10-K: Annual report pursuant to Section 13 and 15(d)
Published on February 29, 2024
UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
FORM 10-K
(Mark One)
| ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 | |||||
For the fiscal year ended December 31 , 2023
OR
| TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
|||||
for the transition period from ___ to ___ .
Commission file number: 001-37392

(Exact name of registrant as specified in its charter)
| (State or other jurisdiction of incorporation or organization) |
(I.R.S. Employer Identification No.) |
|||||||
(Address of principal executive offices, including zip code)
Registrant’s telephone number, including area code: (626 ) 282-0288
Securities registered pursuant to Section 12(b) of the Act:
| Title of Each Class | Trading Symbol | Name of Each Exchange on Which Registered | ||||||||||||
Securities registered pursuant to Section 12(g) of the Act:
None
(Title of class)
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ☒ No ☐
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Exchange Act. Yes ☐ No ☒
Indicate by check mark whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ☒ No ☐
Indicate by check mark whether the registrant has submitted electronically every Interactive Data File required to be submitted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit such files). Yes ☒ No ☐
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company, or an emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company,” and “emerging growth company” in Rule 12b-2 of the Exchange Act.
| ☒ | Accelerated filer |
☐
|
|||||||||
| Non-accelerated filer |
☐
|
Smaller reporting company | |||||||||
| Emerging growth company | |||||||||||
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Indicate by check mark whether the registrant has filed a report on and attestation to its management’s assessment of the effectiveness of its internal control over financial reporting under Section 404(b) of the Sarbanes-Oxley Act (15 U.S.C. 7262(b)) by the registered public accounting firm that prepared or issued its audit report. ☒
If securities are registered pursuant to Section 12(b) of the Act, indicate by check mark whether the financial statements of the registrant included in the filing reflect the correction of an error to previously issued financial statements. ☐
Indicate by check mark whether any of those error corrections are restatements that required a recovery analysis of incentive-based compensation received by any of the registrant’s executive officers during the relevant recovery period pursuant to §240.10D-1(b).☐
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Act). ☐ Yes ☒ No
The aggregate market value of common stock held by non-affiliates of the registrant, as of June 30, 2023, the last day of the registrant’s most recently completed second fiscal quarter, was approximately $1.3 billion (based on the closing price for shares of the registrant’s common stock as reported by the Nasdaq Stock Market on June 30, 2023).
As of February 22, 2024, there were 55,423,408 shares of common stock of the registrant, $0.001 par value per share, issued and outstanding, which includes 7,132,698 treasury shares that are owned by Allied Physicians of California, a Professional Medical Corporation d.b.a. Allied Pacific of California IPA (“APC”), a consolidated affiliate of Astrana Health, Inc. These shares are legally issued and outstanding but treated as treasury shares for accounting purposes.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the registrant’s definitive Proxy Statement for the 2024 annual meeting of the stockholders of the registrant are incorporated herein by reference in Part III of this Annual Report on Form 10-K to the extent stated herein. Such Proxy Statement will be filed with the Securities and Exchange Commission (the “SEC”) within 120 days of the registrant’s fiscal year ended December 31, 2023.
Table of Contents
Astrana Health, Inc.
Form 10-K
Fiscal Year Ended December 31, 2023
| Page | ||||||||
| ITEM | ||||||||
2
Glossary
The following abbreviations or acronyms that may be used in this document shall have the adjacent meanings set forth below:
| AAMG | All-American Medical Group | ||||
ACO REACH |
ACO Realizing Equity, Access, and Community Health | ||||
| AHMC | AHMC Healthcare Inc. | ||||
AHM |
Astrana Health Management, Inc. (f/k/a Network Medical Management Inc.) |
||||
| AIPBP | All-Inclusive Population-Based Payments | ||||
| APAACO | APA ACO, Inc. | ||||
| APC | Allied Physicians of California, a Professional Medical Corporation | ||||
| APC-LSMA | APC-LSMA Designated Shareholder Medical Corporation | ||||
Astrana Medical |
Astrana Health Medical Corporation (f/k/a AP-AMH Medical Corporation) |
||||
Astrana Care Partners Medical |
Astrana Care Partners Medical Corporation (f/k/a AP - AMH 2 Medical Corporation) |
||||
| CAIPA MSO | CAIPA MSO, LLC | ||||
| CMS | Centers for Medicare & Medicaid Services | ||||
| DMHC | California Department of Managed Health Care |
||||
| DMG | Diagnostic Medical Group of Southern California | ||||
| GPDC | Global and Professional Direct Contracting | ||||
| HSMSO | Health Source MSO Inc., a California corporation | ||||
| IPA | Independent Practice Association | ||||
| Jade | Jade Health Care Medical Group, Inc. | ||||
| LMA | LaSalle Medical Associates | ||||
| NGACO | Next Generation Accountable Care Organization | ||||
| PMIOC | Pacific Medical Imaging and Oncology Center, Inc. | ||||
| Sun Labs | Sun Clinical Labs | ||||
| VIE | Variable Interest Entity | ||||
3
INTRODUCTORY NOTE
Unless the context dictates otherwise, references in this Annual Report on Form 10-K to the “Company,” “we,” “us,” “our,” and similar words are references to Astrana Health, Inc., a Delaware corporation (“Astrana”), and its consolidated subsidiaries and affiliated entities, as appropriate, including its consolidated variable interest entities (“VIEs”).
The following discussion and analysis provides information that management believes is relevant to an assessment and understanding of our results of operations and financial performance. This discussion should be read in conjunction with the consolidated financial statements and notes thereto appearing elsewhere herein, and with our prior filings with the Securities and Exchange Commission (the “SEC”).
The Centers for Medicare & Medicaid Services (“CMS”) have not reviewed any statements contained in this Report, including statements describing the participation of APA ACO, Inc. (“APAACO”) in the Global and Professional Direct Contracting Model (“GPDC Model”) or the ACO Realizing Equity, Access, and Community Health Model (“ACO REACH Model”).
Trade names and trademarks of Astrana and its subsidiaries referred to herein, and their respective logos, are our property. This Annual Report on Form 10-K may contain additional trade names and/or trademarks of other companies, which are the property of their respective owners. We do not intend our use or display of other companies’ trade names and/or trademarks, if any, to imply an endorsement or sponsorship of us by such companies, or any relationship with any of these companies.
4
NOTE ABOUT FORWARD-LOOKING STATEMENTS
This Annual Report on Form 10-K contains “forward-looking statements” within the meaning of the Private Securities Litigation Reform Act of 1995, Section 27A of the Securities Act of 1933, as amended (the “Securities Act”), and Section 21E of the Securities Exchange Act of 1934, as amended (the “Exchange Act”). All statements other than statements of historical fact are “forward-looking statements” for purposes of federal and state securities laws, including, but not limited to, any statements about our business, financial condition, operating results, plans, objectives, expectations, and intentions; any projections of earnings, revenue, earnings before interest, taxes, depreciation, and amortization (“EBITDA”), Adjusted EBITDA, or other financial items, such as our projected capitation from CMS, our forward-looking guidance and our future liquidity; any statements of any plans, strategies, and objectives of management for future operations, such as the material opportunities that we believe exist for our Company; any statements concerning proposed services, developments, mergers, or acquisitions; any statements with respect to dividends or stock repurchases and timing, methods, and payment of same; any statements regarding the outlook of the GPDC Model, ACO REACH Model, or strategic transactions; any statements regarding management’s view of future expectations and prospects for us; any statements about prospective adoption of new accounting standards or effects of changes in accounting standards; our ability to maintain effective internal control over financial reporting and disclosure controls and procedures; any statements regarding potential changes to our tax structure; any statements regarding future economic conditions or performance; any statements of belief; any statements of assumptions underlying any of the foregoing; and other statements that are not historical facts. Forward-looking statements may be identified by the use of forward-looking terms, such as “anticipate,” “could,” “can,” “may,” “might,” “potential,” “predict,” “should,” “estimate,” “expect,” “project,” “believe,” “think,” “plan,” “envision,” “intend,” “continue,” “target,” “seek,” “contemplate,” “budgeted,” “will,” or “would,” and the negative of such terms, other variations on such terms or other similar or comparable words, phrases, or terminology.
Forward-looking statements involve risks and uncertainties, many of which are difficult to predict and are outside of our control, and are based on the current beliefs, expectations, and certain assumptions of management. Some or all of such beliefs, expectations, and assumptions may not materialize or may vary significantly from actual results. Such statements are qualified by important economic, competitive, governmental, and technological factors that could cause our business, strategy, or actual results or events to differ materially from those in our forward-looking statements. Factors that might cause or contribute to such differences include, but are not limited to, those discussed in this Annual Report on Form 10-K, including the risk factors discussed under the heading “Risk Factors” in Part I, Item 1A below. Although we believe that the expectations reflected in our forward-looking statements are reasonable, actual results could differ materially from those projected or assumed in any of our forward-looking statements. Our future financial condition and results of operations, as well as any forward-looking statements, are subject to change and significant risks and uncertainties that could cause actual conditions, outcomes, and results to differ materially from those indicated by such statements. Any forward-looking statement made by the Company in this Form 10-K speaks only as of the date on which it is made. The Company undertakes no obligation to publicly update any forward-looking statement, whether as a result of new information, future developments or otherwise, except as may be required by any applicable securities laws.
5
PART I
Item 1. Business
Overview
On February 26, 2024, Apollo Medical Holdings, Inc. rebranded as Astrana Health, Inc. Astrana is a leading provider-centric, technology-powered, risk-bearing healthcare company. Leveraging its proprietary end-to-end technology solutions, Astrana operates an integrated healthcare delivery platform that enables providers to successfully participate in value-based care arrangements, thus empowering them to deliver accessible, high-quality care to patients in a cost-effective manner. We, together with our affiliated physician groups and consolidated entities, provide coordinated outcomes-based medical care serving patients in California, Nevada, and Texas, the majority of whom are covered by private or public insurance provided through Medicare, Medicaid, and health maintenance organizations (“HMOs”), with a small portion of our revenue coming from non-insured patients. We provide care coordination services to each major constituent of the healthcare delivery system, including patients, families, primary care physicians, specialists, acute care hospitals, alternative sites of inpatient care, physician groups, and health plans. Our physician network consists of primary care physicians, specialist physicians, physician and specialist extenders, and hospitalists. Astrana’s common stock is listed on The Nasdaq Stock Market LLC (“Nasdaq”) and trades under the symbol “ASTH”.
Led by a management team with several decades of experience, we have built a company and culture that is focused on physicians providing high-quality medical care, population health management, and care coordination for patients. Through our integrated health network, with more than 10,000 contracted physicians, we are responsible for coordinating value-based care for approximately 0.9 million patients as of December 31, 2023. As a result, we believe we are well-positioned to take advantage of the shift in the U.S. healthcare industry toward providing value-based and results-oriented healthcare with a focus on patient satisfaction, high-quality care, and cost efficiency. We implement and operate different innovative healthcare models, primarily including the following three reportable segments:
•Care Partners;
•Care Delivery; and
•Care Enablement.
Care Partners
Our Care Partners segment is focused on building and managing high-quality and high-performance provider networks by partnering with, empowering, and investing in strong provider partners aligned on a shared vision for coordinated care delivery. Astrana meets providers where they are and enables independent providers to remain independent while succeeding in value-based care. Astrana acts as “single payer” for our network of providers, enabling value-based care arrangements including hospital shared-risk contracts. By leveraging our unique care enablement platform and ability to recruit, empower, and incentivize physicians to effectively manage total cost of care, we are able to organize partnered providers into successful multi-payer risk-bearing organizations that take on varying levels of risk based on total cost of care across membership in all lines of business, including Medicare fee for service (“FFS”), Medicare Advantage, Medicaid, Commercial, and Exchange. Through our network of “independent practice associations” (“IPAs”), “accountable care organizations” (“ACOs”), and Restricted Knox-Keene (“RKK”) licensed health plan, our healthcare delivery entities are responsible for coordinating and delivering high-quality care to our patients and ensuring continuity of care in Astrana’s ecosystem across age, stage of life, or life circumstance.
An IPA is an association of independent physicians, or other organization that contracts with independent physicians, and provides services to HMOs, which are medical insurance groups that provide health services generally for a fixed annual fee, on a negotiated per capita rate, flat retainer fee, or negotiated FFS basis. Our affiliated IPAs comprise a network of independent primary care physicians and specialists who collectively care for patients. Our IPAs contract with various HMOs and other licensed healthcare service plans, as defined in the California Knox-Keene Health Care Service Plan Act of 1975, to provide physician services to their enrollees typically under capitated arrangements. Each HMO negotiates a fixed amount per member per month (“PMPM”) that is to be paid to our IPAs. In return, the IPAs arrange for the delivery of healthcare services by contracting with physicians or professional medical corporations for primary care and specialty care services. Our IPAs assume the financial risk of the cost of delivering healthcare services in excess of the fixed amounts received. Some of the risk is transferred to the contracted physicians or professional corporations. The risk is subject to stop-loss provisions in contracts with HMOs.
6
An ACO participates in in one or more payment and delivery models sponsored by Centers for Medicare & Medicaid Services (“CMS”) that provides high-quality and affordable care to Medicare FFS patients. The CMS programs allow provider groups to assume higher levels of financial risk and potentially achieve a higher reward from participation in the respective program’s attribution-based risk-sharing model. For the year ended December 31, 2023, one of the Company’s ACO participated in the ACO REACH Model.
Beginning in 2024, in addition to participating in the ACO REACH Model, our other ACO began participating in the Medicare Shared Savings Program (“MSSP”). The MSSP was created to promote accountability and improve coordination of care for Medicare beneficiaries. The MSSP has multiple risk tracks, and we are currently participating in the ENHANCED risk track. Much like the ACO REACH Model, under the MSSP Model, we recruit a group of Participant and Preferred (in-network) Providers. Based on the Participant Providers that join our ACO, CMS grants us a pool of Traditional Medicare patients (beneficiaries) to manage (the “MSSP Aligned Beneficiaries”). Our MSSP Aligned Beneficiaries will receive services from physicians and other medical service providers that are both in-network and out-of-network. Unlike the ACO REACH Program, CMS continues to pay participant and preferred providers on a FFS basis for Medicare-covered services provided to MSSP Aligned Beneficiaries. However, we continue to bear risk on all Medicare expenditures (both in-network and out-of-network), excluding drug expenditures covered by Medicare Part D, based on a budgetary benchmark established with CMS. Our shared savings or losses in managing our beneficiaries are generally determined on an annual basis after reconciliation with CMS.
With our Restricted Knox-Keene licensed health plan, we can assume full financial responsibility, including both professional and institutional risk, for the medical costs of our members under the plans, which allows our Care Partners to manage a full spectrum of care.
Care Delivery
Our Care Delivery segment is a patient-centric, data-driven care delivery organization focused on delivering high-quality and accessible care to all patients that sees over 800,000 patients annually. As medical care has increasingly been delivered in clinic settings, many integrated health networks also operate healthcare facilities primarily focused on the diagnosis and/or care of outpatients, including those with chronic conditions such as heart disease and diabetes, to cover the primary healthcare needs of local communities. Our Care Delivery organization spans approximately 60 locations across 3 states and includes:
•Primary care clinics, including post-acute care services;
•Multi-specialty care clinics and medical groups, including hospitalist, intensivist, and physician advisory services, cardiac care and diagnostic testing, and specialized care for women’s health; and
•Ancillary service providers, such as urgent care centers, outpatient imaging centers, ambulatory surgery centers, and full-service labs.
We analyze our Care Partners networks by specialty and geography and then build or acquire practices and provider groups to fulfill network gaps in access to ensure patients have high-quality access to care. Our ability to build Care Delivery clinics tailor-made for specific markets helps us scale as we enter de novo into new markets.
Care Enablement
Our Care Enablement segment is an integrated, end-to-end clinical, operational, financial, and administrative platform powered by our proprietary technology suite and underpinned by 35+ years of real-world data, that enhances delivery of high-quality, value-based care to our patients and leading to superior clinical and financial outcomes. Our Care Enablement tools are leveraged across our Care Partners and Care Delivery lines of business as well as 3rd party providers outside of our Astrana ecosystem. Care Enablement provides solutions to providers, including independent physicians, provider and medical groups, ACOs, and payers, including health plans and other risk-bearing organizations. Our platform meets providers and payers where they are, with a wide spectrum of solutions across the total cost of care risk spectrum, ranging from solutions for FFS entities to full risk-bearing entities, and across patient types, including Medicare, Medicaid, Commercial, and Exchange-insured patients. By leveraging our care enablement platform, we believe that providers and payers can improve their ability to deliver high-quality care to their patients and achieve better patient outcomes.
7
Population health management (“PHM”) is a central trend within healthcare delivery, which includes the aggregation of patient data across multiple health information technology resources, the analysis of that data into a single, actionable patient record, and the actions through which care providers can improve both clinical and financial outcomes. PHM seeks to improve health outcomes by monitoring and identifying individual patients, aggregating data, and providing a comprehensive clinical picture of each patient. Using that data, providers can track, and hopefully improve, clinical outcomes while lowering costs. A successful PHM platform requires a robust care and risk management infrastructure, a cohesive delivery system, and a well-managed partnership network.
Our Care Enablement segment includes management service organizations (“MSOs”) that provide non-medical services, under management service agreements (“MSAs”) to IPAs, ACOs, or clinics. Under these arrangements, the MSOs have authority over various non-medical decision-making related to ongoing business operations. These services include but are not limited to:
•Physician recruiting;
•Physician and health plan contracting;
•Care management, including utilization management, medical management, and quality management;
•Provider relations;
•Member services, including annual wellness evaluations;
•Claims processing;
•Pre-negotiating contracts with specialists, labs, imaging centers, nursing homes, and other vendors; and
•Revenue cycle management.
Integrated Health Network
An integrated health network that is able to pool a large number of patients, such as the Company and its affiliated physician groups, is positioned to take advantage of industry trends, meet patient and government demands, and benefit from cost advantages resulting from their scale of operation and integrated approach of care delivery. In addition, an integrated health network with years of managed care experience can leverage their expertise and sizeable medical data to identify specific treatment strategies and interventions, improve the quality of medical care and lower costs. Many integrated health networks, including the Company and its affiliated physician groups, have also established physician performance metrics that allow them to monitor quality and service outcomes achieved by participating physicians in order to reward efficient, high-quality care delivered to members and initiate improvement efforts for physicians whose performance can be enhanced.
Through our ACOs, network of IPAs and Restricted-Knox-Keene licensed health plan with approximately 10,000 contracted healthcare providers, which have agreements with various health plans, hospitals, and other HMOs, we are responsible for coordinating the care of approximately 0.9 million patients, as of December 31, 2023. These patients are comprised of managed care members whose health coverage is provided through their employers, or who have acquired health coverage directly from a health plan or as a result of their eligibility for Medicaid or Medicare benefits. Our managed patients benefit from an integrated approach that places physicians at the center of patient care and utilizes sophisticated risk management techniques and clinical protocols to provide high-quality, cost-effective care. To implement a patient-centered, physician-centric experience, we also have other integrated and synergistic operations, including (i) MSOs that provide management and other services to our affiliated IPAs, (ii) primary care clinics, (iii) multi-specialty care clinics and medical groups, and (iv) ancillary service providers.
Human Capital
As of December 31, 2023, Astrana, its subsidiaries, and consolidated VIEs had approximately 1,800 employees. None of our employees are members of a labor union, and we have not experienced any work stoppage.
8
We are committed to supporting the professional development of our employees, providing competitive compensation and benefits and a safe and inclusive workplace. We measure employee engagement on an ongoing basis to create a more innovative, productive, and profitable company. The results from engagement surveys are used to implement programs and processes designed to support employee retention and satisfaction. The Company believes a diverse workforce fosters innovation and cultivates an environment filled with unique perspectives and growth. Respect for human rights is fundamental to the Company’s business and its commitment to ethical business conduct.
Our dedication to employee growth is reflected in the various learning and development programs offered at Astrana. We organize leadership programs, including a bi-annual summit, the Becoming Leaders program, individual coaching, and ad hoc training sessions, to support our employees in their professional advancement. Our professional development reimbursement program empowers employees to attend classes, seminars, or obtain certifications, enhancing their skill sets and opening up new opportunities for advancement within the Company.
We actively promote and support employees seeking to make a positive impact on their communities and charitable causes through the donation of time, talents, and resources. In 2023, Astrana contributed to several charitable organizations, including the Children's Hospital of Los Angeles, American Heart Association, American Red Cross, and a blanket drive dedicated to supporting residents in our nursing homes.
Organization
We operate through our wholly owned subsidiaries and their consolidated entities, including consolidated VIEs. Our wholly owned subsidiaries are MSOs and ACOs. Our MSOs operate within our Care Enablement segment and are in the business of providing management services. Our ACOs operate within our Care Partners segment and participate in CMS programs. The consolidated IPAs operate within our Care Partners segment and the clinics and ancillary service providers operate within our Care Delivery segment. Our IPAs, clinics and ancillary service businesses are consolidated by the Company as VIEs. We consolidate a VIE if we have both power and benefits – that is, (i) we have the power to direct the activities of a VIE that most significantly influence the VIE’s economic performance, and (ii) we have the obligation to absorb losses of, or the right to receive benefits from, the VIE that could potentially be significant to the VIE.
Some states have laws that prohibit business entities with non-physician owners, such as Astrana and its subsidiaries, from practicing medicine, employing physicians to practice medicine, or exercising control over medical decisions by physicians. These laws are generally referred to as corporate practice of medicine laws. States that have corporate practice of medicine laws permit only physicians to practice medicine, exercise control over medical decisions, or engage in certain arrangements, such as fee-splitting, with physicians.
Due to these laws, we operate by maintaining long-term MSAs with our affiliated IPAs and medical groups, each of which is owned and operated by physicians only, and employs or contracts with additional physicians to provide medical services. Astrana Health Management, Inc. (“AHM”), formerly known as Network Medical Management Inc., is a wholly owned subsidiary of the Company and has entered into MSAs with several affiliated IPAs, including Allied Physicians of California IPA, a Professional Medical Corporation, d.b.a. Allied Pacific of California IPA (“APC”). APC contracts with various HMOs or licensed healthcare service plans, each of which pays a fixed payment (“capitation”). In return, APC arranges for the delivery of healthcare services by contracting with physicians or professional medical corporations for primary care and specialty care services. APC assumes the financial risk of the cost of delivering healthcare services in excess of the fixed amounts received. The risk is subject to stop-loss provisions in contracts with HMOs. Some risk is transferred to the contracted physicians or professional corporations. The physicians in the IPA are exclusively in control of, and responsible for, all aspects of the practice of medicine for enrolled patients. In accordance with relevant accounting guidance, APC has been determined to be a VIE of AHM, as AHM is its primary beneficiary with the ability, through majority representation on the APC Joint Planning Board and otherwise, to direct the activities (excluding clinical decisions) that most significantly affect APC’s economic performance. Therefore, APC and its wholly owned subsidiaries and VIEs are consolidated in the accompanying financial statements.
Due to laws prohibiting a California professional corporation that has more than one shareholder, such as Astrana and APC, from being a shareholder in another California professional corporation, the Company cannot directly own shares in other professional corporations. However, an exception to this regulation permits a professional corporation that has only one shareholder to own shares in another professional corporation. In reliance on this exception, the Company will designate certain key personnel as a nominee shareholder of the professional corporation which holds controlling and non-controlling ownership interests in several medical corporations. Via a Physician Shareholder Agreement with the nominee shareholder, the Company has the ability to designate another person to be the equity holder of each professional corporation. In addition, these entities are managed by our wholly owned MSOs via MSAs. Under the MSAs, we provide and perform non-medical management and
9
administrative services. In accordance with relevant accounting guidance, the professional corporations and their consolidated medical corporations are consolidated by the Company in the accompanying financial statements.
See Note 18 – “Variable Interest Entities (VIEs)” to our consolidated financial statements for information on our entities that qualify as consolidated VIEs.
Investments
We invested in several entities in the healthcare industry. Astrana holds a 30% interest in CAIPA MSO, LLC (“CAIPA MSO”). CAIPA MSO is a New York-based management services organization affiliated with Chinese-American IPA d.b.a. Coalition of Asian-American IPA (“CAIPA”), a leading independent practice association serving the greater New York City area. APC-LSMA, a consolidated VIE of APC, holds a 25% interest in the IPA line of business of LaSalle Medical Associates (“LMA”) and a 40% interest in Pacific Medical Imaging and Oncology Center, Inc. (“PMIOC”). PMIOC provides comprehensive diagnostic imaging services using state-of-the-art technology. PMIOC offers high-quality diagnostic services, such as MRI/MRA, PET/CT, CT, nuclear medicine, ultrasound, digital X-rays, bone densitometry, and digital mammography, at its facilities. These investments are accounted for under the equity method as the Company has the ability to exercise significant influence, but not control over operations.
APC holds 2.8% membership interests of MediPortal LLC, a New York limited liability company, and AHM holds a 10% interest in AchievaMed, Inc., a California corporation. The Company also holds equity securities in Nutex Health Inc. (“Nutex”). As of December 31, 2023, the value of the equity securities was $0.3 million.
The Company entered into a Simple Agreement for Future Equity (“SAFE”) with Third Way Health, Inc. (“Third Way Health”) and Seen Health, Inc. (“Seen Health”). Based on certain triggering events defined in each SAFE agreement, the Company has rights to Third Way Health and Seen Health shares. The number of shares to be acquired will be calculated when the triggering event occurs. As of December 31, 2023, the related investment balance for Third Way Health SAFE and Seen Health SAFE was $3.5 million and $2.0 million, respectively.
Excluded Assets
In September 2019, the Company completed the following series of transactions with its affiliates, Astrana Health Medical Corporation (“Astrana Medical”), formerly known as AP-AMH Medical Corporation, a consolidated VIE of Astrana, and APC, a consolidated VIE of AHM:
1.A $545.0 million loan from the Company to Astrana Medical, pursuant to a 10-year secured loan agreement (the “Astrana Medical Loan”). The loan bears interest at a rate of 10% per annum simple interest, is not prepayable (except in certain limited circumstances), requires quarterly payments of interest only in arrears, and is secured by a first-priority security interest in all of Astrana Medical’s assets. To the extent that Astrana Medical is unable to make any interest payment when due because it has received dividends on the APC Series A Preferred Stock insufficient to pay in full such interest payment, then the outstanding principal amount of the loan will be increased by the amount of any such accrued but unpaid interest, and any such increased principal amounts will bear interest at the rate of 10.75% per annum simple interest.
2.A $545.0 million private placement, where Astrana Medical purchased 1,000,000 shares of APC Series A Preferred Stock which entitles Astrana Medical to receive preferential, cumulative dividends that accrue on a daily basis. During the years ended December 31, 2023 and 2022, APC declared $58.0 million and $58.3 million, respectively, as preferred returns.
3.A $300.0 million private placement, where APC purchased 15,015,015 shares of the Company’s common stock and in connection therewith, the Company granted APC certain registration rights with respect to the purchased shares.
4.Astrana licensed to Astrana Medical the right to use certain tradenames for specified purposes for a fee equal to a percentage of the aggregate gross revenues of Astrana Medical. The license fee is payable out of any Series A Preferred Stock dividends received by Astrana Medical from APC.
5.Through its subsidiary, AHM, the Company agreed to provide certain administrative services to Astrana Medical for a fee equal to a percentage of the aggregate gross revenues of Astrana Medical. The
10
administrative fee is also payable out of any APC Series A Preferred Stock dividends received by Astrana Medical from APC.
As part of the series of transactions, in September 2019, APC and Astrana Medical entered into a Second Amendment to the Series A Preferred Stock Purchase Agreement, clarifying the term excluded assets (“Excluded Assets”). Excluded Assets means (i) assets received from the sale of shares of the Series A Preferred equal to the Series A purchase price, (ii) the assets of APC that are not Healthcare Services Assets (as defined in the purchase agreement), including APC’s equity interests in Astrana Health, Inc., and any entity that is primarily engaged in the business of owning, leasing, developing, or otherwise operating real estate, (iii) any assets acquired with the proceeds of the sale, assignment, or other disposition of any of the assets described in clauses (i) or (ii), and (iv) any proceeds of the assets described in clauses (i), (ii), and (iii).
On December 26, 2023, APC completed a restructuring transaction to spin-off its real estate business and investments, a component of Excluded Assets (“the Spin-Off”). To effect the restructuring, APC contributed its real estate investments to a wholly owned subsidiary in exchange for 100% of the subsidiary’s membership interest units, which membership interests were then distributed to holders of APC’s outstanding common stock as a dividend, with each such stockholder receiving one membership interest unit for each share of outstanding APC common stock held. As a result of the distribution, the real estate investments are no longer included within our consolidated financial statements after December 26, 2023.
As of December 31, 2023, APC also held a 13.22% ownership interest in Astrana. APC’s ownership interest in Astrana is eliminated upon consolidation.
Our Industry
Industry Overview
U.S. healthcare spending has increased steadily over the past two decades. CMS estimates that total U.S. healthcare expenditures are expected to grow at an average annual rate of 5.4% from 2022 to 2031 and will reach $7.2 trillion by 2031. Health spending is projected to grow 0.8% faster than the U.S. gross domestic product per year on average over 2022-2031, and as a result, the healthcare share of gross domestic product is expected to grow from 18.3% in 2021 to 19.6% in 2031. Medicare spending increased by 5.9% to $944.3 billion and Medicaid spending increased by 9.6% to $805.7 billion in 2022, which accounted for 21% and 18% of total health expenditures, respectively. Private health insurance spending increased by 5.9% to $1.3 trillion in 2022, accounting for 29% of total health expenditures. Medicare spending is expected to have the fastest growth (7.5% per year for 2022-2031) primarily due to the projected enrollment growth.
Managed care health plans were developed in the U.S., primarily during the 1980s, in an attempt to mitigate the rising cost of providing healthcare to populations covered by health insurance. These managed care health plans enroll members through their employers in connection with federal Medicare benefits or state Medicaid programs. As a result of the prevalence of these health plans, many seniors now becoming eligible for Medicare have been interacting with managed care companies through their employers for the last 30 years. Individuals now turning 65 are likely more familiar with the managed care setting than previous Medicare populations. The healthcare industry, however, is highly regulated by various government agencies and heavily relies on reimbursement and payments from government-sponsored programs such as Medicare and Medicaid. Companies in the healthcare industry, therefore, have to organize, operate around, and face challenges from idiosyncratic laws and regulations.
Many health plans recognize both the opportunity for growth from adding members, as well as the potential risks and costs associated with managing additional members. In California, many health plans subcontract a significant portion of the responsibility for managing patient care to an integrated health network such as Astrana and our affiliated physician groups. These integrated healthcare systems offer a comprehensive medical delivery system, sophisticated care management know-how, and infrastructure to more efficiently provide for the healthcare needs of the population enrolled with that health plan. While reimbursement models for these arrangements vary around the U.S., health plans often prospectively pay the integrated healthcare system a fixed capitation payment, which is frequently based on a percentage of the amount received by the health plan. Capitation payments to integrated healthcare systems, in the aggregate, represent a prospective budget from which the system manages care-related expenses on behalf of the population enrolled with that system. To the extent that these systems manage such expenses under the capitated levels, the system realizes an operating profit. On the other hand, if the expenses exceed projected levels, the system will realize an operating deficit. Since premiums paid represent a substantial amount per person, there is a significant revenue opportunity for an integrated health network that is able to effectively manage healthcare costs for the capitated arrangements entered into by its affiliated physician groups.
11
Industry Trends and Demand Drivers
We believe that the healthcare industry is undergoing a significant transformation and the demand for our offerings is driven by the confluence of a number of fundamental healthcare industry trends, including:
Shift to Value-Based and Results-Oriented Models. According to the 2022 National Health Expenditure Historical Data prepared by CMS, healthcare spending in the U.S. increased by 4.1% to $4.5 trillion in 2022, representing 17.3% of the U.S. Gross Domestic Product. CMS projects healthcare spending in the U.S. to increase at an average rate of 5.4% for 2022-2031 and to reach approximately $7.2 trillion by 2031. To address this expected significant rise in healthcare costs, the U.S. healthcare market is seeking more efficient and effective methods of delivering care. The FFS reimbursement model has arguably played a major role in increasing the level and growth rate of healthcare spending. In response, both the public and private sectors are shifting away from the FFS reimbursement model toward value-based, capitated payment models that are designed to incentivize value and quality at an individual patient level. The number of Americans covered by capitated payment programs continues to increase, which drives more coordinated and outcomes-based patient care.
Increasingly Patient-Centered. More patients are becoming actively involved and taking an informed role in how their own healthcare is delivered, resulting in the healthcare marketplace becoming increasingly patient-centered, and thus requiring providers to deliver team-based, coordinated, and accessible care to stay competitive.
Added Complexity. In the healthcare space, more sophisticated technology has been employed, new diagnostics and treatments have been introduced, research and development have expanded, and regulations have multiplied. This expanding complexity drives a growing and continuous need for integrated care delivery systems.
Integration of Healthcare Information. Across the healthcare landscape, a significant amount of data is being created every day, driven by patient care, payment systems, regulatory compliance, and record keeping. As the amount of healthcare data continues to grow, it becomes increasingly important to connect disparate data and apply insights in a targeted manner in order to better achieve the goals of higher quality and more efficient care.
Our Revenue Streams
Our revenue reflected in the accompanying consolidated financial statements includes revenue generated by our subsidiaries and consolidated entities. Our revenue streams are diversified among our various operations and multi-year renewable contractual arrangements as follows:
•Capitation revenue;
•Risk pool settlements and incentives;
•ACO REACH capitation revenue;
•Management fee income; and
•FFS revenue.
Capitation Revenue
Our capitation revenue consists primarily of capitated fees for medical services we provide under capitated arrangements made directly with various managed care providers, including HMOs. Under the capitated model, an HMO pays the IPA a capitation payment and assigns it the responsibility for providing physician services required by patients. The IPA physicians are exclusively in control of, and responsible for, all aspects of the practice of medicine for enrolled patients. Capitation revenue for our Restricted Knox-Keene licensed health plan consists of “global” capitation arrangements whereby the Restricted Knox-Keene licensed health plan accepts financial risk for hospital and other institutional services in addition to professional medical services (whereas IPA capitation contracts are typically limited to accepting financial risk for professional medical services). Most of the HMO agreements have an initial term of two years, renewing automatically for successive one-year terms. The HMO agreements generally allow either party to terminate the HMO agreements without cause, typically with a four to six months advance notice and provide for a termination for cause by the HMO at any time.
Capitation revenue is typically prepaid monthly to us based on the number of enrollees selecting us as their healthcare provider. Capitation is a fixed payment amount per patient per unit of time paid in advance for the delivery of healthcare
12
services, whereby the service providers are generally liable for excess medical costs. The actual amount paid is determined by the ranges of services provided, the number of patients enrolled, and the period of time during which the services are provided. Capitation rates are generally based on local costs and average utilization of services. Because Medicare pays capitation using a “Risk Adjustment” model, which compensates managed care providers based on the health status (acuity) of each individual enrollee, managed care providers with higher acuity enrollees receive more, and those with lower acuity enrollees receive less, capitation that can be allocated to service providers. Under the Risk Adjustment model, capitation is paid on an interim basis based on enrollee data submitted for the preceding year and is adjusted in subsequent periods after the final data is compiled.
PMPM managed care contracts generally have a term of one year or longer. All managed care contracts have a single performance obligation that constitutes a series for the provision of managed healthcare services for a population of enrolled members for the duration of the contract. The transaction price for PMPM contracts is variable, as it primarily includes PMPM fees associated with unspecified membership that fluctuates throughout the term of the contract. In certain contracts, PMPM fees also include adjustments for items such as performance incentives, performance guarantees, and risk shares.
Risk Pool Settlements and Incentives
Capitation arrangements are supplemented by risk-sharing arrangements. Our affiliated IPAs have two different types of capitation risk-sharing arrangements: hospital shared-risk and health plan shared-risk arrangements.
Our affiliated IPAs may enter into hospital shared-risk capitation arrangements with certain health plans and local hospitals, where the hospital is responsible for providing, arranging, and paying for institutional risk, and the IPA is responsible for providing, arranging, and paying for professional risk. Under a hospital shared-risk pool-sharing agreement, we generally receive a percentage of the net surplus from the affiliated hospital’s risk pools with HMOs after deductions for the affiliated hospital’s costs, whereas deficits, if any, are not payable until and unless (and only to the extent) risk-sharing surpluses are generated. At the termination of the hospital shared-risk pool-sharing agreement, any accumulated deficit will be extinguished. Advance settlement payments are typically made quarterly in arrears if there is a surplus. Risk pool settlements under arrangements with health plans and hospitals are recognized using the most likely amount methodology and amounts are only included in revenue to the extent that it is probable that a significant reversal of cumulative revenue will not occur once any uncertainty is resolved. Assumptions for medical loss ratios (“MLR”), incurred but not reported (“IBNR”) completion factors and constraint percentages were used by management in applying the most likely amount methodology.
Under capitation arrangements with certain HMOs, our affiliated IPAs may participate in one or more health plan shared-risk arrangements relating to the provision of institutional services to enrollees (health plan shared-risk arrangements) and thus can earn additional revenue or incur losses based upon the enrollee utilization of institutional services. Health plan shared-risk capitation arrangements are entered into with certain health plans, which are administered by the health plan, where we are responsible for rendering professional services, but the health plan does not enter into a capitation arrangement with a hospital and therefore, the health plan retains the institutional risk. Health plan shared-risk deficits, if any, are not payable until and unless (and only to the extent of any) risk-sharing surpluses are generated. At the termination of the HMO contract, any accumulated deficit will be extinguished.
In addition to risk-sharing revenues, we also receive incentives under “pay-for-performance” programs for quality medical care, based on various criteria. As an incentive to promote quality care, certain HMOs have designed quality incentive programs and commercial generic pharmacy incentive programs to compensate us for our efforts to improve the quality of services and to promote the efficient and effective use of pharmacy supplemental benefits provided to HMO members. The incentive programs track specific performance measures and calculate payments to us based on the performance measures. Generally, for the foregoing arrangements, the final settlement is dependent on each distinct day’s performance within the annual measurement period, but cannot be determined until the full measurement period has occurred and performance can be assessed.
ACO REACH Capitation Revenue
Through one of our ACOs, we participate in the Global Risk track with Total Care Capitation (“TCC”) in the Accountable Care Organization Realizing Equity, Access, and Community Health (“ACO REACH”) Model sponsored by CMS. Under the ACO REACH Model, we recruit a group of Participant and Preferred (in-network) Providers. Based on the Participant Providers that join our ACO, CMS grants us a pool of Traditional Medicare patients (beneficiaries) to manage (the “Aligned Beneficiaries”). Our Aligned Beneficiaries will receive services from physicians and other medical service providers that are both in-network and out-of-network. Under TCC, CMS estimates an average of in-network monthly expenditures for our ACO’s Aligned Beneficiaries and pays that projected amount to us in monthly installments. We are then responsible for paying our in-network providers for all Medicare-covered services provided to our Aligned Beneficiaries by those providers. In
13
addition, we bear risk on all Medicare expenditures (both in-network and out-of-network), excluding drug expenditures covered by Medicare Part D, based on a budgetary benchmark established with CMS. Claims from out-of-network providers are processed and paid by CMS. Our shared savings or losses in managing our beneficiaries are generally determined on an annual basis after reconciliation with CMS. Pursuant to our risk-share agreement with CMS, we are eligible to receive the surplus (shared savings) or are liable for the deficit (shared losses) according to the budgetary benchmark established by CMS based on our efficiency, or lack thereof, in managing the expenditures associated with our Aligned Beneficiaries. Using the most recent data from CMS, the Company estimates the potential savings or deficit for the performance year. We also recognize the budgetary benchmark established by CMS, net of any ACO REACH program discounts and adjustments, as revenue. Our maximum shared savings or losses are determined by the risk track we elect with CMS. Under the Global Risk track, we are responsible for 100% of shared savings or losses up to 25% of the total budgetary benchmark established by CMS, with adjusted risk corridors taking effect for any proportion of shared savings / losses exceeding 25% of the benchmark—for savings/losses of 25-35% of the benchmark, we assume 50% risk responsibility, for savings/losses 35%-50% of the benchmark we assume 25% of the risk responsibility, and for savings/losses exceeding 50% of the benchmark, we assume only 10% of the risk responsibility.
Management Fee Income
Management fee income encompasses fees paid for management, physician advisory, healthcare staffing, administrative, and other non-medical services provided by us to IPAs, hospitals, and other healthcare providers. Our MSOs enter into management service agreements with terms generally ranging from one to ten years, although they may be terminated earlier under the terms of the applicable contracts. Management fees may be in the form of billings at agreed-upon hourly rates, percentages of revenue, or fee collections, or amounts fixed on a monthly, quarterly, or annual basis. The revenue may include variable arrangements measuring factors such as hours staffed, patient visits, or collections per visit against benchmarks, and, in certain cases, may be subject to achieving quality metrics or fee collections.
Fee For Service (“FFS”) Revenue
FFS revenue represents revenue earned under contracts in which we bill and collect the professional component of charges for medical services rendered by our contracted physicians and employed physicians. Under the FFS arrangements, we bill, and receive payments from, the hospitals and third-party payers for physician staffing and further bill patients or their third-party payers for patient care services provided.
Our Key Payers
A limited number of payers represent a significant portion of our net revenue. For the years ended December 31, 2023, 2022 and 2021, four payers accounted for an aggregate of 61.7%, 59.0%, and 49.6% of our total net revenue, respectively.
Our Strengths and Advantages
The following are some of the material opportunities that we believe exist for our company:
Combination of Clinical, Administrative and Technology Capabilities
We believe our key strength lies in our combined clinical, administrative, and technology capabilities. While many companies separately provide clinical, MSO, or technology support services, to our knowledge, there are currently very few organizations like ours that provide all three types of services to approximately 0.9 million patients as of December 31, 2023.
Diversification
Through our subsidiaries, consolidated affiliates, and invested entities, we have been able to reduce our business risk and increase revenue opportunities by diversifying our service offerings and expanding our ability to manage patient care across a horizontally integrated care network. Our revenue is spread across our operations. Additionally, with our ability to monitor and manage care within our wide network, we believe we are an attractive business partner to health plans, hospitals, IPAs, and other medical groups seeking to provide better care at lower costs.
14
Strong Management Team
Our management team has, collectively, several decades of experience managing physician practices, risk-based organizations, health plans, hospitals, and health systems, a deep understanding of the healthcare marketplace and emerging trends, and a vision for the future of healthcare delivery led by physician-driven healthcare networks.
A Robust Physician Network
As of December 31, 2023, our physician network consisted of approximately 10,000 contracted physicians, including primary care physicians, specialist physicians, and hospitalists, through our affiliated physician groups and ACOs.
Cultural Affinities with Patients
In addition to delivering premium healthcare, we believe in the importance of providing services that are sensitive to the needs of local communities, including their cultural affinities. This value is shared by physicians within our affiliated IPAs and medical groups, and promotes patient comfort in communicating with care providers.
Long-Standing Relationships with Partners
We have developed long-standing relationships with multiple health plans, hospitals, IPAs, and other medical groups that have helped to generate recurring contractual revenue for us.
Comprehensive and Effective Healthcare Management Programs
We offer comprehensive and effective healthcare management programs to patients. We have developed expertise in population health management and care coordination, and in proper medical coding, which results in improved Risk Adjustment Factor (“RAF”) scores and higher payments from health plans, and in improved quality metrics in both inpatient and outpatient settings and thus patient satisfaction and CMS scores. Using our own proprietary risk assessment scoring tool, we have also developed our own protocol for identifying high-risk patients.
Competition
The healthcare industry is highly competitive and fragmented. We compete for customers across all of our services with other healthcare management companies, including MSOs and healthcare providers, such as local, regional, and national networks of physicians, medical groups, and hospitals, many of which are substantially larger than us and have significantly greater financial and other resources, including personnel, than we have.
IPAs
Our affiliated IPAs compete with other IPAs, medical groups, and hospitals, many of which have greater financial, personnel, and other resources available to them. In the greater Los Angeles area, such competitors include Regal Medical Group and Lakeside Medical Group, which are part of Heritage Provider Network (“Heritage”), as well as Optum (f/k/a HealthCare Partners), a subsidiary of UnitedHealth Group.
ACOs
Our ACOs competes with other sophisticated provider groups in the creation, administration, and management of ACOs, many of which have greater financial, personnel, and other resources available to them. Major competitors of APAACO include Privia Health and Aledade.
Outpatient Clinics
Our outpatient clinics compete with large ambulatory surgery centers and/or diagnostic centers such as RadNet and Envision Healthcare, many of which have greater financial, personnel, and other resources available to them, as well as smaller
15
clinics that have ties to local communities. Optum (f/k/a HealthCare Partners) also has its own urgent care centers, clinics, and diagnostic centers.
MSOs
Our MSOs compete with other MSOs in providing management, administrative and other support services. Such competitors include Prospect Medical Systems and Conifer Health Solutions.
Regulatory Matters
As a healthcare company, our operations and relationships with healthcare providers, such as hospitals, other healthcare facilities, and healthcare professionals, are subject to extensive and increasing regulation by numerous federal, state, and local government agencies, including the Office of Inspector General, the Department of Justice, CMS, and various state authorities. These laws and regulations often are interpreted broadly and enforced aggressively. Imposition of liabilities associated with a violation of any of these healthcare laws and regulations could have a material adverse effect on our business, financial condition, or results of operations. We cannot guarantee that our practices will not be subject to government scrutiny or be found to violate certain healthcare laws. Government investigations and prosecutions, even if we are ultimately found to be without fault, can be costly and disruptive to our business. Moreover, changes in healthcare legislation or government regulation may restrict our existing operations, limit our expansion, or impose additional compliance requirements and costs, any of which could have a material adverse effect on our business, financial condition, or results of operations. Below are brief descriptions of some, but not all, of such laws and regulations that affect our business operations. There are many other laws and regulations that impact us; for instance, California has enacted new laws requiring additional disclosure with respect to certain climate-related risks and greenhouse gas emissions reduction claims. Non-compliance with these new laws may result in the imposition of substantial fines or penalties.
Corporate Practice of Medicine
Our consolidated financial statements include our subsidiaries and VIEs. Some states have laws that prohibit business entities with non-physician owners, such as Astrana and its subsidiaries, from practicing medicine, employing physicians to practice medicine, or exercising control over medical decisions by physicians. These laws are generally referred to as corporate practice of medicine laws. States that have corporate practice of medicine laws permit only physicians to practice medicine, exercise control over medical decisions, or engage in certain arrangements, such as fee-splitting, with physicians. In these states, a violation of the corporate practice of medicine prohibition constitutes the unlawful practice of medicine, which is a public offense punishable by fines and other criminal penalties. In addition, any physician who participates in a scheme that violates the state’s corporate practice of medicine prohibition may be punished for aiding and abetting a lay entity in the unlawful practice of medicine.
California, Nevada and Texas are corporate practice of medicine states, and we operate by maintaining long-term MSAs with our affiliated IPAs and medical groups, each of which is owned and operated by physicians only, and employs or contracts with additional physicians to provide medical services. Under such MSAs, our wholly owned MSOs are contracted to provide non-medical management and administrative services, such as financial and risk management, as well as information systems, marketing, and administrative support to the IPAs and medical groups. The MSAs typically have an initial term of one to thirty years and are generally not terminable by our affiliated IPAs and medical groups except in the case of bankruptcy, gross negligence, fraud, or other illegal acts by the contracting MSO.
Through the MSAs and the relationship with the physician owners of our medical affiliates, we have exclusive authority over all non-medical decisions related to the ongoing business operations of those affiliates. Consequently, Astrana consolidates the revenue and expenses of such affiliates as their primary beneficiary from the date of execution of the applicable MSA. When necessary, our Vice Chairman of the Board, Dr. Thomas Lam, or a locally-licensed physician (where State laws require a physician licensed in that State) serves as nominee shareholder of affiliated medical practices on Astrana’s behalf, in order to comply with corporate practice of medicine laws and certain accounting rules applicable to consolidated financial reporting by our affiliates as VIEs. In Texas, a nonprofit health organization meeting certain criteria and approved by the Texas Medical Board is an alternative structure for compliance with corporate practice of medicine laws.
Under these arrangements, our MSOs perform only non-medical functions, do not represent to offer medical services, and do not exercise influence or control over the practice of medicine by physicians. The California Medical Board, as well as other states’ regulatory bodies, has taken the position that MSAs that confer too much control over a physician practice to MSOs may violate the prohibition against corporate practice of medicine. Some of the relevant laws, regulations, and agency interpretations in California and other states that have corporate practice prohibitions have been subject to limited judicial and
16
regulatory interpretation. Moreover, state laws and regulatory interpretations are subject to change. Other parties, including our affiliated physicians, may assert that, despite these arrangements, Astrana and its subsidiaries are engaged in the prohibited corporate practice of medicine or that such arrangements constitute unlawful fee-splitting between physicians and non-physicians. If this occurred, we could be subject to civil or criminal penalties, our MSAs could be found legally invalid and unenforceable in whole or in part, and we could be required to restructure arrangements with our affiliated IPAs and medical groups. If we were required to change our operating structures due to determination that a corporate practice of medicine violation existed, such a restructuring might require revising our MSOs’ management fees.
False Claims Acts
The False Claims Act imposes civil liability on individuals or entities that submit false or fraudulent claims for payment to the federal government. The False Claims Act provides, in part, that the federal government may bring a lawsuit against any person whom it believes has knowingly or recklessly presented, or caused to be presented, a false or fraudulent request for payment from the federal government, or who has made a false statement or used a false record to get a claim for payment approved. Private parties may initiate qui tam whistleblower lawsuits against any person or entity under the False Claims Act in the name of the federal government and may share in the proceeds of a successful suit. The federal government has used the False Claims Act to prosecute a wide variety of alleged false claims and fraud allegedly perpetrated against Medicare and state healthcare programs. By way of illustration, these prosecutions may be based upon alleged coding errors, billing for services not rendered, billing services at a higher payment rate than appropriate, and billing for care that is not considered medically necessary. The federal government and a number of courts have taken the position that claims presented in violation of certain other statutes, including the federal Anti-Kickback Statute or the Stark Law, can also be considered a violation of the False Claims Act based on the theory that a provider impliedly certifies compliance with all applicable laws, regulations, and other rules when submitting claims for reimbursement.
Penalties for False Claims Act violations include substantial fines for each false claim, plus up to three times the amount of damages sustained by the government. A False Claims Act violation may provide the basis for the imposition of administrative penalties as well as exclusion from participation in governmental healthcare programs, including Medicare and Medicaid. In addition to the provisions of the False Claims Act, which provide for civil enforcement, the federal government can also use several criminal statutes to prosecute persons who are alleged to have submitted false or fraudulent claims to the government for payments.
A number of states, including California, have enacted laws that are similar to the federal False Claims Act. Under Section 6031 of the Deficit Reduction Act of 2005 (“DRA”), as amended, if a state enacts a false claims act that is at least as stringent as the federal statute and that also meets certain other requirements, the state will be eligible to receive a greater share of any monetary recovery obtained pursuant to certain actions brought under the state’s false claims act. As a result, a number of states have adopted, and more states are expected to enact laws that are similar to the federal False Claims Act, along with an expected corresponding increase in state false claims enforcement efforts. In addition, Section 6032 of the DRA requires entities that make or receive annual Medicaid payments of $5.0 million or more from any one state to provide their employees, contractors, and agents with written policies and employee handbook materials on federal and state false claims acts and related statues.
Anti-Kickback Statutes
The federal Anti-Kickback Statute is a provision of the Social Security Act of 1972 that prohibits as a felony offense the knowing and willful offer, payment, solicitation or receipt of any form of remuneration in return for, or to induce, (1) the referral of a patient for items or services for which payment may be made in whole or part under Medicare, Medicaid, or other federal healthcare programs, (2) the furnishing or arranging for the furnishing of items or services reimbursable under Medicare, Medicaid, or other federal healthcare programs or (3) the purchase, lease, or order or arranging or recommending the purchasing, leasing, or ordering of any item or service reimbursable under Medicare, Medicaid, or other federal healthcare programs. The Patient Protection and Affordable Care Act (“ACA”) amended section 1128B of the Social Security Act to make it clear that a person need not have actual knowledge of the statute, or specific intent to violate the statute, as a predicate for a violation. The Office of Inspector General (“OIG”), which has the authority to impose administrative sanctions for violation of the statute, has adopted as its standard for review a judicial interpretation, which concludes that the statute prohibits any arrangement where even one purpose of the remuneration is to induce or reward referrals. A violation of the Anti-Kickback Statute is a felony punishable by imprisonment, criminal fines, civil fines, and three times the amount of the unlawful remuneration. A violation also can result in exclusion from Medicare, Medicaid, or other federal healthcare programs. In addition, pursuant to the changes of the ACA, a claim that includes items or services resulting from a violation of the Anti-Kickback Statute is a false claim for purposes of the False Claims Act.
17
Due to the breadth of the Anti-Kickback Statute’s broad prohibitions, statutory exceptions exist that protect certain arrangements from prosecution. In addition, the OIG has published safe harbor regulations that specify arrangements that are deemed protected from prosecution under the Anti-Kickback Statute, provided all applicable criteria are met. The failure of an activity to meet all of the applicable safe harbor criteria does not necessarily mean that the particular arrangement violates the Anti-Kickback Statute, but these arrangements may be subject to scrutiny and prosecution by enforcement agencies. We may be less willing than some competitors to take action or enter into arrangements that do not clearly satisfy the OIG safe harbors and suffer a competitive disadvantage.
On December 2, 2020, in conjunction with the U.S. Department of Health and Human Services’ (“HHS”) Regulatory Sprint to Coordinated Care, the OIG finalized modifications to existing safe harbors to the Anti-Kickback Statute and added new safe harbors and a new exception to the civil monetary penalty provision prohibiting inducements to beneficiaries, the purpose of which was to remove potential barriers to more effective coordination and management of patient care and delivery of value-based care. The changes implemented by the final rules went into effect on January 19, 2021. These or other changes implemented by OIG in the future may impact our business, results of operations and financial condition.
Some states have enacted statutes and regulations similar to the Anti-Kickback Statute, but which may be applicable regardless of the payer source for the patient. These state laws may contain exceptions and safe harbors that are different from and/or more limited than those of the federal law and that may vary from state to state. For example, California has adopted the Physician Ownership and Referral Act of 1993 (“PORA”). PORA makes it unlawful for physicians, surgeons, and other licensed professionals to refer a person for certain healthcare services if they have a financial interest with the person or entity that receives the referral. While PORA also provides certain exemptions from this prohibition, failure to fit within an exemption in violation of PORA can lead to a misdemeanor offense that may subject a physician to civil penalties and disciplinary action by the Medical Board of California.
For example, Section 445 of the California Health and Safety Code provides that “no person, firm, partnership, association or corporation, or agent or employee thereof, shall for profit refer or recommend a person to a physician, hospital, health-related facility, or dispensary for any form of medical care or treatment of any ailment or physical condition. The imposition of a fee or charge of any such referral or recommendation creates a presumption that the referral or recommendation is for profit.” A violation of Section 445 is a misdemeanor and may subject the offender to imprisonment and/or monetary fines. Further, a violation of Section 445 may be enjoined by the California Attorney General. Section 650 of the California Business and Professions Code contains prohibitions against self-referral and kickbacks. Business & Professions Code Section 650 makes it unlawful for a “licensee,” including a physician, to pay or receive any compensation or inducement for referring patients, clients, or customers to any person or entity, irrespective of any membership or proprietary interest in or with the person or entity receiving the referral. Violation of the statute is a public offense punishable by imprisonment and/or monetary fines. Section 650 further provides that it is not unlawful for a physician to refer a patient to a healthcare facility solely because the physician has a proprietary interest or co-ownership in a healthcare facility, provided that (1) the physician’s return on investment for that proprietary interest or co-ownership is based upon the amount of capital investment or proportional ownership of the physician; and (2) the ownership interest is not based on the number or value of any patients referred. A violation of Section 650 is a misdemeanor and may subject the offender to imprisonment and/or monetary fines.
We cannot assure that the applicable regulatory authorities will not determine that some of our arrangements with physicians violate the federal Anti-Kickback Statute or other applicable laws. An adverse determination could subject us to different liabilities, including criminal penalties, civil monetary penalties, and exclusion from participation in Medicare, Medicaid, or other healthcare programs, any of which could have a material adverse effect on our business, financial condition, or results of operations.
Antitrust Laws
The federal government and most states have enacted antitrust laws that prohibit certain types of conduct deemed to be anti-competitive. These laws prohibit price fixing, market allocation, concerted refusal to deal, market monopolization, price discrimination, tying arrangements, acquisitions of competitors and other practices that have, or may have, an adverse effect on competition. Violations of federal or state antitrust laws can result in various sanctions, including criminal and civil penalties. Antitrust enforcement in the health care industry is currently a priority of the Federal Trade Commission and the U.S. Department of Justice. A review or action by regulatory authorities or the courts that is negative in nature as to the relationship between us and the physician groups or IPAs that we manage or contract with, could force us to terminate those contractual relationships. We believe we are in compliance with such federal and state laws, but courts or regulatory authorities may reach a determination in the future that could adversely affect our operations.
18
Stark Laws
The federal Stark Law, also known as the physician self-referral law, generally prohibits a physician from referring Medicare and Medicaid patients to an entity (including hospitals) providing “designated health services” if the physician or a member of the physician’s immediate family has a “financial relationship” with the entity, unless a specific exception applies. Designated health services include, among other services, inpatient hospital services, outpatient prescription drug services, clinical laboratory services, certain imaging services (e.g., MRI, CT, ultrasound), and other services that our affiliated physicians may order for their patients. The prohibition applies regardless of the reasons for the financial relationship and the referral, and therefore, unlike the federal Anti-Kickback Statute, intent to violate the law is not required. Like the Anti-Kickback Statute, the Stark Law contains statutory and regulatory exceptions intended to protect certain types of transactions and arrangements. Unlike safe harbors under the Anti-Kickback Statute, with which compliance is voluntary, an arrangement must comply with every requirement of a Stark Law exception or the arrangement is in violation of the Stark Law.
Because the Stark Law and implementing regulations continue to evolve and are detailed and complex, while we attempt to structure our relationships to meet an exception to the Stark Law, there can be no assurance that the arrangements entered into by us with affiliated physicians and facilities will be found to be in compliance with the Stark Law, as it ultimately may be implemented or interpreted. The penalties for violating the Stark Law can include the denial of payment for services ordered in violation of the statute, mandatory refunds of any sums paid for such services, and civil penalties for each violation, double damages, and possible exclusion from future participation in the governmental healthcare programs. A person who engages in a scheme to circumvent the Stark Law’s prohibitions may face substantial fines for each applicable arrangement or scheme.
On December 2, 2020, in conjunction with HHS’s Regulatory Sprint to Coordinated Care, CMS issued a final rule intended to address the regulatory impact and burden of the Stark Law that impeded the healthcare system’s move toward value-based reimbursement. CMS added new exceptions to attempt to address potential barriers to coordinated care and value-based care. The changes implemented by the final rules went into effect on January 19, 2021. These or other changes implemented by CMS in the future may impact our business, results of operations, and financial condition.
Some states have enacted statutes and regulations against self-referral arrangements similar to the federal Stark Law, but which may be applicable to the referral of patients regardless of their payer source and which may apply to different types of services. These state laws may contain statutory and regulatory exceptions that are different from those of the federal law and that may vary from state to state. For example, California has adopted PORA, which makes it unlawful for physicians, surgeons, and other licensed professionals to refer a person for certain healthcare services if they have a financial interest with the person or entity that receives the referral. While PORA also provides certain exemptions from this prohibition, failure to fit within an exemption in violation of PORA can lead to a misdemeanor offense that may subject a physician to civil penalties and disciplinary action by the Medical Board of California.
An adverse determination under these state laws and/or the federal Stark Law could subject us to different liabilities, including criminal penalties, civil monetary penalties, and exclusion from participation in Medicare, Medicaid, or other healthcare programs, any of which could have a material adverse effect on our business, financial condition, or results of operations.
Health Information Privacy and Security Standards
The privacy regulations promulgated under the Health Insurance Portability and Accountability Act of 1996 (“HIPAA”), as amended, contain detailed requirements concerning the use and disclosure of individually identifiable patient health information (“PHI”) by entities like our MSOs and affiliated IPAs and medical groups. HIPAA-covered entities must implement certain administrative, physical, and technical security standards to protect the integrity, confidentiality, and availability of certain electronic health information received, maintained, or transmitted. HIPAA also implemented standard transaction code sets and standard identifiers that covered entities must use when submitting or receiving certain electronic healthcare transactions, including billing and claim collection activities. New health information standards could have a significant effect on the manner in which we do business, and the cost of complying with new standards could be significant.
Violations of the HIPAA privacy and security rules may result in civil and criminal penalties, including a tiered system of civil money penalties. A HIPAA-covered entity must also promptly notify affected individuals where a breach affects more than 500 individuals and report annually any breaches affecting fewer than 500 individuals.
State attorneys general may bring civil actions on behalf of state residents for violations of the HIPAA privacy and security rules, obtain damages on behalf of state residents, and enjoin further violations. Many states also have laws that protect
19
the privacy and security of confidential, personal information, which may be similar to or even more stringent than HIPAA. Where applicable state laws are more protective than HIPAA, we are required to comply with the stricter provisions. Some of these state laws may impose fines and penalties on violators and may afford private rights of action to individuals who believe their personal information has been misused. California’s patient privacy laws, for example, provide for monetary penalties and permit injured parties to sue for damages. Both state and federal laws are subject to modification or enhancement of privacy protection at any time.
If we fail to comply with HIPAA or similar state laws, we could incur substantial civil monetary or criminal penalties. We expect increased federal and state privacy and security enforcement efforts.
Knox-Keene Act and State Insurance Laws
The Knox-Keene Health Care Service Plan Act of 1975, as amended (the “Knox-Keene Act”), is the California law that regulates managed care plans. Neither our MSOs nor their managed medical groups and IPAs hold a Knox-Keene license. Some of the medical groups and IPAs that have entered into MSAs with our MSOs have historically contracted with health plans and other payers to receive capitation payments and assumed the financial responsibility for professional services. In many of these cases, the health plans or other payers separately enter into contracts with hospitals that receive payments and assume some type of contractual financial responsibility for their institutional services. In some instances, our affiliated medical groups and IPAs have been paid by their contracting payers or hospitals for the financial outcome of managing the care costs associated with both the professional and institutional services received by patients, and have recognized a percentage of the surplus of institutional revenues less institutional expense as the medical groups’ and IPAs’ net revenues; and, under certain circumstances, may be responsible for a percentage of any shortfall in the event that institutional expenses exceed institutional revenues. While our MSOs and their managed medical groups and IPAs are not contractually obligated to pay claims to hospitals or other institutions under these arrangements, if it is determined that our MSOs or the medical groups and IPAs have been inappropriately taking financial risk for institutional and professional services without a Knox-Keene license or regulatory exemption as a result of their hospital and physician arrangements, we may be required to obtain a restricted Knox-Keene license to resolve such violations and we could be subject to civil and criminal liability, any of which could have a material adverse effect on our business, financial condition, or results of operations.
In addition, some states require ACOs to be registered or otherwise comply with state insurance laws. Our ACOs are not registered with any state insurance agency. If it is determined that we have been inappropriately operating an ACO without state registration or licensure, we may be required to obtain such registration or licensure to resolve such violations and we could be subject to liability, which could have a material adverse effect on our business, financial condition, or results of operations.
Environmental and Occupational Safety and Health Administration Regulations
We are subject to federal, state, and local regulations governing the storage, use, and disposal of waste materials and products. Although we believe that our safety procedures for storing, handling, and disposing of these materials and products comply with the standards prescribed by law and regulation, we cannot eliminate the risk of accidental contamination or injury from those hazardous materials. In the event of an accident, we could be held liable for any damages that result and any liability could exceed the limits or fall outside the coverage of our insurance policies, which we may not be able to maintain on acceptable terms, or at all. We could incur significant costs and the attention of our management could be diverted to comply with current or future environmental laws and regulations. Federal regulations promulgated by the Occupational Safety and Health Administration impose additional requirements on us, including those protecting employees from exposure to elements such as blood-borne pathogens. We cannot predict the frequency of compliance, monitoring, or enforcement actions to which we may be subject as those regulations are being implemented, which could adversely affect our operations.
Other Federal and State Healthcare Laws
We are also subject to other federal and state healthcare laws that could have a material adverse effect on our business, financial condition, or results of operations. The Health Care Fraud Statute prohibits any person from knowingly and willfully executing, or attempting to execute, a scheme to defraud any healthcare benefit program, which can be either a government or private payer plan. Violation of this statute, even in the absence of actual knowledge of or specific intent to violate the statute, may be charged as a felony offense and may result in fines, imprisonment, or both. The Health Care False Statement Statute prohibits, in any matter involving a federal healthcare program, anyone from knowingly and willfully falsifying, concealing, or covering up, by any trick, scheme, or device, a material fact, or making any materially false, fictitious, or fraudulent statement or representation, or making or using any materially false writing or document knowing that it contains a materially false or fraudulent statement. A violation of this statute may be charged as a felony offense and may result in fines, imprisonment, or
20
both. Under the Civil Monetary Penalties Law of the Social Security Act, a person (including an organization) is prohibited from knowingly presenting or causing to be presented to any United States officer, employee, agent, or department, or any state agency a claim for payment for medical or other items or services where the person knows or should know (a) the items or services were not provided as described in the coding of the claim, (b) the claim is a false or fraudulent claim, (c) the claim is for a service furnished by an unlicensed physician, (d) the claim is for medical or other items or service furnished by a person or an entity that is in a period of exclusion from the program, or (e) the items or services are medically unnecessary items or services. Violations of the law may result in substantial penalties, treble damages, and exclusion from federal healthcare programs. In addition, the OIG may impose civil monetary penalties against any physician who knowingly accepts payment from a hospital (as well as against the hospital making the payment) as an inducement to reduce or limit medically necessary services provided to Medicare or Medicaid program beneficiaries. Further, except as permitted under the Civil Monetary Penalties Law, a person who offers or transfers to a Medicare or Medicaid beneficiary any remuneration that the person knows or should know is likely to influence the beneficiary’s selection of a particular provider of Medicare or Medicaid payable items or services may be liable for civil money penalties for each wrongful act.
In addition to the state laws previously described, we may also be subject to other state fraud and abuse statutes and regulations as we expand our operations beyond California, including into Nevada and Texas. Many states, such as California, Nevada and Texas, have adopted a form of anti-kickback law, self-referral prohibition, and false claims and insurance fraud prohibition. Many states have adopted a form of anti-kickback law, self-referral prohibition, and false claims and insurance fraud prohibition. The scope and interpretations of these laws vary from state to state and are enforced by state courts and regulatory authorities, each with broad discretion. Generally, state laws reach all healthcare services and not just those covered under a governmental healthcare program. A determination of liability under any of these laws could result in fines, penalties, and restrictions on our ability to operate in these states. We cannot assure that our arrangements or business practices will not be subject to government scrutiny or be found to violate applicable fraud and abuse laws.
Licensure, Certification, Accreditation, and Related Laws and Guidelines
Our clinical personnel are subject to numerous federal, state, and local licensing laws and regulations relating to, among other things, professional credentialing and professional ethics. Clinical professionals are also subject to state and federal regulations regarding prescribing medication and controlled substances. Our affiliated physicians and hospitalists must satisfy and maintain their individual professional licensing in each state where they practice medicine, including California, and many states require that nurse practitioners and physician assistants work in collaboration with or under the supervision of a physician. Each state defines the scope of practice of clinical professionals through legislation and through the respective Boards of Medicine and Nursing. Activities that qualify as professional misconduct under state law may subject our clinical personnel to sanctions, or to even lose their license and could potentially subject us to sanctions as well. Some state boards of medicine impose reciprocal discipline—that is, if a physician is disciplined for having committed professional misconduct in one state where they are licensed, another state where they are also licensed may impose the same discipline even though the conduct occurred in another state. Since we and our affiliated medical groups perform services at hospitals and other healthcare facilities, we may indirectly be subject to laws, ethical guidelines, and operating standards of professional trade associations and private accreditation commissions (such as the American Medical Association and The Joint Commission) applicable to those entities. Penalties for non-compliance with these laws and standards include loss of professional license, civil or criminal fines and penalties, loss of hospital admitting privileges, and exclusion from participation in various governmental and other third-party healthcare programs. In addition, our affiliated facilities are subject to state and local licensing regulations ranging from the adequacy of medical care to compliance with building codes and environmental protection laws. Our ability to operate profitably will depend, in part, upon our ability, and the ability of our affiliated physicians and facilities, to obtain and maintain all necessary licenses and other approvals and operate in compliance with applicable healthcare and other laws and regulations that evolve rapidly. We provide home health, hospice, and palliative care, which require compliance with additional regulatory requirements. Reimbursement for palliative care and house call services is generally conditioned on clinical professionals providing the correct procedure and diagnosis codes and properly documenting both the service and the medical necessity for the service. Incorrect or incomplete documentation and billing information, or the incorrect selection of codes for the level and type of service provided, could result in non-payment for services rendered or lead to allegations of billing fraud. We must also comply with laws relating to hospice care eligibility, development, and maintenance of care plans and coordination with nursing homes or assisted living facilities where patients live.
Professional Liability and Other Insurance Coverage
Our business has an inherent and significant risk of claims of medical malpractice against us and our affiliated physicians. We and our affiliated physician groups pay premiums for third-party professional liability insurance that provides indemnification on a claims-made basis for losses incurred related to medical malpractice litigation in order to carry out our operations. Our physicians are required to carry first-dollar coverage with limits of liability equal to not less than $1.0 million
21
for claims based on occurrence up to an aggregate of $3.0 million per year. Our IPAs purchase stop-loss insurance, which will reimburse them for claims from service providers on a per-enrollee basis. The specific retention amount per enrollee per policy period is $45,000 to $90,000 for professional coverage. We also maintain workers’ compensation, director and officer, and other third-party insurance coverage subject to deductibles and other restrictions that we believe are in accordance with industry standards. While we believe that our insurance coverage is adequate based upon claims experience and the nature and risks of our business, we cannot be certain that our insurance coverage will be adequate to cover liabilities arising out of pending or future claims asserted against us or our affiliated physician groups in the future where the outcomes of such claims are unfavorable. The ultimate resolution of pending and future claims in excess of our insurance coverage may have a material adverse effect on our business, financial position, results of operations, or cash flows.
Available Information
We maintain a website at www.astranahealth.com and make available there, free of charge, our periodic reports filed with the SEC, and any amendments to such reports, as soon as is reasonably practicable after filing. Information contained on or accessible through, including any reports available on, our website is not a part of, and is not incorporated by reference into, this Annual Report on Form 10-K or any other report or document we file with the SEC. Any reference to our website in this Annual Report on Form 10-K is intended to be an inactive textual reference only. The SEC maintains a website at http://www.sec.gov that contains reports, proxy and information statements, and other information regarding issuers such as us that file electronically with the SEC.
Item 1A. Risk Factors
Investing in our common stock involves a high degree of risk. You should carefully consider the risks and uncertainties described below, together with all of the other information in this Annual Report on Form 10-K, including the section titled “Management’s Discussion and Analysis of Financial Condition and Results of Operations” in Part II, Item 7, and our consolidated financial statements and related notes, before making a decision to invest in our common stock. Disclosures of risks should not be interpreted to imply that the risks have not already materialized, and the risks and uncertainties described below may not be the only ones we face. If any of the risks actually occur, our business, financial condition, operating results, and prospects could be materially and adversely affected. In that event, the market price of our common stock could decline, and you could lose part or all of your investment.
Summary of Risk Factors
Our business is subject to numerous risks and uncertainties, discussed in more detail in the following section. These include, among others, the following key risks:
•We may need to raise additional capital to grow, which might not be available.
•We could be negatively impacted by uncertain or adverse economic conditions and/or public health crises.
•Potential changes in laws, accounting principles, and regulations related to VIEs could impact our consolidation of total revenues derived from our affiliated physician groups.
•The arrangements we have with our VIEs are not as secure as direct ownership of such entities.
•We currently derive a substantial portion of our revenues in California and are vulnerable to changes in that state.
•Our business strategy involves acquisitions and strategic partnerships, which can be costly, risky, and complex.
•The Company’s complex legal structure may cause tax authorities to question our tax filing status. The Company can be adversely impacted if a tax authority does not agree with our position.
•We may encounter difficulties in managing our growth, and the nature of our business and rapid changes in the healthcare industry make it difficult to reliably predict future growth and operating results.
•We could experience significant losses under capitation contracts if our expenses exceed revenues.
22
•If our agreements with affiliated physician groups are deemed invalid or are terminated under applicable law, our results of operations and financial condition will be materially impaired.
•Our revenues and operations are dependent on a limited number of key payers.
•We may be impacted by a shift in payer mix, including eligibility changes to government and private insurance programs.
•Many of our agreements with hospitals and medical groups have limited durations, may be terminated without cause by them, and prohibit us from acquiring physicians or patients from or competing with them.
•Changes to federal, state, and local healthcare law, including the ACA and/or the adoption of a primarily publicly funded healthcare system, may negatively impact our business.
•The success of our emphasis on the ACO REACH Model is not guaranteed, due to political risks, uncertainties of ACO REACH administration, program economics, the requirement of the Company to maintain significant capital reserves, and the possibility that the ACO REACH Program will not be expanded beyond 2025.
•Laws regulating the corporate practice of medicine could restrict the manner in which we are permitted to conduct our business and the failure to comply with such laws could subject us to penalties and restructuring.
•The healthcare industry is intensely regulated at the federal, state, and local levels, and government authorities may determine that we fail to comply with applicable laws or regulations and take action against us.
•Controls imposed by Medicare, Medicaid, and private payers designed to reduce inpatient services and associated costs may reduce our revenues.
•If our affiliated physician groups are not able to satisfy California regulations related to financial solvency and operational performance, they could become subject to sanctions and their ability to do business in California could be limited or terminated.
•Our current principal stockholders, executive officers, and directors have significant influence over our operations and strategic direction, and they could cause us to take actions with which other stockholders might not agree and could delay, deter, or prevent a change of control or a business combination with respect to us.
Risks Relating to Our General Business and Operations.
In 2019, the Company, Astrana Medical, and APC consummated a series of interrelated transactions that may expose the Company and its subsidiaries and VIEs to additional risks, including the inability to repay a significant loan made in connection with such transactions.
On September 11, 2019, the Company, Astrana Medical, and APC concurrently consummated a series of interrelated transactions (collectively, the “APC Transactions”), which included a $545.0 million ten-year secured loan made by the Company to Astrana Medical, which Astrana Medical used to purchase 1,000,000 shares of Series A Preferred Stock of APC. The Company obtained the funds to make the loan to Astrana Medical (i) by entering into a credit agreement with Truist Bank, in its capacity as administrative agent for various lenders, and the lenders from time to time party thereto, for a $290.0 million senior secured credit facility (the “Credit Agreement” and the credit facility thereunder, the “Credit Facility”), and then immediately drawing down $250.0 million in cash, and (ii) by selling $300.0 million of shares of the Company’s common stock to APC, the purchase price of which was offset against $300.0 million of Astrana Medical’s purchase price for its APC Series A Preferred Stock. AHM guaranteed the obligations of the Company under the Credit Facility, and both the Company and AHM have granted the lenders a security interest in all of their assets, including, without limitation, in all stock and other equity issued by their subsidiaries (including the shares of AHM) and all rights with respect to the loan to Astrana Medical. The Credit Agreement was amended and restated on June 16, 2021 and was most recently amended on November 3, 2023 to, among other things, provide a new term loan to the Company in an aggregate amount of up to $300.0 million (as amended, the “Amended Credit Agreement” and the credit facility thereunder, the “Amended Credit Facility”).
23
The APC Transactions may expose the Company, its subsidiaries and its VIEs to additional risks, including without limitation, the following: Astrana Medical may never be able to repay the loan from the Company; even if Astrana Medical does not, or cannot repay the loan, the Company will be obligated to pay principal and interest on the Amended Credit Facility; in connection with the Credit Facility, the lenders were granted a first priority perfected security interest over all of the assets of the Company and its subsidiaries, and such lenders have the right to foreclose on those assets if the Company defaults on its obligations under the Amended Credit Facility; a disconnect could arise between APC achieving net income, declaring and paying dividends to Astrana Medical, and Astrana Medical making its required payments to the Company, which disconnect could materially negatively impact the Company’s financial results and its ability to make its required payments under the Amended Credit Facility; APC may be prohibited from paying, or may otherwise be unable to pay, the dividends on its Series A Preferred Stock, including under the California Corporations Code; regulators could determine that the current, post-APC Transactions consolidated structure amounts to the Company violating California’s corporate practice of medicine doctrine; and the Company may be deemed an investment company, which could impose burdensome compliance requirements on the Company and restrict its future activities.
Our failure to raise additional capital or generate cash flows necessary to expand our operations and invest in new technologies in the future could reduce our ability to compete successfully and harm our results of operations.
We may, in the future, require additional capital to grow our business and may have to raise additional funds by selling equity, issuing debt, borrowing, refinancing our existing debt, or selling assets or subsidiaries. We may not be able to obtain additional debt or equity financing on favorable terms, in a timely manner, or at all. If we raise additional equity financing, our security holders may experience significant dilution of their ownership interests. If we engage in additional debt financing, we may be required to accept terms that restrict our ability to incur additional indebtedness, force us to maintain specified liquidity or other ratios or restrict our ability to pay dividends or make acquisitions. In addition, the covenants in our Amended Credit Agreement may limit our ability to obtain additional debt or issue additional equity securities, and any failure to adhere to these covenants could result in penalties or defaults that could further restrict our liquidity or limit our ability to obtain financing. In addition, our ability to obtain additional capital may be adversely impacted by factors beyond our control, such as the market demand for our securities, the state of financial markets generally and other relevant factors, including potential worsening global economic conditions resulting from increasing inflation and interest rates, ongoing supply chain disruptions and shortages, labor shortages and geopolitical conditions, and any disruptions to, or volatility in, the credit and financial markets in the United States and worldwide that arise from any economic downturn or recession. If we need additional capital and cannot raise it on acceptable terms, or at all, we may not be able to, among other things, develop and enhance our patient services; continue to expand our organization; hire, train and retain employees; respond to competitive pressures or unanticipated working capital requirements; or pursue acquisition opportunities.
The Company has a complex legal structure, and tax regulatory authorities may disagree with our positions and conclusions regarding certain tax positions, resulting in unanticipated costs or non-realization of expected benefits.
The Company has a complex legal structure, and a tax authority may disagree with tax positions that we have taken. For example, the Internal Revenue Service or another tax authority could challenge our allocation of income by tax jurisdiction and the amounts paid between our affiliated companies pursuant to our intercompany arrangements and transfer pricing policies, including amounts paid with respect to our legal structure. A tax authority may take the position that material income tax liabilities, interest, and penalties are payable by us, in which case, we expect that we might contest such assessment. Contesting such an assessment may be lengthy and costly, and if we were unsuccessful in disputing the assessment, the implications could be materially adverse to us and affect our anticipated effective tax rate or operating income, and we could be required to pay substantial penalties and interest where applicable. The Company is currently under examination by the Internal Revenue Service for our 2019-2021 tax returns.
Our net operating loss carryforwards and certain other tax attributes will be subject to limitations.
If a corporation undergoes an “ownership change” within the meaning of Section 382 of the Internal Revenue Code of 1986, as amended, its net operating loss carryforwards and certain other tax attributes arising from before the ownership change are subject to limitations on use after the ownership change. In general, an ownership change occurs if there is a cumulative change in the corporation’s equity ownership by certain stockholders that exceeds 50 percentage points over a rolling three-year period. Similar rules may apply under state tax laws. Ownership changes in the future could result in additional limitations on our net operating loss carryforwards. Consequently, we may not be able to utilize a material portion of our net operating loss carryforwards and other tax attributes to offset our tax liabilities, which could have a material adverse effect on our cash flows and results of operations.
24
Uncertain or adverse economic conditions could adversely impact us.
The U.S. and global economy, as well as our business and results of operations, may be negatively impacted by a variety of factors, including inflation, interest rate increases, supply chain and labor disruptions, decreased consumer spending, unemployment rates, banking instability, geopolitical events and uncertainty, such as the Ukraine-Russia conflict and Israel-Hamas war, any U.S. government shutdown, any downgrades in the U.S. government’s sovereign credit rating, public health crises and an economic downturn or recession. A downturn in economic conditions could have a material adverse effect on our results of operations, financial condition, business prospects, and stock price. Historically, government budget limitations have resulted in reduced spending. Given that Medicaid is a significant component of state budgets, an economic downturn would put continued cost containment pressures on Medicaid outlays for healthcare services, including in California and other states in which we operate. The existing federal deficit and continued deficit spending by the federal government could lead to reduced government expenditures, including for government-funded programs in which we participate, such as Medicare. An economic downturn and sustained unemployment may also impact the number of enrollees in managed care programs and the profitability of managed care companies, which could result in reduced reimbursement rates. Although we attempt to stay informed, any sustained failure to identify and respond to these trends could have a material adverse effect on our results of operations, financial condition, business, and prospects.
We may be required to take write-downs or write-offs, restructuring, and impairment or other charges that could have a significant negative effect on our financial condition, results of operations, and stock price.
The Company may be forced to write-down or write-off assets in the future, restructure its operations, or incur impairment or other charges that could result in losses. Even though these charges may not have an immediate impact on our liquidity, the fact that we report charges of this nature could contribute to negative market perceptions about us or our securities and may make our future financing difficult to obtain on favorable terms or at all.
From time to time, our intangible assets are subject to impairment testing. Under current accounting standards, our goodwill, including acquired goodwill, is tested for impairment on an annual basis and may be subject to impairment losses as circumstances change (e.g., after an acquisition). If we record an impairment loss, it could have a material adverse effect on our results of operations for the year in which the impairment is recorded.
A prolonged disruption of or any actual or perceived difficulties in the capital and credit markets may adversely affect our future access to capital, our cost of capital, and our ability to continue operations.
Our operations and performance depend primarily on California and U.S. economic conditions and their impact on purchases of, or capitated rates for, our healthcare services, and our business is significantly exposed to risks associated with government spending and private payer reimbursement rates. A number of factors have negatively impacted the economy in recent years, including inflation, increased interest rates, supply chain and labor disruptions, geopolitical events and uncertainty, and declines in consumer and business confidence, as well as private and government spending, together with significant reductions in the availability of and increases in the cost of credit and volatility in the capital and credit markets. Such factors have adversely affected the business and economic environment in which we operate and our profitability and could, in the future, adversely affect our patients’ spending habits, private payers’ access to capital, and governmental budgetary processes, which, in turn, could result in reduced revenue for us. The continuation or recurrence of any of these conditions may adversely affect our cash flows, results of operations, and financial condition. As economic uncertainty may continue in future periods, our patients, private payers, and government payers may alter their purchasing activities of healthcare services. Our patients may scale back healthcare spending, and private and government payers may reduce reimbursement rates, which may also cause delay or cancellation of consumer spending for discretionary and non-reimbursed healthcare. This uncertainty may also affect our ability to prepare accurate financial forecasts or meet specific forecasted results, and we may be unable to adequately respond to or forecast further changes in demand for healthcare services. Volatility and disruption of capital and credit markets may adversely affect our access to capital and increase our cost of capital. Should current economic and market conditions deteriorate, our ability to finance ongoing operations and our expansion may be adversely affected, we may be unable to raise necessary funds, our cost of debt or equity capital may increase significantly, and future access to capital markets may be adversely affected.
If there is a change in accounting principles or the interpretation thereof affecting consolidation of VIEs, it could impact our consolidation of total revenues derived from our affiliated physician groups.
Our financial statements are consolidated and include the accounts of our majority-owned subsidiaries and various non-owned affiliated physician groups that are VIEs, whose consolidation is effectuated in accordance with applicable accounting rules promulgated by the Financial Accounting Standards Board (“FASB”). Such accounting rules require that,
25
under some circumstances, the VIE consolidation model be applied when a reporting enterprise holds a variable interest (e.g., equity interests, debt obligations, certain management, and service contracts) in a legal entity. Under this model, an enterprise must assess the entity in which it holds a variable interest to determine whether it meets the criteria to be consolidated as a VIE. If the entity is a VIE, the consolidation framework next identifies the party, if one exists, that possesses a controlling financial interest in the VIE, and then requires that party to consolidate the VIE as it is the primary beneficiary. An enterprise’s determination of whether it has a controlling financial interest in a VIE requires that a qualitative determination be made, and is not solely based on voting rights. If an enterprise determines the entity in which it holds a variable interest is not subject to the VIE consolidation model, the enterprise should apply the traditional voting control model, which focuses on voting rights.
In our case, the VIE consolidation model applies to our controlled, but not owned, physician-affiliated entities. Our determination regarding the consolidation of our affiliates, however, could be challenged, which could have a material adverse effect on our operations. In addition, in the event of a change in accounting rules or FASB’s interpretations thereof, or if there were an adverse determination by a regulatory agency or a court or a change in state or federal law relating to the ability to maintain present agreements or arrangements with our affiliated physician groups, we may not be permitted to continue to consolidate the revenues of our VIEs.
Breaches or compromises of our information security systems or our information technology systems or infrastructure could result in exposure of private information, disruption of our business, and damage to our reputation, which could harm our business, results of operation, and financial condition.
In the ordinary course of our business, we create, receive, maintain, transmit, collect, store, use, disclose, share and process sensitive data, including PHI and other types of personal data or personally identifiable information (collectively, “PII” and, together with PHI, “PHI/PII”) relating to our patients, employees, vendors, and others. We also contract with third-party service providers to process sensitive information, including PHI/PII, confidential information and other proprietary business information. We are highly dependent on information technology networks and systems, including the internet, to securely process PHI/PII and other sensitive data and information. Security breaches of this infrastructure, whether ours or of our third-party service providers, including physical or electronic break-ins, employee or service provider error, third-party action, including actions of foreign actors, insider attacks, phishing or denial-of-service attacks, computer viruses, ransomware or other malware, social engineering, malfeasance, other unauthorized physical or electronic access, or other vulnerabilities, could create system disruptions, shutdowns or unauthorized access, acquisition, use, disclosure or modifications of such data or information, and could cause PHI/PII to be accessed, acquired, used, disclosed or modified without authorization, to be made publicly available, or to be further accessed, acquired, used or disclosed. To our knowledge, we have not experienced any material breach of our cybersecurity systems.
We use third-party service providers for important aspects of the processing of employee and patient PHI/PII and other confidential and sensitive data and information, and therefore rely on third parties to manage functions that have material cybersecurity risks. Because of the sensitivity of the PHI/PII and other sensitive data and information that we and our service providers process, the security of our technology platform and other aspects of our services, including those provided or facilitated by our third-party service providers, are important to our operations and business strategy. We have implemented certain administrative, physical and technological safeguards to address these risks; however, such policies and procedures may not address certain HIPAA requirements or address situations that could lead to increased privacy or security risks. We may be required to expend significant capital and other resources to protect against security breaches, to safeguard the privacy, security, and confidentiality of PHI/PII and other sensitive data and information, to investigate, contain, remediate, and mitigate actual or potential security breaches, and/or to report security breaches to patients, employees, regulators, media, credit bureaus, and other third parties in accordance with applicable law and to offer complimentary credit monitoring, identity theft protection, and similar services to patients and/or employees where required by law or otherwise appropriate. Cyber-attacks are becoming more sophisticated and frequent, and we or our third-party service providers may be unable to anticipate these techniques or implement adequate protective measures against them or to prevent future attacks, and future cyber-attacks could go undetected and persist for an extended period of time. Furthermore, to the extent artificial intelligence capabilities improve and are increasingly adopted, they may be used to identify vulnerabilities and craft increasingly sophisticated cybersecurity attacks, and vulnerabilities may be introduced from the use of artificial intelligence by us and our third-party service providers.
Our third-party service providers and others to whom we entrust confidential data, and on whom we rely to provide products and services, face similar threats and growing requirements. We depend on such parties to implement adequate controls and safeguards to protect against and report cyber incidents. If such parties fail to deter, detect or report cyber incidents in a timely manner, we may suffer from financial and other harm, including to our information, operations, performance, employees and reputation.
26
A security breach, security incident, or privacy violation that leads to unauthorized use, disclosure, access, acquisition, loss or modification of, or that prevents access to or otherwise impacts the confidentiality, security, or integrity of, patient or employee information, including PHI/PII that we or our third-party service providers process, or other confidential information could harm our reputation and business, compel us to comply with breach notification laws, cause us to incur significant costs for investigation, containment, remediation, mitigation, fines, penalties, settlements, notification to individuals, regulators, media, credit bureaus, and other third parties, complimentary credit monitoring, identity theft protection, training and similar services to participants and/or employees where required by law or otherwise appropriate, for measures intended to repair or replace systems or technology and to prevent future occurrences. We may also be subject to potential increases in insurance premiums, resulting in increased costs or loss of revenue.
If we or our third-party service providers are unable to prevent or mitigate security breaches, security incidents or privacy violations in the future, or if we or our third-party service providers are unable to implement satisfactory remedial measures with respect to known or future security incidents, or if it is perceived that we have been unable to do so, our operations could be disrupted, we may be unable to provide access to our systems, and we could suffer a loss of patients, loss of reputation, adverse impacts on patient and investor confidence, financial loss, litigation, governmental investigations or other actions, regulatory or contractual penalties, and other claims and liability. In addition, security breaches and incidents and other compromises or inappropriate access to, or acquisition or processing of, PHI/PII or other sensitive data or information can be difficult to detect, and any delay in identifying such breaches or incidents or in providing timely notification of such incidents may lead to increased harm and increased penalties. While we carry cyber insurance, we cannot be certain that our coverage will be adequate for liabilities actually incurred, that insurance will continue to be available to us on economically reasonable terms, or at all, or that any insurer will not deny coverage as to any future claim.
We rely on complex software systems and hosted applications to operate our business, and our business may be disrupted if we are unable to successfully or efficiently update these systems or convert to new systems.
We are increasingly dependent on technology systems to operate our business, reduce costs, and enhance customer service. These systems include complex software systems and hosted applications that are provided by third parties. Software systems need to be updated on a regular basis with patches, bug fixes, and other modifications. Hosted applications are subject to service availability and reliability of hosting environments. We also migrate from legacy systems to new systems from time to time. Maintaining existing software systems, implementing upgrades, and converting to new systems are costly and require personnel and other resources. The implementation of these systems upgrades and conversions is a complex and time-consuming project involving substantial expenditures for implementation activities, consultants, system hardware and software, so it often requires transforming our current business and processes to conform to new systems, and therefore, may take longer, be more disruptive, and cost more than forecast and may not be successful. If the implementation is delayed or otherwise is not successful, it may hinder our business operations and negatively affect our financial condition and results of operations. There are many factors that may materially and adversely affect the schedule, cost, and execution of the implementation process, including, without limitation, problems in the design and testing of new systems; system delays and malfunctions; the deviation by suppliers and contractors from the required performance under their contracts with us; the diversion of management attention from our daily operations to the implementation project; reworks due to unanticipated changes in business processes; difficulty in training employees in the operation of new systems and maintaining internal control while converting from legacy systems to new systems; and integration with our existing systems. Some of such factors may not be reasonably anticipated or may be beyond our control.
If our internal control over financial reporting is not considered effective, our business and stock price could be adversely affected.
Section 404 of the Sarbanes-Oxley Act of 2002 requires us to evaluate the effectiveness of our internal control over financial reporting as of the end of each fiscal year, and to include a management report assessing the effectiveness of our internal control over financial reporting in our Annual Report on Form 10-K for that fiscal year. Section 404 also requires our independent registered public accounting firm to attest to, and report on, management’s assessment of our internal control over financial reporting. Our management, including our principal executive officer and principal financial officer, does not expect that our internal control over financial reporting will prevent all errors and fraud. A control system, no matter how well-designed and operated, can provide only reasonable, not absolute, assurance that the control system’s objectives will be met. Further, the design of a control system must reflect the fact that there are resource constraints, and the benefits of controls must be considered relative to their costs. Because of the inherent limitations in all control systems, no evaluation of controls can provide absolute assurance that all control issues and instances of fraud involving a company have been, or will be, detected. The design of any system of controls is based in part on certain assumptions about the likelihood of future events, and we cannot assure you that any design will succeed in achieving its stated goals under all potential future conditions. Over time, controls may become ineffective because of changes in conditions or deterioration in the degree of compliance with policies or
27
procedures. Because of the inherent limitations in a cost-effective control system, misstatements due to error or fraud may occur and not be detected, such as those that resulted in the restatement of certain of our previously issued consolidated financial statements and related material weakness in August 2023. We identified a material weakness in our internal control over financial reporting in connection with the restatement, and we cannot assure you that we or our independent registered public accounting firm will not identify a material weakness in our internal controls in the future. A material weakness in our internal control over financial reporting would require management and our independent registered public accounting firm to consider our internal controls as ineffective. While we continue to take meaningful steps to enhance our disclosure controls and procedures and our internal control over financial reporting by strengthening our financial reporting and accounting functions, we cannot provide any assurance that we will be able to maintain adequate controls over our financial processes and reporting in the future or that we will not identify additional significant deficiencies and material weaknesses in our internal control over financial reporting in the future. Any failure of our internal controls could result in material misstatements in our consolidated financial statements, significant deficiencies, material weaknesses, costs, failure to timely meet our periodic reporting obligations and erosion of investor confidence. Such failure could also negatively affect the market price and trading liquidity of our common stock, subject us to civil and criminal investigations and penalties and could have a material adverse effect on our business, financial condition, results of operations or cash flow.
We may be unable to renew our leases on favorable terms or at all as our leases expire, which could adversely affect our business, financial condition, and results of operations.
We operate several leased premises. There is no assurance that we will be able to continue to occupy such premises in the future. For example, we currently rent our corporate headquarters on a month-to-month basis. We could thus spend substantial resources to meet the current landlords’ demands or look for other premises. We may be unable to timely renew such leases or renew them on favorable terms, if at all. If any current lease is terminated or not renewed, we may be required to relocate our operations at substantial costs or incur increased rental expenses, which could adversely affect our business, financial condition, and results of operations.
We currently derive a substantial portion of our revenues in California and are vulnerable to changes in that state.
We primarily operate in California. Any material changes with respect to consumer preferences, taxation, reimbursements, financial requirements, or other aspects of healthcare delivery in California or the state’s economic conditions could have an adverse effect on our business, results of operations, and financial condition.
Our success depends, to a significant degree, upon our ability to adapt to the ever-changing healthcare industry and continued development of additional services.
Although we expect to provide a broad and competitive range of services, there can be no assurance of acceptance of current services by the marketplace. Our ability to procure new contracts may be dependent upon the continuing results achieved at the current facilities, upon pricing and operational considerations, and the potential need for continuing improvement to our existing services. Moreover, the markets for our new services may not develop as expected nor can there be any assurance that we will be successful in marketing any such services.
Our reputation could be adversely impacted by environmental, social and governance (“ESG”), policies and practices.
The increasing focus by stakeholders on our ESG policies and practices, including corporate citizenship and sustainability, could result in additional costs, and could adversely impact our reputation, consumer perception, employee retention, and willingness of third parties to do business with us. Additionally, public interest and legislative pressure related to public companies’ ESG practices continues to grow. If our ESG policies and practices fail to meet regulatory requirements or stakeholders’ evolving expectations and standards for responsible corporate citizenship, our reputation and employee retention may be negatively impacted. We could also incur additional costs and require additional resources to monitor, report and comply with various ESG practices, laws and regulations, as well as any initiatives or goals we may establish or announce. If we do establish such initiatives or goals, there can be no assurance that our stakeholders will agree with our strategy or that we will be successful in achieving such initiatives or goals. Moreover, we may determine that it is in the best interest of our Company and our stockholders to prioritize other business, social, governance or sustainability investments over the achievement of any such initiatives or goals based on economic, regulatory and social factors, business strategy or pressure from investors, activist groups or other stakeholders. Inconsistency of legislation and regulations among jurisdictions, including anti-ESG policies or legislation, and expected additional regulations may also affect the costs of compliance with such laws and regulations. If we fail to adopt ESG standards or practices as quickly as stakeholders desire, fail, or are perceived to fail, in our achievement of any initiatives or goals, or fail in fully and accurately reporting our progress on any such initiatives and goals,
28
our reputation, business, financial performance and growth may be adversely impacted. Any such matters, or related corporate citizenship and sustainability matters, could have a material adverse effect on our business.
Risks Relating to Our Growth Strategy and Business Model.
Our growth strategy may not prove viable and we may not realize expected results.
Our business strategy is to grow rapidly by building a network of medical groups and integrated physician networks and is significantly dependent on locating and acquiring, partnering or contracting with medical practices to provide healthcare delivery services. We seek growth opportunities both organically and through acquisitions of or alliances with other medical service providers. As part of our growth strategy, we regularly review potential strategic opportunities, including acquisitions, partnerships, investments and divestitures. Identifying and establishing suitable strategic relationships is time-consuming and costly. There can be no assurance that we will be successful. We cannot guarantee that we will be successful in pursuing such strategic opportunities or assure the consequences of any strategic transactions. If we fail to evaluate and execute strategic transactions properly, we may not achieve anticipated benefits and may incur increased costs.
Our strategic transactions involve a number of risks and uncertainties, including:
•We may not be able to successfully identify suitable strategic opportunities, complete desired strategic transactions, or realize their expected benefits. In addition, we compete for strategic transactions with other potential players, some of whom may have greater resources than we do. This competition may intensify due to the ongoing consolidation in the healthcare industry, which may increase our costs to pursue such opportunities.
•We may not be able to establish suitable strategic relationships and may fail to integrate them into our business. We cannot be certain of the extent of any unknown, undisclosed or contingent liabilities of any acquired business, including liabilities for failure to comply with applicable laws. We may incur material liabilities for past activities from strategic relationships. Also, depending on the location of the strategic transactions, we may be required to comply with laws and regulations that may differ from those of California, the state in which we currently operate.
•We may form strategic relationships with medical practices that operate with lower profit margins as compared with ours or that have a different payer mix than our other practice groups, which would reduce our overall profit margin. Depending upon the nature of the local market, we may not be able to implement our business model in every local market that we enter, which could negatively impact our revenues and financial condition.
•We may incur substantial costs to complete strategic transactions, integrate strategic relationships into our business, or expand our operations, including hiring more employees and engaging other personnel, to provide services to additional patients that we are responsible for managing pursuant to the new relationships. If such relationships terminate or diminish before we can realize their expected benefits, any costs that we have already incurred may not be recovered.
•If we finance strategic transactions by issuing our equity securities or securities convertible thereto, our existing stockholders could be diluted. If we finance strategic transactions with debt, it could result in higher leverage and interest costs for us.
•If we are not successful in our efforts to identify and execute strategic transactions on beneficial terms, our ability to implement our business plan and achieve our targets could be adversely affected.
The process of integrating strategic relationships also involves significant risks, including:
•difficulties in coping with demands on management related to the increased size of our business;
•difficulties resulting from the diversion of management’s attention from our daily operations;
•difficulties in assimilating different corporate cultures and business practices;
•difficulties in converting other entities’ books and records and conforming their practices to ours;
•difficulties in integrating operating, accounting, and information technology systems of other entities with ours and in maintaining uniform procedures, policies, and standards such as internal accounting controls;
29
•difficulties in retaining employees who may be vital to the integration of the acquired entities; and
•difficulties in maintaining contracts and relationships with payers of other entities.
We may be required to make certain contingent payments in connection with strategic transactions from time to time. The fair value of such payments is reevaluated periodically based on changes in our estimate of future operating results and changes in market discount rates. Any changes in our estimated fair value are recognized in our results of operations. The actual payments, however, may exceed our estimated fair value. Increases in actual contingent payments compared to the amounts recognized may have an adverse effect on our financial condition.
There can be no assurance that we will be able to effectively integrate strategic relationships into our business, which may negatively impact our business model, revenues, results of operations, and financial condition. In addition, strategic transactions are time-intensive, requiring significant commitment of our management’s focus. If our management spends too much time assessing potential opportunities, completing strategic transactions, and integrating strategic relationships, our management may not have sufficient time to focus on our existing operations. This diversion of attention could have material and adverse consequences on our operations and profitability.
Obligations in our credit or loan documents could restrict our operations, particularly our ability to respond to changes in our business or to take specified actions. An event of default could harm our business, and creditors having security interests over our assets would be able to foreclose on our assets.
The terms of our Amended Credit Agreement and other indebtedness we may incur from time to time require us to comply with a number of financial and other obligations, which may include maintaining debt service coverage and leverage ratios and maintaining insurance coverage, that impose significant operating and financial restrictions on us, including restrictions on our ability to take actions that may be in our interests. These obligations may limit our flexibility in our operations, and breaches of these obligations could result in defaults under the agreements or instruments governing the indebtedness, even if we had satisfied our payment obligations. Moreover, if we defaulted on these obligations, creditors having security interests over our assets could exercise various remedies, including foreclosing on and selling our assets. Unless waived by creditors, for which no assurance can be given, defaulting on these obligations could result in a material adverse effect on our financial condition and ability to continue our operations.
We may encounter difficulties in managing our growth, and the nature of our business and rapid changes in the healthcare industry make it difficult to reliably predict future growth and operating results.
We may not be able to successfully grow and expand. Successful implementation of our business plan will require management of growth, including potentially rapid and substantial growth, which could result in an increase in the level of responsibility for management personnel and strain on our human and capital resources. To manage growth effectively, we will be required, among other things, to continue to implement and improve our operating and financial systems, procedures, and controls and to expand, train, and manage our employee base. If we are unable to implement and scale improvements to our existing systems and controls in an efficient and timely manner or if we encounter deficiencies, we will not be able to successfully execute our business plans. Failure to attract and retain sufficient numbers of qualified personnel could also impede our growth. If we are unable to manage our growth effectively, it will have a material adverse effect on our business, results of operations, and financial condition.
The evolving nature of our business and rapid changes in the healthcare industry make it difficult to anticipate the nature and amount of medical reimbursements, third-party private payments, and participation in certain government programs and thus to reliably predict our future growth and operating results.
We could experience significant losses under capitation contracts if our expenses exceed revenues.
Under a capitation contract, a health plan typically prospectively pays an IPA periodic capitation payments based on a percentage of the amount received by the health plan. Capitation payments, in the aggregate, represent a prospective budget from which an IPA manages care-related expenses on behalf of the population enrolled with that IPA. If our affiliated IPAs are able to manage care-related expenses under the capitated levels, we realize operating profits from capitation contracts. However, if care-related expenses exceed projected levels, our affiliated IPAs may realize substantial operating deficits, which are not capped and could lead to substantial losses. For example, the State of California’s Budget Act of 2023 (AB 118) mandated a “targeted rate increase” in reimbursement rates under the Medi-Cal program for providers of primary care and obstetric care services commencing January 1, 2024, including where applicable, an equivalent adjustment to capitation rates for those providers reimbursed on a capitated basis. If the required capitation rate adjustments payable to such primary care and
30
obstetric care providers exceed the corresponding capitation rate increase received by us from our contracted Medi-Cal health plans, substantial losses could result.
Additionally, factors beyond our control, such as natural disasters, the potential effects of climate change, and major epidemics, pandemics, or newly emergent viruses (such as COVID-19), could reduce our ability to effectively manage the costs of providing healthcare.
Following the acquisition of our Restricted Knox-Keene licensed health plan (For Your Benefit Inc., “FYB”), we may expand the use of “global” capitation arrangements whereby FYB accepts financial risk for hospital and other institutional services in addition to professional medical services (whereas IPA capitation contracts are typically limited to accepting financial risk for professional medical services). However, if care-related expenses under these global capitation arrangements exceed projected levels, our Restricted Knox-Keene licensed health plan may realize substantial operating deficits, which are not capped and could lead to substantial losses. Expansion of global capitation arrangements may also require the funding of additional capital to our Restricted Knox-Keene licensed health plan in order to comply with DMHC regulations relating to tangible net equity which could result in having less cash available for other parts of our operations.
If our agreements with affiliated physician groups are deemed invalid or are terminated under applicable law, our results of operations and financial condition will be materially impaired.
There are various state laws, including laws in California and other states in which we operate, regulating the corporate practice of medicine, which prohibit us from directly owning medical professional entities. These prohibitions are intended to prevent unlicensed persons from interfering with or inappropriately influencing a physician’s professional judgment. These and other laws may also prevent fee-splitting, which is the sharing of professional service income with non-professional or business interests. The interpretation and enforcement of these laws vary significantly from state to state. We currently derive revenues from MSAs or similar arrangements with our affiliated IPAs, whereby we provide management and administrative services to them. If these agreements and arrangements are held to be invalid under laws prohibiting the corporate practice of medicine and other laws or new laws are adopted that prohibit such agreements or arrangements, a significant portion of our revenues would be lost, resulting in a material adverse effect on our results of operations and financial condition.
The arrangements we have with our VIEs are not as secure as direct ownership of such entities.
Because of corporate practice of medicine laws, we have entered into contractual arrangements to manage certain affiliated physician practice groups, which allow us to consolidate those groups for financial reporting purposes. We do not have direct ownership interests in any of our VIEs and are not able to exercise rights as an equity holder to directly change the members of the boards of directors of these entities so as to affect changes at the management and operational level. Under our arrangements with our VIEs, we must rely on their equity holders to exercise our control over the entities. If our affiliated entities or their equity holders fail to perform as expected, we may have to incur substantial costs and expend additional resources to enforce such arrangements.
Any failure by our affiliated entities or their owners to perform their obligations under their agreements with us would have a material adverse effect on our business, results of operations and financial condition.
Our affiliated physician practice groups are owned by individual physicians who could die, become incapacitated, or become no longer affiliated with us. Although our MSAs with these affiliates provide that they will be binding on successors of current owners, as the successors are not parties to the MSAs, it is uncertain in case of the death, bankruptcy, or divorce of a current owner whether their successors would be subject to such MSAs.
Our revenues and operations are dependent on a limited number of key payers.
Our operations are dependent on a concentrated number of payers. Four payers accounted for an aggregate of 61.7% and 59.0% of our total net revenue for the years ended December 31, 2023 and 2022, respectively. We believe that a majority of our revenues will continue to be derived from a limited number of key payers, which may terminate their contracts with us, or our physicians credentialed by them, upon the occurrence of certain events. They may also amend the material terms of the contracts under certain circumstances. Failure to maintain such contracts on favorable terms, or at all, would materially and adversely affect our results of operations and financial condition.
31
An exodus of our patients could have a material adverse effect on our results of operations. We may also be impacted by a shift in payer mix, including eligibility changes to government and private insurance programs.
A material decline in the number of patients that we and our affiliated physician groups serve, whether a government or a private entity is paying for their healthcare, could have a material adverse effect on our results of operations and financial condition, which could result from increased competition, new developments in the healthcare industry, or regulatory overhauls. In light of the repeal of the individual mandate requirement under the ACA via the Tax Cuts and Jobs Act of 2017, some people are expected to lose their health insurance and thus may not continue to afford services by our managed medical groups. In addition, due to potential decreased availability of healthcare through private employers, the number of patients who are uninsured or participate in governmental programs may increase. A shift in payer mix from managed care and other private payers to government payers or the uninsured may result in a reduction in our rates of reimbursement or an increase in our uncollectible receivables or uncompensated care, with a corresponding decrease in our net revenue. Changes in the eligibility requirements for governmental programs could also change the number of patients who participate in such programs or the number of uninsured patients. For those patients who remain with private insurance, changes in those programs could increase patient responsibility amounts, resulting in a greater risk for uncollectible receivables. Such events could have a material adverse effect on our business, results of operations and financial condition.
Our future growth could be harmed if we lose the services of our key management personnel.
Our success depends to a significant extent on the continued contributions of our key management personnel, particularly our Chief Executive Officer and President Brandon K. Sim, M.S. for the management of our business and implementation of our business strategy. The loss of his services, or services of other key members of management, could have a material adverse effect on our business, financial condition, and results of operations.
If having our key personnel serving as nominee equity holders of our VIEs is deemed invalid under applicable laws, or if we lose the services of key personnel for any reason, it could have a material adverse impact on our results of operations and financial condition.
There are various state laws, including laws in California and other states in which we operate, regulating the corporate practice of medicine, which prohibit us from owning various healthcare entities. These corporate practice of medicine prohibitions are intended to prevent unlicensed persons from interfering with or inappropriately influencing a physician’s professional judgment. The interpretation and enforcement of these laws vary significantly from state to state. As a result, many of our affiliated physician practice groups are either wholly owned or primarily owned by key personnel as the nominee shareholder for our benefit. If these arrangements were held to be invalid under applicable laws, which may change from time to time, a significant portion of our consolidated revenues would be affected, which may result in a material adverse effect on our results of operations and financial condition. Similarly, if such key personnel die, become incapacitated, or otherwise are no longer affiliated with us, our relationships and arrangements with those VIEs could be in jeopardy, and our business could be adversely affected.
We are dependent in part on referrals from third parties and preferred provider status with payers.
Our business relies in part on referrals from third parties for our services. We receive referrals from community medical providers, emergency departments, payers, and hospitals in the same manner as other medical professionals receive patient referrals. We do not provide compensation or other remuneration to referral sources for referring patients to us. A decrease in these referrals due to competition, concerns about our services and other factors could result in a significant decrease in our revenues and adversely impact our financial condition. Similarly, we cannot assure that we will be able to obtain or maintain preferred provider status with significant third-party payers in the communities where we operate. If we are unable to maintain our referral base or our preferred provider status with significant third-party payers, it may negatively impact our revenues and financial performance.
Partner facilities may terminate agreements with our affiliated physician groups or reduce their fees.
Our hospitalist physician services net revenue is derived from contracts directly with hospitals and other inpatient and post-acute care facilities. Our current partner facilities may decide not to renew contracts with, impose unfavorable terms on, or reduce fees paid to our affiliated physician groups. Any of these events may impact the ability of our affiliated physician groups to operate at such facilities, which would negatively impact our revenues, results of operations, and financial condition.
Many of our agreements with hospitals and medical groups have limited durations, may be terminated without cause by them, and prohibit us from acquiring physicians or patients from or competing with them.
32
Many of our agreements with hospitals and medical groups are limited in their terms or may be terminated without cause by providing advance notice. If such agreements are not renewed or terminated, we would lose the revenue generated by them. Any such events could have a material adverse effect on our results of operations, financial condition, and future business plans. Because many of such agreements with hospitals and medical groups prohibit us from acquiring physicians or patients from or competing with them, our ability to hire physicians, attract patients, or conduct business in certain areas may be limited in some cases.
Our business model depends on numerous complex management information systems, and any failure to successfully maintain these systems or implement new systems could undermine our ability to receive payments and otherwise materially harm our operations and may result in violations of healthcare laws and regulations.
We depend on a complex, specialized, integrated management information system and standardized procedures for operational and financial information, as well as for our billing operations. We may be unable to enhance existing management information systems or implement new management information systems when necessary. We may experience unanticipated delays, complications, or expenses in implementing, integrating, and operating our systems. Our management information systems may require modifications, improvements, or replacements that may require both substantial expenditures, as well as interruptions in operations. Our ability to create and implement these systems depends on the availability of technology and skilled personnel. Our failure to successfully implement and maintain all of our systems could undermine our ability to receive payments and otherwise have a material adverse effect on our business, results of operations, and financial condition. Our failure to successfully operate our billing systems could also lead to potential violations of healthcare laws and regulations.
We currently, and may in the future, have assets held at financial institutions that exceed the insurance coverage offered by the Federal Deposit Insurance Corporation (“FDIC”); the loss of such assets would have a severe negative affect on our operations and liquidity.
We maintain our cash assets at certain financial institutions in the U.S. in amounts that are significantly in excess of the FDIC insurance limit of $250,000. As of December 31, 2023, our deposit accounts with banks exceeded the FDIC’s insured limit by approximately $318.9 million. In the event of a failure of any financial institutions where we maintain our deposits or other assets, we may incur a significant loss to the extent such loss exceeds the FDIC insurance limitation, which could have a material adverse effect on our liquidity, financial condition and our results of operations.
Risks Relating to the Healthcare Industry.
The healthcare industry is highly competitive.
We compete directly with national, regional, and local providers of inpatient healthcare for patients and physicians. There are many other companies and individuals currently providing healthcare services, many of which have been in business longer and/or have substantially more resources. Since there are virtually no substantial capital expenditures required for providing healthcare services, there are few financial barriers to entry into the healthcare industry. Other companies could enter the healthcare industry in the future and divert some or all of our business. On a national basis, our competitors include, but are not limited to, Optum, Heritage, Privia Health, and Aledade, each of which has greater financial and other resources available to them. We also compete with physician groups and privately-owned healthcare companies in local markets. In addition, our relationships with governmental and private third-party payers are not exclusive and our competitors have established or could seek to establish relationships with such payers to serve their covered patients. Competitors may also seek to compete with us for acquisitions, which could have the effect of increasing the price and reducing the number of suitable acquisitions, which would have an adverse impact on our growth strategy. Individual physicians, physician groups, and companies in other healthcare industry segments, including those with which we have contracts, and some of which have greater financial, marketing, and staffing resources, may become competitors in providing healthcare services, and this competition may have a material adverse effect on our business operations and financial position. We therefore may be unable to compete successfully and even after we expend significant resources.
33
Hospitals where our affiliated physicians provide services may deny privileges to our physicians.
In general, our affiliated physicians may only provide services in a hospital where they have maintained certain credentials, also known as privileges, which are granted by the medical staff according to the bylaws of the hospital. The medical staff could decide that our affiliated physicians can no longer receive privileges to practice there. Such a decision would limit our ability to furnish services at the hospital, decrease the number of our affiliated physicians, or preclude us from entering new hospitals. In addition, hospitals may attempt to enter into exclusive contracts for certain physician services, which would reduce our access to patient populations within the hospital.
Changes associated with reimbursements by third-party payers or decreases in payer rates may adversely affect our operations.
The medical services industry is undergoing significant changes with government and other third-party payers that are taking measures to reduce reimbursement rates or, in some cases, denying reimbursement altogether. There is no assurance that government or other third-party payers will continue to pay for the services provided by our affiliated medical groups. Furthermore, there has been, and continues to be, a great deal of discussion and debate about the repeal and replacement of existing government reimbursement programs, such as the ACA. As a result, the future of healthcare reimbursement programs is uncertain, making long-term business planning difficult and imprecise. In addition, decreases in payer rates, either prospectively or retroactively, could have a significant adverse effect on our revenues, cash flows, and results of operations. The failure of government or other third-party payers to adequately cover the medical services provided by us could have a material adverse effect on our business, results of operations, and financial condition.
Our business may be significantly and adversely affected by legislative initiatives aimed at or having the effect of reducing healthcare costs associated with Medicare and other government healthcare programs and changes in reimbursement policies. In order to participate in the Medicare program, our affiliated provider groups must comply with stringent and often complex enrollment and reimbursement requirements; failure to do so could result in the provider group’s participation in the federal health care programs being terminated, or civil and/or criminal penalties being imposed. These programs generally provide for reimbursement on a fee-schedule basis rather than on a charge-related basis. As a result, we cannot increase our revenue by increasing the amount that we and our affiliates charge for services. To the extent that our costs increase, we may not be able to recover the increased costs from these programs. In addition, cost containment measures in non-governmental insurance plans have generally restricted our ability to recover, or shift to non-governmental payers, these increased costs. In attempts to limit federal and state spending, there have been, and we expect that there will continue to be, a number of proposals to limit or reduce Medicare reimbursement for various services. For example, the Medicare Access and CHIP Reauthorization Act of 2015 made numerous changes to Medicare, Medicaid, and other healthcare-related programs, including new systems for establishing annual updates to Medicare rates for physicians’ services.
We may have difficulty collecting payments from third-party payers in a timely manner.
We derive significant revenue from third-party payers, and delays in payment or refunds to payers may adversely impact our net revenue. We assume the financial risks relating to uncollectible and delayed payments. In particular, we rely on some key governmental payers. Governmental payers typically pay on a more extended payment cycle, which could require us to incur substantial expenses prior to receiving corresponding payments. In the current healthcare environment, as payers continue to control expenditures for healthcare services, including through revising their coverage and reimbursement policies, we may continue to experience difficulties in collecting payments from payers who may seek to reduce or delay such payments. If we are not timely paid in full or if we need to refund some payments, our revenues, cash flows, and financial condition could be adversely affected.
Federal and state laws may limit our ability to collect monies owed by patients.
We use third-party collection agencies whom we do not control to collect from patients any co-payments and other payments for services that our physicians provide. The federal Fair Debt Collection Practices Act of 1977 (the “FDCPA”) restricts the methods that third-party collection companies may use to contact and seek payment from consumer debtors regarding past-due accounts. State laws vary with respect to debt collection practices, although most state requirements are similar to those under the FDCPA. Therefore, such agencies may not be successful in collecting payments owed to us and our affiliated physician groups. If the practices of collection agencies utilized by us are inconsistent with these standards, we may be subject to actual damages and penalties. These factors and events could have a material adverse effect on our business, results of operations, and financial condition.
34
We have established reserves for our potential medical claim losses, which are subject to inherent uncertainties, and a deficiency in the established reserves may lead to a reduction in our assets or net income.
We establish reserves for estimated IBNR claims. IBNR estimates are developed using actuarial methods and are based on many variables, including the utilization of healthcare services, historical payment patterns, cost trends, product mix, seasonality, changes in membership, and other factors. The estimation methods and the resulting reserves are periodically reviewed and updated.
Many of our contracts are complex in nature and may be subject to differing interpretations regarding amounts due for the provision of various services. Such interpretations may not come to light until a substantial period of time has passed. The inherent difficulty in interpreting contracts and estimating necessary reserves could result in significant fluctuations in our estimates from period to period. Our actual losses and related expenses therefore may differ, even substantially, from the reserve estimates reflected in our financial statements. If actual claims exceed our estimated reserves, we may be required to increase reserves, which would lead to a reduction in our assets or net income.
Competition for qualified physicians, employees, and management personnel is intense in the healthcare industry, and we may not be able to hire and retain or contract with qualified physicians and other personnel.
We depend on our affiliated physicians to provide services and generate revenue. We compete with many types of healthcare providers, including teaching, research and government institutions, hospitals, and other practice groups, for the services of clinicians and management personnel. The limited number of residents and other licensed providers on the job market with the expertise necessary to provide services within our business makes it challenging to meet our hiring needs and may require us to train new employees, contract temporary physicians, or offer more attractive wage and benefit packages to experienced professionals, which could decrease our profit margins. The limited number of available residents and other licensed providers also impacts our ability to renew contracts with existing physicians on acceptable terms or replace physicians as they retire from practice. As a result, our ability to provide services could be adversely affected. In some markets, the lack of availability of clinical personnel, such as physicians and allied health professionals, has become a significant operating issue facing all healthcare providers. This shortage has required us to enhance wages and benefits to recruit and retain qualified personnel or to contract for more expensive temporary personnel. In addition, our labor costs have increased due to higher wage rates associated with the increased competitive labor market. Because the majority of our revenue consists of prospective monthly capitated, or fixed, payments per patient, our ability to pass along increased labor costs is limited. In particular, if labor costs rise at an annual rate greater than our net annual consumer price index basket update from Medicare, our results of operations and cash flows will likely be adversely affected. Any failure to recruit and retain or contract with qualified management and medical personnel, or to control our labor costs, could have a material adverse effect on our business, prospects, results of operations and financial condition. Even though our physician turnover rate has remained stable over the last three years, if the turnover rate were to increase significantly, our growth could be adversely affected. Moreover, unlike some of our competitors who sometimes pay additional compensation to physicians who agree to provide services exclusively to that competitor, our affiliated IPAs have historically not entered into such exclusivity agreements and have allowed our affiliated physicians to affiliate with multiple IPAs. This practice may place us at a competitive disadvantage regarding the hiring and retention of physicians relative to those competitors who do enter into such exclusivity agreements.
If we are unable to effectively adapt to changes in the healthcare industry, including changes to laws and regulations regarding or affecting U.S. healthcare reform, our business may be harmed.
Due to the importance of the healthcare industry in the lives of all Americans, federal, state, and local legislative bodies frequently pass legislation and promulgate regulations relating to healthcare reform or that affect the healthcare industry. As has been the trend in recent years, it is reasonable to assume that there will continue to be increased government oversight and regulation of the healthcare industry in the future. We cannot assure our stockholders as to the ultimate content, timing, or effect of any new healthcare legislation or regulations, nor is it possible at this time to estimate the impact of potential new legislation or regulations on our business. It is possible that future legislation enacted by Congress or state legislatures, or regulations promulgated by regulatory authorities at the federal or state level, could adversely affect our business or could change the operating environment of the hospitals and other facilities where our affiliated physicians provide services. It is possible that the changes to Medicare, Medicaid, or other governmental healthcare program reimbursements may serve as precedent to possible changes in other payers’ reimbursement policies in a manner adverse to us. Similarly, changes in private payer reimbursements could lead to adverse changes in Medicare, Medicaid, and other governmental healthcare programs, which could have a material adverse effect on our business, financial condition, and results of operations.
35
Although we do not anticipate that a single-payer national health insurance system will be enacted by the current Congress, several legislative initiatives have been proposed by members of Congress and presidential candidates that would establish some form of a single public or quasi-public agency that organizes healthcare financing, but under which healthcare delivery would remain private. If enacted, such a system could adversely affect our business.
Consolidation in the healthcare industry could have a material adverse effect on our business, financial condition, and results of operations.
Many healthcare industry participants and payers are consolidating to create larger and more integrated healthcare delivery systems with greater market power. We expect regulatory and economic conditions to result in additional consolidation in the healthcare industry in the future. As consolidation accelerates, the economies of scale of our partners’ organizations may grow. If a partner experiences sizable growth following consolidation, it may determine that it no longer needs to rely on us and may reduce its demand for our products and services. In addition, as healthcare providers consolidate to create larger and more integrated healthcare delivery systems with greater market power, these providers may try to use their market power to negotiate fee reductions for our products and services. Finally, consolidation may also result in the acquisition or future development by our partners of products and services that compete with our products and services. Any of these potential results of consolidation could have a material adverse effect on our business, financial condition and results of operations.
Risks Relating to ACO REACH.
There are uncertainties regarding the design and administration of the ACO REACH Model and CMS’ financial reports to ACO REACH participants, which could negatively impact our results of operations.
Due to the novelty of the ACO REACH Model, we are subject to program challenges, including, but not limited to, process design, data, and other related aspects. We rely on CMS for the design, oversight, and governance of the ACO REACH Model. If CMS cannot provide accurate data, guidance on claims processing, claims benchmarking and calculations, make timely payments, and conduct periodic process reviews, our results of operations and financial condition could be materially and adversely affected. CMS relies on various third parties to effect the ACO REACH program, including other departments of the U.S. government, such as Centers for Medicare & Medicaid Services Innovation Center (“CMMI”). CMS also relies on multiple third-party contractors to manage the ACO REACH Model program, including claims and auditing. As a result, there is the potential for errors, delays, and poor communication among the differing entities involved, which are beyond our control. As CMS is implementing extensive reporting protocols for the ACO REACH Model, CMS has indicated that because of inherent biases in reporting the results, its initial financial reports under the ACO REACH Model may not be indicative of final results of actual risk sharing and revenues that we receive. Were that to be the case, we might not report accurately our revenues for relevant periods, which could result in adjustments in a later period when we receive final results from CMS.
We chose to participate in the TCC mechanism and Global risk tracks of ACO REACH, which entails certain special risks.
Under the TCC mechanism, CMS estimates the total annual Part A and Part B Medicare expenditures of our assigned Medicare beneficiaries and pays us that projected amount in per beneficiary per month payments. We chose the Global risk track, under which we assume 100% risk for Part A and Part B Medicare expenditures where shared savings and losses are less than 25% of the benchmark, with adjusted risk corridors taking effect for any portion of shared savings/losses equaling or exceeding 25% of the benchmark—for savings/losses of 25-35%, we assume 50% risk, for savings/losses 35%-50% we assume 25% of the risk, and for savings/losses exceeding 50% of the benchmark, we assume only 10% of the risk. Under the Global risk track of the TCC mechanism, we could have profits or be liable for losses of up to 100% of the first 25% of such benchmarked expenditures, with adjusted risk corridors taking effect afterward. While performance can be monitored throughout the year, end results for any given performance year will not be known until the third quarter of the subsequent year.
Shared savings retained by our ACO are impacted by the amount of the Quality Withhold earned back.
Throughout the ACO REACH programs, a substantial portion of our ACO’s spending benchmark is held at-risk by CMS, subject to our ACO meeting certain quality measures as determined by CMS. In the ACO REACH program, the portion of the benchmark held at-risk by CMS for quality is 2% of the benchmark. Failing to earn back all or part of the portion of our ACO’s spending benchmark held at-risk by CMS for quality metrics could materially affect our financial performance in the ACO REACH programs.
We may suffer losses and may not generate savings through our participation in the ACO REACH Model.
36
Through the ACO REACH Model, CMS provides an opportunity to provider groups that are willing to assume higher levels of financial risk and reward to participate in this relatively new attribution-based risk-sharing model. The ACO REACH Model uses a prospectively set preliminary benchmark that is retrospectively adjusted throughout and at the end of the performance year. The preliminary benchmark is based on baseline historical expenditures by Participant Providers in the benchmark years trended forward using the US Per Capita Cost (“USPCC”) growth trend, and subsequently blended with regional expenditure rates, which are contained in the ACO REACH / Kidney Care Choices (“KCC”) Rate Book. The benchmark years are set at CY2017-2019 for the duration of the model. In PY2024, historical baseline expenditures are weighted at 55%, regional expenditures are weighted at 45%, and historical expenditures will be weighted less in future performance years. Throughout the performance year and after the performance year concludes, the preliminary benchmark is adjusted for numerous factors, such as the ACO’s developing risk and quality scores and beneficiaries who became ineligible for the program over the course of the performance year. If necessary, a Retrospective Trend Adjustment (“RTA”) may be applied as well. An RTA is applied if the USPCC trend differs by at least 1% from the observed expenditure trend in the National Reference Population. It adjusts the benchmark by the difference between the observed expenditure trend and the predicted USPCC trend. Once all adjustments are made to the benchmark, our ACO’s expenditures will be compared to a final benchmark to calculate shared savings or shared losses. Under the ACO REACH Model, we are responsible for savings and losses related to care received by assigned patients by covering claims from physicians, nurses, and other medical professionals. If claim costs exceed the benchmarked expenditures, or the baseline years used in benchmark calculations are statistical anomalies, we could experience losses, which could be significant. Among other things, this could result from factors beyond our control, such as inflation, natural disasters, the potential effects of climate change, and major epidemics, pandemics, or newly emergent viruses (such as COVID-19). As we are providing care coordination through our ACO, but do not provide direct patient care, our influence could be limited. Because of our limited influence, it is possible that we may not be able to control care providers’ behavior, utilization, and costs. As a result, we may not be able to generate savings through our participation in the ACO REACH Model to cover our administrative and care coordination operating costs, and any savings generated, if at all, will be earned in arrears and uncertain in both timing and amount. Furthermore, the process by which the final benchmark is calculated from the preliminary benchmark is complex, and we may have limited ability to understand what the final benchmark may be before the value is reported to us by CMS. Due to this dynamic, we may have limited ability to predict our final performance and shared savings/losses amount prior to receiving a final report from CMS in the third quarter of the year following any given performance year.
We do not control, but are responsible for savings and losses related to, care received by assigned patients at out-of-network providers, which could negatively impact our ability to control claim costs.
Medicare beneficiaries in the ACO REACH Model are not required to receive care from a specified network of contracted providers and facilities, which could make it difficult for us to control the financial risks of those beneficiaries. While we are not responsible for directly paying claims for out-of-network providers, we may have difficulty managing patient care and costs in relation to such out-of-network providers as compared to contracted, in-network providers, which could adversely impact our financial results as we are responsible for savings and losses of assigned beneficiaries, irrespective of whether they are using in-network or out-of-network providers. In addition, even if we are successful in encouraging more assigned patients to receive care from our contracted, in-network providers, there is the possibility that the monthly TCC from CMS will be insufficient to cover our expenditures, since the TCC is generally based on historical in-network/out-of-network ratios. If CMS fails to monitor the in-network/out-of-network provider ratio for our assigned patients on a frequent basis, or CMS’s reconciliation payments to us are not timely made, this could result in negative cash flows for us, especially if increased payments will need to be made to our contracted, in-network providers.
Our continued participation in other CMS Advanced Alternative Payment Models, such as the ACO REACH, cannot be guaranteed.
Our ACO participated in the GPDC Model in 2022, the ACO Reach Model in 2023 and has an active participation agreement with CMS for 2024. However, the Participation Agreement for the ACO REACH Model may be terminated sooner by CMS as specified therein and CMS has the flexibility to alter or change the program over time. Among many requirements to be eligible to participate in the ACO REACH Model, we must have at least 5,000 aligned Medicare beneficiaries and must maintain that number throughout each performance year. If that number were not maintained, we would become ineligible for the ACO REACH Model. In addition, we are required to comply with all applicable laws and regulations regarding provider-based risk-bearing entities. We could be terminated from the ACO REACH Model at any time if we do not continue to comply with the ACO REACH participation requirements. If future compliance or performance issues arise, we may lose our current eligibility and may be subject to CMS’s enforcement or contract actions, including our potential inability to participate in the TCC mechanism (where the payment mechanism would default to traditional FFS) or dismissal from the ACO REACH Model, which would have a material adverse effect on our revenues and cash flows. In addition, the payments from CMS to us will
37
decrease if the number of beneficiaries assigned to our ACO declines or if the contracted providers terminate their relationships with us, which could have a material adverse effect on our results of operations on a consolidated basis.
Risks Relating to MSSP Participation Beginning in 2024.
We may be unable to generate revenue under the MSSP or continue to participate in the MSSP.
The MSSP is consistently being updated by CMS. Beginning in 2024, the calculation of the benchmark is being adjusted to address prior performance, to incorporate a prospective administrative growth factor, and to attempt to reduce the cap on negative regional adjustments. These changes will impact how savings under the model are calculated and may impact our ability to generate revenue under the model. In addition, our participation in the MSSP requires our participant providers maintain at least 5,000 MSSP Aligned Beneficiaries. If we fail to meet the threshold, we will not be eligible to participate for the applicable year.
We may suffer losses and may not generate savings through our participation in the MSSP.
We are participating in the MSSP Level ENHANCED, pursuant to which we may be responsible for 1st dollar losses at a rate determined using a sliding scale based on the ACO’s health equity adjusted quality performance score, if an applicable quality performance standard established by CMS is met with a minimum shared loss rate of 40% and a maximum of 75%. If an applicable quality performance standard is not met, we are responsible for 1st dollar losses at a rate of 75%. Total losses for which we are responsible are not to exceed 15% of the updated benchmark. We are responsible for savings and losses related to care received by patients by covering claims from physicians, nurses, and other medical professionals. If claim costs exceed the benchmarked expenditures, we could experience losses, which could be significant. Among other things, this could result from factors beyond our control, such as inflation, natural disasters, the potential effects of climate change, and major epidemics, pandemics, or newly emergent viruses (such as COVID-19). As we are providing care coordination through our ACO, but do not provide direct patient care, our influence could be limited. Because of our limited influence, it is possible that we may not be able to control care providers’ behavior, utilization, and costs. As a result, we may not be able to generate savings through our participation in the MSSP to cover our administrative and care coordination operating costs, and any savings generated, if at all, will be earned in arrears and uncertain in both timing and amount.
We do not control, but are responsible for savings and losses related to, care received by assigned patients at out-of-network providers, which could negatively impact our ability to control claim costs.
Medicare beneficiaries in the MSSP Model are not required to receive care from a specified network of contracted providers and facilities, which could make it difficult for us to control the financial risks of those beneficiaries. While we are not responsible for directly paying claims for out-of-network providers, we may have difficulty managing patient care and costs in relation to such out-of-network providers as compared to contracted, in-network providers, which could adversely impact our financial results as we are responsible for savings and losses of assigned beneficiaries, irrespective of whether they are using in-network or out-of-network providers.
Risks Relating to Regulatory Compliance.
Laws regulating the corporate practice of medicine could restrict the manner in which we are permitted to conduct our business and the failure to comply with such laws could subject us to penalties and restructuring.
Some states have laws that prohibit business entities from practicing medicine, employing physicians to practice medicine, exercising control over medical decisions by physicians (also known collectively as the corporate practice of medicine) or engaging in some arrangements, such as fee-splitting, with physicians. In some states, these prohibitions are expressly stated in a statute or regulation, while in other states, the prohibition is a matter of judicial or regulatory interpretation. California, where a substantial amount of our operations are located, is one of the states that prohibit the corporate practice of medicine.
In California, Nevada, and Texas, we operate by maintaining contracts with our affiliated physician groups, which are each owned and operated by physicians, and which employ or contract with additional physicians to provide physician services. Under these arrangements, we or our subsidiaries provide management services, receive a management fee for providing management services, do not represent to offer medical services, and do not exercise influence or control over the practice of medicine by the physicians or the affiliated physician groups.
38
In addition to the above management arrangements, in certain instances, we have contractual rights relating to the transfer of equity interests in our affiliated physician groups under physician shareholder agreements that we entered into with the controlling equity holder of such affiliated physician groups. However, even in such instances, such equity interests cannot be transferred to or held by us or by any non-professional organization. Accordingly, we do not directly own any equity interests in any affiliated physician groups in California, Nevada, and Texas. In the event that any of these affiliated physician groups or their equity holders fail to comply with these management or ownership transfer arrangements, these arrangements are terminated, we are unable to enforce such arrangements, or these arrangements are invalidated under applicable laws, there could be a material adverse effect on our business, results of operations, and financial condition and we may have to restructure our organization and change our arrangements with our affiliated physician groups, which may not be successful.
The healthcare industry is intensely regulated at the federal, state, and local levels, and government authorities may determine that we fail to comply with applicable laws or regulations and take action against us.
As a company involved in providing healthcare services, we are subject to numerous federal, state, and local laws and regulations. There are significant costs involved in complying with these laws and regulations. If we are found to have violated any applicable laws or regulations, we could be subject to civil and/or criminal damages, fines, sanctions, or penalties, including exclusion from participation in governmental healthcare programs, such as Medicare and Medicaid, and we may be required to change our method of operations and business strategy. These consequences could be the result of our current conduct or even conduct that occurred a number of years ago. We could incur significant costs to defend ourselves if we become the subject of an investigation or legal proceeding alleging a violation of these laws and regulations. We cannot predict whether a federal, state, or local government will determine that we are not operating in accordance with the law, or whether, when or how the laws will change in the future and impact our business. The following is a non-exhaustive list of some of the more significant healthcare laws and regulations that could affect us:
•The False Claims Act, which provides for penalties against entities and individuals who knowingly or recklessly make claims to Medicare, Medicaid, and other governmental healthcare programs, as well as third-party payers, that contain or are based upon false or fraudulent information;
•A provision of the Social Security Act, commonly referred to as the “Anti-Kickback Statute,” that prohibits the knowing and willful offering, payment, solicitation, or receipt of any bribe, kickback, rebate, or other remuneration, in cash or in kind, in return for the referral or recommendation of patients for items and services covered, in or in part, by federal healthcare programs such as Medicare and Medicaid;
•A provision of the Social Security Act, commonly referred to as the Stark Law or physician self-referral law (subject to limited exceptions), prohibits physicians from referring Medicare patients to an entity for the provision of specific “designated health services” if the physician or a member of such physician’s immediate family has a direct or indirect financial relationship with the entity, and prohibits the entity from billing for services arising out of such prohibited referrals;
•A provision of the Social Security Act that provides for criminal penalties on healthcare providers who fail to disclose known overpayments;
•A provision of the Social Security Act that provides for civil monetary penalties on healthcare providers who fail to repay known overpayments within 60 days of identification or the date any corresponding cost report was due, if applicable, and also allows improper retention of known overpayments to serve as a basis for False Claims Act violations;
•Provisions of the Social Security Act (emanating from the DRA) require entities that make or receive annual Medicaid payments of $5 million or more from a single Medicaid program to provide its employees, contractors, and agents with written policies and employee handbook materials on federal and state false claims acts and related statutes, that establish a Medicaid Integrity Program designed to enhance federal and state efforts to detect Medicaid fraud, waste, and abuse, and that increase financial incentives for both states and individuals to bring fraud and abuse claims against healthcare companies;
•State law provisions pertaining to anti-kickback, self-referral, and false claims issues;
39
•Provisions of, and regulations relating to, HIPAA that provide penalties for knowingly and willfully executing a scheme or artifice to defraud a healthcare benefit program or falsifying, concealing, or covering up a material fact or making any materially false, fictitious, or fraudulent statement in connection with the delivery of or payment for healthcare benefits, items, or services;
•Provisions of HIPAA and the Health Information Technology for Economic and Clinical Health Act of 2009 (“HITECH”) limiting how covered entities, business associates, and business associate sub-contractors may use and disclose PHI and the security measures that must be taken in connection with protecting that information and related systems, as well as similar or more stringent state laws;
•Federal and state laws provide penalties for providers for billing and receiving payments from a governmental healthcare program for services unless the services are medically necessary and reasonable, adequately and accurately documented, and billed using codes that accurately reflect the type and level of services rendered;
•State laws that provide for financial solvency requirements relating to risk-bearing organizations (“RBOs”), plan operations, plan-affiliate operations and transactions, plan-provider contractual relationships, and provider-affiliate operations and transactions, such as California Business & Professions Code Section 1375.4;
•Federal laws that provide for administrative sanctions, including civil monetary penalties for, among other violations, inappropriate billing of services to federal healthcare programs, payments by hospitals to physicians for reducing or limiting services to Medicare or Medicaid patients, or employing or contracting with individuals or entities who/which are excluded from participation in federal healthcare programs;
•Federal and state laws and policies require healthcare providers to enroll in the Medicare and Medicaid programs before submitting any claims for services, to promptly report certain changes in their operations to the agencies that administer these programs, and to re-enroll in these programs when changes in direct or indirect ownership occur or in response to revalidation requests from Medicare and Medicaid;
•State laws that prohibit general business entities from practicing medicine, controlling physicians’ medical decisions or engaging in certain practices, such as splitting fees with physicians;
•State laws that require timely payment of claims, including §1371.38, et al., of the California Health & Safety Code, which imposes time limits for the payment of uncontested covered claims and requires healthcare service plans to pay interest on uncontested claims not paid promptly within the required time period;
•Laws in some states that prohibit non-domiciled entities from owning and operating medical practices in such states;
•Federal and state laws and regulations restricting the techniques that may be used to collect past due accounts from consumers, such as our patients, for services provided to the consumer; and
•State laws that require healthcare providers that assume professional and institutional risk (i.e., full risk) to either obtain a license under the Knox-Keene Health Care Service Plan Act of 1975 or receive an exemption from the California Department of Managed Healthcare (“DMHC”) for the contract(s) under which the entity assumes full risk.
Any violation or alleged violation of any of these laws or regulations by us or our affiliates could have a material adverse effect on our business, financial condition and results of operations.
Changes in healthcare laws could create an uncertain environment and materially impact us. We cannot predict the effect that the ACA (also known as Obamacare) and its implementation, amendment, or repeal and replacement, may have on our business, results of operations, or financial condition.
Any changes in healthcare laws or regulations that reduce, curtail, or eliminate payments, government-subsidized programs, government-sponsored programs, and/or the expansion of Medicare or Medicaid, among other actions, could have a material adverse effect on our business, results of operations, and financial condition.
40
For example, the ACA dramatically changed how healthcare services are covered, delivered, and reimbursed. The ACA requires insurers to accept all applicants, regardless of pre-existing conditions, cover an extensive list of conditions and treatments, and charge the same rates, regardless of pre-existing conditions or gender. The ACA and the Health Care and Education Reconciliation Act of 2010 (collectively, the “Health Care Reform Acts”) also mandated changes specific to home health and hospice benefits under Medicare. In 2012, the U.S. Supreme Court upheld the constitutionality of the ACA, including the “individual mandate” provisions of the ACA that generally require all individuals to obtain healthcare insurance or pay a penalty. However, the U.S. Supreme Court also held that the provision of the ACA that authorized the Secretary of the U.S. Department of Health and Human Services (“HHS”) to penalize states that choose not to participate in the expansion of the Medicaid program by removing all of its existing Medicaid funding was unconstitutional. In response to the ruling, a number of state governors opposed their state’s participation in the expanded Medicaid program, which resulted in the ACA not providing coverage to some low-income persons in those states. In addition, several bills have been, and are continuing to be, introduced in U.S. Congress to amend all or significant provisions of the ACA, or repeal and replace the ACA with another law. In December 2017, the individual mandate was repealed via the Tax Cuts and Jobs Act of 2017. Afterward, legal and political challenges as to the constitutionality of the remaining provisions of the ACA resumed. Just as the fate of the ACA is uncertain, so is the future of care organizations established under the ACA, such as ACOs and ACO REACH. Under its ACO REACH Participation Agreement with CMS, our operations are always subject to the nation’s healthcare laws, as amended, repealed, or replaced from time to time.
The net effect of the ACA on our business is subject to numerous variables, including the law’s complexity, lack of complete implementing regulations and interpretive guidance, gradual and potentially delayed implementation, or possible amendment, as well as the uncertainty as to the extent to which states will choose to participate in the expanded Medicaid program. The continued implementation of provisions of the ACA, the adoption of new regulations thereunder and ongoing challenges thereto, also add uncertainty about the current state of U.S. healthcare laws and could negatively impact our business, results of operations, and financial condition.
Healthcare providers could be subject to federal and state investigations and payer audits.
Due to our and our affiliates’ participation in government and private healthcare programs, we are from time to time involved in inquiries, reviews, audits, and investigations by governmental agencies and private payers of our business practices, including assessments of our compliance with coding, billing, and documentation requirements. Federal and state government agencies have active civil and criminal enforcement efforts against healthcare companies and their executives and managers. The DRA, provides a financial incentive to states to enact their own false claims acts, and similar laws encourage investigations against healthcare companies by different agencies. These investigations could also be initiated by private whistleblowers. Responding to audit and investigative activities are costly and disruptive to our business operations, even when the allegations are without merit. If we are subject to an audit or investigation, a finding could be made that we or our affiliates erroneously billed or were incorrectly reimbursed, and we may be required to repay such agencies or payers, may be subjected to pre-payment reviews, which can be time-consuming and result in non-payment or delayed payments for the services we or our affiliates provide, and may be subject to financial sanctions or required to modify our operations.
Controls imposed by Medicare, Medicaid, and private payers designed to reduce inpatient services and associated costs may reduce our revenues.
Controls imposed by Medicare, Medicaid, and private payers designed to reduce admissions and lengths of stay, commonly referred to as “utilization review,” have affected and are expected to continue to affect our operations. Federal law contains numerous provisions designed to ensure that services rendered by hospitals and other care providers to Medicare and Medicaid patients meet professionally recognized standards and are medically necessary and that claims for reimbursement are properly filed. These provisions include a requirement that a sampling of admissions of Medicare and Medicaid patients must be reviewed by quality improvement organizations, which review the appropriateness of Medicare and Medicaid patient admissions and discharges, the quality of care provided, and the appropriateness of cases of extraordinary length of stay or cost on a post-discharge basis. Quality improvement organizations may deny payment for services or assess fines and also have the authority to recommend to the HHS that a provider is in substantial non-compliance with the standards of the quality improvement organization and should be excluded from participation in the Medicare program. The ACA potentially expands the use of prepayment review by Medicare contractors by eliminating statutory restrictions on its use, and, as a result, efforts to impose more stringent cost controls are expected to continue. Utilization review is also a requirement of most non-governmental managed care organizations and other third-party payers. Inpatient utilization, average lengths of stay and occupancy rates continue to be negatively affected by payer-required pre-admission authorization and utilization review and by third-party payer pressure to maximize outpatient and alternative healthcare delivery services for less acutely ill patients. Although we are unable to predict the effect these controls and any changes thereto may have on our operations, significant
41
limits on the scope of our services reimbursed and on reimbursement rates and fees could have a material, adverse effect on our business, financial position, and results of operations.
We do not have a Knox-Keene license covering all of our lines of business.
The Knox-Keene Health Care Service Plan Act of 1975 was passed by the California State Legislature to regulate California managed care plans and is currently administered by the DMHC. A Knox-Keene Act license is required to operate a healthcare service plan, e.g., an HMO, or an organization that accepts full risk, i.e., accepts full risk for a patient population, including risk related to institutional services, e.g., hospital and professional services. Applying for and obtaining such a license is a time-consuming and detail-oriented undertaking. Although FYB is licensed by the DMHC as a full-service Restricted Knox-Keene licensed health plan, its license is limited to its Medicare Advantage line of business in designated California counties only and does not extend to all of our lines of business, such as Medi-Cal and commercial lines of business.
As such, for those lines of business not covered by our Restricted Knox-Keene license, if the DMHC were to determine that we have been inappropriately taking risk for institutional and professional services as a result of our various hospital and physician arrangements without having any Knox-Keene license or applicable regulatory exemption, we may be required to obtain a Knox-Keene license and could be subject to civil and criminal liability, any of which could have a material adverse effect on our business, results of operations, and financial condition.
If our affiliated physician groups and Restricted Knox-Keene licensed health plan are not able to satisfy California regulations related to financial solvency and operational performance, they could become subject to sanctions and their ability to do business in California could be limited or terminated.
The DMHC has instituted regulations that are intended to provide a formal mechanism for monitoring the financial solvency and operational performance of RBOs (including capitated physician groups) and Restricted Knox-Keene licensed health plans in California. Under current DMHC regulations, our affiliated physician groups, as applicable, are required to, among other things:
•Maintain, at all times, a minimum “cash-to-claims ratio” (which means the organization’s cash, marketable securities, and certain qualified receivables, divided by the organization’s total unpaid claims liability) of 0.75; and
•Submit periodic reports to the DMHC containing various data and attestations regarding their performance and financial solvency, including IBNR calculations, documentation, and attestations as to whether or not the organization (i) was in compliance with the “Knox-Keene Act” requirements related to claims payment timeliness, and (ii) had maintained compliance with minimum “cash-to-claims ratio”, tangible net equity, and positive working capital requirements.
In the event that a physician group is not in compliance with any of the above criteria, it would be required to describe in a report submitted to the DMHC the reasons for non-compliance and actions to be taken to bring it into compliance. Under such regulations, the DMHC can also make some of the information contained in the reports public, including, but not limited to, whether or not a particular physician organization met each of the criteria.
In the event that a physician group is not in compliance with any of the above criteria, it would be required to describe in a report submitted to the DMHC the reasons for non-compliance and actions to be taken to bring it into compliance. Under such regulations, the DMHC can also make some of the information contained in the reports public, including, but not limited to, whether or not a particular physician organization met each of the criteria.
Our revenue will be negatively impacted if our physicians fail to appropriately document their services.
We rely upon our affiliated physicians to appropriately and accurately complete necessary medical record documentation and assign appropriate reimbursement codes for their services. Reimbursement is conditioned upon, in part, our affiliated physicians providing the correct procedure and diagnosis codes and properly documenting the services themselves, including the level of service provided and the medical necessity for the services. If our affiliated physicians have provided incorrect or incomplete documentation or selected inaccurate reimbursement codes, this could result in non-payment for services rendered or lead to allegations of billing fraud. This could subsequently lead to civil and criminal penalties, including exclusion from government healthcare programs, such as Medicare and Medicaid. In addition, third-party payers may disallow, in whole or in part, requests for reimbursement based on determinations that certain amounts are not covered, services provided
42
were not medically necessary, or supporting documentation was not adequate. Retroactive adjustments may change amounts realized from third-party payers and result in recoupments or refund demands, affecting revenue already received.
Primary care physicians may seek to affiliate with our competitors’ IPAs.
It is common in the medical services industry for primary care physicians to be affiliated with multiple IPAs. Our affiliated IPAs, therefore, may enter into agreements with physicians who are also affiliated with our competitors. However, some of our competitors at times have agreements with physicians that require the physician to provide exclusive services. Our affiliated IPAs often have no knowledge, and no way of knowing, whether a physician is subject to an exclusivity agreement without being informed by the physician. Competitors have, in the past, initiated lawsuits against us alleging in part interference with such exclusivity arrangements, and may do so again in the future. An adverse outcome from any such lawsuit could adversely affect our business, cash flows, and financial condition.
If we inadvertently employ or contract with an excluded person, we may face government sanctions.
Individuals and entities can be excluded from participating in the Medicare and Medicaid programs for violating certain laws and regulations, or for other reasons such as the loss of a license in any state, even if the person retains other licensure. This means that the excluded person and others are prohibited from receiving payments for such person’s services rendered to Medicare or Medicaid beneficiaries, and if the excluded person is a physician, all services ordered (not just provided) by such physician are also non-covered and non-payable. Entities that employ or contract with excluded individuals are prohibited from billing the Medicare or Medicaid programs for the excluded individual’s services, and are subject to civil penalties if they do. The HHS Office of the Inspector General maintains a list of excluded persons. Although we have instituted policies and procedures to minimize such risks, there can be no assurance that we will not inadvertently hire or contract with an excluded person, or that our employees or contracts will not become excluded in the future without our knowledge. If this occurs, we may be subject to substantial repayments and civil penalties, and the hospitals at which we furnish services may also be subject to repayments and sanctions, for which they may seek recovery from us, which could adversely affect our business, cash flows, and financial condition.
Compliance with federal and state privacy and data security laws is expensive, and we may be subject to government or private actions due to privacy and security breaches.
We must comply with various federal and state laws and regulations governing the collection, dissemination, access, use, security, and confidentiality of PHI, including HIPAA and HITECH. As part of our medical record keeping, third-party billing, and other services, we collect and maintain PHI in paper and electronic format. Privacy and data security laws and regulations thus could have a significant effect on the manner in which we handle healthcare-related data and communicate with payers. In addition, compliance with these standards could limit our ability to offer services, thereby negatively impacting the business opportunities available to us. Despite our efforts to prevent privacy and security breaches, they may still occur. If any non-compliance with such laws and regulations results in privacy or security breaches, we could be subject to monetary fines, suits, penalties, or sanctions. As a result of the expanded scope of HIPAA through HITECH, we may incur significant costs in order to minimize the amount of “unsecured PHI” that we handle and retain, and/or to implement improved administrative, technical, or physical safeguards to protect PHI. We may have to demonstrate and document our compliance efforts, even if there is a low probability that PHI has been compromised, in order to overcome the presumption that an impermissible use or disclosure of PHI results in a reportable breach. We may incur significant costs to notify the relevant individuals, government entities and, in some cases, the media, in the event of a breach and to provide appropriate remediation and monitoring to mitigate any potential damage.
We may be subject to liability for failure to fully comply with applicable corporate and securities laws.
We are subject to various corporate and securities laws. Any failure to comply with such laws could cause government agencies to take action against us, which could restrict our ability to issue securities and result in fines or penalties. Any claim brought by such an agency could also cause us to expend resources to defend ourselves, divert the attention of our management from our business and could significantly harm our business, operating results, and financial condition, even if the claim is resolved in our favor.
We may face lawsuits not covered by insurance and related expenses may be material. Our failure to avoid, defend, and accrue for claims and litigation could negatively impact our results of operations or cash flows.
43
We are exposed to and become involved in various litigation matters arising out of our business, including from time to time, actual or threatened lawsuits. Malpractice lawsuits are common in the healthcare industry. The medical malpractice legal environment varies greatly by state. The status of tort reform, availability of non-economic damages, or the presence or absence of other statutes, such as elder abuse or vulnerable adult statutes, influence the incidence and severity of malpractice litigation. We may also be subject to other types of lawsuits, such as those initiated by our competitors, stockholders, employees, service providers, contractors, or by government agencies, including when we terminate relationships with them, which may involve large claims and significant defense costs. Many states have joint and several liabilities for providers who deliver care to a patient and are at least partially liable. As a result, if one provider is found liable for medical malpractice for the provision of care to a particular patient, all other providers who furnished care to that same patient, which could potentially include us and our affiliated physicians, may also share in the liability, which could be substantial individually or in aggregate.
The defense of litigation, including fees of legal counsel, expert witnesses, and related costs, is expensive and difficult to forecast accurately. Such costs may be unrecoverable even if we ultimately prevail in litigation and could consume a significant portion of our limited capital resources. To defend lawsuits, it may also be necessary for us to divert officers and other employees from our normal business functions to gather evidence, give testimony, and otherwise support litigation efforts. If we lose any material litigation, we could face material judgments or awards against them. An unfavorable resolution of one or more of the proceedings in which we are involved now or in the future could have a material adverse effect on our business, cash flows, and financial condition. We may also in the future find it necessary to file lawsuits to recover damages or protect our interests. The cost of such litigation could also be significant and unrecoverable, which may also deter us from aggressively pursuing even legitimate claims.
We currently maintain malpractice liability insurance coverage to cover professional liability and other claims for certain hospitalists and clinic physicians. All of our affiliated physicians are required to carry first-dollar coverage with limits of coverage equal to $1.0 million for all claims based on occurrence up to an aggregate of $3.0 million per year. We cannot be certain that our insurance coverage will be adequate to cover liabilities arising out of claims asserted against us, our affiliated professional organizations, or our affiliated physicians. Liabilities incurred by us or our affiliates in excess of our insurance coverage, including coverage for professional liability and other claims, could have a material adverse effect on our business, financial condition, and results of operations. Our professional liability insurance coverage generally must be renewed annually and may not continue to be available to us in future years at acceptable costs and on favorable terms, which could increase our exposure to litigation.
We may also be subject to laws and regulations not specifically targeting the healthcare industry.
Certain regulations not specifically targeting the healthcare industry could also have material effects on our operations. For example, the California Finance Lenders Law (the “CFLL”) could be applied to us as a result of our various affiliate and subsidiary loans and similar arrangements. If a regulator were to take the position that such loans were covered by the CFLL, we could be subject to regulatory action that could impair our ability to continue to operate and may have a material adverse effect on our profitability and business as we currently do not hold a CFLL licensure. Pursuant to an exemption under the CFLL, a person may make five or fewer commercial loans in a 12-month period without a CFLL licensure if the loans are “incidental” to the business of the person. This exemption, however, creates some uncertainty as to which loans could be deemed as incidental to our business. In addition, a person without a CFLL licensure may also make a single commercial loan in a 12-month period without the loan being “incidental” to such person’s business.
Risks Relating to the Ownership of Astrana’s Common Stock.
We have to meet certain requirements in order to remain as a Nasdaq-listed public company.
As a public company, Astrana is required to comply with various regulatory and reporting requirements, including those required by the SEC. Astrana is also subject to Nasdaq listing rules. Complying with these requirements is time-consuming and expensive. No assurance can be given that Astrana can continue to meet the SEC reporting and Nasdaq listing requirements.
Astrana’s common stock may be thinly traded and its market price may be subject to fluctuations and volatility. Stockholders may be unable to sell their shares at a profit and might incur losses.
44
The trading price of Astrana’s common stock has been volatile in the past and may continue to be so from time to time in the future. The price at which Astrana’s common stock trades could be subject to significant fluctuation and may be affected by a variety of factors, including the trading volume, our results of operations, the announcement and consummation of certain transactions, and our ability or inability to raise additional capital and the terms thereof, and therefore could fluctuate, and potentially decline, significantly. Other factors that may cause the market price of Astrana’s common stock to fluctuate include:
•Variations in our operating results, such as actual or anticipated quarterly and annual increases or decreases in revenue, gross margin or earnings;
•Changes in our business, operations, or prospects, including announcements relating to strategic relationships, mergers, acquisitions, partnerships, collaborations, joint ventures, dispositions, other corporate transactions, financings, capital commitments, or other events by us or our competitors;
•Developments, conditions, or trends in the healthcare industry;
•Changes in the economic performance or market valuations of other healthcare-related companies;
•General market conditions or domestic or international macroeconomic and geopolitical factors unrelated to our performance or financial condition, including economic or political instability, inflation, wars, civil unrest, terrorism, public health crises, and natural disasters;
•Sales of stock by Astrana’s stockholders generally and Astrana’s larger stockholders, including insiders, in particular, including sale or distributions of large blocks of common stock by our executives and directors or large stockholders;
•Volatility and limitations in trading volumes of Astrana’s common stock and the stock market;
•Approval, maintenance, and withdrawal of our and our affiliates’ certificates, permits, registration, licensure, certification, and accreditation by the applicable regulatory or other oversight bodies;
•Our financing activities, including our ability to obtain financings and prices at which we sell our equity securities, including securities convertible to or exercisable for shares of Astrana’s common stock;
•Failures to meet external expectations or management guidance;
•Changes in our capital structure and cash position;
•Analyst research reports on Astrana’s common stock, including analysts’ recommendations and changes in recommendations, price targets, and withdrawals of coverage;
•Departures and additions of our key personnel, including our officers or directors;
•Disputes and litigations related to intellectual properties, proprietary rights, and contractual obligations;
•Changes in applicable laws, rules, regulations, or accounting practices and other dynamics; and
•Other events or factors, many of which may be out of our control.
There may be a limited trading market for Astrana’s common stock. A lack of an active market may contribute to stock price volatility or supply/demand imbalances, make an investment in Astrana’s common stock less attractive to certain investors, and/or impair the ability of Astrana’s stockholders to sell shares at the time they desire or at a price that they consider favorable. The lack of an active market may also reduce the fair market value of Astrana’s common stock, impair our ability to raise capital by selling shares of Astrana’s common stock, or use such stock as consideration to attract and retain talent or engage in business transactions.
If analysts do not report about us, or negatively evaluate us, Astrana’s stock price could decline.
45
The trading market for Astrana’s common stock will rely in part on the availability of research and reports that third-party analysts publish about us. There are many large companies active in the healthcare industry, which makes it more difficult for us to receive widespread coverage. Furthermore, if one or more of the analysts who do cover us downgrade Astrana’s common stock, its price would likely decline. If one or more of these analysts cease coverage of us, we could lose market visibility, which in turn could cause Astrana’s stock price to decline.
Because we have no current plans to pay regular cash dividends on our common stock, you may not receive any return on investment unless you sell your common stock for a price greater than that which you paid for it.
We do not anticipate paying any regular cash dividends on our common stock. Any decision to declare and pay dividends in the future will be made at the discretion of our board of directors and will depend on, among other things, our results of operations, financial condition, cash requirements, contractual restrictions and other factors that our board of directors may deem relevant. In addition, our ability to pay dividends is, and may be, limited by covenants of existing and any future outstanding indebtedness we or our subsidiaries incur. Similarly, we may not repurchase any shares through our public repurchase program or otherwise return capital to our stockholders. Therefore, any return on investment in our common stock is dependent upon the appreciation of the price of our common stock on the open market, which may not occur.
Our current principal stockholders, executive officers, and directors have significant influence over our operations and strategic direction and they could cause us to take actions with which other stockholders might not agree and could delay, deter, or prevent a change of control or a business combination with respect to us.
As of December 31, 2023, our executive officers, directors, five percent or greater stockholders, and their respective affiliated entities in the aggregate own approximately 44.1% of our outstanding common stock (including restricted stock awards held by them, but excluding stock options). As a result, these stockholders, who are entitled to vote their shares in their own interests, acting together, exert a significant degree of influence over our management and affairs and over matters requiring stockholder approval, including the election of directors and approval of significant corporate transactions. This concentration of ownership may have the effect of delaying or preventing a change of control, merger, consolidation, sale of all or substantially all of our assets or other corporate transactions that other stockholders may view as beneficial, or conversely, this concentrated control could result in the consummation of a transaction that other stockholders may not support. This may harm the value of our shares and discourage investors from investing in us.
Provisions under Delaware law and Astrana’s charter and bylaws could deter takeover attempts or attempts to remove its board members or management that might otherwise be beneficial to its stockholders.
Astrana is subject to Section 203 of the Delaware General Corporation Law, which generally provides that a corporation may not engage in any business combination with any interested stockholder during the three-year period following the time that such stockholder becomes an interested stockholder unless certain approval requirements are met. This provision, and others that could be adopted in the future, could make the acquisition of Astrana and the removal of its incumbent officers and directors more difficult for potential acquirers, deter unsolicited takeovers or delay or prevent changes in Astrana’s control or management, including transactions in which Astrana’s stockholders might otherwise receive a premium for their shares over then current market prices. These provisions may also limit the ability of Astrana’s stockholders to approve transactions that they may deem to be in their best interests.
Additionally, Astrana’s charter and bylaws contain additional provisions, such as the authorization for its board of directors to issue one or more classes of preferred stock and determine the rights, preferences, and privileges of the preferred stock, which could cause substantial dilution to a person or group that attempts to acquire Astrana on terms not approved by the board, and the ownership requirement for Astrana’s stockholders to call special meetings, that could deter, discourage, or make it more difficult for a change in control of Astrana or for a third party to acquire Astrana, even if such a change in control could be deemed in the interest of Astrana’s stockholders, or if such an acquisition would provide Astrana’s stockholders with a substantial premium for their shares over the market price of Astrana’s common stock.
As such, these provisions could discourage a potential acquirer from acquiring us or otherwise attempting to obtain control of us and increase the likelihood that our incumbent directors and officers will retain their positions.
We may issue additional equity securities in the future, which may result in dilution to existing investors.
46
If Astrana issues additional equity securities, its existing stockholders may experience substantial dilution. Astrana may sell equity securities and may issue securities convertible into or exercisable for common stock in one or more transactions at prices and manners as we may determine from time to time, including at prices (or conversion or exercise prices) below the market price of Astrana’s common stock, for capital-raising purposes, including in any debt financing, registered offering, or private placement, and new investors could have superior rights such as liquidation and other preferences. To attract and retain the right talent, Astrana also issues equity awards under its equity compensation plans to its officers, other employees, directors, and consultants from time to time. Astrana may also issue additional shares of its common stock or other securities that are convertible into or exercisable for common stock in connection with future acquisitions or for other business purposes. In addition, the exercise or conversion of outstanding options or warrants to purchase shares of Astrana’s stock may result in dilution to its existing stockholders upon any such exercise or conversion.
Item 1B. Unresolved Staff Comments
None.
Item 1C. Cybersecurity
Astrana, like the rest of the healthcare industry, continues to innovate and rely on digital technology, further increasing the importance of cybersecurity to the business. The world is seeing an increase in cyberattacks by nation-states, hacktivists, organized cybercriminal groups, and insider threat actors, all of which may, among other avenues of attack, be using artificial intelligence (“AI”) and distributed hosted environments across different geographies to attack their victims. These threat actors may be individuals or part of a cyber organized crime group that leverages large-scale Cybercrime-as-a-Service (“CaaS”) subscriptions to quickly scale the impact of attacks and avoid disruption to their operations.
The Company’s digital systems are distributed across various architectures, including on-premises, hosted, Software-as-a-Service (“SaaS”), and other architectures operated by third-party service providers. If these architectures and third-party environments fail to operate as contracted, Astrana’s systems could stop functioning for some time, placing Astrana’s strategy, data, clients, and users at risk.
As noted in Item 1 and Item 1A of Part I of this report, a breach of Astrana’s network, hosted service providers, or vendor systems may expose Astrana to a risk of loss or misuse of information, litigation, and potential liability. Therefore, the Company has a team of experienced professionals with expertise in cybersecurity leadership, risk management, incident response, and security operations overseeing Astrana’s program. This team is responsible for developing and implementing our cybersecurity strategy, identifying and mitigating risks, and responding to incidents. Astrana utilizes external resources from reputable cybersecurity firms to supplement certain Chief Information Security Officer (“CISO”) functions, including risk assessments, strategy, and security, while integrating these activities with Astrana’s risk management processes. Astrana assesses third-party cybersecurity controls through cybersecurity questionnaires and includes security and privacy addendums to our contracts, where applicable.
To address cybersecurity, privacy, and overall business risk adequately, Astrana employs a consistent risk management process that assigns risks to functional owners. Risks can be strategic (e.g., loss of market share, technology shifts), reputational (e.g., loss of trust, revenue decline), regulatory (e.g., regulatory fines, business restrictions), or operational (e.g., operational downtime, productivity loss) in nature.
The cybersecurity team collaborates with leaders in management to assess materiality, align on a remediation roadmap, and comply with disclosure requirements. On an ongoing basis, the board of directors and the audit committee oversee Astrana’s cybersecurity risks and remediation strategies to prevent and mitigate cyberattacks.
As of the date of this report, the Company is not aware of any risks from cybersecurity threats that have materially affected or are reasonably likely to materially affect the Company, including its business strategy, results of operations, or financial condition.
47
Item 2. Properties
Our corporate headquarters are located in Alhambra, California, where we lease approximately 35,000 square feet of office space in two adjacent buildings from a related party. We also lease approximately 47,500 square feet of office space in Monterey Park, California, from a related party.
We lease other offices and medical spaces located in Los Angeles, Riverside, and San Mateo County in California. We also maintain offices and medical spaces in Nevada, Texas and New York. Monthly rental payments range from approximately $1,000 to $42,000 and have terms that expire between January 2024 and, subject to options to extend provided thereunder, January 2041.
We believe our existing facilities are in good condition and are suitable and adequate for our current requirements. Based on current information and subject to future events and circumstances, we anticipate that we may extend leases on our various facilities as necessary, as they expire, and lease additional facilities to accommodate possible future growth.
Item 3. Legal Proceedings
We are, from time to time, party to lawsuits, threatened lawsuits, disputes and other claims arising in the normal course of business. We assess our liabilities and contingencies in connection with outstanding legal proceedings utilizing the latest information available. Where it is probable that we will incur a loss and the amount of the loss can be reasonably estimated, we record a liability in our consolidated financial statements. These legal accruals may be increased or decreased to reflect any relevant developments on a quarterly basis. Where a loss is not probable or the amount of the loss is not estimable, we do not record an accrual, consistent with applicable accounting guidance. In the opinion of management, while the outcome of such claims and disputes cannot be predicted with certainty, our ultimate liability in connection with these matters is not expected to have a material adverse effect on our results of operations, financial position or cash flows, and the amounts accrued for any individual matter are not material. However, legal proceedings are inherently uncertain. As a result, the outcome of a particular matter or a combination of matters may be material to our results of operations for a particular period, depending upon the size of the loss or our income for that particular period.
Certain of the pending or threatened legal proceedings or claims in which we are involved are discussed under Note 14 - “Commitments and Contingencies,” to our consolidated financial statements in this Annual Report on Form 10-K, which disclosure is incorporated by reference herein.
Item 4. Mine Safety Disclosures
Not applicable.
48
PART II
Item 5. Market for Registrant’s Common Equity, Related Stockholder Matters, and Issuer Purchases of Equity Securities
Market Information
Astrana’s common stock is listed on Nasdaq under the symbol “ASTH.” Prior to the Company’s rebranding in February 2024, the Company’s common stock was listed on Nasdaq under the symbol “AMEH.”
Record Holders
As of February 22, 2024, there were approximately 599 holders of record of Astrana’s common stock based on our transfer agent’s report. Because many shares of Astrana’s common stock are held by brokers and other nominees on behalf of stockholders, including in trust, we are unable to estimate the total number of stockholders represented by these record-holders.
Dividends
To date, we have not paid any cash dividends on Astrana’s common stock, and we do not contemplate the payment of cash dividends thereon in the foreseeable future. Our future dividend policy will depend on our earnings, capital requirements, financial condition, and other factors relevant to our ability to pay dividends, including any contractual restrictions contained in our Amended Credit Agreement.
Recent Sales of Unregistered Securities
None.
Purchases of Equity Securities by the Issuer and Affiliated Purchasers
During the three months ended December 31, 2023, no shares were repurchased under the Company’s share repurchase plan. In December 2022, Astrana’s Board of Directors approved a share repurchase plan authorizing the Company to repurchase up to $50.0 million of its shares of common stock on the open market and through privately negotiated transactions. This share repurchase plan does not have an expiration date. The Board may suspend or discontinue the repurchase program at any time. This repurchase program does not obligate the Company to make additional repurchases at any specific time or in any specific situation. As of December 31, 2023, $40.5 million remained available for repurchase under the repurchase plan.
The following table provides information about purchases made by the Company of shares of the Company's common stock during the three months ended December 31, 2023.
| Period |
Total Number of Shares Purchased (1)
|
Average Price Paid per Share | Total Number of Shares Purchased as Part of Publicly Announced Plans or Programs | Approximate Dollar Value of Shares that May Yet be Purchased Under the Program (in thousands) |
||||||||||||||||||||||
| October 1- October 31 | 1,375 | $ | 32.20 | — | $ | 40,461 | ||||||||||||||||||||
| November 1 - November 30 | 3,170,770 | (2) |
$ | 31.58 | — | $ | 40,461 | |||||||||||||||||||
| December 1 - December 31 | 15,993 | (3) |
$ | 33.51 | — | $ | 40,461 | |||||||||||||||||||
| Total | 3,188,138 | $ | 33.51 | — | $ | 40,461 | ||||||||||||||||||||
(1) Includes shares repurchased to satisfy tax withholding obligations due upon the vesting of restricted stock held by certain employees. We did not pay cash to repurchase these shares, nor were these repurchases part of a publicly announced plan or program.
49
(2) Includes 3,166,561 shares of common stock repurchased from APC on November 14, 2023, pursuant to a stock repurchase agreement with APC entered into on November 6, 2023. The Company’s Board of Directors and the Audit Committee of the Board of Directors approved the repurchase.
(3) Includes 15,000 shares of common stock repurchased from two members of the Board of Directors on December 6, 2023.
Performance Measurement Comparison
The following chart compares the cumulative total return of our common stock with the cumulative total return of the Russell 3000 Index and the S&P 500 Healthcare Index from December 31, 2018 to December 31, 2023. The annual changes for the five-year period shown in the graph are based on the assumption that $100 was invested in our common stock and each index on December 31, 2018, and that all dividends were reinvested. The stock price performance included in the line graph below is not necessarily indicative of future stock price performance.
We believe the Russell 3000 Index is an appropriate independent broad market index because it measures the performance of similar-sized companies in numerous sectors. In addition, we believe the S&P 500 Health Care Index is an appropriate third-party published industry index because it measures the performance of healthcare companies.
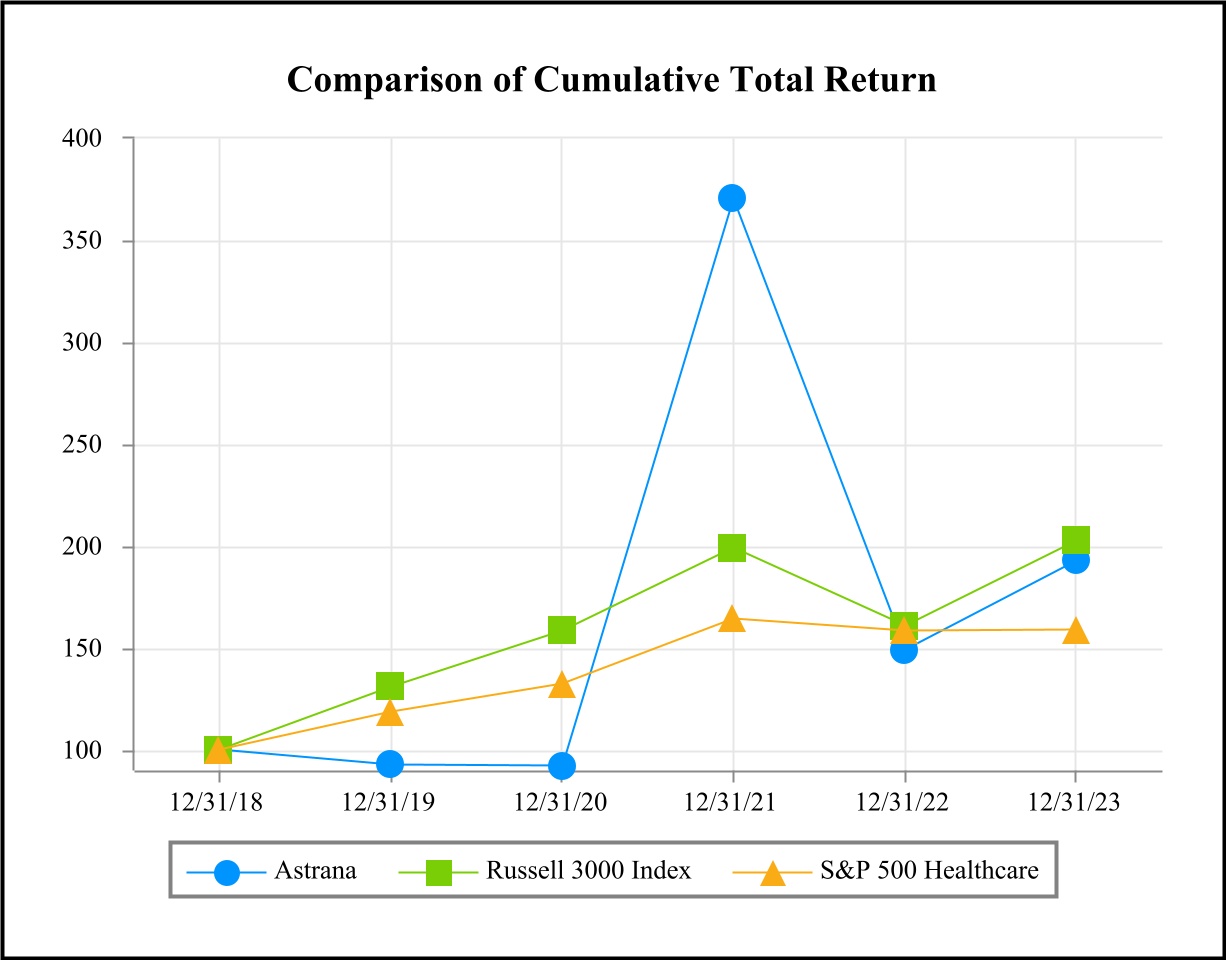
| Indexed Returns for the Years Ended | ||||||||||||||||||||||||||||||||||||||
| Company/Index |
Base Period
12/31/2018
|
12/31/2019 | 12/31/2020 | 12/31/2021 | 12/31/2022 | 12/31/2023 | ||||||||||||||||||||||||||||||||
| Astrana | $ | 100.00 | $ | 92.75 | $ | 92.04 | $ | 370.18 | $ | 149.07 | $ | 192.95 | ||||||||||||||||||||||||||
| Russell 3000 Index | 100.00 | 131.02 | 158.39 | 199.03 | 160.80 | 202.54 | ||||||||||||||||||||||||||||||||
| S&P 500 Healthcare | 100.00 | 118.68 | 132.24 | 164.20 | 158.37 | 158.85 | ||||||||||||||||||||||||||||||||
50
Item 6. [Reserved]
Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations
The following management’s discussion and analysis should be read in conjunction with the audited consolidated financial statements and the notes thereto included in Part II, Item 8, “Financial Statements and Supplementary Data” of this Annual Report on Form 10-K.
In this section, “we,” “our,” “ours,” and “us” refer to Astrana Health, Inc. (“Astrana”) and its consolidated subsidiaries and affiliated entities, as appropriate, including its consolidated variable interest entities (“VIEs”).
Overview
Astrana Health, Inc. is a leading physician-centric, technology-powered, risk-bearing healthcare management company. Leveraging its proprietary population health management and healthcare delivery platform, Astrana operates an integrated, value-based healthcare model, which aims to empower the providers in its network to deliver the highest quality of care to its patients in a cost-effective manner. We, together with our affiliated physician groups and consolidated entities, provide coordinated outcomes-based medical care in a cost-effective manner.
Through our accountable care organization and our network of IPAs we were responsible for coordinating the care for approximately 0.9 million patients, primarily in California, as of December 31, 2023. These covered patients are comprised of managed care members whose health coverage is provided either through their employers, acquired directly from a health plan, or as a result of their eligibility for Medicaid or Medicare benefits. Our managed patients benefit from an integrated approach that places physicians at the center of patient care and utilizes sophisticated risk management techniques and clinical protocols to provide high-quality, cost-effective care.
2023 Highlights
Company’s Credit Facility Increased to $700.0 million
On November 3, 2023, the Company entered into a Third Amendment to the Amended Credit Agreement (as amended, the “Amended Credit Agreement”) with the banks and other financial institutions party thereto and Truist Bank, as administrative agent, which provided a term loan to the Company in an aggregate amount of up to $300.0 million. This increased the Company’s facility (the “Amended Credit Facility”) to $700.0 million with our existing $400.0 million revolver.
Distribution of APC Excluded Assets
On December 26, 2023, APC completed a restructuring transaction to spin-off its real estate investments, a component of Excluded Assets (“the Spin-Off”). To effect the restructuring, APC contributed its real estate investments to a wholly owned subsidiary in exchange for 100% of the subsidiary’s membership interest units, which membership interests were then distributed to holders of APC’s outstanding common stock as a dividend, with each such stockholder receiving one membership interest unit for each share of outstanding APC common stock held. As a result of the distribution, the real estate investments are no longer included within our consolidated financial statements after December 26, 2023.
In connection with the restructuring, APC amended certain provisions of the Certificate of Determination of Preferences of Series A Preferred Stock relating to dividend restrictions and liquidation rights. Astrana Medical, a consolidated VIE of Astrana holds all of APC’s outstanding Series A Preferred Stock.
Share Repurchase
On November 6, 2023, the Company entered into a stock repurchase agreement with APC to repurchase approximately $100.0 million, or 3,166,561 shares, of the Company’s common stock from APC. The Company repurchased the shares on November 14, 2023. The Company financed the share repurchase with borrowings under its Amended and Restated Credit Agreement.
Business and Asset Acquisitions and Partnerships
Texas Independent Providers, LLC
51
On September 1, 2023, the Company acquired certain assets relating to Texas Independent Providers, LLC (“TIP”). The acquired assets allow the Company to provide high-quality care services to Medicare Advantage patients in Texas. The purchase price consisted of cash funded on September 1, 2023.
IntraCare
In July 27, 2023, the Company announced an agreement to partner with IntraCare, an operator of a value-based primary care provider network and primary care clinics located predominantly in Texas with a growing presence in Oklahoma. On July 27, 2023, the Company entered into a 5-year convertible promissory note with IntraCare as the borrower. The principal on the note is $25.0 million with interest on the outstanding principal amount and unpaid interest at a rate per annum equal to 8.81%, compounded annually.
FYB
On May 1, 2023, the Company acquired 100% of the equity interest in FYB. FYB is licensed by the California Department of Managed Health Care as a full-service Restricted Knox-Keene licensed health plan, which enables FYB to assume full financial responsibility, including both professional and institutional risk, for the medical costs of its members under the Knox-Keene Health Care Service Plan Act of 1975.
Chinese Community Health Care Association (“CCHCA”)
On March 1, 2023, the Company acquired certain healthcare assets from CCHCA. The acquired assets allow the Company to provide high-quality care to more patients in the San Francisco Community. The purchase price consisted of cash funded on May 1, 2023.
Recent Developments
Corporate Name Change
Effective February 26, 2024, the Company changed its name to Astrana Health, Inc.. Alongside the corporate name change, the Company's common stock is trading under the new symbol "ASTH" on Nasdaq.
Closing of Acquiring Community Family Care Medical Group IPA, Inc. Assets
In November 2023, the Company entered into an Asset and Equity Purchase Agreement (the “Purchase Agreement”) to acquire the partnership interests of Advanced Health Management Systems, L.P. (“AHMS”) and certain assets of Community Family Care Medical Group IPA, Inc. (“CFC”), which acquisitions the Company expected would occur in two separate closings. In November 2023, AHM also entered into a Stock Purchase Agreement (the “I Health Purchase Agreement”) to purchase 25% of the outstanding shares of common stock of I Health, Inc. (“I Health”). On January 31, 2024, the first closing under the Purchase Agreement occurred, and the Company completed its acquisition of CFC’s assets. CFC IPA manages the healthcare of over 200,000 members in the Los Angeles, California area, serving patients across Medicare, Medicaid, and Commercial payers. The Company expects to complete the second closing under the Purchase Agreement and acquire the outstanding general and limited partnership interests of AHMS during the first quarter of 2024, subject to obtaining required regulatory approvals. It is currently expected that the I Health Purchase Agreement closing will occur during the first quarter of 2024.
BASS Medical Group
On January 29, 2024, the Company announced its strategic long-term partnership with BASS Medical Group, one of the largest multi-specialty medical groups in the Greater San Francisco Bay Area. Together, the two organizations will aim to bring high-quality care via value-based arrangements to patients of all insurance types, including Medicare, Medicaid, ACA Marketplace, and Commercial. Astrana has provided BASS Medical Group with a $20 million senior secured promissory note (“BASS secured promissory note”), which is intended to be used, in partnership with Astrana, to continue to grow their footprint and invest in high-quality, high-value, and accessible primary and multi-specialty care for communities across California. The BASS secured promissory note matures on January 11, 2031 and has an interest rate per annum equal to 2.9% plus the Secured Overnight Financing Rate as administered by the Federal Reserve Bank of New York (or a successor administrator) compounded annually.
52
Leadership Transitions
On January 24, 2024, the Company announced the following executive appointments effective January 19, 2024:
•Thomas S. Lam, M.D., M.P.H., previously Co-Chief Executive Officer and President and a director, was appointed Vice Chairman of the Board;
•Brandon K. Sim, M.S., previously Co-Chief Executive Officer, was appointed Chief Executive Officer and President; and
•Chandan Basho, previously Chief Financial Officer and Chief Strategy Officer, was appointed Chief Financial Officer and Chief Operating Officer.
In addition, Dinesh Kumar, M.D., was appointed Chief Medical Officer effective January 23, 2024.
Employee Stock Purchase Plan (“ESPP”)
On January 1, 2024, the Company’s ESPP came into effect. The Company’s ESPP allows eligible employees to contribute a portion of their eligible earnings toward the semi-annual purchase of the Company’s common stock at a discounted price, subject to an annual maximum dollar amount.
Medicare Shared Savings Program (“MSSP”)
On January 1, 2024, in addition to participating in the ACO REACH Model, one of our other ACOs will participate in the Medicare Shared Savings Program (“MSSP”). The MSSP was created to promote accountability and improve coordination of care for Medicare beneficiaries. Unlike the ACO REACH Program, CMS continues to pay participant and preferred providers on a fee-for-service basis for Medicare-covered services provided to MSSP Aligned Beneficiaries. Our shared savings or losses in managing our beneficiaries are generally determined on an annual basis after reconciliation with CMS.
Key Financial Measures and Indicators
Operating Revenues
Our revenue, which is recorded in the period in which services are rendered and earned, primarily consists of capitation revenue, risk pool settlements and incentives, ACO REACH capitation revenue, management fee income, and fee-for-services (“FFS”) revenue. The form of billing and related risk of collection for such services may vary by type of revenue and the customer.
Operating Expenses
Our largest expenses consist of the cost of: (i) patient care paid to contracted providers; (ii) information technology equipment and software; and (iii) hiring staff to provide management and administrative support services to our affiliated physician groups, as further described in the following sections. These services include claims processing, utilization management, contracting, accounting, credentialing, and administrative oversight.
Adjusted EBITDA and Adjusted EBITDA Margin
Our Adjusted EBITDA and Adjusted EBITDA margin are supplemental performance measures of our operations for financial and operational decision-making, and as a supplemental means of evaluating period-to-period comparisons on a consistent basis. Adjusted EBITDA is calculated as earnings before interest, taxes, depreciation, and amortization, excluding income or loss from equity method investments, non-recurring and non-cash transactions, stock-based compensation, and APC excluded assets costs. The Company defines Adjusted EBITDA margin as Adjusted EBITDA over total revenue.
53
Results of Operations
2023 Compared to 2022
Our consolidated operating results for the year ended December 31, 2023, as compared to the year ended December 31, 2022 were as follows:
Astrana Health, Inc.
Consolidated Statements of Income (in thousands)
| Years Ended December 31, | |||||||||||||||||||||||
| 2023 | 2022 | $ Change | % Change | ||||||||||||||||||||
| Revenue | |||||||||||||||||||||||
| Capitation, net | $ | 1,215,614 | $ | 930,131 | $ | 285,483 | 31 | % | |||||||||||||||
| Risk pool settlements and incentives | 63,468 | 117,254 | (53,786) | (46) | % | ||||||||||||||||||
| Management fee income | 38,677 | 41,094 | (2,417) | (6) | % | ||||||||||||||||||
| Fee-for-service, net | 59,658 | 49,517 | 10,141 | 20 | % | ||||||||||||||||||
| Other revenue | 9,244 | 6,167 | 3,077 | 50 | % | ||||||||||||||||||
| Total revenue | 1,386,661 | 1,144,163 | 242,498 | 21 | % | ||||||||||||||||||
| Operating expenses | |||||||||||||||||||||||
| Cost of services, excluding depreciation and amortization | 1,171,703 | 944,685 | 227,018 | 24 | % | ||||||||||||||||||
| General and administrative expenses | 112,597 | 77,670 | 34,927 | 45 | % | ||||||||||||||||||
| Depreciation and amortization | 17,748 | 17,543 | 205 | 1 | % | ||||||||||||||||||
| Total expenses | 1,302,048 | 1,039,898 | 262,150 | 25 | % | ||||||||||||||||||
| Income from operations | 84,613 | 104,265 | (19,652) | (19) | % | ||||||||||||||||||
Other income (expense) |
|||||||||||||||||||||||
Income from equity method investments |
5,579 | 5,622 | (43) | (1) | % | ||||||||||||||||||
| Interest expense | (16,102) | (7,920) | (8,182) | 103 | % | ||||||||||||||||||
| Interest income | 14,208 | 1,976 | 12,232 | * | |||||||||||||||||||
| Unrealized loss on investments | (4,581) | (21,271) | 16,690 | (78) | % | ||||||||||||||||||
Other income |
6,121 | 3,944 | 2,177 | 55 | % | ||||||||||||||||||
Total other income (expense), net |
5,225 | (17,649) | 22,874 | (130) | % | ||||||||||||||||||
| Income before provision for income taxes | 89,838 | 86,616 | 3,222 | 4 | % | ||||||||||||||||||
| Provision for income taxes | 31,989 | 40,875 | (8,886) | (22) | % | ||||||||||||||||||
| Net income | $ | 57,849 | $ | 45,741 | $ | 12,108 | 26 | % | |||||||||||||||
| Net (loss) income attributable to noncontrolling interests | (2,868) | 570 | (3,438) | * | |||||||||||||||||||
Net income attributable to Astrana Health, Inc. |
$ | 60,717 | $ | 45,171 | $ | 15,546 | 34 | % | |||||||||||||||
* Percentage change of over 500%
Physician Groups and Patients
As of December 31, 2023 and 2022, the total number of affiliated physician groups we managed were 15 groups and 14 groups, respectively, and the total number of patients for whom we managed the delivery of healthcare services was approximately 0.9 million and 1.3 million, respectively. The decrease in membership is primarily due to an IPA ending its MSA with the Company. This was partially offset by managing 2 new physician groups in 2023.
Revenue
54
Our total revenue in 2023 was $1,386.7 million, as compared to $1,144.2 million in 2022, an increase of $242.5 million or 21%. The increase in total revenue was primarily attributable to the following:
(i) An overall increase of $285.5 million in capitation revenue primarily driven by membership growth in our ACO participating in a value-based Medicare FFS model and our acquisition of a Restricted Knox-Keene licensed health plan in 2023.
(ii) An overall decrease of $53.8 million in risk pool settlements and incentive revenue due to the Company recognizing the shared savings from the NGACO program in 2022 for the 2021 performance year. With the end of the NGACO program ending on December 31, 2021, the Company began participating in the ACO REACH model.
(iii) An increase of $10.1 million in FFS revenue attributable to fees generated from Astrana primary, multi-specialty, and ancillary care delivery entities and expanding our locations.
Cost of Services, Excluding Depreciation and Amortization
Expenses related to the cost of services, excluding depreciation and amortization, in 2023 were $1,171.7 million, as compared to $944.7 million in 2022, an increase of $227.0 million or 24%. The overall increase was primarily due to increased participation in a value-based Medicare FFS model, medical costs associated with both professional and institutional risk of our Restricted Knox-Keene licensed health plan, and increased patient visits, which were commensurate to our increase in revenue.
General and Administrative Expenses
General and administrative expenses in 2023 were $112.6 million, as compared to $77.7 million in 2022, an increase of $34.9 million or 45%. This increase was primarily due to an increase in headcount and personnel-related costs to support the continued growth in the depth and breadth of our operations and nonrecurring costs related to acquisitions, tax restructuring fees, and an excise tax related to the repurchase of the Company’s stock from APC.
Depreciation and Amortization
Depreciation and amortization expense were $17.7 million and $17.5 million for the years ended December 31, 2023 and 2022, respectively. This amount includes depreciation of property and equipment and the amortization of intangible assets.
Income From Equity Method Investments
Income from equity method investments in 2023 was $5.6 million, as compared to income of $5.6 million in 2022. This amount includes the Company’s portion of the equity method investment’s net earnings or losses.
Interest Expense
Interest expense in 2023 was $16.1 million, as compared to $7.9 million in 2022, an increase of $8.2 million. The increase in interest expense for the year was primarily due to higher interest rates and an increase in amounts borrowed under the Amended Credit Facility. On December 31, 2023, the outstanding principal and interest rate on the Amended Credit Agreement was $280.0 million and 7.69% compared to $180.0 million and 5.92% on December 31, 2022.
Interest Income
Interest income in 2023 was $14.2 million, as compared to $2.0 million in 2022, an increase of $12.2 million. The increase in interest income was due to more bank accounts becoming interest-bearing and interest income from the IntraCare convertible promissory note. On July 27, 2023, the Company entered into a 5-year convertible promissory note with IntraCare as the borrower. The principal on the note is $25.0 million with interest on the outstanding principal amount and unpaid interest at a rate per annum equal to 8.81%, compounded annually.
Unrealized Loss on Investments
Unrealized loss on investments in 2023 was $4.6 million, as compared to an unrealized loss on investments of $21.3 million in 2022, a decrease of $16.7 million. The decrease in unrealized loss on investments was primarily driven by a $21.2 million decrease as a result of APC selling all of its equity securities in a payer partner and the change in the share price of our
55
remaining equity securities held. This was offset by a $4.3 million increase in unrealized loss as a result of the change in the fair value of our interest rate swaps and collar arrangements.
Other Income
Other income in 2023 was $6.1 million, as compared to other income of $3.9 million in 2022, an increase of $2.2 million primarily due to an increase in rental income.
Provision for Income Taxes
Provision for income taxes was $32.0 million in 2023, as compared to $40.9 million in 2022, a decrease of $8.9 million or 22%. This was primarily attributable to changes to our tax structure resulting in a decreased tax rate.
Net (Loss) Income Attributable to Noncontrolling Interests
Net loss attributable to non-controlling interests was $2.9 million in 2023, as compared to net income of $0.6 million in 2022, a decrease of $3.4 million. The decrease was primarily attributable to more expenses incurred by APC’s Excluded Assets. Operations from Excluded Assets are for the benefit of APC and its common shareholders. As such, any income pertaining to APC’s interests in Excluded Assets do not affect net income attributable to Astrana.
Net Income Attributable to Astrana Health, Inc.
Net income attributable to Astrana Health, Inc. was $60.7 million in 2023, as compared to net income of $45.2 million in 2022, an increase of $15.5 million. The increase was primarily due to a decrease in the provision for income taxes and an increase in interest income.
56
2022 Compared to 2021
Our consolidated operating results for the year ended December 31, 2022, as compared to the year ended December 31, 2021, were as follows:
Astrana Health, Inc.
Consolidated Statements of Income (in thousands)
| Years Ended December 31, | |||||||||||||||||||||||
| 2022 | 2021 | $ Change | % Change | ||||||||||||||||||||
| Revenue | |||||||||||||||||||||||
| Capitation, net | $ | 930,131 | $ | 593,224 | $ | 336,907 | 57 | % | |||||||||||||||
| Risk pool settlements and incentives | 117,254 | 111,627 | 5,627 | 5 | % | ||||||||||||||||||
| Management fee income | 41,094 | 35,959 | 5,135 | 14 | % | ||||||||||||||||||
Fee-for-service, net |
49,517 | 26,564 | 22,953 | 86 | % | ||||||||||||||||||
Other revenue |
6,167 | 6,541 | (374) | (6) | % | ||||||||||||||||||
| Total revenue | 1,144,163 | 773,915 | 370,248 | 48 | % | ||||||||||||||||||
| Operating expenses | |||||||||||||||||||||||
| Cost of services, excluding depreciation and amortization | 944,685 | 596,142 | 348,543 | 58 | % | ||||||||||||||||||
| General and administrative expenses | 77,670 | 62,077 | 15,593 | 25 | % | ||||||||||||||||||
| Depreciation and amortization | 17,543 | 17,517 | 26 | 0 | % | ||||||||||||||||||
| Total expenses | 1,039,898 | 675,736 | 364,162 | 54 | % | ||||||||||||||||||
| Income from operations | 104,265 | 98,179 | 6,086 | 6 | % | ||||||||||||||||||
| Other income (expense) | |||||||||||||||||||||||
Income (loss) from equity method investments |
5,622 | (4,306) | 9,928 | (231) | % | ||||||||||||||||||
| Gain on sale of equity method investment | — | 2,193 | (2,193) | (100) | % | ||||||||||||||||||
| Interest expense | (7,920) | (5,394) | (2,526) | 47 | % | ||||||||||||||||||
| Interest income | 1,976 | 1,571 | 405 | 26 | % | ||||||||||||||||||
| Unrealized loss on investments | (21,271) | (10,745) | (10,526) | 98 | % | ||||||||||||||||||
Other income (expense) |
3,944 | (3,750) | 7,694 | (205) | % | ||||||||||||||||||
Total other expense, net |
(17,649) | (20,431) | 2,782 | (14) | % | ||||||||||||||||||
| Income before provision for income taxes | 86,616 | 77,748 | 8,868 | 11 | % | ||||||||||||||||||
| Provision for income taxes | 40,875 | 31,693 | 9,182 | 29 | % | ||||||||||||||||||
| Net income | $ | 45,741 | $ | 46,055 | $ | (314) | (1) | % | |||||||||||||||
Net income (loss) attributable to noncontrolling interests |
570 | (22,868) | 23,438 | (102) | % | ||||||||||||||||||
Net income attributable to Astrana Health, Inc. |
$ | 45,171 | $ | 68,923 | $ | (23,752) | (34) | % | |||||||||||||||
Physician Groups and Patients
As of December 31, 2022 and 2021, the total number of affiliated physician groups we managed were 14 groups and 12 groups, respectively, and the total number of patients for whom we managed the delivery of healthcare services was approximately 1.3 million and 1.2 million, respectively.
Revenue
Our total revenue in 2022 was $1,144.2 million, as compared to $773.9 million in 2021, an increase of $370.2 million or 48%. The increase in total revenue was primarily attributable to the following:
(i) An overall increase of $336.9 million in capitation revenue primarily driven by organic membership growth in our core IPAs and participation in a value-based Medicare FFS model.
57
(ii) An increase of $23.0 million in FFS revenue attributable to fees generated from Astrana primary, multi-specialty, and ancillary care delivery entities.
Cost of Services, Excluding Depreciation and Amortization
Expenses related to the cost of services, excluding depreciation and amortization, in 2022 were $944.7 million, as compared to $596.1 million in 2021, an increase of $348.5 million or 58%. The overall increase was primarily due to the expected return to pre-COVID-19 medical expense run rates, participation in a value-based Medicare FFS model and growth in membership, which was commensurate to our increase in revenue.
General and Administrative Expenses
General and administrative expenses in 2022 were $77.7 million, as compared to $62.1 million in 2021, an increase of $15.6 million or 25%. This increase was primarily due to a $14.8 million increase in personnel-related costs to support the continued growth in the depth and breadth of our operations.
Depreciation and Amortization
Depreciation and amortization expense were $17.5 million and $17.5 million for the years ended December 31, 2022 and 2021, respectively. These amounts included depreciation of property and equipment and the amortization of intangible assets.
Income (Loss) From Equity Method Investments
Income from equity method investments in 2022 was $5.6 million, as compared to a loss of $4.3 million in 2021, an increase of $9.9 million. The increase in income from equity method investments was primarily due to our investment partner having a favorable contract change, including rate and division of financial responsibility on certain claims.
Gain on Sale of Equity Method Investment
Gain on sale of equity method investment in 2022 was $0, as compared to $2.2 million in 2021, a decrease of $2.2 million. The decrease in gain on the sale of equity method investment is due to APC selling 21.25% of its interest in one if its equity method investments back to Dr. Arteaga for the year ended December 31, 2021. There was no sale of our equity method investment for the year ended December 31, 2022.
Interest Expense
Interest expense in 2022 was $7.9 million, as compared to $5.4 million in 2021, an increase of $2.5 million. The increase in interest expense for the year was primarily due to higher interest rates. On December 31, 2022, the interest rate on the Amended Credit Agreement was 5.92% compared to 1.71% on December 31, 2021.
Interest Income
Interest income in 2022 was $2.0 million, as compared to $1.6 million in 2021, an increase of $0.4 million. Interest income reflects interest earned on cash held in money market and certificate of deposit accounts and the interest from notes receivable.
Unrealized Loss on Investments
Unrealized loss on investments in 2022 was $21.3 million, as compared to an unrealized loss on investments of $10.7 million in 2021, an increase of $10.5 million. The increase in unrealized loss on investments was primarily driven by a decrease in the stock price of a payer partner in which we hold shares and Nutex.
Other Income (Expense)
Other income in 2022 was $3.9 million, as compared to other expenses of $3.8 million in 2021, an increase of $7.7 million. The increase was primarily due to the write-off of certain beneficial interest related to the disposition of ownership
58
interest in one of APC’s equity method investments totaling $15.7 million for the year ended December 31, 2021. The beneficial interest was an Excluded Assets that was deemed solely for the benefit of APC and its common shareholders. As such, the write-off did not result in any impact on net income attributable to Astrana Health, Inc. This was partially offset by non-recurring income recognized for the year ended December 31, 2021 relating to $2.8 million income from consolidating an equity method investment, $5.3 million income from the stock purchase agreement with Nutex, and $1.7 million income in stimulus checks. In addition, the Company recognized a $2.3 million gain on sale of equity securities for the year ended December 31, 2022.
Provision for Income Taxes
Provision for income taxes was $40.9 million in 2022, as compared to $31.7 million in 2021, an increase of $9.2 million or 29%. This was primarily attributable to an increase in pre-tax income in 2022, as compared to 2021, due to the factors described above.
Net Income (Loss) Attributable to Noncontrolling Interests
Net income attributable to non-controlling interests was $0.6 million in 2022, as compared to a net loss of $22.9 million in 2021, an increase of $23.4 million. The increase in net income attributable to noncontrolling interest was primarily due to non-recurring write-offs recognized for the year ended December 31, 2021 related to certain beneficial interest totaling $15.7 million.
Segment Financial Performance
Beginning in the first quarter of 2023, the Company began providing reporting for three reportable segments consisting of Care Partners, Care Delivery and Care Enablement. The Company evaluates the performance of its operating segments based on segment revenue growth as well as operating income. Management uses revenue growth and total segment operating income as a measure of the performance of operating businesses separate from non-operating factors. For more information about our segments, refer to Note 1 — “Description of Business” and Note 20 - “Segments” to our consolidated financial statements under Item 8 in this Annual Report on Form 10-K for additional information.
2023 Segments Compared to 2022 Segments
The following table sets forth our revenue and operating income by segment for the year ended December 31, 2023, as compared to the year ended December 31, 2022:
| Years Ended December 31, | |||||||||||||||||||||||
| Segment Revenue (in thousands) | 2023 | 2022 | $ Change |
% Change | |||||||||||||||||||
| Care Partners | $ | 1,300,112 | $ | 1,051,521 | $ | 248,591 | 24 | % | |||||||||||||||
| Care Delivery | $ | 119,904 | $ | 96,132 | $ | 23,772 | 25 | % | |||||||||||||||
| Care Enablement | $ | 135,824 | $ | 120,200 | $ | 15,624 | 13 | % | |||||||||||||||
| Years Ended December 31, | |||||||||||||||||||||||
Segment Operating Income (in thousands) |
2023 | 2022 | $ Change |
% Change | |||||||||||||||||||
| Care Partners | $ | 91,721 | $ | 85,222 | $ | 6,499 | 8 | % | |||||||||||||||
| Care Delivery | $ | 5,873 | $ | 8,971 | $ | (3,098) | (35) | % | |||||||||||||||
| Care Enablement | $ | 19,077 | $ | 27,041 | $ | (7,964) | (29) | % | |||||||||||||||
Care Partners Segment
Revenue was $1,300.1 million in 2023, as compared to $1,051.5 million in 2022, an increase of $248.6 million. Operating income was $91.7 million in 2023, as compared to $85.2 million in 2022, an increase of $6.5 million. The increase in revenue and operating income was primarily driven by membership growth in our ACO participating in a value-based Medicare FFS model and our acquisition of a Restricted Knox-Keene licensed health plan in 2023. The increase in revenue was partially
59
offset by a decrease in incentive revenue due to the Company recognizing the shared savings from the NGACO program in 2022 for the 2021 performance year.
Care Delivery Segment
Revenue was $119.9 million in 2023, as compared to $96.1 million in 2022, an increase of $23.8 million. Operating income was $5.9 million in 2023, as compared to income of $9.0 million in 2022, a decrease in operating income of $3.1 million. The increase in revenue was primarily due to more clinic locations opening during 2023 from our primary, multi-specialty, and ancillary care delivery entities. The decrease in operating income was due to more costs incurred for expanding to new locations.
Revenue was $119.9 million in 2023, as compared to $96.1 million in 2022, an increase of $23.8 million. Operating income was $5.9 million in 2023, as compared to income of $9.0 million in 2022, a decrease in operating income of $3.1 million. The increase in revenue was primarily due to more clinic locations opening during 2023 from our primary, multi-specialty, and ancillary care delivery entities. The decrease in operating income was due to more costs incurred for expanding to new locations.
Care Enablement Segment
Revenue was $135.8 million in 2023, as compared to $120.2 million in 2022, an increase of $15.6 million. Operating income was $19.1 million in 2023, as compared to $27.0 million in 2022, a decrease of $8.0 million. The increase in revenue was due to more managed independent physician groups. As of December 31, 2023 and 2022, the total number of affiliated physician groups we managed were 15 groups and 14 groups, respectively. The decrease in operating income was due to an increase in personnel-related costs to support the increase in our managed independent physician groups.
2022 Segments Compared to 2021 Segments
The following table sets forth our revenue and operating income by segment for the year ended December 31, 2022, as compared to the year ended December 31, 2021:
| Years Ended December 31, | |||||||||||||||||||||||
| Segment Revenue (in thousands) | 2022 | 2021 | $ Change | % Change | |||||||||||||||||||
| Care Partners | $ | 1,051,521 | $ | 709,714 | $ | 341,807 | 48 | % | |||||||||||||||
| Care Delivery | $ | 96,132 | $ | 46,691 | $ | 49,441 | 106 | % | |||||||||||||||
| Care Enablement | $ | 120,200 | $ | 107,693 | $ | 12,507 | 12 | % | |||||||||||||||
| Years Ended December 31, | |||||||||||||||||||||||
| Segment Operating Income (Loss) (in thousands) | 2022 | 2021 | $ Change | % Change | |||||||||||||||||||
| Care Partners | $ | 85,222 | $ | 72,578 | $ | 12,644 | 17 | % | |||||||||||||||
| Care Delivery | $ | 8,971 | $ | (540) | $ | 9,511 | * | ||||||||||||||||
| Care Enablement | $ | 27,041 | $ | 37,499 | $ | (10,458) | (28) | % | |||||||||||||||
* Percentage change of over 500%
Care Partners Segment
Revenue was $1,051.5 million in 2022, as compared to $709.7 million in 2021, an increase of $341.8 million. Operating income was $85.2 million in 2022, as compared to $72.6 million in 2021, an increase of $12.6 million. The increase in revenue and operating income was primarily driven by organic membership growth in our core IPAs and participation in a value-based Medicare FFS model.
Care Delivery Segment
Revenue was $96.1 million in 2022, as compared to $46.7 million in 2021, an increase of $49.4 million. Operating income was $9.0 million in 2022, as compared to a loss of $0.5 million in 2021, an increase of $9.5 million. The increase in revenue and operating income was primarily due to increased visits from our primary, multi-specialty, and ancillary care delivery entities.
Revenue was $96.1 million in 2022, as compared to $46.7 million in 2021, an increase of $49.4 million. Operating income was $9.0 million in 2022, as compared to a loss of $0.5 million in 2021, an increase of $9.5 million. The increase in revenue and operating income was primarily due to increased visits from our primary, multi-specialty, and ancillary care delivery entities.
60
Care Enablement Segment
Revenue was $120.2 million in 2022, as compared to $107.7 million in 2021, an increase of $12.5 million. Operating income was $27.0 million in 2022, as compared to $37.5 million in 2021, a decrease of $10.5 million. The increase in revenue was due to more managed independent physician groups. As of December 31, 2022 and 2021, the total number of affiliated physician groups we managed were 14 groups and 12 groups, respectively. The decrease in operating income was due to an increase in personnel-related costs to support the increase in our managed independent physician groups.
2024 Guidance
Astrana is providing the following guidance for total revenue, net income attributable to Astrana, Adjusted EBITDA, and EPS — diluted. These guidance assumptions are based on the Company's existing business, current view of existing market conditions and assumptions for the year ending December 31, 2024.
($ in millions, except per share amounts) |
2024 Guidance Range |
||||||||||
| Low | High | ||||||||||
| Total revenue | $ | 1,650.0 | $ | 1,850.0 | |||||||
Net income attributable to Astrana Health, Inc. |
$ | 61.0 | $ | 73.0 | |||||||
| Adjusted EBITDA | $ | 165.0 | $ | 185.0 | |||||||
| EPS – diluted | $ | 1.28 | $ | 1.52 | |||||||
See “Guidance Reconciliation of Net Income to EBITDA and Adjusted EBITDA” and “Use of Non-GAAP Financial Measures” below for additional information. There can be no assurance that actual amounts will not be materially higher or lower than these expectations. See “Note About Forward-Looking Statements” above for additional information.
| Guidance Reconciliation of Net Income to EBITDA and Adjusted EBITDA | ||||||||||||||
| (in thousands) | 2024 Guidance Range | |||||||||||||
| Low | High | |||||||||||||
| Net income | $ | 71,500 | $ | 85,500 | ||||||||||
Interest expense, net |
14,500 | 12,500 | ||||||||||||
| Provision for income taxes | 36,500 | 44,500 | ||||||||||||
| Depreciation and amortization | 14,500 | 14,500 | ||||||||||||
| EBITDA | 137,000 | 157,000 | ||||||||||||
Loss (income) from equity method investments |
(5,000) | (5,000) | ||||||||||||
| Other, net | 6,000 | 6,000 | ||||||||||||
| Stock-based compensation | 27,000 | 27,000 | ||||||||||||
| Adjusted EBITDA | $ | 165,000 | $ | 185,000 | ||||||||||
Set forth below are reconciliations of Net Income to EBITDA and Adjusted EBITDA for the years ended December 31, 2023 and 2022:
61
Reconciliation of Net Income to EBITDA, Adjusted EBITDA, and Adjusted EBITDA Margin(1)
|
||||||||||||||||||||
| Year Ended December 31, |
||||||||||||||||||||
| (in thousands) | 2023 | 2022 | ||||||||||||||||||
| Net income | $ | 57,849 | $ | 45,741 | ||||||||||||||||
| Interest expense | 16,102 | 7,920 | ||||||||||||||||||
| Interest income | (14,208) | (1,976) | ||||||||||||||||||
| Provision for income taxes | 31,989 | 40,875 | ||||||||||||||||||
| Depreciation and amortization | 17,748 | 17,543 | ||||||||||||||||||
| EBITDA | $ | 109,480 | $ | 110,103 | ||||||||||||||||
| Income from equity method investments | (5,149) | (5,680) | (2) |
|||||||||||||||||
| Other, net | 6,228 | (3) |
3,309 | (4) |
||||||||||||||||
| Stock-based compensation | 22,040 | 16,101 | ||||||||||||||||||
| APC excluded assets costs | 13,988 | 16,193 | (2) |
|||||||||||||||||
| Adjusted EBITDA | $ | 146,587 | $ | 140,026 | ||||||||||||||||
Total Revenue |
$ | 1,386,661 | $ | 1,144,163 | ||||||||||||||||
Adjusted EBITDA margin |
11 | % | 12 | % | ||||||||||||||||
(1) The Company defines Adjusted EBITDA margin as Adjusted EBITDA over total revenue.
(2) Certain APC minority interests where APC owns the asset but not the right to the dividends are reclassified from APC excluded asset costs to income from equity method investments.
(3) Other, net for the year ended December 31, 2023 consists of nonrecurring transaction costs and tax restructuring fees incurred, non-cash gains and losses related to the changes in the fair value of our financing obligation to purchase the remaining equity interests, contingent liabilities, and the Company's collar agreement relating to interest on the Revolver Loan, and excise tax related to a nonrecurring buyback of the Company’s stock from APC.
(4) Other, net for the year ended December 31, 2022 consists of one-time transaction costs incurred and non-cash gains and losses related to the changes in the fair value of our financing obligation to purchase the remaining equity interests and contingent considerations.
Use of Non-GAAP Financial Measures
This Annual Report on Form 10-K contains the non-GAAP financial measures EBITDA, Adjusted EBITDA, and Adjusted EBITDA margin, of which the most directly comparable financial measure presented in accordance with U.S. generally accepted accounting principles (“GAAP”) is net income. These measures are not in accordance with, or alternatives to GAAP, and may be calculated differently from similar non-GAAP financial measures used by other companies. The Company uses Adjusted EBITDA as a supplemental performance measure of our operations for financial and operational decision-making, and as a supplemental means of evaluating period-to-period comparisons on a consistent basis. Adjusted EBITDA is calculated as earnings before interest, taxes, depreciation, and amortization, excluding income or loss from equity method investments, non-recurring and non-cash transactions, stock-based compensation, and APC excluded assets costs. The Company defines Adjusted EBITDA margin as Adjusted EBITDA over total revenue.
The Company believes the presentation of these non-GAAP financial measures provides investors with relevant and useful information, as it allows investors to evaluate the operating performance of the business activities without having to account for differences recognized because of non-core or non-recurring financial information. When GAAP financial measures are viewed in conjunction with non-GAAP financial measures, investors are provided with a more meaningful understanding of the Company’s ongoing operating performance. In addition, these non-GAAP financial measures are among those indicators
62
the Company uses as a basis for evaluating operational performance, allocating resources, and planning and forecasting future periods. Non-GAAP financial measures are not intended to be considered in isolation, or as a substitute for, GAAP financial measures. Other companies may calculate both EBITDA and Adjusted EBITDA differently, limiting the usefulness of these measures for comparative purposes. To the extent this Form 10-K contains historical or future non-GAAP financial measures, the Company has provided corresponding GAAP financial measures for comparative purposes. The reconciliation between certain GAAP and non-GAAP measures is provided above.
Liquidity and Capital Resources
Cash, cash equivalents, and investments in marketable securities at December 31, 2023 totaled $296.3 million. Working capital totaled $242.8 million at December 31, 2023, compared to $279.5 million at December 31, 2022, a decrease of $36.7 million.
We have historically financed our operations primarily through internally generated funds. We generate cash primarily from capitation contracts, risk pool settlements and incentives, fees for medical management services provided to our affiliated physician groups, and FFS reimbursements. We generally invest cash in money market accounts, which are classified as cash and cash equivalents. We also have the Amended Credit Agreement, which provides for a five-year revolving credit facility of $400.0 million and a term loan of up to $300.0 million and expires in June 2026 and November 2028, respectively. In addition, we have a current shelf registration statement filed with the SEC under which we may issue common stock, preferred stock, debt securities and other securities that may be offered in one or more offerings on terms to be determined at the time of the offering. We believe we have sufficient liquidity to fund our operations through at least the next 12 months and the foreseeable future.
Cash Flow Activities
Our cash flows for the years ended December 31, 2023 and 2022 are summarized as follows (in thousands):
| Twelve Months Ended December 31, |
|||||||||||||||||||||||
| 2023 | 2022 | $ Change |
% Change | ||||||||||||||||||||
Net cash provided by operating activities |
$ | 68,227 | $ | 82,128 | $ | (13,901) | (17) | % | |||||||||||||||
| Net cash used in investing activities | (65,523) | (7,113) | (58,410) | * | |||||||||||||||||||
Net cash provided by (used in) financing activities |
3,421 | (20,085) | 23,506 | (117) | % | ||||||||||||||||||
Net increase in cash, cash equivalents, and restricted cash |
$ | 6,125 | $ | 54,930 | $ | (48,805) | (89) | % | |||||||||||||||
* Percentage change of over 500%
Our cash, cash equivalents, and restricted cash increased by $6.1 million from $288.0 million at December 31, 2022, to $294.2 million at December 31, 2023. Cash provided by operating activities during the year ended December 31, 2023 was $68.2 million, as compared to $82.1 million during the year ended December 31, 2022. The decrease in cash provided by operating activities was primarily driven by changes in net income and working capital. For the year ended December 31, 2023, net income exclusive of depreciation and amortization, amortization of debt issuance costs, share-based compensation, non-cash lease expense, income from equity method investments, gains or losses on investments and contingent liabilities, deferred tax, and gains or losses from distribution or consolidation of investments was $91.6 million compared to $84.1 million for the year ended December 31, 2022. Working capital for the year ended December 31, 2023, decreased operating cash flow by $23.4 million, compared to a $2.0 million increase in operating cash flow at December 31, 2022. The change in working capital for the year ended December 31, 2023, was mainly driven by an increase in our receivable, net, other receivable, prepaid and other current assets, and income tax receivable. These are due to the timing of when our receivables are collected and the timing of paying our income taxes. The decrease in working capital was partially offset by a decrease in our receivable, net — related parties and increase in our medical liabilities. The decrease in our receivable, net — related parties was attributable to cash received from our risk pool arrangements and the increase in our medical liabilities was attributable to the timing of claims paid and the Company’s participation in the value-based Medicare FFS model.
Cash used in investing activities during the year ended December 31, 2023, was $65.5 million, primarily due to purchases of property and equipment of $28.5 million, issuance of loans of $26.5 million, business acquisition, net of cash, of $6.5 million, purchase of investments in privately held entities for payments for $4.0 million, contributions to an equity method
63
investment of $0.7 million, and purchase of marketable securities of $2.2 million. The cash used in investing activities was partially offset by proceeds from repayment of a loan receivable of $2.7 million and proceeds from the sale of marketable securities of $0.5 million. Cash used in investing activities during the year ended December 31, 2022, was $7.1 million, primarily due to purchases of property and equipment of $22.9 million, payments for business acquisition, net of cash, of $16.4 million, purchase of marketable securities of $1.9 million, and funding for equity method investments of $2.1 million. The cash used in investing activities was partially offset by proceeds from the sale of marketable securities of $31.7 million, repayment of a loan receivable of $4.1 million, and distributions from an equity method investment of $0.4 million.
Cash provided by financing activities during the year ended December 31, 2023 was $3.4 million, as compared to cash used in financing activities of $20.1 million for the year ended December 31, 2022. Cash provided by financing activities during the year ended December 31, 2023 was primarily attributable to borrowings on our debt of $284.5 million and proceeds from the exercise of stock options of $1.5 million. This was partially offset by repayment of debt for $204.7 million, dividends payments of $62.1 million, repurchase of common shares of $10.2 million, debt issuance costs of $3.9 million for our Amended Credit Agreement, payments related to our contingent liabilities of $1.0 million, and repayment of finance lease obligations of $0.7 million. Cash used in financing activities for the year ended December 31, 2022 was $20.1 million, which was attributable to dividend payments of $14.0 million, repurchase of common shares of $9.3 million, purchase of non-controlling interest of $5.0 million, repayment of debt of $3.9 million, and repayment of finance lease obligations of $0.6 million. This was partially offset by proceeds from the exercise of options and warrants of $8.6 million, borrowings from the Construction Loan of $3.6 million and proceeds from the sale of non-controlling interest of $0.4 million.
Excluded Assets
In September 2019, APC and Astrana Medical entered into the Second Amendment to Series A Preferred Stock Purchase Agreement, clarifying the term Excluded Assets. “Excluded Assets” means (i) assets received from the sale of shares of the Series A Preferred equal to the Series A purchase price, (ii) the assets of APC that are not Healthcare Services Assets, including the APC’s equity interests in Astrana Health, Inc., and any entity that is primarily engaged in the business of owning, leasing, developing, or otherwise operating real estate, (iii) any assets acquired with the proceeds of the sale, assignment, or other disposition of any of the assets described in clauses (i) or (ii), and (iv) any proceeds of the assets described in clauses (i), (ii), and (iii).
On December 26, 2023, APC completed a restructuring transaction to spin-off its real estate investments, a component of Excluded Assets (“the Spin-Off”). To effect the restructuring, APC contributed its real estate investments to a wholly owned subsidiary in exchange for 100% of the subsidiary’s membership interest units, which membership interests were then distributed to holders of APC’s outstanding common stock as a dividend, with each such stockholder receiving one membership interest unit for each share of outstanding APC common stock held. As a result of the distribution, the real estate investments are no longer included within our consolidated financial statements after December 26, 2023. Net loss from Excluded Assets for the year ended December 26, 2023 and years ended December 31, 2022 and 2021 consisted of the following (in thousands):
Year ended December 26, |
Years ended December 31, | |||||||||||||||||||
| 2023 | 2022 | 2021 | ||||||||||||||||||
| Total operating expenses | $ | 18,127 | $ | 2,351 | $ | 2,588 | ||||||||||||||
Total other income (expense), net |
$ | 3,917 | $ | (15,242) | $ | (10,854) | ||||||||||||||
Excluded Assets net loss |
$ | (16,667) | $ | (23,314) | $ | (13,461) | ||||||||||||||
Credit Facilities
The Company’s debt balance consisted of the following (in thousands):
64
| December 31, 2023 | |||||
| Term Loan | $ | 280,000 | |||
| Promissory Note Payable | 2,000 | ||||
| Total debt | 282,000 | ||||
| Less: Current portion of debt | (19,500) | ||||
| Less: Unamortized financing costs | (3,561) | ||||
| Long-term debt | $ | 258,939 | |||
The following are the future commitments of the Company’s debt for the years ending December 31 (in thousands):
| Amount | |||||
| 2024 | $ | 19,500 | |||
| 2025 | 15,750 | ||||
| 2026 | 21,000 | ||||
| 2027 | 22,750 | ||||
| 2028 | 203,000 | ||||
| Total | $ | 282,000 | |||
Amended Credit Agreement
On June 16, 2021, the Company entered into an amended and restated credit agreement (as subsequently amended as described below, the “Amended Credit Agreement”) with Truist Bank, in its capacity as administrative agent for the lenders, issuing bank, swingline lender and lender, and the banks and other financial institutions from time to time party thereto, to, among other things, amend and restate that certain credit agreement, dated September 11, 2019, by and among the Company, Truist Bank, and certain lenders thereto, in its entirety. The Amended Credit Agreement provides for a five-year revolving credit facility to the Company of $400.0 million (“Revolver Loan”), which includes a letter of credit sub-facility of up to $25.0 million and a swingline loan sub-facility of $25.0 million.
On December 20, 2022, an amendment was made to the Amended Credit Facility, in which all amounts borrowed under the Amended Credit Agreement as of the effective date were automatically converted from LIBOR Loans to SOFR Loans with an initial interest period of one month on and as of the amendment effective date.
On September 8, 2023, a Second Amendment to the Amended Credit Agreement was entered into which, among other things, increased the letter of credit sub-facility from $25.0 million to $50.0 million.
On November 3, 2023, the Company entered into a Third Amendment to the Amended Credit Agreement (“Third Amendment”) with Truist Bank and the other financial institutions party thereto. The Third Amendment provided a new term loan to the Company in an aggregate amount of up to $300.0 million, with $180.0 million funded at the closing of the Third Amendment, and $120.0 million available to be drawn by the Company as delayed draw loans during the six months subsequent to the closing of the Third Amendment (collectively, the “Term Loan”). The Term Loan matures on November 3, 2028 (or such earlier date on which it is terminated in accordance with the provisions of the Amended Credit Agreement) and amortizes quarterly at 5% per annum for each of the first two years, 7.5% per annum for years three and four, and 10% per annum for year five.
Refer to Note 10 – “Credit Facility, Bank Loans, and Lines of Credit” to our consolidated financial statements under Item 8 in this Annual Report on Form 10-K for additional information on the Amended Credit Agreement.
Promissory Note Payable
65
In May 2021, FYB entered into a promissory note agreement with CCHCA. The principal on the promissory note is $2.0 million with a maturity date of May 9, 2024. Refer to Note 10 – “Credit Facility, Bank Loans, and Lines of Credit” to our consolidated financial statements under Item 8 in this Annual Report on Form 10-K for additional information on the Promissory Note Payable.
Deferred Financing Costs
As of December 31, 2023, the Amended Credit Agreement had unamortized deferred financing costs of $6.1 million. $2.6 million of unamortized deferred financing costs was related to unborrowed amounts available on the Term Loan and the unamortized deferred financing costs for the Revolver Loan. $3.6 million of unamortized deferred financing costs were netted against amounts borrowed on the Term Loan.
Effective Interest Rate
The Company’s average effective interest rate on its total debt during the years ended December 31, 2023, 2022, and 2021 was 6.19%, 3.22%, and 2.06%, respectively. Interest expense in the consolidated statements of income included amortization of deferred debt issuance costs for the years ended December 31, 2023, 2022, and 2021 of $1.1 million, $0.9 million, and $1.2 million, respectively.
Real Estate Loans and Construction Loan (Excluded Assets for the benefit of APC and its subsidiaries)
Real Estate - East West Bank
In December 2020, APC’s Excluded Assets entered into three real estate loans with East West Bank. As of December 31, 2022, the principal on each loan was $5.9 million, $0.6 million, and $0.6 million, respectively, and had a variable interest rate of 0.50%, 0.50%, and 0.30% less than the independent index, which is the daily Wall Street Journal “Prime Rate”, respectively. The maturity date of each loan was August 5, 2030.
Real Estate - MUFG Union Bank N.A.
In January 2022, a subsidiary of APC, which was included in Excluded Assets, entered into a loan agreement with MUFG Union Bank N.A. with a maturity date of March 1, 2032. The variable interest rate was 2.0% in excess of Daily Simple SOFR (as defined in the loan agreement). As of December 31, 2022 the principal on the loan was $16.0 million. On December 14, 2023, APC paid off the outstanding loan balance of $15.6 million.
Construction Loan
In April 2021, an entity included in Excluded Assets entered into a construction loan agreement with MUFG Union Bank N.A. (“Construction Loan”). The Construction Loan had a borrowing capacity of $10.7 million with a maturity date of March 1, 2024 or, upon completion of the construction and certain other requirements defined in the loan agreement, March 1, 2034. The loan balance as of December 31, 2022 was $4.2 million. On December 14, 2023, APC paid off the outstanding loan balance of $8.5 million.
These Real Estate Loans and the Construction Loan are deemed Excluded Assets and were spun-off on December 26, 2023 as part of the Spin-Off. Refer to Note 10 – “Credit Facility, Bank Loans, and Lines of Credit” to our consolidated financial statements under Item 8 in this Annual Report on Form 10-K for additional information on the Real Estate Loans and the Construction Loan.
Lines of Credit
On September 10, 2019, APC amended its promissory note agreement with Preferred Bank (“APC Business Loan Agreement”), which is affiliated with one of the Company’s board members, to modify loan availability to $4.1 million. This decrease further limited the purpose of the indebtedness under the APC Business Loan Agreement to the issuance of standby letters of credit, and added as a permitted lien the security interest in all of its assets granted by APC in favor of AHM under a Security Agreement dated on or about September 11, 2019 securing APC’s obligations to AHM under, and as required pursuant to, that certain Management Services Agreement dated as of July 1, 1999, as amended.
Standby Letters of Credit
66
Under the Amended Credit Agreement, the Company established irrevocable standby letters of credit with Truist Bank for a total of $36.5 million for the benefit of CMS and certain health plans as of December 31, 2023. Unless the institution provides notification that the standby letters of credit will be terminated prior to the expiration date, the letters will be automatically extended without amendment for additional one-year periods from the present, or any future expiration date.
Certain IPAs consolidated by the Company established irrevocable standby letters of credit with a financial institution for a total of $3.9 million for the benefit of certain health plans as of December 31, 2023. The standby letters of credit are automatically extended without amendment for additional one-year periods from the present or any future expiration date, unless notified by the institution in advance of the expiration date that the letter will be terminated.
Critical Accounting Policies and Estimates
The consolidated financial statements have been prepared in accordance with generally accepted accounting principles in the United States of America (“U.S. GAAP”), which require management to make a number of estimates and assumptions relating to the reported amount of assets and liabilities and the disclosure of contingent assets and liabilities at the date of the consolidated financial statements and to the reported amounts of revenues and expenses during the period. The Company bases its estimates on historical experience and on various other assumptions that the Company believes are reasonable under the circumstances. Changes in estimates are recorded if and when better information becomes available. Actual results could differ from those estimates under different assumptions and conditions. The Company believes that the accounting policies discussed below are those that are most important to the presentation of its financial condition and results of operations and that require its management’s most difficult, subjective, and complex judgments. Our significant accounting policies are described in Note 2 – “Basis of Presentation and Summary of Significant Accounting Policies” to our consolidated financial statements under Item 8 in this Annual Report on Form 10-K.
Principles of Consolidation
The consolidated balance sheets as of December 31, 2023 and 2022 and consolidated statements of income for the years ended December 31, 2023, 2022 and 2021 include Astrana’s wholly owned subsidiaries and consolidated variable interest entities (“VIEs”).
Use of Estimates
The preparation of the consolidated financial statements and related disclosures in conformity with U.S. GAAP requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the consolidated financial statements and the reported amounts of revenues and expenses during the reporting period. Significant items subject to such estimates and assumptions include collectability of receivables, recoverability of long-lived and intangible assets, business combination and goodwill valuation and impairment, accrual of medical liabilities (incurred but not reported (“IBNR”) claims), determination of hospital shared-risk and health plan shared-risk revenue and receivables (including constraints, completion factors and historical margins), income tax-valuation allowance, share-based compensation, and right-of-use assets and lease liabilities. Management evaluates its estimates and assumptions on an ongoing basis using historical experience and other factors, including the current economic environment, and makes adjustments when facts and circumstances dictate. As future events and their effects cannot be determined with precision, actual results could differ materially from those estimates and assumptions.
Receivables and Receivables – Related Parties
The Company’s receivables are comprised of accounts receivable, capitation and claims receivable, risk pool settlements, incentive receivables, management fee income, and other receivables. Accounts receivables are recorded and stated at the amount expected to be collected.
The Company’s receivables – related parties are comprised of risk pool settlements, management fee income, and other receivables. Receivables – related parties are recorded and stated at the amount expected to be collected.
Capitation and claims receivables relate to each health plan’s capitation and are received by the Company in the month following the month of service. Risk pool settlements and incentive receivables mainly consist of the Company’s hospital shared-risk pool receivable that is recorded quarterly based on reports received from the Company’s hospital partners and management’s estimate of the Company’s portion of the estimated risk pool surplus for open performance years. Settlement of risk pool surplus or deficits occurs approximately 18 months after the risk pool performance year is completed. Other
67
receivables consist of receivables from FFS reimbursement for patient care, certain expense reimbursements, transportation reimbursements from the hospitals, and stop-loss insurance premium reimbursements.
The Company maintains reserves for potential credit losses on accounts receivable. Management reviews the composition of accounts receivable and analyzes historical bad debts, customer concentrations, customer credit worthiness, current economic trends, and changes in customer payment patterns to evaluate the adequacy of these reserves. The Company also regularly analyzes the ultimate collectability of accounts receivable after certain stages of the collection cycle using a look-back analysis to determine the amount of receivables subsequently collected and adjustments are recorded when necessary. Reserves are recorded primarily on a specific identification basis.
Receivables are recorded when the Company is able to determine amounts receivable under applicable contracts and agreements based on information provided and collection is reasonably likely to occur. In regard to the credit loss standard, the Company continuously monitors its collections of receivables, and our expectation is that the historical credit loss experienced across our receivable portfolio is materially similar to any current expected credit losses that would be estimated under the current expected credit losses (“CECL”) model.
Fair Value Measurements
The Company’s financial instruments include cash and cash equivalents, restricted cash, investment in marketable securities, receivables, loans receivable – related parties, accounts payable, certain accrued expenses, capital lease obligations, bank loan, line of credit – related party, and long-term debt. The carrying values of the financial instruments classified as current in the accompanying consolidated balance sheets are considered to be at their fair values, due to the short maturity of these instruments. The carrying amount of the loan receivables – related parties, net of current portion, bank loan, capital lease obligations line of credit - related party, and long-term debt approximate fair value as they bear interest at rates that approximate current market rates for debt with similar maturities and credit quality. The FASB’s Accounting Standards Codification 820, Fair Value Measurement (“ASC 820”), applies to all financial assets and financial liabilities that are measured and reported on a fair value basis and requires disclosure that establishes a framework for measuring fair value and expands disclosure about fair value measurements. ASC 820 establishes a fair value hierarchy for disclosures of the inputs to valuations used to measure fair value.
This hierarchy prioritizes the inputs into three broad levels as follows:
Level 1—Inputs are unadjusted quoted prices in active markets for identical assets or liabilities that can be accessed at the measurement date.
Level 2—Inputs include quoted prices for similar assets and liabilities in active markets, quoted prices for identical or similar assets or liabilities in markets that are not active, inputs other than quoted prices that are observable for the asset or liability (i.e., interest rates and yield curves), and inputs that are derived principally from or corroborated by observable market data by correlation or other means (market corroborated inputs).
Level 3—Unobservable inputs that reflect assumptions about what market participants would use in pricing the asset or liability. These inputs would be based on the best information available, including the Company’s own data.
Business Combinations
We use the acquisition method of accounting for all business combinations, which requires assets and liabilities of the acquiree to be recorded at fair value, to measure the fair value of the consideration transferred, including contingent consideration, to be determined on the acquisition date, and to account for acquisition-related costs separately from the business combination.
Intangible Assets and Long-Lived Assets
Intangible assets with finite lives include network-payer relationships, management contracts, and member relationships and are stated at cost, less accumulated amortization and impairment losses. These intangible assets are amortized on the accelerated method using the discounted cash flow rate. Intangible assets with finite lives also include a patient management platform, as well as trade names and trademarks, whose valuations were determined using the cost to recreate method and the relief from royalty method, respectively. These assets are stated at cost, less accumulated amortization and impairment losses, and are amortized using the straight-line method.
68
Finite-lived intangibles and long-lived assets are reviewed for impairment whenever events or changes in circumstances indicate that the carrying amount of an asset may not be recoverable. If the expected future cash flows from the use of such assets (undiscounted and without interest charges) are less than the carrying value, a write-down would be recorded to reduce the carrying value of the asset to its estimated fair value. Fair value is determined based on appropriate valuation techniques.
Goodwill and Intangible Assets
Under ASC 350, Intangibles – Goodwill and Other, goodwill and indefinite-lived intangible assets are reviewed at least annually for impairment under a two step process.
•Step 1— Under a qualitative assessment, determine if there are indicators of impairment. If so, proceed to Step 2.
•Step 2 — Under a quantitative assessment, if the fair value of each reporting unit is less than its carrying value, there is an impairment.
The Company may also elect to skip the qualitative testing and proceed directly to quantitative testing. The Company’s four reporting units consist of the following:
•Care Partners – IPA;
•Care Partners – ACO;
•Care Delivery; and
•Care Enablement.
An impairment loss is recognized if the carrying value of a reporting unit exceeds its fair value. If this event arises, the impairment loss recorded is equal to the excess of the carrying value of the reporting unit over its fair value.
At least annually, indefinite-lived intangible assets are tested for impairment. Impairment for intangible assets with indefinite lives exists if the carrying value of the intangible asset exceeds its fair value. The fair values of indefinite-lived intangible assets are determined using valuation techniques based on estimates, judgments, and assumptions management believes are appropriate in the circumstances.
Accrual of Medical Liabilities
The Company’s Care Partners segment is responsible for integrated care that the associated physicians and contracted hospitals provide to their enrollees. The Company’s Care Partners segment provides integrated care to HMOs, Medicare, and Medi-Cal enrollees through a network of contracted providers under sub-capitation and direct patient service arrangements. Medical costs for professional and institutional services rendered by contracted providers are recorded as cost of services, excluding depreciation and amortization, in the accompanying consolidated statements of income.
An estimate of amounts due to contracted physicians, hospitals, and other professional providers is included in medical liabilities in the accompanying consolidated balance sheets. Medical liabilities include claims reported as of the balance sheet date and estimated IBNR claims. Such estimates are developed using actuarial methods and are based on numerous variables, including the utilization of healthcare services, historical payment patterns, cost trends, product mix, seasonality, changes in membership, and other factors. The estimation methods and the resulting reserves are periodically reviewed and updated. Many of the medical contracts are complex in nature and may be subject to differing interpretations regarding amounts due for the provision of various services. Such differing interpretations may not come to light until a substantial period of time has passed following the contract implementation.
Risk Pool Settlements and Incentives
69
Certain IPAs enter into hospital shared-risk capitation arrangements with certain health plans and local hospitals, where the hospital is responsible for providing, arranging and paying for institutional risk and the IPA is responsible for providing, arranging, and paying for professional risk. Under a hospital shared-risk pool-sharing agreement, the IPA generally receives a percentage of the net surplus from the affiliated hospital’s risk pools with HMOs after deductions for the affiliated hospital’s costs. Advance settlement payments are typically made quarterly in arrears if there is a surplus. The Company’s risk pool settlements under arrangements with health plans and hospitals are recognized using the most likely amount methodology and amounts are only included in revenue to the extent that it is probable that a significant reversal of cumulative revenue will not occur once any uncertainty is resolved. The assumptions for historical margin, IBNR completion factors, and constraint percentages were used by management in applying the most likely amount methodology.
Under capitated arrangements with certain HMOs, certain IPAs participate in one or more health plan shared-risk arrangements relating to the provision of institutional services to enrollees and thus can earn additional revenue or incur losses based upon the enrollee utilization of institutional services. Health plan shared-risk arrangements are entered into with certain health plans, which are administered by the health plan, where the IPA is responsible for rendering professional services, but the health plan does not enter into a capitation arrangement with a hospital and therefore the health plan retains the institutional risk. Health plan shared-risk deficits, if any, are not payable until and unless (and only to the extent) risk-sharing surpluses are generated. At the termination of the HMO contract, any accumulated deficit will be extinguished.
The Company's risk pool settlements under arrangements with HMOs are recognized, using the most likely methodology, and only included in revenue to the extent that it is probable that a significant reversal of cumulative revenue will not occur. Given the lack of access to the health plans’ data and control over the members assigned to the IPA, the adjustments and/or the withheld amounts are unpredictable and as such the IPAs risk-share revenues are deemed to be fully constrained until they are notified of the amount by the health plan. Final settlement of risk pools for prior contract years generally occurs in the third or fourth quarter of the following year.
In addition to risk-sharing revenues, the Company also receives incentives under “pay-for-performance” programs for quality medical care, based on various criteria. As an incentive to promote quality care, certain HMOs have designed quality incentive programs and commercial generic pharmacy incentive programs to compensate the Company for its efforts to improve the quality of services and efficient and effective use of pharmacy supplemental benefits provided to HMO members. The incentive programs track specific performance measures and calculate payments to the Company based on the performance measures. The Company’s incentives under “pay-for-performance” programs are recognized using the most likely methodology. However, as the Company does not have sufficient insight from the health plans on the amount and timing of the health plan shared-risk pool and incentive payments, these amounts are considered to be fully constrained and only recorded when such payments are known and/or received.
Generally, for the foregoing arrangements, the final settlement is dependent on each distinct day’s performance within the annual measurement period, but cannot be allocated to specific days until the full measurement period has occurred and performance can be assessed. As such, this is a form of variable consideration estimated at contract inception and updated through the measurement period (i.e., the contract year), to the extent the risk of reversal does not exist and the consideration is not constrained.
Share-Based Compensation
The Company maintains a stock-based compensation program for employees, non-employees, directors, and consultants. From time to time, the Company issues shares of its common stock to its employees, directors, and consultants, which shares may be subject to the Company’s repurchase right (but not obligation), that vests based on time-based and/or performance-based vesting schedules. The value of share-based awards is recognized as compensation expense and adjusted for forfeitures as they occur. Compensation expenses for time-based awards are recognized on a cumulative straight-line basis over the vesting period of the awards. Share-based awards with performance conditions are recognized to the extent the performance conditions are probable of being achieved. Compensation expenses for performance-based awards are recognized on an accelerated attribution method. The grant date fair value of the restricted stock awards is the grant date’s closing market price of the Company’s common stock. The fair value of options granted is determined using the Black-Scholes option pricing model and include several assumptions, including expected term, expected volatility, expected dividends, and risk-free rates. The expected term is presumed to be the midpoint between the vesting date and the end of the contractual term. The expected stock price volatility is determined based on an average of historical volatility. The expected dividend yield is based on the Company’s expected dividend payouts. The risk-free interest rate is based on the U.S. Constant Maturity curve over the expected term of the option at the time of grant.
Leases
70
The Company determines if an arrangement is a lease at its inception. The expected term of the lease used for computing the lease liability and right-of-use asset and determining the classification of the lease as operating or financing may include options to extend or terminate the lease when it is reasonably certain that the Company will exercise that option. The Company elected practical expedients for ongoing accounting that were provided by the new standard comprised of the following:
•The election for classes of underlying assets to not separate non-lease components from lease components, and
•The election for short-term lease recognition exemption for all leases with an under twelve-month terms.
The present value of the lease payments is calculated using a rate implicit in the lease, when readily determinable. However, as most of the Company’s leases do not provide an implicit rate, the Company uses its incremental borrowing rate to determine the present value of the lease payments for the majority of its leases.
Variable Interest Model
If an entity is determined to be a VIE, the Company evaluates whether the Company is the primary beneficiary. The primary beneficiary analysis is a qualitative analysis based on power and economics. The Company consolidates a VIE if both power and benefits belong to the Company – that is, the Company has:
•The power to direct the activities of a VIE that most significantly influence the VIE’s economic performance (power), and
•The obligation to absorb losses of, or the right to receive benefits from, the VIE that could potentially be significant to the VIE (economics).
The Company consolidates VIEs whenever it is determined that the Company is the primary beneficiary.
Investment in Other Entities - Equity Method
The Company accounts for certain investments using the equity method of accounting when it is determined that the investment provides the Company with the ability to exercise significant influence, but not control, over the investee. Significant influence is generally deemed to exist if the Company has an ownership interest in the voting stock of the investee of between 20% and 50%, although other factors, such as representation on the investee’s board of directors, are considered in determining whether the equity method of accounting is appropriate. Under the equity method of accounting, the investment, originally recorded at cost, is adjusted to recognize the Company’s share of net earnings or losses of the investee and is recognized in the accompanying consolidated statements of income under “Income (loss) from equity method investments” and also is adjusted by contributions to and distributions from the investee. During the year ended December 31, 2023, the Company recognized no impairment loss.
Non-controlling Interests
The Company consolidates entities in which the Company has a controlling financial interest. The Company consolidates subsidiaries in which the Company holds, directly or indirectly, more than 50% of the voting rights, and VIEs in which the Company is the primary beneficiary. Non-controlling interests represent third-party equity ownership interests (including equity ownership interests held by certain VIEs) in the Company’s consolidated entities. Net income attributable to non-controlling interests is disclosed in the consolidated statements of income.
Mezzanine Equity
Pursuant to APC’s shareholder agreements, in the event of a disqualifying event, as defined in the agreements, APC could be required to repurchase its shares from the respective shareholders based on certain triggers outlined in the shareholder agreements. As the redemption feature of the shares is not solely within the control of APC, the equity of APC does not qualify as permanent equity and has been classified as mezzanine or temporary equity. Accordingly, the Company recognizes non-controlling interests in APC as mezzanine equity in the consolidated financial statements. APC’s shares were not redeemable, and it was not probable that the shares would become redeemable as of December 31, 2023 and 2022.
Income Taxes
71
Federal and state income taxes are computed at currently enacted tax rates less tax credits using the asset and liability method. Deferred taxes are adjusted both for items that do not have tax consequences and for the cumulative effect of any changes in tax rates from those previously used to determine deferred tax assets or liabilities. Tax provisions include amounts that are currently payable, changes in deferred tax assets and liabilities that arise because of temporary differences between the timing of when items of income and expense are recognized for financial reporting and income tax purposes, changes in recognition of tax positions, and any changes in the valuation allowance caused by a change in judgment about the realizability of the related deferred tax assets. A valuation allowance is established when necessary to reduce deferred tax assets to amounts expected to be realized.
The Company uses a recognition threshold of more-likely-than-not and a measurement attribute on all tax positions taken or expected to be taken in a tax return in order to be recognized in the consolidated financial statements. Once the recognition threshold is met, the tax position is then measured to determine the actual amount of benefit to recognize in the consolidated financial statements.
Effect of New Accounting Standards
Refer to “Recent Accounting Pronouncements Not Yet Adopted” under Note 2 — “Basis of Presentation and Summary of Significant Accounting Policies” to our consolidated financial statements under Item 8 in this Annual Report on Form 10-K for additional information.
Item 7A. Quantitative and Qualitative Disclosures About Market Risk
Interest Rate Risk
Borrowings under the Term Loan provided for under our Amended Credit Agreement, as of December 31, 2023, were $280.0 million. The Term Loan bears interest at an annual rate equal to either, at the Company’s option, (a) the Term SOFR Reference Rate (as defined in the Amended Credit Agreement), adjusted for any Term SOFR Adjustment (as defined in the Amended Credit Agreement ), plus a spread from 1.50% to 2.75%, as determined on a quarterly basis based on the Company’s Consolidated Total Net Leverage Ratio, or (b) a base rate, plus a spread of 0.50% to 1.75%, as determined on a quarterly basis based on the Company’s Consolidated Total Net Leverage Ratio. As of December 31, 2023, there were no borrowings under the Revolver Loan. The Revolver Loan bears interest at an annual rate equal to either, at the Company’s option, (a) the Term SOFR Reference Rate (as defined in the Amended Credit Agreement ), adjusted for any Term SOFR Adjustment (as defined in the Amended Credit Agreement) plus a spread ranging from 1.25% to 2.50%, as determined on a quarterly basis based on the Company’s Consolidated Total Net Leverage Ratio (as defined in the Amended Credit Agreement), or (b) a base rate, plus a spread ranging from 0.25% to 1.50%, as determined on a quarterly basis based on the Company’s Consolidated Total Net Leverage Ratio. Borrowings under the Promissory Note Payable, as of December 31, 2023, was $2.0 million. The interest rate is defined as the prime rate plus 1.0%. The prime rate is updated annually on the effective date of the note and published by the Wall Street Journal. The Company has entered into a collar agreement for its Revolver Loan to effectively convert its floating-rate debt to a fixed-rate basis. The principal objective of the collar agreement is to eliminate or reduce the variability of the cash flows in interest payments associated with the Company’s floating-rate debt, thus reducing the impact of interest rate changes on future interest payment cash flows. A hypothetical 1% change in our interest rates for our outstanding borrowings under our Credit Agreement would have increased or decreased our interest expense for the year ended December 31, 2023, by $2.8 million.
72
Item 8. Financial Statements and Supplementary Data
| Index to the Consolidated Financial Statements | Page | ||||
Report of Independent Registered Public Accounting Firm (PCAOB ID No. |
|||||
73
Report of Independent Registered Public Accounting Firm
To the Stockholders and the Board of Directors of Astrana Health, Inc.
Opinion on the Financial Statements
We have audited the accompanying consolidated balance sheets of Astrana Health, Inc. (formerly known as Apollo Medical Holdings, Inc.) (the Company) as of December 31, 2023 and 2022, the related consolidated statements of income, mezzanine and stockholders' equity (deficit) and cash flows for each of the three years in the period ended December 31, 2023, and the related notes (collectively referred to as the “consolidated financial statements”). In our opinion, the consolidated financial statements present fairly, in all material respects, the financial position of the Company at December 31, 2023 and 2022, and the results of its operations and its cash flows for each of the three years in the period ended December 31, 2023, in conformity with U.S. generally accepted accounting principles.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (PCAOB), the Company's internal control over financial reporting as of December 31, 2023, based on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (2013 framework), and our report dated February 29, 2024 expressed an unqualified opinion thereon.
Basis for Opinion
These financial statements are the responsibility of the Company's management. Our responsibility is to express an opinion on the Company’s financial statements based on our audits. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. Our audits included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audits provide a reasonable basis for our opinion.
Critical Audit Matters
The critical audit matters communicated below are matters arising from the current period audit of the financial statements that were communicated or required to be communicated to the audit committee and that: (1) relate to accounts or disclosures that are material to the financial statements and (2) involved our especially challenging, subjective or complex judgments. The communication of critical audit matters does not alter in any way our opinion on the consolidated financial statements, taken as a whole, and we are not, by communicating the critical audit matters below, providing separate opinions on the critical audit matters or on the accounts or disclosures to which they relate.
74
Risk Pool Settlements and Related Receivables
| Description of the Matter |
As described in Note 2 of the consolidated financial statements, the Company enters into hospital shared-risk capitation arrangements with certain health plans and local hospitals, where the hospital is responsible for providing, arranging and paying for institutional risk and the Company is responsible for providing, arranging and paying for professional risk. Under a hospital shared-risk pool-sharing agreement, the Company generally receives a percentage of the net surplus from the affiliated hospitals’ risk pools with health plans after deductions for the affiliated hospitals’ costs. The Company recognizes risk pool settlements relating to such arrangements using the most likely amount methodology and amounts are only included in revenues to the extent that it is probable that a significant reversal of cumulative revenue will not occur once any uncertainty is resolved. The amount of such risk pool settlements recorded is calculated by the Company using historical margin, incurred but not reported (IBNR) completion factors and constraint percentages and various data and information provided by the affiliated hospitals. Auditing management’s estimate of the risk pool settlements and related receivables involved a high degree of subjectivity used by management and the nature of the significant assumptions, which include a margin factor based on historical trends and other available information. The Company relies on data provided by other parties in its estimation model. Additionally, judgment is used to develop the margin factor used to account for the expected performance of the risk pools for each settlement year and is derived based on an evaluation of historical data provided by the affiliated hospitals and communications between the Company and the affiliated hospitals. |
||||
| How We Addressed the Matter in Our Audit |
We obtained an understanding, evaluated the design, and tested the operating effectiveness of internal controls over the Company’s process for estimating risk pool settlements and related receivable amounts. For example, we tested controls over management’s review controls of the reasonableness of the data (including capitation revenue and related claims and other administrative expenses) underlying the risk pool calculations provided by the affiliated hospitals and management’s review controls analyzing the historical trends and appropriateness of the method used in determining the estimated risk pool surplus. We also reviewed relevant Service Organization Control (SOC) 1 reports to evaluate that such affiliated hospitals and administrator have effective controls over the completeness and accuracy of the data they process and provide to the Company. We also assessed and tested complementary user entity controls relevant to the SOC 1 reports.
To test the Company’s estimates of risk pool settlements and related receivables, our audit procedures included, among others, confirming the external data used in the calculations of risk pools directly with the affiliated hospitals, testing the receivables amount by comparing it to subsequent cash receipts, and testing the margin factor used by the Company in its estimate. In order to test the margin factor, we evaluated historical margin trends within the risk pools, and reviewed the Company’s own volumes and margins to identify any trends which may provide contrary evidence. Additionally, we assessed the precision of the Company’s prior year estimates by comparing the Company’s prior year estimates to the final settled amounts.
|
||||
75
Valuation of Incurred but not Reported (IBNR) Claims Liability
| Description of the Matter |
At December 31, 2023, the Company’s medical liabilities totaled $106.7 million. As described in Note 2 of the consolidated financial statements, medical liabilities include reserves for incurred but not reported claims. The IBNR liability is an estimate that management developed using actuarial methods and is based on numerous variables, including the utilization of healthcare services, historical payment patterns, cost trends, product mix, seasonality, changes in membership, and other factors. Auditing management’s estimate of the IBNR claims liability involved a high degree of subjectivity due to the complexity of the models used by management and the nature of the significant assumptions used in the estimation of the liability. These assumptions have a significant effect on the valuation of the IBNR liability. |
||||
| How We Addressed the Matter in Our Audit |
We obtained an understanding, evaluated the design, and tested the operating effectiveness of the Company’s internal controls over the process for estimating the IBNR claims liability. For example, we tested controls over management’s review controls of the completion factor and per member per month trend factor assumptions, and management’s review controls of the actuarial methods used to calculate the IBNR claims liability, including the completeness and accuracy of data inputs and outputs of those models.
To test the Company’s estimate of the IBNR claims liability, our audit procedures included, among others, testing the completeness and accuracy of data used in the Company’s models by testing reconciliations of underlying claims and membership data recorded in source systems to the actuarial reserve models, and comparing claims to source documentation. We involved our actuarial specialists to assist with the testing due to the highly judgmental nature of assumptions used in the valuation process, including completion factors and per member per month trend factors. With the assistance of our actuarial specialists, we used the Company’s underlying claims and membership data to develop an independent range of IBNR estimates and compared management’s recorded IBNR claims liability to our range. Additionally, we performed a hindsight review of prior period estimates by comparing to subsequent claims development, and we evaluated the Company’s disclosures surrounding IBNR claims liability in the financial statements.
|
||||
/s/ |
|||||
| We have served as the Company’s auditor since 2020. | |||||
February 29, 2024
76
ASTRANA HEALTH, INC. | ||||||||||||||
| CONSOLIDATED BALANCE SHEETS | ||||||||||||||
| (in thousands) | ||||||||||||||
| December 31, | December 31, | |||||||||||||
| 2023 | 2022 | |||||||||||||
| Assets | ||||||||||||||
| Current assets | ||||||||||||||
| Cash and cash equivalents | $ | $ | ||||||||||||
| Investment in marketable securities | ||||||||||||||
| Receivables, net | ||||||||||||||
| Receivables, net – related parties | ||||||||||||||
| Income taxes receivable | ||||||||||||||
| Other receivables | ||||||||||||||
| Prepaid expenses and other current assets | ||||||||||||||
| Loans receivable, net | ||||||||||||||
| Loans receivable – related party | ||||||||||||||
| Total current assets | ||||||||||||||
| Non-current assets | ||||||||||||||
| Land, property and equipment, net | ||||||||||||||
| Intangible assets, net | ||||||||||||||
| Goodwill | ||||||||||||||
| Income taxes receivable | ||||||||||||||
| Loans receivable, non-current | ||||||||||||||
| Investments in other entities – equity method | ||||||||||||||
| Investments in privately held entities | ||||||||||||||
| Restricted cash | ||||||||||||||
| Operating lease right-of-use assets | ||||||||||||||
| Other assets | ||||||||||||||
| Total non-current assets | ||||||||||||||
Total assets(1)
|
$ | $ | ||||||||||||
77
ASTRANA HEALTH, INC. | ||||||||||||||
CONSOLIDATED BALANCE SHEETS (Continued)
| ||||||||||||||
| (in thousands, except share data) | ||||||||||||||
| December 31, | December 31, | |||||||||||||
| 2023 | 2022 | |||||||||||||
Liabilities, Mezzanine Equity (Deficit), and Stockholders’ Equity |
||||||||||||||
| Current liabilities | ||||||||||||||
| Accounts payable and accrued expenses | $ | $ | ||||||||||||
| Fiduciary accounts payable | ||||||||||||||
| Medical liabilities | ||||||||||||||
| Income taxes payable | ||||||||||||||
| Dividend payable | ||||||||||||||
| Finance lease liabilities | ||||||||||||||
| Operating lease liabilities | ||||||||||||||
| Current portion of long-term debt | ||||||||||||||
| Other liabilities | ||||||||||||||
| Total current liabilities | ||||||||||||||
| Non-current liabilities | ||||||||||||||
| Deferred tax liability | ||||||||||||||
| Finance lease liabilities, net of current portion | ||||||||||||||
| Operating lease liabilities, net of current portion | ||||||||||||||
| Long-term debt, net of current portion and deferred financing costs | ||||||||||||||
| Other long-term liabilities | ||||||||||||||
| Total non-current liabilities | ||||||||||||||
Total liabilities(1)
|
||||||||||||||
Commitments and contingencies (Note 14)
|
||||||||||||||
Mezzanine (deficit) equity |
||||||||||||||
| Non-controlling interest in Allied Physicians of California, a Professional Medical Corporation (“APC”) | ( |
|||||||||||||
| Stockholders’ equity | ||||||||||||||
Series A Preferred stock, par value $ |
||||||||||||||
Series B Preferred stock, par value $ |
||||||||||||||
Common stock, par value $ |
||||||||||||||
| Additional paid-in capital | ||||||||||||||
| Retained earnings | ||||||||||||||
| Non-controlling interest | ||||||||||||||
| Total stockholders’ equity | ||||||||||||||
78
Total liabilities, mezzanine equity (deficit), and stockholders’ equity |
$ | $ | ||||||||||||
(1) The Company’s consolidated balance sheets include the assets and liabilities of its consolidated VIEs. The consolidated balance sheets include total assets that can be used only to settle obligations of the Company’s consolidated VIEs totaling $540.8 million and $579.8 million as of December 31, 2023 and December 31, 2022, respectively, and total liabilities of the Company’s consolidated VIEs for which creditors do not have recourse to the general credit of the primary beneficiary of $146.0 million and $149.6 million as of December 31, 2023 and December 31, 2022, respectively. These VIE balances do not include $273.2 million of investment in affiliates and $107.3 million of amounts due to affiliates as of December 31, 2023 and $304.8 million of investment in affiliates and $11.6 million of amounts due from affiliates as of December 31, 2022 as these are eliminated upon consolidation and not presented within the consolidated balance sheets. See Note 18 – “Variable Interest Entities (VIEs)” for further detail.
See accompanying notes to consolidated financial statements.
79
ASTRANA HEALTH, INC. | ||||||||||||||||||||
| CONSOLIDATED STATEMENTS OF INCOME | ||||||||||||||||||||
| (in thousands, except per share data) | ||||||||||||||||||||
| Years ended December 31, | ||||||||||||||||||||
| 2023 | 2022 | 2021 | ||||||||||||||||||
| Revenue | ||||||||||||||||||||
| Capitation, net | $ | $ | $ | |||||||||||||||||
| Risk pool settlements and incentives | ||||||||||||||||||||
| Management fee income | ||||||||||||||||||||
| Fee-for-service, net | ||||||||||||||||||||
| Other revenue | ||||||||||||||||||||
| Total revenue | ||||||||||||||||||||
| Operating expenses | ||||||||||||||||||||
| Cost of services, excluding depreciation and amortization | ||||||||||||||||||||
| General and administrative expenses | ||||||||||||||||||||
| Depreciation and amortization | ||||||||||||||||||||
| Total expenses | ||||||||||||||||||||
| Income from operations | ||||||||||||||||||||
| Other income (expense) | ||||||||||||||||||||
| Income (loss) from equity method investments | ( |
|||||||||||||||||||
| Gain on sale of equity method investment | ||||||||||||||||||||
| Interest expense | ( |
( |
( |
|||||||||||||||||
| Interest income | ||||||||||||||||||||
| Unrealized loss on investments | ( |
( |
( |
|||||||||||||||||
| Other income (loss) | ( |
|||||||||||||||||||
Total other income (expense), net |
( |
( |
||||||||||||||||||
| Income before provision for income taxes | ||||||||||||||||||||
| Provision for income taxes | ||||||||||||||||||||
| Net income | ||||||||||||||||||||
| Net (loss) income attributable to noncontrolling interests | ( |
( |
||||||||||||||||||
Net income attributable to Astrana Health, Inc. |
$ | $ | $ | |||||||||||||||||
| Earnings per share – basic | $ | $ | $ | |||||||||||||||||
| Earnings per share – diluted | $ | $ | $ | |||||||||||||||||
See accompanying notes to consolidated financial statements.
80
ASTRANA HEALTH, INC. | |||||||||||||||||||||||||||||||||||||||||
CONSOLIDATED STATEMENTS OF MEZZANINE AND STOCKHOLDERS’ EQUITY (DEFICIT) | |||||||||||||||||||||||||||||||||||||||||
| (in thousands, except share data) | |||||||||||||||||||||||||||||||||||||||||
|
Mezzanine
Equity (Deficit) –
Non-controlling
Interest in APC
|
Additional Paid-in Capital |
Retained
Earnings
|
Non-controlling Interest |
Stockholders’ Equity |
|||||||||||||||||||||||||||||||||||||
| Common Stock Outstanding | |||||||||||||||||||||||||||||||||||||||||
| Shares | Amount | ||||||||||||||||||||||||||||||||||||||||
| Balance at January 1, 2021 | $ | $ | $ | $ | $ | $ | |||||||||||||||||||||||||||||||||||
| Net (loss) income | ( |
— | — | — | |||||||||||||||||||||||||||||||||||||
| Purchase of non-controlling interest | ( |
— | — | — | — | ( |
( |
||||||||||||||||||||||||||||||||||
| Sale of non-controlling interest | — | — | — | — | — | — | |||||||||||||||||||||||||||||||||||
| Sale of shares by non-controlling interest | — | — | — | ||||||||||||||||||||||||||||||||||||||
| Shares issued for vesting of restricted stock awards | — | — | — | — | — | — | |||||||||||||||||||||||||||||||||||
| Shares issued for exercise of options and warrants | — | — | — | ||||||||||||||||||||||||||||||||||||||
| Purchase of treasury shares | — | ( |
— | ( |
— | — | ( |
||||||||||||||||||||||||||||||||||
| Share-based compensation | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||
| Investment in non-controlling interest | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||
| Acquisition of non-controlling interest | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||
| Cancellation of restricted stock awards | — | ( |
— | ( |
— | — | ( |
||||||||||||||||||||||||||||||||||
| Non-controlling interest capital change | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||
| Dividends | ( |
— | — | — | — | ( |
( |
||||||||||||||||||||||||||||||||||
Balance at December 31, 2021 |
$ | $ | $ | $ | $ | $ | |||||||||||||||||||||||||||||||||||
| Net (loss) income | ( |
— | — | — | |||||||||||||||||||||||||||||||||||||
| Purchase of non-controlling interest | — | — | — | — | — | ( |
( |
||||||||||||||||||||||||||||||||||
| Sale of non-controlling interest | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||
| Share buy back | ( |
— | — | — | — | — | — | ||||||||||||||||||||||||||||||||||
| Shares issued for vesting of restricted stock awards | — | — | ( |
— | — | ( |
|||||||||||||||||||||||||||||||||||
| Shares issued for cash and exercise of options and warrants | — | — | — | ||||||||||||||||||||||||||||||||||||||
| Purchase of treasury shares | — | ( |
— | ( |
— | — | ( |
||||||||||||||||||||||||||||||||||
| Share-based compensation | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||
81
ASTRANA HEALTH, INC. | |||||||||||||||||||||||||||||||||||||||||
CONSOLIDATED STATEMENTS OF MEZZANINE AND STOCKHOLDERS’ EQUITY (DEFICIT) | |||||||||||||||||||||||||||||||||||||||||
| (in thousands, except share data) | |||||||||||||||||||||||||||||||||||||||||
|
Mezzanine
Equity (Deficit) –
Non-controlling
Interest in APC
|
Additional Paid-in Capital |
Retained
Earnings
|
Non-controlling Interest |
Stockholders’ Equity |
|||||||||||||||||||||||||||||||||||||
| Common Stock Outstanding | |||||||||||||||||||||||||||||||||||||||||
| Shares | Amount | ||||||||||||||||||||||||||||||||||||||||
| Issuance of shares for business acquisition | — | — | — | — | |||||||||||||||||||||||||||||||||||||
| Investment in non-controlling interest | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||
| Cancellation of restricted stock awards | — | ( |
— | ( |
— | — | ( |
||||||||||||||||||||||||||||||||||
| Tax impact of acquisition | ( |
— | — | — | — | — | — | ||||||||||||||||||||||||||||||||||
| AAMG stock contingent consideration (see Note 21) | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||
| Dividends | ( |
— | ( |
||||||||||||||||||||||||||||||||||||||
Balance at December 31, 2022 |
$ | $ | $ | $ | $ | $ | |||||||||||||||||||||||||||||||||||
| Net income | ( |
— | — | — | |||||||||||||||||||||||||||||||||||||
| Purchase of non-controlling interest | — | — | — | — | — | ( |
( |
||||||||||||||||||||||||||||||||||
| Sale of non-controlling interest | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||
| Shares issued for vesting of restricted stock awards | — | — | ( |
— | — | ( |
|||||||||||||||||||||||||||||||||||
| Shares issued for cash and exercise of options and warrants | — | — | — | — | |||||||||||||||||||||||||||||||||||||
| Purchase of treasury shares | ( |
( |
— | ( |
— | — | ( |
||||||||||||||||||||||||||||||||||
| Share-based compensation | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||
| Issuance of shares for business acquisition | — | — | — | — | |||||||||||||||||||||||||||||||||||||
| Dividends | ( |
— | — | — | — | ( |
( |
||||||||||||||||||||||||||||||||||
| Transfer of common control entities | — | — | ( |
— | — | ( |
|||||||||||||||||||||||||||||||||||
| Tax impact from dividends | ( |
— | — | — | — | — | — | ||||||||||||||||||||||||||||||||||
| Tax impact from investments | ( |
— | — | — | — | — | — | ||||||||||||||||||||||||||||||||||
Balance at December 31, 2023 |
$ | ( |
$ | $ | $ | $ | $ | ||||||||||||||||||||||||||||||||||
See accompanying notes to consolidated financial statements.
82
ASTRANA HEALTH, INC. | ||||||||||||||||||||
| CONSOLIDATED STATEMENTS OF CASH FLOWS | ||||||||||||||||||||
| (in thousands) | ||||||||||||||||||||
| Years ended December 31, | ||||||||||||||||||||
| 2023 | 2022 | 2021 | ||||||||||||||||||
| Cash flows from operating activities | ||||||||||||||||||||
| Net income | $ | $ | $ | |||||||||||||||||
| Adjustments to reconcile net income to net cash provided by operating activities: | ||||||||||||||||||||
| Depreciation and amortization | ||||||||||||||||||||
| Amortization of debt issuance cost | ||||||||||||||||||||
| Share-based compensation | ||||||||||||||||||||
| Non-cash lease expense | ||||||||||||||||||||
| (Income) loss from equity method investments, net | ( |
( |
||||||||||||||||||
| Unrealized loss on investments | ||||||||||||||||||||
| Unrealized (gain) loss on interest rate swaps | ( |
( |
||||||||||||||||||
| Gain on sale or distribution of investments | ( |
( |
( |
|||||||||||||||||
| Deferred tax | ( |
( |
||||||||||||||||||
| Loss (gain) on consolidation of equity method investment | ( |
|||||||||||||||||||
| Gain on contingent equity securities | ( |
|||||||||||||||||||
| Gain from investment in warrants | ( |
|||||||||||||||||||
| Impairment of beneficial interest | ||||||||||||||||||||
| Other | ||||||||||||||||||||
| Changes in operating assets and liabilities, net of acquisition amounts: | ||||||||||||||||||||
| Receivable, net | ( |
( |
( |
|||||||||||||||||
| Receivable, net – related parties | ( |
|||||||||||||||||||
| Other receivable | ( |
|||||||||||||||||||
| Prepaid expenses and other current assets | ( |
|||||||||||||||||||
| Other assets | ( |
( |
||||||||||||||||||
| Accounts payable and accrued expenses | ( |
( |
||||||||||||||||||
| Fiduciary accounts payable | ( |
( |
||||||||||||||||||
| Medical liabilities | ||||||||||||||||||||
| Income taxes payable/receivable | ( |
( |
||||||||||||||||||
| Operating lease liabilities | ( |
( |
( |
|||||||||||||||||
| Net cash provided by operating activities | ||||||||||||||||||||
| Cash flows from investing activities | ||||||||||||||||||||
| Payments for business and asset acquisition, net of cash acquired | ( |
( |
( |
|||||||||||||||||
| Proceeds from repayment of loans receivable - related parties | ||||||||||||||||||||
| Purchases of marketable securities | ( |
( |
( |
|||||||||||||||||
| Proceeds from sale of marketable securities | ||||||||||||||||||||
| Issuance of loans receivable | ( |
|||||||||||||||||||
| Purchases of investments –privately held | ( |
|||||||||||||||||||
| Purchases of property and equipment | ( |
( |
( |
|||||||||||||||||
| Purchases of investments – equity method | ( |
( |
||||||||||||||||||
| Proceeds from sale of equity method investment | ||||||||||||||||||||
| Distribution from investment - equity method | ||||||||||||||||||||
83
ASTRANA HEALTH, INC. | ||||||||||||||||||||
| CONSOLIDATED STATEMENTS OF CASH FLOWS | ||||||||||||||||||||
| (in thousands) | ||||||||||||||||||||
| Years ended December 31, | ||||||||||||||||||||
| 2023 | 2022 | 2021 | ||||||||||||||||||
| Contribution to investment - equity method | ( |
( |
||||||||||||||||||
| Cash recorded from consolidation of VIE | ||||||||||||||||||||
| Net cash (used in) provided by investing activities | ( |
( |
||||||||||||||||||
| Cash flows from financing activities | ||||||||||||||||||||
| Dividends paid | ( |
( |
( |
|||||||||||||||||
| Repayments on long-term debt | ( |
( |
( |
|||||||||||||||||
| Borrowings on long-term debt | ||||||||||||||||||||
| Payment of finance lease obligations | ( |
( |
( |
|||||||||||||||||
| Proceeds from exercise of stock options and warrants | ||||||||||||||||||||
| Repurchase of shares | ( |
( |
( |
|||||||||||||||||
| Proceeds from sale of common stock | ||||||||||||||||||||
| Purchase of non-controlling interest | ( |
( |
( |
|||||||||||||||||
| Proceeds from sale of noncontrolling interest | ||||||||||||||||||||
| Cost of debt issuances | ( |
( |
||||||||||||||||||
| Payment of contingent consideration liabilities | ( |
|||||||||||||||||||
| Net cash provided by (used in) financing activities | ( |
( |
||||||||||||||||||
| Net increase in cash, cash equivalents, and restricted cash | ||||||||||||||||||||
| Cash, cash equivalents, and restricted cash, beginning of year | ||||||||||||||||||||
| Cash, cash equivalents and restricted cash, end of year | $ | $ | $ | |||||||||||||||||
| Supplemental disclosures of cash flow information | ||||||||||||||||||||
| Cash paid for income taxes | $ | $ | $ | |||||||||||||||||
| Cash paid for interest | $ | $ | $ | |||||||||||||||||
| Supplemental disclosures of non-cash investing and financing activities | ||||||||||||||||||||
| Right-of-use assets obtained in exchange for operating lease liabilities | ||||||||||||||||||||
| Tax impact from APC dividends to APC Shareholders | ||||||||||||||||||||
| Distribution of real estate investments | ||||||||||||||||||||
| Dividend declared included in dividend payable | ||||||||||||||||||||
| Issuance of financing obligation for business combinations | ||||||||||||||||||||
| Cashless exercise of warrants | ||||||||||||||||||||
| Fixed asset obtained in exchange for finance lease liabilities | ||||||||||||||||||||
| Common stock issued in business combination | ||||||||||||||||||||
| Mortgage loan | ||||||||||||||||||||
| Cancellation of Restricted Stock Awards | ||||||||||||||||||||
84
The following table provides a reconciliation of cash and cash equivalents and restricted cash reported within the consolidated balance sheets that sum to the total amounts of cash, cash equivalents, and restricted cash shown in the consolidated statements of cash flows (in thousands).
| Years Ended December 31, | |||||||||||||||||
| 2023 | 2022 | 2021 | |||||||||||||||
| Cash and cash equivalents | $ | $ | $ | ||||||||||||||
| Restricted cash | |||||||||||||||||
| Total cash, cash equivalents, and restricted cash shown in the statement of cash flows | $ | $ | $ | ||||||||||||||
See accompanying notes to consolidated financial statements.
85
1. Description of Business
Overview
On February 26, 2024, Apollo Medical Holdings, Inc. rebranded as Astrana Health, Inc (“Astrana”). Unless the context dictates otherwise, references in these notes to the financial statements, the “Company,” “we,” “us,” “our,” and similar words are references to Astrana and its consolidated subsidiaries and affiliated entities, as appropriate, including its consolidated variable interest entities (“VIEs”).
Headquartered in Alhambra, California, Astrana is a leading provider-centric, technology-powered, risk-bearing healthcare company. Leveraging its proprietary end-to-end technology solutions, Astrana operates an integrated healthcare delivery platform that enables providers to successfully participate in value-based care arrangements, thus empowering them to deliver accessible, high-quality care to patients in a cost-effective manner. Together with Astrana’s affiliated physician groups and consolidated subsidiaries and VIEs, the Company provides value-based care enablement services and care delivery with its consolidated care partners to serve patients in California, Nevada, and Texas, the majority of whom are covered by private or public insurance provided through Medicare, Medicaid, and health maintenance organizations (“HMOs”), with a small portion of our revenue coming from non-insured patients. The Company provides care coordination services to each major constituent of the healthcare delivery system, including patients, families, primary care physicians, specialists, acute care hospitals, alternative sites of inpatient care, physician groups, and health plans. The Company’s physician network consists of primary care physicians, specialist physicians, physician and specialist extenders, and hospitalists.
Segments
The Company’s reportable segments changed from one to three in the first quarter of 2023 as a result of certain changes to the information regularly provided to the Company’s chief operating decision maker when reviewing the Company’s performance as well as an effort to provide additional transparency to investors and other financial statement users. The three segments identified by the Company are Care Partners, Care Delivery and Care Enablement, which are described as follows:
Care Partners
The Care Partners segment is focused on building and managing high-quality and high-performance provider networks by partnering with, empowering, and investing in strong provider partners aligned on a shared vision for coordinated care delivery. By leveraging the Company’s unique care enablement platform and ability to recruit, empower, and incentivize physicians to effectively manage total cost of care, the Company is able to organize partnered providers into successful multi-payer risk-bearing organizations that take on varying levels of risk based on total cost of care across membership in all lines of business, including Medicare fee for service (“FFS”), Medicare Advantage, Medicaid, Commercial, and Exchange. Through the Company’s network of “independent practice associations” (“IPAs”), “accountable care organizations” (“ACOs”), and Restricted Knox-Keene licensed health plan, the Company’s healthcare delivery entities are responsible for coordinating and delivering high-quality care to the Company’s patients and ensuring continuity of care in Astrana’s ecosystem across age, stage of life, or life circumstance.
One of the Company’s Accountable Care Organizations (“ACO”) began participating in the Next Generation Accountable Care Organization (“NGACO”) Model of CMS in January 2017. The NGACO Model was a Center for Medicare & Medicaid Services (“CMS”) program that allowed provider groups to assume higher levels of financial risk and potentially achieve a higher reward from participating in this new attribution-based risk-sharing model. With the termination of the NGACO Model on December 31, 2021, the Company’s ACO participated as a Direct Contracting Entity (“DCE”) in the standard track of CMS’s Global and Professional Direct Contracting (“GPDC”) Model for Performance Year 2022 (“PY22”), beginning January 1, 2022. CMS has since redesigned the GPDC Model in response to the current Administration’s health care priorities, including their commitment to advancing health equity, stakeholder feedback, and participant experience, and renamed the GPDC Model to ACO Realizing Equity, Access, and Community Health (“ACO REACH”) Model. The Company began participation in the ACO REACH Model on January 1, 2023.
Care Delivery
The Company’s Care Delivery segment is a patient-centric, data-driven care delivery organization focused on delivering high-quality and accessible care to all patients. The Company’s care delivery organization includes primary care, multi-specialty care, and ancillary care services. This segment includes the following:
86
•Primary care clinics, including post-acute care services;
•Multi-specialty care clinics and medical groups, including hospitalist, intensivist, and physician advisory services, cardiac care and diagnostic testing, and specialized care for women’s health; and
•Ancillary service providers, such as urgent care centers, outpatient imaging centers, ambulatory surgery centers, and full-service labs.
Care Enablement
The Company’s Care Enablement segment is an integrated, end-to-end clinical, operational, financial, and administrative platform, powered by the Company’s proprietary technology suite, that enhances delivery of high-quality, value-based care to patients and leading to superior clinical and financial outcomes. The Company provides solutions to providers, including independent physicians, provider and medical groups, accountable care organizations, and payers, including health plans and other risk-bearing organizations. The Company’s platform meets providers and payers where they are, with a wide spectrum of solutions across the total cost of care risk spectrum, ranging from solutions for fee-for-service entities to full risk-bearing entities, and across patient types, including Medicare, Medicaid, Commercial, and Exchange patients. This segment includes the Company’s wholly owned subsidiaries which operate as management services organizations (“MSOs”), which enter into long-term management and/or administrative services agreements with Independent Practice Associations (“IPAs”), ACOs, or clinics. By leveraging the Company’s care enablement platform, providers and payers can improve their ability to deliver high-quality care to their patients and achieve better patient outcomes.
Other Affiliates
The Company’s other affiliates are not included as a reportable segment and primarily consist of the real estate operations and other entities that are individually immaterial. The real estate operations are deemed Excluded Assets that are solely for the benefit of Allied Physicians of California, a Professional Medical Corporation d.b.a. Allied Pacific of California IPA (“APC”) and its shareholders. Excluded Assets means (i) assets received from the sale of shares of APC’s Series A Preferred equal to the Series A purchase price, (ii) the assets of APC that are not Healthcare Services Assets (as defined in the Series A Preferred purchase agreement), including APC’s equity interests in Astrana Health, Inc., and any entity that is primarily engaged in the business of owning, leasing, developing, or otherwise operating real estate, (iii) any assets acquired with the proceeds of the sale, assignment, or other disposition of any of the assets described in clauses (i) or (ii), and (iv) any proceeds of the assets described in clauses (i), (ii), and (iii). As such, any income pertaining to Excluded Assets have no impact on the Series A Preferred dividend payable by APC to Astrana Health Medical Corporation (“Astrana Medical”), formerly known as AP-AMH Medical Corporation, and consequently will not affect net income attributable to Astrana. APC and Astrana Medical are consolidated variable interest entities of the Company. See Note 18 – “Variable Interest Entities (VIEs)” to the consolidated financial statements for information on the Company’s entities that qualify as consolidated VIEs.
87
2. Basis of Presentation and Summary of Significant Accounting Policies
Basis of Presentation
The accompanying consolidated financial statements have been prepared by management in accordance with generally accepted accounting principles in the United States of America (“U.S. GAAP”).
Principles of Consolidation
The consolidated balance sheets as of December 31, 2023 and 2022 and consolidated statements of income for the years ended December 31, 2023, 2022 and 2021 include Astrana’s wholly owned subsidiaries and consolidated variable interest entities (“VIEs”).
Reclassifications
Certain amounts disclosed in prior period financial statements have been reclassified to conform to the current period presentation. These reclassifications were made between other assets and investments in privately held entities on the accompanying consolidated balance sheet as of December 31, 2022. The reclassification had no effect on net income, earnings per share, retained earnings, cash flows or total assets.
Use of Estimates
The preparation of the consolidated financial statements and related disclosures in conformity with U.S. GAAP requires management to make estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the consolidated financial statements and the reported amounts of revenues and expenses during the reporting period. Significant items subject to such estimates and assumptions include collectability of receivables, recoverability of long-lived and intangible assets, business combinations and goodwill valuation and impairment, accrual of medical liabilities (incurred but not reported (“IBNR”) claims), determination of hospital shared-risk and health plan shared-risk revenue and receivables (including constraints, completion factors, and historical margins), income tax valuation allowance, share-based compensation, and right-of-use assets and lease liabilities. Management evaluates its estimates and assumptions on an ongoing basis using historical experience and other factors, including the current economic environment, and makes adjustments when facts and circumstances dictate. As future events and their effects cannot be determined with precision, actual results could differ materially from those estimates and assumptions.
Variable Interest Entities
On an ongoing basis, as circumstances indicate the need for reconsideration, the Company evaluates each legal entity that is not wholly owned by the Company in accordance with the consolidation guidance. The evaluation considers all of the Company’s variable interests, including equity ownership, as well as management services agreements. To fall within the scope of the consolidation guidance, an entity must meet both of the following criteria:
•The entity has a legal structure that has been established to conduct business activities and to hold assets; such entity can be in the form of a partnership, limited liability company, or corporation, among others; and
•The Company has a variable interest in the legal entity; i.e., variable interests that are contractual, such as equity ownership, or other financial interests that change with changes in the fair value of the entity’s net assets.
If an entity does not meet both criteria above, the Company applies other accounting guidance, such as the cost or equity method of accounting. If an entity does meet both criteria above, the Company evaluates such entity for consolidation under either the variable interest model if the legal entity meets any of the following characteristics to qualify as a VIE, or under the voting model for all other legal entities that are not VIEs.
A legal entity is determined to be a VIE if it has any of the following three characteristics:
•The entity does not have sufficient equity to finance its activities without additional subordinated financial support;
88
•The entity is established with non-substantive voting rights (i.e., where the entity deprives the majority economic interest holder(s) of voting rights); or
•The equity holders, as a group, lack the characteristics of a controlling financial interest. Equity holders meet this criterion if they lack any of the following:
•The power, through voting rights or similar rights, to direct the activities of the entity that most significantly influence the entity’s economic performance, as evidenced by:
•Substantive participating rights in day-to-day management of the entity’s activities; or
•Substantive kick-out rights over the party responsible for significant decisions;
•The obligation to absorb the entity’s expected losses; or
•The right to receive the entity’s expected residual returns.
If the Company determines that any of the three characteristics of a VIE are met, the Company will conclude that the entity is a VIE and evaluate it for consolidation under the variable interest model.
Variable interest model
If an entity is determined to be a VIE, the Company evaluates whether the Company is the primary beneficiary. The primary beneficiary analysis is a qualitative analysis based on power and economics. The Company consolidates a VIE if both power and benefits belong to the Company – that is, the Company has:
•The power to direct the activities of a VIE that most significantly influence the VIE’s economic performance (power), and
•The obligation to absorb losses of, or the right to receive benefits from, the VIE that could potentially be significant to the VIE (economics).
The Company consolidates VIEs whenever it is determined that the Company is the primary beneficiary. Refer to Note 18 – “Variable Interest Entities (VIEs)” to the consolidated financial statements for information on the Company’s consolidated VIEs. If there are variable interests in a VIE but the Company is not the primary beneficiary, the Company may account for the investment using the equity method of accounting, refer to Note 6 – “Investments in Other Entities” for entities that qualify as VIEs but the Company is not the primary beneficiary.
Business Combinations
The Company uses the acquisition method of accounting for all business combinations, which requires assets and liabilities of the acquiree to be recorded at fair value, to measure the fair value of the consideration transferred, including contingent consideration, to be determined on the acquisition date, and to account for acquisition-related costs separately from the business combination.
Reportable Segments
The Company operates as three
89
•Care Partners;
•Care Delivery; and
•Care Enablement.
Refer to Note 1 — “Description of Business” and Note 20 — “Segments” to the consolidated financial statements for information on the Company’s segments.
Cash and Cash Equivalents
The Company’s cash and cash equivalents primarily consist of money market funds and certificates of deposit. The Company considers all highly liquid investments that are both readily convertible into known amounts of cash and mature within 90 days from their date of purchase to be cash equivalents.
Restricted Cash
Investments in Marketable Securities
Investments in marketable securities consist of equity securities and certificates of deposit with various financial institutions. The appropriate classification of investments is determined at the time of purchase and such designation is reevaluated at each balance sheet date. Certificates of deposit in investments in marketable securities are reported at par value, plus accrued interest, with maturity dates greater than ninety days . Equity securities are reported at fair value. These securities are classified as Level 1 in the valuation hierarchy, where quoted market prices from reputable third-party brokers are available in an active market and unadjusted. Equity securities with low trading volume are determined to not have an active market with buyers and sellers ready to trade. Accordingly, the Company classifies such equity securities as Level 2 in the valuation hierarchy, and their valuation is based on weighted-average share prices from observable market data.
Receivables, Receivables – Related Parties, Other Receivables, Loan Receivable, and Loan Receivable - Related Party
The Company’s receivables are comprised of accounts receivable, capitation and claims receivable, risk pool settlements, incentive receivables, management fee income, and other receivables. Accounts receivables are recorded and stated at the amount expected to be collected.
The Company’s receivables – related parties are comprised of risk pool settlements, management fee income, and other receivables. Receivables – related parties are recorded and stated at the amount expected to be collected.
The Company’s loan receivable and loan receivable - related party consists of promissory notes that accrue interest per annum. As of December 31, 2023, promissory notes are expected to be collected by their maturity date.
Capitation receivables relate to each health plan’s capitation and are received by the Company in the month following the month of service. Risk pool settlements and incentive receivables mainly consist of the Company’s hospital shared-risk pool receivable that is recorded quarterly based on reports received from the Company’s hospital partners and management’s estimate of the Company’s portion of the estimated risk pool surplus for open performance years. Settlement of risk pool surplus or deficits occurs approximately 18 months after the risk pool performance year is completed. Other receivables consist of receivables from fee-for-services (“FFS”) reimbursement for patient care, certain expense reimbursements, transportation reimbursements from the hospitals, and stop-loss insurance premium reimbursements.
90
The Company maintains reserves for potential credit losses on accounts receivable. Management reviews the composition of accounts receivable and analyzes historical bad debts, customer concentrations, customer credit worthiness, current economic trends, and changes in customer payment patterns to evaluate the adequacy of these reserves. The Company also regularly analyzes the ultimate collectability of accounts receivable after certain stages of the collection cycle using a look-back analysis to determine the amount of receivables subsequently collected and adjustments are recorded when necessary. Reserves are recorded primarily on a specific identification basis.
Concentrations of Credit Risks
| Years Ended December 31, | |||||||||||||||||
| 2023 | 2022 | 2021 | |||||||||||||||
| Commercial | $ | $ | $ | ||||||||||||||
| Medicare | |||||||||||||||||
| Medicaid | |||||||||||||||||
| Other third parties | |||||||||||||||||
| Revenue | $ | $ | $ | ||||||||||||||
The Company had major payers from its Care Partners segment that contributed the following percentages of net revenue:
| Years Ended December 31, | |||||||||||||||||
| 2023 | 2022 | 2021 | |||||||||||||||
| Payer A | *% | *% | % | ||||||||||||||
| Payer B | % | % | |||||||||||||||
| Payer C | % | *% | *% | ||||||||||||||
| Payer D | *% | *% | % | ||||||||||||||
* Less than 10% of total net revenues
The Company had major payers that contributed to the following percentages of net receivables and receivables - related parties:
| As of December 31, | ||||||||||||||
| 2023 | 2022 | |||||||||||||
| Payer B | % | % | ||||||||||||
| Payer E | % | % | ||||||||||||
Land, Property, and Equipment, Net
Land is carried at cost and is not depreciated as it is considered to have an indefinite useful life.
91
Property and equipment, including leasehold improvements, are carried at cost less accumulated depreciation and amortization. Depreciation is provided principally on the straight-line method over the estimated useful lives of the assets ranging from to thirty-nine years . Leasehold improvements are amortized on a straight-line basis over the shorter of the terms of the respective leases or the expected useful lives of those improvements.
Maintenance and repairs are charged to expense as incurred. Upon sale or retirement, the asset cost and related accumulated depreciation and amortization are removed from the accounts, and any related gain or loss is included in the determination of consolidated net income.
Fair Value Measurements of Financial Instruments
The Company’s financial instruments consist of cash and cash equivalents, fiduciary cash, investment in marketable securities, receivables, loans receivable, accounts payable, certain accrued expenses, finance lease obligations, long-term debt, and certain other liabilities. The carrying values of the financial instruments classified as current in the accompanying consolidated balance sheets are considered to be at their fair values, due to the short maturity of these instruments. The carrying amounts of finance lease obligations and long-term debt approximate fair value as they bear interest at rates that approximate current market rates for debt with similar maturities and credit quality.
Financial Accounting Standards Board (“FASB”) Accounting Standards Codification (“ASC”) 820, Fair Value Measurement (“ASC 820”), applies to all financial assets and financial liabilities that are measured and reported on a fair value basis and requires disclosure that establishes a framework for measuring fair value and expands disclosure about fair value measurements. ASC 820 establishes a fair value hierarchy for disclosure of the inputs to valuations used to measure fair value.
This hierarchy prioritizes the inputs into three broad levels as follows:
Level 1 —Inputs are unadjusted quoted prices in active markets for identical assets or liabilities that can be accessed at the measurement date.
Level 2 —Inputs include quoted prices for similar assets and liabilities in active markets, quoted prices for identical or similar assets or liabilities in markets that are not active, inputs other than quoted prices that are observable for the asset or liability (i.e., interest rates and yield curves), and inputs that are derived principally from or corroborated by observable market data by correlation or other means (market corroborated inputs).
Level 3 —Unobservable inputs that reflect assumptions about what market participants would use in pricing the asset or liability. These inputs would be based on the best information available, including the Company’s own data.
There have been no changes in Level 1, Level 2, or Level 3 classification and no changes in valuation techniques for these assets and liabilities for the years ended December 31, 2023 and 2022.
Intangible Assets and Long-Lived Assets
Intangible assets with finite lives include network-payer relationships, management contracts, member relationships, subscriber relationships, and developed technology and are stated at cost, less accumulated amortization, and impairment losses. These intangible assets are amortized using the accelerated method based on the discounted cash flow rate or using the straight-line method.
Intangible assets with finite lives also include a patient management platform, as well as trade names and trademarks, whose valuations were determined using the cost to recreate method and the relief from royalty method, respectively. These assets are stated at cost, less accumulated amortization, and impairment losses, and are amortized using the straight-line method.
Goodwill and Indefinite-Lived Intangible Assets
92
Under ASC 350, Intangibles – Goodwill and Other, goodwill and indefinite-lived intangible assets are reviewed at least annually for impairment under a two step process.
•Step 1— Under a qualitative assessment, determine if there are indicators of impairment. If so, proceed to Step 2.
•Step 2 — Under a quantitative assessment, if the fair value of each reporting unit is less than its carrying value, there is an impairment.
The Company may also elect to skip the qualitative testing and proceed directly to quantitative testing. The Company’s four reporting units consist of the following:
•Care Partners – IPA;
•Care Partners – ACO;
•Care Delivery; and
•Care Enablement.
An impairment loss is recognized if the carrying value of a reporting unit exceeds its fair value. If this event arises, the impairment loss recorded is equal to the excess of the carrying value of the reporting unit over its fair value.
At least annually, indefinite-lived intangible assets are tested for impairment. Impairment for intangible assets with indefinite lives exists if the carrying value of the intangible asset exceeds its fair value. The fair values of indefinite-lived intangible assets are determined using valuation techniques based on estimates, judgments, and assumptions management believes are appropriate in the circumstances.
The Company had no
Investments in Other Entities – Equity Method
The Company accounts for certain investments using the equity method of accounting when it is determined that the investment provides the Company with the ability to exercise significant influence, but not control, over the investee. Significant influence is generally deemed to exist if the Company has an ownership interest in the voting stock of the investee of between 20% and 50%, although other factors, such as representation on the investee’s board of directors, are considered in determining whether the equity method of accounting is appropriate. Under the equity method of accounting, the investment, originally recorded at cost, is adjusted to recognize the Company’s share of net earnings or losses of the investee and is recognized in the accompanying consolidated statements of income under “Income (loss) from equity method investments” and also is adjusted by contributions to and distributions from the investee.
Investments in Privately Held Entities
The Company accounts for certain investments using the cost method of accounting when it is determined that the investment provides the Company with little or no influence over the investee. Under the cost method of accounting, the investment is measured at cost, adjusted for observable price changes and impairments, with changes recognized in net income. The investments in privately held entities that do not report net asset value are subject to qualitative assessment for indicators of impairments.
Medical Liabilities
The Company’s Care Partners segment is responsible for integrated care that the associated physicians and contracted hospitals provide to their enrollees. The Company’s Care Partners segment provides integrated care to HMOs, Medicare, and Medi-Cal enrollees through a network of contracted providers under sub-capitation and direct patient service arrangements. Medical costs for professional and institutional services rendered by contracted providers are recorded as cost of services, excluding depreciation and amortization, in the accompanying consolidated statements of income.
93
Fiduciary Cash and Payable
Revenue Recognition
The Company receives payments from the following sources for services rendered:
•Commercial insurers;
•Federal government under the Medicare program administered by CMS;
•State governments under Medicaid and other programs;
•Other third-party payers (e.g., hospitals and IPAs); and
•Individual patients and clients.
Revenue primarily consists of the following:
•Capitation revenue;
•Risk pool settlements and incentives;
•GPDC/ACO REACH capitation revenue;
•Management fee income; and
•FFS revenue.
Revenue is recorded in the period in which services are rendered or the period in which the Company is obligated to provide services. The form of billing and related risk of collection for such services may vary by type of revenue and the customer.
Nature of Services and Revenue Streams
Revenue primarily consists of capitation revenue, risk pool settlements and incentives, GPDC/ACO REACH capitation revenue, management fee income, and FFS revenue. Revenue is recorded in the period in which services are rendered or the period in which the Company is obligated to provide services. The form of billing and related risk of collection for such services may vary by type of revenue and the customer. The following is a summary of the principal forms of the Company’s billing arrangements and how revenue is recognized for each.
Capitation, Net
Managed care revenues of the Company consist primarily of capitated fees for medical services provided by the Company under a capitated arrangement directly made with various managed care providers, including HMOs. Capitation revenue is
94
typically prepaid monthly to the Company based on the number of enrollees selecting the Company as their healthcare provider. Capitation revenue is recognized in the month in which the Company is obligated to provide services to plan enrollees under contracts with various health plans. Minor ongoing adjustments to prior months’ capitation, primarily arising from contracted HMOs finalizing their monthly patient eligibility data for additions or subtractions of enrollees, are recognized in the month they are communicated to the Company. Additionally, Medicare pays capitation using a “Risk Adjustment” model, which compensates managed care organizations and providers based on the health status (acuity) of each individual enrollee. Health plans and providers with higher acuity enrollees will receive more and those with lower acuity enrollees will receive less. Under Risk Adjustment, capitation is determined based on health severity, measured using patient encounter data. Capitation is paid on a monthly basis based on data submitted for the enrollee for the preceding year and is adjusted in subsequent periods after the final data is compiled. Positive or negative capitation adjustments are made for Medicare enrollees with conditions requiring more or fewer healthcare services than assumed in the interim payments. Since the Company cannot reliably predict these adjustments, periodic changes in capitation amounts earned as a result of Risk Adjustment are recognized when those changes are communicated by the health plans to the Company.
Per member per month (“PMPM”) managed care contracts generally have a term of one year or longer. The Company assesses the profitability of its managed care contracts to identify contracts where current operating results or forecasts indicate probable future losses. If anticipated future variable costs exceed anticipated future revenues, a premium deficiency reserve is recognized. No premium deficiency reserves were recorded as of December 31, 2023. All managed care contracts have a single performance obligation that constitutes a series for the provision of managed healthcare services for a population of enrolled members for the duration of the contract. The transaction price for PMPM contracts is variable as it primarily includes PMPM fees associated with unspecified membership that fluctuates throughout the contract. In certain contracts, PMPM fees also include adjustments for items such as performance incentives, performance guarantees, and risk sharing. The Company generally estimates the transaction price using the most likely amount methodology and amounts are only included in the net transaction price to the extent that it is probable that a significant reversal of cumulative revenue will not occur once any uncertainty is resolved. The majority of the Company’s net PMPM transaction price relates specifically to the Company’s efforts to transfer the service for a distinct increment of the series (e.g., day or month) and is recognized as revenue in the month in which members are entitled to service.
GPDC/ACO REACH Capitation Revenue
CMS contracts with ACOs, which are composed of healthcare providers operating under a common legal structure and accept financial accountability for the overall quality and cost of medical care furnished to Medicare FFS beneficiaries aligned to the entity. The combination of the FFS model and the GPDC/ACO REACH model changes the distribution of responsibilities, risks, costs, and rewards among CMS, ACOs and providers. By entering into a contract with CMS, an ACO voluntarily takes on operational, financial, and legal responsibilities and risks that no party has, individually or collectively, under the existing FFS model. Each ACO bears the economic costs, and reaps the economic rewards, of fulfilling its responsibilities and managing its risks as an ACO. APAACO has participated in ACO REACH, and its predecessor model, Global and Professional Direct Contracting Model (“GPDC Model”), since January 1, 2022.
For each performance year, CMS will pay a total benchmark amount, determined unilaterally by CMS in advance but subject to prospective adjustments throughout the year, for the totality of care provided to the ACO’s population of aligned beneficiaries over the course of that year. The benchmark is net of a quality withholding applied by CMS. At the end of each performance year, a portion, or all, of the quality withholding can be earned based on APAACO’s performance. ACO REACH capitation revenue is recognized based on the estimated transaction price to transfer the service for a distinct increment of the series (i.e., month) and is recognized net of quality incentives/penalties. ACO REACH capitation revenue is recognized in the accompanying consolidated statements of income under capitation, net.
Risk Pool Settlements and Incentives
95
Certain IPAs enter into hospital shared-risk capitation arrangements with certain health plans and local hospitals, where the hospital is responsible for providing, arranging and paying for institutional risk and the IPA is responsible for providing, arranging, and paying for professional risk. Under a hospital shared-risk pool-sharing agreement, the IPA generally receives a percentage of the net surplus from the affiliated hospital’s risk pools with HMOs after deductions for the affiliated hospital’s costs. Advance settlement payments are typically made quarterly in arrears if there is a surplus. The Company’s risk pool settlements under arrangements with health plans and hospitals are recognized using the most likely amount methodology and amounts are only included in revenue to the extent that it is probable that a significant reversal of cumulative revenue will not occur once any uncertainty is resolved. The assumptions for historical margin, IBNR completion factors, and constraint percentages were used by management in applying the most likely amount methodology.
Under capitated arrangements with certain HMOs, certain IPAs participate in one or more health plan shared-risk arrangements relating to the provision of institutional services to enrollees and thus can earn additional revenue or incur losses based upon the enrollee utilization of institutional services. Health plan shared-risk arrangements are entered into with certain health plans, which are administered by the health plan, where the IPA is responsible for rendering professional services, but the health plan does not enter into a capitation arrangement with a hospital and therefore the health plan retains the institutional risk. Health plan shared-risk deficits, if any, are not payable until and unless (and only to the extent) risk-sharing surpluses are generated. At the termination of the HMO contract, any accumulated deficit will be extinguished.
The Company's risk pool settlements under arrangements with HMOs are recognized, using the most likely methodology, and only included in revenue to the extent that it is probable that a significant reversal of cumulative revenue will not occur. Given the lack of access to the health plans’ data and control over the members assigned to the IPA, the adjustments and/or the withheld amounts are unpredictable and as such, the IPA’s risk-share revenues are deemed to be fully constrained until they are notified of the amount by the health plan. Final settlement of risk pools for prior contract years generally occur in the third or fourth quarter of the following year.
In addition to risk-sharing revenues, the Company also receives incentives under “pay-for-performance” programs for quality medical care, based on various criteria. As an incentive to promote quality care, certain HMOs have designed quality incentive programs and commercial generic pharmacy incentive programs to compensate the Company for its efforts to improve the quality of services and efficient and effective use of pharmacy supplemental benefits provided to HMO members. The incentive programs track specific performance measures and calculate payments to the Company based on the performance measures. The Company’s incentives under “pay-for-performance” programs are recognized using the most likely methodology. However, as the Company does not have sufficient insight from the health plans on the amount and timing of the health plan shared-risk pool and incentive payments, these amounts are considered to be fully constrained and only recorded when such payments are known and/or received.
Generally, for the foregoing arrangements, the final settlement is dependent on each distinct day’s performance within the annual measurement period but cannot be allocated to specific days until the full measurement period has occurred and performance can be assessed. As such, this is a form of variable consideration estimated at contract inception and updated through the measurement period (i.e., the contract year), to the extent the risk of reversal does not exist and the consideration is not constrained.
NGACO AIPBP Revenue
Under the NGACO Model, CMS aligned beneficiaries to the Company to manage direct care and pay providers based on a budgetary benchmark established with CMS. The Company was responsible for managing medical costs for these beneficiaries. The beneficiaries received services from physicians and other medical service providers that were both in-network and out-of-network. The Company received capitation-like All Inclusive Population Based Payment (“AIPBP”) payments from CMS on a monthly basis to pay claims from in-network providers. The Company recorded such AIPBPs received from CMS as revenue as the Company was primarily responsible and liable for managing the patient care and for satisfying provider obligations, was assuming the credit risk for the services provided by in-network providers through its arrangement with CMS, and had control of the funds, the services provided and the process by which the providers were ultimately paid. Claims from out-of-network providers were processed and paid by CMS, while claims from APAACO’s in-network contracted providers were paid by APAACO. The Company’s shared savings or losses in managing the services provided by out-of-network providers were generally determined on an annual basis after reconciliation with CMS. Pursuant to the Company’s risk share agreement with CMS, the Company was eligible to receive the savings or was liable for the deficit according to the budget established by CMS based on the Company’s efficiency in managing how the beneficiaries aligned to the Company by CMS were served by in-network and out-of-network providers. The Company’s savings or losses on providing such services were both capped by CMS,
96
and were subject to significant estimation risk, whereby payments would vary significantly depending upon certain patient characteristics and other variable factors. Accordingly, the Company recognized such surplus or deficit upon substantial completion of reconciliation and determination of the amounts. The Company recorded NGACO AIPBP revenues monthly. Excess AIPBPs over claims paid, plus an estimate for the related IBNR claims were deferred and recorded as a liability until actual claims were paid or incurred. CMS determined if there were any excess AIPBPs for the performance year and the excess was refunded to CMS.
For each performance year, CMS paid the Company in accordance with the alternative payment mechanism, if any, for which CMS had approved the Company; the risk arrangement for which the Company has been approved by CMS, and was otherwise provided in an NGACO Participation Agreement between APAACO and CMS (the “Participation Agreement”). Following the end of each performance year and at such other times as would be required under the Participation Agreement, CMS would issue a settlement report to the Company setting forth the amount of any shared savings or shared losses and the amount of other monies. If CMS owed the Company shared savings or other monies, CMS would pay the Company in full within 30 days after the date on which the relevant settlement report was deemed final, except as provided in the Participation Agreement. If the Company owed CMS shared losses or other monies owed as a result of a final settlement, the Company would pay CMS in full within 30 days after the relevant settlement report was deemed final. If the Company failed to pay the amounts due to CMS in full within 30 days after the date of a demand letter or settlement report, CMS would assess simple interest on the unpaid balance at the rate applicable to other Medicare debts under current provisions of law and applicable regulations. In addition, CMS and the U.S. Department of the Treasury would use any applicable debt collection tools available to collect any amounts owed by the Company.
The Company participated in the AIPBP track of the NGACO Model. Under the AIPBP track, CMS estimated the total annual expenditures for APAACO’s assigned patients and paid that projected amount to the Company in monthly installments, and the Company was responsible for all Part A and Part B costs for in-network participating providers and preferred providers contracted by the Company to provide services to the assigned patients.
As APAACO did not have sufficient insight into the financial performance of the shared risk pool with CMS because of unknown factors related to IBNR claims, risk adjustment factors, and stop-loss provisions, among other factors, an estimate couldn’t be developed. Due to these limitations, APAACO could not determine the amount of surplus or deficit that would likely be recognized in the future and therefore this shared risk pool revenue was considered fully constrained. With the ending of the NGACO Model on December 31, 2021, the Company no longer received AIPBPs but remained eligible to recognize any shared savings or loss for performance year 2021 upon issuance of the settlement report from CMS. Pursuant to the Participation Agreement, the Company recognized $48.8 million related to savings from the 2021 performance year as revenue in risk pool settlements and incentives in the accompanying consolidated statements of income for the year ended December 31, 2022.
Management Fee Income
Management fee income encompasses fees paid for management, physician advisory, healthcare staffing, administrative, and other non-medical services provided by the Company to IPAs, hospitals, and other healthcare providers. Such fees may be in the form of billings at agreed-upon hourly rates, percentages of gross revenue or fee collections, or amounts fixed on a monthly, quarterly, or annual basis. The revenue may include variable arrangements measuring factors, such as hours staffed, patient visits, or collections per visit, against benchmarks, and, in certain cases, may be subject to achieving quality metrics or fee collections. The Company recognizes such variable supplemental revenues in the period when such amounts are determined to be fixed and therefore contractually obligated as payable by the customer under the terms of the applicable agreement.
The Company provides a significant service of integrating the services selected by the Company’s clients into one overall output for which the client has contracted. Therefore, such management contracts generally contain a single performance obligation. The nature of the Company’s performance obligation is to stand ready to provide services over the contractual period. Also, the Company’s performance obligation forms a series of distinct periods of time over which the Company stands ready to perform. The Company’s performance obligation is satisfied as the Company completes each period’s obligations.
Consideration from management contracts is variable in nature because the majority of the fees are generally based on revenue or collections, which can vary from period to period. The Company has control over pricing. Contractual fees are invoiced to the Company’s clients generally monthly and payment terms are typically due within 30 days. The variable consideration in the Company’s management contracts meets the criteria to be allocated to the distinct period of time to which it relates because (i)
97
it is due to the activities performed to satisfy the performance obligation during that period and (ii) it represents the consideration to which the Company expects to be entitled.
The Company’s management contracts generally have terms ranging from to thirty years , although they may be terminated earlier under the terms of the applicable contracts. Since the remaining variable consideration will be allocated to a wholly unsatisfied promise that forms part of a single performance obligation recognized under the series guidance, the Company has applied the optional exemption to exclude disclosure of the allocation of the transaction price to remaining performance obligations.
Fee-for-Service Revenue
FFS revenue represents revenue earned under contracts in which the professional component of charges for medical services rendered by the Company’s affiliated physician-owned medical groups are billed and collected from third-party payers, hospitals, and patients. FFS revenue related to patient care services is reported net of contractual allowances and policy discounts and is recognized in the period in which the services are rendered to specific patients. All services provided are expected to result in cash flows and are therefore reflected as net revenue in the consolidated financial statements. The recognition of net revenue (gross charges, less contractual allowances) from such services is dependent on such factors as proper completion of medical charts following a patient visit, the forwarding of such charts to the Company’s billing center for medical coding and entering into the Company’s billing system and the verification of each patient’s submission or representation at the time services are rendered as to the payer(s) responsible for payment of such services. Revenue is recorded based on the information known at the time of entering such information into the Company’s billing systems, as well as an estimate of the revenue associated with medical services.
The Company is responsible for confirming member eligibility, performing program utilization review, potentially directing payment to the provider and accepting the financial risk of loss associated with services rendered, as specified within the Company’s client contracts. The Company has the ability to adjust contractual fees with clients and possesses the financial risk of loss in certain contractual obligations. These factors indicate the Company is the principal and, as such, the Company records gross fees contracted with clients in revenues.
Consideration from FFS arrangements is variable in nature because fees are based on patient encounters, credits due to clients, and reimbursement of provider costs, all of which can vary from period to period. Patient encounters and related episodes of care and procedures qualify as distinct goods and services, provided simultaneously together with other readily available resources, in a single instance of service, and thereby constitute a single performance obligation for each patient encounter and, in most instances, occur at readily determinable transaction prices. As a practical expedient, the Company adopted a portfolio approach for the FFS revenue stream to group together contracts with similar characteristics and analyze historical cash collection trends. The contracts within the portfolio share the characteristics conducive to ensuring that the results do not materially differ under the new standard if it were to be applied to individual patient contracts related to each patient encounter.
Estimating net FFS revenue is a complex process, largely due to the volume of transactions, the number and complexity of contracts with payers, the limited availability at times of certain patient and payer information at the time services are provided, and the length of time it takes for collections to fully mature. These expected collections are based on fees and negotiated payment rates in the case of third-party payers, the specific benefits provided for under each patient’s healthcare plans, mandated payment rates in the case of Medicare and Medicaid programs, and historical cash collections (net of recoveries) in combination with expected collections from third-party payers.
The relationship between gross charges and the transaction price recognized is significantly influenced by payer mix, as collections on gross charges may vary significantly, depending on whether the patients, to whom services are provided, in the period are insured and the contractual relationships with those payers. Payer mix is subject to change as additional patient and payer information is obtained after the period services are provided. The Company periodically assesses the estimates of unbilled revenue, contractual adjustments and discounts, and payer mix by analyzing actual results, including cash collections, against estimates. Changes in these estimates are charged or credited to the consolidated statements of income in the period that the assessment is made. Significant changes in payer mix, contractual arrangements with payers, specialty mix, acuity, general economic conditions, and healthcare coverage provided by federal or state governments or private insurers may have a significant impact on estimates and significantly affect the results of operations and cash flows.
Contract Assets
98
Revenues and receivables are recognized once the Company has satisfied its performance obligation. Accordingly, contract assets are comprised of receivables and receivables - related parties.
The Company’s billing and accounting systems provide historical trends of cash collections and contractual write-offs, accounts receivable aging, and established fee adjustments from third-party payers. These estimates are recorded and monitored monthly as revenues are recognized. The principal exposure for uncollectible fees for service visits is from self-pay patients and, to a lesser extent, for co-payments and deductibles from patients with insurance.
Contract Liabilities (Deferred Revenue)
Income Taxes
Income taxes are accounted for using the asset and liability method. Deferred tax assets and liabilities are recognized for the future tax consequences attributable to differences between the consolidated financial statement carrying amounts of existing assets and liabilities and their respective tax bases. Deferred tax assets and liabilities are measured using the enacted tax rates expected to apply to taxable income in the years in which those temporary differences are expected to be recovered or settled. The effect on deferred tax assets and liabilities of a change in tax rates is recognized in income in the period of enactment. The Company records a valuation allowance to reduce deferred tax assets to an amount for which realization is more likely than not.
The Company recognizes the tax benefit from an uncertain tax position if it is more likely than not that the tax position will be sustained upon examination by the tax authorities, based on the merits of the position. The Company’s policy is to recognize interest and penalties related to the underpayment of income taxes as a component of income tax expense or benefit. To date, there have been no interest or penalties incurred in relation to the unrecognized tax benefits.
Share-Based Compensation
The Company maintains a stock-based compensation program for employees, non-employees, directors, and consultants. From time to time, the Company issues shares of its common stock to its employees, directors, and consultants, which shares may be subject to the Company’s repurchase right (but not obligation), that vests based on time-based and/or performance-based vesting schedules. The value of share-based awards is recognized as compensation expense and adjusted for forfeitures as they occur. Compensation expenses for time-based awards are recognized on a cumulative straight-line basis over the vesting period of the awards. Share-based awards with performance conditions are recognized to the extent the performance conditions are probable of being achieved. Compensation expenses for performance-based awards are recognized on an accelerated attribution method. The grant date fair value of the restricted stock awards is the grant date’s closing market price of the Company’s common stock. The fair value of options granted is determined using the Black-Scholes option pricing model and includes several assumptions, including expected term, expected volatility, expected dividends, and risk-free rates. The expected term is presumed to be the midpoint between the vesting date and the end of the contractual term. The expected stock price volatility is determined based on an average of historical volatility. The expected dividend yield is based on the Company’s expected dividend payouts. The risk-free interest rate is based on the U.S. Constant Maturity curve over the expected term of the option at the time of grant.
Basic and Diluted Earnings Per Share
Basic earnings per share (“EPS”) is computed by dividing net income attributable to holders of the Company’s common stock by the weighted-average number of shares of common stock outstanding during the periods presented. Diluted earnings per share is computed using the weighted-average number of shares of common stock outstanding, plus the effect of dilutive securities outstanding during the periods presented, using the treasury stock method. Refer to Note 17 — “Earnings Per Share” for a discussion of shares treated as treasury shares for accounting purposes.
Non-controlling Interests
99
The Company consolidates entities in which the Company has a controlling financial interest. The Company consolidates subsidiaries in which the Company holds, directly or indirectly, more than 50 % of the voting rights, and VIEs in which the Company is the primary beneficiary. Non-controlling interests represent third-party equity ownership interests (including equity ownership interests held by certain VIEs) in the Company’s consolidated entities. Net income attributable to non-controlling interests is disclosed in the consolidated statements of income.
Mezzanine Equity
Leases
The Company determines if an arrangement is a lease at its inception. The expected term of the lease used for computing the lease liability and right-of-use asset and determining the classification of the lease as operating or financing may include options to extend or terminate the lease when it is reasonably certain that the Company will exercise that option. The Company elected practical expedients for ongoing accounting that is provided by the standard comprised of the following:
•The election for classes of underlying assets to not separate non-lease components from lease components, and
•The election for short-term lease recognition exemption for all leases under twelve-month terms.
The present value of the lease payments is calculated using a rate implicit in the lease, when readily determinable. However, as most of the Company’s leases do not provide an implicit rate, the Company uses its incremental borrowing rate to determine the present value of the lease payments for the majority of its leases.
Beneficial Interest
In April 2020, APC received a beneficial interest as a result of selling one of its equity method investments, pursuant to the terms of the stock purchase agreement. The estimated fair value of such interest in April 2020 was $15.7 million. In 2021, the beneficial interest was determined to not be collectible and the $15.7 million was written off and expensed in other income (expense) in the accompanying consolidated statements of income for the year ended December 31, 2021.
Recent Accounting Pronouncements Not Yet Adopted
In November 2023, the Financial Standards Accounting Board (FASB) issued Accounting Standards Update (ASU) 2023-07 "Segment Reporting (Topic 280): Improvements to Reportable Segment Disclosures" which expands annual and interim disclosure requirements for reportable segments, primarily through enhanced disclosures about significant segment expenses. ASU 2023-07 is effective for the Company’s annual periods beginning January 1, 2024, and for interim periods beginning January 1, 2025, with early adoption permitted. The Company is currently evaluating the potential effect that the updated standard will have on its financial statement disclosures.
In December 2023, the FASB issued ASU 2023-09 "Income Taxes (Topics 740): Improvements to Income Tax Disclosures" to expand the disclosure requirements for income taxes, specifically related to the rate reconciliation and income taxes paid. ASU 2023-09 is effective for the Company’s annual periods beginning January 1, 2025, with early adoption permitted. The Company is currently evaluating the potential effect that the updated standard will have on its financial statement disclosures.
100
3. Business Combinations, Asset Acquisitions, and Goodwill
Texas Independent Providers, LLC (“TIP”)
On September 1, 2023, the Company acquired certain assets relating to TIP. The acquired assets allow the Company to provide high-quality care services to Medicare Advantage patients in Texas. The purchase price consisted of cash funded on September 1, 2023.
For Your Benefit, Inc. (“FYB”)
On May 1, 2023, the Company acquired 100 % of the equity interest in FYB. FYB is licensed by the California Department of Managed Health Care as a full-service Restricted Knox-Keene licensed health plan to serve Medicare Advantage members only in designated California counties. As a Restricted Knox-Keene licensed health plan, FYB is not permitted to market directly to Medicare beneficiaries, but rather, contracts with “upstream” Medicare Advantage payer plans on a “global capitation” basis, which enables FYB to assume full financial responsibility, including both professional and institutional risk, for the medical costs of its Medicare Advantage members under the Knox-Keene Health Care Service Plan Act of 1975.
Chinese Community Health Care Association (“CCHCA”)
On March 1, 2023, the Company acquired certain healthcare assets from CCHCA. The acquired assets allow the Company to provide high-quality care to more patients in the San Francisco Community. The purchase price consisted of cash funded on May 1, 2023.
All American Medical Group (“AAMG”)
On October 31, 2022, Astrana Care Partners Medical Corporation (“Astrana Care Partners Medical”), formerly known as AP-AMH 2 Medical Corporation, a consolidated VIE of the Company, acquired 100 % of the equity interest in AAMG. AAMG is an IPA operating in Northern California. The purchase price consisted of cash funded upon close of the transaction and additional consideration (“AAMG contingent consideration”) and stock consideration (“AAMG stock contingent consideration”) contingent on AAMG meeting revenue and capitated member metrics for fiscal year 2023 and 2024. The fair value of the AAMG contingent consideration and AAMG stock contingent consideration on the date of acquisition was $5.9 million and $5.6 million, respectively. Refer to Note 21 - “Fair Value Measurements of Financial Instruments” for additional information on contingent considerations.
Valley Oaks Medical Group (“VOMG”)
On October 14, 2022, one of the Company’s key personnel acquired 100 % of the equity interest in VOMG, resulting in the Company consolidating VOMG as a VIE. VOMG owns primary care clinics in Nevada and Texas. The purchase price consists of cash funded upon the close of transaction and additional cash consideration (“VOMG contingent consideration”) contingent on VOMG meeting financial metrics for fiscal years 2023 and 2024. Refer to Note 21 - “Fair Value Measurements of Financial Instruments” for additional information on contingent considerations.
Jade Health Care Medical Group, Inc. (“Jade”)
On April 19, 2022, the Company acquired 100 % of the capital stock of Jade. The purchase was paid in cash. Jade is a primary and specialty care physicians’ group focused on providing high-quality care to its patients in the San Francisco Bay Area in Northern California.
Orma Health, Inc., and Provider Growth Solutions LLC (together, “Orma Health”)
On January 27, 2022, the Company acquired 100 % of the capital stock of Orma Health, Inc., and Provider Growth Solutions, LLC (together, “Orma Health”). The purchase was paid in cash and in the Company’s capital stock. Orma Health’s real-time Clinical AI platform ingests data from multiple sources and utilizes advanced risk-stratification models to identify patients for various clinical programs, including remote patient monitoring (“RPM”), mental health support, chronic care management, and more. Its clinical platform is also deeply integrated with Orma Health’s proprietary RPM ecosystem, which consists of smart health devices and a suite of technology tools to manage patient health.
The acquisitions were accounted for under the acquisition method of accounting. The fair value of the consideration for the acquired companies were allocated to acquired tangible and intangible assets and liabilities based upon their fair values. The
101
excess of the purchase consideration over the fair value of the net tangible and identifiable intangible assets acquired was recorded as goodwill. The determination of the fair value of assets and liabilities acquired requires the Company to make estimates and use valuation techniques when market value is not readily available. The results of operations of the acquisitions have been included in the Company’s consolidated financial statements from the date of acquisition. Transaction costs associated with business acquisitions are expensed as they are incurred.
At the time of acquisition, the Company estimates the amount of the identifiable intangible assets based on a valuation and the facts and circumstances available at the time. The Company determines the final value of the identifiable intangible assets as soon as information is available, but not more than one year from the date of acquisition.
Goodwill is not deductible for tax purposes.
The change in the carrying value of goodwill for the years ended December 31, 2023 and 2022 was as follows (in thousands):
| Amount | |||||
| Balance at January 1, 2022 | $ | ||||
| Acquisitions | |||||
| Adjustments | |||||
| Balance at December 31, 2022 | |||||
| Acquisitions | |||||
| Adjustments | |||||
| Balance at December 31, 2023 | $ | ||||
102
4. Land, Property, and Equipment, Net
Land, property, and equipment, net consisted of (in thousands):
| Useful Life (Years) | December 31, 2023 | December 31, 2022 | |||||||||||||||
Land* |
N/A | $ | $ | ||||||||||||||
Buildings* |
|||||||||||||||||
| Computer software | |||||||||||||||||
| Furniture and equipment | |||||||||||||||||
Construction in progress* |
N/A | ||||||||||||||||
| Leasehold improvements | |||||||||||||||||
| Less accumulated depreciation and amortization | ( |
( |
|||||||||||||||
| Land, property, and equipment, net | $ | $ | |||||||||||||||
*Certain land, property, and equipment, net that were deemed Excluded Assets that are solely for the benefit of APC and its common shareholders were spun-off as part of the Spin-Off. Refer to Note 1 — “Description of Business” to the consolidated financial statements for information on the Spin-Off.
As of December 31, 2023 and 2022, the Company had finance leases totaling $1.7 million and $1.8 million, respectively, included in land, property, and equipment, net in the accompanying consolidated balance sheets.
5. Intangible Assets, Net
At December 31, 2023, intangible assets, net consisted of the following (in thousands):
| Useful Life (Years) |
Gross January 1, 2023 |
Additions | Impairment/ Disposal |
Gross December 31, 2023 |
Accumulated Amortization |
Net December 31, 2023 |
|||||||||||||||||||||||||||||||||||
| Indefinite lived assets: | |||||||||||||||||||||||||||||||||||||||||
| Trademarks | N/A | $ | $ | $ | $ | $ | — | $ | |||||||||||||||||||||||||||||||||
| Amortized intangible assets: | |||||||||||||||||||||||||||||||||||||||||
| Network relationships | ( |
||||||||||||||||||||||||||||||||||||||||
| Management contracts | ( |
||||||||||||||||||||||||||||||||||||||||
| Member relationships | ( |
||||||||||||||||||||||||||||||||||||||||
| Patient management platform | ( |
||||||||||||||||||||||||||||||||||||||||
| Tradename/trademarks | ( |
||||||||||||||||||||||||||||||||||||||||
| Developed technology | ( |
||||||||||||||||||||||||||||||||||||||||
| $ | $ | $ | $ | $ | ( |
$ | |||||||||||||||||||||||||||||||||||
103
At December 31, 2022, intangible assets, net consisted of the following (in thousands):
| Useful Life (Years) |
Gross January 1, 2022 | Additions | Impairment/ Disposal |
Gross December 31, 2022 |
Accumulated Amortization |
Net December 31, 2022 |
|||||||||||||||||||||||||||||||||||
| Indefinite Lived Assets: | |||||||||||||||||||||||||||||||||||||||||
| Trademarks | N/A | $ | $ | $ | $ | $ | — | $ | |||||||||||||||||||||||||||||||||
| Amortized intangible assets: | |||||||||||||||||||||||||||||||||||||||||
| Network relationships | ( |
||||||||||||||||||||||||||||||||||||||||
Management contracts |
( |
||||||||||||||||||||||||||||||||||||||||
| Member relationships | ( |
||||||||||||||||||||||||||||||||||||||||
| Patient management platform | ( |
||||||||||||||||||||||||||||||||||||||||
Tradename/trademarks |
( |
||||||||||||||||||||||||||||||||||||||||
Developed technology |
( |
||||||||||||||||||||||||||||||||||||||||
| $ | $ | $ | $ | $ | ( |
$ | |||||||||||||||||||||||||||||||||||
As of December 31, 2023, network relationships, management contracts, member relationships, tradename/trademarks, and developed technology had weighted-average remaining useful lives of 9.4 years, 6.5 years, 11.1 years, 13.9 years, and 4.1 years respectively. Total weighted-average remaining useful lives for all amortized intangible assets as of December 31, 2023 was 9.6 years. Amortization expense was $12.7 million, $13.7 million and $15.4 million for the years ended December 31, 2023, 2022, and 2021, respectively, which is included in depreciation and amortization in the accompanying consolidated statements of income.
There was no impairment loss recorded related to intangibles for the years ended December 31, 2023, 2022 and 2021.
Future amortization expense is estimated to be as follows for the years ending December 31 (in thousands):
| Amount | |||||
| 2024 | $ | ||||
| 2025 | |||||
| 2026 | |||||
| 2027 | |||||
| 2028 | |||||
| Thereafter | |||||
| $ | |||||
104
6. Investments in Other Entities
Equity Method
For the twelve months ended December 31, 2023 and 2022, the Company’s equity method investment balance consisted of the following (in thousands):
| % of Ownership | December 31, 2022 |
Initial Investment | Allocation of Net Income (Loss) | Funding | Adjustment of Fair Value* | Distribution | December 31, 2023 |
||||||||||||||||||||||||||||||||||||||||
| LaSalle Medical Associates – IPA Line of Business | $ | $ | $ | $ | $ | $ | $ | ||||||||||||||||||||||||||||||||||||||||
| Pacific Medical Imaging & Oncology Center, Inc. | ( |
||||||||||||||||||||||||||||||||||||||||||||||
| 531 W. College, LLC * | ( |
( |
|||||||||||||||||||||||||||||||||||||||||||||
| One MSO, LLC * | ( |
||||||||||||||||||||||||||||||||||||||||||||||
| CAIPA MSO, LLC | |||||||||||||||||||||||||||||||||||||||||||||||
| Other ** | |||||||||||||||||||||||||||||||||||||||||||||||
| $ | $ | $ | $ | $ | $ | ( |
$ | ||||||||||||||||||||||||||||||||||||||||
* Investments deemed Excluded Assets that are solely for the benefit of APC and its common shareholders. These Excluded Assets were spun-off on December 26, 2023 as part of the Spin-Off. On the date of distribution, the investments were recorded at fair value. The gain, representing the difference between the fair value and the carrying value of the investment, was $3.4 million and is presented within other income in the accompanying consolidated statement of net income. Refer to Note 1 — “Description of Business” to the consolidated financial statements for information on the Spin-Off.
** Other consists of smaller equity method investments.
| % of Ownership | December 31, 2021 | Allocation of Net Income (Loss) | Funding Reclassified to Loan Receivable | Funding | Entity Consolidated | Distribution | December 31, 2022 | ||||||||||||||||||||||||||||||||||||||||
| LaSalle Medical Associates – IPA Line of Business | $ | $ | $ | ( |
$ | $ | $ | $ | |||||||||||||||||||||||||||||||||||||||
| Pacific Medical Imaging & Oncology Center, Inc. | |||||||||||||||||||||||||||||||||||||||||||||||
| 531 W. College, LLC * | ( |
||||||||||||||||||||||||||||||||||||||||||||||
| One MSO, LLC * | ( |
||||||||||||||||||||||||||||||||||||||||||||||
| Tag-6 Medical Investment Group, LLC* | ( |
||||||||||||||||||||||||||||||||||||||||||||||
| CAIPA MSO, LLC | |||||||||||||||||||||||||||||||||||||||||||||||
| $ | $ | $ | ( |
$ | $ | ( |
$ | ( |
$ | ||||||||||||||||||||||||||||||||||||||
* Investments deemed Excluded Assets that are solely for the benefit of APC and its common shareholders. These Excluded Assets were spun-off on December 26, 2023 as part of the Spin-off. Refer to Note 1 — “Description of Business” to the consolidated financial statements for information on the Spin-Off.
Equity method investments are subject to impairment evaluation. There was no impairment loss recorded related to equity method investments for the years ended December 31, 2023, 2022, and 2021.
Investments in privately held entities that do not report net asset value
MediPortal, LLC
In May 2018, APC purchased 270,000 membership interests of MediPortal LLC, a New York limited liability company, for $0.4 million or $1.50 per membership interest, which represented approximately 2.8 % ownership interest. In connection with
105
the initial purchase, APC received a five-year warrant to purchase an additional 270,000 membership interests. A five-year option to purchase an additional 380,000 membership interests and a -year warrant to purchase 480,000 membership interests were contingent upon the portal completion date. These warrants and options were not exercised and are expired as of December 31, 2023. As APC does not have the ability to exercise significant influence, and lacks control over the investee, this investment is accounted for using a measurement alternative, which allows the investment to be measured at cost, adjusted for observable price changes and impairments, with changes recognized in net income. During the years ended December 31, 2023 and 2022, there were no observable price changes to APC’s investment.
AchievaMed
In July 2019, Astrana Health Management, Inc. (“AHM”), formerly known as Network Medical Management Inc., and AchievaMed, Inc., a California corporation (“AchievaMed”), entered into an agreement in which AHM would purchase 50 % of the aggregate shares of capital stock of AchievaMed over a period of time not to exceed five years . As a result of this transaction, AHM invested $0.5 million for a 10 % interest. The related investment balance of $0.5 million is included in investments in privately held entities in the accompanying consolidated balance sheets as of December 31, 2023. As AHM does not have the ability to exercise significant influence, and lacks control, over the investee, this investment is accounted for using a measurement alternative, which allows the investment to be measured at cost, adjusted for observable price changes and impairments, with changes recognized in net income. During the years ended December 31, 2023 and 2022, there were no observable price changes to AHM’s investment.
Third Way Health, Inc.
In August 2022, the Company entered into a Simple Agreement for Future Equity (“SAFE”) with Third Way Health, Inc. (“Third Way Health”). Based on certain triggering events defined in the SAFE, the Company has rights to Third Way Health’s shares. The number of shares to be acquired will be calculated when the triggered event occurs. As of December 31, 2023 and 2022, the related investment balance of $3.5 million and $1.5 million, respectively, is included in investments in privately held entities in the accompanying consolidated balance sheets. As the Company does not have the ability to exercise significant influence, and lacks control, over the investee, this investment is accounted for using a measurement alternative, which allows the investment to be measured at cost, adjusted for observable price changes and impairments, with changes recognized in net income. During the years ended December 31, 2023 and 2022, there were no observable price changes to the Third Way Health investment.
Seen Health, Inc.
On April 1, 2023, the Company entered into a SAFE with Seen Health, Inc. (“Seen Health”). Based on certain triggering events defined in the SAFE, the Company has rights to Seen Health’s shares. The number of shares to be acquired will be calculated when the triggering event occurs. As of December 31, 2023, the related investment balance of $2.0 million is included in investments in privately held entities in the accompanying consolidated balance sheets. As the Company does not have the ability to exercise significant influence, and lacks control, over the investee, this investment is accounted for using a measurement alternative, which allows the investment to be measured at cost, adjusted for observable price changes and impairments, with changes recognized in net income. During the year ended December 31, 2023, there were no observable price changes to the Seen Health investment.
7. Loan Receivable and Loan Receivable – Related Parties
Loans receivable
Pacific6
In October 2020, AHM received a promissory note from 6 Founder LLC, a California limited liability company doing business as Pacific6 Enterprises totaling $0.5 million as a result of the sale of the Company’s interest in MWN. Interest accrues at a rate of 5 % per annum and is payable monthly through the maturity date of December 1, 2023.
IntraCare
106
On July 27, 2023, the Company entered into a five-year convertible promissory note with IntraCare as the borrower. The principal on the note is $25.0 million, with interest on the outstanding principal amount and unpaid interest at a rate per annum equal to 8.81 %, compounded annually. In the event that the convertible promissory note remains outstanding on or after the maturity date of July 27, 2028, the outstanding principal balance and any unpaid accrued interest shall, upon the election of the Company, convert into IntraCare preferred shares. As of December 31, 2023, the related note balance of $26.0 million is included in loan receivable, non-current in the accompanying consolidated balance sheets.
The Company assessed the outstanding loan receivable under the CECL model by assessing the party’s ability to pay by reviewing their interest payment history quarterly, financial history annually, and reassessing any identified insolvency risk.
Loan receivable — related party
LaSalle Medical Associates Loan (“LMA Loan”)
8. Accounts Payable and Accrued Expenses
The Company’s accounts payable and accrued expenses consisted of the following (in thousands):
| December 31, 2023 | December 31, 2022 | |||||||||||||
| Accounts payable and other accruals | $ | $ | ||||||||||||
| Capitation payable | ||||||||||||||
| Subcontractor IPA payable | ||||||||||||||
| Professional fees | ||||||||||||||
| Due to related parties | ||||||||||||||
| Contract liabilities | ||||||||||||||
| Accrued compensation | ||||||||||||||
| Other provider payable | ||||||||||||||
Total accounts payable and accrued expenses |
$ | $ | ||||||||||||
9. Medical Liabilities
The Company’s medical liabilities consisted of the following (in thousands):
107
| December 31, 2023 | December 31, 2022 | |||||||||||||
| Medical liabilities, beginning of year | $ | $ | ||||||||||||
| Acquired (see Note 3) | ||||||||||||||
| Components of medical care costs related to claims incurred: | ||||||||||||||
| Current period | ||||||||||||||
| Prior periods | ( |
|||||||||||||
| Total medical care costs | ||||||||||||||
| Payments for medical care costs related to claims incurred: | ||||||||||||||
| Current period | ( |
( |
||||||||||||
| Prior periods | ( |
( |
||||||||||||
| Total paid | ( |
( |
||||||||||||
| Adjustments | ( |
|||||||||||||
| Medical liabilities, end of year | $ | $ | ||||||||||||
10. Credit Facility, Bank Loans, and Lines of Credit
Credit Facility
The Company’s debt balance consists of the following (in thousands):
| December 31, 2023 | December 31, 2022 | ||||||||||
| Revolver Loan | $ | $ | |||||||||
| Term Loan | |||||||||||
| Real Estate Loans* | |||||||||||
| Construction Loan * | |||||||||||
| Promissory Note Payable | |||||||||||
| Total debt | |||||||||||
| Less: Current portion of debt | ( |
( |
|||||||||
| Less: Unamortized financing costs | ( |
( |
|||||||||
| Long-term debt | $ | $ | |||||||||
The estimated fair value of the Company’s long-term debt was determined using Level 2 inputs primarily related to comparable market prices. As of December 31, 2023 and 2022, the carrying value was not materially different from fair value, as the interest rates on the Company’s debt approximated rates currently available to the Company.
The following are the future commitments of the Company’s debt for the years ending December 31 (in thousands):
108
| Amount | |||||
| 2024 | $ | ||||
| 2025 | |||||
| 2026 | |||||
| 2027 | |||||
| 2028 | |||||
| Thereafter | |||||
| Total | $ | ||||
Credit Facility
Amended Credit Agreement
On June 16, 2021, the Company entered into an amended and restated credit agreement (as subsequently amended as described below, the “Amended Credit Agreement”) with Truist Bank, in its capacity as administrative agent for the lenders, issuing bank, swingline lender and lender, and the banks and other financial institutions from time to time party thereto, to, among other things, amend and restate that certain credit agreement, dated September 11, 2019, by and among the Company, Truist Bank, and certain lenders thereto, in its entirety. The Amended Credit Agreement provides for a five-year revolving credit facility to the Company of $400.0 million (“Revolver Loan”), which includes a letter of credit sub-facility of up to $25.0 million and a swingline loan sub-facility of $25.0 million. As of December 31, 2023, the Company did not have any outstanding borrowings under the Revolver Loan.
On December 20, 2022, the Company entered into the First Amendment to the Amended Credit Agreement in which all amounts borrowed under the Amended Credit Agreement as of the effective date were automatically converted from LIBOR Loans to SOFR Loans with an initial interest period of one month on and as of the amendment effective date. Amounts borrowed under the Revolver Loan bear interest at an annual rate equal to either, at the Company’s option, (a) the Term SOFR Reference Rate (as defined in the Amended Credit Agreement), adjusted for any Term SOFR Adjustment (as defined in the Amended Credit Agreement) plus a spread ranging from 1.25 % to 2.50 %, as determined on a quarterly basis based on the Company’s Consolidated Total Net Leverage Ratio (as defined in the Amended Credit Agreement), or (b) a base rate, plus a spread ranging from 0.25 % to 1.50 %, as determined on a quarterly basis based on the Company’s Consolidated Total Net Leverage Ratio.
On September 8, 2023, a Second Amendment to the Amended Credit Agreement was entered into which, among other things, (i) increased the letter of credit sub-facility from $25.0 million to $50.0 million; (ii) revised the form of compliance certificate required to be submitted by the Company to the lenders on a quarterly basis; and (iii) waived the Specified Events of Default (as defined in the amendment) that occurred under the Amended Credit Agreement, relating to the Company’s calculation of Consolidated Total Net Leverage Ratio and payment of certain interest and letter of credit fees, in each case, for the periods from the quarter ended September 30, 2021 through the quarter ended March 31, 2023.
On November 3, 2023, the Company entered into a Third Amendment to the Amended Credit Agreement (“Third Amendment”) with Truist Bank and the other financial institutions party thereto. The Third Amendment provided a new term loan to the Company in an aggregate amount of up to $300.0 million, with $180.0 million funded at the closing of the Third Amendment, and $120.0 million available to be drawn by the Company as delayed draw loans during the six months subsequent to the closing of the Third Amendment (collectively, the “Term Loan”). The Term Loan matures on November 3, 2028 (or such earlier date on which it is terminated in accordance with the provisions of the Amended Credit Agreement) and amortizes quarterly at 5 % per annum for each of the first two years, 7.5 % per annum for years three and four, and 10 % per annum for year five. As of December 31, 2023, the Company made total drawdowns under the Term Loan of $280.0 million, of which $180.0 million was used to pay down outstanding amounts borrowed on the Revolver Loan as of the Third Amendment closing date.
The Company will pay a quarterly ticking fee on the delayed draw portion of the Term Loan, during the draw period, in an amount equal to 0.375 % per annum multiplied by the average daily unused portion of the delayed draw maximum amount. The
109
Term Loan will be secured by substantially all assets of the Company and subsidiaries of the Company that are not designated as excluded subsidiaries pursuant to the terms of the Amended Credit Agreement.
The Term Loan bears interest at an annual rate equal to either, at the Company’s option, (a) the Term SOFR Reference Rate, adjusted for any Term SOFR Adjustment, plus a spread from 1.50 % to 2.75 %, as determined on a quarterly basis based on the Company’s Consolidated Total Net Leverage Ratio, or (b) a base rate, plus a spread of 0.50 % to 1.75 %, as determined on a quarterly basis based on the Company’s Consolidated Total Net Leverage Ratio. As of December 31, 2023, the interest rate on the Term Loan was 7.69 %.
Under the Amended Credit Agreement, the Company is required to pay an annual agent fee of $50,000 and an annual facility fee of 0.175 % to 0.35 % on the available commitments under the Amended Credit Agreement, regardless of usage, with the applicable fee determined on a quarterly basis based on the Company’s Consolidated Total Net Leverage Ratio. The Company will pay fees for standby letters of credit at an annual rate equal to 1.25 % to 2.50 %, as determined on a quarterly basis based on the Company’s Consolidated Total Net Leverage Ratio, plus fronting fees and standard fees payable to the issuing bank on the respective letter of credit. The Company is also required to pay customary fees between the Company and Truist Bank, the lead arranger of the Amended Credit Agreement.
The Amended Credit Agreement requires the Company to comply with two key financial ratios, each calculated on a consolidated basis. The Company must maintain a maximum consolidated total net leverage ratio of not greater than 3.75 to 1.00 as of the last day of each fiscal quarter, provided that for any fiscal quarter during which the Company or certain subsidiaries consummate a permitted acquisition or investment, the aggregate purchase price is greater than $75.0 million, the maximum consolidated total net leverage ratio may temporarily increase by 0.25 to 1.00 to 4.00 to 1.00. The Company must maintain a minimum consolidated interest coverage ratio of not less than 3.25 to 1.00 as of the last day of each fiscal quarter. The Third Amendment also revised certain negative covenants in the Credit Agreement, providing the Company with additional baskets and increased flexibility with respect to restrictions on indebtedness, liens, investments, acquisitions and restricted payments. The Third Amendment also updates the definition of Consolidated EBITDA to include additional addbacks and to clarify certain components of the calculation thereof.
Under the Amended Credit Agreement, the terms and conditions of the Guaranty and Security Agreement (the “Guaranty and Security Agreement”) between the Company, AHM and Truist Bank remain in effect. Pursuant to the Guaranty and Security Agreement, the Company and AHM have granted the lenders under the Amended Credit Agreement a security interest in substantially all of their assets to secure obligations under the Amended Credit Agreement, including, without limitation, all stock and other equity issued by their subsidiaries (including AHM) and all rights with respect to the $545.0 million loan from the Company to Astrana Medical.
In the ordinary course of business, certain of the lenders under the Amended Credit Agreement and their affiliates have provided to the Company and its subsidiaries and the associated practices, and may in the future provide, (i) investment banking, commercial banking, cash management, foreign exchange or other financial services, and (ii) services as a bond trustee and other trust and fiduciary services, for which they have received compensation and may receive compensation in the future.
Deferred Financing Costs
As of December 31, 2023 and 2022, unamortized deferred financing costs were $6.1 million and $3.3 million, respectively. During the year ended December 31, 2023, the Company recorded additional deferred financing costs of $3.9 million related to the Third Amendment. As of December 31, 2023, $2.6 million of unamortized deferred financing costs was recognized in prepaid expenses and other current assets in the accompanying consolidated balance sheets and consisted of unamortized deferred financing costs related to unborrowed amounts available on the Term Loan and the unamortized deferred financing costs for the Revolver Loan. As of December 31, 2023, $3.6 million of unamortized deferred financing costs was recorded as a direct reduction against the amounts borrowed on the Term Loan. The remaining unamortized deferred financing costs related to the Revolver Loan are amortized over the life of the Revolver Loan using the straight-line method. The remaining unamortized deferred financing costs related to the Term Loan are amortized over the life of the Term Loan using the effective interest rate method.
Real Estate Loans (Excluded Assets for the benefit of APC and its subsidiaries)
Real Estate - East West Bank
110
In December 2020, APC purchased three entities, each of which was included in Excluded Assets and had entered into real estate loan with East West Bank. As of December 31, 2022, the principal on each loan was $5.9 million, $0.6 million and $0.6 million, respectively, and had a variable interest rate of 0.50 %, 0.50 % and 0.30 % less than the independent index, which is the daily Wall Street Journal “Prime Rate”, respectively. The maturity date of each loan was August 5, 2030. These loans are a component of Excluded Assets that are solely for the benefit of APC and its shareholders. These loans were spun off on December 26, 2023 as part of the Spin-Off. Refer to Note 1 — “Description of Business” to the consolidated financial statements for information on the Spin-Off.
Real Estate - MUFG Union Bank N.A.
In January 2022, a subsidiary of APC, which was included in Excluded Assets, entered into a loan agreement with MUFG Union Bank N.A. with the principal on the loan of $16.3 million and a maturity date of March 1, 2032. The loan was used to purchase property in Monterey Park, California. The variable interest rate was 2.0 % in excess of Daily Simple SOFR (as defined in the loan agreement). As of December 31, 2022, the principal on the loan was $16.0 million. On December 14, 2023, APC paid off the outstanding loan balance of $15.6 million. This loan was a component of Excluded Assets that are solely for the benefit of APC and its shareholders.
Construction Loan (Excluded Assets for the benefit of APC and its subsidiaries)
In April 2021, an entity included in Excluded Assets entered into a construction loan agreement with MUFG Union Bank N.A. (“Construction Loan”). The Construction Loan has a borrowing capacity of $10.7 million with a maturity date of March 1, 2024 or, upon completion of the construction and certain other requirements defined in the loan agreement, March 1, 2034. The loan balance as of December 31, 2022 was $4.2 million. On December 14, 2023, APC paid off the outstanding loan balance of $8.5 million. This loan was a component of Excluded Assets that are solely for the benefit of APC and its shareholders.
Promissory Note Payable
FYB Promissory Note Agreement with CCHCA
In May 2021, FYB entered into a promissory note agreement with CCHCA. The principal on the promissory note is $2.0 million, with a maturity date of May 9, 2024. The interest rate is the prime rate plus 1.0 %. The prime rate is updated annually on the effective date of the note and published by the Wall Street Journal.
Effective Interest Rate
The Company’s average effective interest rate on its total debt during the years ended December 31, 2023, 2022 and 2021, was 6.19 %, 3.22 % and 2.06 %, respectively. Interest expense in the consolidated statements of income included amortization of deferred debt issuance costs for the years ended December 31, 2023, 2022 and 2021, of $1.1 million, $0.9 million and $1.2 million, respectively.
Lines of Credit
APC Business Loan
In September 2019, the APC Business Loan Agreement with Preferred Bank (the “APC Business Loan Agreement”) was amended to, among other things, decrease loan availability to $4.1 million, limit the purpose of the indebtedness under the APC Business Loan Agreement to the issuance of standby letters of credit, and include as a permitted lien, the security interest in all of its assets that APC granted to AHM under a Security Agreement dated on or about September 11, 2019, securing APC’s obligations to AHM under their management services agreement dated as of July 1, 1999, as amended.
Standby Letters of Credit
The Company established irrevocable standby letters of credit with Truist Bank under the Amended Credit Agreement for a total of $36.5 million for the benefit of CMS and certain health plans as of December 31, 2023. Unless the institution provides notification that the standby letters of credit will be terminated prior to the expiration date, the letters will be automatically extended without amendment for additional one-year periods from the present, or any future expiration date.
111
Certain IPAs consolidated by the Company established irrevocable standby letters of credit with Preferred Bank under the APC Business Loan Agreement for a total of $3.9 million for the benefit of certain health plans as of December 31, 2023. The standby letters of credit are automatically extended without amendment for additional one-year periods from the present or any future expiration date, unless notified by the institution in advance of the expiration date that the letter will be terminated.
11. Income Taxes
Provision for income taxes consisted of the following (in thousands):
| Years ended December 31, | |||||||||||||||||
| 2023 | 2022 | 2021 | |||||||||||||||
| Current | |||||||||||||||||
| Federal | $ | $ | $ | ||||||||||||||
| State | |||||||||||||||||
| Deferred | |||||||||||||||||
| Federal | ( |
( |
|||||||||||||||
| State | ( |
( |
|||||||||||||||
| ( |
( |
||||||||||||||||
| Total provision for income taxes | $ | $ | $ | ||||||||||||||
The provision for income taxes differs from the amount computed by applying the federal income tax rate as follows:
| Years ended December 31, | |||||||||||||||||
| 2023 | 2022 | 2021 | |||||||||||||||
| Tax provision at U.S. federal statutory rates | % | % | % | ||||||||||||||
| State income taxes net of federal benefit | |||||||||||||||||
| Non-deductible permanent items | |||||||||||||||||
| Variable interest entities | ( |
( |
( |
||||||||||||||
| Stock-based compensation | ( |
( |
|||||||||||||||
| Change in valuation allowance | ( |
||||||||||||||||
Gain on sale of investment |
( |
||||||||||||||||
| NOL adjustment | ( |
||||||||||||||||
| Undistributed dividend | ( |
||||||||||||||||
| Spin-off transaction | |||||||||||||||||
| Other | ( |
||||||||||||||||
| Effective income tax rate | % | % | % | ||||||||||||||
The Company’s effective tax rate differs from the Federal statutory rate of 21 % due to increases from state taxes, non-deductible permanent items, stock-based compensation, gain on sale of investment, and a one-time gain in connection with the December 26, 2023 Spin-Off transaction. This is offset by variable interest entities, change in valuation allowance, and a benefit related to the reversal on deferred taxes on undistributed dividends. The Company had previously recorded deferred tax liabilities related to undistributed dividends for taxpaying groups that could not consolidate under US federal tax law. As a result of the spinoff transaction that occurred on December 26, 2023, the separate taxpaying groups now have the ability to consolidate under US federal tax law, resulting in tax benefits on the future payment of the dividends.
112
Significant components of the Company’s deferred tax assets (liabilities) as of December 31, 2023 and 2022, are shown below (in thousands).
| 2023 | 2022 | ||||||||||
| Deferred tax assets | |||||||||||
| State taxes | $ | $ | |||||||||
| Accrued expenses | |||||||||||
| Allowance for bad debts | |||||||||||
| Investment in other entities | |||||||||||
| Net operating loss carryforward | |||||||||||
| Lease liability | |||||||||||
| Unrealized gain | |||||||||||
| Stock options | |||||||||||
| Other | |||||||||||
| Deferred tax assets before valuation allowance | |||||||||||
| Valuation allowance | ( |
( |
|||||||||
| Net deferred tax assets | |||||||||||
| Deferred tax liabilities | |||||||||||
| Property and equipment | ( |
( |
|||||||||
| Acquired intangible assets | ( |
( |
|||||||||
| Right-of-use assets | ( |
( |
|||||||||
| Debt issuance cost | ( |
( |
|||||||||
Undistributed dividend |
( |
||||||||||
| Deferred tax liabilities | ( |
( |
|||||||||
Net deferred tax liabilities |
$ | ( |
$ | ( |
|||||||
A valuation allowance of $5.9 million and $8.3 million as of December 31, 2023 and 2022, respectively, has been established against the Company’s deferred tax assets related to loss entities the Company cannot consolidate under the federal consolidation rules, as realization of these assets is uncertain. Valuation allowance decreased by $2.4 million in 2023 and increased by $4.3 million in 2022.
As of December 31, 2023, the Company had federal and California net operating loss carryforwards of approximately $21.0 million and $44.8 million, respectively. The federal and California net operating loss carryforwards will expire at various dates from 2027 through 2043; however, $5.3 million of the federal net operating loss carryforwards do not expire and can be carried forward indefinitely. The Company has determined certain NOLs are limited pursuant to Internal Revenue Code Sections 382 and 383, but does not anticipate these NOLs will expire before utilization.
As of December 31, 2023 and 2022, the Company does not have any unrecognized tax benefits related to various federal and state income tax matters. The Company will recognize accrued interest and penalties related to unrecognized tax benefits in income tax expense.
The Company is subject to U.S. federal income tax, as well as income tax in California. The Company’s and its subsidiaries’ state and federal income tax returns are open to audit under the statute of limitations for the years ended December 31, 2019 through December 31, 2022 and for the years ended December 31, 2020 through December 31, 2022, respectively. The Company is currently under audit for federal and California amended tax years ended December 31, 2019, 2020 and 2021. The Company does not anticipate any significant changes to unrecognized tax benefits over the next 12 months.
12. Mezzanine and Stockholders’ Equity (Deficit)
113
Mezzanine Equity (Deficit)
APC
As the redemption feature (see Note 2 — “Basis of Presentation and Summary of Significant Accounting Policies”) of APC’s shares of common stock is not solely within the control of APC, the equity of APC does not qualify as permanent equity and has been classified as non-controlling interests in mezzanine or temporary equity. APC’s shares were not redeemable, and it was not probable that the shares would become redeemable as of December 31, 2023, 2022 and 2021.
Stockholders’ Equity
Preferred Stock – Series A
In October 2015, Astrana entered into an agreement with AHM, a wholly owned subsidiary of Astrana, pursuant to which Astrana sold to AHM, and AHM purchased from Astrana, in a private offering of securities, 1,111,111 units, each unit consisting of one share of Astrana’s Series A Preferred Stock and a common stock warrant to purchase one share of Astrana’s common stock at an exercise price of $9.00 per share. AHM paid Astrana an aggregate of $10.0 million for the units. Holders of the Company’s shares of Series A preferred stock are entitled to receive dividends out of legally available assets, on parity with the holders of the Company’s shares of common stock. The Series A preferred stock has a liquidation preference in the amount of $9.00 per share plus any declared and unpaid dividends, and is convertible into common stock, at the option of the holder thereof, at any time after issuance, at an initial conversion rate of one -for-one, in each case, subject to adjustment in the event of stock dividends, stock splits and certain other similar transactions.
Preferred Stock – Series B
In March 2016, Astrana entered into an agreement with AHM pursuant to which Astrana sold to AHM, and AHM purchased from Astrana, in a private offering of securities, 555,555 units, each unit consisting of one share of Astrana’s Series B Preferred Stock and a common stock warrant to purchase one share of Astrana’s common stock at an exercise price of $10.00 per share. AHM paid Astrana an aggregate $5.0 million for the units. Holders of the Company’s shares of Series B preferred stock are entitled to receive dividends out of legally available assets, on parity with the holders of the Company’s shares of common stock. The Series B preferred stock has a liquidation preference in the amount of $9.00 per share plus any declared and unpaid dividends, and is convertible into common stock, at the option of the holder thereof, at any time after issuance, at an initial conversion rate of one -for-one, in each case, subject to adjustment in the event of stock dividends, stock splits and certain other similar transactions.
Common Stock
Subject to the rights of preferred stockholders, if any, holders of the Company’s common stock are entitled to receive such dividends, if any, as may be declared from time to time by the Company’s board of directors, at its discretion, from legally available funds. In the event of a liquidation, dissolution or winding up, the holders of common stock will be entitled to share ratably in the net assets legally available for distribution to stockholders after the payment of all of the Company’s known debts and other liabilities and the satisfaction of any liquidation preference granted to the holders of any then-outstanding shares of preferred stock.
2017 Share Issuances and Repurchases
In December 2017, Astrana completed its business combination with AHM following the satisfaction or waiver of the conditions set forth in the Agreement and Plan of Merger, dated December 21, 2016, as amended, pursuant to which the merger subsidiary of Astrana merged with and into AHM, with AHM surviving as a wholly owned subsidiary of Astrana (“2017 Merger”).
In connection with the 2017 Merger, former AHM shareholders received Astrana common stock subject to a 10% holdback. As of December 31, 2023, 41,048 holdback shares have not been issued to certain former AHM shareholders who were AHM shareholders at the time of closing of the 2017 Merger, as they have yet to submit properly completed letters of transmittal to Astrana in order to receive their pro rata portion of Astrana common stock as contemplated under the Merger Agreement. Pending such receipt, such former AHM shareholders have the right to receive, without interest, their pro rata share of dividends or distributions with a record date after the effectiveness of the 2017 Merger. The consolidated financial statements
114
have treated such shares of common stock as outstanding, given the receipt of the letter of transmittal is considered perfunctory and the Company is legally obligated to issue these shares in connection with the 2017 Merger.
Dividends
During the years ended December 31, 2023, 2022 and 2021, APC declared dividends of $58.0 million, $58.3 million and $57.9 million, respectively, to their Series A Preferred shareholders.
During the years ended December 31, 2023, 2022 and 2021, APC declared dividends of $210.9 million, $37.9 million and $29.9 million, respectively, to their common shareholders.
During the years ended December 31, 2023, 2022 and 2021, certain consolidated subsidiaries of the Company paid distributions of $3.9 million, $4.1 million and $1.2 million, respectively, to the shareholders who own the non-controlling interests in the entities.
Treasury Stock
As of December 31, 2023 and 2022, APC owned 7,132,698 and 10,299,259 shares of Astrana’s common stock, respectively. While such shares of Astrana’s common stock are legally issued and outstanding, they are treated as treasury shares for accounting purposes and excluded from shares of common stock outstanding in the consolidated financial statements. APC's ownership in Astrana was 13.22 % and 18.12 % as of December 31, 2023 and 2022, respectively.
During the year ended December 31, 2023, Astrana bought back 3,451,642 shares of its common stock, which included 3,166,561 shares of common stock purchased from APC for $100.0 million on November 14, 2023.
As of December 31, 2023 and 2022, the total treasury stock, including the Company’s stock held by APC, was 10,584,340 and 10,299,259 , respectively.
13. Stock-Based Compensation
Equity Incentive Plans
In connection with the 2017 Merger, the Company assumed the 2013 Equity Incentive Plan (the “2013 Plan”), pursuant to which 500,000 shares of the Company’s common stock were reserved for issuance thereunder. The Company issued new shares to satisfy stock options and warrant exercises under the 2013 Plan. As of December 31, 2023, there were no shares available for future grants under the 2013 Plan.
In connection with the 2017 Merger, the Company assumed the 2015 Equity Incentive Plan (as amended, the “2015 Plan”), pursuant to which 1,500,000 shares of the Company’s common stock were reserved for issuance thereunder. The Company’s stockholders approved an amendment to the 2015 Plan at the 2021 annual meeting of stockholders to increase the maximum number of shares authorized for issuance thereunder by 2,000,000 shares, from 1,500,000 shares to 3,500,000 shares. In addition, shares that are subject to outstanding grants under the Company’s 2013 Plan, but that ordinarily would have been restored to such plans reserve due to award forfeitures and terminations, were rolled into and became available for awards under the 2015 Plan. The 2015 Plan provides for awards, including incentive stock options, non-qualified options, restricted common stock, and stock appreciation rights. The 2015 Plan was approved by Astrana’s stockholders at Astrana’s 2016 annual meeting of stockholders that was held in September 2016. As of December 31, 2023, 2022 and 2021, there were approximately 0.4 million, 1.1 million and 1.7 million shares available for future grants under the 2015 Plan, respectively.
On November 15, 2023, the Company adopted the Employment Inducement Award Plan (the “Inducement Plan”), pursuant to which the Company may from time to time grant equity-based awards to new employees as a material inducement to their employment. Awards granted under the Inducement Plan may be in the form of non-qualified stock options, stock appreciation rights, restricted stock awards, restricted stock units, and other stock-based awards. A total of 500,000 shares of the Company’s common stock, par value $0.001 per share, have been reserved for issuance pursuant to awards granted under the Inducement Plan (subject to adjustment as provided in the Inducement Plan). As of December 31, 2023, there were approximately 0.5 million shares available for future grants in the Inducement Plan.
115
The following table summarizes the stock-based compensation expense recognized under all of the Company’s stock plans in 2023, 2022 and 2021, and associated with the issuance of restricted shares of common stock and vesting of stock options that are included in general and administrative expenses in the accompanying consolidated statements of income recognized (in thousands):
| Years ended December 31, | ||||||||||||||||||||
| 2023 | 2022 | 2021 | ||||||||||||||||||
| Stock options | $ | $ | $ | |||||||||||||||||
| Restricted stock awards | ||||||||||||||||||||
| Total share-based compensation expense | $ | $ | $ | |||||||||||||||||
Unrecognized compensation expense related to total share-based payments outstanding as of December 31, 2023 was $32.2 million and is expected to be recognized over a weighted-average period of 2.1 years.
Options
The Company’s outstanding stock options consisted of the following:
| Shares | Weighted-Average Exercise Price |
Weighted-Average Remaining Contractual Term (Years) |
Aggregate Intrinsic Value (in millions) |
||||||||||||||||||||
| Options outstanding at January 1, 2023 | $ | $ | |||||||||||||||||||||
| Options granted | — | — | |||||||||||||||||||||
| Options exercised | ( |
— | |||||||||||||||||||||
| Options canceled, forfeited or expired | ( |
— | — | ||||||||||||||||||||
| Options outstanding at December 31, 2023 | $ | $ | |||||||||||||||||||||
| Options exercisable at December 31, 2023 | $ | $ | |||||||||||||||||||||
During the years ended December 31, 2023 and 2022, stock options were exercised for 140,000 and 41,603 shares, respectively, of the Company’s common stock, which resulted in proceeds of approximately $1.5 million and $0.7 million, respectively. The exercise prices ranged from $10.00 to $18.11 per share for the exercises during the year ended December 31, 2023 and $15.35 to $23.24 per share for the exercises during the year ended December 31, 2022. The total intrinsic value of stock options exercised was $3.5 million, $1.0 million and $2.8 million during the years ended December 31, 2023, 2022 and 2021, respectively. The intrinsic value of stock options is defined as the difference between the Company’s stock price on the exercise date and the grant date exercise price.
During the year ended December 31, 2023, no options were granted. The weighted-average grant-date fair value of options granted during the years ended December 31, 2022 and 2021 was $22.32 , and $32.63 , respectively.
Restricted Stock Awards
The Company’s unvested restricted stock award activity for the year ended December 31, 2023 consisted of the following:
116
| Restricted Stock Awards | Performance Based Restricted Stock Awards | ||||||||||||||||||||||
| Number of Shares |
Weighted Average Grant-Date Fair Value |
Number of Shares |
Weighted Average Grant-Date Fair Value |
||||||||||||||||||||
| Unvested as of January 1, 2023 | $ |
$ |
|||||||||||||||||||||
| Granted | |||||||||||||||||||||||
| Vested | ( |
( |
|||||||||||||||||||||
| Forfeited | ( |
( |
|||||||||||||||||||||
| Unvested as of December 31, 2023 | $ |
$ |
|||||||||||||||||||||
The Company grants restricted stock awards to employees and executives, which are earned based on service conditions. The awards will vest over a period of one month to four years in accordance with the terms of those plans. The grant date fair value of the restricted stock awards is the grant date’s closing market price of the Company’s common stock. During the year ended December 31, 2023, the Company granted 561,386 shares of restricted stock awards with performance based conditions and 480,228 shares of restricted stock without performance conditions. During the year ended December 31, 2023, the weighted average grant date fair value of restricted stock with and without performance based conditions was $33.61 and $33.90 , respectively. Shares of restricted stock with performance conditions are recognized to the extent the performance conditions are probable of being achieved. The total fair value of restricted stock awards, as of their respective vesting dates during the years ended December 31, 2023, 2022 and 2021, was $14.3 million, $10.8 million and $1.1 million, respectively.
Warrants
14. Commitments and Contingencies
Regulatory Matters
Laws and regulations governing the Medicare program and healthcare generally are complex and subject to interpretation. The Company believes it complies with all applicable laws and regulations and is unaware of any pending or threatened investigations involving allegations of potential wrongdoing. While no regulatory inquiries have been made, compliance with such laws and regulations can be subject to future government review and interpretation, as well as significant regulatory action, including fines, penalties, and exclusion from the Medicare and Medi-Cal programs.
117
As a risk-bearing organization, the Company is required to follow regulations of the Department of Managed Health Care (“DMHC”). The Company must comply with a minimum working capital requirement, tangible net equity (“TNE”) requirement, cash-to-claims ratio, and claims payment requirements prescribed by the DMHC. TNE is defined as net assets less intangibles, less non-allowable assets (which include amounts due from affiliates), plus subordinated obligations. At December 31, 2023 and 2022, the consolidated IPAs were in compliance with these regulations.
Many of the Company’s payer and provider contracts are complex in nature and may be subject to differing interpretations regarding amounts due for the provision of medical services. Such differing interpretations may not come to light until a substantial period of time has passed following contract implementation. Liabilities for claims disputes are recorded when the loss is probable and can be estimated. Any adjustments to reserves are reflected in current operations.
Standby Letters of Credit
The Company established irrevocable standby letters of credit with Truist Bank for a total of $36.5 million for the benefit of CMS and certain health plans as of December 31, 2023 (see Note 10 — “Credit Facility, Bank Loans, and Lines of Credit — Standby Letters of Credit”).
Certain IPAs consolidated by the Company established irrevocable standby letters of credit with Preferred Bank for a total of $3.9 million, for the benefit of certain health plans as of December 31, 2023 (see Note 10 — “Credit Facility, Bank Loans, and Lines of Credit — Standby Letters of Credit”).
Litigation
From time to time, the Company is involved in various legal proceedings and other matters arising in the normal course of its business. The resolution of any claim or litigation is subject to inherent uncertainty and could have a material adverse effect on the Company’s financial condition, cash flows, or results of operations.
Liability Insurance
The Company believes that its insurance coverage is appropriate based upon the Company’s claims experience and the nature and risks of the Company’s business. In addition to the known incidents that have resulted in the assertion of claims, the Company cannot be certain that its insurance coverage will be adequate to cover liabilities arising out of claims asserted against the Company, the Company’s affiliated professional organizations or the Company’s affiliated hospitalists in the future where the outcomes of such claims are unfavorable. The Company believes that the ultimate resolution of all pending claims, including liabilities in excess of the Company’s insurance coverage, will not have a material adverse effect on the Company’s financial position, results of operations, or cash flows; however, there can be no assurance that future claims will not have such a material adverse effect on the Company’s business. Contracted physicians are required to obtain their own insurance coverage.
The Company’s contracted physicians are required to carry first-dollar coverage with limits of liability equal to not less than $1.0 million for claims based on occurrence up to an aggregate of $3.0 million per year. The Company’s IPAs purchase stop-loss insurance, which will reimburse them for claims from service providers on a per enrollee basis. The specific retention amount per enrollee per policy period is $45,000 to $90,000 for professional coverage.
Although the Company currently maintains liability insurance policies on a claims-made basis, which are intended to cover malpractice liability and certain other claims, the coverage must be renewed annually, and may not continue to be available to the Company in future years at acceptable costs, and on favorable terms.
118
15. Related-Party Transactions
Equity Method Investments
During the years ended December 31, 2023, 2022, and 2021, AHM recognized approximately $16.7 million, $21.2 million, and $18.7 million, respectively, in management fee income, from LMA. On August 31, 2023, the management service agreement between LMA’s IPA and AHM was terminated. LMA is accounted for under the equity method based on 25 % equity ownership interest held by APC (see Note 6 — “Investments in Other Entities”).
During the years ended December 31, 2023, 2022 and 2021, APC paid approximately $2.7 million, $2.7 million and $2.4 million, respectively, to Pacific Medical Imaging and Oncology Center, Inc. (“PMIOC”) for provider services. APC and PMIOC have an Ancillary Service Contract together whereby PMIOC provides covered services on behalf of APC to enrollees of the plans of APC. PMIOC is accounted for under the equity method based on 40 % equity ownership interest held by APC (see Note 6 — “Investments in Other Entities”).
During the year ended December 31, 2023, the Company paid approximately $1.1 million, to James Song, M.D., a Professional Corporation (“Song PC”) for provider services. Song PC is accounted for under the equity method accounting based on 25 % equity ownership interest held by a subsidiary of the Company (see Note 6 — “Investments in Other Entities”).
Astrana Board Members and Officers
During the years ended December 31, 2023, 2022 and 2021, AHM recognized approximately $2.1 million, $1.8 million and $1.6 million, respectively, in management fee income from Arroyo Vista Family Health Center (“Arroyo Vista”). Arroyo Vista’s chief executive officer is a member of the Company’s board of directors. The Company has a managed service agreement with Arroyo Vista.
During the years ended December 31, 2023 2022 and 2021, the Company paid approximately $0.3 million, $0.3 million and $0.4 million respectively, to Arroyo Vista for services as a provider. The Company has provider contracts with Arroyo Vista.
For the year ended December 31, 2023, the Company recognized $14.1 million in operating lease right-of-use assets and $14.5 million in operating lease liabilities from certain lease agreements with properties that were spun-off as part of the Spin-Off. The chief executive officer of the real estate business managing these properties is also a member of the Company’s board of directors. Refer to Note 1 — “Description of Business” to the consolidated financial statements for information on the Spin-Off.
During the years ended December 31, 2023, 2022 and 2021, APC paid approximately $0.3 million, $0.6 million and $0.7 million, respectively, to Advanced Diagnostic Surgery Center for services as a provider. Advanced Diagnostic Surgery Center shares common ownership with certain board members of Astrana. The Company has provider contracts with Advanced Diagnostic Surgery Center.
During the years ended December 31, 2023, 2022 and 2021, APC recognized approximately $0.6 million, $0.6 million and $0.6 million respectively, in rental income from Advanced Diagnostic Surgery Center. Advanced Diagnostic Surgery Center is leasing from a property that is a component of Excluded Assets. The property was spun-off on December 26, 2023, as part of the Spin-Off. Refer to Note 1 — “Description of Business” to the consolidated financial statements for information on the Spin-Off.
During the years ended December 31, 2023, 2022 and 2021, APC paid approximately $10,000 , $0.6 million and $2.0 million respectively, to Fulgent Genetics, Inc. for services as a provider. One of the Company’s board members is a board member of Fulgent Genetics, Inc. The Company has provider contracts with Fulgent Genetics, Inc.
During the year ended December 31, 2023, the Company incurred approximately $1.3 million in expenses payable to Third Way Health for call center services. One of Astrana’s officers is a board member of Third Way Health in 2023.
During the years ended December 31, 2023, 2022 and 2021, the Company paid approximately $2.6 million, $1.9 million and $1.3 million, respectively, to Sunny Village Care Center for services as a provider. Sunny Village Care Center shares common ownership with certain Astrana board members and officers. The Company has provider contracts with Sunny Village Care Center.
119
During the years ended December 31, 2023 and 2022, APC recognized approximately $1.1 million and $0.3 million, respectively, in rental income from Sunny Village Care Center. Sunny Village Care Center is leasing from a property that is a component of Excluded Assets. The property was spun-off on December 26, 2023 as part of the Spin-Off. Refer to Note 1 — “Description of Business” to the consolidated financial statements for information on the Spin-Off.
In November 2023, the Company entered into a three-year promissory note with Sunny Village Care Center as the borrower for a principal amount of $0.5 million. The loan balance is presented within long-term debt, net of current portion and deferred financing costs in the accompanying consolidated balance sheets.
During the year ended December 31, 2023, the Company incurred rent expense of approximately $0.1 million from First Commonwealth Property, LLC for office leases. First Commonwealth Property, LLC shares common ownership with certain board members of Astrana. The Company has lease arrangements with First Commonwealth Property, LLC.
During the year ended December 31, 2023, Astrana paid approximately $9.8 million, to purchase Astrana’s stock from certain board members. During the year ended December 31, 2022, APC paid approximately $9.3 million to purchase Astrana’s stock from a board member.
During the year ended December 31, 2021, AHM paid approximately $44,000 to an Astrana board member for consulting services. The Company did not incur any similar expenses for the years ended December 31, 2023 and 2022.
The Company has agreements with Health Source MSO Inc., a California corporation (“HSMSO”), Aurion Corporation (“Aurion”), and AHMC for services provided to the Company. One of the Company’s board members is an officer of AHMC, HSMSO, and Aurion. Aurion is also partially owned by one of the Company’s board members. Revenue with AHMC and HSMSO consists of capitation, risk pool, and miscellaneous fees and expenses consist of claims expense, management fees, and consulting fees.
The following table sets forth fees incurred and income received related to AHMC, HSMSO, and Aurion (in thousands):
| Year Ended December 31, 2023 | Year Ended December 31, 2022 | ||||||||||||||||||||||
| AHMC | HSMSO | AURION | AHMC | HSMSO | AURION | ||||||||||||||||||
| Revenue | $ | $ | $ | $ | $ | $ | |||||||||||||||||
| Expenses | |||||||||||||||||||||||
| Net | $ | $ | $ | ( |
$ | $ | ( |
$ | ( |
||||||||||||||
The Company and AHMC have a risk-sharing agreement with certain AHMC hospitals to share the surplus and deficits of each of the hospital pools. Under this agreement, during the years ended December 31, 2023, 2022 and 2021, the Company has recognized risk pool revenue of $43.8 million, $50.5 million and $60.1 million, respectively, of which $54.0 million and $58.7 million, remained outstanding as of December 31, 2023 and 2022, respectively.
APC Board Members
During the years ended December 31, 2023, 2022, and 2021, the Company paid an aggregate of approximately $23.1 million, $34.5 million, and $32.5 million, respectively, to board members for provider services which included approximately $4.2 million, $3.7 million and $3.4 million, respectively, to Astrana board members and officers who are also board members and officers of APC.
On November 6, 2023, the Company entered into a stock repurchase agreement with APC, pursuant to which the Company agreed to repurchase approximately $100.0 million, or 3,166,561 shares, of the Company’s common stock from APC. APC is a consolidated affiliate of the Company of which Dr. Thomas Lam, the Company’s Co-Chief Executive Officer and President and a director, is the Chief Executive Officer and Chief Financial Officer and a director and stockholder; Dr. Kenneth Sim, the Company’s Executive Chairman, is Chairman and a director and stockholder; and Dr. Albert Young, the Company’s Chief Administrative Officer, is Senor Executive Vice President and a stockholder. The Company’s Board of Directors and the Audit Committee of the Board of Directors approved the proposed repurchase.
120
In addition, affiliates wholly owned by the Company’s key personnel, are reported in the accompanying consolidated statements of income on a consolidated basis, together with the Company’s subsidiaries, and therefore, the Company does not separately disclose transactions between such affiliates and the Company’s subsidiaries as related-party transactions.
Intercompany Transactions
Because of corporate practice of medicine laws, the Company uses designated shareholder professional corporations, of which the sole shareholder is a member of the Company’s key personnel, to engage in certain transactions and make intercompany loans from time to time.
For equity method investments, loans receivable and line of credits from related parties, see Note 6 — “Investments in Other Entities,” and Note 7 — “Loans Receivable and Loan Receivable — Related Parties,” respectively.
16. Employee Benefit Plan
17. Earnings Per Share
Basic earnings per share is calculated using the weighted average number of shares of the Company’s common stock issued and outstanding during a certain period, and is calculated by dividing net income attributable to Astrana by the weighted average number of shares of the Company’s common stock issued and outstanding during such period. Diluted earnings per share is calculated using the weighted average number of shares of common stock and potentially dilutive shares of common stock outstanding during the period, using the as-if converted method for secured convertible notes, preferred stock, and the treasury stock method for options and common stock warrants. The non-controlling interests in APC are allocated their share of Astrana’s income from APC’s ownership of Astrana common stock and this is included in the net income attributable to non-controlling interests on the consolidated statements of income. Therefore, none of the shares of Astrana held by APC are considered outstanding for the purposes of basic or diluted earnings per share computation.
As of December 31, 2023, 2022 and 2021, APC held 7,132,698 , 10,299,259 and 10,925,702 shares of Astrana's common stock, respectively, which are treated as treasury shares for accounting purposes and not included in the number of shares of common stock outstanding used to calculate earnings per share.
For the years ended December 31, 2023, 2022 and 2021, restricted stock of 186,290 , 133,480 and 9,137 , respectively, were excluded from the computation of diluted weighted average common shares outstanding because the assumed proceeds, as calculated under the treasury stock method, resulted in these awards being anti-dilutive.
For the years ended December 31, 2023 and 2022, restricted stock with performance conditions of 782,484 and 245,478 , respectively, were excluded from the computation of diluted weighted average common shares outstanding because these conditions were not achieved as of December 31, 2023 or 2022, as applicable.
Below is a summary of the earnings per share computations:
| Years ended December 31, | ||||||||||||||||||||
| 2023 | 2022 | 2021 | ||||||||||||||||||
Earnings per share – basic |
$ | $ | $ | |||||||||||||||||
Earnings per share – diluted |
$ | $ | $ | |||||||||||||||||
| Weighted-average shares of common stock outstanding – basic | ||||||||||||||||||||
| Weighted-average shares of common stock outstanding – diluted | ||||||||||||||||||||
121
Below is a summary of the shares included in the diluted earnings per share computations:
| Years ended December 31, | ||||||||||||||||||||
| 2023 | 2022 | 2021 | ||||||||||||||||||
| Weighted-average shares of common stock outstanding – basic | ||||||||||||||||||||
| Stock options | ||||||||||||||||||||
| Warrants | ||||||||||||||||||||
| Restricted stock awards | ||||||||||||||||||||
| Contingently issuable shares | ||||||||||||||||||||
| Weighted-average shares of common stock outstanding – diluted | ||||||||||||||||||||
18. Variable Interest Entities (VIEs)
The Company’s consolidated financial statements include its subsidiaries and consolidated VIEs. A VIE is defined as a legal entity whose equity owners do not have sufficient equity at risk, or, as a group, the holders of the equity investment at risk lack any of the following three characteristics: decision-making rights, the obligation to absorb losses, or the right to receive the expected residual returns of the entity. The primary beneficiary is identified as the variable interest holder that has both the power to direct the activities of the VIE that most significantly affect the entity’s economic performance and the obligation to absorb expected losses or the right to receive benefits from the entity that could potentially be significant to the VIE.
Some states have laws that prohibit business entities with non-physician owners, such as Astrana and its subsidiaries, from practicing medicine, employing physicians to practice medicine, or exercising control over medical decisions by physicians. These laws are generally referred to as corporate practice of medicine laws. States that have corporate practice of medicine laws permit only physicians to practice medicine, exercise control over medical decisions, or engage in certain arrangements, such as fee-splitting, with physicians.
Due to these laws, the Company operates by maintaining long-term MSAs with its affiliated IPAs and medical groups, each of which is owned and operated by physicians only, and employs or contracts with additional physicians to provide medical services. AHM is a wholly owned subsidiary of the Company and has entered into MSAs with several affiliated IPAs, including APC. APC contracts with various HMOs or licensed healthcare service plans, each of which pays a fixed payment (“capitation”). In return, APC arranges for the delivery of healthcare services by contracting with physicians or professional medical corporations for primary care and specialty care services. APC assumes the financial risk of the cost of delivering healthcare services in excess of the fixed amounts received. The risk is subject to stop-loss provisions in contracts with HMOs. Some risk is transferred to the contracted physicians or professional corporations. The physicians in the IPA are exclusively in control of, and responsible for, all aspects of the practice of medicine for enrolled patients. In accordance with relevant accounting guidance, APC has been determined to be a VIE of AHM, as AHM is its primary beneficiary with the ability, through majority representation on the APC Joint Planning Board and otherwise, to direct the activities (excluding clinical decisions) that most significantly affect APC’s economic performance. Therefore, APC and its wholly owned subsidiaries and VIEs are consolidated in the accompanying financial statements.
Certain state laws prohibit a professional corporation that has more than one shareholder from being a shareholder in another professional corporation. As a result, the Company cannot directly own shares in other professional corporations. However, an exception to this regulation permits a professional corporation that has only one shareholder to own shares in another professional corporation. In reliance on this exception, the Company designated certain key personnel as the nominee shareholder of professional corporations which hold controlling and non-controlling ownership interests in several medical corporations. Via a Physician Shareholder Agreement with the nominee shareholder. the Company has the ability to designate another person to be the equity holder of the professional corporation. In addition these entities are managed by the Company’s wholly owned MSOs via MSA. In accordance with relevant accounting guidance, the professional corporations, and their consolidated medical corporations are consolidated by the Company in the accompanying financial statements.
Astrana Medical and Astrana Health Care Partners were formed in May 2019 and July 2021, respectively, as a designated shareholder professional corporation. The Company’s Vice Chairman is the sole shareholder of Astrana Medical and Astrana Health Care Partners via a Physician Shareholder Agreement, Astrana makes all the decisions on behalf of Astrana Medical and
122
Astrana Health Care Partners. Astrana has the obligation to absorb losses of, or the right to receive benefits from, Astrana Medical and Astrana Health Care Partners. Therefore, Astrana Medical and Astrana Health Care Partners are controlled by and consolidated by Astrana as the primary beneficiary of the VIEs.
On February 23, 2023, Astrana Health Care Partners purchased 100 % of certain Care Delivery companies (AMG, a Professional Medical Corporation, 1 World Medicine Urgent Care Corporation, and Eleanor Leung M.D., a Professional Medical Corporation) from APC. As a result, these entities are now consolidated by Astrana Health Care Partners instead of APC. On May 1, 2023, Astrana Health Care Partners sold 25 % of Eleanor Leung M.D. to two of its physicians. As a result, Astrana Health Care Partners now owns 75 % of Eleanor Leung M.D.
The following table includes assets that can only be used to settle the liabilities of the Company’s VIEs, and to which the creditors of Astrana have no recourse, and liabilities to which the creditors of the Company’s VIEs have no recourse to the general credit of Astrana, as the primary beneficiary of the VIEs. These assets and liabilities, with the exception of the investment in a privately held entity that does not report net asset value per share and amounts due to, or from, affiliates, which are eliminated upon consolidation, are included in the accompanying consolidated balance sheets (in thousands).
123
| December 31, | ||||||||||||||
| 2023 | 2022 | |||||||||||||
| Assets | ||||||||||||||
| Current assets | ||||||||||||||
| Cash and cash equivalents | $ | $ | ||||||||||||
| Investment in marketable securities | ||||||||||||||
| Receivables, net | ||||||||||||||
| Receivables, net – related party | ||||||||||||||
| Income taxes receivable | ||||||||||||||
| Other receivables | ||||||||||||||
| Prepaid expenses and other current assets | ||||||||||||||
| Loans receivable | ||||||||||||||
| Loans receivable — related parties | ||||||||||||||
| Amounts due from affiliates* | ||||||||||||||
Total current assets |
||||||||||||||
| Non-current assets | ||||||||||||||
| Land, property and equipment, net | ||||||||||||||
| Intangible assets, net | ||||||||||||||
| Goodwill | ||||||||||||||
| Income taxes receivable, non-current | ||||||||||||||
| Investments in other entities – equity method | ||||||||||||||
| Investment in a privately held entity | ||||||||||||||
| Investment in affiliates* | ||||||||||||||
| Restricted cash | ||||||||||||||
| Operating lease right-of-use assets | ||||||||||||||
| Other assets | ||||||||||||||
Total non-current assets |
||||||||||||||
Total assets |
$ | $ | ||||||||||||
| Current liabilities | ||||||||||||||
| Accounts payable and accrued expenses | $ | $ | ||||||||||||
| Fiduciary accounts payable | ||||||||||||||
| Medical liabilities | ||||||||||||||
| Dividend payable | ||||||||||||||
| Finance lease liabilities | ||||||||||||||
| Operating lease liabilities | ||||||||||||||
| Current portion of long-term debt | ||||||||||||||
| Amount due to affiliates* | ||||||||||||||
Total current liabilities |
||||||||||||||
| Non-current liabilities | ||||||||||||||
| Deferred tax liability | ||||||||||||||
| Finance lease liabilities, net of current portion | ||||||||||||||
124
| Operating lease liabilities, net of current portion | ||||||||||||||
| Long-term debt, net of current portion | ||||||||||||||
| Other long-term liabilities | ||||||||||||||
| Total non-current liabilities | ||||||||||||||
Total liabilities |
$ | $ | ||||||||||||
* Investment in affiliates represents APC’s investment in Astrana, which is reflected as treasury shares and eliminated upon consolidation. Amounts due to, or from, affiliates are receivables with Astrana’s subsidiaries. As a result, these balances are eliminated upon consolidation and are not reflected on Astrana’s consolidated balance sheets as of December 31, 2023 and 2022.
125
19. Leases
The Company has operating and finance leases for corporate offices, physicians’ offices, and certain equipment. This includes leases with properties that were spun-off as part of the Spin-Off. These leases have remaining lease terms ranging from one month seventeen years ten years one year 1.7 million and $1.8 million, respectively, and accumulated depreciation associated with finance leases was $1.6 million and $1.0 million, respectively.
The Company rents or subleases certain real estate to third parties, which are accounted for as operating leases.
As of December 31, 2023, the Company has entered into a lease arrangement for seven years with an option to extend an additional five years . The tentative move date is March 2024, once the unit is made available. Base rent during the initial seven-year term of the 2024 lease agreement will total $2.3 million.
Leases with an initial term of 12 months or less are not recorded on the consolidated balance sheets.
The components of lease expense were as follows (in thousands):
| December 31, 2023 | December 31, 2022 | ||||||||||
| Operating lease cost | $ | $ | |||||||||
| Finance lease cost | |||||||||||
| Amortization of lease expense | |||||||||||
| Interest on lease liabilities | |||||||||||
| Sublease income | ( |
( |
|||||||||
| Total lease cost | $ | $ | |||||||||
126
Other information related to leases was as follows (dollars in thousands):
| December 31, 2023 | December 31, 2022 | ||||||||||
| Supplemental Cash Flows Information | |||||||||||
| Cash paid for amounts included in the measurement of lease liabilities: | |||||||||||
| Operating cash flows from operating leases | $ | $ | |||||||||
| Operating cash flows from finance leases | |||||||||||
| Financing cash flows from finance leases | |||||||||||
| Right-of-use assets obtained in exchange for lease liabilities: | |||||||||||
| Operating leases | |||||||||||
| Finance leases | |||||||||||
| December 31, 2023 | December 31, 2022 | ||||||||||
| Weighted-Average Remaining Lease Term | |||||||||||
| Operating leases | |||||||||||
| Finance leases | |||||||||||
| Weighted-Average Discount Rate | |||||||||||
| Operating leases | % | % | |||||||||
| Finance leases | % | % | |||||||||
Future minimum lease payments under non-cancellable leases as of December 31, 2023 were as follows (in thousands):
| Years ending December 31, | Operating Leases | Finance Leases | |||||||||
| 2024 | $ | $ | |||||||||
| 2025 | |||||||||||
| 2026 | |||||||||||
| 2027 | |||||||||||
| 2028 | |||||||||||
| Thereafter | |||||||||||
| Total future minimum lease payments | |||||||||||
| Less: imputed interest | |||||||||||
| Total lease obligations | |||||||||||
| Less: current portion | |||||||||||
| Long-term lease obligations | $ | $ | |||||||||
127
20. Segments
The Company determined its operating segments in accordance with ASC 280, “Segment Reporting” (“ASC 280”). The Company currently has three reportable segments consisting of: 1) Care Partners; 2) Care Delivery; and 3) Care Enablement (See Note 1 – Description of Business). The Company’s reportable segments changed from one to three in the first quarter of 2023 as a result of certain changes to the information regularly provided to the Company’s chief operating decision maker when reviewing the Company’s performance as well as an effort to provide additional transparency to investors and other financial statement users which the Company believes will assist in the evaluation of changes in the operating results of the Company’s segments separate from non-operational factors that affect net income, thus providing insight into both operations and other factors impacting reported results.
The Company evaluates the performance of its operating segments based on segment revenue growth as well as operating income. Management uses revenue growth and total segment operating income as a measure of the performance of operating businesses separate from non-operating factors. The Company’s operations are based in the United States. All revenues of the Company are derived from the United States. The Company’s segments are not evaluated using asset information.
The Company’s Care Partners segment is focused on building and managing high-quality and high-performance provider networks by partnering with, empowering, and investing in strong provider partners with a shared vision for coordinated care delivery. Under relevant accounting guidance, while the Company’s Care Partners – IPAs and Care Partners – ACO are two operating segments, they share similar economic characteristics and meet other criteria, which permits the Company to aggregate them into a single reportable segment, which the Company has done. Revenue for this segment is primarily comprised of capitation and risk pool settlements and incentives.
The Company’s Care Delivery segment is a patient-centric, data-driven care delivery organization focused on delivering high-quality and accessible care to all patients. The care delivery organization includes primary care, multi-specialty care, and ancillary care services. Revenue is primarily earned based on fee-for-service reimbursements, capitation, and performance-based incentives.
The Company’s Care Enablement segment is an integrated, end-to-end clinical and administrative platform powered by the Company’s proprietary technology suite, which provides operational, clinical, financial, technology, management, and strategic services to enable success in the delivering of high-quality, value-based care for providers and payers. Revenue for this segment is primarily comprised of management and software fees, charged as a percentage of gross revenue or on a per-member-per-month basis.
Other is not a reportable segment and primarily consists of real estate operations and other entities that are individually immaterial. Revenue is primarily comprised of equipment sales and real estate revenue is presented in other income.
In the normal course of business, the Company’s reportable segments enter into transactions with each other. While intersegment transactions are treated like third-party transactions to determine segment performance, the revenues recognized by a segment and expenses incurred by the counterparty are eliminated in consolidation and do not affect consolidated results.
Corporate costs are unallocated and primarily include corporate initiatives, corporate infrastructure costs and corporate shared costs, such as finance, human resources, legal, and executives.
The following table presents information about our segments and prior periods have been recast to conform to the current presentation (in thousands):
128
| Year Ended December 31, 2023 | ||||||||||||||||||||||||||||||||||||||||||||
Care Partners |
Care Delivery | Care Enablement |
Other | Intersegment Elimination | Corporate Costs | Consolidated Total | ||||||||||||||||||||||||||||||||||||||
| Third Party | $ | $ | $ | $ | $ | $ | $ | |||||||||||||||||||||||||||||||||||||
| Intersegment | ( |
|||||||||||||||||||||||||||||||||||||||||||
| Total revenues | ( |
|||||||||||||||||||||||||||||||||||||||||||
| Cost of services | ( |
|||||||||||||||||||||||||||||||||||||||||||
General and administrative(1)
|
( |
|||||||||||||||||||||||||||||||||||||||||||
| Total expenses | ( |
|||||||||||||||||||||||||||||||||||||||||||
| Income (loss) from operations | $ | $ | $ | $ | ( |
$ | (2) |
$ | ( |
$ | ||||||||||||||||||||||||||||||||||
| Year Ended December 31, 2022 | ||||||||||||||||||||||||||||||||||||||||||||
Care Partners |
Care Delivery | Care Enablement |
Other | Intersegment Elimination | Corporate Costs | Consolidated Total | ||||||||||||||||||||||||||||||||||||||
| Third Party | $ | $ | $ | $ | $ | $ | $ | |||||||||||||||||||||||||||||||||||||
| Intersegment | ( |
|||||||||||||||||||||||||||||||||||||||||||
| Total revenues | ( |
|||||||||||||||||||||||||||||||||||||||||||
| Cost of services | ( |
|||||||||||||||||||||||||||||||||||||||||||
General and administrative(1)
|
( |
|||||||||||||||||||||||||||||||||||||||||||
| Total expenses | ( |
|||||||||||||||||||||||||||||||||||||||||||
| Income (loss) from operations | $ | $ | $ | $ | ( |
$ | (2) |
$ | ( |
$ | ||||||||||||||||||||||||||||||||||
| Year Ended December 31, 2021 | ||||||||||||||||||||||||||||||||||||||||||||
Care Partners |
Care Delivery | Care Enablement |
Other | Intersegment Elimination | Corporate Costs | Consolidated Total | ||||||||||||||||||||||||||||||||||||||
| Third Party | $ | $ | $ | $ | $ | $ | $ | |||||||||||||||||||||||||||||||||||||
| Intersegment | ( |
|||||||||||||||||||||||||||||||||||||||||||
| Total revenues | ( |
|||||||||||||||||||||||||||||||||||||||||||
| Cost of services | ( |
( |
||||||||||||||||||||||||||||||||||||||||||
General and administrative(1)
|
( |
|||||||||||||||||||||||||||||||||||||||||||
| Total expenses | ( |
|||||||||||||||||||||||||||||||||||||||||||
| Income (loss) from operations | $ | $ | ( |
$ | $ | ( |
$ | (2) |
$ | ( |
$ | |||||||||||||||||||||||||||||||||
(1) Balance includes general and administrative expenses and depreciation and amortization.
129
21. Fair Value Measurements of Financial Instruments
The carrying amounts and fair values of the Company’s financial instruments as of December 31, 2023 are presented below (in thousands):
Fair Value Measurements |
||||||||||||||||||||||||||
Level 1 |
Level 2 |
Level 3 |
Total |
|||||||||||||||||||||||
| Assets | ||||||||||||||||||||||||||
| Money market accounts* | $ | $ | $ | $ | ||||||||||||||||||||||
| Marketable securities – certificates of deposit | ||||||||||||||||||||||||||
| Marketable securities – equity securities | ||||||||||||||||||||||||||
| Total assets | $ | $ | $ | $ | ||||||||||||||||||||||
| Liabilities | ||||||||||||||||||||||||||
| AAMG contingent consideration | $ | $ | $ | $ | ||||||||||||||||||||||
| VOMG contingent consideration | ||||||||||||||||||||||||||
| DMG remaining equity interest purchase | ||||||||||||||||||||||||||
| Sun Labs remaining equity interest purchase | ||||||||||||||||||||||||||
| Interest rate collar | ||||||||||||||||||||||||||
| Total liabilities | $ | $ | $ | $ | ||||||||||||||||||||||
* Included in cash and cash equivalents
The carrying amounts and fair values of the Company’s financial instruments as of December 31, 2022 are presented below (in thousands):
| Fair Value Measurements | ||||||||||||||||||||||||||
| Level 1 | Level 2 | Level 3 | Total | |||||||||||||||||||||||
| Assets | ||||||||||||||||||||||||||
| Money market accounts* | $ | $ | $ | $ | ||||||||||||||||||||||
| Marketable securities – equity securities | ||||||||||||||||||||||||||
| Contingent equity securities | ||||||||||||||||||||||||||
| Interest rate swaps | ||||||||||||||||||||||||||
Total assets |
$ | $ | $ | $ | ||||||||||||||||||||||
| Liabilities | ||||||||||||||||||||||||||
| APCMG contingent consideration | $ | $ | $ | $ | ||||||||||||||||||||||
| AAMG contingent consideration | ||||||||||||||||||||||||||
| VOMG contingent consideration | ||||||||||||||||||||||||||
| DMG remaining equity interest purchase | ||||||||||||||||||||||||||
| Sun Labs remaining equity interest purchase | ||||||||||||||||||||||||||
| Total liabilities | $ | $ | $ | $ | ||||||||||||||||||||||
* Included in cash and cash equivalents
The change in the fair value of existing Level 3 liabilities is recognized in in the accompanying consolidated statements of income. As of December 31, 2023, the reconciliation of our Level 3 liabilities was as follows (in thousands):
130
| Amount | |||||
| Balance at January 1, 2023 | $ | ||||
| Change in fair value of existing Level 3 liabilities | |||||
| APCMG contingent consideration paid | ( |
||||
| Balance at December 31, 2023 | $ | ||||
Investments in Marketable Securities
As of December 31, 2023 and 2022, certificates of deposit amounted to approximately $2.2 million and $0 , respectively. Investments in certificates of deposit are classified as Level 1 investments in the fair value hierarchy.
As of December 31, 2023, equity securities held by the Company are primarily comprised of common stock of Nutex Health, Inc. (formerly known as Clinigence Holdings, Inc.) (“Nutex”). In September 2021, Astrana and Nutex entered into a stock purchase agreement in which Astrana purchased shares of common stock, warrants, and potentially additional shares of common stock if certain metrics were not met (such additional shares “contingent equity securities”) for $3.0 million. The common stock is included in investments in marketable securities in the accompanying consolidated balance sheets. In May 2022, the Company exercised the warrants and subsequently recognized the shares within investments in marketable securities in the accompanying consolidated balance sheet. In March 2023, the contingent equity securities were settled and the Company received additional Nutex common stock. The additional common stock received from the contingent equity securities is included in investments in marketable securities in the accompanying consolidated balance sheets.
As of December 31, 2023 and 2022, the equity securities were approximately $0.3 million and $5.6 million, respectively, in the accompanying consolidated balance sheets. In December 2023, APC sold all of its common stock in a payer partner. The components comprising total gains and losses on equity securities are as follows (in thousands) for the periods listed below:
| Twelve Months Ended December 31, |
|||||||||||||||||||||||
| 2023 | 2022 | ||||||||||||||||||||||
Total losses recognized on equity securities |
$ | ( |
$ | ( |
|||||||||||||||||||
Less (loss) gains recognized on equity securities sold |
( |
||||||||||||||||||||||
Unrealized losses recognized on equity securities held at end of period |
$ | ( |
$ | ( |
|||||||||||||||||||
Derivative Financial Instruments
Interest Rate Swap Agreements and Collar Agreements
The Company’s collar agreement is designed to limit the interest rate risk associated with the Company’s Revolver Loan. The principal objective of the collar agreement is to eliminate or reduce the variability of the cash flows in interest payments associated with the Company’s floating-rate debt, thus reducing the impact of interest rate changes on future interest payment cash flows. Refer to Note 10 - “Credit Facility, Bank Loans, and Lines of Credit,” for further information on the Company’s
131
debt. Under the terms of the agreement, the ceiling is 5.0 % and the floor is 2.34 %. The collar agreement is not designated as a hedging instrument. Changes in the fair value on this contract is recognized as unrealized gain or loss on investments in the accompanying consolidated statements of income and reflected in the accompanying consolidated statements of cash flows as unrealized loss on investments. The estimated fair value of the collar was determined using Level 2 inputs. As of December 31, 2023 the fair value of the collar was $0.3 million and was presented within other long-term liabilities in the accompanying consolidated balance sheets. For the year ended December 31, 2023, the Company recognized an unrealized loss of $0.3 million.
Contingent Equity Securities
Astrana was entitled to additional common stock if Nutex did not pay AHM management fees exceeding a threshold by the end of December 31, 2022. The contingent equity securities are considered to be derivatives but are not designated as hedging instruments. Changes in the fair value on these contracts are recognized as unrealized gain or loss on investments in the accompanying consolidated statements of income and accompanying consolidated statements of cash flows. The Company determined the fair value of the contingent equity security using a probability-weighted model, which includes significant unobservable inputs (Level 3). Specifically, the Company considered various scenarios of recognizing management fees and assigned probabilities to each such scenario in determining fair value. During the year ended December 31, 2023, the metric was not achieved. Subsequently, the common stock received from the contingent equity securities were accounted for as investments in marketable securities (refer to the subsection above on investments in marketable securities and Note 2 - “Basis of Presentation and Summary of Significant Accounting Policies” for further information on the Company’s investments in marketable securities). As of December 31, 2022, the contingent equity securities were valued at $1.9 million and were presented within prepaid and other current assets in the accompanying consolidated balance sheets. For the year ended December 31, 2022, when the equity securities were still contingent, the Company recognized unrealized losses of $2.4 million.
Remaining equity interest purchase
In 2021, the Company entered into a financing obligation to purchase the remaining equity interest in Diagnostic Medical Group of Southern California (“DMG”) and Sun Clinical Laboratories (“Sun Labs”) within three years from the date the Company consolidated DMG and Sun Labs. The purchase of the remaining DMG equity value is considered a financing obligation with a carrying value of $8.5 million as of both December 31, 2023 and December 31, 2022. Changes in the fair value of the remaining equity purchase are presented in unrealized loss on investments in the accompanying consolidated statements of income. The purchase of the remaining Sun Labs equity value is considered a financing obligation with a carrying value of $7.8 million and $5.8 million as of December 31, 2023 and December 31, 2022, respectively. For the years ended December 31, 2023 and 2022, the change in the fair value of Sun Labs equity value obligation was $2.0 million and $1.7 million, respectively, and is presented in unrealized loss on investments in the accompanying consolidated statements of income. As the financing obligations are embedded in the non-controlling interest, the non-controlling interests are recognized in other liabilities as of December 31, 2023 and other long-term liabilities as of December 31, 2022 in the accompanying consolidated balance sheets.
Contingent considerations
VOMG
Upon consolidating VOMG as a VIE, the purchase price consisted of cash funded upon the close of transaction and additional cash consideration (“VOMG contingent consideration”) contingent on VOMG meeting financial metrics for fiscal years 2023 and 2024. The Company determined the fair value of the contingent consideration using a probability-weighted model that includes significant unobservable inputs (Level 3). The contingent consideration is included within other long-term liabilities in the accompanying consolidated balance sheets. The contingent consideration was valued at $17,000 as of both December 31, 2023 and December 31, 2022. Changes in the VOMG contingent consideration are presented in general and administrative expenses in the accompanying consolidated statements of income.
AAMG
Upon acquiring 100 % of the equity interest in AAMG, the purchase price consisted of cash funded upon close of the transaction and additional consideration (“AAMG contingent consideration”) and stock consideration (“AAMG stock contingent consideration”) contingent on AAMG meeting revenue and capitated member metrics for fiscal years 2023 (“2023 metric”) and 2024 (“2024 metric”). If the contingent considerations are met, the settlement will be paid in the Company’s common stock. The total amount of stock that can be issued for the 2023 and 2024 metrics is 157,048 and 184,361 , respectively. The Company determined the fair value of the contingent considerations using a probability-weighted model that includes significant
132
unobservable inputs (Level 3). Specifically, the Company considered various scenarios of revenue and assigned probabilities to each such scenario in determining fair value.
The AAMG contingent consideration for the 2023 metric was valued at $2.6 million and presented within other liabilities in the accompanying consolidated balance sheets as of December 31, 2023. The AAMG contingent consideration for the 2024 metric was valued at $2.9 million and presented within other long-term liabilities in the accompanying consolidated balance sheets as of December 31, 2023. As of December 31, 2022, for capitated member metrics for fiscal years 2023 and 2024, the AAMG contingent consideration was valued at $5.9 million and was presented within other long-term liabilities in the accompanying consolidated balance sheets. Changes in the AAMG contingent consideration are presented in general and administrative expenses in the accompanying consolidated statements of income. The AAMG stock contingent consideration was valued at $5.6
22. Subsequent Events
Drawdown on Term Loan and Revolver Loan
Subsequent to December 31, 2023, the Company drew down $20 million on its Term Loan and $90 million on its Revolver Loan.
Closing of Acquiring Community Family Care Medical Group IPA, Inc. (“CFC”) Assets
In November 2023, the Company entered into an Asset and Equity Purchase Agreement (the “Purchase Agreement”) to acquire the partnership interests of Advanced Health Management Systems, L.P. (“AHMS”) and certain assets of Community Family Care Medical Group IPA, Inc. (“CFC”), which acquisitions the Company expected would occur in two separate closings. In November 2023, AHM also entered into a Stock Purchase Agreement (the “I Health Purchase Agreement”) to purchase 25 % of the outstanding shares of common stock of I Health, Inc. (“I Health”). On January 31, 2024, the first closing under the Purchase Agreement occurred, and the Company completed its acquisition of CFC’s assets. The Company expects to complete the second closing under the Purchase Agreement and acquire the outstanding general and limited partnership interests of AHMS during the first quarter of 2024, subject to obtaining required regulatory approvals. It is currently expected that the I Health Purchase Agreement closing will occur during the first quarter of 2024. The purchase price consisted of $93.8 million cash and 631,712 shares of common stock of the Company. In addition, the Purchase Agreement contains earnout payments of up to $15.0 million cash. The Company is in the process of finalizing its purchase price allocation of CFC.
Bass Medical Group
On January 29, 2024, the Company announced its strategic long-term partnership with BASS Medical Group, one of the largest multi-specialty medical groups in the Greater San Francisco Bay Area. Together, the two organizations will aim to bring high-quality care via value-based arrangements to patients of all insurance types, including Medicare, Medicaid, ACA Marketplace, and Commercial. Astrana has provided BASS Medical Group with a $20 million senior secured promissory note (“BASS secured promissory note”),which is intended to be used, in partnership with Astrana, to continue to grow their footprint and invest in high-quality, high-value, and accessible primary and multi-specialty care for communities across California. The BASS secured promissory note matures on January 11, 2031 and has an interest rate per annum equal to 2.9 % plus the Secured Overnight Financing Rate as administered by the Federal Reserve Bank of New York (or a successor administrator) compounded annually.
Advanced Diagnostic and Surgical Center, Inc.
On January 18, 2023, the Company acquired 95 % of the equity interest of Advanced Diagnostic and Surgical Center, Inc. (“ADSC”). ADSC is a diagnostic and surgical center that also provides ambulatory surgery services. Certain Astrana board members previously owned ADSC. The transaction was funded with cash. In addition, the arrangement contains earnout payments. The Company is in the process of finalizing its purchase price allocation.
Employee Stock Purchase Plan (“ESPP”)
On January 1, 2024, the Company’s ESPP came into effect. The Company’s ESPP allows eligible employees to contribute a portion of their eligible earnings toward the semi-annual purchase of the Company’s common stock at a discounted price, subject to an annual maximum dollar amount.
133
Medicare Shared Savings Program (“MSSP”)
Beginning in 2024, in addition to participating in the ACO REACH Model, one of the Company’s ACOs will participate in the Medicare Shared Savings Program (“MSSP”). The MSSP was created to promote accountability and improve coordination of care for Medicare beneficiaries. The MSSP has multiple risk tracks, and the Company is currently participating in the ENHANCED risk track. Much like the ACO REACH Model, under the MSSP Model, the Company recruits a group of Participant and Preferred (in-network) Providers. Based on the Participant Providers that join the Company’s ACO, CMS grants the Company a pool of Traditional Medicare patients (beneficiaries) to manage (the “MSSP Aligned Beneficiaries”). MSSP Aligned Beneficiaries will receive services from physicians and other medical service providers that are both in-network and out-of-network. Unlike the ACO REACH Program, CMS continues to pay participant and preferred providers on a fee-for-service basis for Medicare covered services provided to MSSP Aligned Beneficiaries. However, the Company continues to bear risk on all Medicare expenditures (both in-network and out-of-network), excluding drug expenditures covered by Medicare Part D, based on a budgetary benchmark established with CMS. The Company’s shared savings or losses in managing its beneficiaries are generally determined on an annual basis after reconciliation with CMS.
134
Item 9. Changes in and Disagreements with Accountants on Accounting and Financial Disclosure
None
Item 9A. Controls and Procedures
Evaluation of Disclosure Controls and Procedures
The Company maintains “disclosure controls and procedures,” as defined in Rules 13a-15(e) and 15d-15(e) under the Exchange Act, designed to ensure that information required to be disclosed by a company in the reports filed or submitted under the Exchange Act is recorded, processed, summarized and reported within the time periods specified in the SEC’s rules and forms. Disclosure controls and procedures include, without limitation, controls and procedures designed to ensure that information required to be disclosed by a company in the reports that it files or submits under the Exchange Act is accumulated and communicated to the company’s management, including its principal executive and principal financial officers, as appropriate to allow timely decisions regarding required disclosure. Management recognizes that any controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving their objectives.
As of December 31, 2023, we carried out an evaluation, under the supervision and with the participation of our management, including our Chief Executive Officer and Chief Financial and Operating Officer, of the effectiveness of the design and operation of our disclosure controls and procedures. Based on that evaluation, our management, including our Chief Executive Officer and Chief Financial and Operating Officer, concluded that our disclosure controls and procedures were effective as of December 31, 2023.
Management’s Report on Internal Control Over Financial Reporting
Management is responsible for establishing and maintaining adequate “internal control over financial reporting,” as such term is defined in Exchange Act Rules 13a-15(f) and 15d-15(f). A company’s internal control over financial reporting is a process designed by, or under the supervision of, its principal executive officer and principal financial officer, and effected by such company’s board of directors, management and other personnel to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles and includes those policies and procedures that:
i.Pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company;
ii.Provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles and the receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and
iii.Provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Our management, with the participation of our Chief Executive Officer and Chief Financial and Operating Officer, assessed the effectiveness of our internal control over financial reporting as of December 31, 2023, the end of our fiscal year. Our management based its assessment on criteria established in Internal Control—Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission. Our management’s assessment included evaluation and testing of the design and operating effectiveness of key financial reporting controls, process documentation, accounting policies, and our overall control environment.
Based on our management’s assessment, our management has concluded that our internal control over financial reporting was effective as of December 31, 2023. Our management communicated the results of its assessment to the Audit Committee of our Board of Directors.
135
Our independent registered public accounting firm, Ernst & Young, LLP, audited our consolidated financial statements for the fiscal year ended December 31, 2023 included in this Annual Report on Form 10-K, and has issued an audit report with respect to the effectiveness of the Company’s internal control over financial reporting, a copy of which is included below in this Annual Report on Form 10-K.
Remediation of Previously Reported Material Weakness
The material weakness in our internal control over financial reporting related to the inadequate design of controls associated with the accounting for income taxes, as disclosed in the Company’s Annual Report on Form 10-K/A for the year ended December 31, 2022, has been remediated as of December 31, 2023. Specifically, as of December 31, 2022, the Company did not sufficiently design controls to properly analyze, document, and review the completeness and accuracy of the Company’s assessment of the tax implications of intercompany dividends and the rationale for conclusions with respect to which entities were (or should have been) included in consolidated tax returns.
Management’s remediation actions included, but were not limited to, the following:
i.We implemented controls to ensure the completeness and accuracy of the Company’s tax filing structure.
ii.We designed and implemented relevant controls to enable an effective and timely review of the income tax consequences of intercompany transactions and consolidated tax group determinations. This includes the identification of relevant supporting documentation and the retention of sufficient detailed evidence of review procedures performed.
Changes in Internal Control Over Financial Reporting
Except with respect to the remediation of the material weakness, as described above, there were no changes in our internal control over financial reporting during the quarter ended December 31, 2023 that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
136
Report of Independent Registered Public Accounting Firm
To the Stockholders and the Board of Directors of Astrana Health, Inc.
Opinion on Internal Control Over Financial Reporting
We have audited Astrana Health, Inc.’s (formerly known as Apollo Medical Holdings, Inc.) internal control over financial reporting as of December 31, 2023, based on criteria established in Internal Control—Integrated Framework issued by the Committee of Sponsoring Organizations of the Treadway Commission (2013 framework) (the COSO criteria). In our opinion, Astrana Health, Inc. (the Company) maintained, in all material respects, effective internal control over financial reporting as of December 31, 2023, based on the COSO criteria.
We also have audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (PCAOB), the consolidated balance sheets of the Company as of December 31, 2023 and 2022, the related consolidated statements of income, mezzanine and stockholders' equity (deficit) and cash flows for each of the three years in the period ended December 31, 2023, and the related notes and our report dated February 29, 2024 expressed an unqualified opinion thereon.
Basis for Opinion
The Company’s management is responsible for maintaining effective internal control over financial reporting and for its assessment of the effectiveness of internal control over financial reporting included in the accompanying Management’s Annual Report on Internal Control Over Financial Reporting. Our responsibility is to express an opinion on the Company’s internal control over financial reporting based on our audit. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audit in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects.
Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, testing and evaluating the design and operating effectiveness of internal control based on the assessed risk, and performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
Definition and Limitations of Internal Control Over Financial Reporting
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
| /s/ Ernst & Young LLP | |||||
Los Angeles, California
February 29, 2024
137
Item 9B. Other Information
Rule 10b5-1 Trading Plans
During the three months ended December 31, 2023, none of the Company’s directors or executive officers adopted terminated
Item 9C. Disclosure Regarding Foreign Jurisdictions that Prevent Inspections
Not applicable.
138
PART III
Item 10. Directors, Executive Officers, and Corporate Governance
The information required by this Item will be contained in the Company’s Proxy Statement for the 2024 Annual Meeting to be filed with the SEC not later than 120 days following the end of the Company’s fiscal year ended December 31, 2023, which information is incorporated herein by reference.
The Company has adopted a Code of Ethics that applies to all of its officers, directors and employees. The Code of Ethics is available on the “Investors” section of its website, www.astranahealth.com, under the “Governance—Governance Documents” heading. The Company intends to satisfy the disclosure requirement under Item 5.05 of Form 8-K regarding an amendment to, or waiver from, a provision of its Code of Ethics by posting such information on its website at the web address and location specified above within four business days following the date of the amendment or waiver.
Item 11. Executive Compensation
The information required by this Item will be contained in the Company’s Proxy Statement for the 2024 Annual Meeting to be filed with the SEC not later than 120 days following the end of the Company’s fiscal year ended December 31, 2023, which information is incorporated herein by reference.
Item 12. Security Ownership of Certain Beneficial Owners and Management and Related Stockholder Matters
The information required by this Item will be contained in the Company’s Proxy Statement for the 2024 Annual Meeting to be filed with the SEC not later than 120 days following the end of the Company’s fiscal year ended December 31, 2023, which information is incorporated herein by reference.
Item 13. Certain Relationships and Related Transactions, and Director Independence
The information required by this Item will be contained in the Company’s Proxy Statement for the 2024 Annual Meeting to be filed with the SEC not later than 120 days following the end of the Company’s fiscal year ended December 31, 2023, which information is incorporated herein by reference.
Item 14. Principal Accounting Fees and Services
The information required by this Item will be contained in the Company’s Proxy Statement for the 2024 Annual Meeting to be filed with the SEC not later than 120 days following the end of the Company’s fiscal year ended December 31, 2023, which information is incorporated herein by reference.
139
PART IV
Item 15. Exhibits and Financial Statement Schedules
(a)The following documents are filed as part of this Annual Report on Form 10-K:
1.Consolidated financial statements
The consolidated financial statements and notes thereto contained herein are as listed on the “Index to Consolidated Financial Statements” in Part II, Item 8 of this Annual Report on Form 10-K.
2.Financial Statement Schedules
All financial statement schedules have been omitted, since the required information is not applicable or is not present in amounts sufficient to require submission of the schedule, or because the information required is included in the consolidated financial statements and notes thereto included in this Annual Report on Form 10-K.
3.Exhibits required by Item 601 of Regulation S-K.
140
| Exhibit No. | Description | |||||||
| 3.4 | ||||||||
| 3.5 |
|
|||||||
| 3.6 | ||||||||
| 3.7 | ||||||||
| 3.8 | ||||||||
4.1* |
||||||||
10.1+* |
||||||||
10.2+* |
||||||||
10.3+* |
||||||||
10.4+* |
||||||||
10.5+* |
||||||||
10.6+ |
||||||||
10.7+ |
||||||||
10.8+ |
||||||||
10.9+ |
||||||||
10.10+ |
||||||||
141
142
143
144
145
| Exhibit No. | Description | |||||||
10.58+* |
||||||||
10.59+* |
||||||||
10.60+†* |
||||||||
10.61* |
||||||||
10.62* |
||||||||
19.1* |
||||||||
| 21.1* | ||||||||
| 23.1* | ||||||||
24.1* |
Power of Attorney (included on the signatures page of this Annual Report on Form 10-K). | |||||||
| 31.1* | ||||||||
| 31.2* | ||||||||
| 32** | ||||||||
97.1* |
||||||||
| 101.INS* | Inline XBRL Instance Document | |||||||
| 101.SCH* | Inline XBRL Taxonomy Extension Schema Document | |||||||
| 101.CAL* | Inline XBRL Taxonomy Extension Calculation Linkbase Document | |||||||
| 101.DEF* | Inline XBRL Taxonomy Extension Definition Linkbase Document | |||||||
| 101.LAB* | Inline XBRL Taxonomy Extension Label Linkbase Document | |||||||
| 101.PRE* | Inline XBRL Taxonomy Extension Presentation Linkbase Document | |||||||
| 104* | Cover Page Interactive Data File (the cover page XBRL tags are embedded within the inline XBRL document) | |||||||
* Filed herewith
** Furnished herewith
146
+ Management contract or compensatory plan, contract or arrangement
† Certain of the exhibits and schedules to this exhibit have been omitted in accordance with Regulation S-K Item 601(a)(5). The Company agrees to furnish a copy of all omitted exhibits and schedules to the SEC upon its request.
Item 16. Form 10-K Summary
None.
147
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned, thereunto duly authorized.
ASTRANA HEALTH, INC. |
||||||||
| Date: February 29, 2024 | By: | /s/ Brandon K. Sim, M.S. |
||||||
Brandon K. Sim, M.S. |
||||||||
Chief Executive Officer and President |
||||||||
| (Principal Executive Officer) | ||||||||
148
POWER OF ATTORNEY
KNOW ALL PERSONS BY THESE PRESENTS, that each person whose signature appears below constitutes and appoints, jointly and severally, Brandon K. Sim, M.S., as their true and lawful attorneys-in-fact and agents, with full power of substitution and resubstitution, for him and in his name, place, and stead, in any and all capacities, to sign any and all amendments to this Annual Report on Form 10-K, and to file the same, with all exhibits thereto, and other documents in connection therewith, with the Securities and Exchange Commission, granting unto said attorneys-in-fact and agents, and each of them, full power and authority to do and perform each and every act and thing requisite and necessary to be done in connection therewith, as fully to all intents and purposes as they might or could do in person, hereby ratifying and confirming all that said attorneys-in-fact and agents, or any of them, or their or his substitute or substitutes, may lawfully do or cause to be done by virtue hereof.
Pursuant to the requirements of the Securities Exchange Act of 1934 this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
| SIGNATURE | TITLE | DATE | |||||||||||||||
| By: | /s/ Brandon K. Sim, M.S. |
Chief Executive Officer and President (Principal Executive Officer) |
February 29, 2024 | ||||||||||||||
Brandon K. Sim, M.S. |
|||||||||||||||||
| By: | /s/ Chandan Basho | Chief Financial and Operating Officer (Principal Financial Officer) |
February 29, 2024 | ||||||||||||||
| Chandan Basho | |||||||||||||||||
| By: | /s/ John Vong | Chief Accounting Officer (Principal Accounting Officer) | February 29, 2024 | ||||||||||||||
| John Vong | |||||||||||||||||
| By: | /s/ Kenneth Sim |
Executive Chairman, Director | February 29, 2024 | ||||||||||||||
| Kenneth Sim, M.D | |||||||||||||||||
| By: | /s/ Thomas Lam | Vice Chairman, Director |
February 29, 2024 | ||||||||||||||
| Thomas Lam, M.D., M.P.H. | |||||||||||||||||
| By: | /s/ John Chiang |
Director | February 29, 2024 | ||||||||||||||
| John Chiang | |||||||||||||||||
| By: | /s/ Weili Dai |
Director | February 29, 2024 | ||||||||||||||
| Weili Dai | |||||||||||||||||
| By: | /s/ J. Lorraine Estradas |
Director | February 29, 2024 | ||||||||||||||
| J. Lorraine Estradas | |||||||||||||||||
| By: | /s/ Mitchell Kitayama |
Director | February 29, 2024 | ||||||||||||||
| Mitchell Kitayama | |||||||||||||||||
| By: | /s/ Linda Marsh |
Director | February 29, 2024 | ||||||||||||||
| Linda Marsh | |||||||||||||||||
| By: | /s/ Matthew Mazdyasni |
Director | February 29, 2024 | ||||||||||||||
| Matthew Mazdyasni | |||||||||||||||||
| By: | /s/ David Schmidt |
Director | February 29, 2024 | ||||||||||||||
| David Schmidt | |||||||||||||||||
149