and 2016, respectively. Four HMOs accounted for 69% and 70% of the total capitation revenue for the three months ended June 30, 2017 and 2016, respectively. The loss of these HMO contracts would have an adverse impact on the operations of APC.
Three and two hospitals accounted for 94% and 93%, respectively, of the total risk pool settlements and incentives revenue for the six months ended June 30, 2017 and 2016, respectively. Two hospitals accounted for 99.7% and 93% of the total risk pool settlements and incentives revenue for the three months ended June 30, 2017 and 2016, respectively.
One provider accounted for approximately 68% of total management fee income for the six months ended June 30, 2017 and 2016. One provider accounted for approximately 70% and 69% of total management fee income for the three months ended June 30, 2017 and 2016, respectively. The loss of provider would have an adverse impact on the operations of NMM.
Three and two HMOs accounted for 86% and 76% of the total fee-for-service revenue for the six months ended June 30, 2017 and 2016, respectively. Three and two HMO’s accounted for 88% and 82% of the total fee-for-service revenue for the three months ended June 30, 2017 and 2016, respectively. The loss of these HMO contracts would have an adverse impact on the operations of APC.
No provider accounted for 10% or more of the total surgery center income for the three and six months ended June 30, 2017 and 2016, respectively.
F-128
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
As of June 30, 2017 and December 31, 2016, two providers accounted for approximately 33% and 29% respectively, of total accounts receivable balance.
As of June 30, 2017 and December 31, 2016, two providers and one provider accounted for 100% of the total capitation and claims receivable balance, respectively.
As of June 30, 2017 and December 31, 2016, two providers accounted for 88% and 97%, respectively, of the total risk pool and incentive receivable balance.
Fair Value Measurements
The Company’s financial instruments consist of cash and cash equivalents, restricted cash, fiduciary cash, investment in marketable securities, accounts receivable, loans receivable - related parties, derivative asset - warrants, accounts payable, certain accrued expenses, bank loan, loan payable - related party and the line of credit. The carrying values of the financial instruments classified as current in the accompanying condensed consolidated balance sheets are considered to be at their fair values, due to the short maturity of these instruments. The carrying amount of the long-term bank loan and line of credit approximates fair value as they bear interest at rates that approximate current market rates for debt with similar maturities and credit quality.
Financial Accounting Standards Board (“FASB”) Accounting Standards Codification (“ASC”) 820, Fair Value Measurement (“ASC 820”), applies to all financial assets and financial liabilities that are measured and reported on a fair value basis and requires disclosure that establishes a framework for measuring fair value and expands disclosure about fair value measurements. ASC 820 establishes a fair value hierarchy for disclosures of the inputs to valuations used to measure fair value.
This hierarchy prioritizes the inputs into three broad levels as follows:
Level 1—Inputs are unadjusted quoted prices in active markets for identical assets or liabilities that can be accessed at the measurement date.
Level 2—Inputs include quoted prices for similar assets and liabilities in active markets, quoted prices for identical or similar assets or liabilities in markets that are not active, inputs other than quoted prices that are observable for the asset or liability (i.e., interest rates and yield curves), and inputs that are derived principally from or corroborated by observable market data by correlation or other means (market corroborated inputs).
Level 3—Unobservable inputs that reflect assumptions about what market participants would use in pricing the asset or liability. These inputs would be based on the best information available, including the Company’s own data.
F-129
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
The carrying amounts and fair values of the Company’s financial instruments as of June 30, 2017 are presented below:
| Common Stock | ||||||||||||||||
| Level 1 | Level 2 | Level 3 | Total | |||||||||||||
| Assets | ||||||||||||||||
| Money market accounts* | $ | 52,871,032 | $ | - | $ | - | $ | 52,871,032 | ||||||||
| Marketable securities - certificates of deposit | 1,053,108 | - | - | 1,053,108 | ||||||||||||
| Derivative asset (warrants) | - | - | 5,466,665 | 5,466,665 | ||||||||||||
| Total | $ | 53,924,140 | $ | - | $ | 5,466,665 | $ | 59,390,805 | ||||||||
* Included in cash and cash equivalents
The level 3 assets represent warrants in the common stock of Apollo Medical Holdings, Inc. (“AMEH”) and are included in derivative asset - warrants in the condensed consolidated balance sheets.
The following is a reconciliation of the opening and closing balances for financial instruments measured at fair value on a recurring basis using significant unobservable inputs (Level 3) for the period ended June 30, 2017:
| Derivative Asset (Warrants) |
||||
| Balance, December 31, 2016 | $ | 5,338,886 | ||
| Change in fair value of warrants | 127,779 | |||
| Balance, June 30, 2017 | $ | 5,466,665 | ||
The carrying amounts and fair values of the Company’s financial instruments as of December 31, 2016 are presented below:
| Common Stock | ||||||||||||||||
| Level 1 | Level 2 | Level 3 | Total | |||||||||||||
| Assets | ||||||||||||||||
| Money market accounts | $ | 42,553,887 | $ | - | $ | - | $ | 42,553,887 | ||||||||
| Marketable securities -certificates of deposit | 1,051,807 | - | - | 1,051,807 | ||||||||||||
| Derivative asset (warrants) | - | - | 5,338,886 | 5,338,886 | ||||||||||||
| Total | $ | 43,605,694 | $ | - | $ | 5,338,886 | $ | 48,944,580 | ||||||||
F-130
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
The following is a reconciliation of the opening and closing balances for financial instruments measured at fair value on a recurring basis using significant unobservable inputs (Level 3) for the period ended June 30, 2016:
| Derivative Asset (Warrants) |
||||
| Balance, January 1, 2016 | $ | 2,088,889 | ||
| Estimated fair value of new warrants | 1,527,776 | |||
| Change in fair value of warrants | (594,444 | ) | ||
| Balance, June 30, 2016 | $ | 3,022,221 | ||
The fair value of the derivative asset - warrants of approximately $5.5 million at June 30, 2017 was estimated using the Monte Carlo valuation model, using the following inputs: term of 3.29 - 3.75 years, risk free rate of 1.50% - 1.60%, no dividends, volatility of 38.9% - 39.1%, share price of $10.00 per share based on the trading price of the AMEH common stock, and a 0% probability of redemption of the warrant shares issued along with the shares of AMEH’s convertible preferred stock issued in the financing (see Note 5).
The fair value of the derivative asset - warrants of approximately $5.3 million at December 31, 2016 was estimated using the Monte Carlo valuation model, using the following inputs: term of 3.79 - 4.24 years, risk free rate of 1.67% - 1.76%, no dividends, volatility of 63.0% - 62.5%, share price of $7.50 per share based on the trading price of the AMEH common stock adjusted for a marketability discount, and a 0% probability of redemption of the warrant shares issued along with the shares of AMEH’s convertible preferred stock issued in the financing (see Note 5).
The fair value of the derivative asset - warrants of approximately $3.0 million at June 30, 2016 was estimated using the Monte Carlo valuation model, using the following inputs: term of 4.29 - 4.75 years, risk free rate of 0.9% - 1.0%, no dividends, volatility of 64.4% - 65.7%, share price of $5.00 per share based on the trading price of the AMEH common stock, and a 0% probability of redemption of the warrant shares issued along with the shares of AMEH’s convertible preferred stock issued in the financing (see Note 5).
There have been no changes in Level 1, Level 2, or Level 3 classification and no changes in valuation techniques for these assets for the six months and three months ended June 30, 2017 and 2016.
Reportable Segments
The Company operates as one reportable segment, the healthcare delivery segment, and implements and operates innovative health care models to create a patient-centered, physician-centric experience. The Company reports its condensed consolidated financial statements in the aggregate, including all activities in one reportable segment.
F-131
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
Medical Liabilities
APC is responsible for integrated care that the associated physicians and contracted hospitals provide to its enrollees. APC provides integrated care to health plan enrollees through a network of contracted providers under sub-capitation and direct patient service arrangements. Medical costs for professional and institutional services rendered by contracted providers are recorded as contracted physicians and other services expenses in the accompanying condensed consolidated statements of income.
Costs incurred by CDSC for operating its ambulatory surgical center, are included in general and administrative expenses in the condensed consolidated statements of income.
An estimate of amounts due to contracted physicians, hospitals, and other professional providers is included in medical liabilities in the accompanying condensed consolidated balance sheets. Medical liabilities include claims reported as of the balance sheet date and estimates of incurred, but not reported claims (“IBNR”). Such estimates are developed using actuarial methods and are based on numerous variables, including the utilization of health care services, historical payment patterns, cost trends, product mix, seasonality, changes in membership, and other factors. The estimation methods and the resulting reserves are periodically reviewed and updated. Many of the medical contracts are complex in nature and may be subject to differing interpretations regarding amounts due for the provision of various services. Such differing interpretations may not come to light until a substantial period of time has passed following the contract implementation. APC has a $60,000 retention per member professional stop loss and $55,000 per member stop loss for Medi-Cal patients for professional claims. Any adjustments to reserves are reflected in current operations.
Revenue Recognition
Revenue primarily consists of capitation revenue, risk pool settlements and incentives, management fee income, surgery center income and fee-for-services. Revenue is principally recorded in the period in which services are rendered. The form of billing and related risk of collection for such services may vary by customer. The following is a summary of the principle forms of the Company’s billing arrangements and how revenue is recognized for each.
Capitation, net
Capitation revenue (net of capitation withheld to fund risk share deficits) is recognized in the month in which the services are provided. Minor ongoing adjustments to prior months’ capitation, primarily arising from HMOs finalizing of monthly eligibility data for additions or subtractions of enrollees, are recognized in the month they are communicated to APC. Managed care revenues of APC consist primarily of capitated fees for medical services provided by APC under a provider service agreement (“PSA”) or capitated arrangements directly made with various managed care providers including HMOs and management service organizations (“MSOs”). Capitation revenue under the PSA and HMO contracts is prepaid monthly to APC based on the number of enrollees electing APC as their healthcare provider. Health plans and providers with higher acuity enrollees will receive more and those with lower acuity enrollees will receive less.
F-132
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
Risk Pool Settlements and Incentives
Contracts with HMOs also include provisions for APC to participate in the risk (shared risk capitation arrangements) relating to the provision of institutional services (institutional risk) to enrollees, such that APC can earn additional incentive revenue or incur losses based upon the enrollee utilization of hospital services. Typically, any shared risk deficits are not payable until and unless APC generates future risk sharing surpluses, or if the HMO withholds a portion of the capitation revenue to fund any risk share deficits. At the termination of the HMO contract, any accumulated risk share deficit is typically extinguished. Due to the lack of access to information necessary to estimate the related healthcare costs (“IBNR”), revenue from shared risk amounts are recorded when such amounts are known. In addition to risk sharing revenues, APC is also eligible to participate in an incentive program. As an incentive to control enrollee utilization and to promote quality care, the HMOs have designed the quality incentive programs and commercial generic pharmacy incentive programs to compensate APC for efforts it takes to improve the quality of services and for efficient and effective use of pharmacy supplemental benefits provided to the HMO’s members. The incentive programs track specific performance measures and calculate payments to the IPA based on the performance measures.
APC also enter into risk sharing arrangements with affiliated hospitals (full risk capitation arrangements) who in turn have entered into capitation arrangements with various HMOs, pursuant to which the affiliated hospital provides, arranges and pays for institutional risk. Under a risk pool sharing agreement, APC is allocated a percentage of the affiliated hospitals surplus or deficit from the risk pool, after deductions for the affiliated hospitals costs. Advance settlement payments are typically made quarterly in arrears if there is a surplus. However, due to the uncertainty around the settlement of the related IBNR reserve, APC recognizes any excess IBNR reserve on settlement as risk pool settlement revenue when amounts are known. Any excess IBNR is normally settled and paid after a period of approximately one year from the related service period.
Management Fee Income
NMM provides utilization management, claims processing and other administrative services for other IPAs. NMM receives management fee income for the services rendered. Management fees are calculated as a percentage of revenue under capitation contracts with various insurance companies.
Surgery Center Income
CDSC’s surgery center income consists primarily of net patient service revenues that are recorded based upon established billing rates less allowance for contractual adjustments. Revenues are recorded in the period in which the healthcare services are provided, based upon the estimated amounts due from patients and third-party payors, including commercial health plans, employers, workers’ compensation plans and federal and state agencies (under the Medicare and Medicaid programs). CDSC utilizes the payment history specific to each payor and services to record estimated net revenues to ensure the appropriateness of these estimates. Third-party payor contractual payment terms are generally based upon predetermined rates per procedure or fee-for-service rates.
F-133
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
Fee-for-Service
Fee-for-service revenue primarily represents professional component of charges for medical services rendered by the Company’s contracted physicians and paid to the Company for certain reimbursable services, which is recognized at the time reimbursements are received from the health plans.
Stop-Loss Provisions
Stop-loss insurance limits the cost of medical services for enrollees whose professional care costs exceed a specified level. Stop-loss insurance premiums are reported as medical expenses and insurance recoveries are reported as a reduction of related medical expenses. The Company is contingently liable to the extent that any insurer becomes unable to meet its contractual obligation. As of June 30, 2017 and December 31, 2016, there was no liability balance with respect to the stop-loss provision.
The Company has purchased stop-loss insurance, which will reimburse the Company for claims from service providers on a per enrollee basis. The specific retention amount per enrollee per policy period is $55,000 to $60,000 for professional coverage.
Basic and Diluted Earnings Per Share
Basic earnings (loss) per share is computed by dividing net income (loss) attributable to NMM’s shareholders by the weighted average number of common shares outstanding during the periods presented. Diluted earnings per share is computed using the weighted average number of common shares outstanding plus the effect of dilutive securities outstanding during the periods presented, using treasury method. See Note 13 for more details.
Noncontrolling Interests
The Company consolidates entities in which the Company has a controlling financial interest. The Company consolidates subsidiaries in which the Company hold, directly or indirectly, more than 50% of the voting rights, and variable interest entities (VIEs) in which the Company is the primary beneficiary. Noncontrolling interests represent third-party equity ownership interests in the Company’s consolidated entities. The amount of net income attributable to noncontrolling interests is disclosed in the condensed consolidated statements of income.
Mezzanine Equity
Based on the shareholder agreements for both NMM and APC, in the event of a disqualifying event, as defined in the agreements, NMM and APC could be required to repurchase the shares from their respective shareholders based on certain triggers outlined in the shareholder agreements. The triggers that could cause NMM to redeem the shares are not solely within the control of NMM. As the redemption feature of the shares is not solely within the control of NMM, the common stock and additional paid-in capital of NMM has been classified in mezzanine or temporary equity as redeemable common stock. In addition, as the redemption feature of the shares is not solely within the control of APC, the equity of APC does not qualify as permanent equity and has been classified as mezzanine or temporary equity. Accordingly, the Company recognizes noncontrolling interests in APC as mezzanine equity in the condensed consolidated financial statements.
F-134
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
| 3. | Intangible Assets, Net |
At June 30, 2017, intangible assets, net consists of the following:
| Useful Life (Years) |
Gross January 1, 2017 |
Additions | Gross June 30, 2016 |
Accumulated Amortization |
Net June 30, 2017 |
|||||||||||||||||||
| Network/payor relationships | 15 | $ | 106,660,000 | $ | - | $ | 106,660,000 | $ | (29,177,692 | ) | $ | 77,482,308 | ||||||||||||
| Management contracts | 15 | 22,832,000 | - | 22,832,000 | (3,750,972 | ) | 19,081,028 | |||||||||||||||||
| Member relationships | 5-7 | 3,235,000 | - | 3,235,000 | (401,604 | ) | 2,833,396 | |||||||||||||||||
| $ | 132,727,000 | $ | - | $ | 132,727,000 | $ | (33,330,268 | ) | $ | 99,396,732 | ||||||||||||||
At December 31, 2016, intangible assets, net consists of the following:
| Useful Life (Years) |
Gross January 1, 2016 |
Additions | Gross December 31, 2016 |
Accumulated Amortization |
Net December 31, 2016 |
|||||||||||||||||||
| Network/payor relationships | 15 | $ | 106,660,000 | $ | - | $ | 106,660,000 | $ | (22,186,665 | ) | $ | 84,473,335 | ||||||||||||
| Management contracts | 15 | 22,832,000 | - | 22,832,000 | (2,446,286 | ) | 20,385,714 | |||||||||||||||||
| Member relationships | 5-7 | - | 3,235,000 | 3,235,000 | - | 3,235,000 | ||||||||||||||||||
| $ | 129,492,000 | $ | 3,235,000 | $ | 132,727,000 | $ | (24,632,951 | ) | $ | 108,094,049 | ||||||||||||||
Included in depreciation and amortization on the condensed consolidated statements of income is amortization expense of $4,322,476 and $3,998,831 for the three months ended June 30, 2017 and 2016, respectively, and $8,697,317 and $7,700,930 for the six months ended June 30, 2017 and 2016, respectively.
Future amortization expense is estimated to be approximately as follows for the years ending December 31:
| Amount | ||||
| 2017 (remaining six months) | $ | 8,500,000 | ||
| 2018 | 15,300,000 | |||
| 2019 | 13,000,000 | |||
| 2020 | 11,300,000 | |||
| 2021 | 9,700,000 | |||
| Thereafter | 41,596,732 | |||
| $ | 99,396,732 | |||
F-135
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
The member relationship assets of $3,235,000 acquired in the acquisitions of both APCN-ACO and AP-ACO during the year ended December 31, 2016 represent member lives that are to be utilized by APA-ACO. APA-ACO, is an entity owned 50% by NMM and 50% by Apollo Medical Holdings, Inc. (“AMEH”) and is also a Next Gen ACO (“NGACO”), which was approved in January 2017. The Center for Medicare and Medicaid services (“CMS”) is implementing the NGACO Model under section 1115A of the Social Security Act, which authorizes CMS, through its Center for Medicare and Medicaid Innovation, to test innovative payment and service delivery models that have the potential to reduce Medicare, Medicaid or Children’s Health Insurance Program expenditures while maintaining or improving the quality of beneficiaries’ care. The purpose of the NGACO Model is to test innovative payment and service delivery models that have the potential to reduce Medicare, Medicaid or Children’s Health Insurance Program expenditures while maintaining or improving the quality of beneficiaries’ care. These member relationships acquired in 2016 were reenrolled under APA-ACO on January 1, 2017. Members of APCN-ACO and AP-ACO may opt out of the automatic enrollment into APA-ACO.
| 4. | Joint Venture |
NMM entered into a Joint Venture Agreement dated as of January 25, 2017, with Mediportal LLC, a New York limited liability company (“Mediportal”), and Rulemeister Inc., a California corporation, to form a joint venture company to be named Netlytics Enterprise LLC (“Netlytics”) for the purpose of developing and implementing a fully-integrated electronic platform that will enable ACOs, IPAs, health plans and other health care payers and providers to aggregate data and utilize analytic tools to effectively engage in population health management. Netlytics was formed on November 1, 2016. The respective ownership interests of NMM, Mediportal and Rulemeister in Netlytics will be 55%, 30% and 15%. In exchange for its 55% interest, NMM will contribute $275,000 as its capital contribution to Netlytics. In June 2017, APC and Mediportal entered into a subscription agreement. Pursuant to the subscription agreement, APC is to pay Mediportal $405,000 to purchase 270,000 membership interest of Mediportal at a price of $1.50 per membership interest. The effective date of the subscription agreement between APC and Mediportal is subject to completion of due diligence by APC. The effective date of the Joint Venture Agreement is also subject to completion of due diligence by NMM. In addition, there has been no activity in Netlytics and no amounts have been contributed to Netlytics through the date of this filing; therefore this transaction has not been completed and accordingly, these consolidated financial statements do not include any amounts related to this joint venture.
The remainder of this page intentionally left blank.
F-136
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
| 5. | Investments in Other Entities |
Equity Method
LaSalle Medical Associates
LaSalle Medical Associates, Inc., (“LMA”) was founded by Dr. Albert Arteaga in 1996 and currently operates four neighborhood medical centers employing more than 120 dedicated healthcare professionals, treating children, adults and seniors in San Bernardino County. LMA’s patients are primarily served by Medi-Cal and they also accept Blue Cross, Blue Shield, Molina, Care 1st, Health Net and Inland Empire Health Plan. LMA is also an IPA of independently contracted doctors, hospitals and clinics, delivering high quality care to more than 245,000 patients in Fresno, Kings, Los Angeles, Madera, Riverside, San Bernardino and Tulare Counties. During 2012, APC-LSMA, a VIE of APC, entered into a share purchase agreement whereby APC-LSMA invested $5,000,000 for a 25% interest in LMA’s IPA line of business. NMM has a management services agreement with LMA. APC accounts for its investment in LMA under the equity method as APC has the ability to exercise significant influence, but not control over LMA’s operations. For the three months ended June 30, 2017 and 2016, APC recorded a (loss) income from this investment of $(798,185) and $1,013,494, respectively, in the accompanying condensed consolidated statements of income. For the six months ended June 30, 2017 and 2016, APC recorded income from this investment of $513,554 and $2,901,700, respectively, in the accompanying condensed consolidated statements of income. During the six months ended June 30, 2017, APC received dividends of $1,000,000 from LMA. The investment balance was $9,017,429 and $9,503,875 at June 30, 2017 and December 31, 2016, respectively.
PMIOC
PMIOC was incorporated in 2004 in the state of California. PMIOC provides comprehensive diagnostic imaging services using state-of-the-art technology. PMIOC offers high quality diagnostic services such as MRI/MRA, PET/CT, CT, nuclear medicine, ultrasound, digital x-rays, bone densitometry and digital mammography at their facilities.
In July 2015, APC-LSMA entered into a share purchase agreement whereby APC-LSMA, a VIE of APC, invested $1,200,000 for a 40% ownership in PMIOC. APC paid $564,000 cash, and APCN-ACO and AP-ACO paid an aggregate of $36,000 on behalf of APC, for this investment with the remaining $600,000 due on or before December 31, 2016, pursuant to a promissory note dated July 1, 2015. The remaining balance of $600,000 was repaid in full in 2016.
The remainder of this page intentionally left blank.
F-137
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
APC and PMIOC have an Ancillary Service Contract together whereby PMIOC provides covered services on behalf of APC to enrollees of the plans of APC. Under the Ancillary Service Contract for the three and six months ended June 30, 2017 and 2016, APC paid PMIOC fees of approximately $0.6 million and $0.5 million, respectively and approximately $1.1 million and $0.9 million, respectively. APC accounts for its investment in PMIOC under the equity method of accounting as APC has the ability to exercise significant influence, but not control over PMIOC’s operations. During the three months ended June 30, 2017 and 2016, APC recorded income from this investment of $58,539 and $60,297, respectively, in the accompanying condensed consolidated statements of income. During the six months ended June 30, 2017 and 2016, APC recorded income from this investment of $109,619 and $120,593, respectively, in the accompanying condensed consolidated statements of income and has an investment balance of $1,456,047 and $1,346,428 at June 30, 2017 and December 31, 2016, respectively.
Universal Care, Inc.
Universal Care, Inc. (“UCI”) is a privately held health plan that has been in operation since 1985 in order to help its members through the complexities of the healthcare system. UCI holds a license under the California Knox-Keene Health Care Services Plan Act (Knox-Keene Act) to operate as a full-service health plan. UCI contracts with the CMS under the Medicare Advantage Prescription Drug Program.
On August 10, 2015, UCAP, an entity solely owned 100% by APC with APC’s executives, Dr. Thomas Lam, Dr. Pen Lee and Dr. Kenneth Sim, as designated managers of UCAP, purchased from UCI 100,000 shares of UCI class A-2 voting common stock (comprising 48.9% of the total outstanding UCI shares, but 50% of UCI’s voting common stock) for $10,000,000. APC accounts for its investment in UCI under the equity method of accounting as APC has the ability to exercise significant influence, but not control over UCI’s operations. During the three months ended June 30, 2017 and 2016, the Company recorded (loss) income from this investment of $(280,710) and $1,709,759, respectively, in the accompanying condensed consolidated statements of income. During the six months ended June 30, 2017 and 2016, the Company recorded income from this investment of $242,591 and $2,759,754, respectively, in the accompanying condensed consolidated statements of income and has an investment balance of $11,184,951 and $10,942,360 at June 30, 2017 and December 31, 2016, respectively.
In 2015, the Company also advanced $5,000,000 to UCI for working capital purposes. The subordinated loan accrues interest at the prime rate plus 1%, or 5.25% and 4.75% as of June 30, 2017 and December 31, 2016, respectively, with interest to be paid monthly. Pursuant to the stock purchase agreement, the principal repayment schedule is based on certain contingent criteria. The entire note receivable has been classified as non-current loans receivable - related parties on the condensed consolidated balance sheets as of June 30, 2017 and December 31, 2016 in the amount of $5,000,000.
DMG
On May 14, 2016, David C.P. Chen M.D., Inc., a California professional corporation doing business as Diagnostic Medical Group (“DMG”), David C.P. Chen M.D., individually (collectively “Seller”) and APC-LSMA, a VIE of APC, entered into a share purchase agreement whereby APC-LSMA acquired a 40% ownership interest in DMG for total cash consideration of $1,600,000.
F-138
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
In July 2016, APC advanced $200,000 to DMG pursuant to a promissory note agreement. The note accrued interest at 3.5% per annum and would have matured on June 30, 2018. The balance of $200,000 was collected from DMG during the second quarter of 2017.
During July 2016, APC also contributed its portion of additional capital of $40,000 to DMG for working capital purposes, which represents APC’s 40% investment portion.
APC accounts for its investment in DMG under the equity method of accounting as APC has the ability to exercise significant influence, but not control over DMG’s operations. For the three and six months ended June 30, 2017 and 2016, APC recorded income from this investment of $198,760 and $0 and $560,404 and $0, respectively, in the accompanying condensed consolidated statements of income and has an investment balance of $2,244,102 and $1,683,698 at June 30, 2017 and December 31, 2016, respectively.
PASC
Pacific Ambulatory Surgery Center, LLC (“PASC”), a California limited liability company, is a multi-specialty outpatient surgery center that is certified to participate in the Medicare program and is accredited by the Accreditation Association for Ambulatory Health Care. PASC has entered into agreements with organizations such as healthcare service plans, independent physician practice associations, medical groups and other purchasers of healthcare services for the arrangement of the provision of outpatient surgery center services to subscribers or enrollees of such health plans. On November 15, 2016, PASC and APC, entered into a membership interest purchase agreement whereby PASC sold 40% of its aggregate issued and outstanding membership interests to APC for total consideration of $800,000.
In connection with the membership interest purchase agreement, PASC entered into a management services agreement with NMM, which requires the payment of management fees computed as 2% of PASC revenues, subject to adjustment to a higher tier based on 12-month gross revenues or a maximum of 8% of PASC revenues. The term of the management services agreement commenced on the effective date of November 15, 2016 and extends for a period of 60 months thereafter, and may be extended in writing at the sole option of NMM for an additional period of 60 months following the expiration of the initial term and is automatically renewed for additional consecutive terms of three years unless terminated by either party. PASC shall not be permitted to terminate the management services agreement for any reason during the initial term and, if extended, the extended term.
APC accounts for its investment in PASC under the equity method of accounting as APC has the ability to exercise significant influence, but not control over PASC’s operations. For the three and six months ended June 30, 2017, APC recorded income from this investment of $26,494 and $5,992, respectively, in the accompanying condensed consolidated statements of income and has an investment balance of $785,696 and $779,704 at June 30, 2017 and December 31, 2016, respectively.
F-139
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
APA-ACO
On May 25, 2016, NMM and AMEH established APA-ACO as a joint venture entity to facilitate the member lives acquired by NMM through its acquisitions of AP-ACO and APCN-ACO to NGACO. During the three and six months ended June 30, 2017, NMM’s share in APA-ACO’s net loss was $89,683. As of June 30, 2017, NMM’s share of losses in APA-ACO exceeded its investment in APA-ACO by $89,683. Accordingly, NMM did not account for the losses in APA-ACO, as NMM is not obligated to and does not intend to fund the cash requirements of APA-ACO.
On March 28, 2017, APA-ACO established an irrevocable standby letter of credit with a financial institution for $6,699,329 for the benefit of CMS, which expires on December 31, 2018 and will be automatically extended without amendment for additional one-year periods, unless terminated by the institution prior to 90 days from the expiration date.
AHMC International Cancer Center
On November 15, 2016, APC-LSMA, a VIE of APC, agreed to purchase and acquire from AHMC International Cancer Center (“ICC”) 40% of the aggregate issued and outstanding shares of capital stock of ICC for $400,000 in cash. The closing date of the investment was subject to entering into a shareholder agreement and a management services agreement, both of which occurred on August 1, 2017 and was therefore not accounted for as of June 30, 2017. ICC is a professional medical California corporation and has entered into agreements with organizations such as healthcare service plans, independent physician practice associations, medical groups and other purchasers of medical services (“Healthplans”) for the arrangement of the provision of healthcare services to subscribers or enrollees of said Healthplans. In addition, ICC has entered into written agreements with physicians and other healthcare professionals to provide or arrange for the provision of healthcare services to enrollees of participating Healthplans who have contracted or will contract with ICC for healthcare services. Subsequent to the acquisition, it was agreed that ICC’s working capital needs shall be funded as and when needed through capital contributions and/or subordinated debt by the shareholders of ICC on a pro rata basis based on their respective ownership interests in ICC.
In connection with the share purchase agreement, ICC entered into a management services agreement with NMM, which requires the payment of management fees computed as 2% of ICC revenues, subject to adjustment to a higher tier based on 12-month gross revenues or a maximum of 8% of ICC revenues. The term of the management services agreement commenced on August 1, 2017 and extend for a period of 60 months thereafter, and may be extended in writing at the sole option of NMM for an additional period of 60 months following the expiration of the initial term and is automatically renewed for additional consecutive terms of three years unless terminated by either party. The management services agreement may be terminated by either party if certain metrics specified under Section 5.3 of the management service agreement are not met.
APC accounts for its investment in ICC under the equity method of accounting as APC has the ability to exercise significant influence, but not control over ICC’s operations. The investment of $400,000 was made on September 8, 2017, therefore, no amounts have been recognized for this investment as of June 30, 2017.
F-140
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
Investments in other entities - equity method consists of the following:
| June 30, 2017 |
December 31, 2016 |
|||||||
| LaSalle Medical Associates - IPA Line of Business | $ | 9,017,429 | $ | 9,503,875 | ||||
| Pacific Medical Imaging & Oncology Center, Inc. | 1,456,047 | 1,346,428 | ||||||
| Universal Care, Inc. | 11,184,951 | 10,942,360 | ||||||
| Diagnostic Medical Group | 2,244,102 | 1,683,698 | ||||||
| Pacific Ambulatory Surgery Center, LLC | 785,696 | 779,704 | ||||||
| $ | 24,688,225 | $ | 24,256,065 | |||||
Cost Method
Apollo Medical Holdings, Inc.
On October 14, 2015, the Company invested $10 million in connection with the purchase of shares of Series A preferred stock (“Series A Preferred Stock”) and warrants (“Series A Warrants”) of AMEH, a publicly traded company, in which Dr. Thomas Lam, the CEO of NMM, is also a director.
At the time, the investment represented a 16.9% equity ownership interest of AMEH, and it was determined that NMM does not have the ability to exercise significant influence over the operating and financial policies of AMEH, and as such, is accounted for under the cost method as of June 30, 2017 and December 31, 2016.
On March 30, 2016, NMM purchased 555,555 units of AMEH’s securities for approximately $5,000,000, each unit consisting of one share of Series B convertible preferred stock (“Series B Preferred Stock”) and a stock purchase warrant (a “Series B Warrants”) to purchase one share of AMEH’s common stock at $10.00 per share, none of which securities have yet been converted or exercised for AMEH common stock, but which could result in the issuance by AMEH of up to 1,111,111 shares of AMEH common stock to NMM if they converted all of the Series B Preferred Stock and exercised all of the Series B Warrants that are currently held.
Based on the relative fair values of the investment in the Series A and B preferred stock and the related warrants, the carrying balance of the investment in AMEH as of June 30, 2017 and December 31, 2016 was $10,550,002, and is included in Investments in other entities - cost method in the accompanying condensed consolidated balance sheets.
The Series A and Series B Warrants are accounted for as derivative instruments and recorded at their fair values of $5,466,665 and $5,338,886 (see Note 2) as of June 30, 2017 and December 31, 2016, respectively, and are included in Derivative asset - warrants in the accompanying condensed consolidated balance sheets.
On December 21, 2016, AMEH, entered into an Agreement and Plan of Merger (the “Merger Agreement”) among AMEH, Apollo Acquisition Corp., a California corporation and wholly-owned subsidiary of AMEH (“Merger Subsidiary”), NMM, and Kenneth Sim, M.D., not individually, but in his capacity as the representative of the shareholders of NMM (the “Shareholders’ Representative”).
F-141
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
Thomas Lam, M.D. and Kenneth Sim, M.D. entered into Voting Agreements with AMEH. Under the Voting Agreements, Dr. Sim and Dr. Lam have agreed, among other things, to vote in favor of the approval and adoption of the Merger (as such term is defined below) and the Merger Agreement.
On January 3, 2017, pursuant to a promissory note agreement, NMM provided a loan to AMEH in the principal amount of $5,000,000. The entire outstanding principal amount is due and payable in full on the maturity date of January 3, 2019 and has been classified as non-current loans receivable - related parties on the condensed consolidated balance sheets as of June 30, 2017 in the amount of $5,000,000. Interest accrues at 1% point above the Prime Rate, or 5.25% at June 30, 2017, commencing on the first date of the first month immediately following the execution of the note agreement and is to be paid by AMEH to NMM in successive quarterly installments.
As part of an amendment to the Merger Agreement on March 30, 2017, the merger consideration to be paid by AMEH to NMM was amended to include warrants to purchase 850,000 shares of common stock at an exercise price of $11 per share, that will only be granted in the case that the proposed merger between the NMM and AMEH occurs (such warrant will not vest and will expire if the contemplated merger transaction does not occur), in exchange for NMM providing both a guarantee for AMEH’s convertible note payable to Alliance Apex (“Alliance Note”) and as compensation to NMM for relinquishing their right to additional shares in AMEH based on the agreed upon exchange ratio with NMM in the event that the Alliance Note is converted to AMEH common stock.
| 6. | Accounts Payable and Accrued Expenses |
Accounts payable and accrued expenses consists of the following:
| June 30, 2017 |
December 31, 2016 |
|||||||
| Accounts payable | $ | 55,678 | $ | 420,351 | ||||
| Specialty capitation payable | 518,985 | 678,335 | ||||||
| Subcontractor IPA risk pool payable | 1,381,692 | 1,709,112 | ||||||
| ACA payable | 718,808 | 718,808 | ||||||
| Deferred revenue | 887,868 | 603,041 | ||||||
| Accrued compensation | 996,097 | 2,537,703 | ||||||
| Accrued other | 1,715,428 | 1,415,927 | ||||||
| $ | 6,274,556 | $ | 8,083,277 | |||||
F-142
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
| 7. | Medical Liabilities |
Medical liabilities consists of the following:
| June 30, 2017 |
December 31, 2016 |
|||||||
| Balance, beginning of year | $ | 18,957,465 | $ | 16,011,519 | ||||
| Claims paid for previous year | (16,688,880 | ) | (14,501,482 | ) | ||||
| Incurred health care costs | 50,378,369 | 98,906,764 | ||||||
| Claims paid for current year | (36,167,952 | ) | (84,520,493 | ) | ||||
| Adjustments | 2,040,668 | 3,061,157 | ||||||
| Balance, end of year | $ | 18,519,670 | $ | 18,957,465 | ||||
| 8. | Income Taxes |
The Company accounts for income taxes and the related accounts under the liability method in accordance with ASC Topic 740. Deferred tax assets and liabilities are determined based on the difference between the financial statement and tax bases of assets and liabilities using enacted tax rates expected to be in effect during the year in which the basis differences reverse. Because the Company believes that it is more likely than not that it will realize the full amount of the net deferred tax assets, the Company has not recorded any valuation allowance for the deferred tax assets.
The provision for income taxes for interim periods is based on an estimate of the annual effective tax rate adjusted to reflect the impact of discrete items. Significant management judgment is required in projecting ordinary income (loss) to estimate the Company’s annual effective tax rate.
The Company’s income tax expense of $8.6 million and $5.7 million for the six months ended June 30, 2017 and 2016, respectively, reflects an effective tax rate of 39.8% and 41.5%, respectively. The Company’s income tax expense of $0.7 million and $1.4 million for the three months ended June 30, 2017 and 2016, respectively, reflects an effective tax rate of 35% and 41.7%, respectively. The difference between the effective tax rate and the U.S. statutory tax rate for the three and six months ended June 30, 2017 and 2016 is primarily related to a noncontrolling interest and the dividends received deduction.
As of June 30, 2017 and 2016, the Company does not have any unrecognized tax benefits related to various federal and state income tax matters. The Company will recognize accrued interest and penalties related to unrecognized tax benefits in income tax expense.
APC’s 2015 U.S. Federal tax return was audited by the Internal Revenue Service. The tax liability accrued during 2015 resulting from this audit, which was paid subsequent to June 30, 2017, is not material. The Company does not anticipate a change in its material unrecognized tax benefits within the next 12 months.
F-143
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
| 9. | Mezzanine and Shareholders’ Equity (Deficit) |
All common stock has no par value and is non-transferable and is governed by the stockholders’ agreement. As the redemption feature (see Note 2) of the shares of common stock of NMM was not within the control of the NMM, all common stock and additional paid-in capital did not qualify as permanent equity and was classified as mezzanine or temporary equity as redeemable common stock.
The 24,582,400 shares of common stock classified as treasury stock as of June 30, 2017 and December 31, 2016, represents shares of NMM stock issued to APC. As NMM consolidates APC, such shares are not considered to be outstanding.
NMM
Authorized Share Capital
NMM is authorized to issue 900,000,000 shares of common stock.
During the six months ended June 30, 2017, NMM received cash in the aggregate amount of $248,925 from the exercise of stock options to purchase 1,493,550 shares of NMM common stock at $0.17 per share. In accordance with relevant accounting guidance, the amounts collected are reflected as a long-term liability for unissued equity shares as of June 30, 2017 based on the terms of the forfeiture feature of the option, as noted below.
APC
As the redemption feature (see Note 2) of the shares is not solely within the control of APC, the equity of APC does not qualify as permanent equity and has been classified as noncontrolling interest in mezzanine or temporary equity.
During the six months ended June 30, 2017, APC received cash in the aggregate amount of $176,100 from the exercise of stock options to purchase 1,056,600 shares of APC common stock at $0.17 per share. In accordance with relevant accounting guidance, the amounts collected are reflected as a long-term liability for unissued equity shares as of June 30, 2017 based on the terms of the forfeiture feature of the option, as noted below.
Stock Options
Stock Options Issued Under Primary Care Physician Agreements
On October 1, 2014, NMM and APC entered into an Exclusivity Amendment Agreement as part of the Primary Care Physician Agreement to issue stock options to purchase shares of NMM and APC common stock.
F-144
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
The medical providers agreed to exclusivity to APC for health enrollees in consideration per provider of a sign-on bonus in the amount of $25,000 (or $15,000 if already a preferred provider). The stock options were granted from the date of agreement through May 1, 2015 and are treated as issuances to non-employees. The exercise price of the stock options is $0.167 per share and providers can exercise anytime between August 1, 2015 and October 1, 2019, as long as the providers continue to provide services pursuant to the terms of the agreement through October 1, 2019. If the agreement is terminated by the provider with or without cause, the sign-on bonus and any capitation payment above standard rates made in accordance with the terms of the agreement shall be fully repaid to APC by the terminating medical provider. In addition, any unexercised share options held by the terminating medical provider will be forfeited on effective date of termination, and any share options that have been exercised will be bought back by NMM and APC at the original purchase price.
The stock options under the Exclusivity Amendment Agreement were accounted for at fair value, as determined using the Black-Scholes option pricing model and the following assumptions:
| Six Months ended June 30, | 2017 | 2016 | ||||||
| Expected term | 2.25 years | 3.25 years | ||||||
| Expected volatility | 53.01 | % | 66.62 | % | ||||
| Risk-free interest rate | 1.47 | % | 1.31 | % | ||||
| Market value of common stock | $0.52 - $0.76 | $0.37 - $0.62 | ||||||
| Annual dividend yield | 2.51% - 3.53 % | 0.28% - 0.75 % | ||||||
| Forfeiture rate | 8 | % | 0% -4 % | |||||
The Company’s stock option activity for options grants under the Exclusivity Amendment Agreement for NMM is summarized below:
| Shares | Weighted Average Exercise Price |
Weighted Average Remaining Contractual Term (Years) |
Aggregate Intrinsic Value |
|||||||||||||
| Options outstanding at December 31, 2016 | 2,031,600 | $ | 0.167 | 2.75 | $ | 717,155 | ||||||||||
| Options granted | - | - | - | - | ||||||||||||
| Options exercised | (1,493,550 | ) | 0.167 | - | 527,223 | |||||||||||
| Options forfeited | (538,050 | ) | 0.167 | - | - | |||||||||||
| Options outstanding at June 30, 2017 | - | $ | - | - | $ | - | ||||||||||
F-145
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
The Company’s stock option activity for options grants under the Exclusivity Amendment Agreement for APC is summarized below:
| Shares | Weighted Average Exercise Price |
Weighted Average Remaining Contractual Term (Years) |
Aggregate Intrinsic Value |
|||||||||||||
| Options outstanding at December 31, 2016 | 1,910,400 | $ | 0.167 | 2.75 | $ | 1,138,598 | ||||||||||
| Options granted | - | - | - | - | ||||||||||||
| Options exercised | (1,056,600 | ) | 0.167 | - | 629,734 | |||||||||||
| Options forfeited | - | - | - | - | ||||||||||||
| Options outstanding and exercisable at June 30, 2017 | 853,800 | $ | 0.167 | 2.25 | $ | 508,864 | ||||||||||
The aggregate intrinsic value is calculated as the difference between the exercise price and the estimated fair value of NMM and APC’s common stock as of June 30, 2017.
Share-based compensation expense related to common stock option awards granted in connection with the Exclusivity Amendment Agreement recognized over their respective vesting periods is as follows:
| Six Months ended June 30, | 2017 | 2016 | ||||||
| Contracted physicians and other services | $ | 642,466 | $ | 756,369 | ||||
| Three Months ended June 30, | 2017 | 2016 | ||||||
| Contracted physicians and other services | $ | 321,233 | $ | 378,184 | ||||
The remaining unrecognized share based compensation expense of stock option awards granted in connection with the Exclusivity Amendment Agreement as of June 30, 2017 and 2016 was $991,565 and $1,821,438 for NMM and APC, respectively, which is expected to be recognized over the remaining term of 2.25 years.
Dividends, Reduction of Capital and Distributions
On March 17, 2017, APC paid dividends of $8,750,000 to its shareholders recorded as a reduction of capital as a result of having an accumulated deficit at the time of the declaration.
During the six months ended June 30, 2017, CDSC paid dividends of $740,632.
F-146
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
| 10. | Commitments and Contingencies |
Regulatory Matters
Laws and regulations governing the Medicare program and healthcare generally are complex and subject to interpretation. The Company believes that it is in compliance with all applicable laws and regulations and is not aware of any pending or threatened investigations involving allegations of potential wrongdoing. While no regulatory inquiries have been made, compliance with such laws and regulations can be subject to future government review and interpretation as well as significant regulatory action including fines, penalties, and exclusion from the Medicare and Medi-Cal programs.
As a risk-bearing organization, the Company is required to follow regulations of the California Department of Managed Health Care (“DMHC”). The Company must comply with a minimum working capital requirement, Tangible Net Equity (“TNE”) requirement, cash-to-claims ratio and claims payment requirements prescribed by the DMHC. TNE is defined as net assets less intangibles, less non-allowable assets (which include amounts due from affiliates), plus subordinated obligations. At June 30, 2017 and December 31, 2016, the Company was in compliance with these regulations.
Many of the Company’s payor and provider contracts are complex in nature and may be subject to differing interpretations regarding amounts due for the provision of medical services. Such differing interpretations may not come to light until a substantial period of time has passed following contract implementation. Liabilities for claims disputes are recorded when the loss is probable and can be estimated. Any adjustments to reserves are reflected in current operations.
Legislation and HIPAA
The healthcare industry is subject to numerous laws and regulations of federal, state and local governments. These laws and regulations include, but are not necessarily limited to, matters such as licensure, accreditation, government healthcare program participation requirements, reimbursement for patient services, and Medicare and Medicaid fraud and abuse. Government activity has continued with respect to investigations and allegations concerning possible violations of fraud and abuse statutes and regulations by healthcare providers. Violations of these laws and regulations could result in expulsion from government healthcare programs together with the imposition of significant fines and penalties, as well as significant repayments for patient services previously billed.
The Company believes that it is in compliance with fraud and abuse regulations as well as other applicable government laws and regulations. Compliance with such laws and regulations can be subject to future government review and interpretation as well as regulatory actions unknown or unasserted at this time.
The Health Insurance Portability and Accountability Act (“HIPAA”) assures health insurance portability, reduces healthcare fraud and abuse, guarantees security and privacy of health information, and enforces standards for health information. The Health Information Technology for Economic and Clinical Health Act (“HITECH Act”) expanded upon HIPAA in a number of ways, including establishing notification requirements for certain breaches of protected health information.
F-147
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
In addition to these federal rules, California has also developed strict standards for the privacy and security of health information as well as for reporting certain violations and breaches. The Company may be subject to significant fines and penalties if found not to be compliant with these state or federal provisions.
Affordable Care Act
The Patient Protection and Affordable Care Act (“PPACA”) is resulting in substantial reform in the United States health care system. The legislation impacts multiple aspects of the health care system, including many provisions that change payments from Medicare, Medicaid and insurance companies. Starting in 2014, the legislation required the establishment of health insurance exchanges, which will provide individuals without employer-provided health care coverage the opportunity to purchase insurance. It is anticipated that some employers currently offering insurance to employees will opt to have employees seek insurance coverage through the insurance exchanges. It is possible that the reimbursement rates paid by insurers participating in the insurance exchanges may be substantially different than rates paid under current health insurance products. Another significant component of the PPACA is the expansion of the Medicaid program to a wide range of newly eligible individuals. In anticipation of this expansion, payments under certain existing programs, such as Medicare disproportionate share, will be substantially decreased. Each state’s participation in an expanded Medicaid program is optional. However, the PPACA may be repealed and replaced under the current administration. The potential outcome of the repeal and replacement is unknown at this time and could have a material impact on the Company.
Litigation
The Company is involved from time to time in routine legal matters incidental to its business. In the opinion of the management, resolution of such matters is not expected to have a material effect on its financial position or results of operations.
Liability Insurance
The Company believes that its insurance coverage is appropriate based upon the Company’s claims experience and the nature and risks of the Company’s business. In addition to the known incidents that have resulted in the assertion of claims, the Company cannot be certain that its insurance coverage will be adequate to cover liabilities arising out of claims asserted against the Company, the Company’s affiliated professional organizations or the Company’s affiliated hospitalists in the future where the outcomes of such claims are unfavorable. The Company believes that the ultimate resolution of all pending claims, including liabilities in excess of the Company’s insurance coverage, will not have a material adverse effect on the Company’s financial position, results of operations or cash flows; however, there can be no assurance that future claims will not have such a material adverse effect on the Company’s business. Contracted physicians are required to obtain their own insurance coverage.
Although the Company currently maintains liability insurance policies on a claims-made basis, which are intended to cover malpractice liability and certain other claims, the coverage must be renewed annually, and may not continue to be available to the Company in future years at acceptable costs, and on favorable terms.
F-148
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
| 11. | Lines of Credit |
In April 2012, NMM entered into a promissory note agreement with a bank, which was amended on April 9, 2016 and April 7, 2017 (as amended, the “NMM Business Loan Agreement”). The NMM Business Loan Agreement was amended on April 7, 2017 to increase the loan availability from $10,000,000 to $20,000,000. As of June 30, 2017, NMM was in compliance with the financial debt covenant requirements contained in the loan agreement. As of December 31, 2016, the Company was not in compliance with certain financial debt covenant requirements contained in the loan agreement for which NMM obtained a waiver from the bank. The loan is personally guaranteed by 14 shareholders and a Trust held by NMM’s CEO, 13 of which are also members of the Company’s board of directors. The loan is also collateralized by substantially all assets of NMM. No amounts were outstanding as of June 30, 2017 and December 31, 2016.
In April 2012, APC entered into a promissory note agreement with a bank, which was amended on April 22, 2016 to increase the loan availability from $2,000,000 to $10,000,000. As of June 30, 2017 and December 31, 2016, the Company was not in compliance with certain financial debt covenant requirements contained in the loan agreement for which APC obtained waivers from the bank. The loan is personally guaranteed by 14 shareholders and a Trust held by NMM’s CEO, 13 of which are also members of the Company’s board of directors. The loan is also collateralized by substantially all assets of APC. No amounts were outstanding as of June 30, 2017 and December 31, 2016.
| 12. | Related Party Transactions |
In October 2015, NMM invested $10 million in connection with the purchase of shares of Series A Preferred Stock and Series A Warrants of AMEH in which Dr. Thomas Lam, the CEO of NMM became a director of AMEH. In March 2016, NMM invested an additional $5,000,000 in connection with the purchase of shares of Series B Preferred Stock and Series B Warrants of AMEH. On January 3, 2017, pursuant to a promissory note agreement, NMM provided a loan to AMEH in the principal amount of $5,000,000 (see Note 5). In addition, at June 30, 2017 and December 31, 2016, NMM has a receivable balance of $0 and $200,000, respectively, due from AMEH for reimbursement of expenses included in accounts receivable in the accompanying condensed consolidated balance sheets. In June 2017, AMEH billed NMM $438,307 for its 50% share of the costs related to APA-ACO’s participation in the NGACO Model that AMEH had incurred on behalf of APA-ACO. This amount is included in accounts payable and accrued expenses in the accompanying condensed consolidated balance sheet as of June 30, 2017.
On November 16, 2015, APC entered into a subordinated note receivable agreement with UCI, a 48.9% owned equity method investee, in the amount of $5,000,000 (see Note 5). The note accrues interest at prime plus 1% per annum, or 5.25% and 4.75% at June 30, 2017 and December 31, 2016, respectively. The subordinated note with UCI is classified as a long-term asset as the repayment of the note is contingent upon UCI achieving a specified tangible net equity percentage. As this contingency has not yet been met, it is not probable that the note will be repaid within the next twelve months. At June 30, 2017 and December 31, 2016, the balance of the note was $5,000,000, and is reflected as non-current loans receivable - related parties in the accompanying condensed consolidated balance sheets.
During the three and six months ended June 30, 2017 and 2016, APC paid approximately $62,000 and $69,000, respectively, and approximately $96,000 and $143,000, respectively, to Advance Diagnostic Surgery Center for services as a provider. Advance Diagnostic Surgery Center shares common ownership with certain board members of APC.
F-149
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
During the three and six months ended June 30, 2017 and 2016, NMM received approximately $4.4 million and $4.3 million, respectively, and approximately $8.9 million and $8.5 million, respectively, in management fees from LMA, which is accounted for under the equity method based on 25% equity ownership interest held by APC-LSMA, a VIE of APC (see Note 5).
During the three and six months ended June 30, 2017 and 2016, APC paid approximately $0.6 million and $0.5 million, respectively, and approximately $1.1 million and $0.9 million, respectively, to PMIOC for provider services, which is accounted for under the equity method based on 40% equity ownership interest held by APC-LSMA, a VIE of APC (see Note 5).
During the three and six months ended June 30, 2017 and 2016, APC paid approximately $0.5 million and $0.5 million, respectively, and approximately $1.3 million and $1.1 million, respectively, to AMG, Inc. for services as a provider. AMG, Inc. shares common ownership with certain board members of APC.
During the three and six months ended June 30, 2017 and 2016, APC paid approximately $1.6 million and $1.3 million, respectively, and approximately $3.0 million and $2.4 million, respectively, to DMG for provider services, which is accounted for under the equity method based on 40% equity ownership interest held by APC-LSMA, a VIE of APC (see Note 5).
During the three and six months ended June 30, 2017 and 2016, NMM paid approximately $0.3 million and $0.3 million, respectively, and approximately $0.6 million and $0.6 million, respectively, to Medical Property Partners (“MPP”) for office lease. MPP shares common ownership with certain board members of NMM.
During the three and six months ended June 30, 2017 and 2016, APC paid $90,000 and $90,000, respectively, and $180,000 and $92,200, respectively, to Tag-2 Medical Investment Group, LLC (“Tag-2”) for office lease. Tag-2 shares common ownership with certain board members of APC. APC was also the guarantor for Tag-2’s loan with a bank. In connection with the loan agreement, APC provided collateral to the bank, which represents the $1,000,000 certificate of deposit accounted for as investment in marketable securities. In November 2016, the collateral and guarantee were no longer required, as Tag-2 was able to renew the loan without such collateral and guarantee requirement.
During the three and six months ended June 30, 2017 and 2016, APC paid an aggregate of approximately $6.2 million and $6.5 million, respectively, and approximately $13.6 million and $13.9 million, respectively to shareholders for provider services.
During the three and six months ended June 30, 2017 and 2016, APC paid an aggregate of approximately $3.9 million and $3.8 million, respectively, and approximately $9.3 million and $9.1 million, respectively, to shareholders who are also officers of APC for provider services.
For loans receivable from related parties, see Note 5.
F-150
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
| 13. | Earnings Per Share |
As of June 30, 2017 and 2016, 7,425,900 and 5,932,350 shares in NMM had been issued, respectively, as a result of the exercise of stock options. Despite being legally issued shares, these shares are not considered outstanding due to the forfeiture feature of the stock options (see Note 9), and accordingly these shares are excluded from the basic earnings per share computations and included in the diluted earnings per share computations. In addition, for the three and six months ended June 30, 2017 and 2016, dilutive shares from stock options outstanding of zero and 1,204,095, respectively, and zero and 1,204,095, respectively, are excluded from the basic earnings per share computations as their inclusion would be anti-dilutive and included in the diluted earnings per share computations.
Below is a summary of the earnings per share computations:
| Six months ended June 30, | 2017 | 2016 | ||||||
| Earnings per share - basic | $ | 0.02 | $ | 0.02 | ||||
| Earnings per share - diluted | $ | 0.02 | $ | 0.02 | ||||
| Weighted average shares of common stock outstanding - basic | 366,343,818 | 359,724,706 | ||||||
| Weighted average shares of common stock outstanding - diluted | 373,769,718 | 366,861,151 | ||||||
| Three months ended June 30, | 2017 | 2016 | ||||||
| Earnings per share - basic | $ | 0.01 | $ | 0.01 | ||||
| Earnings per share - diluted | $ | 0.01 | $ | 0.01 | ||||
| Weighted average shares of common stock outstanding - basic | 366,343,818 | 360,537,618 | ||||||
| Weighted average shares of common stock outstanding - diluted | 373,769,718 | 367,674,063 | ||||||
| 14. | Subsequent Events |
The Company has evaluated subsequent events through October 16, 2017, the date the accompanying condensed consolidated financial statements were available to be issued, and determined that except as disclosed in the accompanying notes, no subsequent events have occurred that would require recognition in the condensed consolidated financial statements or disclosure in the notes thereto.
F-151
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
On September 27, 2017, with an effective date of January 1, 2018, NMM entered into a Management Services Agreement (“MSA”) with Joseph M. Molina, M.D., Professional Corporation - Southern California dba Golden Shore Medical Group, a California Professional Corporation (“GSMG”). The MSA requires the payment of management fees in accordance with the management fee schedule therein. The term of the MSA will commence on the effective date through December 31, 2020, and may be extended in writing at the sole option of GSMG for an additional two year term following the expiration of the initial term. GSMG will have the right to terminate the MSA if certain conditions, as defined in the MSA, are met.
On October 9, 2017 (“Effective Date”), NMM and APC-LSMA entered into an agreement with Accountable Health Care IPA (“Accountable”), a California professional medical corporation, Signal Health Solutions, Inc. (“Signal”), a California corporation and George M. Jayatilaka, M.D. (“Dr. Jay”), individually, whereby concurrent with the execution of the agreement, APC-LSMA will extend a line of credit to Dr. Jay in the principal amount of up to $10,000,000 (“Dr. Jay Loan”) to fund the working capital needs of Accountable. The line of credit may be funded in installments, as needed by Accountable and as determined from time to time by APC-LSMA. Interest on the Dr. Jay Loan accrues at a rate that is equal to the prime rate plus 1% and payable in monthly installments of interest only on the first day of each month until the date that is 3 years following the initial date of funding, at which time, all outstanding principal and accrued interest thereon shall be due and payable in full. The Dr. Jay Loan will not be subordinated. The Dr. Jay Loan shall at all times be secured by a first-lien security interest in shares of Accountable owned by Dr. Jay.
Concurrently with the funding of the Dr. Jay Loan, Dr. Jay will loan to Accountable the entire proceeds of the Dr. Jay Loan at the same interest rate and maturity date as the Dr. Jay Loan (Dr. Jay-Accountable Subordinated Loan”). Repayment of the Dr. Jay-Accountable Subordinated Loan will be subordinated to Accountable’s creditors in a manner acceptable to the DMHC.
At any time on or before the date that is one year following the initial funding date of the Dr. Jay Loan, APC-LSMA or its designee shall have the right, but not the obligation, to convert up to $5,000,000 of the principal amount into shares of Accountable’s capital stock. At any time after the date that is one year following the funding date, the Dr. Jay Loan may be prepaid at any time. Within three years following the initial funding of the Dr. Jay Loan, APC-LSMA or its designee shall have the right, but not the obligation, to convert the then outstanding principal amount into Accountable shares based on Accountable’s then-current valuation.
F-152
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
Subsequent to the funding of the Dr. Jay Loan, to the extent needed by Accountable for working capital needs at determined by APC-LSMA, APC-LSMA will extend an additional line of credit in the principal amount up to $8,000,000. The funding mechanism, interest rate and maturity date of such additional line of credit shall be the same as the Dr. Jay Loan and additional collateral security in Accountable’s issued and outstanding shares will be required.
As a condition of funding the Dr. Jay Loan, Accountable entered into a management service agreement with NMM to commence on the termination of the Accountable's existing management agreement with MedPoint Management (currently anticipated to be on or about November 1, 2017) and have a term of ten (10) years from its Effective Date. NMM will be responsible for managing 100% of all health plan membership assigned and delegated to Accountable, and all hospital risk pools. The management service agreement requires the payment of IPA management fees as set forth therein.
Concurrent with the initial funding of the Dr. Jay Loan, the Accountable Board of Directors shall be automatically reconstituted to be comprised of two directors, which will comprise of Dr. Jay and a director appointed by APC-LSMA. Dr. Jay and APC-LSMA will have two and one votes as a director, respectively.
Amendment to Merger Agreement and Loan Receivable from AMEH
On October 16,2017, NMM and AMEH entered into an agreement (“Amendment No. 2 to Agreement and Plan of Merger”) to amend certain terms of the Merger Agreement, which include the following (i) issuance of an aggregate of 1,666,666 additional common shares and 900,000 common shares associated with the convertible promissory note, as described below, (ii) issuance of an aggregate of additional 900,000 five-year warrants to NMM shareholders exercisable at $10.00 per share, (iii) issuance of a convertible promissory note of $9,000,000 from NMM to AMEH to replace the $5,000,000 working capital loan, as further described below; and (iv) extend the merger date from August 31, 2017 to March 31, 2018.
On October 16, 2017, concurrent with the execution of the Amendment No. 2 to Agreement and Plan of Merger, NMM and AMEH entered into an Amended and Restated Convertible Promissory Note to increase the $5,000,000 working capital loan (see Note 5) by an additional principal amount of $4,000,000, which comprises the aggregate principal amount of $9,000,000 evidenced by this note (“Convertible Note”). Upon its execution, (i) this Convertible Note shall amend, restate and replace the $5,000,000 working capital loan, which shall thereupon be canceled, and (ii) the entire outstanding principal balance of the original loan, all accrued and unpaid interest thereon, and all other applicable fees, costs and charges, if any, shall be rolled into and become payable pursuant to the terms of this Convertible Note. Within 10 business days prior to maturity, NMM shall have the right (but not the obligation) in its sole discretion to convert the Convertible Note into shares of AMEH at a conversion price of $10.00 per share. The note is convertible into shares of AMEH common stock at a price of $10.00 per share, subject to standard anti-dilution clauses.
F-153
Network Medical Management, Inc.
Notes to Condensed Consolidated Financial Statements (Unaudited)
In the event AMEH fails to repay the Alliance Note in full when due, NMM acknowledges, agrees and undertakes (regardless of whether demand has been made under the NMM Guaranty by Alliance Apex) to pay to Alliance Apex all amounts owed by AMEH to Alliance Apex under the Alliance Note or enter into another agreement with Alliance Apex, in either case such that the Alliance Apex Note shall be cancelled and AMEH shall have no further obligation thereunder. Upon NMM’s payment to Alliance Apex or entering into another agreement with Alliance Apex as set forth above, (i) the convertible loan amount under this Convertible Note shall be increased to $13,990,000 in the aggregate, and all references in this Convertible Note to the convertible loan amount shall mean that increased amount; and (ii) the entire outstanding principal balance of the Alliance Note, all accrued and unpaid interest thereon, and all other applicable fees, costs and charges under the Alliance Note, if any, shall be evidenced by, and become payable on the Maturity Date, as defined below, or earlier pursuant to the terms of this Convertible Note.
The "Maturity Date" shall mean the date that is the earlier of (i) March 31, 2019; or (ii) the date that is twelve (12) months after the date the Merger Agreement is terminated for any reason pursuant to the terms thereof, at which time (but subject to the exercise of the NMM conversion option, as defined in the agreement), all of the following shall be due and payable in full: (A) the entire principal balance hereof, all accrued interest thereon, and all other applicable fees, costs and charges hereunder, if any, plus (B) all accrued interest under the original loan up to and including the date of cancellation thereof, and all other applicable fees, costs and charges thereunder, if any, plus (C) all accrued interest under the Alliance Note up to and including the date of cancellation thereof, and all other applicable fees, costs and charges thereunder, if any. Interest accrues at 1% point above the Prime Rate, commencing on the first date of the first month immediately following the execution of the Convertible Note agreement and is to be paid by AMEH to NMM in successive quarterly installments.
F-154
CONSOLIDATED FINANCIAL STATEMENTS - TABLE OF CONTENTS:
F-155
Report of Independent Registered Public Accounting Firm
Board of Directors and Stockholders
Apollo Medical Holdings, Inc.
Glendale, California
We have audited the accompanying consolidated balance sheets of Apollo Medical Holdings, Inc. (“Company”) as of March 31, 2017 and 2016 and the related consolidated statements of operations, stockholders’ equity (deficit), and cash flows for the years then ended. These financial statements are the responsibility of the Company’s management. Our responsibility is to express an opinion on these financial statements based on our audits.
We conducted our audits in accordance with the standards of the Public Company Accounting Oversight Board (United States). Those standards require that we plan and perform the audits to obtain reasonable assurance about whether the financial statements are free of material misstatement. The Company is not required to have, nor were we engaged to perform, an audit of its internal control over financial reporting. Our audits included consideration of internal control over financial reporting as a basis for designing audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the Company’s internal control over financial reporting. Accordingly, we express no such opinion. An audit also includes examining, on a test basis, evidence supporting the amounts and disclosures in the financial statements, assessing the accounting principles used and significant estimates made by management, as well as evaluating the overall financial statement presentation. We believe that our audits provide a reasonable basis for our opinion.
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of Apollo Medical Holdings, Inc. at March 31, 2017 and 2016, and the results of its operations and its cash flows for the years then ended, in conformity with accounting principles generally accepted in the United States of America.
The accompanying consolidated financial statements have been prepared assuming that the Company will continue as a going concern. As described in Note 1 to the consolidated financial statements, the Company has suffered recurring losses from operations and has generated negative cash flows from operations since inception, resulting in an accumulated deficit of $37.7 million as of March 31, 2017. These factors among others raise substantial doubt about its ability to continue as a going concern. Management's plans in regard to these matters are also described in Note 1. The consolidated financial statements do not include any adjustments that might result from the outcome of this uncertainty.
/s/ BDO USA, LLP
Los Angeles, California
June 29, 2017
F-156
Consolidated Financial Statements
CONSOLIDATED BALANCE SHEETS
| March 31, | ||||||||
| 2017 | 2016 | |||||||
| ASSETS | ||||||||
| Cash and cash equivalents | $ | 8,664,211 | $ | 9,270,010 | ||||
| Accounts receivable, net of allowance for doubtful accounts of $475,080 and $601,000 at March 31, 2017 and 2016, respectively | 5,506,472 | 3,392,941 | ||||||
| Other receivables | 464,085 | 581,213 | ||||||
| Due from Affiliates | 18,314 | 20,505 | ||||||
| Prepaid expenses and other current assets | 269,168 | 293,828 | ||||||
| Total current assets | 14,922,250 | 13,558,497 | ||||||
| Deferred financing costs, net | - | 37,926 | ||||||
| Property and equipment, net | 1,205,139 | 1,247,973 | ||||||
| Restricted cash | 765,058 | 530,000 | ||||||
| Intangible assets, net | 1,904,269 | 2,353,212 | ||||||
| Goodwill | 1,622,483 | 1,622,483 | ||||||
| Other assets | 225,358 | 216,442 | ||||||
| TOTAL ASSETS | $ | 20,644,557 | $ | 19,566,533 | ||||
| LIABILITIES, MEZZANINE EQUITY AND STOCKHOLDERS’ EQUITY | ||||||||
| Accounts payable and accrued liabilities | $ | 7,883,373 | $ | 4,572,307 | ||||
| Medical liabilities | 1,768,231 | 2,670,709 | ||||||
| Convertible note payable, net of debt issuance cost of $161,000 | 4,829,000 | - | ||||||
| Lines of credit | 62,500 | 188,764 | ||||||
| Total current liabilities | 14,543,104 | 7,431,780 | ||||||
| Note payable – related party | 5,000,000 | - | ||||||
| Warrant liability | - | 2,811,111 | ||||||
| Deferred rent liability | 747,418 | 728,877 | ||||||
| Deferred tax liability | 83,667 | 43,479 | ||||||
| Total liabilities | 20,374,189 | 11,015,247 | ||||||
| COMMITMENTS AND CONTINGENCIES (Note 10) | ||||||||
| MEZZANINE EQUITY | ||||||||
| Series A Preferred stock, par value $0.001; 5,000,000 shares authorized (inclusive of Series B Preferred stock); 1,111,111 issued and outstanding as of March 31, 2016, Liquidation preference of $9,999,999 at March 31, 2016 | - | 7,077,778 | ||||||
| STOCKHOLDERS’ EQUITY | ||||||||
| Series A Preferred stock, par value $0.001; 5,000,000 shares authorized (inclusive of Series B Preferred stock); 1,111,111 issued and outstanding as of March 31, 2017, Liquidation preference of $9,999,999 at March 31, 2017 | 7,077,778 | - | ||||||
| Series B Preferred stock, par value $0.001; 5,000,000 shares authorized (inclusive of Series A Preferred stock) 555,555 issued and outstanding as of March 31, 2017 and 2016, Liquidation preference of $4,999,995 at March 31, 2017 and 2016 | 3,884,745 | 3,884,745 | ||||||
| Common stock, par value $0.001; 100,000,000 shares authorized, 6,033,518 and 5,876,852 shares issued and outstanding at March 31, 2017 and 2016, respectively | 6,033 | 5,876 | ||||||
| Additional paid-in capital | 26,331,948 | 23,524,517 | ||||||
| Accumulated deficit | (37,654,381 | ) | (28,684,565 | ) | ||||
| Stockholders’ deficit attributable to Apollo Medical Holdings, Inc. | (353,877 | ) | (1,269,427 | ) | ||||
| Noncontrolling interest | 624,245 | 2,742,935 | ||||||
| Total stockholders’ equity | 270,368 | 1,473,508 | ||||||
| TOTAL LIABILITIES, MEZZANINE EQUITY AND STOCKHOLDERS’ EQUITY | $ | 20,644,557 | $ | 19,566,533 | ||||
The accompanying notes are an integral part of these consolidated financial statements
F-157
CONSOLIDATED STATEMENTS OF OPERATIONS
| For The Years Ended March 31, | ||||||||
| 2017 | 2016 | |||||||
| Net revenues | $ | 57,427,701 | $ | 44,048,740 | ||||
| Costs and expenses: | ||||||||
| Cost of services | 48,735,537 | 34,000,786 | ||||||
| General and administrative | 18,583,372 | 16,962,687 | ||||||
| Depreciation and amortization | 645,742 | 351,396 | ||||||
| Total costs and expenses | 67,964,651 | 51,314,869 | ||||||
| Loss from operations | (10,536,950 | ) | (7,266,129 | ) | ||||
| Other income (expense) : | ||||||||
| Interest expense | (82,905 | ) | (542,296 | ) | ||||
| Gain (loss) on change in fair value of warrant and conversion feature liabilities | 1,633,333 | (408,692 | ) | |||||
| Gain on deconsolidation of variable interest entity | 242,411 | - | ||||||
| Loss on debt extinguishment | - | (266,366 | ) | |||||
| Other income | 14,701 | 239,057 | ||||||
| Total other income (expense), net | 1,807,540 | (978,297 | ) | |||||
| Loss before benefit from income taxes | (8,729,410 | ) | (8,244,426 | ) | ||||
| Benefit from income taxes | (47,495 | ) | (71,037 | ) | ||||
| Net loss | (8,681,915 | ) | (8,173,389 | ) | ||||
| Net income attributable to noncontrolling interests | 287,901 | 1,170,655 | ||||||
| Net loss attributable to Apollo Medical Holdings, Inc. | $ | (8,969,816 | ) | $ | (9,344,044 | ) | ||
| Net loss per share: | ||||||||
| Basic and diluted | $ | (1.49 | ) | $ | (1.79 | ) | ||
| Weighted average shares of common stock outstanding: | ||||||||
| Basic and diluted | 6,001,680 | 5,212,927 | ||||||
The accompanying notes are an integral part of these consolidated financial statements
F-158
CONSOLIDATED STATEMENTS OF STOCKHOLDERS’ EQUITY (DEFICIT)
For the Years Ended March 31, 2017 and 2016
| Additional | Stockholders’ | |||||||||||||||||||||||||||||||||||||||
| Preferred Stock – Series A | Preferred Stock – Series B | Common Stock | Paid-in | Accumulated | Noncontrolling | (Deficit) | ||||||||||||||||||||||||||||||||||
| Shares | Amount | Shares | Amount | Shares | Amount | Capital | Deficit | Interests | Equity | |||||||||||||||||||||||||||||||
| Balance April 1, 2015 | - | $ | - | - | $ | - | 4,863,389 | $ | 4,863 | $ | 16,517,985 | $ | (19,340,521 | ) | $ | 1,827,489 | $ | (990,184 | ) | |||||||||||||||||||||
| Net income (loss) | - | - | - | - | - | - | - | (9,344,044 | ) | 1,170,655 | (8,173,389 | ) | ||||||||||||||||||||||||||||
| Stock-based compensation expense | - | - | - | - | - | - | 1,103,976 | - | - | 1,103,976 | ||||||||||||||||||||||||||||||
| Issuance of common stock in acquisition | - | - | - | - | 275,000 | 275 | 1,512,225 | - | - | 1,512,500 | ||||||||||||||||||||||||||||||
| Distributions to noncontrolling interest | - | - | - | - | - | - | - | - | (702,642 | ) | (702,642 | ) | ||||||||||||||||||||||||||||
| Reclassification of noncontrolling interest to notes receivable | - | - | - | - | - | - | - | - | 414,716 | 414,716 | ||||||||||||||||||||||||||||||
| Net adjustment from change in APS ownership interest | - | - | - | - | - | - | (338,032 | ) | - | 32,717 | (305,315 | ) | ||||||||||||||||||||||||||||
| Conversion of 9% notes to common stock | - | - | - | - | 138,463 | 138 | 553,713 | - | - | 553,851 | ||||||||||||||||||||||||||||||
| Conversion of 8% notes and warrants to common stock | - | - | - | - | 600,000 | 600 | 3,059,400 | - | - | 3,060,000 | ||||||||||||||||||||||||||||||
| Issuance of preferred stock and equity warrant | - | - | 555,555 | 3,884,745 | - | - | 1,115,250 | - | - | 4,999,995 | ||||||||||||||||||||||||||||||
| Balance at March 31, 2016 | - | - | 555,555 | 3,884,745 | 5,876,852 | 5,876 | 23,524,517 | (28,684,565 | ) | 2,742,935 | 1,473,508 | |||||||||||||||||||||||||||||
| Net income (loss) | - | - | - | - | - | (8,969,816 | ) | 287,901 | (8,681,915 | ) | ||||||||||||||||||||||||||||||
| Stock-based compensation expense | - | - | - | - | - | - | 1,106,454 | - | - | 1,106,454 | ||||||||||||||||||||||||||||||
| Issuance of common stock for exercise of warrants | - | - | - | - | 150,000 | 150 | 171,850 | - | - | 172,000 | ||||||||||||||||||||||||||||||
| Issuance of common stock for vested restricted stock | - | - | - | - | 6,666 | 7 | 61 | - | - | 68 | ||||||||||||||||||||||||||||||
| Relative fair value of warrants issued with debt | - | - | - | - | - | - | 6,880 | - | - | 6,880 | ||||||||||||||||||||||||||||||
| Reclassification of Noncontrolling interest due to acquisition of VIE | - | - | - | - | - | - | 183,408 | - | (183,408 | ) | - | |||||||||||||||||||||||||||||
| Distributions to noncontrolling interest | - | - | - | - | - | - | - | - | (1,200,000 | ) | (1,200,000 | ) | ||||||||||||||||||||||||||||
| Deconsolidation of VIEs, | - | - | - | - | - | - | - | - | (1,023,183 | ) | (1,023,183 | ) | ||||||||||||||||||||||||||||
| Warrants issuable for debt guarantee | - | - | - | - | - | - | 161,000 | - | - | 161,000 | ||||||||||||||||||||||||||||||
| Reclassification of mezzanine equity to permanent equity | 1,111,111 | 7,077,778 | - | - | - | - | - | - | - | 7,077,778 | ||||||||||||||||||||||||||||||
| Reclassification of derivative liability to equity | - | - | - | - | - | - | 1,177,778 | - | - | 1,177,778 | ||||||||||||||||||||||||||||||
| Balance at March 31, 2017 | 1,111,111 | $ | 7,077,778 | 555,555 | $ | 3,884,745 | 6,033,518 | $ | 6,033 | $ | 26,331,948 | $ | (37,654,381 | ) | $ | 624,245 | $ | 270,368 | ||||||||||||||||||||||
The accompanying notes are an integral part of these consolidated financial statements
F-159
CONSOLIDATED STATEMENTS OF CASH FLOWS
| For The Years Ended March 31, | ||||||||
| 2017 | 2016 | |||||||
| CASH FLOWS FROM OPERATING ACTIVITIES: | ||||||||
| Net loss | $ | (8,681,915 | ) | $ | (8,173,389 | ) | ||
| Adjustments to reconcile net loss to net cash used in operating activities: | ||||||||
| Provision for doubtful accounts | 385,597 | 435,838 | ||||||
| Depreciation and amortization | 645,742 | 351,396 | ||||||
| Loss on disposal of assets | 6,938 | 476,745 | ||||||
| Deferred income taxes | 40,188 | (127,736 | ) | |||||
| Stock-based compensation expense | 1,106,454 | 1,103,976 | ||||||
| Gain on deconsolidation of variable interest entity | (242,411 | ) | - | |||||
| Loss on debt extinguishment | - | 266,366 | ||||||
| Amortization of deferred financing costs | 44,806 | 94,912 | ||||||
| Write-off of capitalized offering costs | - | 513,646 | ||||||
| Amortization adjustment to debt discount | - | (29,984 | ) | |||||
| Change in fair value of warrant and conversion feature liability | (1,633,333 | ) | 408,692 | |||||
| Impairment of goodwill and intangible assets | 68,311 | 207,285 | ||||||
| Changes in assets and liabilities: | ||||||||
| Accounts receivable | (2,780,122 | ) | (27,195 | ) | ||||
| Other receivables | 113,303 | 283,704 | ||||||
| Due from affiliates | 2,191 | 15,892 | ||||||
| Prepaid expenses and other current assets | (10,158 | ) | (92,182 | ) | ||||
| Deferred financing costs | - | (43,330 | ) | |||||
| Other assets | (8,916 | ) | 3,181 | |||||
| Accounts payable and accrued liabilities | 3,653,211 | 1,024,991 | ||||||
| Deferred rent liability | 53,514 | 57,907 | ||||||
| Medical liabilities | (902,478 | ) | 1,410,160 | |||||
| Net cash used in operating activities | (8,139,078 | ) | (1,839,125 | ) | ||||
| Cash flows from investing activities: | ||||||||
| Change in restricted cash | (235,058 | ) | - | |||||
| Proceeds from sale of ACC assets | - | 15,000 | ||||||
| Decrease in cash and cash equivalents resulting from deconsolidation of variable interest entities | (858,670 | ) | - | |||||
| Property and equipment acquired | (297,561 | ) | (262,108 | ) | ||||
| Net cash used in investing activities | (1,391,289 | ) | (247,108 | ) | ||||
| Cash flows from financing activities: | ||||||||
| Proceeds from the issuance of Series A preferred stock and warrants | - | 10,000,000 | ||||||
| Proceeds from the issuance of Series B preferred stock and warrants | - | 4,999,995 | ||||||
| Proceeds from issuance of convertible note payable | 4,990,000 | - | ||||||
| Proceeds from issuance of note payable – related party | 5,000,000 | - | ||||||
| Repayments on convertible notes | - | (470,000 | ) | |||||
| Proceeds from notes payable | 400,000 | 100,000 | ||||||
| Principal payments on notes payable | (400,000 | ) | (6,527,500 | ) | ||||
| Proceeds from line of credit | 112,500 | - | ||||||
| Repayments on lines of credit | (150,000 | ) | (1,006,000 | ) | ||||
| Distributions to noncontrolling interest | (1,200,000 | ) | (702,642 | ) | ||||
| Proceeds from exercise of warrants and vested restricted stock | 172,068 | - | ||||||
| Proceeds from issuance of common stock | - | 200,000 | ||||||
| Payment to noncontrolling interest for equity interest | - | (251,852 | ) | |||||
| Net cash provided by financing activities | 8,924,568 | 6,342,001 | ||||||
F-160
APOLLO MEDICAL HOLDINGS, INC.
CONSOLIDATED STATEMENTS OF CASH FLOWS - CONTINUED
| For The Years Ended March 31, | ||||||||
| 2017 | 2016 | |||||||
| Net change in cash and cash equivalents | (605,799 | ) | 4,255,768 | |||||
| Cash and cash equivalents, beginning of year | 9,270,010 | 5,014,242 | ||||||
| Cash and cash equivalents, end of year | $ | 8,664,211 | $ | 9,270,010 | ||||
| SUPPLEMENTARY DISCLOSURES OF CASH FLOW INFORMATION: | ||||||||
| Interest paid | $ | 23,532 | $ | 521,341 | ||||
| Income taxes paid | 30,902 | 176,587 | ||||||
| NON-CASH FINANCING ACTIVITIES: | ||||||||
| Issuance of common stock on conversion of 8% warrants and notes | $ | - | $ | 3,060,000 | ||||
| Issuance of common stock in connection with conversion of 9% notes payable and accrued interest | - | 553,851 | ||||||
| Change in noncontrolling interest ownership | - | 338,032 | ||||||
| Tenant improvement allowance | - | 659,360 | ||||||
| Note receivable related to sale of ACC asset | - | 51,000 | ||||||
| Convertible debt reclassified to accounts payable | - | 100,000 | ||||||
| Common stock issued for acquisition of intangible assets | - | 1,312,500 | ||||||
| Reclassification of derivative liability to equity | 1,177,778 | - | ||||||
| Relative fair value of warrant included in debt discount | 6,880 | - | ||||||
| Reclassification of mezzanine equity to permanent equity | 7,077,778 | - | ||||||
| Reclassification of noncontrolling interest to due to acquisition of BAHA noncontrolling interest | 183,408 | - | ||||||
| Warrants issuable for debt guarantee | 161,000 | - | ||||||
The accompanying notes are an integral part of these consolidated financial statements
F-161
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
1. Description of Business
Apollo Medical Holdings, Inc. (the “Company” or “ApolloMed”) and its affiliated physician groups are a physician-centric integrated population health management company working to provide coordinated, outcomes-based medical care in a cost-effective manner. Led by a management team with over a decade of experience, ApolloMed has built a company and culture that is focused on physicians providing high-quality medical care, population health management and care coordination for patients, particularly senior patients and patients with multiple chronic conditions. ApolloMed believes that the Company is well-positioned to take advantage of changes in the rapidly evolving U.S. healthcare industry, as there is a growing national movement towards more results-oriented healthcare centered on the triple aim of patient satisfaction, high-quality care and cost efficiency.
ApolloMed serves Medicare, Medicaid and health maintenance organization (“HMO”) patients, and uninsured patients, in California. The Company primarily provides services to patients who are covered predominately by private or public insurance, although the Company derives a small portion of its revenue from non-insured patients. The Company provides care coordination services to each major constituent of the healthcare delivery system, including patients, families, primary care physicians, specialists, acute care hospitals, alternative sites of inpatient care, physician groups and health plans.
ApolloMed’s physician network consists of hospitalists, primary care physicians and specialist physicians primarily through ApolloMed’s owned and affiliated physician groups. ApolloMed operates through the following subsidiaries: Apollo Medical Management, Inc. (“AMM”), Pulmonary Critical Care Management, Inc. (“PCCM”), Verdugo Medical Management, Inc. (“VMM”), ApolloMed Accountable Care Organization, Inc. (“ApolloMed ACO”), and Apollo Care Connect, Inc. (“ApolloCare”).
Through its wholly-owned subsidiary, AMM, ApolloMed manages affiliated medical groups, which consist of ApolloMed Hospitalists (“AMH”), a hospitalist company, ApolloMed Care Clinic (“ACC”), Maverick Medical Group, Inc. (“MMG”), AKM Medical Group, Inc. (“AKM”), Southern California Heart Centers (“SCHC”), Bay Area Hospitalist Associates, A Medical Corporation (“BAHA”) and APA ACO, Inc. (“APAACO”). Through its wholly-owned subsidiary PCCM, ApolloMed manages Los Angeles Lung Center (“LALC”) (see below for deconsolidation), and through its wholly-owned subsidiary VMM, ApolloMed manages Eli Hendel, M.D., Inc. (“Hendel”) (see below for deconsolidation). ApolloMed also has a controlling interest in ApolloMed Palliative Services, LLC (“APS”), which owns two Los Angeles-based companies, Best Choice Hospice Care LLC (“BCHC”) and Holistic Health Home Health Care Inc. (“HCHHA”).
AMM, PCCM and VMM each operate as a physician practice management company and are in the business of providing management services to physician practice corporations under long-term management service agreements, pursuant to which AMM, PCCM or VMM, as applicable, manages all non-medical services for the affiliated medical group and has exclusive authority over all non-medical decision making related to ongoing business operations.
ApolloMed ACO participates in the Medicare Shared Savings Program (“MSSP”), the goal of which is to improve the quality of patient care and outcomes through more efficient and coordinated approach among providers. Revenues earned by ApolloMed ACO are uncertain, and, if such amounts are payable by the Centers for Medicare & Medicaid Services (“CMS”), they will be paid on an annual basis significantly after the time earned, and are contingent on various factors, including achievement of the minimum savings rate as determined by MSSP for the relevant period. Such payments are earned and made on an “all or nothing” basis. CMS determined that the Company did not meet the minimum savings threshold in performance year 2015 and therefore did not receive the “all or nothing” annual shared savings payment in fiscal 2017. The Company is eligible to be considered for an “all or nothing” payment under this program for performance year 2016 (which, if it is paid, would be paid to us in fiscal 2018).
In January 2016, the Company formed ApolloCare, which acquired certain technology and other assets of Healarium, Inc., which provides the Company with a cloud and mobile-based population health management platform that includes digital care plans, a case management module, connectivity with multiple healthcare tracking devices and the ability to integrate with multiple electronic health records to capture clinical data.
During fiscal 2016, the Company combined the operations of AKM into those of MMG.
On March 1, 2016, the Company sold substantially all the assets of ACC to an unrelated third party. As the Company still operates various clinics, the sale was not deemed to represent a strategic shift in the Company’s operations and therefore not considered a discontinued operation.
In November 2016, BAHA Acquisition Corp., an affiliated entity owned by the Company’s CEO and consolidated as a variable interest entity, acquired the noncontrolling interest in BAHA which was previously consolidated as a variable interest entity, and continues to have its financial results consolidated with those of the Company as a variable interest entity. As part of the transaction, the Company acquired the noncontrolling interest of BAHA and was reflected as an equity transaction as there was no change in control.
On December 21, 2016, the Company, entered into an Agreement and Plan of Merger (the “Merger Agreement”) among the Company, Apollo Acquisition Corp., a California corporation and wholly-owned subsidiary of the Company (“Merger Subsidiary”), Network Medical Management (“NMM”), and Kenneth Sim, M.D., not individually but in his capacity as the representative of the shareholders of NMM (the “Shareholders’ Representative”) (see Note 10).
F-162
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
On January 1, 2017, PCCM and VMM amended the management services agreements entered into with LALC and Hendel. Based on the Company’s evaluation of current accounting guidance, it was determined that the Company no longer holds an explicit or implicit variable interest in these entities, and accordingly LALC and Hendel are no longer consolidated and their operations are not included in the March 31, 2017 consolidated financial statements of the Company as of such date. In connection with the amendments, the Company recorded a gain on deconsolidation of $242,411 in the consolidated statement of operations, the deconsolidation of the net assets of the LALC and Hendel entities and related noncontrolling interest of $1,023,183 in the consolidated balance sheet, and a decrease in cash and cash equivalents and in the consolidated statements of cash flows in the amount of $858,670.
On January 18, 2017, CMS announced that APAACO, which is owned 50% by ApolloMed and 50% by Network Medical Management, Inc. has been approved to participate in the Next Generation ACO Model “NGACO Model”. Through this new model, CMS will partner with APAACO and other ACOs experienced in coordinating care for populations of patients and whose provider groups are willing to assume higher levels of financial risk and reward under the NGACO Model. The NGACO program began on January 1, 2017.
In connection with the approval by CMS for APAACO to participate in the NGACO Model, CMS and APAACO have entered into the Participation Agreement. The term of the Participation Agreement is two performance years, through December 31, 2018. CMS may offer to renew the Participation Agreement for an additional two performance years. Additionally, the Participation Agreement may be terminated sooner by CMS as specified therein.
Going Concern, Liquidity and Capital Resources
The consolidated financial statements are prepared in accordance with accounting principles generally accepted in the United States of America (“U.S. GAAP”) and have been prepared on a going concern basis, which contemplates the realization of assets and settlement of liabilities in the normal course of business.
As shown in the accompanying consolidated financial statements, the Company has a history of operating losses. The Company had a net loss of approximately $8.7 million and approximately $8.2 million for the years ended March 31, 2017 and 2016, respectively. The Company had negative cash flow from operations of approximately $8.1 million and approximately $1.8 million for the years ended March 31, 2017 and 2016, respectively.
As of March 31, 2017, the Company had an accumulated deficit of approximately $37.7 million. At March 31, 2017, the Company had cash equivalents of approximately $8.7 million compared to cash and cash equivalents of approximately $9.3 million at March 31, 2016. At March 31, 2017, the Company had net borrowings from notes and lines of credit totaling approximately $9.9 million compared to net borrowings at March 31, 2016 of approximately $0.2 million and availability under lines of credit of approximately $0.2 million.
These factors among others raise substantial doubt about the Company’s ability to continue as a going concern. The Company’s long-term ability to continue as a going concern is dependent upon the Company’s ability to increase revenue, reduce costs, achieve a satisfactory level of profitable operations, and obtain additional sources of suitable and adequate financing. The consolidated financial statements do not include any adjustments relating to the recoverability and classification of recorded assets, or the amounts and classification of liabilities that might be necessary in the event that the Company cannot continue as a going concern. The Company’s ability to continue as a going concern is also dependent on management’s ability to further develop business operations. The Company may also have to reduce certain overhead costs through the reduction of salaries and other means, and settle liabilities through negotiation. There can be no assurance that management’s attempts at any or all of these endeavors will be successful.
To date, the Company has funded the Company’s operations from a combination of internally generated cash flow and external sources, including the proceeds from the issuance of equity and/or debt securities. The Company expects to continue to fund the Company’s working capital requirements, capital expenditures and payments of principal and interest on outstanding indebtedness, with cash on hand, cash flows from operations, available borrowings under the Company’s lines of credit and, if available, additional financings of equity and/or debt. Management does not believe that the Company has sufficient liquidity to meet the Company’s obligations for at least the next twelve months without some additional funds, such as funds available from raising capital. However, no assurance can be given that any such funds will be available at all or available on favorable terms. The Company is substantially dependent upon the consummation of the Merger to meet the Company’s liquidity requirements. See “NMM Transaction” in Note 10.
F-163
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
2. Summary of Significant Accounting Policies
Principles of Consolidation
The Company’s consolidated financial statements include the accounts of (1) Apollo Medical Holdings, Inc. and its wholly owned subsidiaries AMM, PCCM, and VMM, (2) the Company’s controlling interest in ApolloMed ACO, and APS, (3) physician practice corporations (“PPCs”) managed under long-term management service agreements including AMH, MMG, ACC, LALC (through December 31, 2016), Hendel (through December 31, 2016), AKM, SCHC and BAHA. Some states have laws that prohibit business entities, such as ApolloMed, from practicing medicine, employing physicians to practice medicine, exercising control over medical decisions by physicians (collectively known as the corporate practice of medicine), or engaging in certain arrangements with physicians, such as fee-splitting. In California, the Company operates by maintaining long-term management service agreements with the PPCs, which are each owned and operated by physicians, and which employ or contract with additional physicians to provide hospitalist services. Under the management agreements, the Company provides and performs all non-medical management and administrative services, including financial management, information systems, marketing, risk management and administrative support. Each management agreement typically has a term from 10 to 20 years unless terminated by either party for cause. The management agreements are not terminable by the PPCs, except in the case of material breach or bankruptcy of the respective PPM.
Through the management agreements and the Company’s relationship with the stockholders of the PPCs, the Company has exclusive authority over all non-medical decision making related to the ongoing business operations of the PPCs. Consequently, the Company consolidates the revenue and expenses of each PPC from the date of execution of the applicable management agreement.
Effective January 1, 2017, as a result of an amendment to their respective MSA’s, LALC and Hendel are no longer controlled by the Company and are therefore not consolidated by the Company as of such date. All intercompany balances and transactions have been eliminated in consolidation.
Business Combinations
The Company uses the acquisition method of accounting for all business combinations, which requires assets and liabilities of the acquiree to be recorded at fair value to measure the fair value of the consideration transferred, including contingent consideration, to be determined on the acquisition date, and to account for acquisition related costs separately from the business combination.
Reportable Segments
The Company operates as one reportable segment, the healthcare delivery segment, and implements and operates innovative health care models to create a patient-centered, physician-centric experience. The Company reports its consolidated financial statements in the aggregate, including all activities in one reportable segment. The Company has determined it has six reporting units, which are comprised of (1) Hospitalist and AMM, (2) IPA, (3) Clinics, (4) Care Connect, (5) ACO, and (6) Palliative Services. While the chief operating decision maker uses financial information related to these reporting units to analyze business performance and allocate resources, the reporting units, as noted above, do not meet the quantitative threshold under U.S. GAAP to be considered a reportable segment. As such, these reporting units are aggregated into a single reportable segment in the consolidated financial statements.
Revenue Recognition
Revenue consists of contracted, fee-for-service (“FFS”) and capitation revenue. Revenue is recorded in the period in which services are rendered. Revenue is principally derived from the provision of healthcare staffing services to patients within healthcare facilities. The form of billing and related risk of collection for such services may vary by customer. The following is a summary of the principal forms of the Company’s billing arrangements and how net revenue is recognized for each.
F-164
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Contracted revenue
Contracted revenue represents revenue generated under contracts for which the Company provides physician and other healthcare staffing and administrative services in return for a contractually negotiated fee. Contract revenue consists primarily of billings based on hours of healthcare staffing provided at agreed-to hourly rates. Revenue in such cases is recognized as the hours are worked by the Company’s staff and contractors. Additionally, contract revenue also includes supplemental revenue from hospitals where the Company may have a FFS contract arrangement or provide physician advisory services to the medical staff at a specific facility. Contract revenue for the supplemental billing in such cases is recognized based on the terms of each individual contract. Such contract terms generally either provides for a fixed monthly dollar amount or a variable amount based upon measurable monthly activity, such as hours staffed, patient visits or collections per visit compared to a minimum activity threshold. Such supplemental revenues based on variable arrangements are usually contractually fixed on a monthly, quarterly or annual calculation basis considering the variable factors negotiated in each such arrangement. Such supplemental revenues are recognized as revenue in the period when such amounts are determined to be fixed and therefore contractually obligated as payable by the customer under the terms of the respective agreement. Additionally, the Company derives a portion of the Company’s revenue as a contractual bonus from collections received by the Company’s partners and such revenue is contingent upon the collection of third-party billings. These revenues are not considered earned and therefore not recognized as revenue until actual cash collections are achieved in accordance with the contractual arrangements for such services.
Fee-for-service revenue
FFS revenue represents revenue earned under contracts in which the Company bills and collects the professional component of charges for medical services rendered by the Company’s contracted physicians. Under the FFS arrangements, the Company bills patients for services provided and receive payment from patients or their third-party payors. FFS revenue is reported net of contractual allowances and policy discounts. All services provided are expected to result in cash flows and are therefore reflected as net revenue in the financial statements. FFS revenue is recognized in the period in which the services are rendered to specific patients and reduced immediately for the estimated impact of contractual allowances in the case of those patients having third-party payor coverage. The recognition of net revenue (gross charges less contractual allowances) from such visits is dependent on such factors as proper completion of medical charts following a patient visit, the forwarding of such charts to the Company’s billing center for medical coding and entering into the Company’s billing system and the verification of each patient’s submission or representation at the time services are rendered as to the payor(s) responsible for payment of such services. Revenue is recorded based on the information known at the time of entering of such information into the Company’s billing systems as well as an estimate of the revenue associated with medical services.
Capitation revenue
Capitation revenue (net of capitation withheld to fund risk share deficits) is recognized in the month in which the Company is obligated to provide services. Minor ongoing adjustments to prior months’ capitation, primarily arising from contracted health maintenance organizations (each, an “HMO”) finalizing of monthly patient eligibility data for additions or subtractions of enrollees, are recognized in the month they are communicated to the Company. Managed care revenues of the Company consist primarily of capitated fees for medical services provided by the Company under a provider service agreement (“PSA”) or capitated arrangements directly made with various managed care providers including HMO’s and management service organizations (“MSOs”). Capitation revenue under the PSA and HMO contracts is prepaid monthly to the Company based on the number of enrollees electing the Company as their healthcare provider. Additionally, Medicare pays capitation using a “Risk Adjustment model,” which compensates managed care organizations and providers based on the health status (acuity) of each individual enrollee. Health plans and providers with higher acuity enrollees will receive more and those with lower acuity enrollees will receive less. Under Risk Adjustment, capitation is determined based on health severity, measured using patient encounter data. Capitation is paid on an interim basis based on data submitted for the enrollee for the preceding year and is adjusted in subsequent periods after the final data is compiled. Positive or negative capitation adjustments are made for Medicare enrollees with conditions requiring more or less healthcare services than assumed in the interim payments. Since the Company cannot reliably predict these adjustments, periodic changes in capitation amounts earned as a result of Risk Adjustment are recognized when those changes are communicated by the health plans to the Company.
HMO contracts also include provisions to share in the risk for enrollee hospitalization, whereby the Company can earn additional incentive revenue or incur penalties based upon the utilization of hospital services. Typically, any shared risk deficits are not payable until and unless the Company generates future risk sharing surpluses, or if the HMO withholds a portion of the capitation revenue to fund any risk share deficits. At the termination of the HMO contract, any accumulated risk share deficit is typically extinguished. Due to the lack of access to information necessary to estimate the related costs, shared-risk amounts receivable from the HMOs are only recorded when such amounts are known. Risk pools for the prior contract years are generally final settled in the third or fourth quarter of the following fiscal year.
In addition to risk-sharing revenues, the Company also receives incentives under “pay-for-performance” programs for quality medical care, based on various criteria. These incentives are generally recorded in the third and fourth quarters of the fiscal year and recorded when such amounts are known.
Under full risk capitation contracts, an affiliated hospital enters into agreements with several HMOs, pursuant to which, the affiliated hospital provides hospital, medical, and other healthcare services to enrollees under a fixed capitation arrangement (“Capitation Arrangement”). Under the risk pool sharing agreement, the affiliated hospital and medical group agree to establish a Hospital Control Program to serve the enrollees, pursuant to which, the medical group is allocated a percentage of the profit or loss, after deductions for costs to affiliated hospitals. The Company participates in full risk programs under the terms of the PSA, with health plans whereby the Company is wholly liable for the deficits allocated to the medical group under the arrangement. The related liability is included in medical liabilities in the accompanying consolidated balance sheets at March 31, 2017 and March 31, 2016 (see "Medical Liabilities" in this Note 2, below).
F-165
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Medicare Shared Savings Program Revenue
The Company, through its subsidiary ApolloMed ACO, participates in the MSSP, which is sponsored by CMS. The goal of the MSSP is to improve the quality of patient care and outcomes through more efficient and coordinated approach among providers. The MSSP allows ACO participants to share in cost savings it generates in connection with rendering medical services to Medicare patients. Payments to ACO participants, if any, will be calculated annually by CMS on cost savings generated by the ACO participant relative to the ACO participants’ cost savings benchmark. The MSSP is a relatively new program managed by CMS that has an evolving payment methodology. Revenues earned by ApolloMed ACO are uncertain, and, if such amounts are payable by the CMS, they will be paid on an annual basis significantly after the time earned, and will be contingent on various factors, including achievement of the minimum savings rate as determined by MSSP for the relevant period. Such payments are earned and made on an “all or nothing” basis. The Company considers revenue, if any, under the MSSP, as contingent upon the realization of program savings as determined by CMS, and are not considered earned and therefore are not recognized as revenue until notice from CMS that cash payments are to be imminently received.
Hospitalist Agreements
During the year, the Company entered into several new hospitalist agreements with hospitals, whereby the Company earns a stipend fee plus a fee based on an agreed percentage of fee-for-service collections. The fee is recorded at an amount net of the portion owed to the hospitals (the Company collects all fees on behalf of the hospitals). The fee revenue is further reduced by a portion subject to quality metrics which is only recorded as revenue upon the Company meeting these metrics. The Company considered the indicators of gross revenue and net revenue reporting under ASC 605-45-45, “Revenue Recognition: Principal Agent Considerations” and determined that revenue from this arrangement is recorded at net.
NGACO Model Revenue
No revenues were generated from the NGACO Model in fiscal 2017 and management is in the process of evaluating the appropriate revenue recognition.
Cash and Cash Equivalents
Cash and cash equivalents consists of highly liquid investments with an initial maturity of three months or less at date of purchase to be cash equivalents.
Restricted Cash
Restricted cash primarily consists of cash held as collateral to secure standby letters of credits as required by certain contracts. The certificates have an interest rate ranging from 0.05% to 0.10%.
Long-Lived Assets
The Company reviews its long-lived assets including definite lived intangible assets for impairment whenever events or changes in circumstances indicate that the carrying amount of the assets may not be fully recoverable. The Company evaluates assets for potential impairment by comparing estimated future undiscounted net cash flows to the carrying amount of the assets. If the carrying amount of the assets exceeds the estimated future undiscounted cash flows, impairment is measured based on the difference between the carrying amount of the assets and fair value.
Goodwill and Indefinite-Lived Intangible Assets
Under Financial Accounting Standards Board (“FASB”) Accounting Standards Codification (“ASC”) 350, Intangibles – Goodwill and Other (“ASC 350”), goodwill and indefinite-lived intangible assets are reviewed at least annually for impairment. Acquired intangible assets with definite lives are amortized over their individual useful lives.
At least annually, at the Company’s fiscal year end, management assesses whether there has been any impairment in the value of goodwill by first comparing the fair value to the net carrying value of the reporting unit. If the carrying value exceeds its estimated fair value, a second step is performed to compute the amount of the impairment. The Company has determined it has six reporting units, which are comprised of (1) Hospitalist and AMM, (2) IPA, (3) Clinics, (4) Care Connect, (5) ACO, and (6) Palliative Services.
An impairment loss is recognized if the implied fair value of the asset being tested is less than its carrying value. In this event, the asset is written down accordingly. The fair values of goodwill are determined using valuation techniques based on estimates, judgments and assumptions management believes are appropriate in the circumstances.
At least annually, indefinite-lived intangible assets are tested for impairment. Impairment for intangible assets with indefinite lives exists if the carrying value of the intangible asset exceeds its fair value. The fair values of indefinite-lived intangible assets are determined using valuation techniques based on estimates, judgments and assumptions management believes are appropriate in the circumstances.
Accounts Receivable and Allowance for Doubtful Accounts
Accounts receivable primarily consists of amounts due from third-party payors, including government sponsored Medicare and Medicaid programs, insurance companies, and amounts due from hospitals and patients. Accounts receivable are recorded and stated at the amount expected to be collected.
The Company maintains reserves for potential credit losses on accounts receivable. Management reviews the composition of accounts receivable and analyzes historical bad debts, customer concentrations, customer credit worthiness, current economic trends and changes in customer payment patterns to evaluate the adequacy of these reserves. The Company also regularly analyses the ultimate collectability of accounts receivable after certain stages of the collection cycle using a look-back analysis to determine the amount of receivables subsequently collected and adjustments are recorded when necessary. Reserves are recorded primarily on a specific identification basis.
F-166
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Concentrations
The Company had major payors that contributed the following percentage of net revenue:
| For The Years Ended March 31, | ||||||||
| 2017 | 2016 | |||||||
| Governmental - Medicare/Medi-Cal | 18.8 | % | 29.8 | % | ||||
| L.A. Care | 13.1 | % | 15.7 | % | ||||
| Allied Physicians | 8.5 | % | 0.0 | % | ||||
| Health Net | 6.8 | % | 9.9 | % | ||||
Receivables from these payors amounted to the following percentage of accounts receivable before the allowance for doubtful accounts:
| As of March 31, | ||||||||
| 2017 | 2016 | |||||||
| Governmental - Medicare/Medi-Cal | 20.5 | % | 39.3 | % | ||||
| Allied Physicians | 12.8 | % | 15.8 | % | ||||
The Company maintains its cash and cash equivalents and restricted cash in bank deposit accounts, which, at times, may exceed federally insured limits. The Company has not experienced any losses in such accounts; however, amounts in excess of the federally insured limit may be at risk if the bank experiences financial difficulties. As of March 31, 2017, approximately $8.5 million was in excess of the Federal Deposit Insurance Corporation limits of $250,000 per depositor.
The Company’s business and operations are concentrated in one state, California. Any material changes by California with respect to strategy, taxation and economics of healthcare delivery, reimbursements, financial requirements or other aspects of regulation of the healthcare industry could have an adverse effect on the Company’s operations and cost of doing business.
Property and Equipment
Property and equipment is recorded at cost and depreciated using the straight-line method over the estimated useful lives of the respective assets. Cost and related accumulated depreciation on assets retired or disposed of are removed from the accounts and any resulting gains or losses are credited or charged to income. Computers and software are depreciated over 3 years. Furniture and fixtures are depreciated over 8 years. Machinery and equipment are depreciated over 5 years. Leasehold improvements are amortized on a straight-line basis over the shorter of the terms of the respective leases or the expected useful lives of the improvements ranging from 5 to 10 years.
Property and equipment consisted of the following:
| As of March 31, | ||||||||
| 2017 | 2016 | |||||||
| Website | $ | 4,568 | $ | 4,568 | ||||
| Computers | 287,570 | 166,043 | ||||||
| Software | 70,971 | 215,439 | ||||||
| Machinery and equipment | 141,977 | 351,090 | ||||||
| Furniture and fixtures | 183,130 | 114,127 | ||||||
| Leasehold improvements | 1,075,760 | 1,094,665 | ||||||
| 1,763,976 | 1,945,932 | |||||||
| Less accumulated depreciation and amortization | (558,837 | ) | (697,959 | ) | ||||
| $ | 1,205,139 | $ | 1,247,973 | |||||
Depreciation and amortization expense was $265,110 and $165,620 for the years ended March 31, 2017 and 2016, respectively.
F-167
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Medical Liabilities
The Company is responsible for integrated care that the associated physicians and contracted hospitals provide to its enrollees under risk-pool arrangements. The Company provides integrated care to health plan enrollees through a network of contracted providers under sub-capitation and direct patient service arrangements, company-operated clinics and staff physicians. Medical costs for professional and institutional services rendered by contracted providers are recorded as cost of services in the accompanying consolidated statements of operations. Costs for operating medical clinics, including the salaries of medical personnel, are also recorded in cost of services, while non-medical personnel and support costs are included in general and administrative expense.
An estimate of amounts due to contracted physicians, hospitals, and other professional providers is included in medical liabilities in the accompanying consolidated balance sheets. Medical liabilities include claims reported as of the balance sheet date and estimates of incurred but not reported claims (“IBNR”). Such estimates are developed using actuarial methods and are based on many variables, including the utilization of health care services, historical payment patterns, cost trends, product mix, seasonality, changes in membership, and other factors. The estimation methods and the resulting reserves are periodically reviewed and updated. Many of the medical contracts are complex in nature and may be subject to differing interpretations regarding amounts due for the provision of various services. Such differing interpretations may not come to light until a substantial period of time has passed following the contract implementation. The Company has a $20,000 per member professional stop-loss and $200,000 per member stop-loss for Medi-Cal patients in institutional risk pools. Any adjustments to reserves are reflected in current operations.
The Company’s medical liabilities were as follows:
| For The Years Ended March 31, | ||||||||
| 2017 | 2016 | |||||||
| Balance, beginning of year | $ | 2,670,709 | $ | 1,260,549 | ||||
| Incurred health care costs: | ||||||||
| Current year | 10,365,502 | 7,844,329 | ||||||
| Claims paid: | ||||||||
| Current year | (8,524,215 | ) | (6,019,186 | ) | ||||
| Prior years | (1,881,869 | ) | (1,159,909 | ) | ||||
| Total claims paid | (10,406,084 | ) | (7,179,095 | ) | ||||
| Risk pool settlement | 814,733 | - | ||||||
| Adjustment related to full risk capitation contracts | (1,676,629 | ) | 803,981 | |||||
| Adjustments | - | (59,055 | ) | |||||
| Balance, end of year | $ | 1,768,231 | $ | 2,670,709 | ||||
Deferred Financing Costs
Costs relating to debt issuance have been deferred and are amortized over the lives of the respective loans, using the effective interest method.
During the year ended March 31, 2016, the Company wrote-off deferred financing costs of approximately $175,000 related to the conversion of NNA of Nevada, Inc. (“NNA”) indebtedness as part of the loss on debt extinguishment expense (see Note 7).
Income Taxes
Federal and state income taxes are computed at currently enacted tax rates less tax credits using the asset and liability method. Deferred taxes are adjusted both for items that do not have tax consequences and for the cumulative effect of any changes in tax rates from those previously used to determine deferred tax assets or liabilities. Tax provisions include amounts that are currently payable, changes in deferred tax assets and liabilities that arise because of temporary differences between the timing of when items of income and expense are recognized for financial reporting and income tax purposes, changes in the recognition of tax positions and any changes in the valuation allowance caused by a change in judgment about the realizability of the related deferred tax assets. A valuation allowance is established when necessary to reduce deferred tax assets to amounts expected to be realized.
The Company uses a recognition threshold of more-likely-than-not and a measurement attribute on all tax positions taken or expected to be taken in a tax return in order to be recognized in the financial statements. Once the recognition threshold is met, the tax position is then measured to determine the actual amount of benefit to recognize in the financial statements.
F-168
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Stock-Based Compensation
The Company maintains a stock-based compensation program for employees, non-employees, directors and consultants, which is more fully described in Note 9. The value of stock-based awards so measured is recognized as compensation expense on a cumulative straight-line basis over the vesting terms of the awards, adjusted for expected forfeitures. The Company sells certain of its restricted common stock to its employees, directors and consultants with a right (but not obligation) of repurchase feature that lapses based on performance of services in the future.
The Company accounts for share-based awards granted to persons other than employees and directors under ASC 505-50 Equity-Based Payments to Non-Employees. As such the fair value of such shares is periodically re-measured using an appropriate valuation model and income or expense is recognized over the vesting period.
Fair Value of Financial Instruments
The Company’s accounting for Fair Value Measurement and Disclosures defines fair value as the exchange price that would be received for an asset or paid to transfer a liability (an exit price) in the principal or most advantageous market for the asset or liability in an orderly transaction between market participants on the measurement date. This topic also establishes a fair value hierarchy which requires classification based on observable and unobservable inputs when measuring fair value. The fair value hierarchy distinguishes between assumptions based on market data (observable inputs) and an entity’s own assumptions (unobservable inputs). The hierarchy consists of three levels:
Level one — Quoted market prices in active markets for identical assets or liabilities;
Level two — Inputs other than level one inputs that are either directly or indirectly observable; and
Level three — Unobservable inputs developed using estimates and assumptions, which are developed by the reporting entity and reflect those assumptions that a market participant would use.
Determining which category an asset or liability falls within the hierarchy requires significant judgment. The Company evaluates its hierarchy disclosures each quarter.
The carrying amount reported in the accompanying consolidated balance sheets for cash and cash equivalents, accounts receivable, accounts payable and accrued expenses approximates fair value because of the short-term maturity of those instruments. The carrying amount for borrowings under the notes payable and the convertible note payable approximates fair value which is determined by using interest rates that are available for similar debt obligations with similar terms at the balance sheet date.
Warrant liability
In October 2015, the Company issued a warrant in connection with the 2015 NMM financing that initially required liability classification (see Note 9). The fair value of the warrant liability of approximately $1.2 million at December 21, 2016, the date on which the Series A Warrant was reclassified from liability to equity, see Note 9, was estimated using the Monte Carlo valuation model which used the following inputs: term of 3.81 years, risk free rate of 1.74%, no dividends, volatility of 62.6%, share price of $9.00 per share based on the trading price of the Company’s common stock adjusted for a marketability discount. The fair value of the warrant liability of approximately $2.8 million at March 31, 2016 was estimated using the Monte Carlo valuation model, using the following inputs: term of 4.5 years, risk free rate of 1.13%, no dividends, volatility of 65.7%, share price of $5.93 per share based on the trading price of the Company’s common stock adjusted for marketability discount, and a 0% probability of redemption of the warrant shares issued along with the shares of the Company’s convertible preferred stock issued in the NMM financing. The fair value of the warrant liability of approximately $2.9 million in October 2015 was estimated at issuance using the Monte Carlo valuation model, using the following inputs: term of 5 years; risk free rate of 1.3%, no dividends, volatility of 63.3%, share price of $6.00 per share based on the trading price of the Company’s common stock adjusted for a marketability discount, and a 0% probability of redemption of the warrant shares issued along with the shares of the Company’s convertible preferred stock issued in the NMM financing.
Conversion feature liability
The 8% NNA Convertible Note was converted into common shares in October 2015 and the related liability was marked to fair value with changes in fair value recorded in the consolidated statement of operations and reclassified to additional paid-in capital on such date. The fair value of the conversion feature liability on the date of conversion was estimated using the Monte Carlo simulation valuation model, using the following input terms: term of 3.45 years; risk free rate of 0.95%, no dividends, volatility of 50.7%, share price of $6.00 per share based on the trading price of the Company’s common stock adjusted for a marketability discount, and a 50% probability of future financing event related to the anti-dilution provision of the convertible feature.
F-169
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
There were no financial instruments measured at fair value on a recurring basis as of March 31, 2017. The carrying amounts and fair values of the Company's financial instruments measured at fair value on a recurring basis are presented below as of March 31, 2016:
| Fair Value Measurements | ||||||||||||||||
| Level 1 | Level 2 | Level 3 | Total | |||||||||||||
| Liabilities: | ||||||||||||||||
| Warrant liability | $ | - | $ | - | $ | 2,811,111 | $ | 2,811,111 | ||||||||
The following summarizes the activity of Level 3 inputs measured on a recurring basis for the years ended March 31, 2017 and 2016:
| Warrant Liability |
Conversion Feature Liability |
Total | ||||||||||
| Balance at April 1, 2015 | $ | 2,144,496 | $ | 442,358 | $ | 2,586,854 | ||||||
| Warrant adjustments | (999,724 | ) | - | (999,724 | ) | |||||||
| Conversion of warrants and convertible note to common stock – NNA | (1,624,029 | ) | (482,904 | ) | (2,106,933 | ) | ||||||
| Fair value of warrant issued – NMM | 2,922,222 | - | 2,922,222 | |||||||||
| Change in fair value of warrant and conversion feature liability | 368,146 | 40,546 | 408,692 | |||||||||
| Balance at March 31, 2016 | 2,811,111 | - | 2,811,111 | |||||||||
| Fair value of warrant reclassified to equity | (1,177,778 | ) | - | (1,177,778 | ) | |||||||
| Change in fair value of warrant liability | (1,633,333 | ) | - | (1,633,333 | ) | |||||||
| Balance at March 31, 2017 | $ | - | $ | - | $ | - | ||||||
The gain on change in fair value of the warrant liability of $1,633,333 for the year ended March 31, 2017 and loss on change in fair value of the warrant liability and conversion feature liability of $408,692 for the year ended March 31, 2016, are included in the accompanying consolidated statements of operations. The change in fair value during the year ended March 31, 2016 relates to a warrant liability and embedded conversion feature resulting from a 2014 financing transaction with NNA which was settled in October 2015. Upon settlement, the Company reclassified the fair value of warrants of $1,177,778 from warrant liability to additional paid in capital – see Note 9.
Noncontrolling Interests
The noncontrolling interests recorded in the Company’s consolidated financial statements includes the equity of those PPC’s in which the Company has determined that it has a controlling financial interest and for which consolidation is required as a result of management contracts entered into with these entities owned by third-party physicians. The nature of these contracts provide the Company with a monthly management fee to provide the services described above, and as such, the adjustments to noncontrolling interests in any period subsequent to initial consolidation would relate to either capital contributions or distributions by the noncontrolling parties as well as income or losses attributable to certain noncontrolling interests. Noncontrolling interests also represent third-party minority equity ownership interests which are majority owned by the Company.
During the year ended March 31, 2016, the Company entered into a settlement agreement with a shareholder of one of the Company’s majority owned subsidiaries. In connection with the settlement agreement, the former shareholder received approximately $400,000, of which approximately $252,000 was paid by the Company and the remaining amount of approximately $148,000 was paid by another shareholder of APS, in exchange for the shareholder’s interest in such subsidiary, resulting in an increase in the Company’s ownership interest in APS from 51% to 56%. The net effect of this settlement was a decrease in additional paid-in capital of approximately $338,000, an adjustment to increase noncontrolling interest by approximately $32,000 and an increase in noncontrolling interest resulting from a reclassification from noncontrolling interest to other receivables of approximately $415,000.
See “Principles of Consolidation” above regarding deconsolidation of LALC and Hendel and related adjustments to noncontrolling interest.
See Note 3 related to the reclassification of noncontrolling interest to additional paid-in capital due to the acquisition of the variable interest entity, BAHA.
Basic and Diluted Earnings (Loss) per Share
Basic net income (loss) per share is calculated using the weighted average number of shares of the Company’s common stock issued and outstanding during a certain period, and is calculated by dividing net income (loss) by the weighted average number of shares of the Company’s common stock issued and outstanding during such period. Diluted net income (loss) per share is calculated using the weighted average number of common and potentially dilutive common shares outstanding during the period, using the as-if converted method for secured convertible notes, and the treasury stock method for options and warrants.
F-170
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
The following table sets forth the number of shares excluded from the computation of diluted earnings per share, as their inclusion would be anti-dilutive:
| As of March 31, | ||||||||
| 2017 | 2016 | |||||||
| Preferred stock | 1,666,666 | 1,666,666 | ||||||
| Options | 902,950 | 1,064,150 | ||||||
| Warrants | 138,500 | 2,091,166 | ||||||
| Convertible notes | 499,000 | - | ||||||
| 3,207,116 | 4,821,982 | |||||||
New Accounting Pronouncements
In February 2016, the FASB issued ASU 2016-02, Leases (“ASU 2016-02”). This new standard establishes a right-of-use (ROU) model that requires a lessee to record a ROU asset and a lease liability on the balance sheet for all leases with terms longer than 12 months. Leases will be classified as either finance or operating, with classification affecting the pattern of expense recognition in the income statement. ASU 2016-02 is effective for fiscal years beginning after December 15, 2018, including interim periods within those fiscal years. Early adoption is permitted. A modified retrospective transition approach is required for lessees for capital and operating leases existing at, or entered into after, the beginning of the earliest comparative period presented in the financial statements, with certain practical expedients available. The Company is currently evaluating the impact of the adoption of ASU 2016-02 on the consolidated financial statements.
In March 2016, the FASB issued ASU 2016-09, Compensation - Stock Compensation (Topic 718): Improvements to Employee Share-Based Payment Accounting (“ASU 2016-09”). This ASU makes several modifications to Topic 718 related to the accounting for forfeitures, employer tax withholding on share-based compensation, and the financial statement presentation of excess tax benefits or deficiencies. ASU 2016-09 also clarifies the statement of cash flows presentation for certain components of share-based awards. The standard is effective for interim and annual reporting periods beginning after December 15, 2016, with early adoption permitted. The Company adopted this guidance on April 1, 2017 and does not expect such adoption to have a material impact on its consolidated financial statements and related disclosures for fiscal 2018.
In January 2016, the FASB issued ASU No. 2016-01, Financial Instruments - Overall (Topic 825-10): Recognition and Measurement of Financial Assets and Financial Liabilities ("ASU 2016-01"). ASU 2016-01 addresses certain aspects of recognition, measurement, presentation and disclosures of financial instruments including the requirement to measure certain equity investments at fair value with changes in fair value recognized in net income. ASU 2016-01 will become effective for the Company beginning interim period April 1, 2018. The Company is currently evaluating the guidance to determine the potential impact on its financial condition, results of operations, cash flows and financial statement disclosures.
F-171
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
The FASB issued the following accounting standard updates related to Topic 606, Revenue Contracts with Customers:
| • | ASU No. 2014-09, Revenue from Contracts with Customers (Topic 606) (“ASU 2014-09”) in May 2014. ASU 2014-09 requires entities to recognize revenue through the application of a five-step model, which includes identification of the contract, identification of the performance obligations, determination of the transaction price, allocation of the transaction price to the performance obligations and recognition of revenue as the entity satisfies the performance obligations. | |
| • | ASU No. 2016-08, Revenue from Contracts with Customers (Topic 606): Principal versus Agent Considerations (Reporting Revenue Gross versus Net) ("ASU 2016-08") in March 2016. ASU 2016-08 does not change the core principle of revenue recognition in Topic 606 but clarifies the implementation guidance on principal versus agent considerations. | |
| • | ASU No. 2016-10, Revenue from Contracts with Customers (Topic 606): Identifying Performance Obligations and Licensing ("ASU 2016-10") in April 2016. ASU 2016-10 does not change the core principle of revenue recognition in Topic 606 but clarifies the implementation guidance on identifying performance obligations and the licensing implementation guidance, while retaining the related principles for those areas. | |
| • | ASU No. 2016-11, Revenue Recognition (Topic 605) and Derivatives and Hedging (Topic 815): Rescission of SEC Guidance Because of Accounting Standards Updates 2014-09 and 2014-16 Pursuant to Staff Announcements at the March 3, 2016 EITF Meeting (SEC Update) ("ASU 2016-11") in May 2016. ASU 2016-11 rescinds SEC paragraphs pursuant to two SEC Staff Announcements at the March 3, 2016 EITF meeting. The SEC Staff is rescinding SEC Staff Observer comments that are codified in Topic 605 and Topic 932, effective upon adoption of Topic 606. | |
| • | ASU No. 2016-12, Revenue from Contracts with Customers (Topic 606): Narrow-Scope Improvements and Practical Expedients in May 2016. ASU 2016-12 does not change the core principle of revenue recognition in Topic 606 but clarifies the implementation guidance on a few narrow areas and adds some practical expedients to the guidance. | |
| • | ASU No. 2016-20, Revenue from Contracts with Customers (Topic 606): Technical Corrections and Improvements (" ASU 2016-20") in December 2016. ASU 2016-20 does not change the core principle of revenue recognition in Topic 606 but summarizes the technical corrections and improvements to ASU 2014-09 and is effective upon adoption of Topic 606. |
These ASUs will become effective for the Company beginning interim period April 1, 2018. The Company currently anticipates adopting the standard using the modified retrospective method. The Company has begun the process of implementing this standard, including performing a review of its revenue streams to identify any differences in the timing, measurement, or presentation of revenue recognition. The Company currently believes that the primary impact will be changes to the timing of recognition of revenues related to FFS and Capitation Revenue and enhanced financial statement disclosures. The Company will continue to assess the impact on all areas of its revenue recognition, disclosure requirements and changes that may be necessary to its internal controls over financial reporting.
In August 2016, the FASB issued ASU No. 2016-15, Statement of Cash Flows (Topic 230) – Classification of Certain Cash Receipts and Cash Payments (“ASU 2016-15”). This ASU provides clarification regarding how certain cash receipts and cash payments are presented and classified in the statement of cash flows. This ASU addresses eight specific cash flow issues with the objective of reducing the existing diversity in practice. The issues addressed in this ASU that will affect the Company are classifying debt prepayments or debt extinguishment costs and contingent consideration payments made after a business combination. This update is effective for annual and interim periods beginning after December 15, 2017, and interim periods within that reporting period. Early adoption is permitted. The Company is currently assessing the impact the adoption of ASU 2016-15 will have on the Company’s consolidated financial statements.
In December 2016, the FASB issued ASU No. 2016-18, Statement of Cash Flows (Topic 230) ("ASU 2016-18”). The amendments in ASU 2016-18 require that a statement of cash flows explain the change during the period in the total of cash, cash equivalents, and amounts generally described as restricted cash or restricted cash equivalents. ASU 2016-17 will become effective for the Company beginning interim period April 1, 2018. Early adoption is permitted, including adoption in an interim period. The Company is currently assessing the impact the adoption of ASU 2016-18 will have on the Company’s consolidated financial statements.
In January 2017, the FASB issued ASU No. 2017-01, Business Combinations (Topic 805): Clarifying the Definition of a Business (“ASU 2017-01”). This ASU provides a screen to determine when a set is not a business, which requires that when substantially all of the fair value of the gross assets acquired (or disposed of) is concentrated in a single identifiable asset or a group of similar identifiable assets, the set is not a business, which reduces the number of transactions that need to be further evaluated. If the screen is not met, this ASU require that to be considered a business, a set much include, at a minimum, an input and a substantive process that together significantly contribute to the ability to create output and also remove the evaluation of whether a market participant could replace missing elements. This update is effective for annual and interim periods beginning after December 15, 2017, including interim periods within those periods. The Company is currently assessing the impact the adoption of ASU 2017-01 will have on the Company’s consolidated financial statements.
F-172
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
In January 2017, the FASB issued ASU No. 2017-04, Intangibles – Goodwill and Other (Topic 350): Simplifying the Test for Goodwill Impairment (“ASU 2017-04”). This ASU eliminates Step 2 from the goodwill impairment test if the carrying amount exceeds the fair value of a reporting unit and also eliminated the requirements for any reporting unit with a zero or negative carrying amount to perform a qualitative assessment and, if it fails that qualitative test, to perform Step 2 of the goodwill impairment test. Therefore, the same impairment assessment applies to all reporting units. An entity is required to disclose the amount of goodwill allocated to each reporting unit with a zero or negative carrying amount of net assets. This update is effective for annual and interim periods beginning after December 15, 2019. Early adoption is permitted for interim or annual goodwill impairment tests performed on testing dates after January 1, 2017. The Company is currently assessing the impact the adoption of ASU 2017-04 will have on the Company’s consolidated financial statements.
Use of Estimates
The preparation of financial statements in conformity with U.S. GAAP requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the reporting period. Actual results may materially differ from these estimates under different assumptions or conditions.
3. Acquisitions
Acquired Technology
In January 2016, Apollo Care Connect acquired certain assets from Healarium Inc., a third party entity, and was determined to be a purchase of assets. According to the asset purchase agreement, as amended, the Company agreed to issue 275,000 shares of its common stock with a fair value of $1,512,500 in exchange for the technology with a fair value of approximately $1.3 million, plus $200,000 in cash. The technology provides a cloud and mobile-based population health management platform, with an emphasis on chronic care management and high-risk patient management in addition to a comprehensive platform for total patient engagement. The acquired technology was placed into service in April 2016 and will be amortized over its estimated useful life of five years. Management evaluated the acquired technology for impairment and no impairment occurred during fiscal 2017 (see Note 4).
BAHA Acquisition
On November 10, 2016, BAHA Acquisition, a Medical Corporation, a California professional corporation (“Acquisition”), an affiliate of the Company, entered into a Stock Purchase Agreement (the “BAHA Stock Purchase Agreement”) dated as of November 4, 2016 with BAHA and Scott Enderby, D.O. (“Enderby”), pursuant to which Enderby sold to Acquisition, and Acquisition purchased from Enderby, 100% of the issued and outstanding stock of BAHA (the “BAHA Stock”), of which Enderby was the sole holder beneficially and of record (the “Transaction”). Warren Hosseinion, M.D., the Company’s Chief Executive Officer, is the sole stockholder of Acquisition, as nominee for AMM. BAHA Acquisition is a consolidated variable interest entity of the Company.
As provided for in the BAHA Stock Purchase Agreement, the purchase price for the BAHA Stock consists of (i) a payment of $25,000 (the “Initial Payment”) at the closing (the “Closing”) of the Transaction, which also took place on November 4, 2016 (the “Closing Date”); (ii) a contingent payment in the aggregate amount of $100,000 to be paid over a period of 18 months following the Closing (the “Contingent Payment”); and (iii) a warrant to purchase 24,000 shares of the Company’s common stock (the “Enderby Warrant”) issued to Enderby. The Company has informally agreed with Enderby to defer the Initial Payment from the Closing until after the delivery of the closing statement calculating Actual Net Working Capital, as described in the following paragraph.
No later than 30 days following the Closing Date, Acquisition shall prepare and deliver to Enderby a written statement of the net working capital of BAHA as of the Closing Date. If the Actual Net Working Capital (as defined in the BAHA Stock Purchase Agreement) as of the Closing Date is less than $300,000 (the “Target Amount”), then Enderby shall, within five business days of the date of final determination of the Actual Net Working Capital as of the Closing Date, pay to Acquisition the amount equal to the absolute value of the difference between the Target Amount and the Actual Net Working Capital as of the Closing Date, together with interest on the amount of such difference calculated at the rate of four percent (4%) per annum from the Closing Date to the date of payment. The Company provided the statement of the net working capital to Enderby, who is reviewing such statement.
The Contingent Payment of up to an aggregate $100,000 will be made to Enderby in connection with personal services to be performed by him pursuant to an employment agreement entered into in connection with the Closing of the Transaction (the “Enderby Employment Agreement”) as follows: (i) $25,000 on the six-month anniversary of the Closing, an additional $50,000 on the first-year anniversary of the Closing and a final $25,000 on the 18-month anniversary of the Closing, if as of each such date, BAHA’s revenue is greater than $6,000,000. The Contingent Payment is in connection with the continued personal services provided under the Enderby Employment Agreement and is deemed to be post combination compensation.
As further inducement for Acquisition to enter into the BAHA Stock Purchase Agreement, BAHA and Enderby entered into a non-competition agreement dated as of November 4, 2016, pursuant to which Enderby has agreed, without the written permission of BAHA, within a radius of 50 miles from BAHA’s offices in San Francisco and for a period of three years from the Closing Date, not to compete with BAHA; hire or induce another person to hire any BAHA employee or independent contractor; or solicit any business, customers, clients or contractors of BAHA.
F-173
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
As part of the Transaction, BAHA and Enderby entered into the Enderby Employment Agreement, pursuant to which Enderby has been hired to serve as Chief Executive Officer of BAHA. Enderby will serve in that capacity for an initial term of two years, automatically extended for additional one-year terms, unless not less than 60 days prior to each such renewal date, either party shall have given written notice to the other that the Enderby Employment Agreement will not be renewed. Enderby shall be paid a base salary of $400,000 per year and shall be entitled to participate in any incentive compensation plans and/or equity compensation plans as are now available or may become available to other similarly positioned employees.
The Enderby Employment Agreement shall be terminated upon Enderby’s death and may be terminated on Enderby’s Disability (as that term is defined in the Enderby Employment Agreement), by BAHA with or without Cause (as that term is defined in the Enderby Employment Agreement) or by Enderby with or without Good Reason (as that term is defined in the Enderby Employment Agreement).
If Enderby’s employment is terminated for any reason during the term of the Enderby Employment Agreement, or if the Enderby Employment Agreement is not renewed, Enderby shall be entitled to be paid any earned but unpaid base salary through the date of termination, unpaid expense reimbursements and accrued but unused paid time off. Additionally, in the event of termination by BAHA without Cause or termination by Enderby for Good Reason, and if, but only if, Enderby signs a general release of claims in a form and manner satisfactory to BAHA, Enderby shall also be entitled to receive a severance payment in an amount equal to (i) four weeks of his most recent base salary for every full year of his active employment, but such amount shall be no less than one month’s worth nor more than six months’ worth of his most recent base salary; plus (ii) the premium amounts paid for coverage under BAHA’s group medical, dental and vision programs for a period of twelve months, to be paid directly to Enderby at the same times such payments would be paid on behalf of a current employee for such coverage, provided that Enderby timely elects continued coverage under such plan(s) pursuant to the Consolidated Omnibus Budget Reconciliation Act of 1985 as amended.
On November 4, 2016, the Company issued the Enderby Warrant to Enderby to purchase up to 24,000 shares of the Company’s common stock, at an exercise price of $4.50 per share, which was the closing price of the common stock on the trading day immediately preceding the Closing Date. The Enderby Warrant may be exercised in equal monthly installments of 1,000 shares over a 24-month period commencing on December 4, 2016 and terminating on November 4, 2018. The fair value of the warrants at the transaction date was deemed to be de minimus.
Prior to the Transaction, the financial results of BAHA were consolidated by the Company as a variable interest entity as the Company was determined to be the primary beneficiary. As part of the Transaction, Acquisition acquired the noncontrolling interest of BAHA.
Based on the Actual Net Working Capital, the Company did not pay the Initial Payment. While it is probable that the contingent payment will be earned, it is probable that the contingent payment will be offset against Actual Net Working adjustment. In addition, the receivable created by the Actual Net Working Capital was not deemed collectible and was not recorded. The Company recorded the reclassification of noncontrolling interest of $183,408 to additional paid-in capital pursuant to this transaction.
4. Goodwill and Intangible Assets
Goodwill
The following is a summary of goodwill activity:
| Balance at April 1, 2015 | $ | 2,168,833 | ||
| Decrease from disposal of ACC assets | (461,500 | ) | ||
| Impairment loss in AKM | (83,943 | ) | ||
| Other | (907 | ) | ||
| Balance at March 31, 2016 | 1,622,483 | |||
| Balance at March 31, 2017 | 1,622,483 |
Intangible Assets, Net
Intangible assets, net consisted of the following:
| Weighted | Gross | Gross | Net | |||||||||||||||||||||||||
| Average | March 31, | Impairment/ | March 31, | Accumulated | March 31, | |||||||||||||||||||||||
| Life (Yrs) | 2016 | Additions | Disposal | 2017 | Amortization | 2017 | ||||||||||||||||||||||
| Indefinite Lived Assets: | ||||||||||||||||||||||||||||
| Medicare License | $ | 704,000 | $ | - | $ | - | $ | 704,000 | $ | - | $ | 704,000 | ||||||||||||||||
| Amortized intangible assets: | ||||||||||||||||||||||||||||
| Acquired Technology | 5 | 1,312,500 | - | - | 1,312,500 | (262,500 | ) | 1,050,000 | ||||||||||||||||||||
| Non-compete | 4 | 117,000 | - | (22,328 | ) | 94,672 | (94,672 | ) | - | |||||||||||||||||||
| Network relationships | 5 | 220,000 | - | - | 220,000 | (117,331 | ) | 102,669 | ||||||||||||||||||||
| Trade name | 5 | 191,000 | - | (45,983 | ) | 145,017 | (97,417 | ) | 47,600 | |||||||||||||||||||
| $ | 2,544,500 | $ | - | $ | (68,311 | ) | $ | 2,476,189 | $ | (571,920 | ) | $ | 1,904,269 | |||||||||||||||
F-174
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
| Weighted | Gross | Gross | Net | |||||||||||||||||||||||||
| Average | March 31, | Impairment/ | March 31, | Accumulated | March 31, | |||||||||||||||||||||||
| Life (Yrs) | 2015 | Additions | Disposal | 2016 | Amortization | 2016 | ||||||||||||||||||||||
| Indefinite Lived Assets: | ||||||||||||||||||||||||||||
| Medicare License | $ | 704,000 | $ | - | $ | - | $ | 704,000 | $ | - | $ | 704,000 | ||||||||||||||||
| Amortized intangible assets: | ||||||||||||||||||||||||||||
| Acquired Technology | 5 | - | 1,312,500 | - | 1,312,500 | - | 1,312,500 | |||||||||||||||||||||
| Exclusivity | 4 | 40,000 | - | (40,000 | ) | - | - | - | ||||||||||||||||||||
| Non-compete | 4 | 185,400 | - | (68,400 | ) | 117,000 | (58,738 | ) | 58,262 | |||||||||||||||||||
| Payor relationships | 5 | 107,000 | - | (107,000 | ) | - | - | - | ||||||||||||||||||||
| Network relationships | 5 | 220,000 | - | - | 220,000 | (73,333 | ) | 146,667 | ||||||||||||||||||||
| Trade name | 5 | 257,000 | - | (66,000 | ) | 191,000 | (59,217 | ) | 131,783 | |||||||||||||||||||
| $ | 1,513,400 | $ | 1,312,500 | $ | (281,400 | ) | $ | 2,544,500 | $ | (191,288 | ) | $ | 2,353,212 | |||||||||||||||
The acquired technology of $1,312,500 was placed into service in April 2016 and the related amortization has been included in the table above from that date.
Included in depreciation and amortization on the consolidated statements of operations is amortization expense of $380,632 and $185,776 for the years ended March 31, 2017 and 2016, respectively.
During the year ended March 31, 2017, the Company recorded an impairment charge on intangible assets of $68,311 in general and administrative expenses as the carrying amount was determined not to be recoverable.
On March 1, 2016, the Company sold substantially all the assets of ACC to an unrelated third party. In connection with the sale, the Company received cash of $10,000 and issued a note receivable in the amount of $51,000, of which $5,000 was repaid prior to year-end. The Company recognized a loss on disposal of $476,745 related to this transaction, which included the write-off of the remaining goodwill and intangible assets of ACC in the amount of $461,500 and $27,427, respectively. In addition, management determined that the remaining goodwill and intangible assets of AKM in the amount of $83,943 and $123,342, respectively, was not recoverable. Accordingly, the Company recorded an impairment charge in the aggregate amount of $207,285 in general and administrative expenses for the year ended March 31, 2016.
Future amortization expense is estimated to be approximately as follows for each for the five years ending March 31 thereafter:
| 2018 | $ | 327,000 | ||
| 2019 | 327,000 | |||
| 2020 | 284,000 | |||
| 2021 | 262,269 | |||
| $ | 1,200,269 |
5. Accounts Payable and Accrued Liabilities
Accounts payable and accrued liabilities consisted of the following:
|
As of March 31, |
||||||||
| 2017 | 2016 | |||||||
| Accounts payable | $ | 3,569,011 | $ | 2,036,615 | ||||
| Physician share of MSSP | - | 62,000 | ||||||
| Accrued compensation | 2,860,340 | 2,156,339 | ||||||
| Income taxes payable | 20,827 | 110,653 | ||||||
| Accrued interest | 54,158 | 4,500 | ||||||
| Accrued professional fees | 1,379,037 | 202,200 | ||||||
| $ | 7,883,373 | $ | 4,572,307 | |||||
F-175
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
6. Notes Payable and Lines of Credit
Lines of credit consist of the following:
| As of March 31, | ||||||||
| 2017 | 2016 | |||||||
| Hendel $100,000 revolving line of credit due to financial institution, bore interest at prime plus 4.5% (8.5% and 8.00%, respectively, interest only payable monthly and matured on March 31, 2017 (Deconsolidated - see Note 1). | $ | - | $ | 88,764 | ||||
| BAHA $150,000 line of credit due to a financial institution, bears interest at prime rate plus 3% (7.0% and 6.50%, respectively), interest only payable monthly and matured in March 2017, currently due on demand. | 62,500 | 100,000 | ||||||
| $ | 62,500 | $ | 188,764 | |||||
Note Payable – Related Party (Chindris)
On November 17, 2016, AMM entered into a promissory note agreement with Liviu Chindris, M.D. (“Chindris Note”), a minority shareholder in APS, pursuant to which the Company borrowed the principal amount of $400,000 at an interest rate of 12% per annum. The Chindris Note required repayment of the outstanding principal and accrued interest, in full, on or before February 18, 2017. In connection with the issuance of the Chindris Note, the Company also issued a two-year stock purchase warrant Dr. Chindris (the “Chindris Warrant”) to purchase up to 5,000 shares of the Company’s common stock at an exercise price of $9.00 per share. The relative fair value of the Chindris Warrant was $6,880 and was recorded as debt discount to be amortized over the term of the Chindris Note using the straight-line method, which approximates the effective interest method. The Company amortized $6,880 of debt discount to interest expense for the year ended March 31, 2017. The Chindris Note was fully repaid prior to March 31, 2017.
Note Payable – Related Party (NMM)
In connection with the Merger Agreement (see Note 10), on January 3, 2017, the Company issued a promissory note to NMM in the amount of $5,000,000. Interest is due quarterly at the rate of Prime plus 1%, or 5% at March 31, 2017, with the entire principal balance being due on January 3, 2019. In the event of default, as defined, all unpaid principal and interest will become due and payable.
NNA Credit Agreements
In 2013, the Company entered into a $2.0 million secured revolving credit facility (the “Revolving Credit Agreement”) with NNA, an affiliate of Fresenius Medical Care Holdings, Inc. On December 20, 2013, the Company entered into the First Amendment to the Credit Agreement (the “Amended Credit Agreement”), which increased the revolving credit facility from $2 million to $4 million. This facility was repaid in October 2015, as explained in more detail below.
2014 NNA Financing
On March 28, 2014, the Company entered into a Credit Agreement (the “Credit Agreement”) pursuant to which NNA, extended to the Company (i) a $1,000,000 revolving line of credit (the “Revolving Loan”) and (ii) a $7,000,000 term loan (the “Term Loan”). The Company drew down the full amount of the Revolving Loan on October 23, 2014 (see Note 7).
| For The Years Ended March 31, | ||||||||
| 2017 | 2016 | |||||||
| Interest expense | $ | 82,905 | $ | 323,708 | ||||
| Amortization of loan fees and discount, net of out of period adjustment (Note 12) | - | (141,066 | ) | |||||
| $ | 82,905 | $ | 182,642 | |||||
F-176
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
7. Convertible Notes Payable
6% Alliance Apex Convertible Note
On March 30, 3017, the Company issued a Convertible Promissory Note to Alliance Apex, LLC (“Alliance Note”) for $4,990,000. The Alliance Note is due and payable to Alliance on (i) December 31, 2017, or (ii) the date on which the Change of Control Transaction (see Note 10 – NMM transaction) is terminated, whichever occurs first (“Maturity Date”). Upon the closing, on or before the Maturity Date, of the Merger, the Alliance Note together with the accrued and unpaid interest, shall automatically be converted (a “Mandatory Conversion”) into shares of the Company’s common stock, at a conversion price of $10.00 per share, subject to adjustment for stock splits, stock dividends, reclassifications and other similar recapitalization transactions that occur after the date of the Alliance Note. As part of an amendment to the Merger Agreement on March 30, 2017, the merger consideration to be paid by the Company to NMM was amended to include warrants to purchase 850,000 shares of common stock in the Company at an exercise price of $11 per share, that will only be granted in the event that the proposed merger between the Company and NMM is consummated (such warrant will not vest and will expire if the contemplated merger transaction does not occur) in exchange for both NMM providing a guarantee for the Alliance Note and as compensation to NMM for giving up their right to additional shares in the Company based on the agreed upon exchange ratio with NMM in the event that the Alliance Note is converted to common stock. As the guarantee was provided in conjunction with the warrants, the guarantee is considered a debt issuance cost. The Company estimated the debt issuance cost and related warrants issuable for the debt guarantee of $161,000 based on the incremental fair value to a market participant of a similar but unsecured debt instrument without such guarantee using a market rate for an unsecured high yield note of 12.4% and a 25% probability of the note not being converted. As of March 31, 2017, the debt issuance cost associated with the guarantee of $161,000 has been offset against the related Alliance convertible note resulting in a net balance of $4,829,000 and the related warrants issuable for the debt guarantee is recorded in additional paid-in capital.
8% NNA Convertible Note
Concurrently with the Credit Agreement entered into with NNA, the Company also entered into the Investment Agreement with NNA, pursuant to which the Company issued to NNA, an 8% Convertible Note in the original principal amount of $2,000,000 (the “Convertible Note”). The Company drew down the full principal amount of the Convertible Note on July 30, 2014. The Convertible Note would have matured on March 28, 2019, subject to NNA’s right to accelerate payment on the occurrence of certain events. The Company could redeem amounts outstanding under the Convertible Note on 60 days’ prior notice to NNA. Amounts outstanding under the Convertible Note were convertible at NNA’s sole election into shares of the Company’s common stock at an initial conversion price of $10.00 per share. The Company’s obligations under the Convertible Note were guaranteed by its subsidiaries and consolidated medical corporations.
On October 14, 2015, the Company entered into the Agreement with NMM pursuant to which the Company sold NMM 1,111,111 units, each Unit consisting of one share of Preferred Stock and one Warrant, for a total purchase price of $10,000,000, the proceeds of which were used by the Company primarily to repay the Revolving Loan and Term Loan owed by the Company to NNA and the balance the Company used for working capital purposes (see Note 9). The Company repaid approximately $7.5 million of the then outstanding NNA debt obligations and recorded a loss on debt extinguishment of approximately $266,000 related to this transaction.
9% Senior Subordinated Convertible Notes
The 9% Notes, issued January 31, 2013, bore interest at a rate of 9% per annum, were payable semiannually on August 15 and February 15, and matured February 15, 2016, and were subordinated. The principal of the 9% Notes, plus any accrued yet unpaid interest, was convertible, at any time by the holder at a conversion price of $4.00 per share, subject to adjustment for stock splits, stock dividends and reverse stock splits, into shares of the Company’s common stock.
In connection with the issuance of the 9% Notes in 2013, the holders of the 9% Notes received warrants to purchase 82,500 shares of the Company’s common stock at an exercise price of $4.50 per share, subject to adjustment for stock splits, reverse stock splits and stock dividends, which warrants are exercisable at any date prior to January 31, 2018, and were classified in equity. Certain holders of the 9% Notes converted an aggregate of approximately $554,000 of outstanding principal and accrued interest into 138,463 shares of the Company’s common stock prior to their maturity on February 15, 2016. Prior to conversion, the Company amortized approximately $14,000 of related debt discount and deferred financing costs in fiscal 2016.
Interest expense associated with the convertible notes payable consisted of the following:
| For The Years Ended March 31, | ||||||||
| 2017 | 2016 | |||||||
| Interest expense | $ | - | $ | 171,027 | ||||
| Amortization of loan fees and discount | - | 188,627 | ||||||
| $ | - | $ | 359,654 | |||||
F-177
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
8. Income Taxes
(Benefit from) provision of income taxes consists of the following:
| For The Years Ended March 31, | ||||||||
| 2017 | 2016 | |||||||
| Current: | ||||||||
| Federal | $ | (81,614 | ) | $ | (9,979 | ) | ||
| State | (6,069 | ) | 66,678 | |||||
| (87,683 | ) | 56,699 | ||||||
| Deferred: | ||||||||
| Federal | 25,598 | (81,277 | ) | |||||
| State | 14,590 | (46,459 | ) | |||||
| 40,188 | (127,736 | ) | ||||||
| Benefit from income taxes | $ | (47,495 | ) | $ | (71,037 | ) | ||
The Company uses the liability method of accounting for income taxes as set forth in ASC 740. Under the liability method, deferred taxes are determined based on differences between the financial statement and tax bases of assets and liabilities using enacted tax rates. As of March 31, 2017, the Company had federal and California tax net operating loss carryforwards of approximately $19.1 million and $21.3 million, respectively. The federal and California net operating loss carryforwards will expire at various dates from 2026 through 2037. Pursuant to Internal Revenue Code Sections 382 and 383, use of the Company’s net operating loss and credit carryforwards may be limited if a cumulative change in ownership of more than 50% occurs within any three-year period since the last ownership change. The Company may have had a change in control under these Sections. However, the Company does not anticipate performing a complete analysis of the limitation on the annual use of the net operating loss and tax credit carryforwards until the time that it projects it will be able to utilize these tax attributes.
Significant components of the Company’s deferred tax assets (liabilities) as of March 31, 2017 and March 31, 2016 are shown below. A valuation allowance of $11,557,356 and $8,369,878 as of March 31, 2017 and March 31, 2016, respectively, has been established against the Company’s deferred tax assets as realization of such assets is uncertain. The Company’s effective tax rate is different from the federal statutory rate of 34% due primarily to operating losses that receive no tax benefit as a result of a valuation allowance recorded for such losses.
Deferred tax assets (liabilities) consist of the following:
| For The Years Ended March 31, | ||||||||
| 2017 | 2016 | |||||||
| Deferred tax assets (liabilities): | ||||||||
| State taxes | $ | 5,718 | $ | 15,114 | ||||
| Stock options | 3,127,225 | 2,617,037 | ||||||
| Accrued payroll and related costs | - | 16,222 | ||||||
| Accrued hospital pool deficit | 25,747 | 329,430 | ||||||
| Net operating loss carryforward | 7,640,802 | 4,754,165 | ||||||
| Property and equipment | 42.623 | 1,588 | ||||||
| Acquired intangible assets | 113,171 | 65,748 | ||||||
| Other | 518,403 | 527,095 | ||||||
| Net deferred tax assets before valuation allowance | 11,473,689 | 8,326,399 | ||||||
| Valuation allowance | (11,557,356 | ) | (8,369,878 | ) | ||||
| Net deferred tax liabilities | $ | (83,667 | ) | $ | (43,479 | ) | ||
The provision for income taxes differs from the amount computed by applying the federal income tax rate as follows:
| For The Years Ended March 31, | ||||||||
| 2017 | 2016 | |||||||
| Tax provision at U.S. Federal statutory rates | 34.0 | % | 34.0 | % | ||||
| State income taxes net of federal benefit | (0.1 | )% | (0.3 | )% | ||||
| Nondeductible permanent items | 0.7 | % | (0.7 | )% | ||||
| Nontaxable entities | 0.3 | % | 5.4 | % | ||||
| Other | (3.4 | )% | 1.9 | % | ||||
| Change in valuation allowance | (31.0 | )% | (39.4 | )% | ||||
| Effective income tax rate | 0.5 | % | 0.9 | % | ||||
As of March 31, 2017 and March 31, 2016, the Company does not have any unrecognized tax benefits related to various federal and state income tax matters. The Company will recognize accrued interest and penalties related to unrecognized tax benefits in income tax expense.
F-178
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
The Company is subject to U.S. federal income tax as well as income tax of multiple state tax jurisdictions. The Company and its subsidiaries’ federal income tax returns are open to audit under the statute of limitations for the years ended March 31, 2014 onwards and state income tax returns are open to audit under the statute of limitations for the years ended January 31, 2013 onward. The Company does not anticipate material unrecognized tax benefits within the next 12 months.
9. Stockholders’ Equity
Preferred Stock – Series A
On October 14, 2015, Company entered into an agreement (the “Agreement”) with NMM pursuant to which the Company sold to NMM, and NMM purchased from the Company, in a private offering of securities, 1,111,111 units, each unit consisting of one share of the Company’s Preferred Stock (the “Series A”) and a stock purchase warrant to purchase one share of the Company’s common stock at an exercise price of $9.00 per share. NMM paid the Company an aggregate $10,000,000 for the units, the proceeds of which were used by the Company primarily to repay certain outstanding indebtedness owed by the Company to NNA and the balance for working capital.
The Series A has a liquidation preference in the amount of $9.00 per share plus any declared and unpaid dividends. The Preferred Stock can be voted for the number of shares of Common Stock into which the Series A could then be converted, which initially is one-for-one. The Series A is convertible into Common Stock, at the option of NMM, at any time after issuance at an initial conversion rate of one-for-one, subject to adjustment in the event of stock dividends, stock splits and certain other similar transactions.
At any time prior to conversion and through the Redemption Expiration Date (as described below), the Series A was able to be redeemed at the option of NMM, on one occasion, in the event that the Company’s net revenues for the four quarters ending September 30, 2016, as reported in its periodic filings under the Securities Exchange Act of 1934, as amended, were less than $60,000,000. In such event, the Company had up to one year from the date of the notice of redemption by NMM to redeem the Series A Preferred Stock, the NMM Warrant and any shares of common stock issued in connection with the exercise of any portion of the NMM Warrant theretofore (collectively the “Redeemed Securities”), for the aggregate price paid therefore by NMM, together with interest at a rate of 10% per annum from the date of the notice of redemption until the closing of the redemption. Any mandatory conversion described previously would not take place until such time as it was determined that that conditions for the redemption of the Redeemed Securities have not been satisfied or, if such conditions exist, NMM decided not to have such securities redeemed. As the redemption feature was not within the control of the Company, the Series A Preferred Stock did not qualify as permanent equity and was classified as mezzanine or temporary equity. The Company did not attain the $60,000,000 net revenues milestone noted above by September 30, 2016. Accordingly, the Series A were subject to redemption for $10,000,000. However, as part of the proposed Merger between NMM and the Company (see Note 10), NMM entered into a Consent and Waiver Agreement dated December 21, 2016 (the “NMM Waiver”), pursuant to which NMM has relinquished its right of redemption of the Series A Preferred Stock and the related common stock warrants. As a result of the NMM Waiver on December 21, 2016, the mezzanine equity was reclassified to permanent equity at its carrying amount of $7,077,778.
The common stock warrants may be exercised at any time after issuance and through October 14, 2020, for $9.00 per share, subject to adjustment in the event of stock dividends and stock splits. The warrants are not separately transferable from the Preferred Stock. The warrants were also subject to redemption in the event the Preferred Stock was redeemed by NMM, as described above. Accordingly, the Company previously accounted for such warrants as liabilities and has marked such liability to its fair value at March 31, 2016. The Company determined the fair value of the warrant liability to be $2,922,222 at inception which was estimated using the Monte Carlo valuation model (see Note 2) with the value of the Series A being the residual value of $7,077,778. As a result of the NMM Waiver, the fair value of the warrant at December 21, 2016 of $1,177,778 (see Note 2) was reclassified from liability to equity.
Without the written consent of NMM, between the Closing Date and the nine-month anniversary of the Closing Date, the Company shall not acquire, sell all or substantially all of its assets to, effect a change of control, or merge, combine or consolidate with, any other Person engaged in the business of being a MSO, ACO or IPA, or enter into any agreement with respect to any of the foregoing.
Preferred Stock – Series B
On March 30, 2016, Company entered into an agreement with NMM pursuant to which the Company sold to NMM, and NMM purchased from the Company, in a private offering of securities, 555,555 units, each Unit consisting of one share of the Company’s Series B Preferred Stock (“Series B”) and a warrant to purchase one share of the Company’s common stock at an exercise price of $10.00 per share. NMM paid the Company an aggregate $4,999,995 for the units. The proceeds were allocated to each Series B units and Series B warrants based upon their relative fair values in the amount of $3,884,745 and $1,115,250, respectively, as each class of securities met the requirements for permanent equity classification. The estimated fair value of the units was estimated using a Black-Scholes equity allocation option pricing method. The Company used a comparable company lookback volatility rate of 65.8%, and a risk-free rate of 1.2% - commensurate with the expected term of 5-years. In valuing the Series B warrants, the Company used a comparable company lookback volatility rate of 65.8%, and a risk-free rate of 1.2% - commensurate with the expected term of 5-years.
The Preferred Stock has a liquidation preference in the amount of $9.00 per share plus any declared and unpaid dividends. The Series B can be voted for the number of shares of Common Stock into which the Preferred Stock could then be converted, which initially is one-for-one. The Preferred Stock is convertible into Common Stock, at the option of NMM or mandatorily at any time prior to and including March 31, 2017, if the Company receives aggregate gross proceeds of not less than $5,000,000 in one or more transactions (other than transactions with NMM), at an initial conversion rate of one-for-one, subject to adjustment in the event of stock dividends, stock splits and certain other similar transactions.
F-179
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
The warrants may be exercised at any time after issuance and through March 30, 2021, for $10.00 per share, subject to adjustment in the event of stock dividends and stock splits.
Equity Incentive Plans
The Company’s 2010 Equity Incentive Plan (the “2010 Plan”) allowed the Board to grant up to 500,000 shares of the Company’s common stock, and provided for awards including incentive stock options, non-qualified options, restricted common stock, and stock appreciation rights. As of March 31, 2017, there were no shares available for grant.
On April 29, 2013 the Company’s Board of Directors approved the Company’s 2013 Equity Incentive Plan (the “2013 Plan”), pursuant to which 500,000 shares of the Company’s common stock were reserved for issuance thereunder. The Company received approval of the 2013 Plan from the Company’s stockholders on May 19, 2013. The Company issues new shares to satisfy stock option and warrant exercises under the 2013 Plan. As of March 31, 2017 there were no shares available for future grants under the 2013 Plan.
On December 15, 2015, the Company’s Board of Directors approved the Company’s 2015 Equity Incentive Plan (the “2015 Plan”), pursuant to which 1,500,000 shares of the Company’s common stock were reserved for issuance thereunder. In addition, shares that are subject to outstanding grants under the Company’s 2010 Plan and 2013 Plan but that ordinarily would have been restored to such plans reserve due to award forfeitures and terminations will roll into and become available for awards under the 2015 Plan. The 2015 Plan provides for awards, including incentive stock options, non-qualified options, restricted common stock, and stock appreciation rights. The 2015 Plan was subject to approval by the Company’s stockholders, which approval was obtained at the 2016 Annual Meeting of Stockholders that was held on September 14, 2016. As of March 31, 2017, there were approximately 1,023,600 shares available for future grants under the 2015 Plan.
Share Issuances
On November 17, 2015, the Company entered into the Conversion Agreement with NNA, Dr. Warren Hosseinion and Dr. Adrian Vazquez. Pursuant to the Conversion Agreement, the Company agreed to issue 275,000 shares of common stock and to pay accrued and unpaid interest of $47,112, to NNA in full satisfaction of NNA’s conversion and other rights under the 8% Convertible Note dated March 28, 2014, issued by NNA, in the principal amount of $2,000,000. Pursuant to the Conversion Agreement, the Company also agreed to issue a total of 325,000 shares of the Company’s Common Stock to NNA in exchange for all Warrants held by NNA, under which NNA had the right to purchase 300,000 shares of the Company’s Common Stock at an exercise price of $10 per share and 200,000 shares at an exercise price of $20 per share, in each case subject to anti-dilution adjustments. On the date of conversion, the fair value of the 600,000 shares of common stock was based on the market price of the stock of $6.00 per share, less a 15% discount for marketability or $3,060,000 at $5.10 per share. The fair value of all the existing warrants held by NNA and of the conversion feature liability, converted in exchange for the 600,000 shares of common stock, was $1,624,029 and $482,904, respectively. These amounts together with the carrying amount of the 8% convertible note and accrued interest of approximately $1,124,000 resulted in a gain of approximately $171,000 which is included as an off-set in the net loss on debt extinguishment of approximately $266,000 in the consolidated statement of operations (see Note 7).
In January 2016, the Company formed Apollo Care Connect, Inc. which acquired certain technology and other assets of Healarium, Inc., which provides us with a population health management platform that includes digital care plans, a case management module, connectivity with multiple healthcare tracking devices and the ability to integrate with multiple electronic health records to capture clinical data. The Company issued 275,000 shares of its common stock with a fair value of $1,512,500 in exchange for the acquired assets and the seller paid the Company $200,000.
On February 15, 2016, the Company issued an aggregate 138,463 shares of Common Stock upon the conversion by certain holders of the principal and accrued interest of the 9% Notes prior to their maturity on February 15, 2016 in the amount $553,851.
During the year ended March 31, 2017, the Company issued 150,000 shares of common stock and received approximately $172,000 from the exercise of certain warrants at an exercise price of $1.1485 per share.
A summary of the Company’s restricted stock issued to employees, directors and consultants with a right of repurchase of unlapsed or unvested shares is as follows:
| Weighted-Average Remaining Vesting Life |
Weighted-Average Per Share | |||||||||||||||
| Shares | (In Years) | Intrinsic Value | Grant Date Fair Value |
|||||||||||||
| Unvested or unlapsed shares at April 1, 2015 | 12,222 | 0.3 | $ | 0.50 | $ | 4.10 | ||||||||||
| Granted | - | - | - | - | ||||||||||||
| Vested/lapsed | (12,222 | ) | - | - | - | |||||||||||
| Forfeited | - | - | - | - | ||||||||||||
| Unvested or unlapsed shares at March 31, 2016 and 2017 | - | - | - | - | ||||||||||||
F-180
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Options
During January and February 2016, the Company issued options to purchase an aggregate of 374,150 shares of the Company’s common stock to certain employees and consultants. The options have exercise prices ranging from $5.79 - $6.37 and vesting terms between immediate through three years. See below for assumptions used to determine the grant date fair value of the stock options using the Black-Scholes Option Pricing Model.
During the year ended March 31, 2017, the Company issued options to purchase an aggregate of 149,200 shares of the Company’s common stock to certain employees, directors and consultants. The options have exercise prices ranging from $4.50 - $6.00 and vesting terms between six months through three years. See below for assumptions used to determine the grant date fair value of the stock options using the Black-Scholes Option Pricing Model.
The following table presents details of the assumptions used to calculate the weighted-average grant date fair value of common stock options granted by the Company:
| Years Ended | ||||||||
| March 31, | March 31, | |||||||
| 2017 | 2016 | |||||||
| Expected term (in years) | 4.6 – 6.0 | 6.0 | ||||||
| Expected volatility | 126.42 -136.04 | % | 133 | % | ||||
| Risk-free interest rate | 0.75 – 1.06 | % | 1.31 – 1.94 | % | ||||
| Expected dividends | $ | - | $ | - | ||||
| Weighted-average grant date fair value per share | $ | 3.92 | $ | 4.75 | ||||
Stock option activity is summarized below:
| Option Shares | Weighted-Average Per Share Exercise Price |
Weighted-Average Remaining Life (Years) |
Weighted-Average Per Share Intrinsic Value |
|||||||||||||
| Balance, April 1, 2015 | 776,500 | $ | 4.69 | 7.40 | $ | 1.50 | ||||||||||
| Granted | 374,150 | 5.97 | - | - | ||||||||||||
| Cancelled/expired | (86,500 | ) | 2.63 | - | - | |||||||||||
| Exercised | - | - | - | - | ||||||||||||
| Balance, March 31, 2016 | 1,064,150 | $ | 4.27 | 7.94 | $ | 2.27 | ||||||||||
| Granted | 149,200 | 4.78 | - | - | ||||||||||||
| Cancelled/expired | (48,000 | ) | 6.75 | - | - | |||||||||||
| Exercised | - | - | - | - | ||||||||||||
| Balance, March 31, 2017 | 1,165,350 | $ | 4.24 | 6.64 | $ | 4.86 | ||||||||||
| Vested and exercisable, March 31, 2017 | 1,028,043 | $ | 4.07 | 6.36 | $ | 5.25 | ||||||||||
ApolloMed ACO 2012 Equity Incentive Plan
On October 18, 2012 ApolloMed ACO’s Board of Directors adopted the ApolloMed Accountable Care Organization, Inc. 2012 Equity Incentive Plan (the “ACO Plan”) and reserved 9,000,000 shares of ApolloMed ACO’s common stock for issuance thereunder. The purpose of the ACO Plan is to encourage selected employees, directors, consultants and advisers to improve operations and increase the profitability of ApolloMed ACO and encourage selected employees, directors, consultants and advisers to accept or continue employment or association with ApolloMed ACO.
F-181
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
The following table summarizes the restricted stock award in the ACO Plan:
| Shares | Weighted-Average Remaining Vesting Life (Years) |
Weighted-Average Per Share Fair Value |
||||||||||
| Balance, April 1, 2015 | 3,752,000 | 0.8 | $ | 0.03 | ||||||||
| Granted | 184,000 | - | 0.77 | |||||||||
| Released | (183,996 | ) | - | 0.03 | ||||||||
| Balance, March 31, 2016 | 3,752,004 | - | 0.07 | |||||||||
| Granted | - | - | - | |||||||||
| Released | (32,000 | ) | - | - | ||||||||
| Balance, March 31, 2017 | 3,720,004 | - | $ | 0.07 | ||||||||
| Vested and exercisable, end of year | 3,720,004 | - | $ | 0.07 | ||||||||
Awards of restricted stock under the ACO Plan vest (i) one-third on the date of grant; (ii) one-third on the first anniversary of the date of grant, if the grantee has remained in service continuously until that date; and (iii) one-third on the second anniversary of the date of grant if the grantee has remained in service continuously until that date.
As of March 31, 2017, total unrecognized compensation costs related to non-vested stock-based compensation arrangements granted under the Company’s 2010, 2013 and 2015 Equity Plans, are as follows:
| Common stock options | $ | 435,739 |
The weighted-average period of years expected to recognize these compensation costs is 1.53 years.
Stock-based compensation expense related to common stock and common stock option awards is recognized over their respective vesting periods and was included in the accompanying consolidated statement of operations as follows:
|
For The Years Ended March 31, |
||||||||
| 2017 | 2016 | |||||||
| Stock-based compensation expense: | ||||||||
| Cost of services | $ | 4,906 | $ | 4,959 | ||||
| General and administrative | 1,101,548 | 1,099,017 | ||||||
| $ | 1,106,454 | $ | 1,103,976 | |||||
Warrants
Warrants consisted of the following:
| Weighted-Average Per Share Intrinsic Value |
Number of Warrants |
|||||||
| Outstanding at April 1, 2015 | $ | 0.46 | 914,500 | |||||
| Granted | - | 1,676,666 | ||||||
| Exercised | - | (500,000 | ) | |||||
| Cancelled | - | - | ||||||
| Outstanding at March 31, 2016 | 3.12 | 2,091,166 | ||||||
| Granted | - | 29,000 | ||||||
| Exercised | 4.87 | (150,000 | ) | |||||
| Cancelled | - | - | ||||||
| Outstanding at March 31, 2017 | $ | 4.68 | 1,970,166 | |||||
F-182
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
| Weighted | Weighted | |||||||||||||||||
| Average | Average | |||||||||||||||||
| Exercise Price Per | Warrants | Remaining | Warrants | Exercise Price Per | ||||||||||||||
| Share | Outstanding | Contractual Life | Exercisable | Share | ||||||||||||||
| $4.00-$5.00 | 188,500 | 0.85 | 169,500 | $ | 4.47 | |||||||||||||
| $9.00-$10.00 | 1,781,666 | 3.54 | 1,781,666 | 9.37 | ||||||||||||||
| $1.15-$10.00 | 1,970,166 | 3.28 | 1,951,166 | $ | 8.90 | |||||||||||||
On October 15, 2015, in connection with the NMM financing the Company issued a 5 year stock warrant to purchase up to 1,111,111 shares of common stock at an exercise price of $9.00 per share.
On March 30, 2016, in connection with the NMM financing the Company issued a 5 year stock warrant to purchase up to 555,555 shares of common stock at an exercise price of $10.00 per share.
Authorized Stock
At March 31, 2017 the Company was authorized to issue up to 100,000,000 shares of common stock. The Company is required to reserve and keep available out of the authorized but unissued shares of common stock such number of shares sufficient to effect the conversion of all outstanding preferred stock, the exercise of all outstanding warrants exercisable into shares of common stock, and shares granted and available for grant under the Company’s stock option plans. The amount of shares of common stock reserved for these purposes is as follows at March 31, 2017:
| Common stock issued and outstanding | 6,033,518 | |||
| Warrants outstanding | 1,970,166 | |||
| Stock options outstanding | 1,165,350 | |||
| Shares issuable upon conversion of convertible note | 499,000 | |||
| Preferred stock | 1,666,666 | |||
| 11,334,700 |
10. Commitments and Contingencies
Lease commitments
The Company’s headquarters are located at 700 North Brand Boulevard, Suite 1400, Glendale, California 91203. Under the original lease of the premises, the Company occupied space in Suite 220. On October 14, 2014, the Company's lease was amended by a Second Amendment (the “Second Lease Amendment”), pursuant to which the Company relocated its corporate headquarters to a larger suite in the same office building in October 2015. The Second Lease Amendment relocates the leased premises from Suite No. 220 to Suite Nos. 1400, 1425 and 1450, which collectively include 16,484 rentable square feet (the “New Premises”). The New Premises were improved with an allowance of $659,360, provided by the landlord, for construction and installation of equipment for the New Premises. The Second Lease Amendment also extends the term of the lease for approximately six years after the Company occupies the New Premises and increases the Company’s security deposit. The Second Lease Amendment sets the New Premises base rent at $37,913 per month for the first year and schedules annual increases in base rent each year until the final rental year, which is capped at $43,957 per month. However, the base rent will be abated by up to $228,049 subject to other terms of the lease. At March 31, 2017 and 2016, deferred rent liability associated with the Company’s leases was $747,418 and $728,877, respectively.
Future minimum rental payments required under the operating leases are as follows:
Year ending March 31,
| 2018 | $ | 982,000 | ||
| 2019 | 977,000 | |||
| 2020 | 994,000 | |||
| 2021 | 1,012,000 | |||
| 2022 | 716,000 | |||
| Thereafter | 910,000 | |||
| $ | 5,591,000 |
F-183
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Rent expense recorded was as follows:
| For The Years Ended March 31, | ||||||||
| 2017 | 2016 | |||||||
| Rent expense | $ | 951,244 | $ | 888,278 | ||||
Letters of Credit
In January 2013, in response to request by Prospect Medical Group, Inc., MMG arranged for City National Bank (“CNB”) to provide an irrevocable standby letter of credit in an amount up to $10,000, and entered into a security agreement in favor of CNB, as required by the Management Service Agreement effective February 1, 2013. In November, 2014 the irrevocable standby letter of credit and the security agreement amounts were increased to $ 500,000. The letter of credit is collateralized by a certificate of deposit which is included in restricted cash in the amount of $500,000 at March 31, 2017.
In December 2016, in response to a request by Humana Insurance Company and Humana Health Plan, Inc. (collectively “Humana”), MMG arranged for CNB to provide an irrevocable standby letter of credit in an amount up to $235,000 through December 31, 2017, and entered into a security agreement in favor of CNB, as required by the Independent Practice Association Participation Agreement effective January 1, 2015, including the addenda and attachments thereto, and as amended. The letter of credit is collateralized by a certificate of deposit which is included in restricted cash in the amount of $235,000 at March 31, 2017.
Other letters of credit consist of approximately $30,000. The cash deposit as part of the securities agreements are listed as restricted cash on the consolidated balance sheets at both March 31, 2017 and 2016.
Regulatory Matters
Laws and regulations governing the Medicare program and healthcare generally are complex and subject to interpretation. The Company believes that it is in compliance with all applicable laws and regulations and is not aware of any pending or threatened investigations involving allegations of potential wrongdoing. While no such regulatory inquiries have been made, compliance with such laws and regulations can be subject to future government review and interpretation as well as significant regulatory action including fines, penalties, and exclusion from the Medicare and Medi-Cal programs.
As a risk-bearing organization, the Company is required to follow regulations of the California Department of Managed Health Care (“DMHC”). The Company must comply with a minimum working capital requirement, Tangible Net Equity (“TNE”) requirement, cash-to-claims ratio and claims payment requirements prescribed by the DMHC. TNE is defined as net assets less intangibles, less non-allowable assets (which include amounts due from affiliates), plus subordinated obligations. The DMHC determined that, as of February 28, 2016, MMG, was not in compliance with the DMHC’s positive TNE requirement for a Risk Bearing Organization (“RBO”). As a result, the DMHC required MMG to develop and implement a corrective action plan (“CAP”) for such deficiency. MMG submitted a CAP to the DMHC, which the DMHC approved. MMG has up to one year to cure the deficiency. MMG achieved positive TNE as of the third quarter of fiscal 2017 and has maintained positive TNE to date. Since DMHC requirements are that an RBO should have positive TNE for one full quarter to be taken off a CAP, the Company believes that MMG is currently in compliance with DMHC requirements. The DMHC is currently reviewing filings the Company has made to confirm this compliance.
Many of the Company's payer and provider contracts are complex in nature and may be subject to differing interpretations regarding amounts due for the provision of medical services. Such differing interpretations may not come to light until a substantial period of time has passed following contract implementation. Liabilities for claims disputes are recorded when the loss is probable and can be estimated. Any adjustments to reserves are reflected in current operations.
In connection with DMHC’s approval of the CAP for MMG, on November 22, 2016, AMM, a wholly-owned subsidiary of the Company, entered into an Intercompany Revolving Loan Agreement (the “Loan Agreement”) with MMG, another affiliate of the Company, pursuant to which AMM has agreed to lend MMG up to $2,000,000 (the “Commitment Amount”) in one or more advances (collectively, “Advances”) that MMG may request from time to time during the term of the Loan Agreement. Interest on outstanding Advances shall accrue interest at a rate equal to the greater of 10% per annum or the LIBOR rate then in effect, and is payable monthly on the first business day of each month.
In an Event of Default (as defined in the Loan Agreement), interest on Advances shall accrue interest at a default rate equal to 3% per annum above the interest rate then in effect. Additionally, in an Event of Default, MMG may, among other things, accelerate all payments due under the Loan Agreement.
The Loan Agreement also contains other provisions typical of an agreement of this nature, including without limitation, representation and warranties, a right of set-off and governing law.
The Loan Agreement replaces substantially similar loan agreements between the parties (other than with respect to the Commitment Amount), including without limitation that certain Intercompany Revolving Loan Agreement dated as of February 1, 2013, that certain Amendment No. l to Intercompany Revolving Loan Agreement dated as of March 28, 2014, that certain Intercompany Revolving Loan Agreement dated as of June 27, 2014, and that certain Amendment No. 2 to Intercompany Revolving Loan Agreement dated as of March 30, 2016, all of which were terminated.
The Loan Agreement was entered into in response to a request of the California Department of Managed Health Care (“DMHC”), in order to comply with DMHC requirements in connection with its review of a pending Corrective Action Plan (“CAP”) for MMG (See Regulatory Matters).
F-184
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Also on November 22, 2016, and also at the request of the DMHC in connection with its review of the pending CAP for MMG, AMM and MMG entered into a Subordination Agreement (the “Subordination Agreement”), pursuant to which AMM has agreed to irrevocably and fully subordinate its right to repayment of Advances, together with interest thereon, under the Loan Agreement, to all other present and future creditors of MMG.
AMM also agreed that the payment by MMG of principal and interest of Advances under the Loan Agreement will be suspended and will not mature when, excluding the liability of MMG to pay AMM principal and interest under the Loan Agreement, if after giving effect to the payment, MMG would not be in compliance with the financial solvency requirements, as defined in and calculated under the Knox-Keene Health Care Service Plan Act of 1975, as amended (the “Knox-Keene Act”), and the rules promulgated thereunder.
AMM further agreed that, in the event of the liquidation or dissolution of MMG, the payment by MMG of principal and interest to AMM under the Loan Agreement shall be fully subordinated and subject to the prior payment or provision for payment in full of all claims of all other present and future creditors of MMG.
Upon the written consent of the director of the DMHC, all previous subordination agreements between AMM and MMG, including without limitation that certain Subordination Agreement dated June 27, 2014 between AMM and MMG and that certain Amended and Restated Subordination Agreement between AMM and MMG dated as of March, 30, 2016, shall be terminated. Once consented to by the director of the DMHC and executed by the parties, the Subordination Agreement may not be cancelled, terminated, rescinded or amended by mutual consent or otherwise, without the prior written consent of the director of the DMHC.
Legislation and HIPAA
The healthcare industry is subject to numerous laws and regulations of federal, state and local governments. These laws and regulations include, but are not necessarily limited to, matters such as licensure, accreditation, government healthcare program participation requirements, reimbursement for patient services, and Medicare and Medicaid fraud and abuse. Government activity has continued with respect to investigations and allegations concerning possible violations of fraud and abuse statutes and regulations by healthcare providers. Violations of these laws and regulations could result in expulsion from government healthcare programs together with the imposition of significant fines and penalties, as well as significant repayments for patient services previously billed.
The Company believes that it is in compliance with fraud and abuse regulations as well as other applicable government laws and regulations. Compliance with such laws and regulations can be subject to future government review and interpretation as well as regulatory actions unknown or unasserted at this time.
The Health Insurance Portability and Accountability Act (“HIPAA”) assures health insurance portability, reduces healthcare fraud and abuse, guarantees security and privacy of health information, and enforces standards for health information. The Health Information Technology for Economic and Clinical Health Act (“HITECH Act”) expanded upon HIPAA in a number of ways, including establishing notification requirements for certain breaches of protected health information. In addition to these federal rules, California has also developed strict standards for the privacy and security of health information as well as for reporting certain violations and breaches. The Company may be subject to significant fines and penalties if found not to be compliant with these state or federal provisions.
Affordable Care Act
The Patient Protection and Affordable Care Act (“ACA”) will substantially reform the United States health care system. The legislation impacts multiple aspects of the health care system, including many provisions that change payments from Medicare, Medicaid and insurance companies. Starting in 2014, the legislation required the establishment of health insurance exchanges, which will provide individuals without employer-provided health care coverage the opportunity to purchase insurance. It is anticipated that some employers currently offering insurance to employees will opt to have employees seek insurance coverage through the insurance exchanges. It is possible that the reimbursement rates paid by insurers participating in the insurance exchanges may be substantially different than rates paid under current health insurance products. Another significant component of the ACA is the expansion of the Medicaid program to a wide range of newly eligible individuals. In anticipation of this expansion, payments under certain existing programs, such as Medicare disproportionate share, will be substantially decreased. Each state’s participation in an expanded Medicaid program is optional. However, the ACA may be amended, or repealed and replaced by the Congress. The potential outcome of the repeal and replacement is unknown at this time but could have a material impact on the Company.
Legal
In the ordinary course of the Company’s business, the Company becomes involved in pending and threatened legal actions and proceedings, most of which involve claims of medical malpractice related to medical services that are provided by our affiliated hospitalists. We may also become subject to other lawsuits which could involve significant claims and/or significant defense costs.
F-185
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
Liability Insurance
The Company believes that the Company’s insurance coverage is appropriate based upon the Company’s claims experience and the nature and risks of the Company’s business. In addition to the known incidents that have resulted in the assertion of claims, the Company cannot be certain that the Company’s insurance coverage will be adequate to cover liabilities arising out of claims asserted against the Company, the Company’s affiliated professional organizations or the Company’s affiliated hospitalists in the future where the outcomes of such claims are unfavorable. The Company believes that the ultimate resolution of all pending claims, including liabilities in excess of the Company’s insurance coverage, will not have a material adverse effect on the Company’s financial position, results of operations or cash flows; however, there can be no assurance that future claims will not have such a material adverse effect on the Company’s business.
Although the Company currently maintains liability insurance policies on a claims-made basis, which are intended to cover malpractice liability and certain other claims, the coverage must be renewed annually, and may not continue to be available to the Company in future years at acceptable costs, and on favorable terms.
Employment and Consulting Agreements
On December 20, 2016, AMM, a wholly-owned subsidiary of the Company, entered into new employment agreements with each of Warren Hosseinion, M.D., Adrian Vazquez, M.D., Gary Augusta and Mihir Shah. The new employment agreements were approved by the Compensation Committee of the Board of Directors of the Company and replace the employment agreements previously entered into with (i) Dr. Hosseinion and Dr. Vazquez on March 28, 2014, as amended on January 12, 2016 and as amended and restated on June 29, 2016, and (ii) Mr. Shah on July 21, 2016. The new employment agreements provide that Dr. Hosseinion, Dr. Vazquez and Mr. Shah will continue to be paid their current base salary in the aggregate amount of $1,160,000, and that Mr. Augusta will be paid a base salary of $300,000 and revise certain term, bonus and severance arrangements as provided therein. Mr. Augusta’s consulting agreement through Flacane Advisers, Inc. (“Flacane”) has been terminated.
Each of the new employment agreements has
an initial term of three years with automatic annual renewals and entitles the executive to 20 business days of paid time off per
calendar year. Accrued and unused paid time off shall be paid in cash at the end of each calendar year. Under the new employment
agreements, each executive is eligible to receive an annual bonus and is granted certain vesting rights and Accrued Benefits (as
such term is defined in the respective employment agreement) if the executive’s employment is terminated without “Cause”
(as such term is defined in the respective employment agreement) or if the executive resigns with “Good Reason” (as
such term is defined in the respective employment agreement) during the employment term.
NMM Transaction
On December 21, 2016, the Company, entered into an Agreement and Plan of Merger (the “Merger Agreement”) among the Company, Apollo Acquisition Corp., a California corporation and wholly-owned subsidiary of the Company (“Merger Subsidiary”), NMM, and Kenneth Sim, M.D., not individually but in his capacity as the representative of the shareholders of NMM (the “Shareholders’ Representative”).
Thomas Lam, M.D. and Kenneth Sim, M.D. entered into Voting Agreements with the Company. Under the Voting Agreements, Dr. Sim and Dr. Lam have agreed, among other things, to vote in favor of the approval and adoption of the Merger and the Merger Agreement.
Under the terms of the Merger Agreement, Merger Subsidiary will merge with and into NMM, with NMM becoming a wholly owned subsidiary of Apollo Medical Holdings, as the Merger. The Merger is intended to qualify for federal income tax purposes as a tax deferred reorganization under the provisions of Section 368(a) of the Internal Revenue Code of 1986. In the transaction NMM will receive such number of shares of ApolloMed common stock such that NMM shareholders will own 82% and the Company shareholders will own 18% of issued and outstanding shares at closing. Additionally, NMM has agreed to relinquish its redemption rights relating to preferred stock it owns in the Company pursuant to the terms of a Consent and Waiver Agreement dated as of December 21, 2016 by and between the Company and NMM. The transaction was approved unanimously by the Board of Directors of both companies. Consummation of the Merger is subject to various closing conditions, including, among other things, approval by the stockholders of the Company and the stockholders of NMM. As part of the Merger Agreement, the Company and NMM have made various mutual representations and warranties.
Within five business days following the execution of the Merger Agreement, NMM was required to provide a working capital loan to the Company in the principal amount of $5,000,000, which loan the Company received on January 3, 2017. The loan is evidenced by a promissory note, which was issued on January 3, 2017. The promissory note has a term of two years, with the Company’s payment obligations commencing on February 1, 2017 and continuing on a quarterly basis thereafter until January 3, 2019. Under the terms of the promissory note, the Company must pay NMM interest on the principal balance outstanding at the prime rate plus one percent (1%). The Company may voluntarily prepay the outstanding principal and interest in whole or in part without penalty or premium. Upon the occurrence of any Event of Default (as such term is defined in the promissory note), the unpaid principal amount of, and all accrued but unpaid interest on, the promissory note will become due and payable immediately at the option of NMM. In such event, NMM may, at its option, declare the entire unpaid balance of the promissory note, together with all accrued interest, applicable fees, and costs and charges, including costs of collection, if any, to be immediately due and payable in cash.
The Merger Agreement grants each party the ability to update disclosure schedules through January 20, 2017. If any updated disclosure schedules are found to be unacceptable to the receiving party, as determined in such receiving party’s sole discretion, then such receiving party may terminate the Merger Agreement no later than February 3, 2017 (see below for amendment to the Merger Agreement).
F-186
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
The Merger Agreement provides that Thomas Lam, M.D., the Chief Executive Officer of NMM, and Warren Hosseinion, M.D., will be Co-Chief Executive Officers of the combined company upon closing of the transaction. Kenneth Sim, M.D., who currently serves as Chairman of NMM, will be Executive Chairman of the Company. Gary Augusta, current Executive Chairman of the Company, will be President, Mihir Shah will continue as Chief Financial Officer, and Hing Ang, current Chief Financial Officer of NMM will be the Chief Operating Officer. Adrian Vazquez, M.D. and Albert Young, M.D. will be Co-Chief Medical Officers. The Board of Directors will consist of nine directors, five of whom will be recommended for nomination to the Company’s Nomination and Corporate Governance Committee from NMM and four of whom will be recommended for nomination of the Company’s Nomination and Corporate Governance Committee from the Company.
Consummation of the Merger is subject to various closing conditions, including, among other things, approval under Hart-Scott-Rodino Act from Department of Justice and Federal Trade Commission, approval by The Company’s stockholders and the stockholders of NMM.
On March 30, 2017, NMM and ApolloMed entered into the Amendment to Agreement and Plan of Merger (“Amended Merger Agreement”) to exclude from the exchange ratio the 499,000 ApolloMed shares issued or issuable pursuant to a securities purchase agreement dated as of March 30, 2017, between ApolloMed and Appliance Apex, LLC. As part of an amendment to the Merger Agreement on March 30, 2017, the merger consideration to be paid by the Company to NMM was amended to include warrants to purchase 850,000 shares of common stock in the Company at an exercise price of $11 per share.
As of the date of this filing, the Merger has not been completed.
Registration Rights Agreement
On June 28, 2016, NNA and the Company entered into the Third Amendment (the “Third Amendment”) to the Registration Rights Agreement dated May 28, 2014, as amended by the First Amendment and Acknowledgement dated as of February 6, 2015, the Second Amendment and Conversion Agreement dated as of November 17, 2015, and the amendments thereto (collectively, the “Registration Agreement”). Pursuant to the Third Amendment, the Company had until April 28, 2017 to register NNA’s registrable securities on a registration statement filed with the SEC and the Company had until the earlier of (i) October 27, 2017 or (ii) the 5th trading day after the date the Company is notified by the SEC that such registration statement will not be reviewed or will not be subject to further review to have such registration statement declared effective by the SEC. All other provisions of the Registration Agreement remain in full force and effect, including paying NNA liquidated damages of 1.5% of the total purchase price of the registrable securities owned by NNA, payable in shares of the Company’s common stock, if the Company does not comply with these deadlines.
On April 26, 2017, the Company entered into a Fourth Amendment (the “Amendment”) with NNA. The Amendment amended the Registration Rights Agreement, dated as of March 28, 2014, between the Company and NNA (as amended by the First Amendment and Acknowledgement, dated as of February 6, 2015, the Amendment to First Amendment and Acknowledgement, dated as of July 7, 2015, the Second Amendment and Conversion Agreement, dated as of November 17, 2015, the Third Amendment, dated as of June 28, 2016, and as further amended by the amendments thereto, the “Registration Rights Agreement”).
The Amendment amended the Registration Rights Agreement to extend the deadline for the Company to file a resale registration statement covering NNA’s registrable securities to December 31, 2017, and also to extend the date by which the Company is required to use its commercially reasonable best efforts to cause such registration statement to be declared effective to June 30, 2018 (or, if earlier, the fifth (5th) trading day after the date on which the Securities and Exchange Commission notifies the Company that such registration statement will not be “reviewed” or will not be subject to further review).
11. Related Party Transactions
On January 12, 2016, the Company entered into a new consulting agreement with Mr. Gary Augusta, the President of Flacane Advisors, Inc. and the Company’s Executive Chairman of the Board of Directors (the “2016 Augusta Consulting Agreement”) to replace the substantially similar 2015 Augusta Consulting Agreement that expired by its terms on December 31, 2015. Under the 2016 Augusta Consulting Agreement, the Augusta Consultant is paid $25,000 per month to provide business and strategic services to the Company; and Augusta Consultant is also eligible to receive options to purchase shares of the Company’s common stock as determined by the Company’s Board of Directors. In addition, Mr. Augusta is subject to a Directors Agreement with the Company dated March 7, 2012. During the years ended March 31, 2017 and 2016, the Company incurred approximately $280,000 and $770,000, respectively, of an aggregate of consulting expense and reimbursement of out of pocket expenses in connection with the 2015 Augusta Consulting Agreement and 2016 Augusta Consulting Agreement. The Company owed the Augusta Consultant approximately $11,300 and $9,500, at March 31, 2017 and 2016, respectively. The 2016 Augusta Consulting Agreement was terminated on December 20, 2016 and replaced by an employment agreement with Mr. Augusta (see Note 10).
During the year ended March 31, 2016, the Company raised approximately $15 million in connection with the sale of shares of Series A and Series B preferred stock and warrants from NMM in which Dr. Thomas Lam, one of the Company’s directors is a significant shareholder (see Note 9). On January 3, 2017, pursuant to a promissory note agreement, NMM provided a loan to ApolloMed in the principal amount of $5,000,000 (see Note 6).
As part of an amendment to the Merger Agreement on March 30, 2017, the merger consideration to be paid by the Company to NMM was amended to include warrants to purchase 850,000 shares of common stock in the Company at an exercise price of $11 per share, that will only be granted in the event that the proposed merger between the Company and NMM is consummated (such warrant will not vest and will expire if the contemplated merger transaction does not occur) in exchange for both NMM providing a guarantee for the Alliance Note and as compensation to NMM for giving up their right to additional shares in the Company based on the agreed upon exchange ratio with NM in the event that the Alliance Note is converted to common stock.
F-187
APOLLO MEDICAL HOLDINGS, INC.
NOTES TO CONSOLIDATED FINANCIAL STATEMENTS
As of March 31, 2 2016, accounts payable in the consolidated balance sheets includes $104,500 for principal and accrued interest owed to a 9% note holder who is also a shareholder of the Company and such amount was paid during the year ended March 31, 2017.
In September 2015, the Company entered into a note receivable with Rob Mikitarian, a minority owner in APS, in the amount of approximately $150,000. The note accrues interest at 3% per annum and is due on or before September 2017. At both March 31, 2017 and 2016, the balance of the note was approximately $150,000 and is included in other receivables in the accompanying consolidated balance sheets.
In September 2015, the Company entered into a note receivable with Dr. Liviu Chindris, a minority owner in APS, in the amount of approximately $105,000. The note accrues interest at 3% per annum and is due on or before September 2017. At both March 31, 2017 and 2016, the balance of the note was approximately $105,000 and is included in other receivables in the accompanying consolidated balance sheets.
In November, 2016 the Company issued the Chindris Note to Dr, Liviu Chindris, a minority owner in APS, in the principal amount of $400,000 that bore interest at the rate of 12% annually. The note was due February 17, 2017 and was repaid. (see Note 6).
In December 2016, the Company billed NMM, current merger candidate, $930,169 for its 50% share of startup costs related to Next Generation ACO (NGACO) model. See more detail about this model in the “Our Operations and Industry” section of the Form 10-K.
F-188
F-189
CONDENSED CONSOLIDATED BALANCE SHEETS
(UNAUDITED)
| June 30, | March 31, | |||||||
| 2017 | 2017 | |||||||
| ASSETS | ||||||||
| Cash and cash equivalents | $ | 31,206,495 | $ | 8,664,211 | ||||
| Accounts receivable, net of allowance for doubtful accounts of $461,650 and $475,080, respectively | 5,423,618 | 5,506,472 | ||||||
| Other receivables | 806,148 | 464,085 | ||||||
| Due from affiliates | - | 18,314 | ||||||
| Prepaid expenses and other current assets | 282,732 | 269,168 | ||||||
| Total current assets | 37,718,993 | 14,922,250 | ||||||
| Property and equipment, net | 1,167,680 | 1,205,139 | ||||||
| Restricted cash | 745,117 | 765,058 | ||||||
| Intangible assets, net | 1,822,542 | 1,904,269 | ||||||
| Goodwill | 1,622,483 | 1,622,483 | ||||||
| Other assets | 221,979 | 225,358 | ||||||
| TOTAL ASSETS | $ | 43,298,794 | $ | 20,644,557 | ||||
| LIABILITIES AND STOCKHOLDERS’ EQUITY | ||||||||
| Accounts payable and accrued liabilities | $ | 16,212,983 | $ | 7,883,373 | ||||
| Medical liabilities | 19,718,135 | 1,768,231 | ||||||
| Convertible note payable, net of debt issuance cost of $107,333 and $161,000, respectively | 4,882,667 | 4,829,000 | ||||||
| Lines of credit | 25,000 | 62,500 | ||||||
| Total current liabilities | 40,838,785 | 14,543,104 | ||||||
| Note payable – related party | 5,000,000 | 5,000,000 | ||||||
| Deferred rent liability | 715,462 | 747,418 | ||||||
| Deferred tax liability | 83,667 | 83,667 | ||||||
|
TOTAL LIABILITIES |
46,637,914 | 20,374,189 | ||||||
| COMMITMENTS AND CONTINGENCIES (see Note 8) | ||||||||
| STOCKHOLDERS’ (DEFICIT) EQUITY | ||||||||
| Series A Preferred stock, par value $0.001; 5,000,000 shares authorized (inclusive of Series B Preferred stock); 1,111,111 issued and outstanding Liquidation preference of $9,999,999 | 7,077,778 | 7,077,778 | ||||||
| Series B Preferred stock, par value $0.001; 5,000,000 shares authorized (inclusive of Series A Preferred stock) 555,555 issued and outstanding Liquidation preference of $4,999,995 | 3,884,745 | 3,884,745 | ||||||
| Common stock, par value $0.001; 100,000,000 shares authorized, 6,033,518 shares issued and outstanding | 6,033 | 6,033 | ||||||
| Additional paid-in capital | 26,555,514 | 26,331,948 | ||||||
| Accumulated deficit | (41,266,193 | ) | (37,654,381 | ) | ||||
| Stockholders’ deficit attributable to Apollo Medical Holdings, Inc. | (3,742,123 | ) | (353,877 | ) | ||||
| Non-controlling interest | 403,003 | 624,245 | ||||||
| Total stockholders’ (deficit) equity | (3,339,120 | ) | 270,368 | |||||
| TOTAL LIABILITIES AND STOCKHOLDERS’ (DEFICIT) EQUITY | $ | 43,298,794 | $ | 20,644,557 | ||||
The accompanying notes are an integral part of these unaudited condensed consolidated financial statements.
F-190
CONDENSED CONSOLIDATED STATEMENTS OF OPERATIONS
(UNAUDITED)
| Three Months Ended June 30, |
||||||||
| 2017 | 2016 | |||||||
| Net revenues | $ | 41,575,480 | $ | 12,371,673 | ||||
| Costs and expenses | ||||||||
| Cost of services | 40,239,642 | 10,133,005 | ||||||
| General and administrative | 4,889,184 | 3,836,475 | ||||||
| Depreciation and amortization | 155,267 | 164,658 | ||||||
| Total costs and expenses | 45,284,093 | 14,134,138 | ||||||
| Loss from operations | (3,708,613 | ) | (1,762,465 | ) | ||||
| Other (expense) income: | ||||||||
| Interest expense | (192,989 | ) | (2,659 | ) | ||||
| Gain on change in fair value of warrant liability | - | 822,222 | ||||||
| Other income |
38,657 |
1,971 | ||||||
| Total other (expense) income, net | (154,332 | ) | 821,534 | |||||
| Loss before benefit from income taxes | (3,862,945 | ) | (940,931 | ) | ||||
| Benefit from income taxes | (29,891 | ) | (41,553 | ) | ||||
| Net loss | (3,833,054 | ) | (899,378 | ) | ||||
| Net loss (income) attributable to non-controlling interest | 221,242 | (415,879 | ) | |||||
| Net loss attributable to Apollo Medical Holdings, Inc. | $ | (3,611,812 | ) | $ | (1,315,257 | ) | ||
| Net loss per share: | ||||||||
| Basic and diluted | $ | (0.60 | ) | $ | (0.22 | ) | ||
| Weighted average number of shares of common stock outstanding: | ||||||||
| Basic and diluted | 6,033,518 | 5,914,826 | ||||||
The accompanying notes are an integral part of these unaudited condensed consolidated financial statements.
F-191
CONSOLIDATED STATEMENTS OF CASH FLOWS
(UNAUDITED)
| Three Months Ended June 30, | ||||||||
| 2017 | 2016 | |||||||
| CASH FLOWS FROM OPERATING ACTIVITIES: | ||||||||
| Net loss | $ | (3,833,054 | ) | $ | (899,378 | ) | ||
| Adjustments to reconcile net loss to net cash provided by (used in) operating activities: | ||||||||
| Provision for doubtful accounts, net of recoveries | 6,642 | 167,496 | ||||||
| Depreciation and amortization expense | 155,267 | 164,658 | ||||||
| Stock-based compensation expense | 223,566 | 247,717 | ||||||
| Amortization of deferred financing costs | 53,667 | 37,926 | ||||||
| Change in fair value of warrant liability | - | (822,222 | ) | |||||
| Changes in assets and liabilities: | ||||||||
| Accounts receivable | 76,212 | (774,087 | ) | |||||
| Other receivables | (342,063 | ) | 265,980 | |||||
| Due from affiliates | 18,314 | 453 | ||||||
| Prepaid expenses and other current assets | (13,564 | ) | (215,182 | ) | ||||
| Restricted cash | 19,941 | - | ||||||
| Other assets | 3,379 | 2,762 | ||||||
| Accounts payable and accrued liabilities | 8,329,610 | (317,451 | ) | |||||
| Deferred rent liability | (31,956 | ) | 33,584 | |||||
| Medical liabilities | 17,949,904 | (158,668 | ) | |||||
| Net cash provided by (used in) operating activities | 22,615,865 | (2,266,412 | ) | |||||
| Cash flows from investing activities: | ||||||||
| Property and equipment acquired | (36,081 | ) | (163,511 | ) | ||||
| Net cash used in investing activities | (36,081 | ) | (163,511 | ) | ||||
| Cash flows from financing activities: | ||||||||
| Principal payments on lines of credit | (37,500 | ) | (12,500 | ) | ||||
| Distributions to non-controlling interest shareholder | - | (450,000 | ) | |||||
| Proceeds from the exercise of warrants | - | 132,002 | ||||||
| Net cash used in financing activities | (37,500 | ) | (330,498 | ) | ||||
| Net increase (decrease) in cash and cash equivalents | 22,542,284 | (2,760,421 | ) | |||||
| Cash and cash equivalents, beginning of period | 8,664,211 | 9,270,010 | ||||||
| Cash and cash equivalents, end of period | $ | 31,206,495 | $ | 6,509,589 | ||||
| Supplementary disclosures of cash flow information: | ||||||||
| Interest paid | $ | 584 | $ | 7,142 | ||||
| Income taxes paid | $ | 17,591 | $ | 16,400 | ||||
The accompanying notes are an integral part of these unaudited condensed consolidated financial statements.
F-192
NOTES TO CONDENSED CONSOLIDATED FINANCIAL STATEMENTS
(UNAUDITED)
| 1. | Description of Business |
Overview
Apollo Medical Holdings, Inc. (“the Company” or “ApolloMed”) and its affiliated physician groups are a physician-centric integrated population health management company working to provide coordinated, outcomes-based medical care in a cost-effective manner. Led by a management team with over a decade of experience, ApolloMed has built a company and culture that is focused on physicians providing high-quality medical care, population health management and care coordination for patients, particularly senior patients and patients with multiple chronic conditions. ApolloMed believes that the Company is well-positioned to take advantage of changes in the rapidly evolving U.S. healthcare industry, as there is a growing national movement towards more results-oriented healthcare centered on the triple aim of patient satisfaction, high-quality care and cost efficiency.
ApolloMed serves Medicare, Medicaid and health maintenance organization (“HMO”) patients, and uninsured patients, in California. The Company primarily provides services to patients who are covered predominantly by private or public insurance, although the Company derives a small portion of its revenue from non-insured patients. The Company provides care coordination services to each major constituent of the healthcare delivery system, including patients, families, primary care physicians, specialists, acute care hospitals, alternative sites of inpatient care, physician groups and health plans.
ApolloMed’s physician network consists of hospitalists, primary care physicians and specialist physicians primarily through ApolloMed’s owned and affiliated physician groups. ApolloMed operates through its subsidiaries, including Apollo Medical Management, Inc. (“AMM”), Pulmonary Critical Care Management, Inc. (“PCCM”), Verdugo Medical Management, Inc. (“VMM”), ApolloMed Palliative Services, LLC (“APS”), ApolloMed Accountable Care Organization, Inc. (“ApolloMed ACO”), and Apollo Care Connect, Inc. (“ApolloCare”).
Through its wholly-owned subsidiary, AMM, ApolloMed manages affiliated medical groups, which consist of ApolloMed Hospitalists (“AMH”), a hospitalist company, Maverick Medical Group, Inc. (“MMG”), AKM Medical Group, Inc. (“AKM”), Southern California Heart Centers (“SCHC”), Bay Area Hospitalist Associates, A Medical Corporation (“BAHA”) and APA ACO, Inc. (“APAACO”). Through its wholly-owned subsidiary PCCM, ApolloMed previously managed Los Angeles Lung Center (“LALC”) (see below for deconsolidation), and through its wholly-owned subsidiary VMM, ApolloMed previously managed Eli Hendel, M.D., Inc. (“Hendel”) (see below for deconsolidation). AMM, PCCM and VMM each operate as a physician practice management company and are in the business of providing management services to physician practice corporations under long-term management service agreements, pursuant to which AMM, PCCM or VMM, as applicable, manages all non-medical services for the affiliated medical group and has exclusive authority over all non-medical decision making related to ongoing business operations.
ApolloMed has a controlling interest in APS, which owns two Los Angeles-based companies, Best Choice Hospice Care LLC (“BCHC”) and Holistic Health Home Health Care Inc. (“HCHHA”).
ApolloMed also has a controlling interest in ApolloMed ACO, which participates in the Medicare Shared Savings Program (“MSSP”), the goal of which is to improve the quality of patient care and outcomes through more efficient and coordinated approach among providers. Revenues earned by ApolloMed ACO are uncertain, and, if such amounts are payable by the Centers for Medicare & Medicaid Services (“CMS”), they will be paid on an annual basis significantly after the time earned (which may take several years), and are contingent on various factors, including achievement of the minimum savings rate as determined by MSSP for the relevant period. Such payments are earned and made on an “all or nothing” basis. The Company considers revenue, if any, under the MSSP, as contingent upon the realization of program savings as determined by CMS, and are not considered earned and therefore are not recognized as revenue until notice from CMS that cash payments are to be imminently received. CMS determined that the Company did not meet the minimum savings threshold in performance year 2015 and therefore did not receive the “all or nothing” annual shared savings payment in fiscal 2017. The Company is eligible to be considered for an “all or nothing” payment under this program for performance year 2016 (which, if it is paid, would be paid to the Company in the second or third quarter of fiscal 2018).
In January 2016, the Company formed ApolloCare, which acquired certain technology and other assets of Healarium, Inc., which provides the Company with a cloud and mobile-based population health management platform that includes digital care plans, a case management module, connectivity with multiple healthcare tracking devices and the ability to integrate with multiple electronic health records to capture clinical data.
During fiscal 2016, the Company combined the operations of AKM into those of MMG.
In November 2016, BAHA Acquisition Corp., an affiliated entity owned by the Company’s CEO and consolidated as a variable interest entity, acquired the non-controlling interest in BAHA which was previously consolidated as a variable interest entity, and continues to have its financial results consolidated with those of the Company as a variable interest entity. As part of the transaction, the Company acquired the non-controlling interest of BAHA and was reflected as an equity transaction as there was no change in control.
F-193
On December 21, 2016, the Company entered into an Agreement and Plan of Merger (the “Merger Agreement”) among the Company, Apollo Acquisition Corp., a wholly-owned subsidiary of ours (“Merger Subsidiary”), Network Medical Management, Inc. (“NMM”) and Kenneth Sim, M.D., in his capacity as the representative of the shareholders of NMM, pursuant to which NMM, one of the largest healthcare management services organizations in the United States that currently is responsible for coordinating the care for over 600,000 covered patients in Southern and Central California through a network of ten IPAs with over 4,000 contracted physicians, will merge into Merger Subsidiary (the “Merger”) and upon consummation of the Merger, NMM shareholders will receive such number of shares of the Company’s common stock (“Common Stock”) such that, after giving effect to the Merger and assuming there would be no dissenting NMM shareholders at the closing, NMM shareholders will own 82% of the total issued and outstanding shares of Common Stock at the closing of the Merger and the Company’s current stockholders will own the other 18% (the “Exchange Ratio”). Additionally, NMM agreed to relinquish its redemption rights relating to the Company’s Series A Preferred Stock that NMM owns.
On March 30, 2017, NMM, the Company and other relevant parties entered into an Amendment to the Merger Agreement (the “Merger Agreement Amendment”) to exclude, for purposes of calculating the Exchange Ratio, from “parent shares” (as defined in the Merger Agreement) 499,000 shares of Common Stock issued or issuable pursuant to a securities purchase agreement dated as of March 30, 2017, between the Company and Appliance Apex, LLC. As part the Merger Agreement Amendment, the merger consideration to be paid by the Company to NMM was amended to include warrants to purchase 850,000 shares of Common Stock at an exercise price of $11 per share in the closing of the proposed Merger. The waiting period under the Hart-Scott-Rodino Antitrust Improvements Act of 1976, as amended (“HSR”), with respect to the proposed Merger expired on July 7, 2017. The expiration of the HSR waiting period satisfies a condition to the closing of Merger. Consummation of the Merger, which remains subject to other conditions described in the Merger Agreement, including approval by stockholders of the Company and the shareholders of NMM, is expected to take place in the second half of calendar year 2017. On August 10, 2017, NMM and the Company filed a registration statement on form S-4 with the Securities and Exchange Commission (the “SEC”) in connection with the proposed Merger.
On January 1, 2017 and March 24, 2017, PCCM and VMM amended the management services agreements that they entered into with LALC and Hendel, respectively, and among other things, reduced the scope of services to be provided by PCCM and VMM to align with the actual course of dealing between the parties. Based on the Company’s evaluation of current accounting guidance, it was determined that the Company no longer holds an explicit or implicit variable interest in these entities, and accordingly LALC and Hendel are no longer consolidated effective January 1, 2017 and their operations are not included in the March 31, 2017 and subsequent consolidated financial statements of the Company as of such date.
On January 18, 2017, CMS announced that APAACO, which is owned 50% by ApolloMed and 50% by NMM, has been approved to participate in CMS’ Next Generation ACO Model (the “NGACO Model”). Through this new model, CMS will partner with APAACO and other accountable care organizations (“ACOs”) experienced in coordinating care for populations of patients and whose provider groups are willing to assume higher levels of financial risk and potentially achieve a higher reward under the NGACO Model. The NGACO program began on January 1, 2017. AMM, one of the Company’s wholly-owned subsidiaries, has a long-term management services agreement with APAACO. APAACO is consolidated as a variable interest entity by AMM as it was determined that AMM is the primary beneficiary of APAACO.
In connection with the approval by CMS for APAACO to participate in the NGACO Model, CMS and APAACO have entered into a NGACO Model Participation Agreement (the “Participation Agreement”), which was last modified on December 15, 2016. The term of the Participation Agreement is for two performance years, from January 1, 2017 through December 31, 2018. CMS may offer to renew the Participation Agreement for an additional term of two performance years. Additionally, the Participation Agreement may be terminated sooner by CMS as specified therein. Under the NGACO Model, CMS grants to APAACO a pool of patients to manage (direct care and pay providers) based on a budget negotiated with CMS. APAACO is responsible to manage medical costs for these patients to receive services from doctors and medical service providers as influenced by the Company. The Company earns revenues based on the negotiated contract terms with in-network providers. The Company’s profits or losses in managing the services provided by out-of-network providers are generally determined on an annual basis after reconciliation with CMS. The Company receives capitation from CMS on a monthly basis. Based on the Company’s efficiency or lack thereof, the Company’s profits/losses on providing such services are capped with CMS. The Company records the receipts from CMS as revenue as the Company is primarily responsible and liable for managing the costs incurred by the patients and to satisfy all provider obligations, assuming the credit risk through the arrangement with CMS, and controlling the funds, the services provided and the process by which the providers are ultimately paid.
Liquidity and Capital Resources
The accompanying condensed consolidated financial statements have been prepared assuming that the Company will continue as a going concern, which contemplates the realization of assets and settlement of liabilities in the normal course of business.
F-194
As shown in the accompanying unaudited condensed consolidated financial statements, the Company has incurred a net loss of approximately $3.8 million during the three months ended June 30, 2017, and, as of June 30, 2017, has a net working capital deficit of approximately $3.1 million and an accumulated deficit of approximately $41.3 million.
These factors among others raise substantial doubt about the Company’s ability to continue as a going concern.
The ability of the Company to continue as a going concern is dependent upon the Company’s ability to increase revenue, reduce costs, attain a satisfactory level of profitability, obtain suitable and adequate financing, and further develop business. In addition, the Company may have to reduce certain overhead costs through the deferral of salaries and other means, and settle liabilities through negotiation. There can be no assurance that management’s plan and attempts will be successful.
The Company’s ability to continue as a going concern also depends, in significant part, on its ability to obtain the necessary financing to meet its obligations and pay the Company’s obligations arising from normal business operations as they come due. To date, the Company has funded the Company’s operations from a combination of internally generated cash flow and external sources, including the proceeds from the issuance of equity and/or debt securities. The Company is substantially dependent upon the consummation of the Merger to meet the Company’s liquidity requirements. The Company is currently exploring sources of additional funding. Without limiting its available options, future equity financings will most likely be through the sale of additional shares of its securities. It is possible that the Company could also offer warrants, options and/or rights in conjunction with any future issuances of its common stock. The Company’s current sources of revenues are insufficient to cover its operating costs, and as such, has incurred an operating loss since its inception. Thus, until the Company can generate sufficient cash flows to fund operations, the Company remains substantially dependent on raising additional capital through debt and/or equity transactions. Currently, the Company does not have any commitments or assurances for the proposed Merger or additional capital, nor can the Company provide assurance that such financing will be available on favorable terms, or at all. If, after utilizing the existing sources of capital available to the Company, further capital needs are identified and the Company is not successful in obtaining the financing, it may be forced to curtail its existing or planned future operations.
The accompanying condensed consolidated financial statements do not include any adjustments relating to the recoverability and classification of recorded assets, or the amounts and classification of liabilities that might be necessary in the event that the Company cannot continue as a going concern.
Certain reclassifications have been made to comparative amounts in order to conform with current period presentation.
| 2. | Summary of Significant Accounting Policies |
Basis of Presentation
The accompanying condensed consolidated balance sheet at March 31, 2017, has been derived from audited consolidated financial statements. The unaudited condensed consolidated financial statements as of June 30, 2017 and for the three months ended June 30, 2017 and 2016, have been prepared in accordance with accounting principles generally accepted in the United States of America (“U.S. GAAP”) for interim financial information and with the instructions to Form 10-Q and Article 8 of Regulation S-X. Accordingly, they do not include all of the information and footnotes required by U.S. GAAP for complete financial statements, and should be read in conjunction with the audited consolidated financial statements and related footnotes included in the Company’s Annual Report on Form 10-K for the year ended March 31, 2017 as filed with the SEC on June 29, 2017. In the opinion of management, all material adjustments (consisting of normal recurring adjustments) considered necessary for a fair presentation have been made in the condensed consolidated financial statements. The condensed consolidated financial statements include all material adjustments (consisting of normal recurring accruals) necessary to make the condensed consolidated financial statements not misleading as required by Regulation S-X, Rule 10-01. Operating results for the three months ended June 30, 2017 are not necessarily indicative of the results that may be expected for the year ending March 31, 2018.
Principles of Consolidation
The Company’s condensed consolidated financial statements include the accounts of Apollo Medical Holdings, Inc. and all its wholly and majority owned subsidiaries as well as all variable interest entities where it is the primary beneficiary, including physician practice corporations (“PPCs”) managed by a subsidiary of the Company under long-term management service agreements (“MSAs”), under which the subsidiary provides and performs all non-medical management and administrative services. Through the MSAs, the Company generally has exclusive authority over all non-medical decision making related to the ongoing business operations of the PPCs. Therefore, the Company typically consolidates the revenue and expenses of a PPC from the date of execution of the applicable MSA. Each MSA typically has a term from 10 to 20 years and is not terminable by the respective PPC (except for a limited number of situations such as material breach by or bankruptcy of the other party). Because, as explained in Note 1, effective on January 1, 2017, the Company no longer holds an explicit or implicit variable interest in LALC and Hendel, the two PPCs are not consolidated as of such date. All intercompany balances and transactions have been eliminated.
Business Combinations
The Company uses the acquisition method of accounting for all business combinations, which requires assets and liabilities of the acquiree to be recorded at fair value to measure the fair value of the consideration transferred, including contingent consideration, to be determined on the acquisition date, and to account for acquisition related costs separately from the business combination.
F-195
Reportable Segments
The Company operates as one reportable segment, the healthcare delivery segment. While the Company has determined it has six reporting units, such reporting units do not meet the quantitative threshold under U.S. GAAP to be considered a reportable segment. As such, these reporting units and all related activities are aggregated into a single reportable segment in the Company’s consolidated financial statements.
Revenue Recognition
Revenue consists of contracted, fee-for-service, capitation, MSSP ACO, hospitalist agreements, and NGACO revenue. Revenue is recorded in the period in which services are rendered. Revenue is principally derived from the provision of healthcare staffing services to patients within healthcare facilities and ACO management. The form of billing and related risk of collection for such services may vary by customer. The following is a summary of the principal forms of the Company’s billing arrangements and how net revenue is recognized for each.
Contracted revenue
Contracted revenue represents revenue generated under contracts for which the Company provides physician and other healthcare staffing and administrative services in return for a contractually negotiated fee. Contract revenue consists primarily of billings based on hours of healthcare staffing provided at agreed-to hourly rates. Revenue in such cases is recognized as the hours are worked by the Company’s staff and contractors. Additionally, contract revenue also includes supplemental revenue from hospitals where the Company may have a fee-for-service contract arrangement or provide physician advisory services to the medical staff at a specific facility. Contract revenue for the supplemental billing in such cases is recognized based on the terms of each individual contract. Such contract terms generally either provide for a fixed monthly dollar amount or a variable amount based upon measurable monthly activity, such as hours staffed, patient visits or collections per visit compared to a minimum activity threshold. Such supplemental revenues based on variable arrangements are usually contractually fixed on a monthly, quarterly or annual calculation basis considering the variable factors negotiated in each such arrangement. Such supplemental revenues are recognized as revenue in the period when such amounts are determined to be fixed and therefore contractually obligated as payable by the customer under the terms of the respective agreement. Additionally, the Company derives a portion of the Company’s revenue as a contractual bonus from collections received by the Company’s partners and such revenue is contingent upon the collection of third-party billings. These revenues are not considered earned and therefore not recognized as revenue until actual cash collections are achieved in accordance with the contractual arrangements for such services.
Fee-for-service revenue
Fee-for-service revenue represents revenue earned under contracts in which the Company bills and collects the professional component of charges for medical services rendered by the Company’s contracted physicians. Under the fee-for-service arrangements, the Company bills patients for services provided and receives payment from patients or their third-party payors. Fee-for-service revenue is reported net of contractual allowances and policy discounts. All services provided are expected to result in cash flows and are therefore reflected as net revenue in the consolidated financial statements. Fee-for-service revenue is recognized in the period in which the services are rendered to specific patients and reduced immediately for the estimated impact of contractual allowances in the case of those patients having third-party payor coverage. The recognition of net revenue (gross charges less contractual allowances) from such visits is dependent on such factors as proper completion of medical charts following a patient visit, the forwarding of such charts to the Company’s billing center for medical coding and entering into the Company’s billing system and the verification of each patient’s submission or representation at the time services are rendered as to the payor(s) responsible for payment of such services. Revenue is recorded based on the information known at the time of entering of such information into the Company’s billing systems as well as an estimate of the revenue associated with medical services.
Capitation revenue
Capitation revenue (net of capitation withheld to fund risk share deficits) is recognized in the month in which the Company is obligated to provide services. Minor ongoing adjustments to prior months’ capitation, primarily arising from contracted HMOs finalizing monthly patient eligibility data for additions or subtractions of enrollees, are recognized in the month they are communicated to the Company. Managed care revenues of the Company consist primarily of capitated fees for medical services provided by the Company under a provider service agreement (“PSA”) or capitated arrangements directly made with various managed care providers including HMOs and management service organizations. Capitation revenue under the PSA and HMO contracts is prepaid monthly to the Company based on the number of enrollees electing the Company as their healthcare provider. Additionally, Medicare pays capitation using a “Risk Adjustment model,” which compensates managed care organizations and providers based on the health status (acuity) of each individual enrollee. Health plans and providers with higher acuity enrollees will receive more and those with lower acuity enrollees will receive less. Under Risk Adjustment, capitation is determined based on health severity, measured using patient encounter data. Capitation is paid on an interim basis based on data submitted for the enrollee for the preceding year and is adjusted in subsequent periods after the final data is compiled. Positive or negative capitation adjustments are made for Medicare enrollees with conditions requiring more or less healthcare services than assumed in the interim payments. Since the Company cannot reliably predict these adjustments, periodic changes in capitation amounts earned as a result of Risk Adjustment are recognized when those changes are communicated by the health plans to the Company. Additionally, Medicare pays capitation using a “Risk Adjustment Model,” which compensates managed care organizations and providers based on the health status (acuity) of each individual enrollee. Health plans and providers with higher acuity enrollees will receive more and those with lower acuity enrollees will receive less. Under Risk Adjustment, capitation is determined based on health severity, measured using patient encounter data. Capitation is paid on an interim basis based on data submitted for the enrollee for the preceding year and is adjusted in subsequent periods after the final data is compiled. Positive or negative capitation adjustments are made for Medicare enrollees with conditions requiring a different level of healthcare services than assumed in making the interim payments. In prior years, periodic changes in capitation amounts earned as a result of Risk Adjustment were recognized when those changes were communicated by the health plans to the Company. Starting in fiscal year 2017, the Company started to record the estimated amount that it expects to be received from Medicare for Risk Adjustment based on its current data, instead of the initially received capitation, as part of revenue. The Company does not believe that this change resulted in a material change in the amount of revenue recognized.
F-196
HMO contracts also include provisions to share in the risk for enrollee hospitalization, whereby the Company can earn additional incentive revenue or incur penalties based upon the utilization of hospital services. Typically, any shared risk deficits are not payable until and unless the Company generates future risk sharing surpluses, or if the HMO withholds a portion of the capitation revenue to fund any risk share deficits. At the termination of the HMO contract, any accumulated risk share deficit is typically extinguished. Due to the lack of access to information necessary to estimate the related costs, shared-risk amounts receivable from the HMOs are only recorded when such amounts are known. Risk pools for the prior contract years are generally final settled in the third or fourth quarter of the following fiscal year.
In addition to risk-sharing revenues, the Company also receives incentives under “pay-for-performance” programs for quality medical care, based on various criteria. These incentives are generally recorded in the third and fourth quarters of the fiscal year and recorded when such amounts are known.
Under full risk capitation contracts, an affiliated hospital enters into agreements with several HMOs, pursuant to which, the affiliated hospital provides hospital, medical, and other healthcare services to enrollees under a fixed capitation arrangement (“Capitation Arrangement”). In addition, under a risk pool sharing agreement, the affiliated hospital and a medical group agree to establish a Hospital Control Program to serve the enrollees, pursuant to which, the medical group is allocated a percentage of the profit or loss, after deductions for costs to the affiliated hospital. The Company typically participates in full risk programs under the terms of a PSA, with health plans whereby the Company is wholly liable for the deficits allocated to the medical group under the arrangement. The related liability is included in medical liabilities in the accompanying consolidated balance sheets at June 30, 2017 and March 31, 2017. See “Medical Liabilities” below.
Medicare Shared Savings Program Revenue
The Company, through its subsidiary ApolloMed ACO, participates in the MSSP, which is sponsored by CMS. The goal of the MSSP is to improve the quality of patient care and outcomes through more efficient and coordinated approach among providers. The MSSP allows ACO participants to share in cost savings it generates in connection with rendering medical services to Medicare patients. Payments to ACO participants, if any, will be calculated annually by CMS on cost savings generated by the ACO participant relative to the ACO participants’ cost savings benchmark. The MSSP is a program managed by CMS that has an evolving payment methodology. Revenues earned by ApolloMed ACO are uncertain, and, if such amounts are payable by the CMS, they will be paid on an annual basis significantly after the time earned (which may take several years), and will be contingent on various factors, including achievement of the minimum savings rate as determined by MSSP for the relevant period. Such payments are earned and made on an “all or nothing” basis. The Company considers revenue, if any, under the MSSP, as contingent upon the realization of program savings as determined by CMS, and are not considered earned and therefore are not recognized as revenue until notice from CMS that cash payments are to be imminently received.
Hospitalist Agreements
During fiscal 2017, the Company entered into several hospitalist agreements with hospitals, whereby the Company earns a stipend fee plus a fee based on an agreed percentage of fee-for-service collections. The fee is recorded at an amount net of the portion owed to the hospitals (the Company collects all fees on behalf of the hospitals). The fee revenue is further reduced by a portion subject to quality metrics which is only recorded as revenue upon the Company meeting these metrics. The Company considered the indicators of gross revenue and net revenue reporting under ASC 605-45-45, “Revenue Recognition: Principal Agent Considerations” and determined that revenue from this arrangement is recorded at net.
Next Generation Accountable Care Organization Revenue
Under the NGACO Model, CMS grants APAACO, which is jointly owned by the Company and NMM, a pool of patients to manage (direct care and pay providers) based on a budget established with CMS. APAACO is responsible to manage medical costs for these patients. The patients will receive services from physicians and other medical service providers that are both in-network and out-of-network. The Company receives capitation from CMS on a monthly basis to pay claims from in-network providers. The Company records such capitation received from CMS as revenue as the Company is primarily responsible and liable for managing the patient care and to satisfy provider obligations, is assuming the credit risk for the services provided by in-network providers through its arrangement with CMS, and has control of the funds, the services provided and the process by which the providers are ultimately paid. Claims from out-of-network providers are generally processed or paid by CMS and the Company’s profits or losses in managing the services provided by out-of-network providers are generally determined on an annual basis after reconciliation with CMS. Pursuant to the Company’s risk share agreement with CMS, the Company will be eligible to receive the surplus or be liable for the deficit according to the budget established by CMS based on the Company’s efficiency or lack thereof, respectively, in managing how the patients assigned to APAACO by CMS are served by in-network and out-of-network providers. The Company’s profits or losses on providing such services are both capped by CMS. The Company will recognize such surplus or deficit upon substantial completion of reconciliation and determination of the amounts. In accordance with ASC 605-45-45, “Revenue Recognition: Principal Agent Considerations” the Company records such revenues on the gross basis.
The Company also has arrangements for billing and payment services with the medical providers within the NGACO network. The Company retains certain defined percentages of the payments made to the providers in exchange for using the Company’s billing and payment services. The revenue for this service is earned as payments are made to medical providers.
F-197
Cash and Cash Equivalents
Cash and cash equivalents consists of highly liquid investments with an initial maturity of three months or less at date of purchase to be cash equivalents.
Restricted Cash
Restricted cash primarily consists of cash held as collateral to secure standby letters of credits as required by certain contracts.
Accounts Receivable and Allowance for Doubtful Accounts
Accounts receivable primarily consists of amounts due from third-party payors, including government sponsored Medicare and Medicaid programs, insurance companies, and amounts due from hospitals and patients. Accounts receivable are recorded and stated at the amount expected to be collected.
The Company maintains reserves for potential credit losses on accounts receivable. The Company reviews the composition of accounts receivable and analyzes historical bad debts, customer concentrations, customer credit worthiness, current economic trends and changes in customer payment patterns to evaluate the adequacy of these reserves. The Company also regularly analyzes the ultimate collectability of accounts receivable after certain stages of the collection cycle using a look-back analysis to determine the amount of receivables subsequently collected and adjustments are recorded when necessary. Reserves are recorded primarily on a specific identification basis.
Concentrations
The Company had the following major payors that contributed the following percentage of net revenue:
| Three Months Ended June 30, 2017 |
Three Months Ended June 30, 2016 |
|||||||
| Governmental – Medicare/Medi-Cal | 72.1 | % | 23.6 | % | ||||
| LA Care | * | 14.5 | % | |||||
| Allied Physicians | * | 14.1 | % | |||||
* Represents less than 10%
Receivables from major payors amounted to the following percentage of total accounts receivable:
| June 30, 2017 | March 31, 2017 | |||||||
| Governmental – Medicare/Medi-Cal | 28.5 | % | 20.5 | % | ||||
| Allied Physicians | 13.8 | % | 12.8 | % | ||||
The increase in government revenue is due to APAACO’s new NGACO contract with CMS of approximately $27.9 million that went into effect in the first quarter of fiscal year 2018.
The Company maintains its cash and cash equivalents and restricted cash in bank deposit accounts, which, at times, may exceed federally insured limits. The Company has not experienced any losses in such accounts; however, amounts in excess of the federally insured limit may be at risk if the bank experiences financial difficulties. Approximately $31.7 million was in excess of the Federal Deposit Insurance Corporation limits of $250,000 per depositor as of June 30, 2017.
The Company’s business and operations are concentrated in one state, California. Any material changes by California with respect to strategy, taxation and economics of healthcare delivery, reimbursements, financial requirements or other aspects of regulation of the healthcare industry could have an adverse effect on the Company’s operations and cost of doing business.
Medical Liabilities
The Company is responsible for integrated care that the associated physicians and contracted hospitals provide to its enrollees under risk-pool arrangements. The Company provides integrated care to health plan enrollees through a network of contracted providers under sub-capitation and direct patient service arrangements, company-operated clinics and staff physicians. Medical costs for professional and institutional services rendered by contracted providers are recorded as cost of services in the accompanying consolidated statements of operations. Costs for operating medical clinics, including the salaries of medical personnel, are also recorded in cost of services, while non-medical personnel and support costs are included in general and administrative expense.
F-198
An estimate of amounts due to contracted physicians, hospitals, and other professional providers is included in medical liabilities in the accompanying consolidated balance sheets. Medical liabilities include claims reported as of the balance sheet date and estimates of incurred but not reported claims (“IBNR”). Such estimates are developed using actuarial methods and are based on many variables, including the utilization of health care services, historical payment patterns, cost trends, product mix, seasonality, changes in membership, and other factors. As APAACO’s NGACO program is new and no sufficient claims history is available, the medical liabilities for the NGACO program are estimated and booked at 100% of the revenue less actual claims processed for or paid to in-network providers (after taking into account the average discount negotiated with the in-network providers). The Company plans to use the traditional lag models as the claims history matures. The estimation methods and the resulting reserves are periodically reviewed and updated. Many of the medical contracts are complex in nature and may be subject to differing interpretations regarding amounts due for the provision of various services. Such differing interpretations may not come to light until a substantial period of time has passed following the contract implementation. The Company has a $20,000 per member professional stop-loss and $200,000 per member stop-loss for Medi-Cal patients in institutional risk pools. Any adjustments to reserves are reflected in current operations.
The Company’s medical liabilities were as follows:
| Three Months Ended June 30, 2017 |
Year Ended March 31, 2017 |
|||||||
| Balance, beginning of period | $ | 1,768,231 | $ | 2,670,709 | ||||
| Incurred health care costs: | ||||||||
| Current year | 30,109,821 | 10,365,502 | ||||||
| Claims paid: | ||||||||
| Current year | (11,017,283 | ) | (8,524,215 | ) | ||||
| Prior years | (1,575,049 | ) | (1,881,869 | ) | ||||
| Total claims paid | (12,592,332 | ) | (10,406,084 | ) | ||||
| Risk pool settlement | - | 814,733 | ||||||
| Accrual for net surplus (deficit) from full risk capitation contracts | 432,415 | (1,676,629 | ) | |||||
| Balance, end of period | $ | 19,718,135 | $ | 1,768,231 | ||||
Deferred Financing Costs
The Company’s costs relating to debt issuance have been deferred and are amortized over the lives of the respective loans, using the effective interest method and is recorded as interest expense in the condensed consolidated statements of operations.
During the three months ended June 30, 2017 and 2016, the Company’s amortization of debt issuance costs amounted to $53,667 and $37,926, respectively.
Stock-Based Compensation
The Company maintains a stock-based compensation program for employees, non-employees, directors and consultants, which is more fully described in Note 6. The value of stock-based awards so measured is recognized as compensation expense on a cumulative straight-line basis over the vesting terms of the awards, adjusted for forfeitures as they occur. The Company sells certain of its restricted common stock to its employees, directors and consultants with a right (but not obligation) of repurchase feature that lapses based on performance of services in the future.
The Company accounts for share-based awards granted to persons other than employees and directors under ASC 505-50, Equity-Based Payments to Non-Employees. As such, the fair value of such shares is periodically re-measured using an appropriate valuation model and income or expense is recognized over the vesting period.
Fair Value of Financial Instruments
The Company’s accounting for Fair Value Measurement and Disclosures defines fair value as the exchange price that would be received for an asset or paid to transfer a liability (an exit price) in the principal or most advantageous market for the asset or liability in an orderly transaction between market participants on the measurement date. This topic also establishes a fair value hierarchy which requires classification based on observable and unobservable inputs when measuring fair value. The fair value hierarchy distinguishes between assumptions based on market data (observable inputs) and an entity’s own assumptions (unobservable inputs). The hierarchy consists of three levels:
Level one — Quoted market prices in active markets for identical assets or liabilities;
Level two — Inputs other than level one inputs that are either directly or indirectly observable; and
Level three — Unobservable inputs developed using estimates and assumptions, which are developed by the reporting entity and reflect those assumptions that a market participant would use.
F-199
Determining which category an asset or liability falls within the hierarchy requires significant judgment. The Company evaluates its hierarchy disclosures each quarter.
The carrying amount reported in the accompanying condensed consolidated balance sheets for cash and cash equivalents, accounts receivable, accounts payable and accrued expenses approximates fair value because of the short-term maturity of those instruments. The carrying amount for borrowings under the lines of credit approximate fair value which is determined by using interest rates that are available for similar debt obligations with similar terms at the balance sheet date.
Warrant liability
In October 2015, the Company issued a stock purchase warrant (the “Series A Warrant”) to NMM in connection with its purchase of the Company’s Series A convertible preferred stock (the “Series A Preferred Stock”) (see Note 6), which initially required liability classification. The fair value of the warrant liability of approximately $2.8 million at March 31, 2016, was estimated using the Monte Carlo valuation model, using the following inputs: term of 4.5 years, risk free rate of 1.13%, no dividends, volatility of 65.7%, share price of $5.93 per share based on the trading price of the Company’s common stock adjusted for marketability discount, and a 0% probability of redemption of the warrant shares issued along with the shares of the Series A Preferred Stock issued to NMM in October 2015. The fair value of the warrant liability of approximately $2 million at June 30, 2016, was estimated using the Monte Carlo valuation model which used the following inputs: term of 4.3 years, risk free rate of 0.90%, no dividends, volatility of 64.4%, share price of $5 per share based on the trading price of the Company’s common stock adjusted for a marketability discount. As of June 30, 2017 and March 31, 2017, the Company’s outstanding warrants did not require liability classification.
There was no financial instrument measured at fair value on a recurring basis as of June 30, 2017 and March 31, 2017.
There was no Level 3 input measured on a recurring basis in the three months ended June 30, 2017. The following summarizes activity of Level 3 inputs measured on a recurring basis in the three months ended June 30, 2016:
| Warrant Liability |
||||
| Balance at March 31, 2016 | $ | 2,811,111 | ||
| Gain on change in fair value of warrant liability | (822,222 | ) | ||
| Balance at June 30, 2016 | $ | 1,988,889 | ||
The gain on change in fair value of the warrant liability of $822,222 for the three months ended June 30, 2016 is included in the accompanying condensed consolidated statement of operations. As there was no warrant liability at either March 31, 2017 or June 30, 2017, there is no change in the fair value of warrant liability for the three months ended June 30, 2017.
Non-controlling Interests
The non-controlling interests recorded in the Company’s consolidated financial statements includes the equity of PPCs in which the Company has determined that it has a controlling financial interest and for which consolidation is required as a result of management contracts entered into with these entities owned by third-party physicians. The nature of these contracts provide the Company with a monthly management fee to provide the services described above, and as such, the adjustments to non-controlling interests in any period subsequent to initial consolidation would relate to either capital contributions or distributions by the non-controlling parties as well as income or losses attributable to certain non-controlling interests. Non-controlling interests also represent third-party minority equity ownership interests which are majority owned by the Company.
Basic and Diluted Earnings per Share
Basic net income (loss) per share is calculated using the weighted average number of shares of the Company’s common stock issued and outstanding during a certain period, and is calculated by dividing net income (loss) by the weighted average number of shares of the Company’s common stock issued and outstanding during such period. Diluted net income (loss) per share is calculated using the weighted average number of common and potentially dilutive common shares outstanding during the period, using the as-if converted method for secured convertible notes, preferred stock, and the treasury stock method for options and warrants.
The following table sets forth the number of shares excluded from the computation of diluted earnings per share, as their inclusion would be anti-dilutive:
| Three Months Ended June 30, | ||||||||
| 2017 | 2016 | |||||||
| Preferred stock | 1,666,666 | 1,666,666 | ||||||
| Options | 1,099,850 | 533,500 | ||||||
| Warrants | 1,264,611 | 199,500 | ||||||
| Convertible notes | 506,547 | - | ||||||
| 4,537,674 | 2,399,666 | |||||||
F-200
New Accounting Pronouncements
In February 2016, the FASB issued ASU 2016-02, Leases (“ASU 2016-02”). This new standard establishes a right-of-use (ROU) model that requires a lessee to record a ROU asset and a lease liability on the balance sheet for all leases with terms longer than 12 months. Leases will be classified as either finance or operating, with classification affecting the pattern of expense recognition in the income statement. ASU 2016-02 is effective for fiscal years beginning after December 15, 2018, including interim periods within those fiscal years. Early adoption is permitted. A modified retrospective transition approach is required for lessees for capital and operating leases existing at, or entered into after, the beginning of the earliest comparative period presented in the financial statements, with certain practical expedients available. The Company is currently evaluating the impact of the adoption of ASU 2016-02 on the consolidated financial statements.
In March 2016, the FASB issued ASU 2016-09, Compensation - Stock Compensation (Topic 718): Improvements to Employee Share-Based Payment Accounting (“ASU 2016-09”). This ASU makes several modifications to Topic 718 related to the accounting for forfeitures, employer tax withholding on share-based compensation, and the financial statement presentation of excess tax benefits or deficiencies. With respect to the accounting for forfeitures, ASU 2016-09 allows an entity to elect as an accounting policy either to continue to estimate the total number of awards for which the requisite service period will not be rendered (as currently required) or to account for forfeitures when they occur. This entity-wide accounting policy election only applies to service conditions; for performance conditions, the entity continues to assess the probability that such conditions will be achieved. An entity must also disclose its policy election for forfeitures. ASU 2016-09 also clarifies the statement of cash flows presentation for certain components of share-based awards. The standard is effective for interim and annual reporting periods beginning after December 15, 2016, with early adoption permitted. The Company adopted this guidance on April 1, 2017 and chose the option to account for forfeitures as they occur. Such adoption did not have a material impact on the Company’s consolidated financial statements and related disclosures.
In January 2016, the FASB issued ASU No. 2016-01, Financial Instruments - Overall (Topic 825-10): Recognition and Measurement of Financial Assets and Financial Liabilities (“ASU 2016-01”). ASU 2016-01 addresses certain aspects of recognition, measurement, presentation and disclosures of financial instruments including the requirement to measure certain equity investments at fair value with changes in fair value recognized in net income. ASU 2016-01 will become effective for the Company beginning interim period April 1, 2018. The Company is currently evaluating the guidance to determine the potential impact on its financial condition, results of operations, cash flows and financial statement disclosures.
Recently, the FASB issued the following accounting standard updates related to ASU 2014-09 (Topic 606), Revenue Contracts with Customers:
| · | ASU No. 2014-09, Revenue from Contracts with Customers (Topic 606) (“ASU 2014-09”) in May 2014. ASU 2014-09 requires entities to recognize revenue through the application of a five-step model, which includes identification of the contract, identification of the performance obligations, determination of the transaction price, allocation of the transaction price to the performance obligations and recognition of revenue as the entity satisfies the performance obligations. |
| · | ASU No. 2016-08, Revenue from Contracts with Customers (Topic 606): Principal versus Agent Considerations (Reporting Revenue Gross versus Net) (“ASU 2016-08”) in March 2016. ASU 2016-08 does not change the core principle of revenue recognition in Topic 606 but clarifies the implementation guidance on principal versus agent considerations. |
| · | ASU No. 2016-10, Revenue from Contracts with Customers (Topic 606): Identifying Performance Obligations and Licensing (“ASU 2016-10”) in April 2016. ASU 2016-10 does not change the core principle of revenue recognition in Topic 606 but clarifies the implementation guidance on identifying performance obligations and the licensing implementation guidance, while retaining the related principles for those areas. |
| · | ASU No. 2016-11, Revenue Recognition (Topic 605) and Derivatives and Hedging (Topic 815): Rescission of SEC Guidance Because of Accounting Standards Updates 2014-09 and 2014-16 Pursuant to Staff Announcements at the March 3, 2016 EITF Meeting (SEC Update) (“ASU 2016-11”) in May 2016. ASU 2016-11 rescinds SEC paragraphs pursuant to two SEC Staff Announcements at the March 3, 2016 EITF meeting. The SEC Staff is rescinding SEC Staff Observer comments that are codified in Topic 605 and Topic 932, effective upon adoption of Topic 606. |
| · | ASU No. 2016-12, Revenue from Contracts with Customers (Topic 606): Narrow-Scope Improvements and Practical Expedients in May 2016. ASU 2016-12 does not change the core principle of revenue recognition in Topic 606 but clarifies the implementation guidance on a few narrow areas and adds some practical expedients to the guidance. |
| · | ASU No. 2016-20, Revenue from Contracts with Customers (Topic 606): Technical Corrections and Improvements (“ASU 2016-20”) in December 2016. ASU 2016-20 does not change the core principle of revenue recognition in Topic 606 but summarizes the technical corrections and improvements to ASU 2014-09 and is effective upon adoption of Topic 606. |
These ASUs will become effective for the Company beginning interim period April 1, 2018. The Company currently anticipates adopting the standard using the modified retrospective method. The Company has begun the process of implementing this standard, including performing a review of its revenue streams to identify any differences in the timing, measurement, or presentation of revenue recognition. The Company currently believes that the primary impact will be changes to the timing of recognition of revenues related to fee-for-service and enhanced financial statement disclosures. The Company will continue to assess the impact on all areas of its revenue recognition, disclosure requirements and changes that may be necessary to its internal controls over financial reporting.
In August 2016, the FASB issued ASU No. 2016-15, Statement of Cash Flows (Topic 230) – Classification of Certain Cash Receipts and Cash Payments (“ASU 2016-15”). This ASU provides clarification regarding how certain cash receipts and cash payments are presented and classified in the statement of cash flows. This ASU addresses eight specific cash flow issues with the objective of reducing the existing diversity in practice. The issues addressed in this ASU that will affect the Company are classifying debt prepayments or debt extinguishment costs and contingent consideration payments made after a business combination. This update is effective for annual and interim periods beginning after December 15, 2017, and interim periods within that reporting period. Early adoption is permitted. The Company is currently assessing the impact the adoption of ASU 2016-15 will have on the Company’s consolidated financial statements.
F-201
In December 2016, the FASB issued ASU No. 2016-18, Statement of Cash Flows (Topic 230) (“ASU 2016-18”). The amendments in ASU 2016-18 require that a statement of cash flows explain the change during the period in the total of cash, cash equivalents, and amounts generally described as restricted cash or restricted cash equivalents. ASU 2016-17 will become effective for the Company beginning interim period April 1, 2018. Early adoption is permitted, including adoption in an interim period. The Company is currently assessing the impact the adoption of ASU 2016-18 will have on the Company’s consolidated financial statements.
In January 2017, the FASB issued ASU No. 2017-01, Business Combinations (Topic 805): Clarifying the Definition of a Business (“ASU 2017-01”). This ASU provides a screen to determine when an asset is not a business, which requires that when substantially all of the fair value of the gross assets acquired (or disposed of) is concentrated in a single identifiable asset or a group of similar identifiable assets, the set is not a business, which reduces the number of transactions that need to be further evaluated. If the screen is not met, this ASU require that to be considered a business, a set much include, at a minimum, an input and a substantive process that together significantly contribute to the ability to create output and also remove the evaluation of whether a market participant could replace missing elements. This update is effective for annual and interim periods beginning after December 15, 2017, including interim periods within those periods. The Company is currently assessing the impact the adoption of ASU 2017-01 will have on the Company’s consolidated financial statements.
In January 2017, the FASB issued ASU No. 2017-04, Intangibles – Goodwill and Other (Topic 350): Simplifying the Test for Goodwill Impairment (“ASU 2017-04”). This ASU eliminates Step 2 from the goodwill impairment test if the carrying amount exceeds the fair value of a reporting unit and also eliminated the requirements for any reporting unit with a zero or negative carrying amount to perform a qualitative assessment and, if it fails that qualitative test, to perform Step 2 of the goodwill impairment test. Therefore, the same impairment assessment applies to all reporting units. An entity is required to disclose the amount of goodwill allocated to each reporting unit with a zero or negative carrying amount of net assets. This update is effective for annual and interim periods beginning after December 15, 2019. Early adoption is permitted for interim or annual goodwill impairment tests performed on testing dates after January 1, 2017. The Company is currently assessing the impact the adoption of ASU 2017-04 will have on the Company’s consolidated financial statements.
In May 2017, the FASB issued ASU No. 2017-09, Compensation – Stock Compensation (Topic 718): Scope of Modification Accounting (“ASU 2017-09”). This ASU provide guidance about which changes to the terms or conditions of a share-based payment award require an entity to apply modification accounting in Topic 718. This update is effective for all entities for annual periods, and interim periods within those annual periods, beginning after December 15, 2017. Early adoption is permitted, including adoption in any interim period, for public business entities for reporting periods for which financial statements have not yet been issued. The amendments in this update should be applied prospectively to an award modified on or after the adoption date, The Company is currently assessing the impact the adoption of ASU 2017-09 will have on the Company’s consolidated financial statements.
In July 2017, the FASB issued ASU No. 2017-11, Earnings Per Share (Topic 260); Distinguishing Liabilities from Equity (Topic 480); Derivatives and Hedging (Topic 815): (Part 1) Accounting for Certain Financial Instruments with Down Round Features, (Part II) Replacement of the Indefinite Deferral for Mandatorily Redeemable Financial Instruments of Certain Nonpublic Entities and Certain Mandatorily Redeemable Non-controlling Interests with a Scope Exception (“ASU 2017-11”). The amendments in Part I of this Update change the classification analysis of certain equity-linked financial instruments (or embedded features) with down round features. When determining whether certain financial instruments should be classified as liabilities or equity instruments, a down round feature no longer precludes equity classification when assessing whether the instrument is indexed to an entity’s own stock. The amendments also clarify existing disclosure requirements for equity-classified instruments. The amendments in Part 1 of this update are effective for fiscal years, and interim periods within those fiscal years, beginning after December 15, 2018. Early adoption is permitted, including adoption in any interim period. If an entity early adopts the amendments in an interim period, any adjustments should be reflected as of the beginning of the fiscal year that includes that interim period. The Company is currently assessing the impact the adoption of ASU 2017-11 will have on the Company’s consolidated financial statements.
Use of Estimates
The preparation of financial statements in conformity with U.S. GAAP requires the Company to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenues and expenses during the reporting period. Actual results may materially differ from these estimates under different assumptions or conditions.
| 3. | Goodwill and Intangible Assets |
Goodwill
There was no change in Goodwill as of June 30, 2017 and March 31, 2017.
F-202
Intangible Assets, Net
Intangible assets, net consisted of the following:
| Weighted | Gross | Net | ||||||||||||||
| Average | June 30, | Accumulated | June 30, | |||||||||||||
| Life (Yrs.) | 2017 | Amortization | 2017 | |||||||||||||
| Indefinite Lived Assets: | ||||||||||||||||
| Medicare License | N/A | $ | 704,000 | $ | - | $ | 704,000 | |||||||||
| Amortized Intangible Assets: | ||||||||||||||||
| Acquired Technology | 5 | 1,312,500 | (328,125 | ) | 984,375 | |||||||||||
| Network Relationships | 5 | 220,000 | (128,333 | ) | 91,667 | |||||||||||
| Trade Name | 5 | 102,000 | (59,500 | ) | 42,500 | |||||||||||
| $ | 2,338,500 | $ | (515,958 | ) | $ | 1,822,542 | ||||||||||
| Weighted | Gross | Net | ||||||||||||||
| Average | March 31, | Accumulated | March 31, | |||||||||||||
| Life (Yrs.) | 2017 | Amortization | 2017 | |||||||||||||
| Indefinite Lived Assets: | ||||||||||||||||
| Medicare License | N/A | $ | 704,000 | $ | - | $ | 704,000 | |||||||||
| Amortized Intangible Assets: | ||||||||||||||||
| Acquired Technology | 5 | 1,312,500 | (262,500 | ) | 1,050,000 | |||||||||||
| Non-Compete | 4 | 94,672 | (94,672 | ) | - | |||||||||||
| Network Relationships | 5 | 220,000 | (117,331 | ) | 102,669 | |||||||||||
| Trade Name | 5 | 145,017 | (97,417 | ) | 47,600 | |||||||||||
| $ | 2,476,189 | $ | (571,920 | ) | $ | 1,904,269 | ||||||||||
There were no additions to the intangible assets in the three months ended June 30, 2017. The amortization expense for the three months ended June 30, 2017 and 2016 was approximately $82,000 and $95,000, respectively.
The following table summarizes the approximate expected future amortization expense as of June 30, 2017 of definite-lived intangible assets for each for the four fiscal years ending March 31 thereafter:
| 2018 (remaining 9 months) | $ | 245,000 | ||
| 2019 | 327,000 | |||
| 2020 | 284,000 | |||
| 2021 | 262,542 | |||
| $ | 1,118,542 |
| 4. | Accounts Payable and Accrued Liabilities |
Accounts payable and accrued liabilities consisted of the following:
| June 30, | March 31, | |||||||
| 2017 | 2017 | |||||||
| Accounts payable | $ | 2,786,643 | $ | 3,569,011 | ||||
| Advance capitation payment to APAACO from CMS | 9,292,564 | - | ||||||
| Accrued compensation | 3,297,093 | 2,860,340 | ||||||
| Income taxes payable | 333 | 20,827 | ||||||
| Accrued interest | 192,895 | 54,158 | ||||||
| Accrued professional fees | 643,455 | 1,379,037 | ||||||
| $ | 16,212,983 | $ | 7,883,373 | |||||
Total accounts payable and accrued liabilities for the six months ended June 30, 2017 increased approximately $8.3 million, or 105.7%, as compared to the same period of 2016, due to the new APAACO NGACO contract with CMS.
F-203
| 5. | Income Taxes |
The Company uses the liability method of accounting for income taxes as set forth in ASC 740. Under the liability method, deferred taxes are determined based on differences between the financial statement and tax bases of assets and liabilities using enacted tax rates.
On an interim basis, the Company estimates what its anticipated annual effective tax rate will be and records a quarterly income tax provision (benefit) in accordance with the estimated annual rate, plus the tax effect of certain discrete items that arise during the quarter. As the fiscal year progresses, the Company refines its estimates based on actual events and financial results during the quarter. This process can result in significant changes to the Company’s estimated effective tax rate. When this occurs, the income tax provision (benefit) is adjusted during the quarter in which the estimates are refined so that the year-to-date provision reflects the estimated annual effective tax rate. These changes, along with adjustments to the Company’s deferred taxes and related valuation allowance, may create fluctuations in the overall effective tax rate from quarter to quarter.
Due to overall cumulative losses incurred in recent years, the Company maintained a full valuation allowance against its deferred tax assets as of June 30, 2017 and March 31, 2017.
The Company’s effective tax rate for the three months ended June 30, 2017 differed from the U.S. federal statutory rate primarily due to operating losses that receive no tax benefit as a result of a valuation allowance recorded for such losses and the exclusion of loss entities from the Company’s overall estimated annual effective rate calculation under guidance from ASC 740-270-30-26a.
As of June 30, 2017 and March 31, 2017, the Company does not have any unrecognized tax benefits related to various federal and state income tax matters. The Company will recognize accrued interest and penalties related to unrecognized tax benefits in income tax expense.
The Company is subject to U.S. federal income tax as well as income tax of multiple state tax jurisdictions. The Company and its subsidiaries’ state income tax returns are open to audit under the statute of limitations for the years ended January 31, 2013 onwards. The Company does not anticipate material unrecognized tax benefits within the next 12 months.
| 6. | Stockholders’ Equity |
Series A Preferred Stock
On October 14, 2015, the Company entered into a Securities Purchase Agreement (the “2015 SPA”) with NMM pursuant to which the Company sold to NMM, and NMM purchased from the Company, in a private offering of securities, 1,111,111 units, each unit consisting of one share of the Company’s Series A Preferred Stock and a stock purchase warrant (the “Series A Warrant”) to purchase one share of the Company’s common stock (“Common Stock”) at an exercise price of $9.00 per share. The Series A Preferred Stock has a liquidation preference in the amount of $9.00 per share plus any declared and unpaid dividends. The Series A Preferred Stock can be voted for the number of shares of Common Stock into which the Series A Preferred Stock could then be converted, which initially is one-for-one. The Series A Preferred Stock is convertible into Common Stock, at the option of NMM, at any time after issuance at an initial conversion rate of one-for-one, subject to adjustment in the event of stock dividends, stock splits and certain other similar transactions. The Series A Preferred Stock is mandatorily convertible not sooner than the earlier to occur of (i) the later of (x) January 31, 2017 or (y) 60 days after the date on which the Company files its quarterly report on Form 10-Q for the period ending September 30, 2016, or (ii) the date on which the Company receives the written, irrevocable decision of NMM not to require a redemption of the Series A Preferred Stock, if the Company receive aggregate gross proceeds of not less than $5,000,000 in one or more transactions for the sale of the Company’s equity or convertible securities (other than transactions with NMM). The Company has not received at least $5,000,000 in one or more transactions for the sale of its equity or convertible securities to parties other than NMM. The Series A Warrant may be exercised at any time after issuance and through October 14, 2020, for $9.00 per share, subject to adjustment in the event of stock dividends and stock splits. The Series A Warrant is not separately transferable from the Series A Preferred Stock. See Note 2 for information on the fair value of the Series A Warrant. The units sold to NMM under the 2015 SPA initially had a redemption feature, however, as part of the proposed Merger between NMM and the Company (see Note 10), NMM entered into a Consent and Waiver Agreement dated December 21, 2016 (the “NMM Waiver”), pursuant to which NMM has relinquished its right of redemption with respect to its shares of Series A Preferred Stock and Series A Warrants.
Series B Preferred Stock
On March 30, 2016, the Company entered into an additional Securities Purchase Agreement (the “2016 SPA”) with NMM pursuant to which the Company sold to NMM, and NMM purchased from the Company, in a private offering of securities, 555,555 units, each unit consisting of one share of the Company’s Series B Preferred Stock and a stock purchase warrant (the “Series B Warrant”) to purchase one share of Common Stock at an exercise price of $10.00 per share. NMM paid the Company an aggregate $4,999,995 for the units. The Series B Preferred Stock has a liquidation preference in the amount of $9.00 per share plus any declared and unpaid dividends. The Series B can be voted for the number of shares of Common Stock into which the Series B Preferred Stock could then be converted, which initially is one-for-one. The Series B Preferred Stock is convertible into Common Stock, (i) at the option of NMM or (ii) mandatorily at any time prior to and including March 30, 2021, if the Company receives aggregate gross proceeds of not less than $5,000,000 in one or more transactions for the sale of the Company’s equity or convertible securities (other than transactions with NMM), at an initial conversion rate of one-for-one, subject to adjustment in the event of stock dividends, stock splits and certain other similar transactions. The Company has not received at least $5,000,000 in one or more transactions for the sale of its equity or convertible securities to parties other than NMM. The Series B Warrant may be exercised at any time after issuance and through March 30, 2021, for $10.00 per share, subject to adjustment in the event of stock dividends and stock splits. The Series B Warrant is not separately transferable from the Series B Preferred Stock. See Note 2 for information on the fair value of the Series B Warrant.
F-204
Common Stock Issuance
During the three months ended June 30, 2017, the Company did not issue shares of Common Stock. The number of shares of Common Stock that are issued and outstanding as June 30, 2017 is 6,033,518.
Equity Incentive Plans
On December 15, 2015, the Company’s Board of Directors (the “Board”) approved the Company’s 2015 Equity Incentive Plan (the “2015 Plan”), pursuant to which 1,500,000 shares of Common Stock were reserved for issuance thereunder. In addition, shares that are subject to outstanding grants under the Company’s 2010 Equity Incentive Plan and 2013 Equity Incentive Plan but that ordinarily would have been restored to such plans reserve due to award forfeitures and terminations will roll into and become available for awards under the 2015 Plan. The 2015 Plan provides for awards, including incentive stock options, non-qualified options, restricted common stock, and stock appreciation rights. The 2015 Plan was approved by the Company’s stockholders at the 2016 Annual Meeting of Stockholders that was held on September 14, 2016. As of June 30, 2017, there were approximately 942,000 shares available for future grants under the 2015 Plan. As of June 30, 2017, there were no shares available for future grants under the 2010 and 2013 Equity Incentive Plans.
Options
On April 6, 2017, the Company granted stock options to employees and a director to purchase up to 80,000 shares of Common Stock. Two of the options expire on the 5th anniversary date from date of grant and have an exercise price of $10.18 per share. The remaining options expire on the 10th anniversary date from date of grant and have an exercise price of $9.25 per share. The fair value of the stock option of $572,000 was computed using the Black-Scholes option pricing model, using the following assumptions: expected term – 3-6 years; stock price $9.25 per share; volatility – 109.95% - 134.83%; risk-free interest rate – 1.53% - 2.09%; and zero annual rate of quarterly dividend. All of these stock options vest over a period of 24 months from date of grant.
Stock option activity for the three months ended June 30, 2017 is summarized below:
| Shares | Weighted Average Per Share Exercise Price |
Weighted Average Remaining Life (Years) |
Weighted Average Per Share Intrinsic Value |
|||||||||||||
| Balance, March 31, 2017 | 1,165,350 | $ | 4.24 | 6.64 | $ | 4.86 | ||||||||||
| Granted | 80,000 | 9.71 | - | - | ||||||||||||
| Exercised | - | - | - | - | ||||||||||||
| Cancelled/expired | (32,222 | ) | 9.71 | - | - | |||||||||||
| Balance, June 30, 2017 | 1,213,128 | $ | 4.42 | 6.61 | $ | 5.57 | ||||||||||
| Vested, June 30, 2017 | 1,041,257 | $ | 4.04 | 6.18 | $ | 5.96 | ||||||||||
As of June 30, 2017, total unrecognized compensation costs related to non-vested stock-based compensation arrangements granted under the Company’s three Equity Incentive Plans was approximately $791,000 and the weighted-average period of years expected to recognize those costs was 1.71 years, which included stock options granted to our executive officers in April 2017 that have subsequently been deemed void and are currently planned to be cancelled without payment by the Company. None of such stock options have been exercised.
Stock-based compensation expense related to common stock option awards is recognized over their respective vesting periods and was included in the accompanying condensed consolidated statement of operations as follows:
| Three Months Ended June 30, |
||||||||
| 2017 | 2016 | |||||||
| Stock-based compensation expense: | ||||||||
| Cost of services | $ | - | $ | 1,227 | ||||
| General and administrative | 223,566 | 246,490 | ||||||
| $ | 223,566 | $ | 247,717 | |||||
F-205
Warrants
Warrants consisted of the following for the three months ended June 30, 2017:
| Weighted Average Per Share |
||||||||
| Intrinsic | Number of | |||||||
| Value | Warrants | |||||||
| Outstanding at March 31, 2017 | $ | 4.68 | 1,970,166 | |||||
| Granted | - | - | ||||||
| Exercised | - | - | ||||||
| Cancelled | - | - | ||||||
| Outstanding at June 30, 2017 | $ | 6.41 | 1,970,166 | |||||
| Weighted | Weighted | |||||||||||||||||
| Average | Average | |||||||||||||||||
| Exercise Price Per | Warrants | Remaining | Warrants | Exercise Price Per | ||||||||||||||
| Share | Outstanding | Contractual Life | Exercisable | Share | ||||||||||||||
| $4.00-$5.00 | 188,500 | 0.60 | 188,500 | 4.47 | ||||||||||||||
| $9.00-$10.00 | 1,781,666 | 3.30 | 1,781,666 | 9.37 | ||||||||||||||
| $4.00-$10.00 | 1,970,166 | 3.03 | 1,970,166 | $ | 8.90 | |||||||||||||
Authorized Stock
At June 30, 2017, the Company was authorized to issue up to 100,000,000 shares of Common Stock and 5,000,000 shares of its preferred stock.
The number of shares of Series A Preferred Stock and Series B Preferred Stock that are issued and outstanding as June 30, 2017 is 1,111,111 and 555,555, respectively. The number of shares of Common Stock that are issued and outstanding as June 30, 2017 is 6,033,518.
The Company is required to reserve and keep available out of the authorized but unissued shares of Common Stock such number of shares sufficient to affect the conversion of all outstanding preferred stock, the exercise of all outstanding warrants exercisable into shares of Common Stock, the conversion of all outstanding notes and accrued interest into shares of Common Stock, and shares granted and available for grant as stock options under the Company’s Equity Incentive Plans. The number of shares of Common Stock reserved for these purposes is as follows at June 30, 2017:
| For warrants outstanding | 1,970,166 | |||
| For stock options outstanding | 1,213,128 | |||
| For debt outstanding and accrued interest | 506,547 | |||
| For preferred stock issued and outstanding | 1,666,666 | |||
| Total | 5,356,507 |
F-206
| 7. | Debt |
Standby Letters of Credit and Lines of Credit
In January 2013, City National Bank (“CNB”) provided to MMG an irrevocable standby letter of credit for $10,000, which was increased to $500,000 in November, 2014. Such letter of credit renews automatically every 5 months. In December 2016, CNB provided to MMG another irrevocable standby letter of credit for $235,000, which expires December 31, 2017. In March, 2017, APAACO established an irrevocable standby letter of credit with a financial institution for $6,699,329 for the benefit of CMS, which expires on December 31, 2018 and will be automatically extended without amendment for additional one-year periods, unless terminated by the institution prior to 90 days from the expiration date. The standby letters of credit are typically collateralized by cash deposits, which are included in restricted cash in the amount of $745,117 and $765,058 on the consolidated balance sheets at June 30, 2017 and March 31, 2017, respectively.
BAHA has a line of credit of $150,000 with First Republic Bank. Borrowings thereunder bear interest at the prime rate (as defined) plus 3.0% (7.25% and 7.0% per annum at June 30, 2017 and March 31, 2017, respectively). The Company has an outstanding balance of $25,000 and $62,500 as of June 30, 2017 and March 31, 2017, respectively. The line of credit is unsecured.
Interest expense associated with the lines of credit amounted to the following:
|
Three Months Ended June 30, |
||||||||
| 2017 | 2016 | |||||||
| Interest expense for lines of credit | $ | 584 | $ | 2,659 | ||||
Notes Payable
NMM Note (Related Party)
In connection with the proposed Merger, on January 3, 2017, the Company issued a promissory note to NMM in the amount of $5,000,000. Interest is due quarterly at the rate of prime plus 1% (or 5.25% at June 30, 2017, with the entire principal balance being due on January 3, 2019. In the event of default, as defined, all unpaid principal and interest will become due and payable.
The NMM Note has a term of two years, with its payment obligations commencing on February 1, 2017 and continuing on a quarterly basis thereafter until January 2019 (the “NMM Note Maturity Date”). Under the terms of the NMM Note, the Company must pay NMM interest on the principal balance outstanding at the prime rate (as such term is defined in the NMM Note) plus 1%. All outstanding principal and accrued but unpaid interest under the NMM Note is due and payable in full on the NMM Note Maturity Date. The Company may voluntarily prepay the outstanding principal and interest in whole or in part without penalty or premium. Upon the occurrence of an event of default (as such term is defined in the NMM Note), the unpaid principal amount of, and all accrued but unpaid interest on, the NMM Note will become due and payable immediately at the option of NMM. In such event, NMM may, at its option, declare the entire unpaid balance of the NMM Note, together with all accrued interest, applicable fees, and costs and charges, including costs of collection, if any, to be immediately due and payable in cash.
Interest expense associated with the outstanding notes payable amounted to $139,322 for the three months ended June 30, 2017. There was no interest on these notes for the three months ended June 30, 2016.
Convertible Notes Payable
Alliance Convertible Note
On March 30, 3017, the Company issued a 6% convertible promissory note to Alliance Apex, LLC (the “Alliance Note”) for $4,990,000. The Alliance Note is due and payable to Alliance on (i) December 31, 2017, or (ii) the date on which the Merger Agreement with NMM is terminated (see Note 1 above), whichever occurs first. Upon the closing of the proposed Merger on or before December 31, 2017, the Alliance Note together with the accrued and unpaid interest, shall automatically be converted into 499,000 shares of Common Stock, at a conversion price of $10.00 per share, subject to adjustment for stock splits, stock dividends, reclassifications and other similar recapitalization transactions that occur after the date of the Alliance Note. If the Merger is not consummated by December 31, 2017, the Company will be obligated to repay the outstanding principal, together with accrued and unpaid interest, on the Alliance Note within 45 days, which would require a significant amount of cash on hand or the need to raise capital to pay off or refinance the Alliance Note. There can be no assurance that is such event arose, the Company would have sufficient cash on hand to repay the Alliance Note or could raise capital on favorable terms, or at all, to repay the Alliance Note.
In the case of an event of default (as defined in the Alliance Note), the entire outstanding principal and all accrued and unpaid interest under the Alliance Note shall automatically become immediately due and payable, without presentment, demand, protest or notice of any kind. If any other event of default occurs and is continuing, Alliance, by written notice to the Company, may declare the outstanding principal and interest under the Alliance Note to be immediately due and payable. After maturity (by acceleration or otherwise), the unpaid balance (both as to principal and unpaid pre-maturity interest) shall bear interest at a default rate equal to the lesser of (a) 3% over the rate of interest in effect immediately prior to maturity or (ii) the then maximum legal rate allowed under the laws of the State of California. Additionally, the Company shall pay all costs of collection incurred by Alliance, including reasonable attorney’s fees incurred in connection with the Alliance’s reasonable collection efforts.
F-207
As part of the Merger Agreement Amendment (see Note 1 above), NMM provided a guarantee for the Alliance Note which was considered a debt issuance cost. The Company estimated the debt issuance cost and related warrants issuable for the debt guarantee of $161,000 based on the incremental fair value to a market participant of a similar but unsecured debt instrument without such guarantee using a market rate for an unsecured high yield note of 12.4% and a 25% probability of the note not being converted. As of June 30, 2017 and March 31, 2017, the debt issuance cost associated with the guarantee was $107,333 and $161,000, respectively, and after being offset against the Alliance Note, resulted in a net balance of $4,882,667 and $4,829,000, respectively.
| 8. | Commitments and Contingencies |
Standby Letters of Credit, Lines of Credit and Outstanding Notes
See Note 7 - Standby Letters of Credit and Lines of Credit above.
Lease Commitments
The Company’s lease for its current corporate headquarters, as amended, sets base rent at $37,913 per month for the first year and schedules annual increases in base rent each year until the final rental year, which is capped at $43,957 per month. The base rent may be abated by up to $228,049 subject to other terms of the lease. At June, 2017, deferred rent liability associated with such leases was $680,486.
Employment Agreements
In December 2016, AMM entered into employment agreements with Warren Hosseinion, M.D., Adrian Vazquez, M.D., Gary Augusta and Mihir Shah, which replaced such officers’ previous employment agreements and revised certain term, bonus and severance arrangements. Such agreements, as amended as of the date of this Report, provide annual base salaries in the aggregate amount of $1,550,000 for such officers. Each of the new employment agreements has an initial term of three years with automatic annual renewals and provide 20 business days of paid time off per calendar year. Accrued and unused paid time off shall be paid in cash at the end of each calendar year. Under the new employment agreements, each officer is eligible to receive an annual bonus and is granted certain vesting rights and accrued benefits (as such term is defined therein) if his employment is terminated without “cause” (as such term is defined therein) or if he resigns with “good reason” (as such term is defined therein) during the employment term.
Regulatory Matters
The healthcare industry and Medicare and Medicaid programs are subject to numerous laws and regulations of federal, state and local governments, including the Health Insurance Portability and Accountability Act, the Health Information Technology for Economic and Clinical Health Act and the Patient Protection and Affordable Care Act, which are generally are complex and subject to interpretation. These laws and regulations govern matters such as licensure, accreditation, security and privacy of health information, health insurance portability, health insurance exchanges, government healthcare program participation requirements, reimbursement for patient services, and Medicare and Medicaid fraud and abuse. Government activity has continued with respect to investigations and allegations concerning possible violations of such laws and regulations by healthcare providers. Compliance with such laws and regulations can be subject to government review and interpretation. Violations of these laws and regulations may result in significant adverse regulatory actions, including fines, penalties, exclusion from government healthcare programs, repayments for patient services previously billed as well as those unknown or unasserted at this time.
As a risk-bearing organization (“RBO”), the Company is required to follow regulations of the California Department of Managed Health Care (“DMHC”). The Company and its applicable affiliates must comply with a minimum working capital requirement, Tangible Net Equity (“TNE”) requirement, cash-to-claims ratio and claims payment requirements prescribed by the DMHC. TNE is defined as net assets less intangibles, less non-allowable assets (which include amounts due from affiliates), plus subordinated obligations. The DMHC determined that, as of February 28, 2016, MMG, was not in compliance with the DMHC’s positive TNE requirement for a RBO. As a result, the DMHC required MMG to develop and implement a corrective action plan (“CAP”) for such deficiency. MMG’s CAP has been submitted and was approved by DMHC in December 2016. Through an intercompany revolving subordinate loan from AMM, MMG achieved positive TNE in the third quarter of fiscal 2017 and has maintained positive TNE to date. The DMHC is in the process of reviewing the Company’s filings for MMG to be taken off the CAP.
Legal Actions and Proceedings
In the ordinary course of the Company’s business, the Company from time to time becomes involved in pending and threatened legal actions and proceedings, most of which involve claims of medical malpractice related to medical services provided by the Company’s affiliated hospitalists. The Company may also become subject to other lawsuits which could involve significant claims and/or significant defense costs. Many of the Company’s payer and provider contracts are complex in nature and may be subject to differing interpretations regarding amounts due for the provision of medical services, which may not come to light until a substantial period of time has passed following contract implementation. Liabilities for claims are recorded when the loss is probable and can be estimated. Any adjustments to reserves are reflected in current operations.
F-208
Liability Insurance
Although the Company currently maintains liability insurance policies on a claims-made basis, which are mainly intended to cover malpractice liability and certain other claims, the coverage must be renewed annually, and may not continue to be available to the Company in future years at acceptable costs, and on favorable terms. In addition, the Company cannot be certain that the Company’s current insurance coverage will be adequate to cover liabilities arising out of claims asserted against the Company, the Company’s affiliated professional organizations or the Company’s affiliated hospitalists in the future where the outcomes of such claims are unfavorable. Liabilities in excess of the Company’s insurance coverage may have a material adverse effect on the Company’s business, financial position, results of operations and cash flows.
| 9. | Related Party Transactions |
Dr. Thomas Lam, one of the Company’s directors is a significant shareholder and the Chief Executive Officer of NMM. See Note 1 for information on the proposed Merger and NMM’s investments in and loan to the Company.
Mark Fawcett, one of the Company’s directors, was nominated by NNA as its representative on the Board. See Note 10 for information in relation to NNA’s registration rights granted by the Company.
In September 2015, the Company entered into a note receivable with Rob Mikitarian, a minority owner in APS, in the amount of approximately $150,000. The note accrues interest at 3% per annum and is due on or before September 2017. At both June 30, 2017 and March 31, 2017, the balance of the note was approximately $150,000 and is included in other receivables in the accompanying consolidated balance sheets.
In September 2015, the Company entered into a note receivable with Liviu Chindris, M.D., a minority owner in APS, in the amount of approximately $105,000. The note accrues interest at 3% per annum and is due on or before September 2017. At June 30, 2017 the balance of the note has been paid and at March 31, 2017, the balance of the note was approximately $105,000 and is included in other receivables in the accompanying consolidated balance sheets. In November, 2016, in connection with a promissory note issued to Dr. Chindris, which the Company has repaid in full, the Company issued Dr. Chindris a warrant to purchase up to 5,000 shares of Common Stock at an exercise price of $9.00 per share (see Note 2).
In December 2016 and June 30, 2017, the Company billed NMM $930,169 and $438,307, respectively, for its 50% share of the costs related to APAACO’s participation in the NGACO Model that the Company had incurred on behalf of APAACO.
In the ordinary course of the Company’s business, the Company from time to time grants options to its employees under its Equity Incentive Plans and enters into employment agreements with its employees, including officers,. See Note 6 and Note 8 above for addition information.
In addition, affiliates wholly-owned by the Company’s officers, including Dr. Hosseinion, are reported in the accompanying condensed consolidated statement of operations on a consolidated basis, together with the Company’s subsidiaries, and therefore, the Company does not separately disclose transactions between such affiliates and the Company’s subsidiaries as related party transactions.
| 10. | Subsequent Events |
On July 1, 2017, APAACO and Universal Care, Inc. dba Brand New Day (“BND”), which is 50% owned by Allied Pacific of California (an IPA and a variable interest entity of NMM), entered into an agreement (the “Care Management Agreement”), pursuant to which BND will provide care management programs for patients with certain chronic diseases. APAACO will pay BND $50.00 per month per patient but may adjust fees upward or downward upon giving BND 60 working days’ prior notice. The initial term of the Care Management Agreement is one year. Thereafter, the Care Management Agreement will renew automatically for successive one-year periods unless either party gives the other party notice of termination. The Care Management Agreement shall terminate automatically upon the revocation, suspension or restriction of any license, certificates or other authority required to be maintained by BND. Additionally, either party may terminate the Care Management Agreement for cause (as defined therein) by giving 45 days’ prior notice or without cause by giving 90 days’ prior notice.
On July 7, 2017, the waiting period under the Hart-Scott-Rodino Antitrust Improvements Act of 1976, as amended (“HSR”), with respect to the proposed Merger expired. While the expiration of the HSR waiting period satisfies a condition to the closing of Merger, consummation of the Merger remains subject to other conditions described in the Merger Agreement, including approval by ApolloMed stockholders and the shareholders of NMM.
On July 26, 2017, the Company entered into a Fifth Amendment to the Registration Rights Agreement, dated as of March 28, 2014, with NNA. The amendment extended the deadline for the Company to file a resale registration statement covering NNA’s registrable securities to March 31, 2018 and removed prohibitions on the Company’s ability to file other registration statements. Previously in April 2017, the Company and NNA agreed to extend the date by which the Company is required to use commercially reasonable best efforts to cause such registration statement to be declared effective to June 30, 2018 (or, if earlier, the 5th trading day after the date on which the SEC notifies the Company that such registration statement will not be “reviewed” or subject to further review).
On August 10, 2017, NMM and ApolloMed filed a registration statement on form S-4 with the Securities and Exchange Commission (the “SEC”) in connection with the proposed Merger.
F-209
EXECUTION
AGREEMENT AND PLAN OF MERGER
by and among
APOLLO MEDICAL HOLDINGS, INC.,
APOLLO ACQUISITION CORP.,
NETWORK MEDICAL MANAGEMENT, INC.,
and
THE SHAREHOLDERS’ REPRESENTATIVE NAMED HEREIN
Dated as of December 21, 2016
-i-
Table of Contents
(continued)
-ii-
Table of Contents
(continued)
-iii-
Table of Contents
(continued)
| Page | ||
| ARTICLE X DISPUTE RESOLUTION | 77 | |
| 10.1 | Executive Administration | 77 |
| 10.2 | Judicial Reference | 77 |
| 10.3 | Equitable Relief and Enforcement | 78 |
| ARTICLE XI SHAREHOLDERS’ REPRESENTATIVE | 79 | |
| 11.1 | Appointment of Shareholders’ Representative | 79 |
| 11.2 | Successor Shareholders’ Representative | 79 |
| 11.3 | Power and Authority | 79 |
| 11.4 | Limitation on Liability; Indemnification | 80 |
| 11.5 | Reliance | 80 |
| ARTICLE XII GENERAL PROVISIONS | 80 | |
| 12.1 | Notices | 80 |
| 12.2 | Assignment | 81 |
| 12.3 | No Third-Party Beneficiaries | 81 |
| 12.4 | Execution of Agreement; Counterparts; Electronic Signature | 82 |
| 12.5 | Governing Law; Exclusive Jurisdiction | 82 |
| 12.6 | Entire Agreement; Modification | 82 |
| 12.7 | Conflict Between Transaction Documents | 82 |
| 12.8 | Construction/Severability | 82 |
| 12.9 | Extension; Waiver | 82 |
| 12.10 | Ambiguities | 83 |
| 12.11 | Interpretation | 83 |
| 12.12 | Expenses | 84 |
| 12.13 | References to U.S. Dollars | 84 |
| 12.14 | Specific Performance | 84 |
| ARTICLE XIII DEFINITIONS | 85 | |
| 13.1 | Definitions | 85 |
-iv-
EXHIBITS
| Exhibit A | Form of Voting Agreement |
| Exhibit B | Form of Shareholder Lock-Up Agreement |
| Exhibit C | Form of Exchange Agent Agreement |
| Exhibit D | Consent and Waiver Agreement |
| Exhibit E | Form of Letter of Transmittal |
| Exhibit F | Working Capital Note |
| Exhibit G | Shareholder Representations |
| Exhibit H-1 | Certificate of Amendment |
| Exhibit H-2 | Amendment to Bylaws |
-i-
AGREEMENT AND PLAN OF MERGER
This Agreement and Plan of Merger (this “Agreement”) is made and entered into as of this 21st day of December, 2016 (the “Execution Date”), by and among Apollo Medical Holdings, Inc., a Delaware corporation (“Parent”), Apollo Acquisition Corp., a California corporation (“Merger Sub”), Network Medical Management, Inc., a California corporation (the “Company”), and Kenneth Sim, M.D. (the “Shareholders’ Representative”). Parent, Merger Sub, the Company, and the Shareholders’ Representative shall sometimes be referred to herein collectively as the “Parties” and individually as a “Party.” The Shareholders’ Representative, acting in such capacity, is a Party to this Agreement solely in his capacity as the Shareholders’ Representative and solely for the purpose of the specific provisions of this Agreement relating to the Shareholders’ Representative. Capitalized terms used herein have the meanings ascribed to them in Article XIII below.
RECITALS
WHEREAS, the board of directors of the Company (the “Company Board”), the board of directors of Parent and the board of directors of Merger Sub have adopted this Agreement and have determined that it is in the best interests of their respective companies and shareholders to consummate the strategic business combination provided for in this Agreement in which Merger Sub will merge with and into the Company, with the Company surviving such merger (collectively, the “Merger”) and continuing as a wholly-owned subsidiary of Parent in accordance with the California General Corporation Law (the “CGCL”) on the terms and subject to the conditions set forth herein;
WHEREAS, the board of directors of Parent and the board of directors of Merger Sub have approved and declared it advisable for Merger Sub to enter into this Agreement providing for the Merger upon the terms and subject to the conditions set forth in this Agreement;
WHEREAS, in connection with this Agreement, the sole shareholder of Maverick Medical Group, Inc., a California professional corporation (“Maverick IPA”) and an affiliate of the Parent, intend to enter into a stock purchase agreement (the “Maverick Purchase Agreement”) no later than January 20, 2017, pursuant to which all of the issued and outstanding capital stock of Maverick IPA will be acquired at the Effective Time (as such term is defined below) by APC-LSMA Designated Shareholder Medical Corporation, a California professional corporation, an affiliate of Allied Physicians of California, a California professional medical corporation (“Allied IPA”);
WHEREAS, as a condition to, and simultaneously with, the execution of this Agreement, certain Shareholders (as such term is defined below) are entering into a voting agreement with Parent in the form attached hereto as Exhibit A (the “Voting Agreement”), pursuant to which they have agreed, among other things, to vote in favor of the approval and adoption of the Merger and this Agreement;
WHEREAS, prior to or concurrently with the consummation of the transactions contemplated by this Agreement and as a condition to the willingness of Parent and Merger Sub to consummate the transactions contemplated hereby, each shareholder of the Company (other than Dissenting Shareholders) (each a “Shareholder,” and collectively the “Shareholders”) will enter into a lock-up agreement with Parent in the form attached hereto as Exhibit B (the “Lock-Up Agreement”);
| -1- |
WHEREAS, prior to or concurrently with the consummation of the transactions contemplated by this Agreement and as a condition to Parent’s and Merger Sub’s willingness to consummate the transactions contemplated hereby, the Shareholders’ Representative will enter into an Exchange Agent Agreement with the Exchange Agent and Parent in the form attached hereto as Exhibit C with such changes as the Exchange Agent reasonably requires (the “Exchange Agreement”);
WHEREAS, concurrently with the consummation of the transactions contemplated by this Agreement and as a condition to Parent’s and Merger Sub’s willingness to consummate the transactions contemplated hereby, the Company shall relinquish its redemption rights to preferred stock of the Parent by entering into a Consent and Waiver Agreement in substantially the form attached hereto as Exhibit D (the “Consent and Waiver Agreement”); and
WHEREAS, for federal income Tax purposes, it is the intent of the Parties that the Merger qualify as a “reorganization” within the meaning of Section 368(a) of the Code, and this Agreement is intended to be and is adopted as a “plan of reorganization” within the meaning of Section 1.368-2(g) of the Treasury Regulations.
NOW, THEREFORE, in consideration of the mutual covenants and agreements set forth herein and other good and valuable consideration, the receipt and sufficiency of which are hereby acknowledged and incorporating the above recitals with and into this Agreement, the Parties hereto agree as follows.
1.1 The Merger. At the Effective Time (as defined in Section 1.3), subject to the terms and conditions of this Agreement and in accordance with the provisions of the CGCL, and in reliance upon the representations, warranties, covenants and agreements contained herein, (i) Merger Sub shall be merged with and into the Company, (ii) the separate corporate existence of Merger Sub shall cease and (iii) the Company shall continue as the surviving entity and a wholly-owned subsidiary of Parent (hereinafter sometimes referred to post-Closing as the (“Surviving Entity”)) and shall continue to be governed by the laws of the State of California, and the separate corporate existence of the Company, with all its rights, privileges, immunities, powers and franchises, shall continue unaffected by the Merger, except as set forth in Section 1.5.
1.2 Closing. The closing of the Merger (the “Closing”) shall take place on the second (2nd) Business Day after all of the conditions set forth in Article VI have been satisfied or waived (other than conditions that by their terms are to be satisfied at the Closing) or at such other date and time as may be mutually agreed upon by the Parties in writing. The Closing shall occur at the offices of McDermott Will & Emery, LLP, 2049 Century Park East, 38th Floor, Los Angeles, California 90067 or such other place as mutually agreed to by the Parties. The time and date on which the Closing is actually held is referred to herein as the “Closing Date.”
| -2- |
1.3 Effective Time. On the Closing Date, the Parties shall cause the Merger to be consummated by filing with the Secretary of State of the State of California a certificate of merger (the “Certificate of Merger”), executed in accordance with the provisions of the CGCL, and shall make all other filings or recordings required under the CGCL in order to effect the Merger. The Merger shall be effective upon the filing of the Certificate of Merger with the Secretary of State of the State of California or at such later time as is agreed to by the Parties in writing and specified in the Certificate of Merger. The time at which the Merger becomes effective is hereinafter referred to as the “Effective Time.”
1.4 Effects of the Merger. The Merger shall have the effects set forth in this Agreement, the Certificate of Merger and the CGCL. Without limiting the generality of the foregoing, at the Effective Time, all of the assets, rights, privileges, powers and franchises of the Company and the Merger Sub shall vest in the Surviving Entity, and all debts, liabilities and duties of the Company and the Merger Sub shall become the debts, liabilities and duties of the Surviving Entity.
1.5 Articles of Incorporation and Bylaws of the Surviving Entity.
(a) The articles of incorporation of the Company shall be amended and restated at and as of the Effective Time to read as did the articles of incorporation of Merger Sub immediately prior to the Effective Time; provided, that such articles of incorporation shall be amended to reflect that the name of the Surviving Entity shall be “Network Medical Management, Inc.” Such amended and restated articles of incorporation shall be the articles of incorporation of the Surviving Entity and shall continue in full force and effect until further amended in the manner prescribed therein and in accordance with the CGCL.
(b) The bylaws of the Company shall be amended and restated at and as of the Effective Time to read as did the bylaws of Merger Sub immediately prior to the Effective Time. Such amended and restated bylaws of the Company shall be the bylaws of the Surviving Entity and shall continue in full force and effect until further amended in the manner prescribed therein and by the CGCL; provided, that such bylaws shall be amended to reflect that the name of the Surviving Entity shall be “Network Medical Management, Inc.”
1.6 Tax Consequences. It is intended that the Merger will qualify as a “reorganization” within the meaning of Section 368(a) of the Code, and that this Agreement shall constitute, and is adopted as, a “plan of reorganization” within the meaning of Section 1.368-2(g) of the Treasury Regulations.
| -3- |
ARTICLE
II
EFFECT ON CAPITAL STOCK; MERGER CONSIDERATION
2.1 Effect on Capital Stock. As of the Effective Time, by virtue of the Merger, and without further action on the part of Parent, Merger Sub, the Company, the Shareholders’ Representative or the Shareholders:
(a) Merger Sub Shares. Each share of common stock of Merger Sub issued and outstanding immediately prior to the Effective Time, shall be converted into one validly issued, fully paid and non-assessable share of common stock of the Surviving Entity.
(b) Company Stock.
(i) Each Company Share that is held by Company as treasury stock or is otherwise owned by Company immediately prior to the Effective Time shall be cancelled and shall cease to exist, and no consideration shall be delivered in exchange therefor.
(ii) Subject to Sections 2.1(b)(i) and 2.8, each Company Share issued and outstanding immediately prior to the Effective Time shall be converted into the right to receive such number of fully paid and nonassessable Parent Shares that would result in the Shareholders having a right to receive an aggregate number of Parent Shares immediately following the Effective Time that represents eighty-two percent (82%) of the total issued and outstanding Parent Shares immediately following the Effective Time, assuming there are no Dissenting Shareholder Interests as of the Effective Time (the “Exchange Ratio”). Notwithstanding the foregoing, and for the avoidance of doubt, for purposes of calculating the Exchange Ratio, the aggregate number of Parent Shares held by the Shareholders immediately following the Effective Time shall exclude (i) any Parent Shares owned by the Shareholders immediately prior to the Effective Time, (ii) the Parent Warrants, and (iii) any Parent Shares issued or issuable to the Shareholders pursuant to the exercise of the Parent Warrants. All such Company Shares, when so converted, shall no longer be outstanding and shall automatically be cancelled and shall cease to exist, and each holder of a certificate that immediately prior to the Effective Time represented any such Company Shares (each, a “Certificate”) and each holder of Company Shares held in book-entry form shall, in each case, cease to have any rights with respect thereto, except the right to receive the Merger Consideration and any cash in lieu of fractional Parent Shares to be issued or paid in consideration therefor and any dividends or other distributions to which holders of Company Shares become entitled in accordance with Section 2.5.
(c) Parent Shares. Parent shall reserve and take all other action necessary or appropriate to have available for issuance or transfer a sufficient number of Parent Shares for delivery in accordance with this Section 2.1.
| -4- |
2.2 No New Shareholders. Immediately prior to the Closing Date, the transfer books of the Company shall be closed and thereafter there shall be no further registration of transfers of Company Shares of any Shareholder Interests on the records of the Company. From and after the Closing Date, any Shareholders who hold Company Shares outstanding immediately prior to the Effective Time shall cease to have any rights with respect to such Company Shares except as otherwise provided herein. In the event of a transfer of ownership of any Company Share prior to the Effective Time that has not been registered in the transfer records of the Company, the applicable Per Share Merger Consideration payable in respect of such Company Share shall be paid to the transferee of such Company Share and not the transferor if the Shareholders’ Representative receives all documents required to evidence and effect such transfer and to evidence that any applicable stock transfer or other Taxes have been paid.
2.3 Merger Consideration. Subject to the terms and conditions of this Agreement, the aggregate consideration to be paid by Parent shall be the Merger Consideration. The “Merger Consideration” is an amount equal to the total of:
| · | Ninety percent (90%) of the aggregate number of Parent Shares the Shareholders are entitled to receive pursuant to Section 2.1(b)(ii) (the “Closing Share Payment”), plus |
| · | the remainder, if any, from the holdback shares (initially, ten percent (10%) of the aggregate number of Parent Shares the Shareholders are entitled to receive pursuant to Section 2.1(b)(ii) (the “Holdback Shares”)). |
(a) Exchange Agent. Prior to the Closing, Parent shall appoint a bank or trust company reasonably acceptable to the Shareholders’ Representative pursuant to the Exchange Agreement to act as exchange agent (the “Exchange Agent”) hereunder.
(b) Deposit of Merger Consideration. At or prior to the Effective Time, Parent shall deposit with the Exchange Agent, in trust for the benefit of the Shareholders, in accordance with this Article II and through the Exchange Agent, sufficient cash and Parent Shares to make all other deliveries pursuant to this Article II; provided, however, that if the Closing Share Payment shall for any reason not include sufficient cash or Parent Shares to make all such deliveries, upon notice thereof from the Exchange Agent to Parent, Parent shall from time to time promptly deposit with the Exchange Agent sufficient cash and Parent Shares to make such Closing Share Payment. Any cash or Parent Shares deposited with the Exchange Agent shall be collectively referred to as the “Exchange Fund.”
(c) Letter of Transmittal. As soon as reasonably practicable after the Effective Time, the Exchange Agent shall mail to each Shareholder which immediately prior to the Effective Time held outstanding Company Shares that were converted into the right to receive the Merger Consideration pursuant to Section 2.1 and any cash in lieu of fractional Parent Shares to be issued or paid in consideration therefor (a) a letter of transmittal in the form attached hereto as Exhibit E (the “Letter of Transmittal”) (which shall specify that delivery shall be effected, and risk of loss and title to Certificate(s) shall pass, only upon actual delivery of Certificate(s) (or affidavits of loss in lieu of such Certificates) to the Exchange Agent and shall be substantially in such form and have such other provisions as shall be prescribed by the Exchange Agreement) and (b) instructions for use in surrendering Certificate(s) in exchange for the applicable Pro Rata Portion of the Closing Share Payment, any cash in lieu of fractional Parent Shares to be issued or paid in consideration therefor and any dividends or distributions to which such holder is entitled pursuant to this Article II. The receipt by each Shareholder of its applicable Pro Rata Portion of the Closing Share Payment, any cash in lieu of fractional Parent Shares and any dividends or distributions upon delivery of the Letters of Transmittal in accordance with this Section 2.4(c) shall be deemed to have been paid in full satisfaction of all rights pertaining to the Shareholder Interests of any such Shareholder and in exchange for the representations, warranties, indemnification obligations and release of claims given by each such Shareholder in such Shareholder’s Letter of Transmittal and herein.
| -5- |
(d) Merger Consideration Received in Connection with Exchange. Upon surrender to the Exchange Agent of its Certificate or Certificates, accompanied by a properly completed Letter of Transmittal, a Shareholder will be entitled to receive promptly after the Effective Time such Shareholder’s Pro Rata Portion of the Closing Share Payment, including any cash in lieu of fractional Parent Shares to be issued or paid in consideration, and the Person surrendering such Certificate or Certificates shall pay any transfer or other similar Taxes required by reason of the surrender or establish to the satisfaction of Parent that the Tax has been paid or is not applicable. Until so surrendered, each such Certificate shall represent after the Effective Time, for all purposes, only the right to receive, without interest, a Pro Rata Portion of the Closing Share Payment, including any cash in lieu of fractional Parent Shares to be issued or paid in consideration therefor in accordance with, and any dividends or distributions to which such holder is entitled pursuant to, this Article II.
(e) Treatment of Unexchanged Certificates and Shares. No dividends or other distributions with respect to Company Shares shall be paid to the Shareholder of any unsurrendered Certificate with respect to the Company Shares represented thereby, in each case unless and until the surrender of such Certificate in accordance with this Article II. Subject to the effect of applicable abandoned property, escheat or similar laws, following surrender of any such Certificate in accordance with this Article II, the record holder thereof shall be entitled to receive, without interest, (a) the amount of dividends or other distributions with a record date after the Effective Time theretofore payable with respect to whole Parent Shares represented by such Certificate and not paid and/or (b) at the appropriate payment date, the amount of dividends or other distributions payable with respect to Company Shares represented by such Certificate with a record date after the Effective Time (but before such surrender date) and with a payment date subsequent to the issuance of the Company Shares issuable with respect to such Certificate.
2.6 Withholding. Each of the Surviving Entity, Parent and Exchange Agent shall have the right to deduct and withhold from the consideration otherwise payable to any Shareholder pursuant to Section 2.3 and any other payments made pursuant to this Agreement such amounts as it is required to deduct and withhold with respect to the making of such payment under any provision of federal, state, local or foreign Tax law. To the extent the amounts are so withheld by the Surviving Entity, Parent or Exchange Agent, as the case may be, and timely paid over to the appropriate Governmental Authority, such withheld amounts shall be treated for all purposes of this Agreement as having been paid to the Shareholders in respect of whom such deduction and withholding was made by the Surviving Entity, Parent or Exchange Agent, as the case may be.
| -6- |
2.7 Stock Transfer Books. After the Effective Time, there shall be no transfers on the stock transfer books of Company of the Company Shares that were issued and outstanding immediately prior to the Effective Time other than to settle transfers of Company Shares that occurred prior to the Effective Time. If, after the Effective Time, Certificates representing such shares are presented for transfer to the Exchange Agent, they shall be cancelled and exchanged for the Merger Consideration and any cash in lieu of fractional Parent Shares to be issued or paid in consideration therefor in accordance with the procedures set forth in this Article II.
2.8 No Fractional Shares. No fractional Parent Shares shall be issued upon the surrender of Certificates for exchange, no dividend or distribution with respect to Parent Shares shall be payable on or with respect to any fractional share, and such fractional share interests shall not entitle the owner thereof to vote or to any other rights of a shareholder of Parent. Notwithstanding anything to the contrary contained herein, each holder of Company Shares who would otherwise have been entitled to receive a fractional Parent Share (after taking into account all Company Shares owned by such Person) shall receive, in lieu thereof, cash (without interest) in an amount equal to such fractional amount multiplied by $4.00. The Parties acknowledge that payment of cash in lieu of issuing fractional shares is solely for the purpose of avoiding the expense and inconvenience of issuing fractional shares and does not represent separately bargained-for consideration.
2.9 Termination of Exchange Fund. Any portion of the Exchange Fund that remains unclaimed by the Shareholders as of the second anniversary of the Effective Time will be paid to Parent. In such event, any former Shareholders who have not theretofore complied with this Article II shall thereafter look only to Parent with respect to the Merger Consideration, any cash in lieu of any fractional shares and any unpaid dividends and distributions on the Parent Shares deliverable in respect of each Parent Share such shareholder holds as determined pursuant to this Agreement, in each case, without any interest thereon. Notwithstanding the foregoing, none of Parent, the Surviving Entity, the Exchange Agent or any other Person shall be liable to any former Shareholder for any amount delivered in good faith to a public official pursuant to applicable abandoned property, escheat or similar laws. Any portion of the Merger Consideration remaining unclaimed by Shareholders as of a date that is immediately prior to such time as such amounts would otherwise escheat to or become property of any Governmental Entity will, to the extent permitted by applicable Legal Requirements, become the property of Parent free and clear of any claims or interest of any person previously entitled thereto.
2.10 Lost Certificates. In the event any Certificate shall have been lost, stolen or destroyed, upon the making of an affidavit of that fact by the person claiming such Certificate to be lost, stolen or destroyed and, if reasonably required by Parent or the Exchange Agent, the posting by such person of a bond in such amount as Parent may determine is reasonably necessary as indemnity against any claim that may be made against it with respect to such Certificate, the Exchange Agent will issue in exchange for such lost, stolen or destroyed Certificate the Merger Consideration deliverable in respect thereof pursuant to this Agreement.
| -7- |
2.11 Investment of Exchange Fund. The Exchange Agent shall invest any cash deposited by Parent in lieu of fractional Parent Shares to be issued or paid in consideration therefor in the Exchange Fund as directed by Parent. Any interest and other income resulting from such investments shall be paid to Parent. If for any reason (including losses) the cash in the Exchange Fund shall be insufficient to fully satisfy all of the payment obligations to be made in cash by the Exchange Agent hereunder, Parent shall promptly deposit cash into the Exchange Fund in an amount which is equal to the deficiency in the amount of cash required to fully satisfy such cash payment obligations.
2.12 No Liability. None of Parent, Merger Sub, Company, the Surviving Entity or the Exchange Agent shall be liable to any Person in respect of any Merger Consideration from the Exchange Fund delivered to a public official pursuant to any applicable abandoned property, escheat or similar Legal Requirements.
2.13 Holdback Shares. Parent will hold back the Holdback Shares, which represent ten percent (10%) of the Merger Consideration otherwise payable to the Shareholders under Section 2.3. The Holdback Shares shall be distributed to the Shareholders in accordance with their Pro Rata Portions as follows:
(a) One half (50%) of the Holdback Shares, subject to and contingent upon any reduction resulting from payments made or to be made pursuant to claims for indemnification by a Parent Indemnified Party during the first twelve (12) months following the Closing Date, shall be released to the Shareholders in accordance with their Pro Rata Portions on the first anniversary of the Closing Date.
(b) The remainder of the Holdback Shares, subject to and contingent upon any reduction resulting from payments made or to be made pursuant to claims for indemnification by a Parent Indemnified Party during the first twenty-four (24) months following the Closing Date, shall be released to the Shareholders on the second anniversary of the Closing Date.
2.14 Release of the Holdback Shares.
(a) Subject to the indemnification limitations set forth in Article VIII, Parent is authorized to set off and apply all indemnifiable Losses of the Parent Indemnified Parties against the amount of the Holdback Shares issuable to the Shareholders. Upon the final determination of any claim for indemnification, the remaining amount of the Holdback Shares shall be reduced by the amount necessary to satisfy and pay such claim. Notwithstanding the foregoing, at the Shareholders’ Representative’s election, the Shareholders’ Representative may tender to Parent cash equal to the indemnifiable Losses in lieu of Shareholder’s recourse to the Holdback Shares.
| -8- |
(b) Notwithstanding anything to the contrary in this Agreement, if any claims for indemnification by a Parent Indemnified Party have not been finally resolved before the Holdback Release Date, Parent may continue to hold back and not issue to the Shareholders a number of Holdback Shares sufficient to offset such pending claims should they be determined in favor of the Parent Indemnified Parties unless the Shareholders’ Representative shall have tendered to Parent cash equal to the indemnifiable Loss. If Parent shall not have tendered cash as set forth in the immediately preceding sentence, then promptly after final resolution of each such pending claim, Parent shall issue or pay to the Shareholders the portion of the withheld Holdback Shares that is in excess of the amount of any then remaining pending claims for indemnification hereunder.
(c) For purposes of placing a value on the Holdback Shares and for determining the number of Holdback Shares used to satisfy any indemnifiable Losses under this Section 2.14, the subject Holdback Shares shall be valued at the volume weighted average price (“VWAP”) per Parent Share averaged over the ten (10) trading days immediately preceding the time of assessment against such Holdback Shares (as adjusted for any stock dividends, combinations, reverse stock splits, stock splits, recapitalizations, reorganizations, reclassifications or other similar event with respect to the Holdback Shares).
2.15 Consideration Spreadsheet. At least three (3) Business Days before the Closing Date, the Company shall prepare and deliver to Parent a spreadsheet (the “Consideration Spreadsheet”), certified by the President of the Company, which shall set forth, as of the Closing Date, (i) such Person’s address and, if available to the Company, social security number (or tax identification number, if applicable), (ii) the number of Company Shares held by such Person, (iii) the respective certificate number(s) representing such Company Shares, (iv) the respective date(s) of acquisition of such Company Shares, (v) the Pro Rata Portion applicable to such Person, (vi) the number of Parent Shares issuable to such Person at the Closing in respect of such Company Shares, (vii) the number of Parent Shares comprising the Holdback Shares on behalf of such Person, (viii) any amounts required to be withheld and (ix) such other information relevant thereto or that Parent may reasonably request.
ARTICLE
III
PRE-CLOSING COVENANTS
3.1 Reasonable Best Efforts. Each Party will use its reasonable best efforts to take all actions necessary, proper or advisable in order to consummate the Merger and the other transactions contemplated by this Agreement (including satisfaction, but not waiver, of the closing conditions set forth in Article VI).
3.2 Operation of the Company. From the Execution Date until the Closing, the Company shall (i) conduct its business operations in the Ordinary Course of Business, (ii) preserve substantially intact its business organization and (iii) preserve its present relationships and goodwill with customers, suppliers and other Persons with which it has material business relations. Without limiting the generality of the foregoing, except for any requirements of CMS or any other Governmental Authority, the Company shall not take any of the following actions from the Execution Date until the Effective Time, without the prior written consent of Parent, which consent shall not be unreasonably withheld, conditioned or delayed:
| -9- |
(i) Amend or modify the articles of incorporation or bylaws of the Company or amend, modify, terminate, violate the requirements of, or let lapse any Permits or Licenses held by the Company;
(ii) Except as set forth in Schedule 3.2 attached, issue, deliver, sell, authorize, pledge or otherwise encumber any shares of capital stock, stock options or any securities convertible into shares of capital stock or other equity, or subscriptions, rights, warrants or options to acquire any shares of capital stock or other equity or any securities convertible into shares of capital stock or other equity, or enter into other agreements or commitments of any character obligating the Company to issue any such shares or convertible securities;
(iii) sell, assign, transfer, distribute, lease, license, impose (or cause or allow to be imposed) any Encumbrance (other than a Permitted Encumbrance) on, or otherwise dispose of, or agree to sell, assign, transfer, distribute, lease, license, impose (or cause or allow to be imposed) any Encumbrance (other than a Permitted Encumbrance) on, or otherwise dispose of, any material assets of the Company other than in the Ordinary Course of Business;
(iv) amend, modify or cease performing in any respect, perform or fail to perform in any manner that could cause a material breach of or default under, or terminate (or cause termination of), or transfer or assign (in whole or in part), any Material Contract;
(v) make or change any Tax election, adopt or change any Tax accounting method, file any amended Tax Return, enter into any closing agreement with respect to Taxes of the Company, settle or compromise any Tax claim or assessment of the Company, surrender any right to a refund with respect to Taxes of the Company, change an annual reporting period, or consent to any extension or waiver of the limitation period applicable to any Tax claim or assessment of the Company, or take any other similar action relating to the filing of any Tax Return or the payment of any Tax, if such election, adoption, change, amendment, agreement, settlement, surrender, consent or other action would have the effect of materially increasing the Tax liability or materially decreasing any Tax attribute of such entity;
(vi) acquire any entity or interest therein;
(vii) other than in the Ordinary Course of Business, increase the direct compensation, bonus compensation, or other compensation or benefits payable to any employee, independent contractor physician, director or officer;
(viii) except as provided in Section 3.12 below, declare, pay, or set aside any dividend or other distribution (whether in cash, stock, or property, or any combination thereof) in respect of its capital stock or other securities or redeem, purchase or otherwise acquire or offer to acquire any shares of its capital stock or other securities;
| -10- |
(ix) amend any Employee Benefit Plan or Other Plan, other than amendments that are required by applicable Legal Requirements;
(x) change its authorized capital structure or authorize for issuance, issue, sell, grant, pledge or dispose of, or agree or commit to issue, sell, grant, pledge or dispose of (whether through the issuance or granting of options, warrants, commitments, subscriptions, rights to purchase or otherwise) any stock of any class of the Company or any other securities or equity equivalents;
(xi) (i) prepay any loans (if any) from its Shareholders (in their capacity as such), officers or directors or any Person affiliated with any of the foregoing, (ii) make any change in its borrowing arrangements, (iii) waive, release or assign any material rights or claims, other than in the Ordinary Course of Business or (iv) incur any Indebtedness other than under its existing credit facilities;
(xii) make, authorize or incur any capital expenditures which individually exceed $50,000, or in the aggregate, exceed $250,000, except in the Ordinary Course of Business;
(xiii) change, alter or terminate any promotions, discounts, pricing, credit, payment or other terms with any customer or vendor, except in the Ordinary Course of Business;
(xiv) enter into any new line of business or discontinue any line of business;
(xv) make any change in the policies or practices of the Company with respect to the payment of accounts payable or accrued expenses, the collection of accounts receivable, or cash management (including with respect to purchases of inventory and supplies, repairs and maintenance, levels of capital expenditures, pricing and credit practices and operation of cash management practices generally) except in the Ordinary Course of Business;
(xvi) make any change in the accounting practices or principles with regard to the Company, other than as required by GAAP;
(xvii) allow to lapse, fail to maintain, abandon or otherwise dispose of any assets or properties except in the Ordinary Course of Business;
(xviii) commence any Action or settle or compromise any pending or threatened Action that (i) is material to the Company or (ii) involves monitoring or reporting obligations to any Governmental Authority;
(xix) incur any obligation or liability to any of its officers, directors, Shareholders, Business Employees or affiliated physicians or any loans or advances made by the Company to any of its officers, directors, Shareholders, Business Employees or affiliated physicians;
| -11- |
(xx) adjust, split, combine, subdivide or reclassify, or redeem, repurchase or otherwise acquire any shares of its capital stock or other equity interests, as the case may be, or effect any like change in the capitalization of the Company;
(xxi) enter into any strategic alliance, affiliate agreement or joint marketing arrangement or agreement;
(xxii) cancel, amend or renew any material insurance policy; or
(xxiii) enter into any executory agreement, commitment or undertaking to do any of the activities prohibited by the foregoing provisions.
For the avoidance of doubt, nothing contained herein shall permit Parent or Merger Sub to control the operation of the Company prior to the Closing.
3.3 Operation of Parent. From the Execution Date until the Closing, Parent shall (i) conduct its business operations in the Ordinary Course of Business, (ii) preserve substantially intact its business organization and (iii) preserve its present relationships and goodwill with customers, suppliers and other Persons with which it has material business relations. Without limiting the generality of the foregoing, except for any requirements of CMS or any other Governmental Authority, Parent shall not take any of the following actions from the Execution Date until the Effective Time, without the prior written consent of the Company, which consent shall not be unreasonably withheld, conditioned or delayed:
(i) Amend or modify the articles of incorporation or bylaws of Parent or amend, modify, terminate, violate the requirements of, or let lapse any Permits or Licenses held by the Parent;
(ii) issue, deliver, sell, authorize, pledge or otherwise encumber any shares of capital stock, stock options or other equity or any securities convertible into shares of capital stock or other equity, or subscriptions, rights, warrants or options to acquire any shares of capital stock or other equity or any securities convertible into shares of capital stock or other equity, or enter into other agreements or commitments of any character obligating Parent to issue any such shares or convertible securities;
(iii) sell, assign, transfer, distribute, lease, license, impose (or cause or allow to be imposed) any Encumbrance (other than a Permitted Encumbrance) on, or otherwise dispose of, or agree to sell, assign, transfer, distribute, lease, license, impose (or cause or allow to be imposed) any Encumbrance (other than a Permitted Encumbrance) on, or otherwise dispose of, any material assets of Parent other than in the Ordinary Course of Business;
(iv) amend, modify or cease performing in any respect, perform or fail to perform in any manner that could cause a material breach of or default under, or terminate (or cause termination of), or transfer or assign (in whole or in part), any Parent Material Contract;
| -12- |
(v) make or change any Tax election, adopt or change any Tax accounting method, file any amended Tax Return, enter into any closing agreement with respect to Taxes of Parent, settle or compromise any Tax claim or assessment of Parent, surrender any right to a refund with respect to Taxes of Parent, change an annual reporting period, or consent to any extension or waiver of the limitation period applicable to any Tax claim or assessment of Parent, or take any other similar action relating to the filing of any Tax Return or the payment of any Tax, if such election, adoption, change, amendment, agreement, settlement, surrender, consent or other action would have the effect of materially increasing the Tax liability of such entity or materially decreasing any Tax attribute of such entity;
(vi) acquire any entity or interest therein;
(vii) other than in the Ordinary Course of Business, increase the direct compensation, bonus compensation, or other compensation or benefits payable to any employee, independent contractor physician, director or officer;
(viii) declare, pay, or set aside any dividend or other distribution (whether in cash, stock, or property, or any combination thereof) in respect of its capital stock or other securities or redeem, purchase or otherwise acquire or offer to acquire any shares of its capital stock or other securities;
(ix) amend any Employee Benefit Plan or Other Plan, other than amendments that are required by applicable Legal Requirements;
(x) change its authorized capital structure or authorize for issuance, issue, sell, grant, pledge or dispose of, or agree or commit to issue, sell, grant, pledge or dispose of (whether through the issuance or granting of options, warrants, commitments, subscriptions, rights to purchase or otherwise) any stock of any class of the Company or any other securities or equity equivalents;
(xi) other than in conjunction with the Working Capital Note, (i) prepay any loans (if any) from Parent’s shareholders (in their capacity as such), officers or directors or any Person affiliated with any of the foregoing, (ii) make any change in its borrowing arrangements, (iii) waive, release or assign any material rights or claims, other than in the Ordinary Course of Business or (iv) incur any Indebtedness other than under its existing credit facilities;
(xii) make, authorize or incur any capital expenditures which individually exceed $50,000, or in the aggregate, exceed $250,000, except in the Ordinary Course of Business;
(xiii) change, alter or terminate any promotions, discounts, pricing, credit, payment or other terms with any customer or vendor, except in the Ordinary Course of Business;
| -13- |
(xiv) enter into any new line of business or discontinue any line of business;
(xv) make any change in the policies or practices of Parent with respect to the payment of accounts payable or accrued expenses, the collection of accounts receivable, or cash management (including with respect to purchases of inventory and supplies, repairs and maintenance, levels of capital expenditures, pricing and credit practices and operation of cash management practices generally) except in the Ordinary Course of Business;
(xvi) make any change in the accounting practices or principles with regard to Parent, other than as required by GAAP;
(xvii) allow to lapse, fail to maintain, abandon or otherwise dispose of any assets or properties except in the Ordinary Course of Business;
(xviii) commence any Action or settle or compromise any pending or threatened Action that (i) is material to Parent or (ii) involves monitoring or reporting obligations to any Governmental Authority;
(xix) incur any obligation or liability to any of Parent’s officers, directors, shareholders, Business Employees or affiliated physicians or any loans or advances made by Parent to any of its officers, directors, shareholders, Business Employees or affiliated physicians;
(xx) adjust, split, combine, subdivide or reclassify, or redeem, repurchase or otherwise acquire any shares of its capital stock or other equity interests, as the case may be, or effect any like change in the capitalization of the Company;
(xxi) enter into any strategic alliance, affiliate agreement or joint marketing arrangement or agreement;
(xxii) cancel, amend or renew any material insurance policy; or
(xxiii) enter into any executory agreement, commitment or undertaking to do any of the activities prohibited by the foregoing provisions.
For the avoidance of doubt, nothing contained herein shall permit Company to control the operation of the Parent.
| -14- |
3.4 Access to Information; Due Diligence. Upon reasonable notice and subject to applicable Legal Requirements relating to the confidentiality of information, each of Parent and Company shall, and shall cause each of its Subsidiaries to, facilitate reasonable due diligence on Parent or the Company, as applicable, and provide information and reasonably cooperate with Parent or the Company, as applicable, in connection with any reasonable request by the Parent or the Company, as applicable, related to such Party’s due diligence review of Parent or the Company, as applicable, and afford to the officers, employees, accountants, counsel, advisors, agents and other representatives of the other Party, reasonable access, during normal business hours, upon reasonable advance notice, during the period prior to the Closing Date, to all its properties, books, contracts, commitments and records, and, during such period, such party shall, and shall cause its Subsidiaries to, make available to the other Party (a) a copy of each report, schedule, registration statement and other document filed or received by it during such period pursuant to the federal securities laws (other than reports or documents that such party is not permitted to disclose under applicable Legal Requirements) and (b) all other information concerning its business, properties and personnel as the other party may reasonably request. Neither Parent nor Company, nor any of their Subsidiaries, shall be required to provide access to or to disclose information where such access or disclosure would jeopardize the attorney-client privilege of such Party or its Subsidiaries or contravene any law, rule, regulation, order, judgment, decree, fiduciary duty or binding agreement entered into prior to the date of this Agreement. The Parties shall make appropriate substitute disclosure arrangements under circumstances in which the restrictions of the preceding sentence apply. All information and materials provided pursuant to this Agreement shall be subject to the provisions of the Confidentiality Agreement and Section 3.7. Each Party agrees that such investigation shall be conducted in such a manner as not to interfere unreasonably with the operations of the other Party.
3.5 Exclusivity; No Negotiation.
(a) Company’s Non-Solicitation.
(i) From the Execution Date until the earlier of the Closing or the termination of this Agreement, the Company agrees that it will not, and will cause its subsidiaries, directors, officers, Business Employees, agents or representatives not to, initiate, solicit, encourage or knowingly facilitate inquiries or proposals with respect to, or engage in any negotiations concerning, or provide any confidential or nonpublic information or data to, or have any discussions with, any person relating to, any Company Acquisition Proposal; provided, that, in the event Company receives an unsolicited Company Acquisition Proposal and the board of directors of Company concludes in good faith that there is a reasonable likelihood that such Company Acquisition Proposal constitutes or is reasonably likely to result in a Superior Company Acquisition Proposal, Company may, and may permit its representatives, to, furnish or cause to be furnished nonpublic information and participate in such negotiations or discussions to the extent that the board of directors of Company concludes in good faith (and based on the advice of counsel) that failure to take such actions would more likely than not result in a violation of its fiduciary duties under applicable Legal Requirements; provided, further, that prior to providing any nonpublic information permitted to be provided pursuant to the foregoing proviso, it shall have entered into a nondisclosure agreement with such third party on terms no less favorable to it than the Nondisclosure Agreement, and it shall simultaneously provide the Parent with any such nonpublic information to the extent it has not previously provided such information to the Parent. Company will immediately cease and cause to be terminated any activities, discussions or negotiations conducted before the date of this Agreement with any persons other than Parent with respect to any Company Acquisition Proposal and will use its reasonable best efforts to enforce any confidentiality or similar agreement relating to a Company Acquisition Proposal. The Company will promptly (and in any event, within two Business Days) advise Parent following receipt of any Company Acquisition Proposal (or any indication by any Person that it is considering making a Company Acquisition Proposal) and the substance thereof (including the identity of the Person making such Company Acquisition Proposal), and will keep Parent apprised of any related developments, discussions and negotiations (including the terms and conditions of the Company Acquisition Proposal) on a current basis.
| -15- |
(ii) The Company Board shall not: (A) (i) withdraw (or modify or qualify in any manner adverse to Parent) the approval, recommendation or declaration of advisability of this Agreement, the Merger and the consummation of the transactions contemplated by this Agreement, (ii) adopt, approve, recommend, endorse or otherwise declare advisable the adoption of any Company Acquisition Proposal or (iii) resolve, agree or propose to take any such actions (each such action, a “Company Adverse Recommendation Change”), (B) cause or permit the Company to enter into any letter of intent, memorandum of understanding, agreement in principle, acquisition agreement, merger agreement, option agreement, joint venture agreement, partnership agreement or other similar agreement constituting or related to, or which is intended to or reasonably likely to lead to, any Company Acquisition Proposal or (C) resolve, agree or propose to take any of such actions. Notwithstanding the foregoing, at any time prior to obtaining the Company’s Shareholder Approval, the Company Board may make a Company Adverse Recommendation Change if it determines in good faith (after consulting with outside counsel) that the failure to do so would result in a breach of its fiduciary duties under applicable Legal Requirements.
(b) Parent’s Non-Solicitation.
(i) From the Execution Date until the earlier of the Closing or the termination of this Agreement, Parent agrees that it will not, and will cause its subsidiaries, directors, officers, Business Employees, agents or representatives not to, initiate, solicit, encourage or knowingly facilitate inquiries or proposals with respect to, or engage in any negotiations concerning, or provide any confidential or nonpublic information or data to, or have any discussions with, any person relating to, any Parent Acquisition Proposal; provided, that, in the event Parent receives an unsolicited Parent Acquisition Proposal and the board of directors of Parent concludes in good faith that there is a reasonable likelihood that such Parent Acquisition Proposal constitutes or is reasonably likely to result in a Superior Proposal, Parent may, and may permit its representatives, to, furnish or cause to be furnished nonpublic information and participate in such negotiations or discussions to the extent that the board of directors of Parent concludes in good faith (and based on the advice of counsel) that failure to take such actions would more likely than not result in a violation of its fiduciary duties under applicable Legal Requirements; provided, further, that prior to providing any nonpublic information permitted to be provided pursuant to the foregoing proviso, it shall have entered into a nondisclosure agreement with such third party on terms no less favorable to it than the Nondisclosure Agreement, and it shall simultaneously provide the Company with any such nonpublic information to the extent it has not previously provided such information to the Company. Parent will immediately cease and cause to be terminated any activities, discussions or negotiations conducted before the date of this Agreement with any persons other than the Company with respect to any Parent Acquisition Proposal and will use its reasonable best efforts to enforce any confidentiality or similar agreement relating to a Parent Acquisition Proposal. Parent will promptly (and in any event, within two Business Days) advise the Company following receipt of any Parent Acquisition Proposal (or any indication by any Person that it is considering making a Parent Acquisition Proposal ) and the substance thereof (including the identity of the person making such Parent Acquisition Proposal), and will keep the Company apprised of any related developments, discussions and negotiations (including the terms and conditions of the Parent Acquisition Proposal) on a current basis.
| -16- |
(ii) The Parent board of directors shall not: (A) (i) withdraw (or modify or qualify in any manner adverse to the Company) the approval, recommendation or declaration of advisability of this Agreement, the Merger and the consummation of the transactions contemplated by this Agreement, (ii) adopt, approve, recommend, endorse or otherwise declare advisable the adoption of any Parent Acquisition Proposal or (iii) resolve, agree or propose to take any such actions (each such action, a “Parent Adverse Recommendation Change”) or (B) cause or permit Parent to enter into any letter of intent, memorandum of understanding, agreement in principle, acquisition agreement, merger agreement, option agreement, joint venture agreement, partnership agreement or other similar agreement constituting or related to, or which is intended to or reasonably likely to lead to, any Parent Acquisition Proposal or (C) resolve, agree or propose to take any of such actions. Notwithstanding the foregoing, at any time prior to obtaining the Parent Shareholder Approval, the Parent board of directors may make a Parent Adverse Recommendation Change if it determines in good faith (after consulting with outside counsel) that the failure to do so would result in a breach of its fiduciary duties under applicable Legal Requirements.
3.6 Notices of Certain Events; Continuing Disclosure.
(a) Each of the Company and Parent shall promptly notify the other Party of, and deliver to such other Party copies of all documentation relating to:
(i) any notice or other communication from any Person alleging that the consent of such Person is or may be required in connection with the transactions contemplated by this Agreement;
(ii) the occurrence of any breach by the Company, the Shareholders or the Parent, as applicable, of any representation, warranty, covenant or agreement contained in this Agreement, promptly after the Company, the Shareholders or the Parent, as applicable, becomes aware of any such breach, including without limitation any such breach that could reasonably be expected to cause any of the closing conditions set forth in Article VI not to be satisfied;
| -17- |
(iii) any Action commenced or, to the Company’s Knowledge or Parent’s Knowledge, as applicable, threatened against or relating to or involving the Company or the Parent, as applicable, that relates to the consummation of the transactions contemplated by this Agreement, or relates to any of the material assets of the Company or the Parent, as applicable, or any developments relating to any Action otherwise disclosed pursuant to this Agreement;
(iv) any written materials or communications sent by or on behalf of the Company to its Shareholders, or received from the Shareholders pursuant to the procedures described in Section 2.5, subsequent to the Execution Date;
(v) any notice, correspondence, document or other communication sent by or on behalf of the Company or Parent, as applicable, to any party to any Material Contract or Parent Material Contract or sent to the Company or Parent, as applicable, by any party to any Material Contract or Parent Material Contract (other than any communication that relates solely to routine commercial transactions between the Company and the other party to any such material contract and that is of the type sent in the Ordinary Course of Business);
(vi) any notice, report or other document either filed with or sent to, or received from, any Governmental Authority, or any governmental investigation on an alleged violation or noncompliance with Legal Requirements on behalf of the Company or Parent, as applicable, subsequent to the Execution Date in connection with the Merger or any of the other transactions contemplated by this Agreement; and
(vii) copies of all material operating and financial reports prepared by the Company or Parent, as applicable, for such Party’s senior management or for use in preparing such Party’s consolidated financial statements, including: (A) copies of the unaudited monthly consolidated balance sheets of the Company or Parent, as applicable, and the related unaudited monthly consolidated statements of operations, statements of shareholders’ equity and statements of cash flows and (B) copies of any forecasts, write-off reports, hiring reports and capital expenditure reports prepared for the Company’s or Parent’s senior management, as applicable.
The delivery of any notice pursuant to this Section 3.6(a) will not limit any of the representations and warranties of the Company set forth in this Agreement or the remedies available hereunder.
(b) The Company may, from time to time up to and including the date that is five (5) days prior to the Closing Date, by notice to Parent, supplement, amend or create any section of the Disclosure Schedule, but only with respect to events occurring after the Execution Date, in order to add information or correct previously disclosed information. The Disclosure Schedule may be supplemented, amended and/or added to, to add immaterial, as well as material, items thereto. No such supplement, amendment or addition shall be deemed to cure any breach for purposes of Article VIII.
| -18- |
3.7 Confidentiality, Press Releases and Public Announcements.
(a) The terms of the Nondisclosure Agreement entered into previously by the Company and Parent are hereby incorporated by reference and shall continue in full force and effect until the Closing. The Parties acknowledge that any information provided to, or otherwise acquired by, it in connection with this Agreement and the transactions contemplated by this Agreement is subject to the terms of the Nondisclosure Agreement, the terms of which are incorporated herein by reference. Each of the Parties agrees for itself and its representatives and Affiliates to use the Confidential Information (as such term is defined in the Nondisclosure Agreement) solely for the purposes of evaluating the Disclosing Party (as such term is defined in the Nondisclosure Agreement) and consummating the Merger and for no other purpose and to keep the Disclosing Party’s Confidential Information confidential. Company covenants and agrees for itself and its representatives and Affiliates not to use the Confidential Information, at any time, for trading in Parent’s securities.
(b) Parent and the Company will consult with each other before issuing, and provide each other the opportunity to review, comment upon and concur with, and use commercially reasonable efforts to agree on, any press release or other public statements with respect to the transactions contemplated by this Agreement, including the Merger, and shall not issue any such press release or make any such public statement prior to such consultation, except as either party may determine is required by applicable Legal Requirements, court process or by obligations pursuant to any securities exchange or stock market. Notwithstanding the foregoing, if Parent determines it is required by applicable Legal Requirements to make a public announcement, including, without limitation, with respect to any filing with the SEC that Parent may be required to make as a result of the execution of this Agreement or the consummation of the transactions contemplated hereby, Parent shall give the Company as much prior notice as is reasonably practicable and shall consult with the Company about the text of such announcement or filing but shall not be required to obtain the consent of the Company with regard to such announcement or filing. Parent and the Company will consult with each other concerning the means by which any employee, customer or supplier of Company (or their respective subsidiaries) or Parent or any other Person having any business relationship with either Company or Parent (or their respective subsidiaries) will be informed of the transactions contemplated by this Agreement, and the other Party will have the right to be present for any such communication.
| -19- |
3.8 Third Party Consents and Approvals.
(a) Subject to the terms and conditions set forth in this Agreement, each of Parent, the Company, and the Shareholders’ Representative shall use its commercially reasonable efforts to take such actions as are necessary or advisable to consummate, as promptly as practicable, the Merger and the other transactions contemplated by this Agreement, including (i) obtaining all necessary consents, authorizations and approvals from any Governmental Authority, including, without limitation, Notification and Report Forms and related material required to be filed with the Federal Trade Commission and the Antitrust Division of the United States Department of Justice under the HSR Act with respect to the transactions contemplated hereby or Third Party, (ii) the execution and delivery of any additional instruments necessary to consummate the Merger and (iii) the other actions contemplated in paragraphs (b) through (e) of this Section 3.8.
(b) Without limiting the generality of the undertakings pursuant to this Section 3.8, the Parties hereto shall (i) provide or cause to be provided as promptly as practicable to Governmental Authorities with regulatory jurisdiction over enforcement of any antitrust law (each such Governmental Authority, a “Governmental Antitrust Authority”) information and documents requested by any Governmental Antitrust Authority or necessary, proper or advisable to permit consummation of the transactions contemplated by this Agreement, including preparing and filing any filings under any antitrust law as promptly as practicable following the Execution Date (but in no event more than fifteen (15) business days from the date hereof except by mutual consent confirmed in writing) and (ii) use their reasonable commercial efforts to take such actions as are necessary or advisable to obtain prompt approval of consummation of the transactions contemplated by this Agreement by any Governmental Authority; provided, however, that no Party or Affiliate of any Party shall be required to divest any assets or business lines, or take any other action unrelated to the transactions contemplated by this Agreement to satisfy such reasonable commercial efforts, unless otherwise agreed by such Party.
(c) Parent and the Company shall, upon request, furnish each other with all information concerning themselves, their respective subsidiaries, directors, officers, Business Employees and shareholders and such other matters as may be reasonably necessary or advisable in connection with any statement, filing, notice, application or other document made by or on behalf of Parent, the Company or any of their respective Affiliates to any Governmental Authority in connection with the Merger and the other transactions contemplated by this Agreement. Parent and the Company shall promptly advise each other upon receiving any communication from any Governmental Authority in respect of any filing, investigation or inquiry concerning this Agreement or the transactions contemplated by this Agreement.
(d) Each of the Company, Parent and Merger Sub shall give (or shall cause their respective Affiliates to give) any notices to Third Parties, and use, and cause their respective Affiliates to use, their commercially reasonable efforts to obtain all Third Party consents necessary or advisable for consummation of the transactions contemplated by this Agreement, including, without limitation, the Company Consents. The Parties shall consult each other with respect to obtaining the Company Consents and all necessary approvals of Governmental Authorities. Each of Parent and the Company shall use its commercially reasonable efforts to resolve any objections that may be asserted by any Governmental Authority with respect to this Agreement and the Merger or the other transactions contemplated by this Agreement, and each of Parent and the Company shall keep the other Party reasonably apprised of the status of matters relating to completion of the transactions contemplated by this Agreement.
| -20- |
(e) All fees paid in connection with filings required under the HSR Act or other antitrust laws in order to consummate the transactions contemplated hereby shall be paid fifty-percent (50%) by the Company and fifty-percent (50%) by Parent. All out-of-pocket expenses incurred by Parent, the Company or the Shareholders in connection with their respective obligations pursuant to this Section 3.8 shall be borne by the party incurring such expenses.
3.9 Proxy/Registration Statement.
(a) As promptly as possible following the Execution Date, Parent and the Company shall jointly prepare and file with the SEC a single document (the “Proxy/Registration Statement”) that will constitute a proxy statement (the “Proxy Statement”) relating to the special meeting of the stockholders of Parent (the “Parent Shareholder Meeting”) to be held to consider the issuance of Parent Shares in connection with the Merger and, if Parent determines in its sole discretion that it is required, a registration statement on Form S-4 relating to the registration under the Securities Act of the Parent Shares to be issued in the Merger (the “Registration Statement”). Parent and the Company shall ensure the Proxy/Registration Statement includes all information required under applicable Legal Requirements to be furnished to the holders of Parent Shares in connection with the Agreement and the transactions contemplated hereby, and complies as to form and substance in all material respects with the applicable Legal Requirements. Parent and the Company each shall furnish all information concerning itself as the other party may reasonably request in connection with the preparation of the Proxy/Registration Statement. Parent and the Company shall use its commercially reasonable efforts to get clearance for the Proxy Statement by the SEC (the “Proxy Clearance Date”) as soon as is practicable following the filing of the Proxy Statement with the SEC and, if applicable, Parent and the Company shall use commercially reasonable efforts to cause the Registration Statement to become effective as promptly as practicable (the date of effectiveness being the “Registration Statement Effective Date”). Parent shall as soon as reasonably practicable (i) notify the Company of the receipt of any comments from the SEC with respect to the Proxy/Registration Statement and any request by the SEC for any amendment to the Proxy/Registration Statement or for additional information and (ii) provide the Company with copies of all correspondence between Parent and its representatives, on the one hand, and the SEC, on the other hand, with respect to the Proxy Statement. As promptly as practicable after the Proxy Clearance Date or, if applicable, the Registration Statement Effective Date, the proxy statement and, if applicable, the prospectus, included in the Proxy/Registration Statement (collectively, the “Proxy Materials”) shall be mailed to the stockholders of Parent.
(b) No amendment or supplement to the Proxy/Registration Statement shall be made without the approval of each of Parent and the Company, which approval shall not be unreasonably withheld, conditioned or delayed. Each of Parent and the Company shall promptly advise the other upon becoming aware of (i) the time when the Proxy Statement has been cleared by the SEC or, if applicable, the Registration Statement has become effective or any supplement or amendment has been filed, (ii) the issuance of any stop order, (iii) the suspension of the qualification of Parent Shares issuable in connection with the Merger for offering or sale in any jurisdiction or (iv) any comments, responses or requests from the SEC relating to the Proxy Materials or, if applicable, the Registration Statement or any of the transactions contemplated by this Agreement.
| -21- |
(c) The information supplied by Parent for inclusion in the Proxy /Registration Statement will not, at (i) the Registration Statement Effective Date, if applicable, (ii) the time the Proxy Materials (or any amendment of or supplement to the Proxy Materials) are first mailed to the shareholders of Parent, (iii) the time of the Company Shareholder Meeting and (iv) the Effective Time, contain any untrue statement of a material fact or fail to state any material fact required to be stated in the Proxy/Registration Statement or necessary in order to make the statements in the Proxy/Registration Statement not misleading. If, at any time prior to the Effective Time, any information relating to Parent or any of its Subsidiaries should be discovered by Parent that should be set forth in an amendment or a supplement to the Proxy/Registration Statement, Parent shall promptly inform the Company.
(d) The information supplied by the Company for inclusion in the Proxy /Registration Statement will not, at (i) the Registration Statement Effective Date, if applicable, (ii) the time the Proxy Materials (or any amendment of or supplement to the Proxy Materials) is first mailed to the shareholders of Parent, (iii) the time of the Parent Shareholders Meeting and (iv) the Effective Time, contain any untrue statement of a material fact or fail to state any material fact required to be stated in the Proxy/Registration Statement or necessary in order to make the statements in the Proxy/Registration Statement not misleading. If, at any time prior to the Effective Time, any information relating to the Company or any of its Subsidiaries should be discovered by the Company that should be set forth in an amendment or a supplement to the Proxy/Registration Statement, the Company shall promptly inform Parent.
3.10 Company Shareholder Approval. As of the date of this Agreement, the Company Board has adopted resolutions approving this Agreement and the transactions contemplated by this Agreement on substantially the terms and conditions set forth in this Agreement, and directing that this Agreement and the other transactions contemplated by this Agreement, on such terms and conditions, be submitted to the Shareholders for their consideration at a special meeting (the “Company Shareholder Meeting”). As soon as practicable following the Proxy Clearance Date and, if applicable, the Registration Statement Effectiveness Date, the Company shall give notice (the “Company Shareholder Meeting Notice”) to the Shareholders for the purpose of approving this Agreement and the other transactions contemplated by this Agreement, together with any other matters required to be approved or adopted by the Shareholders in order to carry out the intentions of this Agreement. Parent and the Company shall cooperate with each other to cause the Company Shareholder Meeting to be held as soon as practicable following the mailing of the Company Shareholder Meeting Notice to the shareholders of the Company. In furtherance of that obligation, the Company will take, in accordance with the federal securities laws, the CGCL and its Articles of Incorporation and Bylaws, all action necessary to duly call, give notice of, convene and hold a special meeting of the holders of Company Common Stock, to be held no later than thirty (30) calendar days following the date the Company sends the Shareholder Meeting Notice (with any and all adjournments to occur within such thirty (30) calendar day period), to consider and vote upon the adoption of this Agreement and approval of the other transactions contemplated by this Agreement as well as any other such matters. Except in the case of a Company Adverse Recommendation Change specifically permitted by Section 3.5(a), the Company Board will use all reasonable best efforts to (a) recommend to its Shareholders that they adopt this Agreement and (b) obtain from its Shareholders the approval of a proposal to adopt this Agreement (the “Company Shareholder Approval”). Parent and the Company shall jointly prepare the Shareholder Meeting Notice and other materials mailed to Shareholders in conjunction with the special meeting of holders of Company Common Stock, which shall be materially consistent with the Proxy Materials. The Company shall submit this Agreement to its Shareholders at the shareholders meeting even if the Company Board shall have withdrawn, modified or qualified its recommendation, unless this Agreement has been terminated in accordance with its terms. Within two (2) Business Days after the special meeting of the Shareholders described in this Section 3.10, the Company shall deliver to the Shareholders’ Representative and to Parent a certificate of an authorized officer of the Company certifying as to the number of Company Shares voted and Shareholders voting in favor of, voting against, or abstaining from voting on the Merger and the terms of this Agreement, and the transactions contemplated hereby at such special meeting.
| -22- |
3.11 Parent Shareholder Approval.
(a) As of the date of this Agreement, the board of directors of Parent has adopted resolutions approving this Agreement and the transactions contemplated by this Agreement on substantially the terms and conditions set forth in this Agreement. As soon as practicable following the Proxy Clearance Date and, if applicable, the Registration Statement Effectiveness Date, Parent shall give notice (the “Parent Shareholder Meeting Notice”) to the shareholders of Parent for the purpose of approving this Agreement and the other transactions contemplated by this Agreement, together with any other matters required to be approved or adopted by the shareholders of Parent in order to submit for approval by the requisite vote of such shareholders a proposal to authorize (i) the Merger, including the issuance of the Parent Shares that will comprise the Merger Consideration, and the other transactions contemplated by this Agreement, (ii) the division of the board of directors of Parent into three classes and the amendments to the Parent’s Certificate of Incorporation and Bylaws to effect such Board classification, (iii) the election to the board of directors of Parent of the persons designated by the Company and Parent as set forth on Schedule 7.3, and (iv) any other action required to be approved by the shareholders of Parent in connection with this Agreement, the Merger or the transactions contemplated hereby. Parent and the Company shall cooperate with each other to cause the Parent Shareholder Meeting to be held as soon as practicable following the mailing of the Proxy Materials to the shareholders of Parent. Parent shall take all action in accordance with the federal securities laws, the Delaware General Corporation Law, and Parent’s Certificate of Incorporation and Bylaws necessary to duly call, give notice of, convene and hold a special meeting of the holders of Parent Shares to be held on the earliest practicable date. Except in the case of a Parent Adverse Recommendation Change specifically permitted by Section 3.5(b), the board of directors of Parent will use all reasonable best efforts to (a) recommend to its shareholders that they adopt this Agreement and approve the issuance of the Merger Consideration, (b) include such recommendation in Parent’s proxy statement and (c) obtain from its shareholders a vote adopting this Agreement and approving the Merger and the classification of the board of directors of Parent, and the election to the board of directors of Parent of the persons designated by the Company and Parent as set forth on Schedule 7.3 (the “Parent Shareholder Approval”); provided, that, such Parent Shareholder Approval shall require (x) the approval of a majority of the Parent Shares and (y) the approval of a majority of the Parent Shares not owned by the Company. The Parent shall submit this Agreement to its shareholders at the shareholders meeting even if the board of directors of Parent shall have withdrawn, modified or qualified its recommendation, unless this Agreement has been terminated in accordance with its terms. Within two (2) Business Days after the special meeting of the shareholders of Parent described in this Section 3.11, Parent shall deliver to the Shareholders’ Representative and to the Company a certificate of an authorized officer of Parent certifying as to the number of Parent Shares voted and shareholders of Parent voting in favor of, voting against, or abstaining from voting on the Merger and the terms of this Agreement, and the transactions contemplated hereby at such special meeting.
| -23- |
3.12 Company Financial Statements. The Company agrees to use its best efforts to deliver to Parent as promptly as practical and in any event no later than March 1, 2017 (i) unaudited consolidated balance sheets of the Company and its Subsidiaries as of September 30, 2015 and 2016 and the related consolidated statements of income, stockholders’ equity and statements of cash flows of the Company and its Subsidiaries for the nine (9) month period ended September 30, 2015 and 2016 and (ii) audited consolidated balance sheets of the Company and its Subsidiaries as of December 31, 2015 and 2016, and the related consolidated statements of income, stockholders’ equity and statements of cash flows of the Company and its Subsidiaries for the annual period ended December 31, 2015 and 2016. All financial statements delivered pursuant to this Section 3.12 will be prepared in accordance with GAAP, will contain all required footnote disclosure and will be prepared in accordance with the financial statement requirements of Regulation S-X and otherwise the requirements of Forms 10-K and 10-Q, as applicable, for purposes of inclusion in documents to be filed by Parent with the SEC.
3.13 Distribution of Company Distributable Cash and Parent Warrants. The Parties agree that prior to the Closing, (i) the Company may at any time or from time to time in the Company’s sole discretion distribute all or any portion of the Company Cash to its shareholders so long as (x) the Company retains sufficient Company Cash to conduct its Business in the Ordinary Course of Business and (y) the Company is able to satisfy the covenant to maintain the minimum level of Company Cash set forth in Section 3.15 (the “Company Distributable Cash”) and (ii) immediately prior to Closing the Company may make an in-kind distribution to its shareholders of the Series A and Series B warrants issued by Parent to the Company to purchase Parent Shares (the “Parent Warrants”) such that the Parent Warrants shall not be exercised prior to the Effective Time.
3.14 Working Capital Loan. Within five (5) Business Days following the Execution Date, the Company shall provide a working capital loan to the Parent in the principal amount of Five Million Dollars ($5,000,000) (the “Working Capital Loan Amount”), which Working Capital Loan Amount shall be evidenced by a promissory note substantially in the form of Exhibit F attached hereto (the “Working Capital Note”). The principal amount of the Working Capital Loan Amount shall be funded by wire of immediately available funds to an account designated by Parent. The Working Capital Loan Amount will be loaned by the Shareholders to the Company as an advance from the proceeds of the Company Distributable Cash that would otherwise have been distributed to the Shareholders. In furtherance of the foregoing, the Company shall execute and deliver a promissory note payable to the Shareholders’ Representative on behalf of the Shareholders in the principal amount of the Working Capital Loan Amount, which promissory note shall in a form reflecting the same principal terms as the Working Capital Note (the “Shareholder Note”).
| -24- |
3.15 Minimum Company Cash. The Company covenants and agrees to maintain minimum Company Cash immediately prior to the Effective Time of not less than Ten Million Dollars ($10,000,000) less the amount of the Working Capital Loan Amount.
3.16 Company Repurchase of Dissenting Shareholder Interests.
(a) The Company shall serve prompt written notice to Parent of any demand, purported demand, objection, notice, petition, or other communication received from any of the Company’s shareholders or provided to shareholders by the Company on or prior to the Closing Date with respect to any Company Shares that will not be voted in favor of the Merger or the other transactions contemplated by this Agreement (each a “Dissenting Shareholder Interest”) or otherwise with respect to any shareholder who intends not to vote in favor of the Merger or the other transactions contemplated by this Agreement (each a “Dissenting Shareholder”);
(b) Within ten (10) days following Company Shareholder Approval of the Merger, the Company shall provide to its shareholders all notices required by Chapter 13 of the CGCL (the “Dissenters’ Rights Rules”) concerning the rights of the shareholders to exercise appraisal rights under the Dissenters’ Rights Rules with respect to the Merger; and
(c) Prior to the Closing Date, the Company shall repurchase and cancel all Company Shares (including any other securities exercisable for or convertible into Company Shares, or rights to acquire Company Shares) that are Dissenting Shareholder Interests or that are otherwise held, directly or indirectly, by Dissenting Shareholders, or by other Shareholders who have exercised their dissenters’ rights in accordance with the Dissenters’ Rights Rules.
ARTICLE
IV
REPRESENTATIONS AND WARRANTIES OF THE COMPANY
Except as set forth in the Disclosure Schedule dated as of the date hereof and delivered by the Company to Parent concurrently with or prior to the execution and delivery of this Agreement (the “Disclosure Schedule”), as an inducement to Parent and to Merger Sub to enter into this Agreement and to consummate the transactions contemplated by this Agreement, the Company makes the following representations and warranties to Parent and to Merger Sub as of the Execution Date and the Closing Date:
| -25- |
4.1 Authority of the Company; No Conflicts. This Agreement constitutes a valid and binding agreement by the Company, enforceable in accordance with its terms, and, except as set forth on Schedule 4.1, neither the execution and delivery of this Agreement nor the consummation of the transactions contemplated hereby nor compliance with any of the provisions hereof will:
(a) conflict with, or result in, a breach of the corporate or governing documents of the Company, as applicable;
(b) violate any applicable statute, Legal Requirement, rule or regulation or any other writ, injunction or decree of any court or Governmental Authority;
(c) violate or conflict with or constitute a default under (or give rise to any right of termination, cancellation or acceleration under, whether after the giving of notice, lapse of time, or both) the terms or conditions or provisions of any note, instrument, bond, lease, mortgage, obligation, Plan Contract or other agreement or understanding, arrangement or restriction of any kind to which the Company, or in the case of Plan Contracts, any of the Company’s clients, is a party or by which the Company or any of its assets or properties may be bound; or
(d) require the consent or approval by or notice to any Governmental Authority or other Third Party beyond those already obtained prior to the date hereof, including consents for any change of control of the Company, pursuant to or as a result of the transactions contemplated under this Agreement and for the continuity of Plan Contracts and reimbursement under those contracts.
4.2 Organization; Power and Authority. The Company is a corporation duly organized, validly existing, and in good standing under the laws of the State of California, and has the right, power, legal capacity and authority to enter into and perform its obligations under this Agreement and the other Transaction Documents to which it is a party in accordance with its terms subject to General Enforceability Exceptions. The Company has all requisite corporate power and authority to own, operate and lease its respective properties and carry on its Business as currently conducted. The Company is qualified to do business as a foreign corporation under the laws of each jurisdiction where failure to so qualify would have a Material Adverse Effect. The copies of the articles of incorporation, bylaws and other organizational and governing instruments for the Company, each as amended to date and made available to Parent’s counsel, are complete and correct, and no amendments thereto are pending other than as contemplated hereby. Other than the Company Shareholder Approval that will occur pursuant to Section 3.10 of this Agreement, all action on the part of the Company necessary for the authorization, execution, delivery and performance of this Agreement and the other Transaction Documents to which it is a party and the consummation of the transactions contemplated hereby and thereby has been taken. The Company Board has approved the Merger and this Agreement in accordance with the CGCL and all requirements of the Company’s organizational and governing documents. Except as set forth on Schedule 4.2, the Company does not have any subsidiary, or any equity interest in another Person.
| -26- |
4.3 Financial Statements; Accounts Receivable. The following have been prepared from the books and records of the Company and are provided in Schedule 4.3 hereto: (i) audited consolidated financial statements of the Company as of and for the periods ended December 31, 2013, 2014 and 2015 (collectively, the “Company Audited Financial Statements”) and (ii) unaudited consolidated financial statements of the Company as of and for the nine (9) month period ended September 30, 2016, subject to normal, recurring year-end adjustments and the absence of notes (the “Company Unaudited Financial Statements” and, together with the Audited Financial Statements, the “Company Financial Statements”). Except as may be set forth in the notes to the Company Financial Statements, the Company Financial Statements fairly present in all material respects the consolidated financial condition and results of operations, as applicable, of the Company as of and for the periods then ended, in each case in conformity with GAAP consistently applied during such periods, except that the Company Unaudited Financial Statements contain estimates of certain accruals, lack footnotes and other presentation items, and are subject to normal immaterial year-end adjustments required by GAAP.
(a) Subject to the introductory paragraph of Section 4.3 above, the books and records of the Company (i) accurately reflect in all material respects all items of income and expense and all material assets and material liabilities of the Company and (ii) are complete and correct in all material respects and do not contain any material inaccuracies or discrepancies.
(b) Subject to the introductory paragraph of Section 4.3 above, the Company has no obligation or liability that would be required to be reflected on, reserved against, or otherwise recorded on a balance sheet prepared in accordance with GAAP, except for (i) the liabilities reflected or reserved against on the balance sheet of the Company, dated December 31, 2015, (ii) liabilities incurred in the Ordinary Course of Business of the Company since December 31, 2015 and (iii) Transaction Expenses.
(c) The accounts receivable, notes receivable and other receivables owed to the Company as of the Closing Date, including, without limitation, those currently outstanding receivables reflected on the Company Financial Statements and all currently outstanding receivables accrued as of the Closing Date, (i) are valid obligations owed to the Company by Third Parties, (ii) result from operations of the Company in the Ordinary Course of Business and (iii) to the Company’s Knowledge, are not disputed or subject to any counterclaim or right of setoff.
4.4 Absence of Certain Changes. Except as set forth on Schedule 4.4, since the date of the Company Audited Financial Statements: (1) the Company has: (x) conducted its respective Business in the Ordinary Course of Business and (y) used its commercially reasonable efforts to preserve the goodwill and organization of its Businesses and its relationships with customers, vendors, Business Employees and other Persons having business relations with the Company; and (2):
(a) no Material Adverse Effect has occurred;
(b) there has been no damage, destruction, or loss, whether or not covered by insurance, of any of the assets of the Company, ordinary wear and tear excepted, in an amount which exceeds $100,000 or which adversely affects the ability of the Company to continue to conduct its Business in all material respects as such Business was conducted during the periods covered by the Company Audited Financial Statements;
| -27- |
(c) no labor dispute or enactment of a state or local Legal Requirement, promulgation of a state or local regulation, or other event or condition has occurred which adversely affects the Company;
(d) there has been no change in the method of accounting or accounting practices of the Company;
(e) there has been no purchase or lease, or commitment for the purchase or lease of, vehicles, equipment, machinery, leasehold improvements, or other capital items not disclosed or reserved for in the Company Financial Statements in an amount which exceeds $100,000, and no sale, transfer, mortgage, pledge, or subjection to any Encumbrance of any kind of, on or affecting any of the assets of the Company having a book value greater than $100,000, except the utilization of inventory and the sale of obsolete assets in the Ordinary Course of Business and the imposition of Permitted Encumbrances;
(f) the Company has not (i) entered into any contract, which, if in effect on the Execution Date, would be a Material Contract, except in the Ordinary Course of Business, (ii) entered into any contract that would limit or otherwise restrict the Company from engaging or competing in any line of business, or that would, after the Execution Date, limit or otherwise restrict the Company from engaging or competing in any line of business or (iii) terminated, canceled, or requested any material change to, ceased performing in any material respect or failed to materially perform under or committed a material default under a Material Contract;
(g) the Company has not incurred any obligation or liability in an amount which exceeds $250,000 (absolute, accrued, contingent or other), whether or not covered by insurance, except in the Ordinary Course of Business;
(h) the Company has not discharged or satisfied any Encumbrance, or paid or satisfied or agreed to extend any obligation or liability in an amount which exceeds $100,000 (absolute, accrued, contingent or otherwise) except in the Ordinary Course of Business;
(i) the Company has not issued any stock, bonds or other securities;
(j) no Action has been commenced or, to the Company’s Knowledge, threatened against or relating to or involving the Company or to any of the material assets of the Company (including, without limitation, any Intellectual Property that is material to or necessary for the Business or operation of the Company) that could reasonably be expected to adversely impact the transactions contemplated by this Agreement;
| -28- |
(k) the Company has not made or changed any Tax election, adopted or changed any Tax accounting method, filed any amended Tax Return, entered into any closing agreement with respect to Taxes of the Company, settled or compromised any Tax claim or assessment of the Company, surrendered any right to a refund with respect to Taxes of the Company, changed an annual reporting period, or consented to any extension or waiver of the limitation period applicable to any Tax claim or assessment of the Company, or took any other similar action relating to the filing of any Tax Return or the payment of any Tax, if such election, adoption, change, amendment, agreement, settlement, surrender, consent or other action would have the effect of increasing the Tax liability of such entity or decreasing any Tax attribute of such entity. The Company has not increased or established any reserve for Taxes or any other liability on its books or otherwise provided therefor;
(l) the Company has not acquired any equity interest in any Person;
(m) (i) except in the Ordinary Course of Business, as reflected and accrued for on the Company Financial Statements, the Company has not amended any Employee Benefit Plan, other than any amendments required by applicable Legal Requirements;
(n) except as provided in Section 3.12, the Company has not made any distribution to Shareholders other than to repurchase the Company’s shares of stock from any Shareholder pursuant to a written agreement in effect prior to the Execution Date if a copy of such agreement has been delivered to Parent on or before the Execution Date;
(o) the Company has not authorized for issuance, issued, sold, granted, pledged or disposed of, or agreed or committed to issue, sell, grant, pledge or dispose of (whether through the issuance or granting of options, warrants, commitments, subscriptions, rights to purchase or otherwise) any stock of any class of the Company or any other securities or equity equivalents;
(p) the Company has not (i) prepaid any loans (if any) from its Shareholders (in their capacity as such), officers or directors or any Person affiliated with any of the foregoing, (ii) made any change in its borrowing arrangements, (iii) waived, released or assigned any rights or claims, except in the Ordinary Course of Business or (iv) incurred any Indebtedness other than under its existing credit facilities;
(q) the Company has not entered into any new line of business or discontinued any line of business;
(r) there has been no failure to maintain, abandonment or other disposition of any assets or properties except in the Ordinary Course of Business;
(s) the Company has not settled or compromised any pending or threatened Action or any Action that involves monitoring or reporting obligations to any Governmental Authority, and except for routine payments made in the Ordinary Course of Business, there has been no payment of any amount to any Governmental Body, incurred, imposed or based upon any Legal Requirement related to the provision of health care items or services by the Company or, to the Company’s Knowledge, any clients of the Company, or environmental protection; and
| -29- |
(t) the Company has not incurred any obligation or liability to any of its officers, directors, Shareholders or Business Employees, or any loans or advances made by the Company to any of its officers, directors, Shareholders or Business Employees.
(a) Except as disclosed on Schedule 4.5, the Company has delivered or made available to Parent an accurate list (attached hereto as Schedule 4.5), and true and complete copies, of all of the material contracts, leases and instruments to which the Company is a party or by which the Company or any of its material assets are bound, including, (i) any contract or agreement with any physician, doctor of osteopathy, doctor of dental surgery, doctor of dental medicine, podiatrist, ophthalmologist, optometrist, chiropractor, nurse anesthesiologist, or other individual health care provider, or with any partnership, professional association, corporation or other entity owned in whole or in part by any such individual health care provider (each a “Provider Contract”); (ii) any loan agreement, promissory note, mortgage, security agreement, guaranty or other documents entered into in connection therewith with respect to any Indebtedness; (iii) any contract or agreement for the maintenance, purchase or sale of equipment or capital assets that involves the expenditure or receipt of more than One Hundred Thousand Dollars ($100,000); (iv) any lease of personal or real property where the Company is lessor or lessee that involves the expenditure or receipt of more than Fifty Thousand Dollars ($50,000); (v) any partnership agreement or joint venture agreement; (vi) any license or other agreement involving the Company’s Intellectual Property that is material and necessary for the operation of the Business; (vii) any agreement with another Person limiting or restricting the ability of the Company to enter into or engage in any market or line of business; (viii) other than in the Ordinary Course of Business, any contracts for the sale of any assets that would be material to the Company taken as a whole or for the grant to any Person of any preferential rights to purchase any of their assets; (ix) any agreement relating to the acquisition by the Company of any material operating business or the material assets or capital stock of any other Person entered into since January 1, 2013; (x) any agreements under which the Company has made material advances or loans to any other Person (which shall not include advances or loans made in the Ordinary Course of Business); (xi) any material settlement since January 1, 2013 or similar contract resolving any litigation against or by the Company that creates reporting obligations to any Governmental Authority; (xii) sales representative or sales or distribution contracts that involve the expenditure or receipt of more than Twenty-Five Thousand Dollars ($25,000); and (xiii) any shareholders or voting agreement or any contract under which the Company has granted any Person any registration rights (collectively, the “Material Contracts”).
(b) With respect to the Material Contracts: (i) Each Material Contract is in full force and effect against the Company, has not been terminated or canceled and no written notice of termination or cancellation has been given or received, (ii) the Company has not been advised in writing that the other party thereto intends to cancel any Material Contract, and (iii) to the Company’s Knowledge, there are no outstanding disputes under any Material Contract.
| -30- |
(a) Except as set forth on Schedule 4.6(a) hereto, there is no Action pending or, to the Company’s Knowledge, threatened, involving the Company or any of its respective officers or directors in their capacities as such. The Company is not subject to any outstanding award, decision, injunction, settlement, sanction, ruling, subpoena, writ, verdict, judgment, order or decree of any Governmental Authority.
(b) There is no Action pending or, to the Company’s Knowledge, threatened, that questions the legality or propriety of the transactions contemplated by this Agreement or seeks to prohibit consummation by the Company of the transactions contemplated hereby or that relates to any of the material assets of the Company.
(c) There is no Action or proceeding pending by any Governmental Authority affecting the Company’s continued ability to provide billing and collection services or other services to participant’s in Medicare, Medicaid, and other governmental payment programs, including managed care programs.
4.7 Business Employees and Employee Relations.
(a) No key Business Employee of the Company has given notice to the Company that such Business Employee intends to cease, or is considering ceasing or reducing, his or her employment upon or after consummation of the transactions contemplated hereby. To the Company’s Knowledge none of the actions described in the preceding sentence is threatened.
(b) The Company is not now, and has not in the last three (3) years been, a party to or otherwise bound by any collective bargaining agreement, contract or other agreement or understanding with a labor union or labor organization. The Company is not now, and has not in the last three (3) years been, the subject of an actual or, to the Company’s Knowledge, threatened (i) labor strike, labor dispute, walkout, work stoppage, slow-down or lockout, (ii) proceeding asserting that the Company has committed an unfair labor practice, (iii) proceeding by which any individual or entity seeks or sought to compel the Company to bargain with any labor union or labor organization or (iv) union organizing campaign involving the Company’s Business Employees.
(c) Except as set forth on Schedule 4.7(c), no employee of the Company, to the Company’s Knowledge, is in violation of any term of any patent disclosure agreement, non-competition agreement, or any other restrictive covenant to a Third Party relating to the right of any such employee to be employed by the Company because of the nature of the Business conducted by the Company or to the use of trade secrets or proprietary information of others. Except as set forth on Schedule 4.7(c), to the Company’s Knowledge, each current employee of the Company has entered into a nondisclosure agreement with the Company. Prior to the date hereof, the Company has heretofore provided Parent with copies of all signed agreements with Business Employees identified in this subparagraph.
| -31- |
(d) (i) The Company is in compliance in all material respects with all Legal Requirements and orders relating to the employment of workers, including all Legal Requirements and orders relating to wages, hours, fair employment practices, discrimination and retaliation, medical or other leave, civil rights, affirmative action, collective bargaining, work authorization and immigration and (ii) since January 1, 2011 there have been no claims, charges, complaints, demands made, or to Company’s Knowledge, threatened to be made, before any Governmental Authority with respect to any alleged violation of any such Legal Requirements. The Company presently is not, nor in the last three (3) years has been, a party to or otherwise bound by any settlement, stipulation or consent decree with, or citation by, any Governmental Authority relating to such Legal Requirements.
(e) The Company has properly completed a U.S. Citizenship and Immigration Services Form I-9 for each Business Employee of the Company and the Company is now, and has been for the past three (3) years, in material compliance with all Legal Requirements governing work authorization in the United States covering the Business Employees of the Company.
(f) Each employee and independent contractor of the Company has been properly classified for all income and employment Tax purposes under the Code and ERISA and has been properly classified as either exempt or nonexempt under the Fair Labor Standards Act and its applicable state Legal Requirements equivalents.
(g) There are (i) to the Company’s Knowledge, no contracts or business relationships that would or could cause the Company to be deemed a federal or state contractor obligated to develop and maintain an affirmative action plan or otherwise comply with affirmative action requirements of Legal Requirements and (ii) within the past five (5) years, no discrimination claim, show cause notice, conciliation proceeding, sanction or debarment proceeding has been filed or is pending or is, to the Company’s Knowledge, threatened with the Office of Federal Contract Compliance Programs or any other federal agency or any comparable state or foreign agency or court and there have been no desk audits or on-site reviews pending or scheduled.
(h) The Company has not (i) effectuated a “plant closing” (as defined in the Worker Adjustment and Retraining Notification Act (the “WARN Act”)) affecting any site of employment or one or more facilities or operating units within any site of employment or facility of the Company, (ii) effectuated a “mass layoff” (as defined in the WARN Act) affecting any site of employment or facility of Company or (iii) engaged in layoffs or employment terminations sufficient in number to trigger application of any similar Legal Requirements. The Company has not suffered an “employment loss” (as defined in the WARN Act) more recently than six (6) months prior to the date hereof.
(i) Except to the extent accrued in the Company Financial Statements, no present or former employee of the Company has or will have as a result of the consummation of the transactions contemplated by this Agreement any claim against the Company (except as specifically set forth in this Agreement), on the account of or for (1) overtime pay for any period on or before the Closing Date, (2) wages, salary, bonuses or amounts due under any Employee Benefit Plan or Other Plan, (3) severance pay or claim for unlawful discharge, (4) workers compensation or (5) unemployment claims.
| -32- |
(a) Schedule 4.8(a) lists each Employee Benefit Plan and Other Plan.
(b) Each Employee Benefit Plan (and related trust, insurance contract or fund) under which any Business Employees of the Company have been covered has complied and currently complies in all material respects with applicable Legal Requirements (including applicable provisions of ERISA and the Code), and all required reports and descriptions (including Form 5500 Annual Reports, Summary Annual Reports, PBGC-1s and Summary Plan Descriptions) have been filed or distributed appropriately with respect to each Employee Benefit Plan. All Employee Benefit Plans and Other Plans have been maintained and administered in all material respects in accordance with their terms and the Company has timely made all required contributions thereto. Nothing has occurred with respect to the operation of any Employee Benefit Plan and Other Plan that would cause the loss of Tax-qualification or exemption or the imposition of any lien, penalty or Tax under ERISA or the Code, or which would otherwise cause a Material Adverse Effect.
(c) With respect to each Employee Benefit Plan and Other Plan, the Company has provided to Parent, to the extent applicable, a copy of: (i) all plan documents, (ii) written summaries of all unwritten plans, (iii) all related trust agreements, insurance contracts, and third-party administration contracts, (iv) the Form 5500 and any attached financial schedules for the last three plan years, (v) summary plan descriptions, summaries of material modifications/reductions, summary annual reports, annual funding notices, and any prospectuses that describe the Employee Benefit Plan and Other Plan, (vi) the annual financial report, for the last three plan years; (vi) the actuarial reports for the last three plan years, (vii) all employee handbooks and (viii) the most recent IRS determination letter or opinion letter for any plan intended to meet the qualification requirements of Section 401(a) of the Code.
(d) No Employee Benefit Plan or Other Plan is subject to Title IV of ERISA and the Company has never maintained an Employee Benefit Plan or Other Plan that was subject to Title IV of ERISA.
(e) No act or omission has occurred and no condition exists with respect to any Employee Benefit Plan or Other Plan that would subject Parent to any: (i) fine, penalty, Tax, or liability of any kind imposed under ERISA, the Code, or other applicable Legal Requirements, or (ii) liability for any such penalty, Tax, or liability under any contractual indemnification or contribution obligation protecting any fiduciary, insurer, or service provider with respect to any Employee Benefit Plan or Other Plan.
(f) No Company employee currently participates in or has participated in the last six years in a Multiemployer Plan or in an Employee Benefit Plan that has two or more contributing sponsors at least two of which are not under common control within the meaning of Section 4063 of ERISA. The Company has not incurred or is expected to incur any “withdrawal liability” within the meaning of Section 4201 of ERISA that has not been satisfied in full.
| -33- |
(g) No employee, consultant, director or former employee (or beneficiary of any of the foregoing) of the Company is entitled to receive any health or disability insurance benefits (whether or not insured) beyond retirement or other termination of employment, other than group health plan continuation coverage as required under Section 601 et seq. of ERISA or Section 4980B of the Code.
(h) There are no pending or, to the Company’s Knowledge, threatened claims (other than routine benefit claims), actions, proceedings, audits, investigations, or lawsuits that have been asserted or instituted by, against, or relating to, any Employee Benefit Plan or Other Plan, nor are there any inquiries or investigations by any governmental authority against or involving any Employee Benefit Plan or Other Plan or asserting claims under or against any Employee Benefit Plan or Other Plan.
(i) Each Employee Benefit Plan that is intended to meet the qualification requirements under Section 401(a) of the Code is covered by a favorable determination or opinion letter issued by the IRS with respect to its tax-qualified status and the Tax-exempt status of its accompanying trust under Section 501(a) of the Code, and, to the Company’s Knowledge, nothing has occurred, including the adoption of or failure to adopt any plan amendment, which could reasonably be expected to adversely affect its Tax-qualification or the Tax-exempt status of its accompanying trust.
(j) Each Employee Benefit Plan and Other Plan and its related documentation or agreement, summary plan description or other written communication distributed generally to Business Employees by its terms expressly reserves the right to amend and terminate such Employee Benefit Plan and Other Plan, and each Employee Benefit Plan and Other Plan may be terminated without liability to the Company, except for vested benefits accrued through the date of termination and the administrative and professional costs incurred in such transaction.
(k) No Employee Benefit Plan is funded by, associated with, or related to a “voluntary employee’s beneficiary association” within the meaning of Section 501(c)(9) of the Code.
(l) Each Employee Benefit Plan and Other Plan or other agreement or arrangement that is a “non-qualified deferred compensation plan” (as such term is defined in Section 409A(d)(1) of the Code), has been maintained, in form and operation in compliance with the requirements of Section 409A of the Code and applicable guidance issued thereunder, and no Tax liabilities have arisen and are currently unpaid in relation to a violation of any applicable Employee Benefit Plan or Other Plan of Section 409A of the Code, nor is any Tax liability expected to arise under Section 409A of the Code in connection with any payment as a result of the transactions contemplated by this Agreement. The Company has no obligation to gross-up or indemnify any individual with respect to any Tax liability under Section 409A of the Code.
| -34- |
(m) There have been no non-exempt “prohibited transactions” within the meaning of Section 4975 of the Code or Part 4 of Subtitle B of Title I of ERISA in connection with any of the Employee Benefit Plans.
(a) The Company has filed all material Tax Returns required to be filed by it, all such Tax Returns are complete and accurate in all material respects, and the Company has paid or made provision in the Company Financial Statements for the payment of all Taxes due and owing by the Company (whether or not shown on a Tax Return); no claim has ever been made by a Governmental Authority in a jurisdiction where the Company does not file Tax Returns that it is or may be subject to Tax by that jurisdiction; and there are no Encumbrances on any of the Company’s assets that arose in connection with any failure (or alleged failure) to pay any Tax.
(b) The Company has withheld and paid all Taxes required to have been withheld and paid in connection with any amounts paid or owing to Business Employees, independent contractors, creditors, Shareholders or other Persons for which withholding or payment is required by any Legal Requirement.
(c) To the Company’s Knowledge, no Governmental Authority intends to assess any additional Taxes for any period for which Tax Returns have been filed. There is no dispute or claim concerning any Tax liability of the Company either claimed or raised by any Governmental Authority in writing, or as to which the Company has notice or knowledge based upon personal contact with any agent of such authority relating to the Company.
(d) The Company has not waived any statute of limitations in respect of Taxes or agreed to any extension of time with respect to a Tax claim or assessment.
(e) The Company is not a party to or bound by any Tax allocation or sharing agreement (other than commercial agreements entered into in the Ordinary Course of Business not primarily related to Taxes). The Company (i) has not been a member of an affiliated group filing a consolidated federal income Tax Return or any similar group for state, local or foreign income Tax purposes (other than a group the common parent of which was the Company) or (ii) has any liability for the Taxes of any Person under Treasury Regulations Section 1.1502-6 (or any similar state, local or foreign Legal Requirement), as a transferee or successor, by contract or otherwise.
(f) The Company is not required to include any item of income in, or exclude any item of deduction from, taxable income for any taxable year or period (or portion thereof) ending after the Closing Date (i) under Section 481 of the Code (or any similar state, local or foreign Legal Requirement) as a result of a change in method of accounting or use of an improper method of accounting, for a taxable year or period that ends on or before the Closing Date, (ii) pursuant to a “closing agreement” as defined in Section 7121 of the Code (or any similar state, local or foreign Legal Requirement) executed on or before the Closing Date, (iii) as a result of the installment method of accounting, the completed contract method of accounting, or the cash method of accounting with respect to a transaction that occurred before the Closing, (iv) as a result of any prepaid amount received on or before the Closing or (v) pursuant to an election under Section 108(i) of the Code.
| -35- |
(g) The Company has not consummated, or participated in, and is not currently participating in, any transaction which is or was a “tax shelter” transaction as defined in Section 6662, 6011, 6111 or 6112 of the Code or applicable Treasury Regulations. The Company has not entered into any “reportable transaction” as defined in Section 6707A(c)(1) of the Code and Treasury Regulations Section 1.6011-4(b).
(h) The Company has not distributed the stock of another Person or has had its stock distributed by another Person in a transaction that was purported or intended to be governed in whole or in part by Section 355 or 361 of the Code.
4.10 Solvency. The Company is not insolvent and will not be rendered insolvent as a result of any of the transactions contemplated by this Agreement. For purposes hereof, the term “solvency” means, that: (1) the fair salable value of the tangible assets of the Company is in excess of the total amount of its liabilities (including for purposes of this definition all liabilities, whether or not reflected on a balance sheet prepared in accordance with GAAP, and whether direct or indirect, fixed or contingent, secured or unsecured, and disputed or undisputed); (2) the Company is able to pay its debts or obligations in the Ordinary Course of Business as they mature; and (3) the Company has capital sufficient to carry on its Business.
4.11 Brokers and Finders. Other than the Company’s engagement of Vantage Point Advisors for financial advisory services, none of the Company or any of its Affiliates, or any officer, trustee, director, employee or agent thereof, has engaged any finder or broker in connection with the transactions contemplated hereunder.
4.12 Sufficiency of Assets. The Company has sufficient assets to operate the Business as conducted on the Execution Date and the Closing Date.
| -36- |
4.13 Equity Interests. Except pursuant to this Agreement and as set forth on Schedule 4.13 attached hereto, there are no outstanding or authorized options, warrants, calls, purchase rights, subscription rights, convertible securities, conversion rights, exchange rights, or other rights, contracts or commitments that require the Company to issue, sell, or otherwise cause to become outstanding any of its equity interests or sell substantially all of its assets, or to effect any merger, consolidation, or other reorganization to enter into any agreements with respect thereto. There is no outstanding or authorized stock or equity appreciation, phantom stock or equity, profit participation, or similar rights with respect to the Company. There are no voting rights, proxies, or other agreements or understandings with respect to any of the voting of the equity interests of the Company, other than as set forth in a Voting Trust Agreement effective as of July 1, 2015 by and among certain Shareholders of the Company (the “Company Voting Trust Agreement”). Other than as set forth in the Company Voting Trust Agreement and Company Shareholders’ Agreement by and among the Shareholders and the Company (the “Company Shareholders’ Agreement”), there are no outstanding contractual obligations of the Company to repurchase, redeem or otherwise acquire any of its equity interests and no Person has any right of first refusal, preemptive right, subscription right or similar right with respect to any equity interests of the Company. The issuance and sale of all of the Company Shares has been in full compliance with all applicable securities laws. All of the Company Shares are duly authorized, validly issued, fully paid and nonassessable. The authorized number of shares of capital stock of the Company is 900,000,000 shares of Common Stock, of which 396,858,568 shares of Common Stock are issued and outstanding and owned of record by the Shareholders as of the Effective Date in the amounts set forth in Schedule 4.13. The Company Shares were issued in accordance with the Company’s articles of incorporation and bylaws in effect at such time and are owned beneficially and of record by the Shareholders, free and clear of all Encumbrances, and constitute the only issued and outstanding capital stock of the Company. Schedule 4.13 attached hereto (a) is a complete and accurate list of the names of the Shareholders of record of the Company and, with respect to any such Shareholders that are entities, the individuals who are the beneficial owners of such entities and (b) sets forth the number and type of Company Shares of the Company Common Stock owned by each such Shareholder. To the Company’s Knowledge, no physician who is currently a director or officer with the Company has been denied privileges or otherwise been suspended or excluded from providing services under any of the Plan Contracts or otherwise had his or her ability to provide services under any of the Plan Contracts limited, nor has any such physician been suspended, debarred or excluded from participation in the Medicare, Medi-Cal or other federal or state program by the U.S. Department of Health and Human Services, Office of the Inspector General or the U.S. General Services Administration or any other Governmental Authority.
4.14 Legal and Regulatory Compliance.
(a) The Company is, and has been, in compliance in all material respects with all Legal Requirements that apply to the Company, and the Company has timely filed all reports, data and other information required to be filed with Governmental Authorities. The Company has not received written notice or communication from any Person of any inquiry, proceeding or investigation by Governmental Authorities alleging or based upon a violation of any Legal Requirements by Company or that involves services furnished or data submitted by Company.
| -37- |
(b) No Governmental Authority or other Person has conducted, or has given the Company any notice or communication that it intends to conduct, any audit or other review of the Company’s services to any of its clients with regard to such client’s participation in, provision of services under, or submission of data in connection with the Medicare or Medi-Cal programs, and no such audit or review would reasonably be expected to result in any liability to the Company for any reimbursement, penalty or interest with respect to payments received by the Company. To the Company’s Knowledge, other than normal claims disputes, none of the Company’s clients has any reimbursement or payment rate appeals, disputes or contested positions currently pending before any Governmental Authority or with any other third-party payor. The Company has used reasonable efforts to confirm that the clients to which it or its Affiliates provides services under Material Contracts have at all times been in compliance with the financial solvency and other applicable requirements of the Knox-Keene Act and its implementing regulations. The Company has not on behalf of any of its clients submitted any false or fraudulent claim to any Third Party and has not received any notice from any Third Party for any allegation of a billing mistake, overpayment claim, false claim or fraud by the Company. All billing practices of the Company have been true, fair and correct and in compliance with all applicable federal and state Legal Requirements, and the Company has not billed for or received any payment or reimbursement in excess of amounts permitted by applicable federal and state Legal Requirements. The Company has not knowingly or willfully solicited, received, paid or offered to pay any remuneration, directly or indirectly, overtly or covertly, in cash or in kind, for the purpose of making or receiving any referral, that violated any applicable federal or state self-referral or anti-kickback law (including without limitation 42 U.S.C. § 1320a-7b(b)), rule, regulation, and Governmental Authority instructions and guidance. Except as set forth on Schedule 4.14, the Company has complied with all applicable security and privacy standards regarding protected health information under the Health Insurance Portability and Accountability Act of 1996, as amended (“HIPAA”) and all applicable state data privacy and security laws with respect to the business operations of the Company. Except as set forth on Schedule 4.14, the Business and operations of the Company has been and is being conducted in compliance with all applicable federal and state licensing and approval requirements of all Governmental Authorities. The Company has not been subject to a corporate integrity agreement, deferred prosecution agreement, consent decree or settlement agreement with or sanction by any Governmental Authority. If required consents timely are obtained and required notices timely are given, the consummation of the transactions contemplated under this Agreement will not adversely affect the reimbursement of the Company’s clients by any third party payor.
(c) The Company has at all times operated in compliance with the federal antitrust laws and guidance from the federal antitrust enforcement agencies (the Department of Justice (“DOJ”) and the Federal Trade Commission (“FTC” and, collectively with the DOJ, the “Antitrust Agencies”). The Company has not negotiated or entered into any contract with a third-party payor on behalf of independent, competing physicians except in compliance with the antitrust laws and guidance from the Antitrust Agencies. The Company has not received any written notice or communication, determination letter, business review letter or advisory opinion from, or entered into any consent decree or settlement agreement with, any third-party payor, the Antitrust Agencies or the State of California Office of the Attorney General (“AG”), and neither of the Antitrust Agencies nor the AG has or is investigating Company’s compliance with federal and/or state antitrust laws, regarding, without limitation, the Company’s ability under federal and/or state antitrust laws to negotiate with third-party payors on behalf of independent, competing providers.
4.15 Permits and Licenses. The Company has all permits, licenses, registrations, certifications and approvals that are necessary to enable the Company to carry on its Business. Schedule 4.15 attached hereto lists all of the Permits and Licenses of the Company. All Permits and Licenses are valid and in full force and effect in all respects, and no violations of any such Permits and Licenses have occurred or have been alleged in writing to have occurred, and no restrictions exist with respect to any such Permits and Licenses. There are no investigations or proceedings pending or, to the Company’s Knowledge, threatened that would have the effect of terminating, revoking, limiting, suspending, restricting, impairing or otherwise affecting the transfer or renewal of any of the Permits and Licenses. The Company has not received written notice of any Action pending or recommended by any Governmental Authority to revoke, withdraw or suspend any of the Permits and Licenses.
| -38- |
(a) The Company has good and marketable title to, a valid leasehold interest in, or has the valid and enforceable right to use, all of the assets that are material to the operation of the Business, free and clear of any and all Encumbrances. Each such asset has been maintained in accordance with normal industry practice, is in good operating condition and repair (subject to normal wear and tear) and is suitable for the purposes for which it presently is used;
(b) All equipment that is necessary for the operation of the Company (the “Equipment”) has been maintained in accordance with normal industry practice, is in good operating condition and repair (subject to normal wear and tear) and is suitable for the purposes for which it presently is used in the Business.
(c) Without limiting the generality of Section 4.16(a) above, the Company has the valid and enforceable right (whether based in ownership, contract or otherwise) to install and use all computer software (including computerized databases) as presently installed or used by the Company in connection with the operation of the Business.
4.17 Financing Statements; Indebtedness. Except for Permitted Encumbrances, no financing statements under the Uniform Commercial Code that name the Company as debtor or lessee have been filed in California or in any other jurisdiction to reflect a security interest in its assets, except financing statements, if any, no longer in effect. Except as set forth on Schedule 4.17, the Company (a) has no Indebtedness, (b) is not subject to any obligation or requirement to provide funds to or make any investment (in the form of a loan, capital contribution or otherwise) in any other Person or (c) has no letters of credit outstanding.
(a) The Company has no ownership, leasehold or other interest in any real property other than a Real Property Lease and the real property and improvements thereon subject to a Real Property Lease comply in all material respects with all Legal Requirements. Schedule 4.18(a) lists each parcel of real property that is leased by the Company as lessee (identified by address).
(b) The Company holds a valid leasehold interest in each parcel of real property listed on Schedule 4.18(a) pursuant to the leases listed on Schedule 4.18(b) (the “Real Property Leases”). A true and complete copy of each Real Property Lease, including any amendments, schedules and exhibits, has been made available to Parent. Each Real Property Lease is valid and binding and has not been amended, modified or assigned, except as otherwise set forth on Schedule 4.18(b). Schedule 4.18(a) describes all real property leased, occupied or otherwise used by the Company. There are no defaults, defenses, offsets or claims by the Company or, to the Company’s Knowledge, by any landlord under any of the Real Property Leases or other arrangements by which the Company leases, occupies or otherwise uses any real property.
| -39- |
(c) There is no proceeding in progress, pending or, to the Company’s Knowledge, threatened against the Company that would reasonably be expected to interfere with the quiet enjoyment by the Company of any parcel of the Real Property that is leased by the Company as lessee.
4.19 Related-Party Transactions. Except as set forth on Schedule 4.19, no current or former officer, director, employee, Shareholder or Affiliate of the Company (i) has any material interest in or owns any property or right used in the conduct of the Business, (ii) is presently, or during the last 12 months has been, a party to any material transaction with Company or (iii) is the direct or indirect owner of an interest in any Person that is a present competitor, supplier or customer of the Business (other than non-affiliated holdings in publicly held companies).
(a) All policies or binders of fire, liability, product liability, worker’s compensation, vehicular, life, fiduciary liability, fidelity bond, directors’ and officers’ liability, malpractice liability, theft, other forms of property and casualty insurance and other insurance held by or on behalf of the Company are listed and described on Schedule 4.20(a), are valid and enforceable in accordance with their terms, and are in full force and effect. Schedule 4.20(a) indicates, for each such policy, whether it provides coverage on a “claims made” or “occurrence” basis. All such policies (i) are for such amounts as are sufficient for all Legal Requirements and all contracts to which the Company is a party or by which the Company is bound and (ii) are in such amounts, with such deductibles and against such risks and losses, as are reasonable for the businesses, assets and properties of the Company. Schedule 4.20(a) lists in respect of each such policy, the policy name, policy number, carrier, term, type and amount of coverage and annual premium, whether the policies may be terminated upon consummation of the transactions contemplated hereby and if and to what extent events being notified to the insurer after the Closing Date are generally excluded from the scope of the respective policy. All premiums on all such policies have been paid to date and the Company has complied with all conditions of such policies. The Company is not in default with respect to its obligations under any of such insurance policies, nor has the Company received any notification of cancellation of any such insurance policies.
(b) Except as set forth on Schedule 4.20(b) no insurance carrier has denied coverage for any claim asserted by the Company during the twelve (12) month period preceding the date hereof, nor has any insurance carrier declined to provide any coverage to the Company during the twelve (12) month period preceding the date hereof. Schedule 4.20(b) hereto sets forth, by year, for the current policy year and each of the two (2) preceding policy years: (i) a summary of the loss experience under each policy of insurance; and (ii) a statement describing each claim under a policy of insurance (including (A) the name of the claimant, (B) a description of the policy by insurer, type of insurance and period of coverage and (C) the amount and brief description of the claims). Except as set forth on Schedule 4.20(b) there are no pending claims under any such policies, and there are no claims under such policies as to which the insurers have denied liability.
| -40- |
(c) Except as set forth on Schedule 4.20(c), no event relating to the Company has occurred which could reasonably be expected to result in a retroactive upward adjustment in premiums under any such insurance policies or which could reasonably be expected to result in a prospective upward adjustment in such premiums. Excluding insurance policies that have expired and been replaced in the Ordinary Course of Business, no insurance policy has been cancelled within the last two (2) years and, to the Company’s Knowledge, no threat has been made to cancel any insurance policy of the Company during such period. Except as noted on Schedule 4.20(c), all such insurance will remain in full force and effect immediately following the consummation of the transactions contemplated hereby. No event has occurred, including the failure by the Company to give any notice or information or the Company giving any inaccurate or erroneous notice or information, which limits or impairs the rights of the Company under any such insurance policies.
4.21 Intangible Personal Property; Software.
(a) Schedule 4.21(a) is a true and complete list of each patent, copyright, trademark, service mark, trade name or other item of Intellectual Property registered by the Company with any Governmental Body.
(b) The Company owns, or holds adequate licenses or other rights to use, all Intellectual Property used by the Company in connection with its operations. No Actions have been instituted, are pending or, to the Company’s Knowledge, are threatened which challenge the validity of the ownership or use by the Company of any Intellectual Property that it has used.
(c) The Company has not received any written notice of any claim, and has no other reasonable grounds to believe, that any Intellectual Property that it has used is infringing any patent, trade name, trademark, service mark, copyright, trade secret, or other Intellectual Property belonging to any other Person.
(d) Schedule 4.21(d) sets forth a list of all computer software programs, computer databases and related documentation and materials that are used by the Company in connection with its Business operations other than commercial off-the-shelf software programs, as well as those subject only to “shrink wrap,” “click through” and/or “click wrap” licenses. The Company either owns such listed software or holds a valid license to use such software and the use by the Company of such listed software that is proprietary to the Company does not conflict with, misappropriate or infringe upon the rights or ownership interests of any other Person.
4.22 Environmental. Except as set forth in Schedule 4.22:
(a) The Company is in compliance in all material respects with, and for the past ten (10) years has been in compliance in all material respects with all applicable Environmental Legal Requirements. No change in facts or circumstances reported or assumed in the applications for or the granting of the Environmental Permits exists. There are no proceedings pending or, to the Company’s Knowledge, threatened which would jeopardize the validity of any of the Environmental Permits.
| -41- |
(b) There are no Environmental Claims pending or, to the Company’s Knowledge, threatened against the Company, the Real Property or any Person whose liability for Environmental Claims, the Company may have assumed contractually or by operation of law and, there are no circumstances that can reasonably be expected to form the basis of any such Environmental Claim.
(c) (i) None of the Company or any of its respective predecessors or, to the Company’s Knowledge, Affiliates, has treated, stored, disposed of, arranged for or permitted the disposal of, transported, handled, or released any substance, including without limitation any Hazardous Materials, or owned or operated such Real Property in such manner as have given or would give rise to any liabilities (contingent or otherwise) or investigative, corrective or remedial obligations, pursuant to CERCLA or any other Environmental Legal Requirements; (ii) there are no underground or above ground storage tanks or any septic tanks, pits, sumps or lagoons at the Real Property; (iii) there is no asbestos or asbestos-containing material located at or on the Real Property; (iv) there is not constructed, placed, deposited, Released, stored, disposed, leaching nor located on the Real Property any polychlorinated biphenyls; and (v) no Environmental Lien or land use limitation has attached to the Real Property or any other property now or formerly operated or used in connection with the Business or the Company’s assets or otherwise by the Company or its predecessors or, to the Company’s Knowledge, Affiliates.
(d) There is no Environmental Condition at, under, in the vicinity of or emanating from, the Real Property, or during the period of the Company’s ownership, lease, use or occupancy thereof, at, under, in the vicinity of or emanating from any property formerly owned, leased, used or occupied by the Company.
(e) The Company has not entered into any consent order, consent decree, settlement agreement or other similar agreement with any Governmental Authority that imposes ongoing or outstanding obligations under Environmental Legal Requirements on the Company, other than the Environmental Permits.
(f) The Company has not assumed by contract any liability, including without limitation any obligation for corrective or Remedial Action, of any other Person relating to Environmental Legal Requirements.
(g) Neither the Real Property nor any other property operated or used in connection with the Company’s Business and/or assets or otherwise by the Company, is listed or proposed for listing on the National Priorities List pursuant to CERCLA, or listed on the Comprehensive Environmental Response Compensation Liability Information System List, or any similar state list of sites, and no condition at such properties exists that, if known to a Governmental Authority, would qualify such property for inclusion on any such list.
| -42- |
(h) The Company has provided Parent with copies of any environmental permits, environmental assessments, remedial investigation reports, remedial action reports, audit reports or other similar studies or analyses relating to the Business, the Real Property and the Company.
4.23 Books and Records. The minute books, stock record books and other books and records of the Company, all of which have been made available to Parent, are complete and correct and have been maintained in accordance with sound business practices and applicable Legal Requirements. The minute books of the Company contain accurate and complete records of all meetings, and actions taken by written consent of, the Shareholders, the Company Board and any committees of the Company Board, and no meeting, or action taken by written consent, of any such Shareholders, Company Board or committee has been held for which minutes have not been prepared and are not contained in such minute books. At the Closing, all of those books and records will be in the possession of the Company.
4.24 Disclosure. No representation or warranty of the Company in this Agreement and no information contained in the Disclosure Schedule contains or will contain any untrue statement of a material fact or omits or will omit to state a material fact required to make the statements herein or therein, in light of the circumstances under which they were made, not misleading. The Company has delivered or caused to be delivered to Parent true, correct and complete copies of all documents, and any and all amendments to any such documents, referred to in this Agreement or in the Disclosure Schedule.
4.25 Accredited Investor. To the Company’s Knowledge, including based upon the shareholder representations made to the Company set forth in subscription agreements executed by each Shareholder, each Shareholder is an accredited investor as defined in Rule 501(a) of Regulation D promulgated under the Securities Act.
ARTICLE
V
REPRESENTATIONS AND WARRANTIES OF PARENT AND MERGER SUB
Except as set forth in the Disclosure Schedule dated as of the date hereof and delivered by Parent to the Company concurrently with or prior to the execution and delivery of this Agreement, as an inducement to the Company to enter into this Agreement and to consummate the transactions contemplated by this Agreement, Parent and Merger Sub jointly and severally make the following representations and warranties to the Company of the Execution Date and the Closing Date:
5.1 Authority of Parent; No Conflicts. This Agreement constitutes a valid and binding agreement by each of Parent and Merger Sub, enforceable in accordance with its terms, and, except as set forth on Schedule 5.1, neither the execution and delivery of this Agreement nor the consummation of the transactions contemplated hereby nor compliance with any of the provisions hereof will:
(a) conflict with, or result in, a breach of Parent’s or Merger Sub’s corporate or governing documents, as applicable;
| -43- |
(b) violate any applicable statute, Legal Requirement, rule or regulation or any other writ, injunction or decree of any court or Governmental Authority;
(c) violate or conflict with or constitute a default under (or give rise to any right of termination, cancellation or acceleration under, whether after the giving of notice, lapse of time, or both) the terms or conditions or provisions of any note, instrument, bond, lease, mortgage, obligation, Plan Contract or other agreement, or understanding, arrangement or restriction of any kind to which Parent, or in the case of Plan Contracts, any of Parent’s clients, is a party or by which Parent, Merger Sub or any of their respective assets or properties may be bound; or
(d) require the consent or approval by or notice to any Governmental Authority or other Third Party beyond those already obtained prior to the date hereof, including consents for any change of control of Parent, pursuant to or as a result of the transactions contemplated under this Agreement and for the continuity of Plan Contracts and reimbursement under those contracts.
5.2 Organization and Power and Authority of Parent. Parent is a corporation duly organized, validly existing, and in good standing under the laws of the State of Delaware, and has the right, power, legal capacity and authority to enter into and perform its obligations under this Agreement and the other Transaction Documents to which it is a party in accordance with its terms subject to General Enforceability Exceptions. Parent has all requisite corporate power and authority to own, operate and lease its respective properties and carry on its Business as currently conducted. Parent is qualified to do business as a foreign corporation under the laws of the State of California and each other jurisdiction where failure to so qualify would have a Material Adverse Effect. The copies of the articles of incorporation, bylaws and other organizational and governing instruments for Parent, each as amended to date and made available to the Company’s counsel, are complete and correct, and no amendments thereto are pending other than as contemplated hereby. Other than the Parent Shareholder Approval that will occur pursuant to Section 3.11 of this Agreement, all action on the part of Parent necessary for the authorization, execution, delivery and performance of this Agreement and the other Transaction Documents to which it is a party and the consummation of the transactions contemplated hereby and thereby has been taken. The board of directors of Parent has approved the Merger and this Agreement in accordance with the CGCL and all requirements of Parent’s organizational and governing documents. Except as set forth on Exhibit 21.1 to Parent Annual Report on Form 10-K for the year ended March 31, 2016, Parent does not have any subsidiary, or any equity interest in another Person.
5.3 Organization and Power and Authority of Merger Sub. Merger Sub is a corporation duly organized, validly existing, and in good standing under the laws of the State of California, and has the right, power, legal capacity and authority to enter into and perform its obligations under this Agreement in accordance with its terms subject to General Enforceability Exceptions. No approvals or consents of any Persons are necessary for the execution, delivery and performance of this Agreement by Merger Sub, except as have been obtained on or before the Closing Date. All action on the part of Merger Sub necessary for the authorization, execution, delivery and performance of this Agreement and the consummation of the transactions contemplated hereby has been taken.
| -44- |
5.4 Financial Statements; Accounts Receivable. The following have been prepared from the books and records of Parent and are attached to Schedule 5.4 hereto: (i) audited consolidated financial statements of Parent as of and for the periods ended March 31, 2014, 2015 and 2016 (collectively, the “Parent Audited Financial Statements”) and (ii) unaudited consolidated financial statements of Parent as of and for the six (6) month period ended September 30, 2016, subject to normal, recurring year-end adjustments and the absence of notes (the “Parent Unaudited Financial Statements” and, together with the Parent Audited Financial Statements, the “Parent Financial Statements”). Except as may be set forth in the notes to Parent Financial Statements, Parent Financial Statements fairly present in all material respects the consolidated financial condition and results of operations, as applicable, of Parent as of and for the periods then ended, in each case in conformity with GAAP consistently applied during such periods, except that the Parent Unaudited Financial Statements contain estimates of certain accruals, lack footnotes and other presentation items, and are subject to normal immaterial year-end adjustments required by GAAP.
(a) Subject to the introductory paragraph of Section 5.4 above, the books and records of Parent (i) accurately reflect in all material respects all items of income and expense and all material assets and material liabilities of Parent and (ii) are complete and correct in all material respects and do not contain any material inaccuracies or discrepancies.
(b) Subject to the introductory paragraph of Section 5.4 above, Parent has no obligation or liability that would be required to be reflected on, reserved against, or otherwise recorded on a balance sheet prepared in accordance with GAAP, except for (i) the liabilities reflected or reserved against on the balance sheet of Parent, dated March 31, 2016, (ii) liabilities incurred in the Ordinary Course of Business of Parent since March 31, 2016 and (iii) Transaction Expenses.
(c) The accounts receivable, notes receivable and other receivables owed to Parent as of the Closing Date, including, without limitation, those currently outstanding receivables reflected on Parent Financial Statements and all currently outstanding receivables accrued as of the Closing Date, (i) are valid obligations owed to Parent by Third Parties, (ii) result from operations of Parent in the Ordinary Course of Business and (iii) to Parent’s Knowledge, are not disputed or subject to any counterclaim or right of setoff.
5.5 Absence of Certain Changes. Except as set forth on Schedule 5.5, since the date of the Parent Audited Financial Statements: (1) Parent has: (x) conducted its respective Business in the Ordinary Course of Business and (y) used its commercially reasonable efforts to preserve the goodwill and organization of its Businesses and its relationships with customers, vendors, Business Employees and other Persons having business relations with Parent; and (2):
(a) no Material Adverse Effect has occurred;
(b) there has been no damage, destruction, or loss, whether or not covered by insurance, of any of the assets of Parent, ordinary wear and tear excepted, in an amount which exceeds $100,000 or which adversely affects the ability of Parent to continue to conduct its Business in all material respects as such Business was conducted during the periods covered by the Parent Audited Financial Statements;
| -45- |
(c) no labor dispute or enactment of a state or local Legal Requirement, promulgation of a state or local regulation, or other event or condition has occurred which adversely affects Parent;
(d) there has been no change in the method of accounting or accounting practices of Parent;
(e) there has been no purchase or lease, or commitment for the purchase or lease of, vehicles, equipment, machinery, leasehold improvements, or other capital items not disclosed or reserved for in Parent Financial Statements in an amount which exceeds $100,000, and no sale, transfer, mortgage, pledge, or subjection to any Encumbrance of any kind of, on or affecting any of the assets of Parent having a book value greater than $100,000, except the utilization of inventory and the sale of obsolete assets in the Ordinary Course of Business and the imposition of Permitted Encumbrances;
(f) Parent has made Parent has not (i) entered into any contract, which, if in effect on the Execution Date, would be a Parent Material Contract, except in the Ordinary Course of Business, (ii) entered into any contract that would limit or otherwise restrict Parent from engaging or competing in any line of business, or that would, after the Execution Date, limit or otherwise restrict Parent from engaging or competing in any line of business or (iii) terminated, canceled, or requested any material change to, ceased performing in any material respect or failed to materially perform under or committed a material default under a Parent Material Contract;
(g) Parent has not incurred any obligation or liability in an amount which exceeds $250,000 (absolute, accrued, contingent or other), whether or not covered by insurance, except in the Ordinary Course of Business;
(h) Parent has not discharged or satisfied any Encumbrance, or paid or satisfied or agreed to extend any obligation or liability in an amount which exceeds $100,000 (absolute, accrued, contingent or otherwise) except in the Ordinary Course of Business;
(i) Except as set forth on Schedule 5.5, Parent has not issued any stock, bonds or other securities;
(j) no Action has been commenced or, to Parent’s Knowledge, threatened against or relating to or involving Parent or to any of the material assets of Parent (including, without limitation, any Intellectual Property that is material to or necessary for the Business or operation of Parent) that could reasonably be expected to adversely impact the transactions contemplated by this Agreement;
| -46- |
(k) Parent has not made or changed any Tax election, adopted or changed any Tax accounting method, filed any amended Tax Return, entered into any closing agreement with respect to Taxes of Parent, settled or compromised any Tax claim or assessment of Parent, surrendered any right to a refund with respect to Taxes of Parent, changed an annual reporting period, or consented to any extension or waiver of the limitation period applicable to any Tax claim or assessment of Parent, or took any other similar action relating to the filing of any Tax Return or the payment of any Tax, if such election, adoption, change, amendment, agreement, settlement, surrender, consent or other action would have the effect of increasing the Tax liability of such entity or decreasing any Tax attribute of such entity. Parent has not increased or established any reserve for Taxes or any other liability on its books or otherwise provided therefor;
(l) Parent has not acquired any equity interest in any Person;
(m) except in the Ordinary Course of Business, as reflected and accrued for on Parent Financial Statements, Parent has not amended any Employee Benefit Plan, other than any amendments required by applicable Legal Requirements;
(n) Parent has not made any distribution to shareholders other than to repurchase Parent’s shares of stock from any shareholder pursuant to a written agreement in effect prior to the Execution Date, if a copy of such agreement has been delivered to the Company on or before the Execution Date;
(o) Except as contemplated by this Agreement, Parent has not authorized for issuance, issued, sold, granted, pledged or disposed of, or agreed or committed to issue, sell, grant, pledge or dispose of (whether through the issuance or granting of options, warrants, commitments, subscriptions, rights to purchase or otherwise) any stock of any class of Parent or any other securities or equity equivalents;
(p) Except as set forth on Schedule 5.5, Parent has not (i) prepaid any loans (if any) from its shareholders (in their capacity as such), officers or directors or any Person affiliated with any of the foregoing, (ii) made any change in its borrowing arrangements, (iii) waived, released or assigned any rights or claims, except in the Ordinary Course of Business or (iv) incurred any Indebtedness other than under its existing credit facilities;
(q) Parent has not entered into any new line of business or discontinued any line of business;
(r) there has been no failure to maintain, abandonment or other disposition of any assets or properties except in the Ordinary Course of Business;
(s) Parent has not settled or compromised any pending or threatened Action or any Action that involves monitoring or reporting obligations to any Governmental Authority, and except for routine payments made in the Ordinary Course of Business, there has been no payment of any amount to any Governmental Body, incurred, imposed or based upon any Legal Requirement related to the provision of health care items or services by Parent or, to Parent’s Knowledge, any clients of Parent, or environmental protection; and
| -47- |
(t) Except as set forth on Schedule 5.5, Parent has not incurred any obligation or liability to any of its officers, directors, shareholders or Business Employees, or any loans or advances made by Parent to any of its officers, directors, shareholders or Business Employees.
(a) Except as disclosed on Schedule 5.6, Parent has delivered or made available to the Company an accurate list (attached hereto as Schedule 5.6), and true and complete copies, of all of the material contracts, leases and instruments to which Parent is a party or by which Parent or any of its material assets are bound, including, (i) any Provider Contract; (ii) any loan agreement, promissory note, mortgage, security agreement, guaranty or other documents entered into in connection therewith with respect to any Indebtedness; (iii) any contract or agreement for the maintenance, purchase or sale of equipment or capital assets that involves the expenditure or receipt of more than One Hundred Thousand Dollars ($100,000); (iv) any lease of personal or real property where Parent is lessor or lessee that involves the expenditure or receipt of more than Fifty Thousand Dollars ($50,000); (v) any partnership agreement or joint venture agreement; (vi) any license or other agreement involving Parent’s Intellectual Property that is material and necessary for the operation of the Business; (vii) any agreement with another Person limiting or restricting the ability of Parent to enter into or engage in any market or line of business; (viii) other than in the Ordinary Course of Business, any contracts for the sale of any assets that would be material to Parent taken as a whole or for the grant to any Person of any preferential rights to purchase any of their assets; (ix) any agreement relating to the acquisition by Parent of any material operating business or the material assets or capital stock of any other Person entered into since January 1, 2013; (x) any agreements under which Parent has made material advances or loans to any other Person (which shall not include advances or loans made in the Ordinary Course of Business); (xi) any material settlement since January 1, 2013 or similar contract resolving any litigation against or by Parent that creates reporting obligations to any Governmental Authority; (xii) sales representative or sales or distribution contracts that involve the expenditure or receipt of more than Twenty-Five Thousand Dollars ($25,000); and (xiii) any shareholders or voting agreement or any contract under which Parent has granted any Person any registration rights (collectively, the “Parent Material Contracts”).
(b) With respect to the Parent Material Contracts: (i) Each Parent Material Contract is in full force and effect against Parent, has not been terminated or canceled and no written notice of termination or cancellation has been given or received, (ii) Parent has not been advised in writing that the other party thereto intends to cancel any Parent Material Contract, and (iii) to Parent’s Knowledge, there are no outstanding disputes under any Parent Material Contract.
(a) Except as set forth on Schedule 5.7(a) hereto, there is no Action pending or to Parent’s Knowledge threatened, involving Parent or any of its respective officers or directors in their capacities as such. Except as set forth on Schedule 5.7(a) hereto, Parent is not subject to any outstanding award, decision, injunction, settlement, sanction, ruling, subpoena, writ, verdict, judgment, order or decree of any Governmental Authority.
| -48- |
(b) There is no Action pending or, to Parent’s Knowledge, threatened, that questions the legality or propriety of the transactions contemplated by this Agreement or seeks to prohibit consummation by Parent of the transactions contemplated hereby or that relates to any of the material assets of Parent.
(c) There is no Action or proceeding pending by any Governmental Authority affecting Parent’s continued ability to provide billing and collection services or other services to participant’s in Medicare, Medicaid, and other governmental payment programs, including managed care programs.
5.8 Business Employees and Employee Relations.
(a) No key Business Employee of Parent has given notice to Parent that such Business Employee intends to cease, or is considering ceasing or reducing, his or her employment upon or after consummation of the transactions contemplated hereby. To Parent’s Knowledge none of the actions described in the preceding sentence is threatened.
(b) Parent is not now, and has not in the last three (3) years been, a party to or otherwise bound by any collective bargaining agreement, contract or other agreement or understanding with a labor union or labor organization. Parent is not now, and has not in the last three (3) years been, the subject of an actual or, to Parent’s Knowledge, threatened (i) labor strike, labor dispute, walkout, work stoppage, slow-down or lockout, (ii) proceeding asserting that Parent has committed an unfair labor practice, (iii) proceeding by which any individual or entity seeks or sought to compel Parent to bargain with any labor union or labor organization or (iv) union organizing campaign involving Parent’s Business Employees.
(c) Except as set forth on Schedule 5.8(c), no employee of Parent, to Parent’s Knowledge, is in violation of any term of any patent disclosure agreement, non-competition agreement, or any other restrictive covenant to a Third Party relating to the right of any such employee to be employed by Parent because of the nature of the Business conducted by Parent or to the use of trade secrets or proprietary information of others. Except as set forth on Schedule 5.8(c), to Parent’s Knowledge, each current employee of Parent has entered into a nondisclosure agreement with Parent. Prior to the date hereof, Parent has heretofore provided the Company with copies of all signed agreements with Business Employees identified in this subparagraph.
(d) (i) Parent is in compliance in all material respects with all Legal Requirements and orders relating to the employment of workers, including all Legal Requirements and orders relating to wages, hours, fair employment practices, discrimination and retaliation, medical or other leave, civil rights, affirmative action, collective bargaining, work authorization and immigration and (ii) since January 1, 2011 there have been no claims, charges, complaints, demands made, or to Parent’s Knowledge, threatened to be made, before any Governmental Authority with respect to any alleged violation of any such Legal Requirements. Parent presently is not, nor in the last three (3) years has been, a party to or otherwise bound by any settlement, stipulation or consent decree with, or citation by, any Governmental Authority relating to such Legal Requirements.
| -49- |
(e) Parent has properly completed a U.S. Citizenship and Immigration Services Form I-9 for each Business Employee of Parent and Parent is now, and has been for the past three (3) years, in material compliance with all Legal Requirements governing work authorization in the United States covering the Business Employees of Parent.
(f) Each employee and independent contractor of Parent has been properly classified for all income and employment Tax purposes under the Code and ERISA and has been properly classified as either exempt or nonexempt under the Fair Labor Standards Act and its applicable state Legal Requirements equivalents.
(g) There are (i) to Parent’s Knowledge, no contracts or business relationships that would or could cause Parent to be deemed a federal or state contractor obligated to develop and maintain an affirmative action plan or otherwise comply with affirmative action requirements of Legal Requirements and (ii) within the past five (5) years, no discrimination claim, show cause notice, conciliation proceeding, sanction or debarment proceeding has been filed or is pending or is, to Parent’s Knowledge, threatened with the Office of Federal Contract Compliance Programs or any other federal agency or any comparable state or foreign agency or court and there have been no desk audits or on-site reviews pending or scheduled.
(h) Parent has not (i) effectuated a “plant closing” (as defined in the Worker Adjustment and Retraining Notification Act (the “WARN Act”)) affecting any site of employment or one or more facilities or operating units within any site of employment or facility of Parent, (ii) effectuated a “mass layoff” (as defined in the WARN Act) affecting any site of employment or facility of Parent or (iii) engaged in layoffs or employment terminations sufficient in number to trigger application of any similar Legal Requirements. Parent has not suffered an “employment loss” (as defined in the WARN Act) more recently than six (6) months prior to the date hereof.
(i) Except to the extent accrued in Parent Financial Statements, no present or former employee of Parent has or will have as a result of the consummation of the transactions contemplated by this Agreement any claim against Parent (except as specifically set forth in this Agreement), on the account of or for (1) overtime pay for any period on or before the Closing Date, (2) wages, salary, bonuses or amounts due under any Employee Benefit Plan or Other Plan, (3) severance pay or claim for unlawful discharge, (4) workers compensation or (5) unemployment claims.
(a) Schedule 5.9(a) lists each Employee Benefit Plan and Other Plan.
| -50- |
(b) Each Employee Benefit Plan (and related trust, insurance contract or fund) under which any Business Employees of Parent have been covered has complied and currently complies in all material respects with applicable Legal Requirements (including applicable provisions of ERISA and the Code), and all required reports and descriptions (including Form 5500 Annual Reports, Summary Annual Reports, PBGC-1s and Summary Plan Descriptions) have been filed or distributed appropriately with respect to each Employee Benefit Plan. All Employee Benefit Plans and Other Plans have been maintained and administered in all material respects in accordance with their terms and Parent has timely made all required contributions thereto. Nothing has occurred with respect to the operation of any Employee Benefit Plan and Other Plan that would cause the loss of Tax-qualification or exemption or the imposition of any lien, penalty or Tax under ERISA or the Code, or which would otherwise cause a Material Adverse Effect.
(c) With respect to each Employee Benefit Plan and Other Plan, Parent has provided to Parent, to the extent applicable, a copy of: (i) all plan documents, (ii) written summaries of all unwritten plans, (iii) all related trust agreements, insurance contracts, and third-party administration contracts, (iv) the Form 5500 and any attached financial schedules for the last three plan years, (v) summary plan descriptions, summaries of material modifications/reductions, summary annual reports, annual funding notices, and any prospectuses that describe the Employee Benefit Plan and Other Plan, (vi) the annual financial report, for the last three plan years; (vi) the actuarial reports for the last three plan years, (vii) all employee handbooks and (viii) the most recent IRS determination letter or opinion letter for any plan intended to meet the qualification requirements of Section 401(a) of the Code.
(d) No Employee Benefit Plan or Other Plan is subject to Title IV of ERISA and Parent has never maintained an Employee Benefit Plan or Other Plan that was subject to Title IV of ERISA.
(e) No act or omission has occurred and no condition exists with respect to any Employee Benefit Plan or Other Plan that would subject Parent to any: (i) fine, penalty, Tax, or liability of any kind imposed under ERISA, the Code, or other applicable Legal Requirements, or (ii) liability for any such penalty, Tax, or liability under any contractual indemnification or contribution obligation protecting any fiduciary, insurer, or service provider with respect to any Employee Benefit Plan or Other Plan.
(f) No Parent employee currently participates in or has participated in the last six years in a Multiemployer Plan or in an Employee Benefit Plan that has two or more contributing sponsors at least two of which are not under common control within the meaning of Section 4063 of ERISA. Parent has not incurred or is expected to incur any “withdrawal liability” within the meaning of Section 4201 of ERISA that has not been satisfied in full.
(g) No employee, consultant, director or former employee (or beneficiary of any of the foregoing) of Parent is entitled to receive any health or disability insurance benefits (whether or not insured) beyond retirement or other termination of employment, other than group health plan continuation coverage as required under Section 601 et seq. of ERISA or Section 4980B of the Code.
| -51- |
(h) There are no pending or, to Parent’s Knowledge, threatened claims (other than routine benefit claims), actions, proceedings, audits, investigations, or lawsuits that have been asserted or instituted by, against, or relating to, any Employee Benefit Plan or Other Plan, nor are there any inquiries or investigations by any governmental authority against or involving any Employee Benefit Plan or Other Plan or asserting claims under or against any Employee Benefit Plan or Other Plan.
(i) Each Employee Benefit Plan that is intended to meet the qualification requirements under Section 401(a) of the Code is covered by a favorable determination or opinion letter issued by the IRS with respect to its tax-qualified status and the Tax-exempt status of its accompanying trust under Section 501(a) of the Code, and, to Parent’s Knowledge, nothing has occurred, including the adoption of or failure to adopt any plan amendment, which could reasonably be expected to adversely affect its Tax-qualification or the Tax-exempt status of its accompanying trust.
(j) Each Employee Benefit Plan and Other Plan and its related documentation or agreement, summary plan description or other written communication distributed generally to Business Employees by its terms expressly reserves the right to amend and terminate such Employee Benefit Plan and Other Plan, and each Employee Benefit Plan and Other Plan may be terminated without liability to Parent, except for vested benefits accrued through the date of termination and the administrative and professional costs incurred in such transaction.
(k) No Employee Benefit Plan is funded by, associated with, or related to a “voluntary employee’s beneficiary association” within the meaning of Section 501(c)(9) of the Code.
(l) Each Employee Benefit Plan and Other Plan or other agreement or arrangement that is a “non-qualified deferred compensation plan” (as such term is defined in Section 409A(d)(1) of the Code), has been maintained, in form and operation in compliance with the requirements of Section 409A of the Code and applicable guidance issued thereunder, and no Tax liabilities have arisen and are currently unpaid in relation to a violation of any applicable Employee Benefit Plan or Other Plan of Section 409A of the Code, nor is any Tax liability expected to arise under Section 409A of the Code in connection with any payment as a result of the transactions contemplated by this Agreement. Parent has no obligation to gross-up or indemnify any individual with respect to any Tax liability under Section 409A of the Code.
(m) There have been no non-exempt “prohibited transactions” within the meaning of Section 4975 of the Code or Part 4 of Subtitle B of Title I of ERISA in connection with any of the Employee Benefit Plans.
| -52- |
(a) Parent has filed all material Tax Returns required to be filed by it, all such Tax Returns are complete and accurate in all material respects, and Parent has paid or made provision in Parent Financial Statements for the payment of all Taxes due and owing by Parent (whether or not shown on a Tax Return); no claim has ever been made by a Governmental Authority in a jurisdiction where Parent does not file Tax Returns that it is or may be subject to Tax by that jurisdiction; and there are no Encumbrances on any of Parent’s assets that arose in connection with any failure (or alleged failure) to pay any Tax.
(b) Parent has withheld and paid all Taxes required to have been withheld and paid in connection with any amounts paid or owing to Business Employees, independent contractors, creditors, shareholders or other Persons for which withholding or payment is required by any Legal Requirement.
(c) To Parent’s Knowledge, no Governmental Authority intends to assess any additional Taxes for any period for which Tax Returns have been filed. There is no dispute or claim concerning any Tax liability of Parent either claimed or raised by any Governmental Authority in writing, or as to which Parent has notice or knowledge based upon personal contact with any agent of such authority relating to Parent.
(d) Parent has not waived any statute of limitations in respect of Taxes or agreed to any extension of time with respect to a Tax claim or assessment.
(e) Parent is not a party to or bound by any Tax allocation or sharing agreement (other than commercial agreements entered into in the Ordinary Course of Business not primarily related to Taxes). Parent (i) has not been a member of an affiliated group filing a consolidated federal income Tax Return or any similar group for state, local or foreign income Tax purposes (other than a group the common parent of which was Parent) or (ii) has any liability for the Taxes of any Person under Treasury Regulations Section 1.1502-6 (or any similar state, local or foreign Legal Requirement), as a transferee or successor, by contract or otherwise.
(f) Parent is not required to include any item of income in, or exclude any item of deduction from, taxable income for any taxable year or period (or portion thereof) ending after the Closing Date (i) under Section 481 of the Code (or any similar state, local or foreign Legal Requirement) as a result of a change in method of accounting or use of an improper method of accounting for a taxable year or period that ends on or before the Closing Date, (ii) pursuant to a “closing agreement” as defined in Section 7121 of the Code (or any similar state, local or foreign Legal Requirement) executed on or before the Closing Date, (iii) as a result of the installment method of accounting, the completed contract method of accounting, or the cash method of accounting with respect to a transaction that occurred before the Closing, (iv) as a result of any prepaid amount received on or before the Closing or (v) pursuant to an election under Section 108(i) of the Code.
(g) Parent has not consummated, or participated in, and is not currently participating in, any transaction which is or was a “tax shelter” transaction as defined in Section 6662, 6011, 6111 or 6112 of the Code or applicable Treasury Regulations. Parent has not entered into any “reportable transaction” as defined in Section 6707A(c)(1) of the Code and Treasury Regulations Section 1.6011-4(b).
| -53- |
(h) Parent has not distributed the stock of another Person or has had its stock distributed by another Person in a transaction that was purported or intended to be governed in whole or in part by Section 355 or 361 of the Code
5.11 Solvency. Parent is not insolvent and will not be rendered insolvent as a result of any of the transactions contemplated by this Agreement. For purposes hereof, the term “solvency” means, that: (1) the fair salable value of the tangible assets of Parent is in excess of the total amount of its liabilities (including for purposes of this definition all liabilities, whether or not reflected on a balance sheet prepared in accordance with GAAP, and whether direct or indirect, fixed or contingent, secured or unsecured, and disputed or undisputed); (2) Parent is able to pay its debts or obligations in the Ordinary Course of Business as they mature; and (3) Parent has capital sufficient to carry on its Business.
5.12 Brokers and Finders. Other than Parent’s engagement of Bank of America Merrill Lynch for financial advisory services, none of Parent or any of its Affiliates, or any officer, trustee, director, employee or agent thereof, has engaged any finder or broker in connection with the transactions contemplated hereunder.
5.13 Sufficiency of Assets. Parent has sufficient assets to operate the Business as conducted on the Execution Date and the Closing Date.
5.14 Equity Interests. Except pursuant to this Agreement and as set forth on Schedule 5.14 attached hereto, there are no outstanding or authorized options, warrants, calls, purchase rights, subscription rights, convertible securities, conversion rights, exchange rights, or other rights, contracts or commitments that require Parent and/or Merger Sub to issue, sell, or otherwise cause to become outstanding any of its equity interests or sell substantially all of its assets, or to effect any merger, consolidation, or other reorganization to enter into any agreements with respect thereto. There is no outstanding or authorized stock or equity appreciation, phantom stock or equity, profit participation, or similar rights with respect to Parent and/or Merger Sub. There are no voting rights, proxies, or other agreements or understandings with respect to any of the voting of the equity interests of Parent and/or Merger Sub. There are no outstanding contractual obligations of Parent and/or Merger Sub to repurchase, redeem or otherwise acquire any of its respective equity interests and no Person has any right of first refusal, preemptive right, subscription right or similar right with respect to any equity interests of Parent and/or Merger Sub. The issuance and sale of all of Parent Shares has been in full compliance with all applicable securities laws. All of the shares of Parent and Merger Sub are duly authorized, validly issued, fully paid and nonassessable. The authorized number of shares of capital stock of Parent is 105,000,000, consisting of 100,000,000 shares of Common Stock and 5,000,000 shares of Preferred Stock, of which 6,033,518 shares of Common Stock and 1,666,660 shares of Preferred Stock, respectively, were issued and outstanding as of the date of Parent’s last public filing prior to the Execution Date. The authorized number of shares of capital stock of Merger Sub is 1,000, consisting of 1,000 shares of Common Stock, all of which are issued and outstanding and owned of record by Parent. All of the shares of Parent and Merger Sub were issued in accordance with their respective articles of incorporation and bylaws in effect at such time and are owned beneficially and of record by the respective shareholders of Parent and Merger Sub, free and clear of all Liens, and constitute the only issued and outstanding capital stock of Parent and Merger Sub. To Parent’s Knowledge, no physician who is currently a director or officer of Parent has been suspended, debarred or excluded from participation in the Medicare, Medi-Cal or other federal or state program by the U.S. Department of Health and Human Services, Office of the Inspector General or the U.S. General Services Administration or any other Governmental Authority.
| -54- |
5.15 Legal and Regulatory Compliance.
(a) Parent is, and has been, in compliance in all material respects with all Legal Requirements that apply to Parent, and Parent has timely filed all reports, data and other information required to be filed with Governmental Authorities. Parent has not received written notice or communication from any Person of any inquiry, proceeding or investigation by Governmental Authorities alleging or based upon a violation of any Legal Requirements by Parent or that involves services furnished or data submitted by Parent.
(b) No Governmental Authority or other Person has conducted, or has given Parent any notice or communication that it intends to conduct, any audit or other review of Parent’s services to any of its clients with regard to such client’s participation in, provision of services under, or submission of data in connection with the Medicare or Medi-Cal programs, and no such audit or review would reasonably be expected to result in any liability to Parent for any reimbursement, penalty or interest with respect to payments received by Parent. To Parent’s Knowledge, other than normal claims disputes, none of Parent’s clients has any reimbursement or payment rate appeals, disputes or contested positions currently pending before any Governmental Authority or with any other third-party payor. Parent has used reasonable efforts to confirm that the clients to which it or its Affiliates provides services under Parent Material Contracts have at all times been in compliance with the financial solvency and other applicable requirements of the Knox-Keene Act and its implementing regulations. Parent has not on behalf of any of its clients submitted any false or fraudulent claim to any Third Party and has not received any notice from any Third Party for any allegation of a billing mistake, overpayment claim, false claim or fraud by Parent. All billing practices of Parent have been true, fair and correct and in compliance with all applicable federal and state Legal Requirements, and Parent has not billed for or received any payment or reimbursement in excess of amounts permitted by applicable federal and state Legal Requirements. Parent has not knowingly or willfully solicited, received, paid or offered to pay any remuneration, directly or indirectly, overtly or covertly, in cash or in kind, for the purpose of making or receiving any referral, that violated any applicable federal or state self-referral or anti-kickback law (including without limitation 42 U.S.C. § 1320a-7b(b)), rule, regulation, and Governmental Authority instructions and guidance. Except as set forth on Schedule 5.15, Parent has complied with all applicable security and privacy standards regarding protected health information under HIPAA and all applicable state data privacy and security laws with respect to the business operations of Parent. Except as set forth on Schedule 5.15, the Business and operations of Parent has been and is being conducted in compliance with all applicable federal and state licensing and approval requirements of all Governmental Authorities. Parent has not been subject to a corporate integrity agreement, deferred prosecution agreement, consent decree or settlement agreement with or sanction by any Governmental Authority. If required consents timely are obtained and required notices timely are given, the consummation of the transactions contemplated under this Agreement will not adversely affect the reimbursement of Parent’s clients by any third party payor.
| -55- |
(c) Parent has at all times operated in compliance with the federal antitrust laws and guidance from the federal Antitrust Agencies. Parent has not negotiated or entered into any contract with a third-party payor on behalf of independent, competing physicians except in compliance with the antitrust laws and guidance from the Antitrust Agencies. Parent has not received any written notice or communication, determination letter, business review letter or advisory opinion from, or entered into any consent decree or settlement agreement with, any third-party payor, the Antitrust Agencies or the AG, and neither of the Antitrust Agencies nor the AG has or is investigating Parent’s compliance with federal and/or state antitrust laws, regarding, without limitation, Parent’s ability under federal and/or state antitrust laws to negotiate with third-party payors on behalf of independent, competing providers.
5.16 Permits and Licenses. Parent has all permits, licenses, registrations, certifications and approvals that are necessary to enable Parent to carry on its Business. Schedule 5.16 attached hereto lists all of the Permits and Licenses of Parent. All Permits and Licenses are valid and in full force and effect in all respects, and no violations of any such Permits and Licenses have occurred or have been alleged in writing to have occurred, and no restrictions exist with respect to any such Permits and Licenses. There are no investigations or proceedings pending or, to Parent’s Knowledge, threatened that would have the effect of terminating, revoking, limiting, suspending, restricting, impairing or otherwise affecting the transfer or renewal of any of the Permits and Licenses. Parent has not received written notice of any Action pending or recommended by any Governmental Authority to revoke, withdraw or suspend any of the Permits and Licenses.
(a) Parent has good and marketable title to, a valid leasehold interest in, or has the valid and enforceable right to use, all of the assets that are material to the operation of the Business, free and clear of any and all Encumbrances. Each such asset has been maintained in accordance with normal industry practice, is in good operating condition and repair (subject to normal wear and tear) and is suitable for the purposes for which it presently is used;
(b) All equipment that is necessary for the operation of Parent has been maintained in accordance with normal industry practice, is in good operating condition and repair (subject to normal wear and tear) and is suitable for the purposes for which it presently is used in the Business.
(c) Without limiting the generality of Section 5.17(a) above, Parent has the valid and enforceable right (whether based in ownership, contract or otherwise) to install and use all computer software (including computerized databases) as presently installed or used by Parent in connection with the operation of the Business.
| -56- |
5.18 Financing Statements; Indebtedness. Except for Permitted Encumbrances, and except in connection with financing arrangements set forth on Schedule 5.18, no financing statements under the Uniform Commercial Code that name Parent as debtor or lessee have been filed in California or in any other jurisdiction to reflect a security interest in its assets, except financing statements, if any, no longer in effect. Except as set forth on Schedule 5.18, Parent (a) Indebtedness does not exceed $1,000,000 in the aggregate, (b) is not subject to any obligation or requirement to provide funds to or make any investment (in the form of a loan, capital contribution or otherwise) in any other Person or (c) has no letters of credit outstanding.
(a) Except as set forth on Schedule 5.19(a), Parent has no ownership, leasehold or other interest in any real property other than a Real Property Lease and the real property and improvements thereon subject to a Real Property Lease comply in all material respects with all Legal Requirements.
(b) Parent holds a valid leasehold interest in each parcel of Real Property set forth on Schedule 5.19(b) (the “Parent Real Property Leases”). A true and complete copy of each Real Property Lease, including any amendments, schedules and exhibits, has been made available to the Company. Except as set forth on Schedule 5.19(b), each Parent Real Property Lease is valid and binding and has not been amended, modified or assigned. There are no defaults, defenses, offsets or claims by Parent or, to Parent’s Knowledge, by any landlord under any of the Parent Real Property Leases or other arrangements by which Parent leases, occupies or otherwise uses any real property.
(c) Except as set forth on Schedule 5.19(c), there is no proceeding in progress, pending or, to Parent’s Knowledge, threatened against Parent that would reasonably be expected to interfere with the quiet enjoyment by Parent of any parcel of the Real Property that is leased by Parent as lessee.
5.20 Related-Party Transactions. Other than with respect to Maverick IPA and except as set forth on Schedule 5.20, no current or former officer, director, employee, Shareholder or Affiliate of Parent (i) has any material interest in or owns any property or right used in the conduct of the Business, (ii) is presently, or during the last 12 months has been, a party to any material transaction with Parent or (iii) is the direct or indirect owner of an interest in any Person that is a present competitor, supplier or customer of the Business (other than non-affiliated holdings in publicly held companies).
| -57- |
(a) All policies or binders of fire, liability, product liability, worker’s compensation, vehicular, life, fiduciary liability, fidelity bond, directors’ and officers’ liability, malpractice liability, theft, other forms of property and casualty insurance and other insurance held by or on behalf of Parent are listed and described on Schedule 5.21(a), are valid and enforceable in accordance with their terms, and are in full force and effect. Schedule 5.21(a) indicates, for each such policy, whether it provides coverage on a “claims made” or “occurrence” basis. All such policies (i) are for such amounts as are sufficient for all Legal Requirements and all contracts to which Parent is a party or by which Parent is bound and (ii) are in such amounts, with such deductibles and against such risks and losses, as are reasonable for the businesses, assets and properties of Parent. Schedule 5.21(a) lists in respect of each such policy, the policy name, policy number, carrier, term, type and amount of coverage and annual premium, whether the policies may be terminated upon consummation of the transactions contemplated hereby and if and to what extent events being notified to the insurer after the Closing Date are generally excluded from the scope of the respective policy. All premiums on all such policies have been paid to date and Parent has complied with all conditions of such policies. Parent is not in default with respect to its obligations under any of such insurance policies, nor has Parent received any notification of cancellation of any such insurance policies.
(b) Except as set forth on Schedule 5.21(b) no insurance carrier has denied coverage for any claim asserted by Parent during the twelve (12) month period preceding the date hereof, nor has any insurance carrier declined to provide any coverage to Parent during the twelve (12) month period preceding the date hereof. Schedule 5.21(b) hereto sets forth, by year, for the current policy year and each of the two (2) preceding policy years: (i) a summary of the loss experience under each policy of insurance; and (ii) a statement describing each claim under a policy of insurance (including (A) the name of the claimant, (B) a description of the policy by insurer, type of insurance and period of coverage and (C) the amount and brief description of the claims). Except as set forth on Schedule 5.21(b) there are no pending claims under any such policies, and there are no claims under such policies as to which the insurers have denied liability.
(c) Except as set forth on Schedule 5.21(c), no event relating to Parent has occurred which could reasonably be expected to result in a retroactive upward adjustment in premiums under any such insurance policies or which could reasonably be expected to result in a prospective upward adjustment in such premiums. Excluding insurance policies that have expired and been replaced in the Ordinary Course of Business, no insurance policy has been cancelled within the last two (2) years and, to Parent’s Knowledge, no threat has been made to cancel any insurance policy of Parent during such period. Except as noted on Schedule 5.21(c), all such insurance will remain in full force and effect immediately following the consummation of the transactions contemplated hereby. No event has occurred, including the failure by Parent to give any notice or information or Parent giving any inaccurate or erroneous notice or information, which limits or impairs the rights of Parent under any such insurance policies.
5.22 Intangible Personal Property; Software.
(a) Schedule 5.22(a) is a true and complete list of each patent, copyright, trademark, service mark, trade name or other item of Intellectual Property registered by Parent with any Governmental Body.
| -58- |
(b) Parent owns, or holds adequate licenses or other rights to use, all Intellectual Property used by Parent in connection with its operations. No Actions have been instituted, are pending or, to Parent’s Knowledge, are threatened which challenge the validity of the ownership or use by Parent of any Intellectual Property that it has used.
(c) Parent has not received any written notice of any claim, and has no other reasonable grounds to believe, that any Intellectual Property that it has used is infringing any patent, trade name, trademark, service mark, copyright, trade secret, or other Intellectual Property belonging to any other Person.
(d) Schedule 5.22(d) sets forth a list of all computer software programs, computer databases and related documentation and materials that are used by Parent in connection with its Business operations other than commercial off-the-shelf software programs, as well as those subject only to “shrink wrap,” “click through” and/or “click wrap” licenses. Parent either owns such listed software or holds a valid license to use such software and the use by Parent of such listed software that is proprietary to Parent does not conflict with, misappropriate or infringe upon the rights or ownership interests of any other Person.
5.23 Environmental. Except as set forth in Schedule 5.23:
(a) Parent is in compliance with, and for the past ten (10) years has been in compliance with all applicable Environmental Legal Requirements, except where the failure to comply, individually or in the aggregate, has not been and would not reasonably be expected to be material to Parent. No change in facts or circumstances reported or assumed in the applications for or the granting of the Environmental Permits exists. There are no proceedings pending or, to Parent’s Knowledge, threatened which would jeopardize the validity of any of the Environmental Permits.
(b) There are no Environmental Claims pending or, to Parent’s Knowledge, threatened against Parent, the Real Property or any Person whose liability for Environmental Claims, Parent may have assumed contractually or by operation of law and, there are no circumstances that can reasonably be expected to form the basis of any such Environmental Claim.
(c) (i) None of Parent or any of its respective predecessors or to Parent’s Knowledge, Affiliates, has treated, stored, disposed of, arranged for or permitted the disposal of, transported, handled, or released any substance, including without limitation any Hazardous Materials, or owned or operated such Real Property in such manner as have given or would give rise to any liabilities (contingent or otherwise) or investigative, corrective or remedial obligations, pursuant to CERCLA or any other Environmental Legal Requirements; (ii) there are no underground or above ground storage tanks or any septic tanks, pits, sumps or lagoons at the Real Property; (iii) there is no asbestos or asbestos-containing material located at or on the Real Property; (iv) there is not constructed, placed, deposited, Released, stored, disposed, leaching nor located on the Real Property any polychlorinated biphenyls; and (v) no Environmental Lien or land use limitation has attached to the Real Property or any other property now or formerly operated or used in connection with the Business and/or Parent’s assets or otherwise by Parent or their respective predecessors or, to Parent’s Knowledge, Affiliates.
| -59- |
(d) There is no Environmental Condition at, under, in the vicinity of or emanating from, the Real Property, or during the period of Parent’s ownership, lease, use or occupancy thereof, at, under, in the vicinity of or emanating from any property formerly owned, leased, used or occupied by Parent.
(e) Parent has not entered into any consent order, consent decree, settlement agreement or other similar agreement with any Governmental Authority that imposes ongoing or outstanding obligations under Environmental Legal Requirements on Parent, other than the Environmental Permits.
(f) Parent has not assumed by contract any liability, including without limitation any obligation for corrective or Remedial Action, of any other Person relating to Environmental Legal Requirements.
(g) Neither the Real Property nor any other property operated or used in connection with Parent’s Business and/or assets or otherwise by Parent, is listed or proposed for listing on the National Priorities List pursuant to CERCLA, or listed on the Comprehensive Environmental Response Compensation Liability Information System List, or any similar state list of sites, and no condition at such properties exists that, if known to a Governmental Authority, would qualify such property for inclusion on any such list.
(h) Parent has provided the Company with copies of any environmental permits, environmental assessments, remedial investigation reports, remedial action reports, audit reports or other similar studies or analyses relating to the Business, the Real Property and Parent.
5.24 Books and Records. The minute books, stock record books and other books and records of Parent, all of which have been made available to the Company, are complete and correct and have been maintained in accordance with sound business practices and applicable Legal Requirements. The minute books of Parent contain accurate and complete records of all meetings, and actions taken by written consent of, the Shareholders, Parent Board and any committees of Parent Board, and no meeting, or action taken by written consent, of any such Shareholders, Parent Board or committee has been held for which minutes have not been prepared and are not contained in such minute books. At the Closing, all of those books and records will be in the possession of Parent.
5.25 Disclosure. No representation or warranty of Parent in this Agreement and no information contained in the Disclosure Schedule contains or will contain any untrue statement of a material fact or omits or will omit to state a material fact required to make the statements herein or therein, in light of the circumstances under which they were made, not misleading. Parent has delivered or caused to be delivered to the Company true, correct and complete copies of all documents, and any and all amendments to any such documents, referred to in this Agreement or in the Disclosure Schedule.
| -60- |
5.26 No Disqualification Event. No “bad actor” disqualifying event described in Rule 506(d)(1)(i)-(viii) of the Securities Act (a “Disqualification Event”) is applicable to Parent or, to Parent’s Knowledge, any Parent Covered Person (as defined in Rule 506(d)), except for a Disqualification Event as to which Rule 506(d)(2)(ii–iv) or (d)(3), is applicable.
5.27 SEC Reports; Financial Statements. Parent has filed all reports, schedules, forms, statements and other documents required to be filed by Parent under the Securities Act and the Exchange Act, including pursuant to Section 13(a) or 15(d) thereof, for the two (2) years preceding the date hereof (or such shorter period as Parent was required by Legal Requirements to file such material) (the foregoing materials, including the exhibits thereto and documents incorporated by reference therein, being collectively referred to herein as the “SEC Reports”) on a timely basis or has received a valid extension of such time of filing and has filed any such SEC Reports prior to the expiration of any such extension or further extension. As of their respective dates, the SEC Reports complied in all material respects with the requirements of the Securities Act and the Exchange Act, as applicable, and none of the SEC Reports, when filed, contained any untrue statement of a material fact or omitted to state a material fact required to be stated therein or necessary in order to make the statements therein, in the light of the circumstances under which they were made, not misleading. The financial statements of Parent included in the SEC Reports comply in all material respects with applicable accounting requirements and the rules and regulations of the SEC with respect thereto as in effect at the time of filing. Such financial statements have been prepared in accordance with GAAP, except as may be otherwise specified in such financial statements or the notes thereto and except that unaudited financial statements may not contain all footnotes required by GAAP, and fairly present in all material respects the financial position of Parent and its consolidated subsidiaries and affiliates as of and for the dates thereof and the results of operations and cash flows for the periods then ended, subject, in the case of unaudited statements, to normal, immaterial, year-end audit adjustments.
ARTICLE
VI
CONDITIONS TO CLOSING
6.1 Conditions to Obligations of All Parties. The obligation of each Party to complete the Closing is subject to the satisfaction on or before the Closing Date of the following conditions:
(a) Company Shareholder Approval. Shareholders of the Company (i) holding at least 95% of the Company Shares and (ii) representing at least 95% in number of the shareholders shall have duly and affirmatively approved the principal terms of this Agreement and the transactions contemplated hereby, including the Merger.
(b) Parent Shareholder Approval. Parent Shareholder Approval of the principal terms of this Agreement and the transactions contemplated hereby, including the Merger, shall have been received in accordance with Section 3.10.
(c) Regulatory Approvals. (i) Any applicable waiting period (or extension thereof) relating to the Merger under the HSR Act shall have expired or been terminated and (ii) any applicable waiting period (or extension thereof) or approval relating to the Merger that is required under antitrust Legal Requirements (other than the HSR Act) prior to the Closing shall have expired, been terminated, or approval shall have been obtained or waived and shall be in full force and effect at the Closing.
| -61- |
(d) Registration Statement. If filed by Parent pursuant to Section 3.9, the Proxy/Registration Statement shall have become effective under the Securities Act. No stop order suspending the effectiveness of the Proxy/Registration Statement shall have been issued, and no proceedings for that purpose shall have been initiated or be threatened by the SEC and not concluded or withdrawn.
(e) No Injunctions or Legal Restraints; Illegality. No Governmental Authority has issued, enacted, entered, promulgated or enforced any Legal Requirements or Order (that has not been vacated, withdrawn or overturned) restraining, enjoining or otherwise prohibiting the Merger.
6.2 Conditions to the Obligations of Parent and Merger Sub. The obligation of Parent and Merger Sub to complete the Closing is subject to the satisfaction on or before the Closing Date of the following conditions, any one or more of which Parent may waive in its sole discretion:
(a) Representations, Warranties and Covenants. The representations and warranties of the Company in Article IV and in any other written instrument the Company (or its representatives) or the Shareholders deliver to Parent (or its representatives) in connection with this Agreement shall be true and correct in all material respects on the date hereof and as of the Closing Date; provided, however, that the representations and warranties of the Company set forth in Section 4.2 and Section 4.13 shall be true and correct in all respects on the date hereof and as of the Closing Date. On or before the Closing Date, the Company and the Shareholders’ Representative shall have performed and complied in all material respects with all covenants and agreements required to be performed and complied with by the Company and the Shareholders’ Representative prior to the Closing under this Agreement. For purposes of the preceding two sentences the word “material” and the term “Material Adverse Effect” in all such representations, warranties, covenants and agreements shall be stricken when reading all such representations, warranties, covenants and agreements so that the concept of materiality is not compounded in understanding and applying those two sentences.
(b) Authority and Third-Party Consents. The Company shall have obtained all consents, authorizations, approvals, novations, and waivers of rights to terminate or modify any rights or obligations of the Company from all Third Parties and Governmental Authorities with respect to the transactions contemplated by this Agreement set forth on Schedule 6.2(b), and all such consents, authorizations, approvals, novations and waivers shall remain in effect.
(c) Delivery of Documents. At or before the Closing, the Company shall deliver or cause to be delivered to Parent (or the Exchange Agent or other applicable Person) the following documents or take the following actions, any of which may be waived by Parent in its sole discretion:
(i) the Exchange Agreement, duly executed by all Parties thereto other than Parent;
| -62- |
(ii) the Lock-Up Agreement, duly executed by all Shareholders;
(iii) a Certificate executed by the Chief Executive Officer and the Chief Financial Officer of the Company to the effect that the conditions set forth in Section 6.2(a) have been satisfied;
(iv) a certificate of an authorized officer of the Company, certifying as to (A) the incumbency of its officers executing documents executed and delivered in connection herewith, (B) copies of the governing and organizational documents of the Company, each as in effect from the Execution Date until the Closing Date and (C) a copy of the resolutions of the board of directors and the Shareholder(s) of the Company authorizing and approving the Merger and applicable matters contemplated hereunder;
(v) an affidavit, duly executed by an authorized officer of the Company certifying that the Company is not, and has not been, a “United States real property holding corporation” for purposes of Section 897(c)(2) of the Code, in a form reasonably acceptable to Parent;
(vi) Letters of Transmittal duly executed by Shareholders (i) holding at least 95% of the Company Shares and (ii) representing at least 95% in number of the shareholders and effective as of the Effective Time;
(vii) evidence of termination of the Company Voting Trust Agreement effective as of the Effective Time;
(viii) evidence of amendments or other documented contractual arrangements between the Company and Allied IPA, in form and substance reasonably satisfactory to Parent, to document the pass-through by Allied IPA to the Company of any fees received by Allied IPA for management services that are subcontracted by Allied IPA to the Company;
(ix) customary investor representations in the form attached hereto as Exhibit G, duly executed by all Shareholders (the “Shareholder Representations”);
(x) such other instruments, certificates, consents or other documents as are reasonably necessary to carry out the transactions contemplated by this Agreement and to comply with the terms hereof, or as required pursuant to the terms of this Agreement.
(d) Litigation. No Action shall have been instituted or threatened in writing before any Governmental Authority to restrain or prevent the carrying out of the Merger or the other transactions contemplated hereby or to seek damages in connection with such transactions.
(e) Material Adverse Effect. Since the Execution Date, no Material Adverse Effect shall have occurred.
| -63- |
(f) Dissenting Shareholder Interests. The Company shall have complied in all respects with its covenants set forth in Section 3.16 and at Closing there shall be no Shareholders who have exercised their dissenters’ rights in accordance with the Dissenters’ Rights Rules (and not withdrawn such exercise or otherwise become ineligible to effect such exercise) in respect of the Merger, or any other Dissenting Shareholders.
(g) Maverick Purchase Agreement. All of the conditions precedent to Allied IPA’s purchase of all of the issued and outstanding capital stock of Maverick IPA under the Maverick Purchase Agreement shall have been satisfied or waived.
6.3 Closing Conditions Precedent to Obligations of the Company. The Company’s obligation to complete the Closing is subject to the satisfaction on or before the Closing Date of the following conditions, any one or more of which the Company may waive in its sole discretion:
(a) Representations, Warranties and Covenants. The representations and warranties of Parent and Merger Sub in Article V, and in any other written instrument Parent or Merger Sub (or their respective representatives), as applicable, delivers to the Company (or its representatives) in connection therewith, shall be true and correct in all material respects on the date hereof and as of the date of the Closing; provided, however, that the representations and warranties of Parent set forth in Section 5.2 and Section 5.14 shall be true and correct in all respects on the date hereof and as of the Closing Date. On or before the Closing Date, Parent and Merger Sub, as applicable shall have performed and complied in all material respects with all covenants and agreements required to be performed or complied with by Parent and Merger Sub, as applicable, prior to the Closing under this Agreement. For purposes of the preceding two sentences the word “material” and the term “Material Adverse Effect” in all such representations, warranties, covenants and agreements shall be stricken when reading all such representations, warranties, covenants and agreements so that the concept of materiality is not compounded in understanding and applying those two sentences.
(a) Representations, Warranties and Covenants. The representations and warranties of Parent and Merger Sub in Article V, and in any other written instrument Parent or Merger Sub (or their respective representatives), as applicable, delivers to the Company (or its representatives) in connection therewith, shall be true and correct in all material respects on the date hereof and as of the date of the Closing; provided, however, that the representations and warranties of Parent set forth in Section 5.2 and Section 5.14 shall be true and correct in all respects on the date hereof and as of the Closing Date. On or before the Closing Date, Parent and Merger Sub, as applicable shall have performed and complied in all material respects with all covenants and agreements required to be performed or complied with by Parent and Merger Sub, as applicable, prior to the Closing under this Agreement. For purposes of the preceding two sentences the word “material” and the term “Material Adverse Effect” in all such representations, warranties, covenants and agreements shall be stricken when reading all such representations, warranties, covenants and agreements so that the concept of materiality is not compounded in understanding and applying those two sentences.
(b) Authority and Third-Party Consents. Parent and Merger Sub shall have obtained all consents, authorizations, approvals, novations, and waivers of rights to terminate or modify any rights or obligations of Parent from all Third Parties and Governmental Authorities with respect to the transactions contemplated by this Agreement set forth on Schedule 6.2(b), and all such consents, authorizations, approvals, novations and waivers shall remain in effect.
(c) Delivery of Documents and Payment. At the Closing, Parent shall deliver or cause to be delivered to the Company (or the Exchange Agent or other applicable Person) the following documents or take the following actions, any of which may be waived by the Company in its sole discretion:
(i) deposit of the Closing Share Payment in such manner as designated by the Exchange Agent;
| -64- |
(ii) the amounts for fractional shares by wire transfer of immediately available funds to an account of the Exchange Agent for distribution to the Shareholders in accordance with the terms hereof;
(iii) certified copies of the resolutions of Parent and Merger Sub authorizing the Merger pursuant to this Agreement;
(iv) a Certificate of an authorized officer of Parent and Merger Sub certifying as to the incumbency of its officers executing documents executed and delivered in connection herewith;
(v) a Certificate executed by the Chief Executive Officer and the Chief Financial Officer of Parent to the effect that the conditions set forth in Section 6.3(a) have been satisfied;
(vi) the Exchange Agreement, duly executed by Parent and the Exchange Agent; and
(vii) such other instruments, certificates, consents, or other documents as are reasonably necessary to carry out the transactions contemplated by this Agreement and to comply with the terms hereof, or as required pursuant to the terms of this Agreement.
(d) Litigation. No Action shall have been instituted or threatened in writing before any Governmental Authority to restrain or prevent the carrying out of the Merger or the other transactions contemplated hereby or to seek damages in connection with such transactions.
(e) Material Adverse Effect. Since the Execution Date, no Material Adverse Effect shall have occurred.
(f) Maverick Purchase Agreement. All of the conditions precedent to Allied IPA’s purchase of all of the issued and outstanding capital stock of Maverick IPA under the Maverick Purchase Agreement shall have been satisfied or waived.
6.4 Frustration of Closing Conditions. None of the Company, Parent or Merger Sub may rely on the failure of any condition set forth in Sections 6.1, 6.2 and 6.3, as the case may be, to be satisfied if such failure was caused by such Party’s failure to comply in any material respect with its obligations under this Agreement to be performed at or prior to the Closing Date.
ARTICLE
VII
POST CLOSING COVENANTS
7.1 Employment and Employee Benefits.
(a) As of the Effective Time, the Surviving Entity shall assume sponsorship of and maintain the Employee Benefit Plan sponsored and maintained by the Company immediately prior to the Closing Date under which each Business Employee will continue to participate on and after the Closing Date until such time as is otherwise determined the board of directors of Parent from and after the Effective Time.
| -65- |
(b) Nothing contained herein, express or implied shall (i) be construed to establish, amend or modify any benefit plan, program, agreement, policy or arrangement or (ii) alter or limit the ability of the Surviving Entity, Parent, the Company or any of their respective affiliates to amend, modify or terminate any benefit plan, program, agreement, policy or arrangement at any time assumed, established, sponsored or maintained by any of them. This Section 7.1 shall be binding upon and inure solely to the benefit of each of the Parties, and nothing in this Section 7.1, express or implied, is intended to confer upon any other person any rights or remedies of any nature whatsoever under or by reason of this Section 7.1.
7.2 Noncompete and Nonsolicitation. In consideration of the representations, warranties, indemnification obligations and release of claims given by each such Shareholder in such Shareholder’s Letter of Transmittal and herein and the compensation to be paid to the Shareholders, each Shareholder (on behalf of such Shareholder’s Affiliates) shall agree to a noncompetition and nonsolicitation in the form attached to such Shareholder’s Letter of Transmittal.
7.3 Post-Closing Parent Governance.
(a) At the Effective Time, the certificate of incorporation and bylaws of Parent shall be amended to divide the board of directors of Parent into three (3) classes, Class I, Class II and Class III, as set forth in the Certificate of Amendment and Amendment to Bylaws attached hereto as Exhibits H-1 and H-2, respectively.
(b) Unless otherwise agreed by Parent and Company in writing prior to the Effective Time, Parent shall use reasonable efforts to cause the board of directors of Parent to consist, on or promptly following the Effective Time, of the persons designated by Parent and Company, respectively, as set forth on Schedule 7.3; provided, however, that if one or more of such designees are not approved for service on the board of directors of Parent by Parent’s existing Board of Directors after consideration in good faith based on NASDAQ board nominating criteria, Parent or Company, as applicable, shall designate a replacement for such designee to be considered in accordance with the same process as the original designee as set forth in this Section 7.3(b).
(c) In accordance with and subject to the Bylaws of Parent, on or promptly following the Effective Time, the officers of Parent shall consist of the persons set forth on Schedule 7.3, each serving until the earlier of his or her resignation or removal or until his or her successor is duly elected and qualified. The duties, powers and responsibilities of such officers shall be as set forth in the bylaws of Parent.
| -66- |
8.1 Survival. All representations and warranties and the covenants and agreements (to the extent such covenant or agreement contemplates or requires performance prior to the Closing) of the Company shall terminate and expire on, and shall cease to have any further force or effect following, the date which is two (2) years from the Closing Date (the “Expiration Date”); provided, however, that if at any time prior to the Expiration Date, an Indemnified Party has duly delivered to the applicable Indemnifying Parties a Claim Notice (satisfying the requirements set forth in Sections 8.4 and 8.5), then the specific indemnification claim asserted in such Claim Notice shall survive the Expiration Date until such time as such claim is resolved. All representations and warranties and the covenants and agreements (to the extent such covenant or agreement contemplates or requires performance prior to the Closing, but not, for the avoidance of doubt, the payment obligations of Parent and Merger Sub pursuant to Section 2.3) made by any of the Parties shall terminate and expire at the Closing. Each covenant and agreement requiring performance at or after the Closing, will, in each case, expressly survive Closing in accordance with its terms, and if no term is specified, then such covenants and agreements shall survive indefinitely following the Effective Time.
8.2 Indemnification of Parent Indemnified Parties. After the Closing Date and subject to the limitations set forth herein, the Parent, together with its Affiliates (including the Surviving Entity after the Closing) and their respective officers, directors, representatives, shareholders, partners, members, managers, agents, Business Employees, successors and permitted assigns (each, an “Parent Indemnified Party” and collectively, the “Parent Indemnified Parties”) shall be entitled to be indemnified solely from the Holdback Shares (except as set forth in Sections 8.2(b) and (d) below) against any Losses, directly or indirectly, arising out of or resulting from:
(a) any breach of any warranty or the inaccuracy of any representation of the Company contained in this Agreement or any Transaction Document (it being understood that for purposes of this Section 8.2(a) such representations shall be deemed to have been made as of the date of this Agreement and as of the Closing (except that any representation or warranty that speaks as of the date of this Agreement or any other date shall only be deemed to have been made as of such date));
(b) any breach or inaccuracy of any representation made by any Shareholder in a Letter of Transmittal; provided that, notwithstanding anything in this Agreement to the contrary, all Losses subject to indemnification as described in this Section 8.2(b) (irrespective of the amount of such Losses) shall be assessed solely against such breaching Shareholder’s respective Holdback Shares, and shall not reduce or otherwise affect the number of Holdback Shares distributable to any of the non-breaching Shareholders;
(c) any breach by the Company or the Shareholders’ Representative, or failure of any such Persons to perform, any of their covenants or obligations contained in this Agreement or any Transaction Document; and
| -67- |
(d) any Action of any Shareholder relating to the allocation or entitlement to a portion of the Merger Consideration, or the calculations and determinations set forth on the Consideration Spreadsheet, or any other matter relating to the Merger or the transactions contemplated by this Agreement, including any such claims under any purported contractual, employment or other rights that assert entitlement to any security of the Company or any portion of the Merger Consideration, other than any claims relating to Parent’s failure to pay any portion of the Merger Consideration pursuant to this Agreement; provided that, notwithstanding anything in this Agreement to the contrary, all Losses subject to indemnification as described in this Section 8.2(d) (irrespective of the amount of such Losses) shall be assessed solely against such breaching Shareholder’s respective Holdback Shares, and shall not reduce or otherwise affect the number of Holdback Shares distributable to any of the non-breaching Shareholders.
All Losses subject to indemnification as described in this Section 8.2 shall be assessed against the Holdback Shares on a joint and several basis in accordance with each Shareholder’s Pro Rata Portion (except as set forth in Sections 8.2(b) and (d) above).
8.3 Indemnification of Shareholder Indemnified Parties. After the Closing Date and subject to the limitations set forth herein, the Shareholders and their respective successors and permitted assigns (each, a “Shareholder Indemnified Party” and collectively, the “Shareholder Indemnified Parties”) shall be entitled to be indemnified solely through the issuance of Parent Indemnity Shares against any Losses, directly or indirectly, arising out of or resulting from:
(a) any breach of any warranty or the inaccuracy of any representation of the Parent and/or the Merger Sub contained in this Agreement or any Transaction Document (it being understood that for purposes of this Section 8.3(a) such representations shall be deemed to have been made as of the date of this Agreement and as of the Closing (except that any representation or warranty that speaks as of the date of this Agreement or any other date shall only be deemed to have been made as of such date)); and
(b) any breach by Parent and/or the Merger Sub, or failure of any such Persons to perform, any of their covenants or obligations contained in this Agreement or any Transaction Document.
All Losses subject to indemnification as described in this Section 8.3 shall be satisfied through the issuance of up to the number of Parent Shares that is equal to the initial number of Holdback Shares as of immediately following the Effective Time (the “Parent Indemnity Shares”). For purposes of placing a value on the Parent Indemnity Shares and for determining the number of Parent Indemnity Shares used to satisfy any indemnifiable Losses under this Section 8.3, the subject Parent Indemnity Shares shall be valued at the VWAP per Parent Share averaged over the ten (10) trading days immediately preceding the time of assessment against such Parent Indemnity Shares (as adjusted for any stock dividends, combinations, reverse stock splits, stock splits, recapitalizations, reorganizations, reclassifications or other similar event with respect to the Parent Indemnity Shares). Subject to the indemnification limitations set forth in this Article VIII, the Shareholder Indemnified Parties are entitled to receive Parent Indemnity Shares in an amount sufficient to satisfy indemnifiable Losses of the Shareholder Indemnified Parties up to the maximum amount of the Parent Indemnity Shares. Upon the final determination of any claim for indemnification, Parent shall issue Parent Indemnity Shares in an aggregate amount necessary to satisfy and pay such claim, and each Shareholder Indemnified Party shall be entitled to receive its respective Pro Rata Portion of the Parent Indemnity Shares, subject to the requirement that such Shareholder Indemnified Party satisfies applicable SEC accredited investor standards, unless the issuance is otherwise exempt under applicable SEC rules.
| -68- |
8.4 Notice of Asserted Liability.
(a) The Indemnified Party shall promptly notify in writing (a “Claim Notice”) the other applicable Parties responsible for indemnification pursuant to this Article VIII (collectively, the “Indemnifying Parties”) of any matter giving rise to an obligation to indemnify setting forth, in reasonable detail, the identity, nature and estimate of the asserted Losses and a reference to the provision of this Agreement or any other agreement, document or instrument executed hereunder or in connection herewith upon which such claim is based; provided, however, that the failure of any Indemnified Party to give the Claim Notice promptly as required by this Section 8.4 shall not affect such Indemnified Party’s rights under this Article VIII except to the extent such failure is actually and materially prejudicial to the rights and obligations of the Indemnifying Parties. For purposes of delivering a Claim Notice delivery to the Shareholders’ Representative shall constitute delivery of a Claim Notice to all Shareholders.
(b) After the giving of any Claim Notice pursuant hereto, the amount of indemnification to which an Indemnified Party shall be entitled under this Article VIII shall be determined: (i) by the written agreement between the Indemnified Party and the Indemnifying Parties; (ii) by dispute resolution in accordance with Article X hereof; or (iii) by any other means to which the Indemnified Party and the Indemnifying Parties shall agree in writing. All compensation due to an Indemnified Party as so finally determined shall be so compensated within fifteen (15) calendar days after such final determination and paid in accordance with Section 8.6 below.
(a) An Indemnified Party must give a written Claim Notice to the Indemnifying Parties within thirty (30) days after receiving notice of any Action against it (a “Third Person Claim”) that the Indemnified Party receives which may give rise to a claim for indemnification under this Article VIII. The Indemnified Party’s failure to notify the Indemnifying Parties will not relieve the Indemnifying Parties of liability to any Indemnified Party except to the extent that the defense of the Third Person Claim is actually and materially prejudiced by the Indemnified Party’s failure to give a timely Claim Notice, and then any such liability of the Indemnifying Parties shall be relieved only to the extent of such prejudice.
| -69- |
(b) The Indemnifying Parties may assume the defense of such Third Person Claim at its sole expense, if it gives notice of its intention to do so within twenty (20) calendar days of its receipt of the Claim Notice, but must retain counsel that is reasonably satisfactory to the Indemnified Party. The Indemnifying Parties may not assume the defense of the Third Person Claim unless it first (i) demonstrates to the Indemnified Party in writing after giving effect to the application of the limitations in Section 8.6 that the Indemnifying Parties would be responsible for a greater portion of the Losses related to such Third Person Claim than the Indemnified Party, and (ii) enters into an agreement with the Indemnified Party (in form and substance reasonably satisfactory to the Indemnified Party) pursuant to which the Indemnifying Parties agree to be fully responsible and provide full indemnification (with no reservation of rights) for its portion of the Losses related to such Third Person Claim; provided, however, that the Indemnifying Parties shall not have the right to assume control of such defense and shall pay the fees and expenses of counsel retained by the Indemnified Party, if (A) the Third Person Claim seeks an injunction or equitable relief or (B) the Third Person Claim involves a criminal proceeding, Action, indictment, allegation or investigation, (C) the Indemnified Party reasonably believes an adverse determination with respect to the Third Person Claim giving rise to such claim for indemnification would have a material adverse effect on the Indemnified Party’s Business or future business prospects; (D) a conflict of interest exists between the Indemnifying Parties and the Indemnified Party; or (E) the Indemnifying Parties failed or are failing to vigorously prosecute or defend such claim. For the avoidance of doubt, the right to defend any Third Person Claim hereunder shall expressly include the obligation to post all appeal bonds, sureties, guaranties or similar obligations in connection with such Third Person Claim or proceedings related thereto. If the Indemnifying Parties are permitted to assume and control the defense and elect to do so, the Indemnified Party shall have the right to employ counsel separate from counsel employed by the Indemnifying Parties in any such Action and to participate in the defense thereof, but the fees and expenses of such counsel employed by the Indemnified Party shall be at the expense of the Indemnified Party unless the retention thereof has been specifically authorized by the Indemnifying Parties in writing.
(c) If the Indemnifying Parties give timely notice to the Indemnified Party of its election to assume the defense of the Third Person Claim pursuant to and in accordance with the terms and conditions set forth in Section 8.5(b), then, except as otherwise provided in Section 8.5(b) and otherwise herein, the Indemnifying Parties shall not be liable to the Indemnified Party for attorneys’ fees or any other expenses that the Indemnified Party subsequently incurs with respect to the defense of the Third Person Claim.
(d) If the Indemnifying Parties assume the defense of a Third Person Claim, such Indemnifying Parties may not effect any compromise or settlement of the Third Person Claim without the Indemnified Party’s consent unless: (i) there is no finding or admission of any violation of any Legal Requirements or any violation of the rights of the Indemnified Party; (ii) the compromise or settlement does not require the Indemnified Party to pay any Losses or bear any non-monetary cost or restriction; and (iii) the compromise or settlement includes as an unconditional term thereof the delivery by the claimant or plaintiff to Indemnified Party of a written release from all liability in respect of such Third Person Claim. Except as provided in this Section 8.5(d), the Indemnified Party shall have no liability with respect to any compromise or settlement of any Third Person Claim effected without its consent.
(e) If the Indemnifying Parties fail to notify the Indemnified Party within twenty (20) calendar days after receiving the Claim Notice that such Indemnifying Parties will assume the defense of the Third Person Claim, the Indemnified Party may, by notice to the Indemnifying Parties, assume the right to defend, compromise or settle the Third Person Claim.
| -70- |
(f) With respect to any Third Person Claim subject to indemnification under this Article VIII:
(i) the Indemnified Party and the Indemnifying Parties, as applicable, will keep the other Person reasonably informed of the status of the Third Person Claim and any related Actions under all circumstances in which such other Person is not represented by its own counsel;
(ii) the Parties (at the Indemnifying Parties expense) will render to each other such assistance as they may reasonably require of each other and to cooperate in good faith with each other to ensure the proper and adequate defense of any Third Person Claim; and
(iii) the Parties will cooperate in such a manner as to preserve in full the attorney-client and work-product privileges.
8.6 Limitations on Indemnification.
(a) Notwithstanding anything in this Agreement to the contrary, the Indemnifying Parties shall not be liable for Losses described in Section 8.2(a) until the aggregate amount of Losses suffered by the Parent Indemnified Parties exceeds $100,000 or the aggregate amount of Losses suffered by the Shareholder Indemnified Parties exceeds $100,000, as the case may be (the “Threshold Amount”). Once the aggregate amount of Losses exceeds the Threshold, the Indemnifying Parties shall be jointly and severally liable for the full amount of all Losses up to the amount of the Holdback Shares or the Parent Indemnity Shares (except as set forth in Sections 8.2(b) and (d) above), as applicable, including any amounts which constituted the Threshold.
(b) (i) The Indemnifying Parties shall not have any liability under Section 8.2 or 8.3 for an aggregate amount of Losses exceeding the Holdback Shares or the Parent Indemnity Shares, respectively (the “Cap”); provided, that (A) the Cap shall not apply to Losses arising from any fraud or intentional misrepresentation (the “Cap Carve Outs”) and (B) any amounts paid on account of the Cap Carve Outs shall not be aggregated with other amounts paid under Section 8.2 or 8.3 for purposes of determining whether the Cap has been met or exceeded.
(c) Any indemnity payment hereunder shall be treated for Tax purposes as an adjustment of the Merger Consideration to the extent such characterization is proper or permissible under relevant Tax law, including court decisions, statutes, regulations and administrative promulgations, unless otherwise required by a determination as defined in Section 1313(a) of the Code.
(d) Except for remedies that cannot be waived under Legal Requirements and injunctive and provisional relief, if the Closing occurs, this Article VIII (as enforced through the application of Article X hereof) shall (in the absence of fraud or intentional misconduct) be the sole and exclusive monetary remedy for breaches of this Agreement (including any covenant, obligation, representation or warranty contained in this Agreement or certificate delivered pursuant to this Agreement).
| -71- |
(e) No Party hereto shall have any liability for any exemplary or punitive damages, or any equitable equivalent thereof or substitute therefor, suffered or incurred by any Indemnified Party, as the case may be, except with respect to a Third Person Claim.
(f) The Shareholders shall have no right of contribution or other recourse against the Company or any of their respective officers, employees, Affiliates, agents, attorneys, representatives, assigns or successors for any Third Person Claims asserted by Parent Indemnified Parties, it being acknowledged and agreed that the covenants and agreements of the Company are solely for the benefit of the Parent Indemnified Parties.
8.7 Recourse for Indemnity Claims. Any payment to any Indemnified Parties pursuant to a claim for indemnification pursuant to Sections 8.2 or Section 8.3 shall be paid, to the extent there are sufficient Company Shares in the Holdback Shares or sufficient Parent Indemnity Shares, within five (5) Business Days after (i) written agreement by Parent and the Shareholders’ Representative by release of Company Shares to the Shareholders’ Representative, if applicable, (ii) written agreement by Parent and the Company to the issuance of the applicable number of Parent Indemnity Shares to the Shareholders, if applicable, or (iii) a copy of the decision pertaining to any unresolved dispute between the Parties issued pursuant to Article X of this Agreement is delivered to the applicable Indemnified Party indicating that the applicable Indemnified Party is entitled to indemnification under this Agreement, which release of Company Shares or issuance of Parent Indemnity Shares shall accordingly reduce the number of Company Shares in the Holdback Shares or the number of Parent Indemnity Shares available for issuance, as applicable.
8.8 Mitigation. Each of the Parties agrees to take all reasonable steps to mitigate their respective Losses upon and after becoming aware of any event or condition which could reasonably be expected to give rise to any Losses that are indemnifiable hereunder.
9.1 Termination Events. This Agreement may be terminated prior to the Effective Time, whether before or after the Company Shareholder Approval or the Parent Shareholder Approval:
(a) by mutual consent of the Company and Parent;
(b) by either Parent or Company, if:
| -72- |
(i) the Merger and the other transactions contemplated by this Agreement have not been consummated on or before August 31, 2017 (the “End Date”); provided, that the right to terminate this Agreement pursuant to this Section 9.1(b)(i) shall not be available to any Party whose failure to fulfill in any material respect any of its obligations under this Agreement has been the primary cause of, or the primary factor that resulted in, the failure of the Merger and the other transactions contemplated by this Agreement to be consummated by such time;
(ii) there shall be any applicable Legal Requirement that (A) makes consummation of the Merger and the other transactions contemplated by this Agreement illegal or otherwise prohibited; or (B) enjoins a Party from consummating the Merger and the other transactions contemplated by this Agreement and such enjoinment shall have become final and nonappealable; provided, that, the Party seeking to terminate this Agreement pursuant to this Section 9.1(b)(ii) shall have used its reasonable efforts to contest, appeal and remove such judgment, order, injunction, rule, decree, ruling or other action in accordance with Section 3.8.
(iii) Parent’s board of directors shall have made a Parent Adverse Recommendation Change;
(iv) the Parent Shareholder Approval shall not have been obtained at a meeting of the Parent shareholders duly convened therefor or at any adjournment or postponement thereof at which a vote was taken in an effort to obtain the Parent Shareholder Approval; provided, that, Parent shall not be permitted to terminate this Agreement pursuant to this Section 9.1(b)(iv) if the failure to obtain such Parent Shareholder approval is primarily caused by any action or failure of Parent that constitutes a beach of this Agreement;
(v) the Company’s Board shall have made a Company Adverse Recommendation Change;
(vi) the Company Shareholder Approval shall not have been obtained at a meeting of the Company Shareholders duly convened therefor or at any adjournment or postponement thereof at which a vote was taken in an effort to obtain the Company Shareholder Approval; provided, that, the Company shall not be permitted to terminate this Agreement pursuant to this Section 9.1(b)(vi) if the failure to obtain such Company Shareholder approval is primarily caused by any action or failure of the Company that constitutes a beach of this Agreement; or
(c) by Parent, if:
(i) a material breach by Company (directly or indirectly, through any subsidiaries, directors, officers, Business Employees, agents or representatives of the Company) of Section 3.5(a) or Section 3.10 shall have occurred;
(ii) there has been a material breach by the Company of any representation, warranty, covenant or agreement contained in this Agreement that has prevented or would prevent the satisfaction of any condition to the obligations of Parent at the Closing and such breach has not been waived by Parent in writing or, to the extent curable, cured by the Company within ten (10) Business Days after receipt by the Company or the Shareholders’ Representative of written notice thereof from Parent;
| -73- |
(iii) at the time of termination holders of more than five percent (5%) of the outstanding Company Shares have validly exercised their dissenters’ rights in accordance with the Dissenters’ Rights Rules (and not withdrawn such exercise or otherwise become ineligible to effect such exercise) in respect of the Merger; or
(iv) a Material Adverse Effect with respect to the Company has occurred and cannot be cured by the Company within ten (10) Business Days after receipt by Parent of written notice thereof from the Company or the Shareholders’ Representative; or
(v) Parent does not accept updated Disclosure Schedules provided by the Company pursuant to Section 12.11(c); or
(d) by Company, if:
(i) a material breach by Parent (directly or indirectly, through any subsidiaries, directors, officers, Business Employees, agents or representatives of Parent) of Section 3.5(b) or Section 3.11 shall have occurred;
(ii) there has been a material breach by Parent or the Merger Sub of any representation, warranty, covenant or agreement contained in this Agreement that has prevented or would prevent the satisfaction of any condition to the obligations of the Company at the Closing and such breach has not been waived by the Company or, to the extent curable, cured by Parent within ten (10) Business Days after receipt by Parent of written notice thereof by the Company;
(iii) if a Material Adverse Effect with respect to Parent and/or MergerSub has occurred and cannot be cured by Parent within ten (10) Business Days days after receipt by the Company of written notice thereof from Parent; or
(iv) the Company does not accept updated Disclosure Schedules provided by Parent pursuant to Section 12.11(c).
The Party desiring to terminate this Agreement pursuant to this Section 9.1 shall give written notice to the other Parties.
9.2 Effects of Termination. In the event of termination pursuant to Section 9.1, this Agreement shall become void and of no effect without further obligation or liability of any Party (or any subsidiaries, directors, officers, Business Employees, agents or representatives of any Party) to the other Parties hereto (except for obligations of confidentiality and non-use with respect to the other Party’s confidential information pursuant to the Nondisclosure Agreement) and no Party shall be entitled to any monetary damages or injunctive relief (including specific performance) as a result of such termination, or any indemnification under Article VIII; provided, that no such termination shall relieve any Party from any liability or Losses resulting from a knowing and intentional breach prior to such termination of any of its representations, warranties, covenants or agreements set forth in this Agreement or any other Transaction Document. Notwithstanding anything to the contrary contained herein, the obligations in Sections 3.7 (Confidentiality), 9.2 (Effects of Termination) and 9.3 (Fees and Expenses) and Article XII (General Provisions) and Article XIII (Definitions) hereof shall remain in full force and effect. For the avoidance of doubt, payment of a Parent Termination Fee or Company Termination Fee, as the case may be, shall be the sole remedy for any breach of this Agreement for which a termination fee is provided pursuant to Section 9.3.
| -74- |
(a) Except as otherwise provided in this Section 9.3, and except with respect to costs and expenses of all filing and other fees in connection with any filing under the HSR Act, each of which shall be borne equally by Parent and the Company, all fees and expenses incurred in connection with this Agreement, the Merger and the other transactions contemplated hereby shall be paid by the Party incurring such fees or expenses, whether or not the Merger is consummated.
(b) In the event that:
(i) this Agreement is terminated:
(1) by the Company or Parent pursuant to Sections 9.1(b)(i) or 9.1(b)(vi) after a Company Acquisition Proposal (whether or not conditional) or intention to make a Company Acquisition Proposal (whether or not conditional) was made directly to the Company’s Shareholders, otherwise publicly disclosed or otherwise communicated to senior management of the Company or Company Board; or
(2) by Parent pursuant to Section 9.1(b)(i) due to failure of the Company to satisfy Section 6.2(c)(ii), Section 6.2(c)(vi), Section 6.2(c)(vii), Section 6.2(c)(viii) or Section 6.2(c)(ix); or
(3) by Parent pursuant to Section 9.1(c)(i) or 9.1(c)(ii); or
(4) by Parent or the Company pursuant to Section 9.1(b)(v); and
(ii) within twelve (12) months of the date of any such termination, the Company enters into any definitive agreement with respect to, or consummates, any Company Acquisition Proposal
then, in any such event, the Company shall pay to Parent a termination fee of $1,500,000 (the “Company Termination Fee”), it being understood that in no event shall the Company be required to pay the Company Termination Fee on more than one occasion.
(c) In the event that:
| -75- |
(i) this Agreement is terminated:
(1) by the Company or Parent pursuant to Sections 9.1(b)(i) or 9.1(b)(iv) after a Parent Acquisition Proposal (whether or not conditional) or intention to make a Parent Acquisition Proposal (whether or not conditional) was made directly to Parent’s shareholders, otherwise publicly disclosed or otherwise communicated to senior management of Parent or Parent’s board of directors; or
(2) by the Company pursuant to Section 9.1(d)(i) or 9.1(d)(ii); or
(3) by Parent or the Company pursuant to Section 9.1(b)(iii); and
(ii) within twelve (12) months of the date of such termination, Parent enters into any definitive agreement with respect to, or consummates, any Parent Acquisition Proposal.
then, in any such event, Parent shall pay to the Company a termination fee of $1,500,000 (the “Parent Termination Fee”), it being understood that in no event shall Parent be required to pay the Parent Termination Fee on more than one occasion.
(d) Payment of the Company Termination Fee by the Company pursuant to Section 9.3(b) shall be made by wire transfer of same day funds to the account or accounts designated by Parent as promptly as reasonably practicable after the date on which the Company enters into a definitive agreement with respect to, or consummates, any Company Acquisition Proposal (and, in any event, within two (2) Business Days of such date).
(e) Payment of the Parent Termination Fee by Parent pursuant to Section 9.3(c) shall be made by wire transfer of same day funds to the account or accounts designated by the Company as promptly as reasonably practicable after the date on which Parent enters into a definitive agreement with respect to, or consummates, any Parent Acquisition Proposal (and, in any event, within two (2) Business Days after such date).
(f) Each of Parent and the Company acknowledge that the agreements contained in this Section 9.3 are an integral part of the transactions contemplated by this Agreement, and that, without these agreements, the other Party would not enter into this Agreement; accordingly, if either Party fails promptly to pay any amounts due pursuant to this Section 9.3, and, in order to obtain such payment, the other Party commences a suit that results in a judgment against Parent or the Company, as applicable, for the amounts set forth in this Section 9.3, the Company or Parent, as applicable, shall pay to the prevailing Party its costs and expenses (including reasonable attorneys’ fees and expenses) in connection with such suit, together with interest on the amounts set forth in this Section 9.3 from the date of termination of this Agreement at a rate per annum equal to the “Prime Rate” prevailing at such time, as published in The Wall Street Journal, from the date such amounts were required to be paid until the date actually received by the other Party.
| -76- |
DISPUTE RESOLUTION
If any controversy, claim, dispute or allegation of breach arises relating to this Agreement, the Parties shall initiate and comply with the following dispute resolution procedures. It is the intent of the Parties that the Parties will attempt to resolve any disputes or disagreements before taking advantage of the dispute resolution procedures set forth herein with the intent that the Parties will first meet and confer at the level of management personnel one level above those management personnel most familiar with the disputes or disagreements within the organization to try to resolve any such dispute or disagreement relating to this Agreement; provided, however, that this Article X shall not preclude any Party from seeking injunctive relief in a court of competent jurisdiction.
10.1 Executive Administration. In the event the Parties are unable to resolve such dispute within a reasonable period of time at a lower level, as described above, the Shareholders’ Representative and an executive officer of Parent who has the authority to negotiate and bind the Parent (together, the “Executive Administrators”) shall meet and attempt in good faith to resolve such dispute as follows: Promptly following the date the dispute was passed on to them, the Executive Administrator of the Party claiming a dispute under this Agreement shall deliver to the other Party notice of such dispute (a “Dispute Notice”) which notice shall set forth in reasonable detail, the identity, nature and estimate of the asserted dispute and a reference to the provision of this Agreement or any other agreement, document or instrument executed hereunder or in connection herewith upon which such dispute is based. Within ten (10) calendar days of receipt of such Dispute Notice, the receiving Party’s Executive Administrator shall meet with the disputing Party’s Executive Administrator, in good faith, to discuss the dispute set forth in the Dispute Notice. If the Executive Administrators are unable to resolve the dispute within fifteen (15) calendar days following their initial meeting, the matter shall be submitted to binding arbitration as set forth below.
(a) Subject to Section 10.3, if the dispute is not resolved pursuant to Section 10.1 above, then either Party may, within thirty (30) days after the completion of the procedures set forth in Section 10.1, upon written notice to the other Party, submit such dispute to judicial reference proceeding in accordance with this Section 10.2.
(b) In the event of any controversy or dispute related to or arising out of this Agreement (whether sounding in contract or tort, and whether or not involving equitable or extraordinary relief), the Parties agree to waive their rights, if any, to a jury trial, and to submit the controversy or dispute as a general reference to a retired judge or justice pursuant to Section 638 et seq. of the California Code of Civil Procedure, or any successor provision, for resolution in accordance with Chapter 6 (References and Trials by Referees), of Title 8 of Part 2 of the California Code of Civil Procedure, or any successor chapter. The Parties agree that the only proper venue for the submission of claims is the County of Los Angeles, California, and that the hearing before the referee shall be concluded within nine (9) months of the filing and service of the complaint. The Parties reserve the right to contest the referee’s decision and to appeal from any award or order of any court. The prevailing party in any such proceeding shall be entitled to recover reasonable attorneys’ fees and costs from the non-prevailing party. The referee will have no authority to award damages in excess or in contravention of Section 8.6.
| -77- |
(c) In lieu of the judicial reference proceeding described in Section 8.2(b) above, the Parties may mutually agree in writing to submit such dispute to binding arbitration as follows; provided that, for the avoidance of doubt, if the Parties fail to agree to binding arbitration, such dispute shall be resolved by the judicial reference proceeding described above:
(i) The arbitration will be held in Los Angeles, California metropolitan area before a panel of three (3) arbitrators. Either Parent or the Shareholders’ Representative may, by notice to the other Party, demand arbitration, by serving on the other party a statement of the dispute, and the facts relating or giving rise thereto, in reasonable detail, and the name of the arbitrator selected by it.
(ii) Within fifteen (15) days after receipt of such notice, the other Party will name its arbitrator, and the two (2) arbitrators named by the Parties will, within fifteen (15) days after the date of such notice, select the third arbitrator.
(iii) The arbitration will be governed by the Commercial Arbitration Rules of the AAA as then in effect, except as expressly provided in this Section 10.2; provided, however, that the arbitration will be administered by any organization agreed upon by the Parties. The arbitrators may not amend or disregard any provision of this Section 10.2.
(iv) The arbitrators will allow such discovery as is appropriate to the purposes of arbitration in accomplishing fair, speedy and cost-effective resolution of disputes. The arbitrators will not be required to make findings of fact or render opinions of law.
(v) The arbitrators will have no authority to award damages in excess or in contravention of Section 8.6.
10.3 Equitable Relief and Enforcement. Notwithstanding any other provision set forth in this Agreement, with respect to the enforcement of any term of this Agreement for which monetary damages would be inadequate, any Party shall be entitled to seek appropriate equitable relief to enforce its rights under this Agreement, without engaging in the process set forth in this Article X (the “Dispute Resolution Process”). Such right to equitable relief shall be in addition to any resolution reached pursuant to the Dispute Resolution Process.
| -78- |
SHAREHOLDERS’ REPRESENTATIVE
11.1 Appointment of Shareholders’ Representative. For purposes of this Agreement, pursuant to the Shareholder Approval and this Agreement, the Shareholders hereby designate the Shareholders’ Representative to serve as the true and lawful attorney-in-fact and agent of the Shareholders for the purposes contemplated by this Agreement.
11.2 Successor Shareholders’ Representative. In the event that the initial Shareholders’ Representative and any subsequent Shareholders’ Representative above resigns or otherwise becomes unable to serve, the Shareholders shall, within thirty (30) days after notice thereof, determine and designate by consent of a majority of the Shareholders, a successor Shareholders’ Representative who shall have all of the rights, powers and authority conferred on the Shareholders’ Representative in this Agreement, and if the Shareholders fail so to designate such successor within such period, any Shareholder, the Parent, or the Surviving Entity may petition a court of appropriate jurisdiction for appointment of such successor Shareholders’ Representative. Each successor Shareholders’ Representative, if required to serve, shall sign an acknowledgement in writing to perform and be bound by all of the provision of this Agreement applicable to the Shareholders’ Representative. Each successor Shareholders’ Representative shall have all power, authority, rights and privileges conferred by this Agreement upon the original Shareholders’ Representative, and the term “Shareholders’ Representative” as used herein shall be deemed to include any successor Shareholders’ Representative.
11.3 Power and Authority. The Shareholders’ Representative is hereby constituted and appointed as agent and attorney in fact for and on behalf of the Shareholders. This power of attorney and all authority hereby conferred is granted and shall be irrevocable and shall not be terminated by any act of any Shareholder, by operation of any Legal Requirement, whether by such Shareholder’s death, disability, protective supervision or any other event. Without limiting the generality of the foregoing, the Shareholders’ Representative has full power and authority, on behalf of each Shareholder and his, her or its successors and assigns, to (i) interpret the terms and provisions of this Agreement and the documents to be executed and delivered by the Shareholders in connection herewith, (ii) execute and deliver and receive deliveries of all agreements, certificates, statements, notices, approvals, extensions, waivers, undertakings, amendments, and other documents required or permitted to be given in connection with the consummation of the transactions contemplated by this Agreement, (iii) receive service of process in connection with any claims under this Agreement, (iv) agree to, negotiate, enter into settlements and compromises of, assume the defense of claims, and demand arbitration and comply with orders of courts and awards of arbitrators with respect to such claims, and to take all actions necessary or appropriate in the judgment of the Shareholders’ Representative for the accomplishment of the foregoing, (v) give and receive notices and communications and (vi) take all actions necessary or appropriate in the judgment of the Shareholders’ Representative on behalf of the Shareholders in connection with this Agreement.
| -79- |
11.4 Limitation on Liability; Indemnification. Neither the Shareholders’ Representative nor any agent employed by the Shareholders’ Representative shall be liable to any Shareholder relating to the performance of such Shareholders’ Representative’s duties under this Agreement for any errors in judgment, negligence, oversight, breach of duty or otherwise except to the extent it is finally determined by a final nonappealable decision of a court of competent jurisdiction that the actions taken or not taken by the Shareholders’ Representative constituted fraud or were taken or not taken in bad faith. The Shareholders’ Representative shall be indemnified and held harmless by the Shareholders against all losses, including costs of defense, paid or incurred in connection with any Action to which the Shareholders’ Representative is made a party by reason of the fact that the Shareholders’ Representative was acting as the Shareholders’ Representative pursuant to this Agreement; provided, however, that the Shareholders’ Representative shall not be entitled to indemnification hereunder to the extent it is finally determined by a final nonappealable decision of a court of competent jurisdiction that the actions taken or not taken by the Shareholders’ Representative constituted actual fraud or were taken or not taken in bad faith. The Shareholders’ Representative shall be protected in acting upon any notice, statement or certificate reasonably believed by the Shareholders’ Representative to be genuine and to have been furnished by the appropriate Person and in acting or refusing to act in good faith on any matter.
11.5 Reliance. Any approval, consent, election, notice, decision, agreement, waiver, delivery, interpretation, amendment or other action of the Shareholders required or permitted under, or otherwise provided for in or contemplated by, this Agreement (each, a “Shareholder Action”) shall be conclusively deemed given, made or taken (as the case may be) if given, made or taken by the Shareholders’ Representative and shall be binding upon each Shareholder and such Shareholder’s successors and assigns as if expressly ratified and confirmed in writing by each of them, and Parent, Merger Sub, the Surviving Entity, and their Affiliates shall be entitled to conclusively and absolutely rely, without inquiry, on any Shareholder Action, notice or other document (of any kind) performed, executed or delivered by the Shareholders’ Representative for all such purposes, and all Shareholder Actions, decisions and instructions of the Shareholders’ Representative shall be conclusive and binding upon all Shareholders and no Shareholder shall have any cause of action against Parent, Merger Sub, the Surviving Entity, and their Affiliates or the Shareholders’ Representative for any action taken or not taken by Shareholders’ Representative in his role as such.
ARTICLE
XII
GENERAL PROVISIONS
12.1 Notices. All notices, requests, claims, demands and other communications under this Agreement shall be in writing, and shall be deemed effective when personally delivered; when mailed by certified or registered mail, return receipt requested; or when deposited with a comparably reliable postal delivery service (such as Federal Express) or other courier service, or sent by facsimile or other electronic transmission system, addressed to the other Party as follows:
| If to Parent, Merger Sub or the Surviving Entity: |
Apollo Medical Holdings, Inc. 700 N. Brand Boulevard |
| -80- |
| With a copy to (which shall not constitute notice): | McDermott Will & Emery LLP 275 Middlefield Road, Suite 100 Menlo Park, California 94025 Fax No.: (650) 815-7401 Attention: Mark J. Mihanovic, Esq. |
|
| If to the Company or the Shareholders’ Representative (prior to Closing): | Network Medical Management, Inc. 1668 S. Garfield Avenue Alhambra, CA 91801 Fax No.: [____________] Attention: Kenneth Sim, M.D. |
|
| With a copy to (which shall not constitute notice): |
Tin Kin Lee Law Offices Attention: Tin Kin Lee, Esq. |
|
| If to the Shareholders’ Representative or the Shareholders (after the Closing): |
Kenneth Sim, M.D. c/o Network Medical Management, Inc. |
|
| With a copy to (which shall not constitute notice): |
Tin Kin Lee Law Offices Attention: Tin Kin Lee, Esq. |
The above addresses may be changed by a notice delivered as set forth in this Section 12.1.
12.2 Assignment. Neither this Agreement nor any of the rights, interests or obligations hereunder shall be assignable by any of the Parties without the prior written consent of the other Parties. This Agreement shall be binding upon and inure to the benefit of the Parties and their respective successors and permitted assigns. Nothing in this Agreement, expressed or implied, is intended or shall be construed to confer upon any Person other than the Parties any right, remedy or claim under or by reason of this Agreement.
12.3 No Third-Party Beneficiaries. This Agreement shall not confer any rights or remedies upon any person other than Parent and the Company and their respective successors and permitted assigns.
| -81- |
12.4 Execution of Agreement; Counterparts; Electronic Signature. This Agreement may be executed in multiple counterparts, each of which shall be deemed an original and all of which shall constitute one and the same instrument. The exchange of copies of this Agreement and signature pages by facsimile transmission, by electronic mail in portable document format form, or by any other electronic means intended to preserve the original graphic and pictorial appearance of a document, or by combination of such means, shall constitute effective execution and delivery of this Agreement as to the Parties and may be used in lieu of the original Agreement for all purposes.
12.5 Governing Law; Exclusive Jurisdiction. All disputes, claims or controversies arising out of or relating to this Agreement or the transactions contemplated hereby shall be construed in accordance with and governed by the internal laws of the State of California without giving effect to any choice or conflict of law provision or rule (whether of the State of California or any other jurisdiction) that would cause the application of laws of any jurisdiction other than those of the State of California.
12.6 Entire Agreement; Modification. This Agreement together with the other Transaction Documents, the Nondisclosure Agreement and the schedules, exhibits and annexes attached hereto and thereto, (a) constitutes, the entire agreement and supersedes all of the prior agreements and understandings, both written and oral, among the Parties, or any of them, with respect to the subject matter hereof and (b) may not be amended except by a written amendment signed by all of the Parties hereto.
12.7 Conflict Between Transaction Documents. The Parties agree and acknowledge that to the extent any terms and provisions of this Agreement are in any way inconsistent with or in conflict with any term, condition or provision of any other agreement, document or instrument contemplated by this Agreement, this Agreement will govern and control.
12.8 Construction/Severability. If any one or more of the provisions of this Agreement, or the applicability of any such provision to a specific situation, is deemed invalid or unenforceable, then such provision shall be modified to the minimum extent necessary to make its application valid and enforceable, and the validity and enforceability of all of the provisions of this Agreement, and all other applications of such provisions, shall not be affected.
12.9 Extension; Waiver. The Parties may, to the extent legally allowed, (a) extend the time for the performance of any of the obligations or other acts of the other Parties hereto, (b) waive any inaccuracies in the representations and warranties of the other Party contained herein or in any document delivered pursuant hereto and (c) waive compliance by the other Party with any of the agreements or conditions contained herein. The waiver by a Party of a breach or violation of any provision of this Agreement shall not operate as, or be construed to be a waiver of, any subsequent breach thereof, nor shall it be deemed or constitute a waiver of any other provisions, whether or not similar, nor shall any waiver constitute a continuing waiver. No waiver shall be binding unless executed in writing by the Party making the waiver.
| -82- |
12.10 Ambiguities. This Agreement has been negotiated at arm’s length and between persons sophisticated and knowledgeable in the matters dealt with in this Agreement. In addition, each Party has had the opportunity for the benefit of legal advice from experienced and knowledgeable legal counsel. Accordingly, any rule of law (including Civil Code Section 1654) or legal decision that would require interpretation of any ambiguities in this Agreement against the Party that has drafted it is not applicable and is waived. In the event an ambiguity or question of intent or interpretation arises with respect to this Agreement, the terms and provisions of the execution version of this Agreement will control and prior drafts of this Agreement and the documents referenced herein will not be considered or analyzed for any purpose (including in support of parol evidence proffered by any Person in connection with this Agreement), will be deemed not to provide any evidence as to the meaning of the provisions hereof or the intent of the parties with respect hereto and will be deemed joint work product of the parties.
(a) Titles and headings to articles, sections and subsections herein are inserted for convenience of reference only and are not intended to be a part of or to affect the meaning or interpretation of this Agreement.
(b) The Disclosure Schedules referred to herein may be incomplete or not attached hereto as of the Effective Date of this Agreement. No later than January 20, 2017, (i) Parent may deliver to the Company updated Disclosure Schedules and (ii) the Company may deliver to Parent updated Disclosure Schedules. If Parent or the Company delivers updated Disclosure Schedules, the other Party shall have until January 27, 2017 to either accept such updated Disclosure Schedules or to deliver a notice to the Party providing such updated Disclosure Schedules (a “Disclosure Schedule Notice”) containing comments or questions to such updated Disclosure Schedules, as determined in such receiving Party’s sole discretion; provided, that if a receiving Party does not deliver a Disclosure Schedule Notice with respect to the providing Party’s updated Disclosure Schedules within such prescribed time period, the receiving Party shall be deemed to have accepted all such updated Disclosure Schedules.
(c) Notwithstanding any Disclosure Schedule Notice provided by a receiving Party, if any updated Disclosure Schedules provided pursuant to Section 12.11(b) are not acceptable to the receiving Party, as determined in such receiving Party’s sole discretion, then such receiving Party may terminate this Agreement no later than February 3, 2017 by written notice to the providing Party. Either Party’s failure to terminate this Agreement in accordance with the terms of the immediately preceding sentence shall constitute such Party’s deemed acceptance of such updated Disclosure Schedules.
(d) The Disclosure Schedules referred to herein shall be construed with and as an integral part of this Agreement to the same extent as if they were set forth verbatim herein. Disclosure of any fact or item in any Disclosure Schedule hereto referenced by a particular Section in this Agreement shall be deemed to have been disclosed with respect to each other applicable Section in this Agreement if it is readily apparent from the disclosure that it applies to another Section. Neither the specification of any dollar amount in any representation or warranty contained in this Agreement nor the inclusion of any specific item in any Schedule hereto is intended to vary the definition of “Material Adverse Effect” or to imply that such amount, or higher or lower amounts, or the item so included or other items, are or are not material, and no Party shall use the fact of the setting forth of any such amount or the inclusion of any such item in any dispute or controversy between the Parties as to whether any obligation, item or matter not described herein or included in any Disclosure Schedule is or is not material for purposes of this Agreement. Unless this Agreement specifically provides otherwise, neither the specification of any item or matter in any representation or warranty contained in this Agreement nor the inclusion of any specific item in any Disclosure Schedule hereto is intended to imply that such item or matter, or other items or matters, are or are not in the Ordinary Course of Business, and no Party shall use the fact of the setting forth or the inclusion of any such item or matter in any dispute or controversy between the Parties as to whether any obligation, item or matter not described herein or included in any Disclosure Schedule is or is not in the Ordinary Course of Business for purposes of this Agreement.
| -83- |
(e) For the purposes of this Agreement, (i) words in the singular shall be held to include the plural and vice versa and words of one gender shall be held to include the other gender as the context requires, (ii) the terms “hereof,” “herein,” and “herewith” and words of similar import shall be construed to refer to this Agreement in its entirety and to all of the schedules and not to any particular provision, unless otherwise stated, and (iii) the term “including” shall mean “including, without limitation.”
12.12 Expenses. Except as otherwise provided for in this Agreement, each Party hereto will pay all costs and expenses incurred by it incident to its negotiation and preparation of this Agreement and to its performance and compliance with all agreements and conditions contained herein on its part to be performed or complied with, including the fees, expenses and disbursements of its counsel, accountants, advisors and consultants. Notwithstanding anything to the contrary contained herein, all transfer, documentary, sales, use, stamp, registration and other similar Taxes, and all conveyance fees, recording charges and other similar charges and fees (including any penalties and interest) incurred in connection with the transactions contemplated by this Agreement shall be paid by the Shareholders’ Representative, acting on behalf of the Shareholders.
12.13 References to U.S. Dollars. All references in this Agreement to amounts of money expressed in dollars are references to United States dollar, unless otherwise indicated.
12.14 Specific Performance. The Parties agree that irreparable damage would occur in the event that any of the provisions of this Agreement were not performed in accordance with their specific terms or were otherwise breached. Accordingly, each of the Parties shall be entitled to specific performance of the terms hereof, including an injunction or injunctions to as a remedy for any such breach, prevent breaches of this Agreement and to enforce specifically the terms and provisions of this Agreement, this being in addition to any other remedy to which they are entitled at law or in equity. Each of the Parties further hereby waives (a) any defense in any Action for specific performance that a remedy at law would be adequate and (b) any requirement under any Legal Requirements to post security as a prerequisite to obtaining equitable relief. The Parties further agree that by seeking the remedies provided for in this Section 12.14, the Parties shall not in any respect waive their right to seek any other form of relief that may be available to them under this Agreement, including in the event that the remedies provided for in this Section 12.14 are not available or otherwise are not granted.
| -84- |
DEFINITIONS
13.1 Definitions. As used in this Agreement, and unless the context requires a different meaning, the following terms have the meanings given below.
“Action(s)” mean any claim, action, cause of action, demand, lawsuit, arbitration, inquiry, audit, notice of violation, proceeding, litigation, citation, summons, subpoena or investigation of any nature, civil, criminal, administrative, regulatory or otherwise, whether at law or in equity.
“Affiliate” means any Person that, directly or indirectly through one or more intermediaries, controls, is controlled by, or is under common control with another Person and includes the power to direct or cause the direction of the management and policies of a Person, whether through the ownership of securities, election or appointment of directors, by contract or otherwise; provided, that in the case of the Parent or Company, as applicable, the term “Affiliate” shall include, without limitation, each subsidiary of Parent or Company, as applicable, or and each and every sister corporation or other form of corporate entity of Parent or Company, as applicable.
“AG” has the meaning set forth in Section 4.14(c).
“Agreement” means this Agreement and Plan of Merger and all exhibits and schedules attached hereto, as amended, consolidated, supplemented, updated or replaced by the Parties from time to time.
“Allied IPA” has the meaning set forth in the Recitals.
“Antitrust Agencies” has the meaning set forth in Section 4.14(c).
“Business” means the existing business of Parent or Company, as applicable, as of the Closing and for the twelve (12) months prior to the Closing Date, including, without limitation, providing back-office, practice management and related services to physicians, medical groups and/or hospitals.
“Business Day” means a day other than Saturday, Sunday or any day on which banks located in the State of California are authorized or obligated to close.
“Business Employees” means all employees of the Parent or Company, as applicable, prior to the Closing and all employees of the Surviving Entity subsequent to the Closing.
“Cap” has the meaning set forth in Section 8.6(b).
“Cap Carve Outs” has the meaning set forth in Section 8.6(b).
“CERCLA” means the Comprehensive Environmental Response, Compensation and Liability Act of 1980, as amended through the Closing.
“Certificate” has the meaning set forth in Section 2.1(b)(ii).
| -85- |
“Certificate of Merger” has the meaning set forth in Section 1.3.
“CGCL” has the meaning set forth in the Recitals.
“Claim Notice” has the meaning set forth in Section 8.4(a).
“Closing” has the meaning set forth in Section 1.2.
“Closing Date” has the meaning set forth in Section 1.2.
“Closing Share Payment” has the meaning set forth in Section 2.3.
“CMS” means the Centers for Medicare & Medicaid Services, U.S. Department of Health and Human Services.
“Code” means the Internal Revenue Code of 1986, as amended and the rules and regulations thereunder.
“Company” has the meaning set forth in the Preamble.
“Company Acquisition Proposal” means a tender or exchange offer, proposal for a merger, consolidation, acquisition of assets, acquisition of equity or other business combination involving the Company or any proposal or offer, in each case that would result in the acquisition in any manner of more than 15% of the voting power in, or more than 15% of the fair market value of the business, assets or deposits of, the Company, other than the transactions contemplated by this Agreement.
“Company Adverse Recommendation Change” has the meaning set forth in Section 3.5(a)(ii).
“Company Audited Financial Statements” has the meaning set forth in Section 4.3.
“Company Board” has the meaning set forth in the Recitals.
“Company Cash” means all of the cash and cash equivalents held from time to time by the Company prior to the Closing.
“Company Common Stock” means all of the shares in the equity of the Company that are issued and outstanding immediately prior to the Effective Time.
“Company Consents” means all consents required, by their terms, to consummate the Merger without breaching any relevant contract, lease, permit, license or Legal Requirement.
“Company Distributable Cash” has the meaning set forth in Section 3.13.
“Company Financial Statements” has the meaning set forth in Section 4.3.
“Company Indemnified Parties” has the meaning set forth in Section 8.3.
| -86- |
“Company’s Knowledge” means the knowledge, after due and reasonable internal inquiry, of the Company Board, Kenneth Sim, MD and Thomas Lam, MD on the date hereof and on the Closing Date or the equivalent position held by an individual at the Company. An individual will be deemed to have “knowledge” of a particular fact or matter if such individual has knowledge of facts or other information or matters which (a) are actually known to the person making such statement or (b) are matters that such person can reasonably be expected to know or learn in the normal course of discharging his or her duties.
“Company Share” means any issued and outstanding shares of common stock of the Company.
“Company Shareholders’ Agreement” has the meaning set forth in Section 4.13.
“Company Shareholder Approval” has the meaning set forth in Section 3.10.
“Company Shareholder Meeting” has the meaning set forth in Section 3.10.
“Company Shareholder Meeting Notice” has the meaning set forth in Section 3.10.
“Company Termination Fee” has the meaning set forth in Section 9.3(b).
“Company Unaudited Financial Statements” has the meaning set forth in Section 4.3.
“Company Voting Trust Agreement” has the meaning set forth in Section 4.13.
“Consent and Waiver Agreement” has the meaning set forth in the Recitals.
“Consideration Spreadsheet” has the meaning set forth in Section 2.15.
“Disclosure Schedule” has the meaning set forth in Article IV.
“Disclosure Schedule Notice” has the meaning set forth in Section 12.11(b).
“Disqualification Event” has the meaning set forth in Section 5.26.
“Dispute Notice” has the meaning set forth in Section 10.1.
“Dispute Resolution Process” has the meaning set forth in Section 10.3.
“Dissenters’ Rights Rules” has the meaning set forth in Section 3.16.
“Dissenting Shareholder” has the meaning set forth in Section 3.16.
“Dissenting Shareholder Interests” has the meaning set forth in Section 3.16.
“DOJ” has the meaning set forth in Section 4.14(c).
“Effective Time” has the meaning set forth in Section 1.3.
| -87- |
“Employee Benefit Plan” means each (i) “Employee Benefit Plan” (as such term is defined in Section 3(3) of ERISA) and (ii) each other written or oral plan, policy, program, agreement or arrangement (excluding any employment or consulting agreement) whether currently in place or terminated within the last six years, involving direct or indirect compensation or benefits, including but not limited to, stock option, stock purchase, stock appreciation right or other stock-based incentive compensation, cash bonus or incentive compensation, deferred compensation, unemployment or severance compensation, insurance coverage, performance, retention, holiday pay, vacation pay, fringe benefits, commission, disability benefit or post-retirement compensation, in each case, maintained by Company or its subsidiaries or Parent, as applicable, for any current or former employee, consultant, officer, or director or that the Company or Parent presently sponsors, participates in, is a party or contributes to, or with respect to which the Company or Parent could reasonably be expected to have any liability.
“Encumbrances” means liabilities, levies, claims, charges, assessments, mortgages, security interests, liens, pledges, conditional sales agreements, title retention contracts, rights of first refusal, options to purchase, restrictions and other encumbrances, and agreements or commitments to create or suffer any of the foregoing, other than Permitted Encumbrances.
“End Date” has the meaning set forth in Section 9.1(b)(i).
“Environment” means surface waters, groundwaters, soil, subsurface strata and ambient air.
“Environmental Claim” means any Claim relating in any way to any Environmental Legal Requirements or any Environmental Permit, including (a) any and all Claims by any Governmental Authority for enforcement, cleanup, removal, response, remedial or other actions or damages pursuant to any applicable Environmental Legal Requirements and (b) any and all Claims by any Person seeking damages, contribution, indemnification, cost recovery, compensation or injunctive relief resulting from Hazardous Materials or arising from alleged injury or threat of injury to health, safety or the Environment.
“Environmental Condition” means a condition of the soil, surface waters, groundwater, stream sediments, air and/or similar environmental media, including a condition resulting from any Release or threatened Release of Hazardous Materials, that, by virtue of Environmental Legal Requirements or otherwise, (a) requires notification, investigatory, corrective or remedial measures, and/or (b) comprises a basis for claims against, demands of and/or liabilities of the Company or Parent, as applicable, in respect of the Company’s or Parent’s operations, assets, or Business or any of the Real Property. “Environmental Condition” shall include those conditions identified or discovered before or after the date hereof resulting from any activity, inactivity or operations whatsoever on or before the Closing Date.
| -88- |
“Environmental Legal Requirements” means all Legal Requirements, now or hereafter in effect and as amended, and any judicial or administrative interpretation thereof, including any judicial or administrative order, consent decree or judgment, relating to the environment, health, safety, natural resources or Hazardous Materials, including CERCLA; the Resource Conservation and Recovery Act, 42 U.S.C. §§ 6901 et seq.; the Hazardous Materials Transportation Act, 49 U.S.C. §§ 6901 et seq.; the Clean Water Act, 33 U.S.C. §§ 1251 et seq.; the Toxic Substances Control Act, 15 U.S.C. §§ 2601 et seq.; the Clean Air Act, 42 U.S.C. §§ 7401 et seq.; the Safe Drinking Water Act, 42 U.S.C. §§ 300f et seq.; the Atomic Energy Act, 42 U.S.C. §§ 2011 et seq.; the Federal Insecticide, Fungicide and Rodenticide Act, 7 U.S.C. §§ 136 et seq.; the Occupational Safety and Health Act, 29 U.S.C. §§ 651 et seq.; and comparable state Legal Requirements.
“Environmental Lien” means any lien in favor of any Governmental Authority in connection with any liability under any Environmental Legal Requirements, or damage arising from, or costs incurred by, such Governmental Authority in response to a Release or threatened Release.
“Environmental Permits” means all permits, approvals, registrations, identification numbers, licenses and other authorizations required under or issued pursuant to any applicable Environmental Legal Requirements.
“Equipment” has the meaning set forth in Section 4.16(b).
“ERISA” means the Employee Retirement Income Security Act of 1974, as amended and the rules and regulations thereunder.
“Exchange Agent” has the meaning set forth in Section 2.4(a).
“Exchange Act” means the Securities Exchange Act of 1934, as amended, and the rules and regulations promulgated thereunder.
“Exchange Agreement” has the meaning set forth in the Recitals.
“Exchange Fund” has the meaning set forth in Section 2.4(b).
“Exchange Ratio” has the meaning set forth in Section 2.1(b)(ii).
“Execution Date” has the meaning set forth in the Preamble.
“Executive Administrators” has the meaning set forth in Section 10.1.
“Expiration Date” has the meaning set forth in Section 8.1.
“FTC” has the meaning set forth in Section 4.14(c).
“Fully Diluted Company Shares Outstanding” means the number of Company Shares issued and outstanding immediately prior to the Effective Time.
“GAAP” means United States generally accepted accounting principles, consistently applied.
“General Enforceability Exceptions” means the effect and limitations as to enforceability caused by bankruptcy, insolvency, moratorium, reorganization, fraudulent conveyance laws, laws affecting the enforcement of creditors’ rights, the application of equitable principles and judicial discretion (regardless of whether enforcement is sought in equity or at law) and by the covenants of commercial reasonableness and good faith and fair dealing which may be implied by law into contracts.
| -89- |
“Governmental Antitrust Authority” has the meaning set forth in Section 3.8(b).
“Governmental Authorities” means all agencies, authorities, bodies, boards, commissions, courts, instrumentalities, legislatures and offices of any nature whatsoever of any federal, state, county, district, municipal, city, foreign or other government or quasi-government unit or political subdivision, and private arbitration panels or dispute resolution makers.
“Hazardous Materials” means (a) petroleum and petroleum products, radioactive materials, asbestos-containing materials, urea formaldehyde foam insulation, transformers or other equipment that contain polychlorinated biphenyls, and radon gas, (b) any other chemicals, materials or substances defined as or included in the definition of “hazardous substances”, “hazardous wastes”, “hazardous materials”, “extremely hazardous wastes”, “restricted hazardous wastes,” “toxic substances”, “toxic pollutants,” “medical waste,” “biohazardous waste,” “contaminants” or “pollutants,” or words of similar import, under any applicable Environmental Legal Requirements, and (c) any other chemical, material or substance that is regulated by or subject to standards of liability pursuant to any Environmental Legal Requirements.
“HIPAA” has the meaning set forth in Section 4.14(b).
“Holdback Shares” has the meaning set forth in Section 2.3.
“Holdback Release Date” means the second anniversary of the Closing Date.
“HSR Act” means the Hart-Scott-Rodino Antitrust Improvements Act of 1976, as amended.
“Indebtedness” means any indebtedness, liabilities or other obligation (including liability for principal, accrued interest, penalties, fees and premiums) (i) for borrowed money, or with respect to deposits or advances of any kind (other than deposits, advances or excess payments accepted in connection with the sale of products or services in the Ordinary Course of Business) whether current, short-term or long-term, secured or unsecured, and all accrued interest, premiums, penalties, expenses, breakage fees and other obligations relating thereto, (ii) evidenced by bonds, debentures, notes or similar instruments, (iii) upon which interest charges are customarily paid (other than obligations accepted in connection with the purchase of products or services in the Ordinary Course of Business), (iv) under conditional sale or other title retention agreements, (v) issued or assumed as the deferred purchase price of property or services (other than accounts payable to suppliers incurred in the Ordinary Course of Business and paid when due), (vi) of others secured by (or for which the holder of such liabilities has an existing right, contingent or otherwise, to be secured by) any Encumbrance or security interest on property owned or acquired by the Person in question whether or not the obligations secured thereby have been assumed, (vii) under leases required to be accounted for as capital leases under GAAP, (viii) any liability of with respect to interest rate swaps, collars, caps and similar hedging obligations, and (ix) any guaranty with respect to any of the foregoing.
| -90- |
“Indemnifying Parties” has the meaning set forth in Section 8.4(a).
“Intellectual Property” means all intellectual property and proprietary rights, including: (i) all trademarks, service marks, trade dress, trade names, logos, corporate names, domain names and other uniform resource locators (URLs), and social media usernames and profile names, including all goodwill associated therewith, and all registrations and applications therefor; (ii) all registered and unregistered copyrights and all copyrightable works, together with all copyright registrations and applications therefor; (iii) all inventions and discoveries (whether patentable or unpatentable and whether or not reduced to practice), all improvements thereto, and all patents, patent applications, and patent disclosures, together with all reissuances, continuations, continuations-in-part, revisions, extensions, and reexaminations thereof; (iv) all trade secrets, confidential information, ideas, research and development, formulas, compositions, processes, techniques, know-how, technical and computer data, customer and supplier lists, financial, business and marketing plans and related information; and (v) all computer software and computerized databases, in both source code and object code forms.
“Knox-Keene Act” means the California Knox-Keene Health Care Service Plan Act of 1975, as amended, and regulations thereunder.
“Legal Requirements” means, with respect to any Person, all statutes, ordinances, bylaws, codes, rules, regulations, restrictions, orders, judgments, writs, injunctions, decrees, determinations or awards of any Governmental Authority having jurisdiction over such Person or any of such Person’s assets or businesses.
“Letter Agreement” has the meaning set forth in the Recitals.
“Letter of Transmittal” has the meaning set forth in Section 2.4(c).
“Lock-Up Agreement” has the meaning set forth in the Recitals.
“Losses” of a Person means any and all losses, liabilities, damages, claims, actions, causes of action, Taxes, awards, judgments, costs and expenses (including interest, penalties, reasonable attorneys’, consultants’ and experts’ fees and expenses) suffered or incurred by such Person whether or not arising out of Third Person Claims.
“Material Adverse Effect” means any change, effect, fact, event, occurrence, state of facts or development that, individually or together with any other changes, effects, facts, events, occurrences, states of facts or developments, materially and adversely affects, or could reasonably be expected to materially and adversely affect (a) the consolidated financial condition, results of operations, assets, liabilities, income, business or prospects of the Company or (b) the ability of the applicable Party to perform its obligations under this Agreement or (c) Parent’s ability to operate the Surviving Entity; provided, however, that Material Adverse Effect shall exclude any adverse changes or conditions as and to the extent such changes or conditions relate to or result from (i) general economic conditions or other conditions generally affecting the industry in which the Company’s Business competes; or (ii) public or industry knowledge of the transactions contemplated by this Agreement (including, without limitation, any action or inaction by the Company’s Business Employees and vendors) except if such conditions in either clause (i) or clause (ii) above have a disproportionate impact on the Company’s Business.
| -91- |
“Material Contracts” has the meaning set forth in Section 4.5(a).
“Maverick IPA” has the meaning set forth in the Recitals.
“Maverick Purchase Agreement” has the meaning set forth in the Recitals.
“Merger” has the meaning set forth in the Recitals.
“Merger Consideration” has the meaning set forth in Section 2.3.
“Merger Sub” has the meaning set forth in the Preamble.
“Multiemployer Plan” has the meaning set forth in section 3(37) of ERISA or section 4001(a)(3) of ERISA.
“Nondisclosure Agreement” means the Mutual Nondisclosure Agreement, dated December 10, 2015, between Parent and the Company.
“Order” means any judgment, order, stipulation, arbitration, decision, award, injunction or decree of any federal, foreign, state or local Governmental Authority.
“Ordinary Course of Business” means, with respect to an action taken by a Person, such action is consistent with the past practices and custom of such Person and is taken in the ordinary course of business of the normal day to day operations of such Person.
“Other Plan” means any contract, program or arrangement which provides cash or non-cash benefits or perquisites to current or former Business Employees of the Company or Parent, as applicable, but which is not an Employee Benefit Plan.
“Parent” has the meaning set forth in the Preamble.
“Parent Acquisition Proposal” means a tender or exchange offer, proposal for a merger, consolidation, acquisition of assets, acquisition of equity or other business combination involving Parent or any other proposal or offer, in each case that would result in the acquisition in any manner of more than 15% of the voting power in, or more than 15% of the fair market value of the business, assets or deposits of Parent, other than the transactions contemplated by this Agreement.
“Parent Adverse Recommendation Change” has the meaning set forth in Section 3.5(b)(ii).
“Parent Audited Financial Statements” has the meaning set forth in Section 5.4.
“Parent Financial Statements” has the meaning set forth in Section 5.4.
“Parent Indemnified Parties” has the meaning set forth in Section 8.2.
“Parent Indemnity Shares” has the meaning set forth in Section 8.3(b).
| -92- |
“Parent Material Contracts” has the meaning set forth in Section 5.6.
“Parent Real Property Leases” has the meaning set forth in Section 5.19(b).
“Parent Share” means any issued and outstanding shares of common stock, par value $0.001 par value, of the Parent; provided, that, for the purpose of the Parent Shareholder Approval, “Parent Shares” shall include preferred stock of Parent entitled to vote with common stock of Parent on an as-converted basis.
“Parent Shareholder Approval” has the meaning set forth in Section 3.11.
“Parent Shareholder Meeting” has the meaning set forth in Section 3.9(a).
“Parent Shareholder Meeting Notice” has the meaning set forth in Section 3.11.
“Parent Termination Fee” has the meaning set forth in Section 9.3(c).
“Parent Unaudited Financial Statements” has the meaning set forth in Section 5.4.
“Parent Warrants” has the meaning set forth in Section 3.13.
“Parent’s Knowledge” means the knowledge, after due and reasonable internal inquiry, of the Parent’s board of directors, Warren Hosseinion, M.D. and Gary Augusta on the date hereof and on the Closing Date or the equivalent position held by an individual at Parent. An individual will be deemed to have “knowledge” of a particular fact or matter if such individual has knowledge of facts or other information or matters which (a) are actually known to the person making such statement, or (b) are matters that such person can reasonably be expected to know or learn in the normal course of discharging his or her duties.
“Party(ies)” has the meaning set forth in the Preamble.
“PBGC” means the Pension Benefit Guaranty Corporation.
“Per Share Merger Consideration” means an amount equal to the Merger Consideration divided by the Fully Diluted Company Shares Outstanding.
“Permits and Licenses” means all of the permits, licenses, registrations, certifications, approvals and provider numbers held by Company or Parent, as applicable, relating to such Party’s respective Business.
“Permitted Encumbrances” means (a) liens for Taxes and other governmental charges and assessments which are not yet due and payable or which are being contested in good faith and for which adequate reserves have been established in accordance with GAAP, (b) liens of landlords and liens of carriers, warehousemen, mechanics and materialmen and other like liens arising in the Ordinary Course of Business for sums not yet due and payable or which are being contested in good faith, (c) other liens or imperfections on property which are not material in amount or do not materially detract from the value of or materially impair the existing use of the property affected by such lien or imperfections, (d) liens relating to deposits made in the Ordinary Course of Business in connection with workers’ compensation, unemployment insurance and other types of social security or to secure the performance of leases, trade contracts or other similar agreements, (e) purchase money liens on personal property acquired in the Ordinary Course of Business, (f) liens specifically identified in the Company Financial Statements, (g) liens securing executory obligations under any lease that constitutes a “capital lease” under GAAP, and (h) any utility company rights, easements and franchises.
| -93- |
“Person” means any individual, company, body corporate, association, partnership, firm, joint venture, trust, trustee or Governmental Authority.
“Plan Contracts” means all contracts and agreements, regardless of form, between any healthcare entities to which the Company or Parent, as applicable, provides administrative or other services, on the one hand, and health maintenance organizations, managed care organizations, third party administrators and other purchasers of health care services, on the other.
“Pro Rata Portion” means, with respect to any Shareholder, a fraction, the numerator of which is the number of Company Shares held by such Shareholder immediately prior to the Effective Time and the denominator of which is the Fully Diluted Company Shares Outstanding.
“Provider Contract” has the meaning set forth in Section 4.5(a).
“Proxy Clearance Date” has the meaning set forth in Section 3.9(a).
“Proxy Statement” has the meaning set forth in Section 3.9(a).
“Proxy Materials” has the meaning set forth in Section 3.9(a).
“Proxy/Registration Statement” has the meaning set forth in Section 3.9(a).
“Real Property” means the real property owned or leased by the Company or Parent, as applicable, together with, to the extent leased by the Company or Parent, as applicable, all buildings and other structures, facilities or improvements currently or hereafter located thereon, all fixtures, systems, equipment and items of personal property of the Company or Parent, as applicable, attached or appurtenant thereto and all easements, licenses, rights and appurtenances relating to the foregoing.
“Real Property Leases” has the meaning set forth in Section 4.18(b).
“Registration Statement” has the meaning set forth in Section 3.9(a).
“Registration Statement Effectiveness Date” has the meaning set forth in Section 3.9(a).
“Release” means disposing, discharging, injecting, spilling, leaking, leaching, dumping, emitting, escaping, emptying, seeping, placing and the like into or upon any land or water or air or otherwise entering into the Environment.
| -94- |
“Remedial Action” means all action to (a) investigate, evaluate, assess, test, monitor, clean up, remove, respond to, treat, abate, remedy, correct or handle in any other way the Release or presence of Hazardous Materials in the Environment, whether on-site or off-site; (b) prevent the Release of Hazardous Materials so that they do not migrate, endanger or threaten to endanger public health or the Environment; or (c) perform remedial investigations, feasibility studies, corrective actions, closures, or post-remedial or post-closure studies, investigations, operations, maintenance and monitoring.
“Reportable Event” has the meaning set forth in section 4043 of ERISA.
“SEC” means the United States Securities and Exchange Commission.
“SEC Reports” means all reports, schedules, forms, statements and other documents, including exhibits and documents incorporated by reference therein, required to be filed by Parent under the Securities Act and the Exchange Act, including pursuant to Section 13(a) or 15(d) thereof.
“Securities Act” means the Securities Act of 1933, as amended.
“Shareholder” or “Shareholders” has the meanings set forth in the Recitals.
“Shareholder Action” has the meaning set forth in Section 11.5.
“Shareholder Interests” means the Shareholders’ entire interest in the Company.
“Shareholder Representations” has the meaning set forth in Section 6.2(c)(ix).
“Shareholders’ Representative” has the meaning set forth in the Preamble.
“Superior Company Acquisition Proposal” means a written Company Acquisition Proposal that the board of directors of Company concludes in good faith to be more favorable from a financial point of view to its shareholders than the Merger, (a) after receiving the advice of its financial advisors, (b) after taking into account the likelihood of consummation of the Merger on the terms set forth therein and (c) after taking into account all legal (with the advice of outside counsel), financial (including the financing terms of any such proposal), regulatory and other aspects of such proposal and any other relevant factors permitted under applicable Legal Requirements; provided, that for purposes of the definition of “Superior Company Acquisition Proposal,” the references to “15%” in the definition of Company Acquisition Proposal shall be deemed to be references to “50%”.
“Superior Parent Acquisition Proposal” means a written Parent Acquisition Proposal that the board of directors of Parent concludes in good faith to be more favorable from a financial point of view to its shareholders than the Merger, (a) after receiving the advice of its financial advisors, (b) after taking into account the likelihood of consummation of the Merger on the terms set forth therein and (c) after taking into account all legal (with the advice of outside counsel), financial (including the financing terms of any such proposal), regulatory and other aspects of such proposal and any other relevant factors permitted under applicable Legal Requirements; provided, that for purposes of the definition of “Superior Parent Acquisition Proposal,” the references to “15%” in the definition of Parent Acquisition Proposal shall be deemed to be references to “50%”.
| -95- |
“Surviving Entity” has the meaning set forth in Section 1.1.
“Tax” means any income, unrelated business income, gross receipts, license, payroll, employment, excise, severance, occupation, privilege, premium, windfall profits, environmental (including taxes under Section 59A of the Code), customs duties, capital stock, franchise, profits, withholding, social security, unemployment, disability, real property, personal property, stamp, sales, use, transfer, registration, escheat, unclaimed property, value added, alternative or add-on minimum, estimated or other tax, assessment, charge, levy or fee of any kind whatsoever, including payments or services in lieu of Taxes, interest or penalties on and additions to all of the foregoing, which are due or alleged to be due to any Governmental Authority, whether disputed or not.
“Tax Return” means any return, declaration, report, claim for refund, information return or statement, including schedules and attachments thereto and amendments, relating to Taxes.
“Third Party” means a Person other than the Parties to this Agreement.
“Third Person Claim” has the meaning set forth in Section 8.5(a).
“Threshold Amount” has the meaning set forth in Section 8.6(a).
“Transaction Documents” means, with respect to a Party hereto, all agreements, certificates and other instruments to be delivered by such Party under this Agreement, including, without limitation, the Voting Agreement, the Shareholder Lock-Up Agreement, the Exchange Agent Agreement, the Working Capital Note, the Consent and Waiver Agreement, the Letter of Transmittal and the Shareholder Representations.
“Transaction Expenses” means (a) the aggregate of the unpaid fees and expenses payable by the Company and the Shareholders’ Representative in connection with this Agreement and the transactions contemplated hereby, including, without limitation, the fees and expenses related to any HSR Act filing payable by the Company pursuant to Section 3.8, the fees and expenses of Vantage Point Advisors and any other advisors engaged by the Company and the Shareholders’ Representative in connection with the transactions contemplated hereby, (b) any unpaid change in control, severance, parachute or similar payments, bonuses or other compensation that are required or planned to be made, paid, vested and accelerated by the Company in connection with or by virtue of the consummation of the transactions contemplated by this Agreement and (c) all payroll, employment or other Taxes required to be paid by Parent or the Company with respect to the amounts described in clauses (a) and (b).
“Voting Agreement” has the meaning set forth in the Recitals.
“Working Capital Loan Amount” has the meaning set forth in Section 3.14.
“Working Capital Note” has the meaning set forth in Section 3.14.
“WARN Act” has the meaning set forth in Section 4.7(h).
[Signatures Page Follows]
| -96- |
IN WITNESS WHEREOF, the Parties have executed this Agreement as of the Execution Date.
| PARENT: | Apollo Medical Holdings, Inc., a Delaware corporation | ||
| By: | /s/ Warren Hosseinion, M.D. | ||
| Name: | Warren Hosseinion, M.D. | ||
| Title: | Chief Executive Officer | ||
| MERGER SUB: | Apollo Acquisition Corp., a California corporation | ||
| By: | /s/ Warren Hosseinion, M.D. | ||
| Name: | Warren Hosseinion, M.D. | ||
| Title: | Chief Executive Officer | ||
| THE COMPANY: | Network Medical Management, Inc., a California corporation | ||
| By: | /s/ Thomas S. Lam, M.D. | ||
| Name: | Thomas S. Lam, M.D. | ||
| Title: | Chief Executive Officer | ||
|
SHAREHOLDERS’ REPRESENTATIVE: |
/s/ Kenneth Sim, M.D. |
| Kenneth Sim, M.D. |
Exhibit A
Form of Voting Agreement
Exhibit B
Form of Shareholder Lock-Up Agreement
Exhibit C
Form of Exchange Agent Agreement
Exhibit D
Consent and Waiver Agreement
-ii-
Exhibit E
Form of Letter of Transmittal
-iii-
Exhibit F
Working Capital Note
Exhibit G
Shareholder Representations
-v-
Exhibit H-1
Certificate of Amendment
-vi-
Exhibit H-2
Amendment to Bylaws
-vii-
Schedule 7.3
Post-Closing Board of Directors and Post-Closing Officers
Class I Directors:
Michael F. Eng (Company designee)
Thomas Lam, M.D. (Company designee)
David G. Schmidt (Parent Designee)
Class II Directors:
Mitchell W. Kitayama (Company
designee)
Kenneth Sim, M.D. (Company designee)
Mark Fawcett (Parent designee)
Class III Directors:
Li Yu (Company designee)
Warren Hosseinion, M.D. (Parent designee)
Gary Augusta (Parent designee)
Post-Closing Officers:
| Kenneth Sim, M.D. | Executive Chairman | |
| Thomas Lam, M.D. | Co-Chief Executive Officer | |
| Warren Hosseinion, M.D. | Co-Chief Executive Officer | |
| Gary Augusta | President | |
| Hing Ang | Chief Operating Officer | |
| Mihir Shah | Chief Financial Officer | |
| Adrian Vazquez, M.D. | Co-Chief Medical Officer | |
| Albert Young, M.D. | Co-Chief Medical Officer |
-viii-
AMENDMENT TO AGREEMENT AND PLAN OF MERGER
This Amendment to Agreement and Plan of Merger (this “Amendment”) is made and entered into as of March 30, 2017 by and among Apollo Medical Holdings, Inc., a Delaware corporation (“Parent”), Apollo Acquisition Corp., a California corporation (“Merger Sub”), Network Medical Management, Inc., a California corporation (the “Company”), and Kenneth Sim, M.D. (the “Shareholders’ Representative”). Parent, Merger Sub, the Company and the Shareholders’ Representative shall sometimes be referred to herein collectively as the “Parties” and individually as a “Party.” Capitalized terms used herein have the meanings ascribed to them in Article XIII of the Merger Agreement.
WHEREAS, Parent, the Company, Merger Sub and the Shareholders’ Representative are parties to the Agreement and Plan of Merger dated as of December 21, 2016 (the “Merger Agreement”);
WHEREAS, Section 12.6 of the Merger Agreement provides that the Merger Agreement may not be amended except by a written amendment signed by all of the Parties thereto; and
WHEREAS, the Parties desire to amend the Merger Agreement as set forth below.
NOW, THEREFORE, in consideration of the premises and the mutual promises contained herein and for other good and valuable consideration, the receipt and sufficiency of which are hereby acknowledged, the parties hereto hereby agree as follows:
1. Amendment to Section 2.1(b)(ii). Section 2.1(b)(ii) of the Merger Agreement is hereby amended and restated as follows:
“(ii) Subject to Sections 2.1(b)(i) and 2.8, each Company Share issued and outstanding immediately prior to the Effective Time shall be converted into the right to receive such number of fully paid and nonassessable Parent Shares that would result in the Shareholders having a right to receive an aggregate number of Parent Shares immediately following the Effective Time that represents eighty-two percent (82%) of the total issued and outstanding Parent Shares immediately following the Effective Time, assuming there are no Dissenting Shareholder Interests as of the Effective Time (the “Exchange Ratio”). Notwithstanding the foregoing, and for the avoidance of doubt, for purposes of calculating the Exchange Ratio, the aggregate number of Parent Shares held by the Shareholders immediately following the Effective Time shall exclude (i) any Parent Shares owned by the Shareholders immediately prior to the Effective Time, (ii) the Parent Warrants, and (iii) any Parent Shares issued or issuable to the Shareholders pursuant to the exercise of the Parent Warrants. Notwithstanding the foregoing, and for the avoidance of doubt, for purposes of calculating the Exchange Ratio, the total number of issued and outstanding Parent Shares immediately following the Effective Time shall exclude four hundred ninety-nine thousand (499,000) Parent Shares issued or issuable pursuant to the Securities Purchase Agreement dated as of March 30, 2017, between Parent and Alliance Apex, LLC (the “Purchase Agreement”). All such Company Shares, when so converted, shall no longer be outstanding and shall automatically be cancelled and shall cease to exist, and each holder of a certificate that immediately prior to the Effective Time represented any such Company Shares (each, a “Certificate”) and each holder of Company Shares held in book-entry form shall, in each case, cease to have any rights with respect thereto, except the right to receive the Merger Consideration and any cash in lieu of fractional Parent Shares to be issued or paid in consideration therefor, and any rights to which holders of Company Shares become entitled in accordance with Section 3.16.”
| A-1 |
2. Amendment to Section 2.3. Section 2.3 of the Merger Agreement is hereby amended and restated as follows:
“2.3 Merger Consideration. Subject to the terms and conditions of this Agreement, the aggregate consideration to be paid by Parent shall be the Merger Consideration. The “Merger Consideration” is an amount equal to the total of:
| · | Ninety percent (90%) of the aggregate number of Parent Shares the Shareholders are entitled to receive pursuant to Section 2.1(b)(ii) (the “Closing Share Payment”), plus |
| · | the remainder, if any, from the holdback shares (initially, ten percent (10%) of the aggregate number of Parent Shares the Shareholders are entitled to receive pursuant to Section 2.1(b)(ii) (the “Holdback Shares”)), plus |
| · | Eight hundred fifty thousand (850,000) warrants of the Parent exercisable at eleven dollars ($11.00) per share (the “Closing Warrant Payment” and together with the Closing Share Payment, the “Closing Payment”).” |
3. Amendment to Section 2.4(b). Section 2.4(b) of the Merger Agreement is hereby amended and restated as follows:
“(b) Deposit of Merger Consideration. At or prior to the Effective Time, Parent shall deposit with the Exchange Agent, in trust for the benefit of the Shareholders, in accordance with this Article II and through the Exchange Agent, sufficient cash, the Closing Warrant Payment and Parent Shares to make all other deliveries pursuant to this Article II; provided, however, that if the Closing Payment shall for any reason not include sufficient cash, warrants or Parent Shares to make all such deliveries, upon notice thereof from the Exchange Agent to Parent, at or prior to the Effective Time, Parent shall from time to time promptly deposit with the Exchange Agent sufficient cash, warrants and Parent Shares to make such Closing Payment. Any cash, warrants or Parent Shares deposited with the Exchange Agent shall be collectively referred to as the “Exchange Fund.””
4. Amendment to Section 2.15. Section 2.15 of the Merger Agreement is hereby amended and restated as follows:
| A-2 |
“2.15 Consideration Spreadsheet. At least three (3) Business Days before the Closing Date, the Company shall prepare and deliver to Parent a spreadsheet (the “Consideration Spreadsheet”), certified by the President of the Company, which shall set forth, as of the Closing Date, (i) such Person’s address and, if available to the Company, social security number (or tax identification number, if applicable), (ii) the number of Company Shares held by such Person, (iii) the respective certificate number(s) representing such Company Shares, (iv) the respective date(s) of acquisition of such Company Shares, (v) the Pro Rata Portion applicable to such Person, (vi) the number of Parent Shares issuable to such Person at the Closing in respect of such Company Shares, (vii) the number of Parent Shares comprising the Holdback Shares on behalf of such Person, (viii) the number of warrants of Parent (from the Closing Warrant Payment) issuable to such Person at the Closing based on the Pro Rata Portion applicable to such Person, (ix) any amounts required to be withheld and (x) such other information relevant thereto or that Parent may reasonably request.”
5. Amendment to Section 6.3(c)(i). Section 6.3(c)(i) of the Merger Agreement is hereby amended and restated as follows:
“(i) deposit of the Closing Payment in such manner as designated by the Exchange Agent;”
6. Amendment to Section 13.1. The following definitions are hereby added to Section 13.1 of the Merger Agreement:
“Closing Payment” has the meaning set forth in Section 2.3.
“Closing Warrant Payment” has the meaning set forth in Section 2.3.
“Purchase Agreement” has the meaning set forth in Section 2.1(b)(ii).
7. Effect of Amendment. Except as expressly set forth in this Amendment, the Merger Agreement remains unchanged and in full force and effect.
8. Governing Law; Exclusive Jurisdiction. All disputes, claims or controversies arising out of or relating to this Amendment or the transactions contemplated hereby shall be construed in accordance with and governed by the internal laws of the State of California without giving effect to any choice or conflict of law provision or rule (whether of the State of California or any other jurisdiction) that would cause the application of laws of any jurisdiction other than those of the State of California
9. Execution of Amendment; Counterparts; Electronic Signature. This Amendment may be executed in multiple counterparts, each of which shall be deemed an original and all of which shall constitute one and the same instrument. The exchange of copies of this Amendment and signature pages by facsimile transmission, by electronic mail in portable document format form, or by any other electronic means intended to preserve the original graphic and pictorial appearance of a document, or by combination of such means, shall constitute effective execution and delivery of this Amendment as to the Parties and may be used in lieu of the original Amendment for all purposes.
| A-3 |
10. Modification. This Amendment may not be amended except by a written amendment signed by all of the Parties hereto.
[Signature Page Follows]
| A-4 |
IN WITNESS WHEREOF, each of the parties hereto has caused this Amendment to Agreement and Plan of Merger to be duly executed on its behalf as of the day and year first above written.
| PARENT: | Apollo Medical Holdings, Inc., a Delaware corporation | ||
| By: | /s/ Warren Hosseinion | ||
| Name: | Warren Hosseinion, M.D. | ||
| Title: | Chief Executive Officer | ||
| MERGER SUB: | Apollo Acquisition Corp., a California corporation | ||
| By: | /s/ Warren Hosseinion | ||
| Name: | Warren Hosseinion, M.D. | ||
| Title: | Chief Executive Officer | ||
| THE COMPANY: | Network Medical Management, Inc., a California corporation | ||
| By: | /s/ Thomas Lam | ||
| Name: | Thomas Lam | ||
| Title: | CEO | ||
| SHAREHOLDERS’ REPRESENTATIVE: |
|
||
| Kenneth Sim, M.D. | |||
| A-5 |
AMENDMENT NO. 2 TO AGREEMENT AND PLAN OF MERGER
This Amendment No. 2 to Agreement and Plan of Merger (this “Amendment”) is made and entered into as of October 17, 2017 by and among Apollo Medical Holdings, Inc., a Delaware corporation (“Parent”), Apollo Acquisition Corp., a California corporation (“Merger Sub”), Network Medical Management, Inc., a California corporation (the “Company”), and Kenneth Sim, M.D. (the “Shareholders’ Representative”). Parent, Merger Sub, the Company and the Shareholders’ Representative shall sometimes be referred to herein collectively as the “Parties” and individually as a “Party.” Capitalized terms used herein have the meanings ascribed to them in Article XIII of the Merger Agreement.
WHEREAS, Parent, the Company, Merger Sub and the Shareholders’ Representative are parties to the Agreement and Plan of Merger dated as of December 21, 2016, as amended on March 30, 2017 (the “Merger Agreement”);
WHEREAS, Section 12.6 of the Merger Agreement provides that the Merger Agreement may be amended by a written amendment signed by all of the Parties thereto; and
WHEREAS, the Parties desire to amend the Merger Agreement as set forth below;
NOW, THEREFORE, in consideration of the premises and the mutual promises contained herein and for other good and valuable consideration the receipt and sufficiency of which are hereby acknowledged, the parties hereto hereby agree as follows:
1. Amendment to Section 1.5(b). Section 1.5(b) of the Merger Agreement is hereby deleted in its entirety.
2. Amendment to Section 2.1(b)(ii). Section 2.1(b)(ii) of the Merger Agreement is hereby amended and restated as follows:
“(ii) Subject to Sections 2.1(b)(i) and 2.8, each Company Share issued and outstanding immediately prior to the Effective Time shall be converted into the right to receive such number of fully paid and nonassessable Parent Shares that would result in the Shareholders having a right to receive (I) an aggregate number of Parent Shares immediately following the Effective Time that represents eighty-two percent (82%) of the total issued and outstanding Parent Shares immediately following the Effective Time, assuming there are no Dissenting Shareholder Interests as of the Effective Time (the “Exchange Ratio”), plus (II) an aggregate of two million five hundred sixty-six thousand six hundred sixty-six (2,566,666) Parent Shares (the “Additional Parent Shares”), assuming there are no Dissenting Shareholder Interests as of the Effective Time. In addition, each Shareholder shall be entitled to receive such Shareholder’s Pro Rata Portion of the aggregate of eight hundred fifty thousand (850,000) warrants of Parent exercisable at eleven dollars ($11.00) per share and the aggregate of nine hundred thousand (900,000) warrants of Parent exercisable at ten dollars ($10.00) per share. Notwithstanding the foregoing, and for the avoidance of doubt, for purposes of calculating the Exchange Ratio, the aggregate number of Parent Shares held by the Shareholders immediately following the Effective Time shall exclude (i) any Parent Shares owned by the Shareholders immediately prior to the Effective Time, (ii) the Additional Parent Shares and (iii) any Parent Shares issuable to the Shareholders pursuant to the exercise of the Parent Warrants and/or the Closing Warrant Payment. Notwithstanding the foregoing, and for the avoidance of doubt, for purposes of calculating the Exchange Ratio, the total number of issued and outstanding Parent Shares immediately following the Effective Time shall exclude four hundred ninety-nine thousand (499,000) Parent Shares issued or issuable pursuant to the Securities Purchase Agreement dated as of March 30, 2017, between Parent and Alliance Apex, LLC (the “Purchase Agreement”). All such Company Shares, when so converted, shall no longer be outstanding and shall automatically be cancelled and shall cease to exist, and each holder of a certificate that immediately prior to the Effective Time represented any such Company Shares (each, a “Certificate”) and each holder of Company Shares held in book-entry form shall, in each case, cease to have any rights with respect thereto, except the right to receive such Shareholder’s Pro Rata Portion of the Merger Consideration and any cash in lieu of fractional Parent Shares to be issued or paid in consideration therefor, and any rights to which holders of Company Shares become entitled in accordance with Section 3.16.”
| A-6 |
3. Amendment to Section 2.3. Section 2.3 of the Merger Agreement is hereby amended and restated as follows:
“2.3 Merger Consideration. Subject to the terms and conditions of this Agreement, the aggregate consideration to be paid by Parent shall be the Merger Consideration. The “Merger Consideration” is an amount equal to the total of:
| · | ninety percent (90%) of the aggregate number of Parent Shares the Shareholders are entitled to receive pursuant to Section 2.1(b)(ii) (the “Closing Share Payment”), plus |
| · | eight hundred fifty thousand (850,000) warrants of Parent exercisable at eleven dollars ($11.00) per share, plus nine hundred thousand (900,000) warrants of Parent exercisable at ten dollars ($10.00) per share (collectively, the “Closing Warrant Payment,” and together with the Closing Share Payment, the “Closing Payment”), which warrants shall be in substantially the same form as the Series B Parent Warrants, plus |
| · | the remainder, if any, from the holdback shares (initially, ten percent (10%) of the aggregate number of Parent Shares the Shareholders are entitled to receive pursuant to Section 2.1(b)(ii) (the “Holdback Shares”)).” |
4. Amendment to Section 3.2(ii). Section 3.2(ii) of the Merger Agreement is hereby amended and restated as follows:
“(ii) except as set forth in Schedule 3.2 attached and except as authorized by the Company Board for issuances, deliveries and/or sales prior to the Closing of common stock of the Company or options to purchase common stock of the Company which options must be exercised or cancelled prior to, and cannot be outstanding at, the Closing, issue, deliver, sell, authorize, pledge or otherwise encumber any shares of capital stock, stock options or any securities convertible into shares of capital stock or other equity, or subscriptions, rights, warrants or options to acquire any shares of capital stock or other equity or any securities convertible into shares of capital stock or other equity, or enter into other agreements or commitments of any character obligating the Company to issue any such shares or convertible securities;”
5. Amendment to Section 3.2(x). Section 3.2(x) of the Merger Agreement is hereby amended and restated as follows:
“(x) except as authorized by the Company Board for issuances, deliveries and/or sales prior to the Closing of common stock of the Company or options to purchase common stock of the Company which options must be exercised or cancelled prior to, and cannot be outstanding at, the Closing, change its authorized capital structure or authorize for issuance, issue, sell, grant, pledge or dispose of, or agree or commit to issue, sell, grant, pledge or dispose of (whether through the issuance or granting of options, warrants, commitments, subscriptions, rights to purchase or otherwise) any stock of any class of the Company or any other securities or equity equivalents;”
6. Amendment to Section 3.13. Section 3.13 of the Merger Agreement is hereby amended to add the following new sentence at the end of such Section:
“For the avoidance of doubt, notwithstanding anything to the contrary in this Agreement, any other agreement, or the governing documents of Parent, the Parties hereby acknowledge and agree that in no event prior to Closing (or earlier termination of this Agreement in accordance with the terms hereof) shall Company take any action to cause a dividend or distribution of or take any other action with respect to the Series A preferred stock and Series B preferred stock of Parent held by Company (the “Preferred Stock”), and the Preferred Stock shall continue to be held by Company until and through the Effective Time such that the value of the Preferred Stock shall thereby effectively be relinquished at the Effective Time, if and only if the Closing occurs and the Agreement has not been terminated, by Company and the Shareholders in exchange for the Merger Consideration.”
| A-7 |
7. Amendment to Section 3.14. Section 3.14 of the Merger Agreement is hereby amended and restated as follows:
“3.14 Working Capital Loans. The Company shall provide a working capital loan to Parent in the principal amount of Nine Million Dollars ($9,000,000), which shall be evidenced by a promissory note in substantially the form of Exhibit F attached hereto and shall be convertible into Parent Shares in accordance with the terms thereof (the “Convertible Note”). Of such amount, (A) Five Million Dollars ($5,000,000) was previously disbursed to Parent pursuant to a working capital loan evidenced by that certain Promissory Note dated January 3, 2017 (the “Original Note”) and (B) Four Million Dollars ($4,000,000) will be used for working capital and shall be funded by wire of immediately available funds to an account designated by Parent on October 17, 2017. Upon its execution, (i) the Convertible Note shall amend, restate and replace the Original Note, which shall thereupon be canceled together with the note previously executed by the Company and payable to the Shareholders’ Representative on behalf of the Shareholders in the principal amount of the Original Note and (ii) the entire outstanding principal balance of the Original Note, all accrued and unpaid interest thereon, and all other applicable fees, costs and charges, if any, shall be rolled into and become payable pursuant to the terms of the Convertible Note. For the avoidance of doubt, notwithstanding anything to the contrary in this Agreement, any other agreement, or the governing documents of Parent, the Parties hereby acknowledge and agree that in no event prior to Closing (or earlier termination of this Agreement in accordance with the terms hereof) shall Company take any action to cause a dividend or distribution of or take any other action with respect to the Convertible Note, and the Convertible Note shall continue to be held by Company until and through the Effective Time such that the value of the Convertible Note shall thereby effectively be relinquished at the Effective Time, if and only if the Closing occurs and the Agreement has not been terminated, by Company and the Shareholders in exchange for the Merger Consideration.”
8. Amendment to Section 3.15. Section 3.15 of the Merger Agreement is hereby amended to delete the words “less the amount of the Working Capital Loan Amount.”
9. Amendment to Section 8.1. Section 8.1 of the Merger Agreement is hereby amended and restated as follows:
“8.1 Survival. All representations and warranties and the covenants and agreements (to the extent such covenant or agreement contemplates or requires performance prior to the Closing) of each of the Parties shall terminate and expire on, and shall cease to have any further force or effect following, the date which is two (2) years from the Closing Date (the “Expiration Date”); provided, however, that if at any time prior to the Expiration Date, an Indemnified Party has duly delivered to the applicable Indemnifying Parties a Claim Notice (satisfying the requirements set forth in Sections 8.4 and 8.5), then the specific indemnification claim asserted in such Claim Notice shall survive the Expiration Date until such time as such claim is resolved. Each covenant and agreement requiring performance at or after the Closing, will, in each case, expressly survive Closing in accordance with its terms, and if no term is specified, then such covenants and agreements shall survive indefinitely following the Effective Time.”
10. Amendment to Section 9.1(b)(i). Section 9.1(b)(i) of the Merger Agreement is hereby amended by replacing “August 31, 2017” with “March 31, 2018.”
| A-8 |
11. Amendment to Section 13.1. Section 13.1 of the Merger Agreement is hereby amended as follows:
| a. | The term “the Convertible Note” is added to the definition of “Transaction Documents” and replaces the term “the Working Capital Note” in such definition; |
| b. | The following definition is added to Section 13.1, inserted in alphabetical order: ““Convertible Note” has the meaning set forth in Section 3.14”; and |
| c. | The definitions “Shareholder Note” and “Working Capital Note” are deleted. |
12. Amendment to Exhibits. The title of Exhibit F of the Merger Agreement is hereby amended to be “Convertible Note.”
13. Effect of Amendment. Except as expressly set forth in this Amendment, the Merger Agreement remains in full force and effect.
14. Governing Law; Exclusive Jurisdiction. All disputes, claims or controversies arising out of or relating to this Amendment shall be construed in accordance with and governed by the internal laws of the State of California without giving effect to any choice or conflict of law provision or rule (whether of the State of California or any other jurisdiction) that would cause the application of laws of any jurisdiction other than those of the State of California.
15. Execution of Amendment; Counterparts; Electronic Signature. This Amendment may be executed in multiple counterparts, each of which shall be deemed an original and all of which shall constitute one and the same instrument. The exchange of copies of this Amendment and signature pages by facsimile transmission, by electronic mail in portable document format form or by any other electronic means intended to preserve the original graphic and pictorial appearance of a document, or by combination of such means, shall constitute effective execution and delivery of this Amendment as to the Parties and may be used in lieu of the original Amendment for all purposes.
16. Modification. This Amendment may not be amended except by a written amendment signed by all of the Parties hereto.
[Signature Page Follows]
| A-9 |
IN WITNESS WHEREOF, each of the parties hereto has caused this Amendment No. 2 to Agreement and Plan of Merger to be duly executed on its behalf as of the day and year first above written.
| PARENT: | Apollo Medical Holdings, Inc., a Delaware corporation | ||
| By: | /s/ Warren Hosseinion | ||
| Name: | Warren Hosseinion | ||
| Title: | CEO | ||
| MERGER SUB: | Apollo Acquisition Corp., a California corporation | ||
| By: | /s/ Warren Hosseinion | ||
| Name: | Warren Hosseinion | ||
| Title: | CEO | ||
| THE COMPANY: | Network Medical Management, Inc., a California corporation | ||
| By: | /s/ Thomas Lam | ||
| Name: | Thomas Lam | ||
| Title: | CEO | ||
| SHAREHOLDERS’ REPRESENTATIVE: |
|
||
| Kenneth Sim, M.D. | |||
| A-10 |
VOTING AGREEMENT
This Voting Agreement (this “Agreement”) is made and entered into as of [___________], by and among Apollo Medical Holdings, Inc., a Delaware corporation (“Parent”), and the undersigned Shareholders of the Company (each a “Holder”). Capitalized terms used but not otherwise defined herein shall have the meanings ascribed to such terms in the Merger Agreement (as such term is defined below).
RECITALS
WHEREAS, concurrently with the execution of this Agreement, Network Medical Management, Inc., a California corporation (the “Company”), Parent and Apollo Acquisition Corp., a California corporation and wholly owned subsidiary of Parent (“Merger Sub”), are entering into an Agreement and Plan of Merger (the “Merger Agreement”), pursuant to which Merger Sub will merge with and into the Company, with the Company continuing as the surviving corporation, upon the terms and subject to the conditions set forth therein;
WHEREAS, as of the date hereof, each Holder is the beneficial owner (as defined under Rule 13d-3 of the Exchange Act) of the outstanding shares of the Company’s Common Stock, no par value (the “Common Stock”), set forth under such Holder’s name on the signature page to this Agreement (the “Existing Shares” and, together with any other shares of Company Common Stock, or other capital stock of the Company acquired (either of record or beneficially owned) by such Holder after the date hereof, collectively, the “Shares”); and
WHEREAS, as a condition to its willingness to enter into the Merger Agreement, Parent has requested that each Holder enter into this Agreement.
AGREEMENT
NOW THEREFORE, in consideration of the premises and of the terms and conditions contained herein and for other good and valuable consideration, the receipt and sufficiency of which is hereby acknowledged, the parties hereto agree as follows:
Section 1. Agreement to Retain Shares.
(a) Transfer. (i) Except as contemplated by the Merger Agreement, and except as provided in Section 1(b) below, during the period beginning on the date hereof and ending on the earlier to occur of (A) the Effective Time and (B) the Expiration Date (as defined below), Holder agrees not to, directly or indirectly, sell, transfer, exchange or otherwise dispose of (including by merger, consolidation or otherwise by operation of law) the Shares, (ii) except in connection with a certain Voting Trust Agreement effective as of July 1, 2015 by and among certain Holders of the Company, and except as provided in Section 2 below, Holder agrees not to, directly or indirectly, grant any proxies or powers of attorney, deposit any of such Holder’s Shares into a voting trust or, enter into a voting agreement with respect to any of such Holder’s Shares, or enter into any agreement or arrangement providing for any of the actions described in this clause (ii), and (iii) Holder agrees not to, directly or indirectly, take any action that could reasonably be expected to have the effect of preventing or disabling Holder from performing Holder’s obligations under this Agreement, in the case of (ii) and (iii), at any time prior to the earlier to occur of (x) the Effective Time and (y) the Expiration Date. As used herein, the term “Expiration Date” shall mean the date of termination of the Merger Agreement in accordance with the terms and provisions thereof.
| B-1 |
(b) Permitted Transfers. Section 1(a) shall not prohibit a transfer of Shares by Holder (i) to any family member, trust for the benefit of any family member or charitable organization to which contributions are deductible for federal income tax, estate or gift purposes so long as the assignee or transferee agrees to be bound by the terms of this Agreement and executes and delivers to the parties hereto a written consent memorializing such agreement, (ii) in connection with the exercise of stock options for Company Common Stock but only to the extent of such Holder’s exercise price and income or other tax liability with respect to such exercise and only to the extent permitted under the Merger Agreement, and (iii) that were acquired upon the exercise of stock options expiring after the date hereof and prior to the Effective Time.
Section 2. Agreement to Vote Shares.
(a) Until the earlier to occur of the Effective Time and the Expiration Date, at every meeting of the Shareholders of the Company called with respect to any of the following, and at every adjournment thereof, and on every action or approval by written consent of the Shareholders of the Company with respect to any of the following, Holder shall appear at such meeting (in person or by proxy) and shall vote or consent the Shares (i) in favor of adoption of the Merger Agreement and the approval of the transactions contemplated thereby and (ii) against any proposal for any recapitalization, merger, sale of assets or other business combination (other than as contemplated by the Merger Agreement) between the Company and any person or entity other than Parent or any other action or agreement that would reasonably be expected to result in a breach of any covenant, representation or warranty or any other obligation or agreement of the Company under the Merger Agreement or Holder under this Agreement or which would reasonably be expected to result in any of the conditions to the Company’s obligations under the Merger Agreement not being fulfilled. This Agreement is intended to bind Holder as a Shareholder of the Company only with respect to the specific matters set forth herein. Except as set forth in clauses (i) and (ii) of this Section 2(a), Holder shall not be restricted from voting in favor of, against or abstaining with respect to any other matter presented to the Shareholders of the Company. Prior to the termination of this Agreement, Holder covenants and agrees not to enter into any agreement or understanding with any person to vote or give instructions in any manner inconsistent with the terms of this Agreement.
(b) Holder further agrees that, until the termination of this Agreement, Holder will not, and will not permit any entity under Holder’s control to, (i) solicit proxies or become a “participant” in a “solicitation” (as such terms are defined in Rule 14A under the Exchange Act) with respect to an Opposing Proposal (as defined below), (ii) initiate a Shareholders’ vote with respect to an Opposing Proposal or (iii) become a member of a “group” (as such term is used in Section 13(d) of the Exchange Act) with respect to any voting securities of the Company with respect to an Opposing Proposal. For the purposes of this Agreement, an “Opposing Proposal” means any action or proposal described in clause (ii) of Section 2(a) above.
| B-2 |
(c) Subject to the provisions set forth in Section 5 hereof and as security for Holder’s obligations under Section 2(a), Holder hereby irrevocably constitutes and appoints Parent and its designees as his or her attorney and proxy in accordance with the CGCL, with full power of substitution and resubstitution, to cause the Shares to be counted as present at the Company Shareholders meeting, to vote his Shares at the Company Shareholders meeting, however called, and to execute consents in respect of his or her Shares as and to the extent provided in Section 2(a). SUBJECT TO THE PROVISIONS SET FORTH IN SECTION 5 HEREOF, THIS PROXY AND POWER OF ATTORNEY IS IRREVOCABLE AND COUPLED WITH AN INTEREST. Upon the execution of this Agreement, Holder hereby revokes any and all prior proxies or powers of attorney given by Holder with respect to voting of the Shares on the matters referred to in Section 2(a) and agrees not to grant any subsequent proxies or powers of attorney with respect to the voting of the Shares on the matters referred to in Section 2(a) until after the Expiration Date. Holder understands and acknowledges that Parent is entering into the Merger Agreement in reliance upon the Holder’s execution and delivery of this Agreement and Holder’s granting of the proxy contained in this Section 2(c). Holder hereby affirms that the proxy granted in this Section 2(c) is given in connection with the execution of the Merger Agreement, and that such Proxy is given to secure the performance of the duties of Holder under this Agreement. Parent acknowledges and agrees that Holder may vote the Shares on all other matters not referred to in Section 2(a), and the attorneys and proxies named above may not exercise the proxy with respect to such other matters.
Section 3. Representations, Warranties and Covenants of Holder. Holder hereby represents, warrants and covenants to Parent that Holder (i) is the record and/or beneficial owner of the Shares, which, at the date of this Agreement and at all times up until the earlier to occur of (A) the Effective Time and (B) the Expiration Date, are and will be free and clear of any liens, claims, options, charges or other encumbrances that would reasonably be expected to have the effect of preventing or disabling Holder from performing Holder’s obligations under this Agreement, and (ii) does not own of record or beneficially any shares of capital stock of the Company other than the Shares (excluding shares as to which Holder currently disclaims beneficial ownership in accordance with applicable law). Holder has the legal capacity, power and authority to enter into and perform all of Holder’s obligations under this Agreement (including under the proxy granted in Section 2(c) above). This Agreement (including the proxy granted in Section 2(c) above) has been duly and validly executed and delivered by Holder and constitutes a valid and binding agreement of Holder, enforceable against Holder in accordance with its terms, subject to (x) laws of general application relating to bankruptcy, insolvency and the relief of debtors and (y) rules of law governing specific performance, injunctive relief and other equitable remedies.
Section 4. No Ownership Interest. Nothing contained in this Agreement shall be deemed to vest in Parent or Merger Sub any direct or indirect ownership or incidence of ownership of or with respect to any Shares, except as expressly provided herein. All rights, ownership and economic benefits of and relating to the Shares shall remain vested in and belong to Holder, and neither Parent nor Merger Sub shall have any authority to direct Holder in the voting or disposition of any of the Shares, except as otherwise provided herein.
| B-3 |
Section 5. Termination. This Agreement and the proxy delivered in connection herewith shall terminate and shall have no further force and effect as of the earlier to occur of (i) the Expiration Date and (ii) the Effective Time.
Section 6. Fiduciary Duties. Notwithstanding anything in this Agreement to the contrary: (i) Holder makes no agreement or understanding herein in any capacity other than in Holder’s capacity as a record holder and/or beneficial owner of the Shares, (ii) nothing in this Agreement shall be construed to limit or affect any action or inaction by Holder acting in his capacity as a director, officer or other fiduciary of the Company, (iii) Holder shall have no liability to Parent, Merger Sub or any of their Affiliates under this Agreement as a result of any action or inaction by Holder acting in his capacity as a director, officer or other fiduciary of the Company and (iv) any breach of this Agreement by Holder shall not entitle any or all of the Parent Indemnified Parties to indemnification and/or assessment against the Holdback Shares under the Merger Agreement.
Section 7. Miscellaneous.
(a) Amendments and Waivers. Any term of this Agreement may be amended or waived with the written consent of the parties or their respective successors and assigns. Any amendment or waiver effected in accordance with this Section 7(a) shall be binding upon the parties and their respective successors and assigns.
(b) Governing Law. All disputes, claims or controversies arising out of or relating to this Agreement or the transactions contemplated hereby shall be construed in accordance with and governed by the internal laws of the State of California without giving effect to any choice or conflict of law provision or rule (whether of the State of California or any other jurisdiction) that would cause the application of laws of any jurisdiction other than those of the State of California.
(c) Counterparts. This Agreement may be executed in multiple counterparts, each of which shall be deemed an original and all of which shall constitute one and the same instrument.
(d) Titles and Subtitles. The titles and subtitles used in this Agreement are used for convenience only and are not to be considered in construing or interpreting this Agreement.
(e) Notices. All notices and other communications under this Agreement shall be in writing, and shall be deemed effective when personally delivered; when mailed by certified or registered mail, return receipt requested; or when deposited with a comparably reliable postal delivery service (such as Federal Express) or other courier service, or sent by facsimile or other electronic transmission system, addressed to the party to be notified at such party’s address or facsimile number as set forth below, or as subsequently modified by written notice.
(f) Severability. If any one or more of the provisions of this Agreement, or the applicability of any such provision to a specific situation, is deemed invalid or unenforceable, then such provision shall be modified to the minimum extent necessary to make its application valid and enforceable, and the validity and enforceability of all of the provisions of this Agreement, and all other applications of such provisions, shall not be affected.
| B-4 |
(g) Specific Performance. The parties agree that irreparable damage would occur in the event that any of the provisions of this Agreement were not performed in accordance with their specific terms or were otherwise breached. Accordingly, each of the parties shall be entitled to specific performance of the terms hereof, including an injunction or injunctions to as a remedy for any such breach, prevent breaches of this Agreement and to enforce specifically the terms and provisions of this Agreement, this being in addition to any other remedy to which they are entitled at law or in equity.
(h) Entire Agreement. This Agreement and the documents referred to herein constitute the entire agreement between the parties hereto pertaining to the subject matter hereof, and any and all other written or oral agreements existing between the parties hereto are expressly canceled.
[Signatures Page Follows]
| B-5 |
The parties have caused this Agreement to be duly executed on the date first above written.
| APOLLO MEDICAL HOLDINGS, INC. | |||
| By: | |||
| Name: | |||
| Title: | |||
| Address: | |
|
Apollo Medical Holdings, Inc. 700 N. Brand Boulevard Facsimile No.: (818) 839-5190 |
|
“Holder”
____________________________
|
|
| Address: | |
| _______________________________ | |
| _______________________________ | |
| Attention: _______________________ | |
| Facsimile No.: ___________________ |
| Shares owned of record: | Beneficially owned shares: | |||||
| Class of Shares | Number | Class of shares | Number | |||
|
[_______] |
[_______] |
[_________] |
[______] |
| B-6 |
APOLLO MEDICAL HOLDINGS, INC.
Common Stock Purchase Warrant
| C-1 |
THIS WARRANT AND THE SHARES ISSUABLE HEREUNDER HAVE NOT BEEN REGISTERED UNDER THE SECURITIES ACT OF 1933, AS AMENDED (THE “SECURITIES ACT”), OR THE SECURITIES LAWS OF ANY STATE AND, EXCEPT AS PROVIDED HEREIN, MAY NOT BE OFFERED, SOLD OR OTHERWISE TRANSFERRED, PLEDGED OR HYPOTHECATED UNLESS AND UNTIL REGISTERED UNDER THE SECURITIES ACT AND APPLICABLE STATE SECURITIES LAWS, OR SUCH OFFER, SALE, TRANSFER, PLEDGE OR HYPOTHECATION IS PERMITTED UNDER RULE 144 OF THE SECURITIES ACT OR IS OTHERWISE EXEMPT FROM SUCH REGISTRATION.
APOLLO MEDICAL HOLDINGS, INC.
Common Stock Purchase Warrant
| Warrant Number: NMM 2017 – [__] | Issue Date: [______ __], 201[_] |
THIS COMMON STOCK PURCHASE WARRANT (the “Warrant”) certifies that, for value received, ____________ or registered assigns (the “Holder”) is entitled, at any time prior to 5:00 p.m., Pacific time, on [________ __, _____]1 (the “Expiration Date”), to purchase from Apollo Medical Holdings, Inc., a Delaware corporation (“Company”), up to the number of fully paid and non-assessable shares (the “Shares”) of Common Stock, par value $0.001 per share, of Company (the “Common Stock”) specified above (the “Warrant Number”) at an exercise price of $1[_].002 per Share (the “Warrant Exercise Price”) or to convert this Warrant into Shares, in each case subject to the provisions and upon the terms and conditions set forth in this Warrant. This Warrant has been issued in connection with the Agreement and Plan of Merger, dated as of December 21, 2016, among the Company, Apollo Acquisition Corp., a wholly-owned subsidiary of the Company, Network Medical Management, Inc. and Kenneth Sim, M.D. (as it may be amended from time to time in accordance with its terms, the “Merger Agreement”). Capitalized terms used herein and not defined shall have the meanings given thereto in the Merger Agreement.
1. EXERCISE.
1.1 Method of Exercise. Holder may exercise this Warrant in whole or in part to purchase the Shares for cash by (a) delivering to Company, in accordance with Section 5.2, a duly executed copy of a Notice of Exercise in substantially the form attached as Appendix 1 not less than sixty one (61) days prior to the date of exercise (unless the Company otherwise agrees to a shorter notice period), and (b) causing this Warrant to be delivered to Company, in accordance with Section 5.2, as soon as reasonably practicable on or following the date on which the Notice of Exercise is delivered to Company (but no later than within sixty one (61) days following the date on which the Notice of Exercise is delivered to Company). Unless Holder is exercising the conversion right provided for in Section 1.2, Holder shall, within three (3) Trading Days following the date of exercise as aforesaid, also deliver to Company a certified or bank cashier’s check, wire transfer of immediately available funds (to an account designated by Company), or other form of payment acceptable to Company, in the amount of the aggregate Warrant Exercise Price for the Shares being purchased.
1 Insert date that is 5 years from the issue date.
2 Insert $11.00 for NMM shareholder’s pro rata portion of warrants to purchase 900,000 shares of the Company common stock
| C-2 |
1.2 Conversion Right. In lieu of exercising this Warrant to purchase Shares for cash in accordance with Section 1.1, Holder may, at its option, from time to time convert this Warrant, in whole or in part and without any obligation to pay the Warrant Exercise Price, into that number of Shares determined by dividing (x) the aggregate Fair Market Value of the Shares in respect of which this Warrant is being converted minus the aggregate Warrant Exercise Price of such Shares by (y) the Fair Market Value of one (1) Share. The Fair Market Value of one (1) Share shall be determined pursuant to Section 1.3. Holder may exercise such conversion right under this Warrant in whole or in part by (a) delivering to Company, in accordance with Section 5.2, a duly executed copy of a Notice of Exercise in substantially the form attached as Appendix l not less than sixty one (61) days prior to the date of conversion (unless the Company otherwise agrees to a shorter notice period), and (b) causing this Warrant to be delivered to Company, in accordance with Section 5.2, as soon as reasonably practicable on or following the date on which Notice of Exercise is delivered to Company (but no later than within two (2) Trading Days following the date on which the Notice of Exercise is delivered to Company). Any reference in this Warrant to the “exercise” of this Warrant or events to occur upon or in connection with the exercise of this Warrant, including without limitation, all provisions of Section 2, will apply equally and with the same equitable effect to any conversion of this Warrant even if reference is not specifically made to conversion of this Warrant.
1.3 Fair Market Value. For purposes of this Warrant, “Fair Market Value” shall mean, with respect to one (1) Share, the price determined by the first of the following clauses that applies: (a) the average of the daily volume weighted average trading price of the Common Stock on the Principal Trading Market for the five (5) Trading Days immediately prior to the date on which the Notice of Exercise for exercising the conversion right under this Warrant is delivered to Company, or (b) if the Common Stock is not so listed or quoted, as reasonably determined by the Board of Directors in good faith.
1.4 Delivery of Certificate and New Warrant. Within three (3) Trading Days after Holder exercises under Section 1.1 or converts under Section 1.2 this Warrant and, if applicable, Company receives payment of the aggregate Warrant Exercise Price, Company shall deliver to Holder certificates (or, if consistent with Company’s practice for issuing shares of Common Stock, non-certificated Shares represented by book-entry on the records of Company or Company’s transfer agent (the “Book-Entry Shares”)) for the Shares so acquired and, if this Warrant has not been fully exercised or converted and has not expired, a new warrant of like tenor representing the Shares not so acquired. The Shares shall be deemed to have been issued, and Holder or any other Person designated by Holder to be named therein shall be deemed to have become a holder of record of such Shares for all purposes as of the date this Warrant shall have been exercised or converted. If Company fails to deliver a certificate or certificates (or, if applicable, Book-Entry Shares) for the Shares as provided herein, in addition to any other remedy available to Holder hereunder, at law or in equity, Holder shall have the right to rescind the exercise or conversion of this Warrant. The Holder acknowledges and understands that any stock certificates issued hereunder and any Warrant issued in replacement of this Warrant upon its exercise, in whole or in part, or for any other reason, shall be subject to the provisions of Section 4A of this Warrant and shall have the legends placed thereon as appear on the first page of this Warrant.
| C-3 |
1.5 Fractional Shares. No fractional Share shall be issuable upon exercise or conversion of this Warrant, and the number of Shares to be issues shall be rounded down to the nearest whole Share. If a fractional share interest arises upon any exercise or conversion of this Warrant, Company shall eliminate such fractional share interest by paying Holder cash in the amount computed by multiplying the fractional share interest by the Fair Market Value (as determined pursuant to Section 1.3) of a full Share.
2. ANTI-DILUTION PROVISIONS; ADJUSTMENT IN WARRANT NUMBER AND WARRANT EXERCISE PRICE. The Warrant Exercise Price and Warrant Number shall be subject to adjustment from time to time as provided in this Section 2.
2.1 Dividends, Subdivisions and Combinations. If Company, at any time and from time to time, (i) takes a record of the holders of its Common Stock for the purpose of entitling them to receive, or otherwise declares or distributes, a dividend payable in, or other distribution of, additional shares of Common Stock or Common Stock Equivalents, (ii) splits or subdivides its outstanding shares of Common Stock into a greater number of shares of Common Stock or Common Stock Equivalents, or (iii) combines its$ outstanding shares of Common Stock into a smaller number of shares of Common Stock or Common Stock Equivalents, then, in each such case, (a) the Warrant Number shall be adjusted to equal the product of (x) the Warrant Number in effect immediately prior to the adjustment multiplied by (y) a fraction, the numerator of which is equal to the number of shares of Common Stock outstanding immediately after such adjustment and the denominator of which is equal to the number of shares of Common Stock outstanding immediately prior to the adjustment, and (b) the Warrant Exercise Price shall be adjusted pursuant to Section 2.2.
2.2 Adjustment of Warrant Exercise Price. Upon any adjustment of the Warrant Number as provided in Sections 2.1, the Warrant Exercise Price shall be adjusted to be equal to the product of (i) the Warrant Exercise Price in effect immediately prior to such adjustment multiplied by (ii) the quotient of the Warrant Number in effect immediately prior to such adjustment divided by the Warrant Number in effect immediately after such adjustment.
2.3 Determination of Adjustments. Upon any event that shall require an adjustment pursuant to this Section 2, Company shall promptly calculate such adjustment in accordance with the terms of this Warrant and prepare a certificate setting forth, in reasonable detail, such adjustment, the method of calculation thereof and the facts upon which such adjustment is based.
3. CERTAIN AGREEMENTS. Company hereby covenants and agrees as follows:
3.1 Shares to be Fully Paid. All Shares shall, upon issuance in accordance with the terms of this Warrant, be duly and validly issued, fully paid and non-assessable.
3.2 Reservation of Shares. Until the Expiration Date, Company at all times shall have authorized, and reserved for the purpose of issuance upon exercise of this Warrant, a sufficient number of shares of Common Stock to provide for the exercise of this Warrant in full.
| C-4 |
3.3 Successors and Assigns. This Warrant shall be binding upon any entity succeeding to Company by merger, consolidation, or acquisition of all or substantially all Company’s assets or all or substantially all of Company’s outstanding capital stock or otherwise.
4. TRANSFER AND REPLACEMENT OF WARRANT.
4.1 Restriction on Transfer. Subject to this Section 4.1, this Warrant and the rights granted to Holder are transferable and assignable, in whole or in part, upon surrender of this Warrant, together with a properly executed assignment in substantially the form attached as Appendix 2, at the office or agency of Company referred to in Section 4.4. Nothing in this Warrant shall prohibit Holder from assigning, delegating or transferring this Warrant and Holder’s rights and obligations under this Warrant to an Affiliate of Holder. Otherwise, Holder may not assign, delegate or otherwise transfer (whether by operation of law, by contract or otherwise) its rights and obligations under this Warrant, or any portion hereof or thereof, to any Person whose principal business is providing integrated healthcare services or who otherwise is a competitor of Company as determined reasonably and in good faith by the Board of Directors. Until due presentment for registration of transfer on the books of Company, Company may treat the registered holder hereof as the owner of this Warrant and Holder for all purposes, and Company shall not be affected by any notice to the contrary. Notwithstanding anything herein contained to the contrary, none of the Warrants may be transferred separately from the Shares of Series B Preferred Stock to which they relate (l-for-1).
4.2 Replacement of Warrant. Upon receipt of evidence reasonably satisfactory to Company of the loss, theft, destruction or mutilation of this Warrant and, in the case of any such loss, theft or destruction, upon delivery of an indemnity agreement reasonably satisfactory in form and amount to Company, or, in the case of any such mutilation, upon surrender and cancellation of this Warrant, Company, at its expense, shall execute and deliver to Holder, in lieu thereof, a new Warrant of like tenor.
4.3 Cancellation; Payment of Expenses. Upon the surrender of this Warrant in connection with any transfer, exchange or replacement, this Warrant shall be promptly canceled by Company. Company shall pay all taxes (other than securities transfer taxes) and all other expenses (other than legal expenses, if any, incurred by Holder or transferees) and charges payable in connection with the preparation, execution, and delivery of a new Warrant issued to Holder or transferees, as applicable.
4.4 Register. Company shall maintain, at its principal executive offices (or such other office or agency of Company as it may designated by notice to Holder), a register for this Warrant, in which Company shall record the name and address of the Person in whose name this Warrant has been issued, as well as the name and address of each transferee and each prior owner of this Warrant.
5. MISCELLANEOUS.
5.1 Term. This Warrant is exercisable or convertible in whole or in part at any time and from time to time before or on the Expiration Date on no less than sixty-one (61) days’ prior written notice to the Company (unless the Company otherwise agrees to a shorter notice period).
| C-5 |
5.2 Notices. All demands, notices, approvals, consents, requests, and other communications hereunder shall be in writing and shall be deemed to have been given when the writing is delivered, if given or delivered by hand, overnight delivery service or facsimile transmitter (with confirmed receipt), or five (5) days after being mailed, if mailed, by first class, registered or certified mail, postage prepaid, to the address or telecopy number set forth below. If any time period for giving notice or taking action hereunder expires on a day that is not a Trading Day, the time period shall automatically be extended to the Trading Day immediately following such day. Such notices, demands, requests, consents and other communications shall be sent to the following Persons at the following addresses:
if to Company:
Apollo Medical Holdings, Inc.
700 N. Brand Blvd., Suite 220
Glendale, California 91203
Attention: Chief Executive Officer
Telephone: (818) 396-8050
Fax: (818) 844-3888
if to Holder:
[______________________]
[______________________]
Attention: [_____________]
Telephone: [____________]
Fax: [ ]
Company or Holder may, by notice given hereunder, designate any further or different addresses or telecopy numbers to which subsequent demands, notices, approvals, consents, requests or other communications shall be sent or persons to whose attention the same shall be directed.
5.3 Waivers. The rights and remedies provided for herein are cumulative and not exclusive of any right or remedy that may be available to Holder whether at law, in equity, or otherwise. No delay, forbearance, or neglect by Holder, whether in one or more instances, in the exercise of any right, power, privilege, or remedy hereunder or in the enforcement of any term or condition of this Warrant shall constitute or be construed as a waiver thereof. No waiver of any provision hereof, or consent required hereunder, or any consent or departure from this Warrant, shall be valid or binding unless expressly and affirmatively made in writing and duly executed by Holder. No waiver shall constitute or be construed as a continuing waiver or a waiver in respect of any subsequent breach, either of similar or different nature, unless expressly so stated in such writing.
5.4 Specific Enforcement. The parties hereto agree that irreparable damage would occur in the event that any of the provisions of this Warrant were not performed in accordance with their specific intent or were otherwise breached. It is accordingly agreed that the parties shall be entitled to an injunction or injunctions to prevent or cure breaches of the provisions of this Warrant and to enforce specifically the terms and provisions hereof, in addition to any other remedy to which they may be entitled by law or equity.
| C-6 |
5.5 Counterparts. This Warrant may be executed simultaneously in two or more counterparts, any one of which need not contain the signatures of more than one party, but all such counterparts taken together shall constitute one and the same Warrant. Counterparts may be delivered via facsimile, electronic mail (including pdf) or other transmission method and any counterpart so delivered shall be deemed to have been duly and validly delivered and be valid and effective for all purposes.
5.6 Governing Law. This Warrant shall be governed by and construed in accordance with the laws of the State of California, without giving effect to any choice or conflict of law provision or rule (whether of the State of California or any other jurisdiction) that would cause the application of the laws of any jurisdiction other than the State of California. Holder agrees that all legal proceedings concerning the interpretations, enforcement and defense of the transactions contemplated by this Warrant (whether brought against Holder, the Company or their respective affiliates, directors, officers, shareholders, partners, members, employees or agents) shall be commenced exclusively in the state and federal courts sitting in the County of Los Angeles. Each party hereby irrevocably submits to the exclusive jurisdiction of the state and federal courts sitting in the County of Los Angeles for the adjudication of any dispute hereunder or in connection herewith or with any transaction contemplated hereby or discussed herein, and hereby irrevocably waives, and agrees not to assert in any suit, action or proceeding, any claim that it is not personally subject to the jurisdiction of any such court, that such suit, action or proceeding is improper or is an inconvenient venue for such proceeding.
5.7 Amendment. This Warrant may be amended, modified, or supplemented only pursuant to a written instrument making specific reference to this Warrant and signed by Company and Holder.
5.8 Severability. Whenever possible, each provision of this Warrant shall be interpreted in such manner as to be effective and valid under applicable law, but if any provision of this Warrant is held to be invalid or unenforceable in any respect, such invalidity or unenforceability shall not render invalid or unenforceable any other provision of this Warrant.
5.9 Descriptive Headings; No Strict Construction. The descriptive headings of this Warrant are inserted for convenience only and do not constitute a substantive part of this Warrant. The parties to this Warrant have participated jointly in the negotiation and drafting of this Warrant. If an ambiguity or question of intent or interpretation arises, this Warrant shall be construed as if drafted jointly by the parties hereto, and no presumption or burden of proof shall arise favoring or disfavoring any party by virtue of the authorship of any of the provisions of this Warrant. The parties agree that prior drafts of this Warrant shall be deemed not to provide any evidence as to the meaning of any provision hereof or the intention of the parties hereto with respect to this Warrant.
[signature page follows]
| C-7 |
IN WITNESS WHEREOF, the parties have duly executed and delivered this Common Stock Purchase Warrant as of the date first above written.
| COMPANY: | ||
| APOLLO MEDICAL HOLDINGS, INC. | ||
| By: | ||
| Name: | Warren Hosseinion | |
| Title: | Chief Executive Officer | |
| HOLDER: | ||
| (PRINT NAME) | ||
| (Signature) | ||
Signature Page to Common Stock Purchase Warrant
| C-8 |
APPENDIX 1
FORM OF NOTICE OF EXERCISE
| TO: | APOLLO MEDICAL HOLDINGS, INC. |
1. The undersigned hereby elects to purchase ______ Shares of the Common Stock of Apollo Medical Holdings, Inc. pursuant to the terms of the attached Common Stock Purchase Warrant (the “Warrant”) issued to the undersigned (or the undersigned’s predecessor or assignor), and shall tender payment of the exercise price in full in accordance with the terms of the Warrant.
2. Payment shall take the form of (check applicable box):
| [ ] | in lawful money of the United States; or |
| [ ] | the cancellation of such number of Shares as is necessary, in accordance with the formula set forth in Section 1.2 of the Warrant, to exercise the Warrant with respect to the maximum number of Shares purchasable pursuant to the cashless exercise procedure set forth in Section 1.2 of the Warrant. |
3. Please issue a certificate or certificates (or, if applicable, Book-Entry Shares) representing said Shares in the name of the undersigned or in such other name as is specified below:
The Shares shall be delivered by physical delivery of a certificate (or, if applicable, Book-Entry Shares) to:
[SIGNATURE OF HOLDER]
Name of Holder:
Name of Authorized Signatory:
Title of Authorized Signatory:
Date:
Date of exercise under Section 1.1 of the Warrant or date of exercise of conversion right under Section 1.2 of the Warrant is the date this Notice is deemed effectively given under Section 5.2 of this Warrant.
| C-9 |
APPENDIX 2
ASSIGNMENT FORM
(To Assign the foregoing Warrant, execute this form and supply required information.
Do not use this form to exercise the Warrant.)
FOR VALUE RECEIVED,
(check first box OR fill in number of Shares in second box)
[__] all of the Warrant
OR
[_______] shares of the foregoing Warrant
and all rights evidenced thereby are hereby assigned to:
| whose address is |
| . |
| Dated: | , | |||
| Holder’s Signature: | ||||
| Holder’s Address: | ||||
| C-10 |
LOCK-UP AGREEMENT
This Lock-Up Agreement (this “Agreement”) is entered into as of _________ _, 2017 by and between the undersigned shareholder (the “Shareholder”) and Apollo Medical Holdings, Inc., a Delaware corporation (“Parent”). Capitalized terms used but not otherwise defined herein shall have the meanings ascribed to such terms in the Merger Agreement (as such term is defined below).
RECITALS
WHEREAS, prior to or concurrently with the execution of this Agreement, Network Medical Management, Inc., a California corporation (the “Company”), Parent and Apollo Acquisition Corp., a California corporation and wholly owned subsidiary of Parent (“Merger Sub”), are entering into an Agreement and Plan of Merger (the “Merger Agreement”), pursuant to which Merger Sub will merge with and into the Company, with the Company continuing as the surviving corporation (the “Merger”), upon the terms and subject to the conditions set forth therein;
WHEREAS, pursuant to the Merger Agreement, shareholders of the Company shall receive shares of common stock, par value $0.001 per share, of Parent (“Parent Stock”) in exchange for the shares of stock of the Company formerly held by them, on the terms set forth in the Merger Agreement; and
WHEREAS, pursuant to the Merger Agreement and as a condition to Parent’s and Merger Sub’s willingness to consummate the Merger, Parent and Merger Sub have required that the Shareholder agree to enter into this Agreement, which, among other things, restricts the sale, assignment, transfer, encumbrance or other disposition of the Covered Securities (as such term is defined below).
AGREEMENT
NOW THEREFORE, in consideration of the premises and of the terms and conditions contained herein and for other good and valuable consideration, the receipt and sufficiency of which is hereby acknowledged, the parties hereto agree as follows:
1. Lock-Up of Securities.
(a) Lock-Up. In recognition of the benefit that the Merger will confer upon the Shareholder as a stockholder, officer and/or director of Parent, and for other good and valuable consideration, the receipt and sufficiency of which are hereby acknowledged, the Shareholder agrees that:
(i) during the period commencing on the effective time of the Merger (the “Effective Time”) to and including the date that is eighteen (18) months from the Effective Time (the “First Lock-Up Period”), the Shareholder will not, without the prior written consent of Parent, directly or indirectly, offer, pledge, sell, contract to sell, sell any option or contract to purchase, purchase any option or contract to sell, grant any option, right or warrant for the sale of, or otherwise dispose of or transfer any Covered Securities whether now owned or hereafter acquired by the Shareholder or with respect to which the Shareholder has or hereafter acquires the power of disposition, or enter into any swap or any other agreement or any transaction that transfers, in whole or in part, directly or indirectly, the economic consequence of ownership of the Covered Securities, whether any such swap or transaction is to be settled by delivery of Parent Stock or other securities, in cash or otherwise (the “Securities Act”) (each of the foregoing, a “Transfer”);
| D-1 |
(ii) during the period commencing on the first calendar day following the end of the First Lock-Up Period to and including the date that is thirty (30) months from the Effective Time (the “Second Lock-Up Period”), the Shareholder will not, without the prior written consent of Parent, directly or indirectly, Transfer more than one-third (1/3) of the Covered Securities; and
(iii) during the period commencing on the first calendar day following the end of the Second Lock-Up Period to and including the date that is forty-two (42) months from the Effective Time (the “Third Lock-Up Period” and collectively with the First Lock-Up Period and Second Lock-Up Period, the “Lock-Up Periods”), the Shareholder will not, without the prior written consent of Parent, directly or indirectly, Transfer more than two-thirds (2/3) of the Covered Securities.
For the purposes of the Agreement, “Covered Securities” shall mean, with respect to the Shareholder, any of the following: (i) any and all shares of Parent Stock which are owned by the Shareholder as of the Effective Time, (ii) any shares of Parent Stock issuable upon exercise, conversion or exchange of any securities of the Parent which are owned by the Shareholder as of the Effective Time, (iii) any securities of the Parent issued in respect of the shares of Parent Stock issued or issuable to the Shareholder by way of stock dividend or stock split or in connection with a combination of shares, recapitalization, merger, consolidation or other reorganization or otherwise and any shares of Parent Stock issuable upon conversion, exercise or exchange thereof, in each case to the extent relating to any securities of the Parent which were owned by the Shareholder as of the Effective Time and (iv) any other securities of the Parent issued or issuable to Shareholder that are convertible into or exercisable or exchangeable for Parent Stock, whether at the option of the Shareholder or otherwise, in each case to the extent relating to any securities of the Parent which were owned by the Shareholder as of the Effective Time.
(b) Permitted Transfers. Notwithstanding the foregoing, the Shareholder may Transfer the Covered Securities to a Permitted Transferee without the prior written consent of Parent, provided, that (i) Parent receives a signed lock-up agreement for the balance of the Lock-Up Period(s) from each donee, trustee, distributee, or transferee, as the case may be, (ii) any such Transfer shall not involve a disposition for value, (iii) such Transfers are not required to be reported with the Securities and Exchange Commission on Form 4 in accordance with Section 16 of the Securities Exchange Act of 1934, as amended and (iv) the Shareholder does not otherwise voluntarily effect any public filing or report regarding such Transfers. For the purposes of this Agreement, “Permitted Transferee” means (1) if the Shareholder is an individual, (x) a member of the Shareholder’s immediate family (which shall mean any relationship by blood, marriage or adoption, not more remote than first cousin) or a trust, corporation, partnership or limited liability company for the benefit of an immediate family member, all of the beneficial interests of which shall be held by the Shareholder or one or more members of the Shareholder’s immediate family, and (y) the Shareholder’s heirs, successors, administrators and executors and any beneficiary pursuant to will, other testamentary document or applicable laws of decent, (2) if the Shareholder is an entity, any Affiliate of the entity, (3) if the Shareholder is a trust, to a trustee or beneficiary of the trust, (4) as a bona fide gift or gifts to any institution qualified as tax-exempt under Section 501(c)(3) of the Internal Revenue Code.
| D-2 |
(c) Open Market Sale. Furthermore, the Shareholder may sell shares of Parent Stock purchased by the Shareholder on the open market if and only if (i) such sales are not required to be reported in any public report or filing with the Securities Exchange Commission, or otherwise and (ii) the Shareholder does not otherwise voluntarily effect any public filing or report regarding such sales.
(d) Stop Transfer. During the Lock-Up Periods, Shareholder hereby authorizes Parent to cause any transfer agent for the Covered Securities subject to this Agreement to decline to transfer, and to note stop transfer restrictions on the stock register and other records relating to the Covered Securities, subject to this Agreement for which the Shareholder is the record holder and, in the case of Covered Securities subject to this Agreement for which the Shareholder is the beneficial owner but not the record holder, agrees during the Lock-Up Periods to cause the record holder to cause the relevant transfer agent to decline to transfer, and to note stop transfer restrictions on the stock register and other records relating to the Covered Securities subject to this Agreement, if such transfer would constitute a violation or breach of this Agreement.
2. Termination. This Agreement shall automatically terminate and be of no further force or effect upon the earlier to occur of (i) the termination of the Merger Agreement and (ii) the first day following the expiration of the Third Lock-Up Period; provided that Sections 3 through 16 of this Agreement shall survive termination under this Section 2.
3. Transfer; Successor and Assigns. The terms and conditions of this Agreement shall inure to the benefit of and be binding upon the respective successors and assigns of the parties. As provided above, any Transfer of Parent Stock shall require the transferee to execute a lock-up agreement in accordance with the same terms set forth herein. Nothing in this Agreement, express or implied, is intended to confer upon any party other than the parties hereto or their respective successors and assigns any rights, remedies, obligations or liabilities under or by reason of this Agreement, except as expressly provided in this Agreement.
4. Compliance with Securities Laws. Shareholder shall not at any time during or following the Second Lock-Up Period, make any Transfer, except (i) Transfers pursuant to an effective registration statement under the Securities Act, (ii) Transfers pursuant to the provisions of Rule 144, or (iii) if such Shareholder shall have furnished Parent with an opinion of counsel, if reasonably requested by Parent, which opinion and counsel shall be reasonably satisfactory to Parent, to the effect that the Transfer is otherwise exempt from registration under the Securities Act and that the Transfer otherwise complies with the terms of this Agreement.
| D-3 |
5. Other Restrictions.
(a) Legends. The Shareholder hereby agrees that each outstanding certificate representing shares of Parent Stock issued to Shareholder shall bear legends reading substantially as follows:
(i) “THE SHARES REPRESENTED HEREBY HAVE NOT BEEN REGISTERED UNDER THE SECURITIES ACT OF 1933, AS AMENDED, AND MAY NOT BE SOLD, TRANSFERRED, ASSIGNED, PLEDGED, OR HYPOTHECATED ABSENT AN EFFECTIVE REGISTRATION THEREOF UNDER SUCH ACT OR COMPLIANCE WITH REGULATION S, OR RULE 144 PROMULGATED UNDER SUCH ACT, OR UNLESS THE COMPANY HAS RECEIVED AN OPINION OF COUNSEL, SATISFACTORY TO THE COMPANY AND ITS COUNSEL, THAT SUCH REGISTRATION IS NOT REQUIRED.”
(ii) “THE SALE OR TRANSFER OF THE SHARES REPRESENTED HEREBY IS SUBJECT TO THE TERMS AND CONDITIONS OF A LOCK-UP AGREEMENT DATED [________ __], 2016, BETWEEN THE COMPANY AND THE STOCKHOLDER LISTED ON THE FACE HEREOF. A COPY OF SUCH AGREEMENT IS ON FILE AT THE PRINCIPAL OFFICE OF THE COMPANY AND WILL BE PROVIDED TO THE HOLDER HEREOF UPON REQUEST. NO TRANSFER OF SUCH SECURITIES WILL BE MADE ON THE BOOKS OF THE COMPANY UNLESS ACCOMPANIED BY EVIDENCE OF COMPLIANCE WITH THE TERMS OF SUCH LOCK-UP AGREEMENT.”
(b) Termination of Restrictive Legends. The restrictions referred to in Section 4(a)(i) shall cease and terminate as to any particular Parent Stock (i) when, in the opinion of counsel for Parent, such restriction is no longer required in order to assure compliance with the Securities Act or (ii) when such shares shall have been Transferred in a Rule 144 transfer or effectively registered under the Securities Act. The restrictions referred to in Section 4(a)(ii) shall cease and terminate at the end of the Lock-Up Periods. Whenever such restrictions shall cease and terminate as to any Parent Stock, Shareholder shall be entitled to receive from Parent, in exchange for such legended certificates, without expense (other than applicable transfer fees and taxes, if any, if such unlegended shares are being delivered and Transferred to any person other than the registered holder thereof), new certificates for a like number of shares not bearing the relevant legend(s) set forth in Section 4(a). Parent may request from Shareholder a certificate or an opinion of counsel of Shareholder with respect to any relevant matters in connection with the removal of the legend(s) set forth in Section 4(a)(i) from Shareholder’s stock certificates, which certificate or opinion of counsel will be reasonably satisfactory to Parent.
(c) Copy of Agreement. A copy of this Agreement shall be filed with the corporate secretary of Parent, shall be kept with the records of Parent and shall be made available for inspection by any shareholder of Parent. In addition, a copy of this Agreement shall be filed with Parent’s transfer agent of record.
| D-4 |
(d) Recordation. Parent shall not record upon its books any Transfer to any person except Transfers in accordance with this Agreement.
6. No Other Rights. The Shareholder understands and agrees that Parent is under no obligation to register the sale, Transfer or other disposition of Shareholder’s Covered Securities under the Securities Act or to take any other action necessary in order to ensure compliance with an exemption from such registration available.
7. Amendments and Waivers. Any term of this Agreement may be amended or waived with the written consent of the parties or their respective successors and assigns. Any amendment or waiver effected in accordance with this Section shall be binding upon the parties and their respective successors and assigns. The Board of Directors of the Company may amend the terms and conditions of this Agreement, including the Lock-Up Periods. In such event, the Company shall amend the terms and conditions of this Agreement on a pro rata basis for each Shareholder that is subject to this Agreement at any time so long as the Board reasonably determines that any such amendment is in the best interests of the Company. Notwithstanding the foregoing, any amendment to this Agreement shall in no way mean or be construed as the amendment, modification or waiver of any other lock-up agreement to which the Company is a party.
8. Governing Law. All disputes, claims or controversies arising out of or relating to this Agreement or the transactions contemplated hereby shall be construed in accordance with and governed by the internal laws of the State of California without giving effect to any choice or conflict of law provision or rule (whether of the State of California or any other jurisdiction) that would cause the application of laws of any jurisdiction other than those of the State of California.
9. Counterparts. This Agreement may be executed in multiple counterparts, each of which shall be deemed an original and all of which shall constitute one and the same instrument.
10. Titles and Subtitles. The titles and subtitles used in this Agreement are used for convenience only and are not to be considered in construing or interpreting this Agreement.
11. Notices. All notices and other communications under this Agreement shall be in writing, and shall be deemed effective when personally delivered; when mailed by certified or registered mail, return receipt requested; or when deposited with a comparably reliable postal delivery service (such as Federal Express) or other courier service, or sent by facsimile or other electronic transmission system, addressed to the party to be notified at such party’s address or facsimile number as set forth below, or as subsequently modified by written notice.
12. Severability. If any one or more of the provisions of this Agreement, or the applicability of any such provision to a specific situation, is deemed invalid or unenforceable, then such provision shall be modified to the minimum extent necessary to make its application valid and enforceable, and the validity and enforceability of all of the provisions of this Agreement, and all other applications of such provisions, shall not be affected.
| D-5 |
13. Specific Performance. The parties agree that irreparable damage would occur in the event that any of the provisions of this Agreement were not performed in accordance with their specific terms or were otherwise breached. Accordingly, each of the parties shall be entitled to specific performance of the terms hereof, including an injunction or injunctions to as a remedy for any such breach, prevent breaches of this Agreement and to enforce specifically the terms and provisions of this Agreement, this being in addition to any other remedy to which they are entitled at law or in equity.
14. Recapitalizations and Exchanges Affecting Shares. Except as otherwise provided in Section 1(b), the provisions of this Agreement shall apply, to the full extent set forth herein with respect to the Covered Securities, and to any and all shares of capital stock or equity securities of Parent which may be issued by reason of any stock dividend, stock split, reverse stock split, combination, recapitalization, reclassification or otherwise.
15. Delays or Omissions. No delay or omission to exercise any right, power or remedy accruing to any party to this Agreement, upon any breach or default of the other party to this Agreement shall impair any such right, power or remedy of such holder nor shall it be construed to be a waiver of any such breach or default, or an acquiescence therein, or of any similar breach or default thereafter occurring; nor shall any waiver of any breach or default be deemed a waiver of any other breach or default theretofore or thereafter occurring. Any waiver, permit, consent or approval of any kind or character on the part of any party to this Agreement of any breach or default under this Agreement, or any waiver on the part of any party of any provisions or conditions of this Agreement, must be in writing and shall be effective only to the extent specifically set forth in such writing. All remedies, either under this Agreement or by law or otherwise afforded to any holder shall be cumulative and not alternative.
16. Entire Agreement. This Agreement and the documents referred to herein constitute the entire agreement between the parties hereto pertaining to the subject matter hereof, and any and all other written or oral agreements existing between the parties hereto are expressly canceled.
[Signature Page Follows]
| D-6 |
IN WITNESS WHEREOF, the parties have executed this Lock-Up Agreement as of the date first written above.
| PARENT: | ||
| APOLLO MEDICAL HOLDINGS, INC. | ||
| By: | ||
| Name: | ||
| Title: | ||
| Address: 700 N. Brand Boulevard, Suite 1400 Glendale, CA 91203 |
||
| Facsimile: (818) 839-5190 | ||
| Attention: Mihir Shah | ||
| SHAREHOLDER: | ||
| (Signature) | ||
| Address: | ||
| Facsimile: | ||
| D-7 |
CERTIFICATE OF AMENDMENT
OF
RESTATED CERTIFICATE OF INCORPORATION
OF
APOLLO MEDICAL HOLDINGS, INC.
Apollo Medical Holdings, Inc., a corporation organized and existing under and by virtue of the General Corporation Law of the State of Delaware (the “Corporation”), does hereby certify as follows:
FIRST: The name of the Corporation is Apollo Medical Holdings, Inc. This Certificate of Amendment amends the Corporation’s Restated Certificate of Incorporation filed on January 16, 2015, and amended on April 24, 2015, October 16, 2015 and March 28, 2016.
SECOND: That Article XIII of the Restated Certificate of Incorporation of this Corporation is hereby amended by appending the following to Article XIII:
“The Board of Directors shall be divided into three (3) classes, Class I, Class II and Class III. The Board of Directors is authorized to assign members of the Board of Directors already in office to Class I, Class II or Class III. Each director shall serve for a term expiring at the third annual meeting following his or her election; provided, that, with respect to the directors serving in the inaugural classes of Class I, Class II and Class III, the terms of the directors serving in Class I shall expire at the Corporation’s first annual meeting of stockholders held after the effectiveness of the division of the Board of Directors into three (3) classes; the terms of the directors serving in Class II shall expire at the Corporation’s second annual meeting of stockholders held after such effectiveness; and the terms of the directors serving in Class III shall expire at the Corporation’s third annual meeting of stockholders held after such effectiveness. Each director shall serve until his or her successor is duly elected and qualified or until his or her death, resignation or removal.
Subject to the rights of the holders of any series of Preferred Stock then outstanding, newly created directorships resulting from any increase in the authorized number of directors or any vacancies in the Board of Directors resulting from death, resignation, retirement, disqualification, removal from office or other cause shall, unless otherwise required by law or by resolution of the Board of Directors, be filled only by a majority vote of the directors then in office, though less than a quorum (and not by the stockholders), and directors so chosen shall serve for a term expiring at the annual meeting of stockholders at which the term of office of the class to which they have been elected expires or until such director’s successor shall have been duly elected and qualified. No decrease in the number of authorized directors shall shorten the term of any incumbent director.
| E-1 |
Subject to the rights of the holders of any series of Preferred Stock then outstanding, any director, or the entire Board of Directors, may be removed from office at any time, but only for cause and only by the affirmative vote of the holders of a majority of the shares then entitled to vote at an election of directors, voting together as a single class.”
THIRD: This Certificate of Amendment has been duly adopted by the Board of Directors and stockholders of the Corporation in accordance with Section 242 of the Delaware General Corporation Law.
IN WITNESS WHEREOF, the Corporation has caused this Certificate of Amendment to be signed by its Chief Executive Officer on this __ day of ______, 2017.
| APOLLO MEDICAL HOLDINGS, INC., | ||
| a Delaware corporation | ||
| By: | ___________________ | |
| Warren Hosseinion, M.D., Chief Executive Officer | ||
| E-2 |
Amendment to Sections 3.1 and 3.2 of Article III of the Bylaws of
Apollo Medical Holdings, Inc.,
a Delaware corporation
Section 3.1 of Article III of the Bylaws of this Corporation shall be amended to by appending the following to Section 3.1:
“The Board of Directors shall be divided into three (3) classes, Class I, Class II and Class III, effective at the same time that the stockholders appoint and elect directors to the inaugural classes of Class I, Class II and Class III. Each director shall serve for a term expiring at the third annual meeting following his or her election; provided, that, with respect to the directors serving in the inaugural classes of Class I, Class II and Class III, the terms of the directors serving in Class I shall expire at the Corporation’s first annual meeting of stockholders held after the effectiveness of the division of the Board of Directors into three (3) classes; the terms of the directors serving in Class II shall expire at the Corporation’s second annual meeting of stockholders held after such effectiveness; and the terms of the directors serving in Class III shall expire at the Corporation’s third annual meeting of stockholders held after such effectiveness.
Section 3.2 of Article III of the Bylaws of this Corporation shall be amended by:
(i) appending the following language to the end of the first sentence of the first paragraph of Section 3.2:
“and directors so chosen shall serve for a term expiring at the annual meeting of stockholders at which the term of office of the class to which they have been elected expires or until such director’s successor shall have been duly elected and qualified”
and
(ii) deleting the second sentence of the first paragraph of Section 3.2.
| F-1 |

CONFIDENTIAL
December 21, 2016
The Board of Directors
Apollo Medical Holdings, Inc.
450 North Brand Blvd.
Suite 600
Glendale CA 91203
Members of the Board of Directors:
We understand that Apollo Medical Holdings, Inc. (“ApolloMed”) proposes to enter into an Agreement and Plan of Merger (the “Agreement”), among ApolloMed, Apollo Acquisition Corporation, a wholly owned subsidiary of ApolloMed (“Merger Sub”), Network Medical Management, Inc. (“NMM”), and Kenneth Sim, M.D. (the “Shareholders’ Representative”), pursuant to which, among other things, Merger Sub will merge with and into NMM (the “Transaction”) and each issued and outstanding share of the common stock with no par value per share of NMM (“NMM Common Stock”) will be converted into the right to receive such number of the common stock, par value $0.001 per share, of ApolloMed (“ApolloMed Common Stock”) that will result in the shareholders of NMM Common Stock holding, immediately following the time at which the Transaction becomes effective (the “Effective Time”), an aggregate number of ApolloMed Common Stock that represents eighty-two percent (82%) of the total issued and outstanding ApolloMed Common Stock immediately following the Effective Time (the “Exchange Ratio”). In arriving at our opinion, we have assumed and relied upon, at the direction of ApolloMed, that the Exchange Ratio will be 0.07002656301. The terms and conditions of the Transaction are more fully set forth in the Agreement.
You have requested our opinion as to the fairness, from a financial point of view, to ApolloMed of the Exchange Ratio provided for in the Transaction.
In connection with this opinion, we have, among other things:
| (i) | reviewed certain publicly available business and financial information relating to ApolloMed; |
| (ii) | reviewed certain internal financial and operating information with respect to the business, operations and prospects of NMM furnished to or discussed with us by the management of NMM, including certain financial forecasts relating to NMM prepared by the management of NMM (such forecasts, the “NMM Forecasts”); |
| (iii) | reviewed certain internal financial and operating information with respect to the business, operations and prospects of ApolloMed (excluding the Next Gen ACO business) furnished to or discussed with us by the management of ApolloMed, including certain financial forecasts relating to ApolloMed (excluding the Next Gen ACO business) prepared by the management of ApolloMed (such forecasts, the “ApolloMed (ex. Next Gen ACO) Forecasts”); |
| G-1 |
The Board of Directors
Apollo Medical Holdings, Inc.
Page 2
| (iv) | reviewed certain internal financial and operating information with respect to the business, operations and prospects of the Next Gen ACO business furnished to or discussed with us by the management of ApolloMed, including certain financial forecasts relating to the Next Gen ACO business prepared by the management of ApolloMed (such forecasts, the “Next Gen ACO Forecasts”); |
| (v) | reviewed certain estimates as to the amount and timing of cost savings and revenue enhancements (collectively, the “Synergies / Cost Savings”) anticipated by the management of ApolloMed to result from the Transaction; |
| (vi) | reviewed certain information, prepared by the management of ApolloMed, regarding the net operating losses held by ApolloMed and certain estimates regarding the utilization of such net operating losses for U.S. federal income tax purposes (the “NOL Projections”); |
| (vii) | discussed the past and current business, operations, financial condition and prospects of NMM with members of senior managements of NMM and ApolloMed, and discussed the past and current business, operations, financial condition and prospects of ApolloMed with members of senior management of ApolloMed; |
| (viii) | reviewed the potential pro forma financial impact of the Transaction on the future financial performance of ApolloMed, including the potential effect on ApolloMed’s estimated earnings per share; |
| (ix) | compared certain financial information of NMM and ApolloMed with similar information of other companies we deemed relevant; |
| (x) | reviewed a draft, dated December 20, 2016 of the Agreement (the “Draft Agreement”); and |
| (xi) | performed such other analyses and studies and considered such other information and factors as we deemed appropriate. |
In arriving at our opinion, we have assumed and relied upon, without independent verification, the accuracy and completeness of the financial and other information and data publicly available or provided to or otherwise reviewed by or discussed with us and have relied upon the assurances of the managements of ApolloMed and NMM that they are not aware of any facts or circumstances that would make such information or data inaccurate or misleading in any material respect. With respect to the NMM Forecasts, we have been advised by NMM, and have assumed, with the consent of ApolloMed, that they have been reasonably prepared on bases reflecting the best currently available estimates and good faith judgments of the management of NMM as to the future financial performance of NMM. In addition, we have assumed, at the direction of ApolloMed, that the NMM Forecasts reflect the best currently available estimates and good faith judgments of the management of ApolloMed as to the future financial performance of NMM. With respect to the ApolloMed (ex. Next Gen ACO) Forecasts, Next Gen ACO Forecasts, Synergies/Cost Savings and NOL Projections, we have assumed, at the direction of ApolloMed, that they have been reasonably prepared on bases reflecting the best currently available estimates and good faith judgments of the management of ApolloMed as to the future financial performance of ApolloMed (excluding the Next Gen ACO business), the Next Gen ACO business and the other matters covered thereby. We have relied, at the direction of ApolloMed, on the assessments of the management of ApolloMed as to ApolloMed’s ability to achieve the Synergies/Cost Savings and have been advised by ApolloMed, and have assumed, that the Synergies/Cost Savings will be realized in the amounts and at the times projected. We have relied, at the direction of ApolloMed, on the assessments of the management of ApolloMed as to the availability to ApolloMed of the net operating losses set out in the NOL Projections and have been advised by ApolloMed, and have assumed, that the NOL Projections will be utilized in the amounts and at the times projected.
| G-2 |
The Board of Directors
Apollo Medical Holdings, Inc.
Page 3
We have not made or been provided with any independent evaluation or appraisal of the assets or liabilities (contingent or otherwise) of NMM or ApolloMed, nor have we made any physical inspection of the properties or assets of NMM or ApolloMed. We have not evaluated the solvency or fair value of NMM or ApolloMed under any state, federal or other laws relating to bankruptcy, insolvency or similar matters. We have assumed, at the direction of ApolloMed, that the Transaction will be consummated in accordance with its terms, without waiver, modification or amendment of any material term, condition or agreement and that, in the course of obtaining the necessary governmental, regulatory and other approvals, consents, releases and waivers for the Transaction, no delay, limitation, restriction or condition, including any divestiture requirements or amendments or modifications, will be imposed that would have an adverse effect on NMM, ApolloMed or the contemplated benefits of the Transaction. We also have assumed, at the direction of ApolloMed, that that the final executed Agreement will not differ in any material respect from the Draft Agreement reviewed by us.
We express no view or opinion as to any terms or other aspects of the Transaction (other than the Exchange Ratio to the extent expressly specified herein), including, without limitation, the form or structure of the Transaction or any ongoing obligations of the parties pursuant to the Agreement. Our opinion is limited to the fairness, from a financial point of view, to ApolloMed of the Exchange Ratio provided for in the Transaction and no opinion or view is expressed with respect to any consideration received in connection with the Transaction by the holders of any class of securities, creditors or other constituencies of any party. In addition, no opinion or view is expressed with respect to the fairness (financial or otherwise) of the amount, nature or any other aspect of any compensation to any of the officers, directors or employees of any party to the Transaction, or class of such persons, relative to the Exchange Ratio. Furthermore, no opinion or view is expressed as to the relative merits of the Transaction in comparison to other strategies or transactions that might be available to ApolloMed or in which ApolloMed might engage or as to the underlying business decision of ApolloMed to proceed with or effect the Transaction. We are not expressing any opinion as to what the value of ApolloMed Common Stock actually will be when issued or the prices at which ApolloMed Stock will trade at any time, including following announcement or consummation of the Transaction. In addition, we express no opinion or recommendation as to how any shareholder should vote or act in connection with the Transaction or any related matter.
We have acted as financial advisor to ApolloMed in connection with the Transaction and will receive a fee for our services, a portion of which is payable in connection with the rendering of this opinion and a significant portion of which is contingent upon consummation of the Transaction. In addition, ApolloMed has agreed to reimburse our expenses and indemnify us against certain liabilities arising out of our engagement.
| G-3 |
The Board of Directors
Apollo Medical Holdings, Inc.
Page 4
We and our affiliates comprise a full service securities firm and commercial bank engaged in securities, commodities and derivatives trading, foreign exchange and other brokerage activities, and principal investing as well as providing investment, corporate and private banking, asset and investment management, financing and financial advisory services and other commercial services and products to a wide range of companies, governments and individuals. In the ordinary course of our businesses, we and our affiliates may invest on a principal basis or on behalf of customers or manage funds that invest, make or hold long or short positions, finance positions or trade or otherwise effect transactions in equity, debt or other securities or financial instruments (including derivatives, bank loans or other obligations) of ApolloMed, NMM and certain of their respective affiliates (including Fresenius SE & Co KGaA and Fresenius Medical Care Corporation (each and together, “Fresenius”), affiliates of NNA of Nevada, Inc., a shareholder in ApolloMed.
We and our affiliates in the past have provided, currently are providing, and in the future may provide, investment banking, commercial banking and other financial services to Fresenius and certain of its affiliates and have received or in the future may receive compensation for the rendering of these services, including having acted or acting as joint bookrunner, co-mandated arranger, administrative agent, and collateral agent for, and/or as a lender (including, in some cases, swing line lender and letter of credit lender) to Fresenius and/or certain of its affiliates and having provided or providing certain treasury, derivatives and foreign exchange trading services to Fresenius and certain of its affiliates.
It is understood that this letter is for the benefit and use of the Board of Directors of ApolloMed (in its capacity as such) in connection with and for purposes of its evaluation of the Transaction.
Our opinion is necessarily based on financial, economic, monetary, market and other conditions and circumstances as in effect on, and the information made available to us as of, the date hereof. It should be understood that subsequent developments may affect this opinion, and we do not have any obligation to update, revise, or reaffirm this opinion. The issuance of this opinion was approved by a fairness opinion review committee of Merrill Lynch, Pierce, Fenner & Smith Incorporated.
| G-4 |
The Board of Directors
Apollo Medical Holdings, Inc.
Page 5
Based upon and subject to the foregoing, including the various assumptions and limitations set forth herein, we are of the opinion on the date hereof that the Exchange Ratio provided for in the Transaction is fair, from a financial point of view, to ApolloMed.
Very truly yours,
/s/ Merrill Lynch, Pierce, Fenner & Smith
MERRILL LYNCH, PIERCE, FENNER & SMITH
INCORPORATED
| G-5 |
|
December 21, 2016
Board of Directors Network Medical Management, Inc. 1668 S. Garfield Avenue #200 Alhambra, CA 91801
Dear Board of Directors: |
VANTAGE POINT ADVISORS, INC. Take aim.
11455 EI Camino Real, Suite 450 San Diego, CA 92130 858.509.7545 www.vpadvisors.com
SAN DIEGO LOS ANGELES PHILADELPHIA NEW YORK |
We understand that Apollo Medical Holdings, Inc., a Delaware corporation (“Apollo” or the “Parent”), Apollo Acquisition Corp., a California corporation (“Merger Sub”), Network Medical Management, Inc., a California corporation (the “Company”) and Kenneth Sim, M.D. (the “Shareholders’ Representative”) intend to enter into an Agreement and Plan of Merger (“Agreement”), pursuant to which Merger Sub will merge with and into the Company, with the Company surviving such merger and continuing as a wholly-owned subsidiary of Parent in accordance with the California General Corporation Law (the “Transaction”). Capitalized terms used herein and not otherwise defined shall have the meanings given them in the Agreement.
Subject to the terms of the Agreement, each Company Share issued and outstanding immediately prior to the Effective Time shall be converted into the right to receive a number of fully paid and nonassessable Parent Shares such that, immediately following the Effective Time, the aggregate number of Parent Shares held by the Company’s Shareholders shall be equal to eighty-two percent (82%) of the total issued and outstanding Parent Shares immediately following the Effective Time (the “Exchange Ratio”). Notwithstanding the foregoing, and for the avoidance of doubt, for purposes of calculating the Exchange Ratio, the aggregate number of Parent Shares held by the Shareholders immediately following the Effective Time shall exclude (i) any Parent Shares owned by the Shareholders immediately prior to the Effective Time, (ii) the Parent Warrants, and (iii) any Parent Shares issued or issuable to the Shareholders pursuant to the exercise of the Parent Warrants.
You have asked us to render our opinion (the “Opinion”) as to whether the Transaction is fair, from a financial point of view, to the Company and its common shareholders. The Opinion addresses only the fairness, from a financial point of view, of the Exchange Ratio, and we do not express any views on any other terms of the Transaction. The Opinion does not address the Company’s underlying business decision to effect the Transaction. We have not been asked to, and did not, solicit third-party expressions of interest in acquiring all or any part of the Company’s assets or securities. Additionally, we have not been asked to negotiate the Transaction or advise you with respect to any alternative business strategies that might exist for the Company. Furthermore, we are not expressing any opinion, counsel or interpretation regarding matters that require legal, regulatory, environmental, accounting, insurance, tax or other similar professional advice. It is assumed that such opinions, counsel or interpretations have been or will be obtained from the appropriate professional sources. For avoidance of doubt, we are not expressing an opinion on the execution and delivery of the Agreement with missing or incomplete Disclosure Schedules, as described in Section 10.3 thereof.
In the course of our analyses for rendering this Opinion, we have among other things:
| H-1 |
Board of Directors
Network Medical Management, Inc.
Page 2 of 3
| 1. | reviewed an execution copy of the Agreement received by us on December 21, 2016; |
| 2. | reviewed the Company’s financial statements, which included audited financial statements for the twelve month periods ended December 31, 2011 through December 31, 2014, unaudited financial statements for the twelve month period ended December 31, 2015 and its unaudited interim financial statements for the nine month periods ended September 30, 2015 and September 30, 2016 (collectively, the “Financial Statements”); |
| 3. | reviewed Apollo Medical Holdings, Inc.’s financial statements as contained in its Form 10-K SEC filings for the 12-month periods ended January 31, 2012 through January 31, 2014, March 31, 2015 and March 31, 2016 and Form 10-Q SEC filings for the 6-month period ended September 30, 2016; |
| 4. | reviewed the Company Shareholders’ Agreement; |
| 5. | reviewed an up-to-date list of the names of the Company’s shareholders, including the total number of shares of capital stock of the Company outstanding as of the date hereof; |
| 6. | reviewed the Company’s Board of Directors Meeting Minutes from 2014 through the date hereof; |
| 7. | reviewed the letter from the Center for Medicare and Medicaid Innovation to APA ACO, Inc. dated August 1, 2016 regarding Next Generation ACO Model Application; |
| 8. | reviewed various corporate documents related to APA ACO, Inc.; |
| 9. | reviewed the Company’s schedule of all dividends paid to stockholders and bonuses paid to employees for the period beginning January 1, 2014 and ending November 21, 2016; |
| 10. | read certain operating and financial information, including projections, provided to us by management relating to the business prospects of the Company, Apollo and APA ACO, Inc.; |
| 11. | met with certain members of the Company’s and Apollo’s senior and operating management to discuss the Company’s operations, historical financial results and business prospects; |
| 12. | visited certain of the Company’s facilities in Alhambra, CA; |
| 13. | visited certain of Apollo’s facilities in Glendale, CA; |
| 14. | read other appraisals involving common stock of the Company; |
| 15. | evaluated the stock price history and press releases of Apollo; |
| H-2 |
Board of Directors
Network Medical Management, Inc.
Page 3 of 3
| 16. | analyzed certain financial, stock market and other publicly available information relating to the businesses of other companies whose operations and financings we considered relevant in evaluating those of the Company and Apollo; and |
| 17. | conducted such other studies, analyses, inquiries and investigations, as we deemed appropriate. |
In the course of our investigation, we have assumed and relied upon the accuracy and completeness of the financial statements, forecasts, projections and other information provided to us by management and we have further relied upon the assurances of management that they were unaware of any facts that would make the information provided to us incomplete or misleading. We have not assumed any responsibility for independent verification of such information or assurances.
In arriving at our Opinion, we have not performed any independent appraisal of the assets of the Company or Parent. Our analysis does not constitute an examination, review of, or compilation of prospective financial statements in accordance with standards established by the American Institute of Certified Public Accountants (“AICPA”). We do not express an opinion or any other form of assurance on the reasonableness of the underlying assumptions or whether any of the prospective financial statements, if used, are presented in conformity with AICPA presentation guidelines. Further, there will usually be differences between prospective and actual results because events and circumstances frequently do not occur as expected and those differences may be material. We have also assumed the Company is not currently involved in any material transaction other than the Transaction, and those activities undertaken in the ordinary course of conducting its business. In addition, we have relied upon and assumed, without independent verification, that the final form of the Agreement will not differ in any respect (relevant for purposes of this opinion) from the execution copy the Agreement identified above.
This Opinion is furnished solely for your benefit in your evaluation of the Transaction and does not constitute a recommendation to any shareholder of the Company as to how such shareholder should vote with respect to the Transaction. This Opinion is delivered to each recipient subject to the conditions, scope of engagement, limitations and understanding set forth in this Opinion and subject to the understanding that the obligations of Vantage Point Advisors, Inc. in the Transaction are solely corporate obligations. Furthermore, no officer, director, employee or shareholder of Vantage Point Advisors, Inc. shall be subjected to any personal liability whatsoever to any person, nor will any such claim be asserted by or on behalf of you or your affiliates.
On the basis of the forgoing, it is our opinion that, as of the date hereof, the Transaction is fair, from a financial point of view, to the Company and its common shareholders.
Very truly yours,
/s/ Vantage Point Advisors, Inc.
Vantage Point Advisors, Inc.
| H-3 |
Excerpt from the California General Corporation Law Concerning Dissenters’ Rights
CORPORATIONS CODE
TITLE 1. CORPORATIONS
DIVISION 1. GENERAL CORPORATION LAW
CHAPTER 13. DISSENTERS’ RIGHTS
§ 1300. Reorganization or short-form merger; dissenting shares; corporate purchase at fair market value; definitions
(a) If the approval of the outstanding shares (Section 152) of a corporation is required for a reorganization under subdivisions (a) and (b) or subdivision (e) or (f) of Section 1201, each shareholder of the corporation entitled to vote on the transaction and each shareholder of a subsidiary corporation in a short-form merger may, by complying with this chapter, require the corporation in which the shareholder holds shares to purchase for cash at their fair market value the shares owned by the shareholder which are dissenting shares as defined in subdivision (b). The fair market value shall be determined as of the day of, and immediately prior to, the first announcement of the terms of the proposed reorganization or short-form merger, excluding any appreciation or depreciation in consequence of the proposed reorganization or short-form merger, as adjusted for any stock split, reverse stock split, or share dividend that becomes effective thereafter.
(b) As used in this chapter, “dissenting shares” means shares to which all of the following apply:
(1) That were not, immediately prior to the reorganization or short-form merger, listed on any national securities exchange certified by the Commissioner of Corporations under subdivision (o) of Section 25100, and the notice of meeting of shareholders to act upon the reorganization summarizes this section and Sections 1301, 1302, 1303 and 1304; provided, however, that this provision does not apply to any shares with respect to which there exists any restriction on transfer imposed by the corporation or by any law or regulation; and provided, further, that this provision does not apply to any shares where the holder of those shares is required, by the terms of the reorganization or short-form merger, to accept for the shares anything except: (A) shares of any other corporation, which shares, at the time the reorganization or short-form merger is effective, are listed on any national securities exchange certified by the Commissioner of Corporations under subdivision (o) of Section 25100; (B) cash in lieu of fractional shares described in the foregoing subparagraph (A); or (C) any combination of the shares and cash in lieu of fractional shares described in the foregoing subparagraphs (A) and (B).
(2) That were outstanding on the date for the determination of shareholders entitled to vote on the reorganization and (A) were not voted in favor of the reorganization or, (B) if described in paragraph (1), were voted against the reorganization, or were held of record on the effective date of a short-form merger; provided, however, that subparagraph (A) rather than subparagraph (B) of this paragraph applies in any case where the approval required by Section 1201 is sought by written consent rather than at a meeting.
(3) That the dissenting shareholder has demanded that the corporation purchase at their fair market value, in accordance with Section 1301.
(4) That the dissenting shareholder has submitted for endorsement, in accordance with Section 1302.
(c) As used in this chapter, “dissenting shareholder” means the recordholder of dissenting shares and includes a transferee of record.
§ 1301. Notice to holders of dissenting shares in reorganizations; demand for purchase; time; contents
(a) If, in the case of a reorganization, any shareholders of a corporation have a right under Section 1300, subject to compliance with paragraphs (3) and (4) of subdivision (b) thereof, to require the corporation to purchase their shares for cash, that corporation shall mail to each of those shareholders a notice of the approval of the reorganization by its outstanding shares (Section 152) within 10 days after the date of that approval, accompanied by a copy of Sections 1300, 1302, 1303, and 1304 and this section, a statement of the price determined by the corporation to represent the fair market value of the dissenting shares, and a brief description of the procedure to be followed if the shareholder desires to exercise the shareholder’s right under those sections. The statement of price constitutes an offer by the corporation to purchase at the price stated any dissenting shares as defined in subdivision (b) of Section 1300, unless they lose their status as dissenting shares under Section 1309.
| I-1 |
(b) Any shareholder who has a right to require the corporation to purchase the shareholder’s shares for cash under Section 1300, subject to compliance with paragraphs (3) and (4) of subdivision (b) thereof, and who desires the corporation to purchase shares shall make written demand upon the corporation for the purchase of those shares and payment to the shareholder in cash of their fair market value. The demand is not effective for any purpose unless it is received by the corporation or any transfer agent thereof (1) in the case of shares described in subdivision (b) of Section 1300, not later than the date of the shareholders’ meeting to vote upon the reorganization, or (2) in any other case, within 30 days after the date on which the notice of the approval by the outstanding shares pursuant to subdivision (a) or the notice pursuant to subdivision (h) of Section 1110 was mailed to the shareholder.
(c) The demand shall state the number and class of the shares held of record by the shareholder which the shareholder demands that the corporation purchase and shall contain a statement of what the shareholder claims to be the fair market value of those shares as determined pursuant to subdivision (a) of Section 1300. The statement of fair market value constitutes an offer by the shareholder to sell the shares at that price.
§ 1302. Submission of share certificates for endorsement; uncertificated securities
Within 30 days after the date on which notice of the approval by the outstanding shares or the notice pursuant to subdivision (h) of Section 1110 was mailed to the shareholder, the shareholder shall submit to the corporation at its principal office or at the office of any transfer agent thereof, (a) if the shares are certificated securities, the shareholder’s certificates representing any shares which the shareholder demands that the corporation purchase, to be stamped or endorsed with a statement that the shares are dissenting shares or to be exchanged for certificates of appropriate denomination so stamped or endorsed or (b) if the shares are uncertificated securities, written notice of the number of shares which the shareholder demands that the corporation purchase. Upon subsequent transfers of the dissenting shares on the books of the corporation, the new certificates, initial transaction statement, and other written statements issued therefor shall bear a like statement, together with the name of the original dissenting holder of the shares.
§ 1303. Payment of agreed price with interest; agreement fixing fair market value; filing; time of payment
(a) If the corporation and the shareholder agree that the shares are dissenting shares and agree upon the price of the shares, the dissenting shareholder is entitled to the agreed price with interest thereon at the legal rate on judgments from the date of the agreement. Any agreements fixing the fair market value of any dissenting shares as between the corporation and the holders thereof shall be filed with the secretary of the corporation.
(b) Subject to the provisions of Section 1306, payment of the fair market value of dissenting shares shall be made within 30 days after the amount thereof has been agreed or within 30 days after any statutory or contractual conditions to the reorganization are satisfied, whichever is later, and in the case of certificated securities, subject to surrender of the certificates therefor, unless provided otherwise by agreement.
§ 1304. Action to determine whether shares are dissenting shares or fair market value; limitation; joinder; consolidation; determination of issues; appointment of appraisers
(a) If the corporation denies that the shares are dissenting shares, or the corporation and the shareholder fail to agree upon the fair market value of the shares, then the shareholder demanding purchase of such shares as dissenting shares or any interested corporation, within six months after the date on which notice of the approval by the outstanding shares (Section 152) or notice pursuant to subdivision (h) of Section 1110 was mailed to the shareholder, but not thereafter, may file a complaint in the superior court of the proper county praying the court to determine whether the shares are dissenting shares or the fair market value of the dissenting shares or both or may intervene in any action pending on such a complaint.
(b) Two or more dissenting shareholders may join as plaintiffs or be joined as defendants in any such action and two or more such actions may be consolidated.
(c) On the trial of the action, the court shall determine the issues. If the status of the shares as dissenting shares is in issue, the court shall first determine that issue. If the fair market value of the dissenting shares is in issue, the court shall determine, or shall appoint one or more impartial appraisers to determine, the fair market value of the shares.
| I-2 |
§ 1305. Report of appraisers; confirmation; determination by court; judgment; payment; appeal; costs
(a) If the court appoints an appraiser or appraisers, they shall proceed forthwith to determine the fair market value per share. Within the time fixed by the court, the appraisers, or a majority of them, shall make and file a report in the office of the clerk of the court. Thereupon, on the motion of any party, the report shall be submitted to the court and considered on such evidence as the court considers relevant. If the court finds the report reasonable, the court may confirm it.
(b) If a majority of the appraisers appointed fail to make and file a report within 10 days from the date of their appointment or within such further time as may be allowed by the court or the report is not confirmed by the court, the court shall determine the fair market value of the dissenting shares.
(c) Subject to the provisions of Section 1306, judgment shall be rendered against the corporation for payment of an amount equal to the fair market value of each dissenting share multiplied by the number of dissenting shares which any dissenting shareholder who is a party, or who has intervened, is entitled to require the corporation to purchase, with interest thereon at the legal rate from the date on which judgment was entered.
(d) Any such judgment shall be payable forthwith with respect to uncertificated securities and, with respect to certificated securities, only upon the endorsement and delivery to the corporation of the certificates for the shares described in the judgment. Any party may appeal from the judgment.
(e) The costs of the action, including reasonable compensation to the appraisers to be fixed by the court, shall be assessed or apportioned as the court considers equitable, but, if the appraisal exceeds the price offered by the corporation, the corporation shall pay the costs (including in the discretion of the court attorneys’ fees, fees of expert witnesses and interest at the legal rate on judgments from the date of compliance with Sections 1300, 1301 and 1302 if the value awarded by the court for the shares is more than 125 percent of the price offered by the corporation under subdivision (a) of Section 1301).
§ 1306. Prevention of immediate payment; status as creditors; interest
To the extent that the provisions of Chapter 5 prevent the payment to any holders of dissenting shares of their fair market value, they shall become creditors of the corporation for the amount thereof together with interest at the legal rate on judgments until the date of payment, but subordinate to all other creditors in any liquidation proceeding, such debt to be payable when permissible under the provisions of Chapter 5.
§ 1307. Dividends on dissenting shares
Cash dividends declared and paid by the corporation upon the dissenting shares after the date of approval of the reorganization by the outstanding shares (Section 152) and prior to payment for the shares by the corporation shall be credited against the total amount to be paid by the corporation therefor.
§ 1308. Rights of dissenting shareholders pending valuation; withdrawal of demand for payment
Except as expressly limited in this chapter, holders of dissenting shares continue to have all the rights and privileges incident to their shares, until the fair market value of their shares is agreed upon or determined. A dissenting shareholder may not withdraw a demand for payment unless the corporation consents thereto.
§ 1309. Termination of dissenting share and shareholder status
Dissenting shares lose their status as dissenting shares and the holders thereof cease to be dissenting shareholders and cease to be entitled to require the corporation to purchase their shares upon the happening of any of the following:
| I-3 |
(a) The corporation abandons the reorganization. Upon abandonment of the reorganization, the corporation shall pay on demand to any dissenting shareholder who has initiated proceedings in good faith under this chapter all necessary expenses incurred in such proceedings and reasonable attorneys’ fees.
(b) The shares are transferred prior to their submission for endorsement in accordance with Section 1302 or are surrendered for conversion into shares of another class in accordance with the articles.
(c) The dissenting shareholder and the corporation do not agree upon the status of the shares as dissenting shares or upon the purchase price of the shares, and neither files a complaint or intervenes in a pending action as provided in Section 1304, within six months after the date on which notice of the approval by the outstanding shares or notice pursuant to subdivision (h) of Section 1110 was mailed to the shareholder.
(d) The dissenting shareholder, with the consent of the corporation, withdraws the shareholder’s demand for purchase of the dissenting shares.
§ 1310. Suspension of right to compensation or valuation proceedings; litigation of shareholders’ approval
If litigation is instituted to test the sufficiency or regularity of the votes of the shareholders in authorizing a reorganization, any proceedings under Sections 1304 and 1305 shall be suspended until final determination of such litigation.
§ 1311. Exempt shares
This chapter, except Section 1312, does not apply to classes of shares whose terms and provisions specifically set forth the amount to be paid in respect to such shares in the event of a reorganization or merger.
§ 1312. Right of dissenting shareholder to attack, set aside or rescind merger or reorganization; restraining order or injunction; conditions
(a) No shareholder of a corporation who has a right under this chapter to demand payment of cash for the shares held by the shareholder shall have any right at law or in equity to attack the validity of the reorganization or short-form merger, or to have the reorganization or short-form merger set aside or rescinded, except in an action to test whether the number of shares required to authorize or approve the reorganization have been legally voted in favor thereof; but any holder of shares of a class whose terms and provisions specifically set forth the amount to be paid in respect to them in the event of a reorganization or short-form merger is entitled to payment in accordance with those terms and provisions or, if the principal terms of the reorganization are approved pursuant to subdivision (b) of Section 1202, is entitled to payment in accordance with the terms and provisions of the approved reorganization.
(b) If one of the parties to a reorganization or short-form merger is directly or indirectly controlled by, or under common control with, another party to the reorganization or short-form merger, subdivision (a) shall not apply to any shareholder of such party who has not demanded payment of cash for such shareholder’s shares pursuant to this chapter; but if the shareholder institutes any action to attack the validity of the reorganization or short-form merger or to have the reorganization or short-form merger set aside or rescinded, the shareholder shall not thereafter have any right to demand payment of cash for the shareholder’s shares pursuant to this chapter. The court in any action attacking the validity of the reorganization or short-form merger or to have the reorganization or short-form merger set aside or rescinded shall not restrain or enjoin the consummation of the transaction except upon 10 days’ prior notice to the corporation and upon a determination by the court that clearly no other remedy will adequately protect the complaining shareholder or the class of shareholders of which such shareholder is a member.
(c) If one of the parties to a reorganization or short-form merger is directly or indirectly controlled by, or under common control with, another party to the reorganization or short-form merger, in any action to attack the validity of the reorganization or short-form merger or to have the reorganization or short-form merger set aside or rescinded, (1) a party to a reorganization or short-form merger which controls another party to the reorganization or short-form merger shall have the burden of proving that the transaction is just and reasonable as to the shareholders of the controlled party, and (2) a person who controls two or more parties to a reorganization shall have the burden of proving that the transaction is just and reasonable as to the shareholders of any party so controlled.
§ 1313. Conversions deemed to constitute a reorganization; application of chapter
A conversion pursuant to Chapter 11.5 (commencing with Section 1150) shall be deemed to constitute a reorganization for purposes of applying the provisions of this chapter, in accordance with and to the extent provided in Section 1159.
| I-4 |
PART II
INFORMATION NOT REQUIRED IN JOINT PROXY STATEMENT/PROSPECTUS
Item 20. Indemnification of Directors and Officers
ApolloMed is a Delaware corporation. Reference is made to Section 102(b)(7) of the Delaware General Corporation Law, which enables a corporation in its original certificate of incorporation or an amendment thereto to eliminate or limit the personal liability of a director for violations of the director’s fiduciary duty, except (1) for any breach of the director’s duty of loyalty to the corporation or its stockholders, (2) for acts or omissions not in good faith or which involve intentional misconduct or a knowing violation of law, (3) pursuant to Section 174 of the Delaware General Corporation Law (providing for liability of directors for unlawful payment of dividends or unlawful stock purchase or redemptions) or (4) for any transaction from which a director derived an improper personal benefit.
Reference also is made to Section 145 of the Delaware General Corporation Law, which provides that a corporation may indemnify any persons, including officers and directors, who are, or are threatened to be made, parties to any threatened, pending or completed legal action, suit or proceeding, whether civil, criminal, administrative or investigative (other than an action by or in the right of such corporation), by reason of the fact that such person was an officer, director, employee or agent of such corporation or is or was serving at the request of such corporation as a director, officer, employee or agent of another corporation or enterprise. The indemnity may include expenses (including attorney’s fees), judgments, fines and amounts paid in settlement actually and reasonably incurred by such person in connection with such action, suit or proceeding, provided such officer, director, employee or agent acted in good faith and in a manner he reasonably believed to be in or not opposed to the corporation’s best interest and, for criminal proceedings, had no reasonable cause to believe that his conduct was unlawful. A Delaware corporation may indemnify officers and directors in an action by or in the right of the corporation under the same conditions, except that no indemnification is permitted without judicial approval if the officer or director is adjudged to be liable to the corporation. Where an officer or director is successful on the merits or otherwise in the defense of any action referred to above, the corporation must indemnify him against the expenses that such officer or director actually and reasonably incurred.
The ApolloMed Bylaws allow for, and the ApolloMed Charter provides for, indemnification of ApolloMed’s current and former directors, officers, committee members or representatives to the full extent permitted by Delaware law. ApolloMed has an existing Directors and Officers Insurance Policy that provides coverage for its directors and officers in certain situations. ApolloMed has also entered into indemnification agreements with its directors and executive officers, in addition to the indemnification provided for in the ApolloMed Charter and ApolloMed Bylaws.
Item 21. Exhibits and Financial Statements
(a) Exhibit Index
A list of exhibits filed with this registration statement on Form S-4 is set forth on the Exhibit Index and is incorporated herein by reference.
(b) Financial Statements
The financial statements filed with this registration statement on Form S-4 are set forth on the Financial Statement Index and is incorporated herein by reference.
Item 22. Undertakings
(a) The undersigned registrant hereby undertakes:
| 1 |
(1) To file, during any period in which offers or sales are being made, a post-effective amendment to this registration statement:
(i) to include any prospectus required by Section 10(a)(3) of the Securities Act of 1933;
(ii) to reflect in the prospectus any facts or events arising after the effective date of the registration statement (or the most recent post-effective amendment thereof) which, individually or in the aggregate, represent a fundamental change in the information set forth in the registration statement. Notwithstanding the foregoing, any increase or decrease in volume of securities offered (if the total dollar value of securities offered would not exceed that which was registered) and any deviation from the low or high end of the estimated maximum offering range may be reflected in the form of prospectus filed with the Securities and Exchange Commission pursuant to Rule 424(b) if, in the aggregate, the changes in volume and price represent no more than a 20 percent change in the maximum aggregate offering price set forth in the “Calculation of Registration Fee” table in the effective registration statement; and
(iii) to include any material information with respect to the plan of distribution not previously disclosed in the registration statement or any material change to such information in the registration statement.
(2) That, for the purpose of determining any liability under the Securities Act of 1933, each such post-effective amendment shall be deemed to be a new registration statement relating to the securities offered therein, and the offering of such securities at that time shall be deemed to be the initial bona fide offering thereof.
(3) To remove from registration by means of a post-effective amendment any of the securities being registered which remain unsold at the termination of the offering.
(b) The undersigned registrant hereby undertakes as follows:
(1) That prior to any public reoffering of the securities registered hereunder through use of a proxy statement/prospectus/information statement which is a part of this registration statement, by any person or party who is deemed to be an underwriter within the meaning of Rule 145(c), the issuer undertakes that such reoffering proxy statement/prospectus/information statement will contain the information called for by the applicable registration form with respect to reofferings by persons who may be deemed underwriters, in addition to the information called for by the other items of the applicable form.
(2) That every proxy statement/prospectus (i) that is filed pursuant to paragraph (b)(1) immediately preceding, or (ii) that purports to meet the requirements of Section 10(a)(3) of the Securities Act and is used in connection with an offering of securities subject to Rule 415, will be filed as a part of an amendment to the registration statement and will not be used until such amendment is effective, and that, for purposes of determining any liability under the Securities Act, each such post-effective amendment shall be deemed to be a new registration statement relating to the securities offered therein, and the offering of such securities at that time shall be deemed to be the initial bona fide offering thereof.
(3) To respond to requests for information that is incorporated by reference into this proxy statement/prospectus/information statement pursuant to Item 4 10(b), 11, or 13 of this Form, within one business day of receipt of such request, and to send the incorporated documents by first class mail or other equally prompt means. This includes information contained in documents filed subsequent to the effective date of the registration statement through the date of responding to the request.
(4) To supply by means of a post-effective amendment all information concerning a transaction, and the company being acquired involved therein, that was not the subject of and included in the registration statement when it became effective.
| 2 |
(c) Insofar as indemnification for liabilities arising under the Securities Act may be permitted to directors, officers and controlling persons of the registrant pursuant to the foregoing provisions, or otherwise, the registrant has been advised that in the opinion of the Securities and Exchange Commission such indemnification is against public policy as expressed in the Securities Act and is, therefore, unenforceable. In the event that a claim for indemnification against such liabilities (other than the payment by the registrant of expenses incurred or paid by a director, officer or controlling person of the registrant in the successful defense of any action, suit or proceeding) is asserted by such director, officer or controlling person in connection with the securities being registered, the registrant will, unless in the opinion of its counsel the matter has been settled by controlling precedent, submit to a court of appropriate jurisdiction the question whether such indemnification by it is against public policy as expressed in the Securities Act and will be governed by the final adjudication of such issue.
| 3 |
Pursuant to the requirements of the Securities Act of 1933, as amended, the registrant has duly caused this registration statement to be signed on its behalf by the undersigned, thereunto duly authorized, in the city of Glendale, State of California, on the 30th day of October, 2017.
| APOLLO MEDICAL HOLDINGS, INC. | ||
| By: | /s/ Warren Hosseinion, M.D. | |
| Warren Hosseinion, M.D. | ||
| Chief Executive Officer | ||
Pursuant to the requirements of the Securities Act of 1933, as amended, this registration statement has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
Signature |
Title |
Date |
||
/s/ Warren Hosseinion, M.D. |
Chief Executive Officer and Director | October 30, 2017 | ||
| Warren Hosseinion, M.D. | (Principal Executive Officer) | |||
/s/ Mihir Shah |
Chief Financial Officer | October 30, 2017 | ||
| Mihir Shah | (Principal Financial Officer and Principal Accounting Officer) | |||
* |
Executive Chairman and Director | October 30, 2017 | ||
| Gary Augusta | ||||
* |
Director | October 30, 2017 | ||
| Mark Fawcett | ||||
* |
Director | October 30, 2017 | ||
| Suresh Nihalani | ||||
* |
Director | October 30, 2017 | ||
| David Schmidt | ||||
* |
Director | October 30, 2017 | ||
| Thomas Lam, M.D. | ||||
* |
Director | October 30, 2017 | ||
Ted Schreck |
||||
| * By: | /s/ Warren Hosseinion, M.D. | ||
| Warren Hosseinion | |||
| Attorney-in-fact |
| 4 |
Exhibit Index
| 1 |
| 2 |
| 3 |
| 4 |
| 5 |
| 101.INS# | XBRL Instance Document. | |
| 101.SCH# | XBRL Taxonomy Extension Schema Document. | |
| 101.CAL# | XBRL Taxonomy Extension Calculation Linkbase Document. | |
| 101.DEF# | XBRL Taxonomy Extension Definition Linkbase Document. | |
| 101.LAB# | XBRL Taxonomy Extension Label Linkbase Document. | |
| 101.PRE# | XBRL Taxonomy Extension Presentation Linkbase Document. | |
|
* ** |
Previously filed To be filed by amendment |
|
| # | Filed herewith | |
| + | Management contract or compensatory plan, contract or arrangement | |
| † | The schedules and exhibits to this exhibit have been omitted pursuant to Item 601(b)(2) of Regulation S-K. A copy of any omitted schedule and/or exhibit will be furnished to the SEC upon request. |
| 6 |